
Abstract
In recent years there has been an increased interest in the immune system as a target for treatment across several psychiatric disorders. To aid this development, methods for patient stratification and treatment monitoring are needed. Positron Emission Tomography (PET) targeting the 18-kD translocator protein (TSPO) is to date the most established method to study brain immune function. In psychosis and schizophrenia, early reports in small samples found evidence for an increase in TSPO, whereas more recent work using radioligands with higher-specific to nonspecific binding ratio has indicated lower levels in patients. In contrast, a series of studies have found higher levels of TSPO in patients with major depressive disorder. Reports of alterations of TSPO in alcohol use disorder, cannabis use, and obsessive-compulsive disorder warrant further research. Methodological limitations such as low signal-to-noise ratio for first-generation radioligands and lack of arterial input function limit the evidential value of some studies. Moreover, the lack of cell-type and functional specificity of TSPO means this biomarker has to be validated for each condition separately.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Molecular imaging
- Immune system
- Translocator protein
- Glial cells
- Schizophrenia
- Depression
- Substance use disorders
1 Introduction
A causative role for the immune system in the manifestation of psychiatric symptoms has been discussed for several decades. Early observations include psychotic symptoms in patients with autoimmune or infectious diseases engaging the brain (Oommen et al. 1982; Felgenhauer 1990) and depressive-like symptoms (also termed “sickness behavior”) in response to experimentally induced immune activation (Reichenberg et al. 2001; Dantzer et al. 2008). Research in psychiatric populations has revealed evidence of genetic (Ripke et al. 2014; Odell et al. 2005; Network and Pathway Analysis Subgroup of Psychiatric Genomics Consortium 2015) and epidemiological (Blomström et al. 2016; Benros et al. 2013) nature in favor of the immune hypothesis, and studies in blood and cerebrospinal fluid (CSF) have shown increases in pro-inflammatory markers across several psychiatric diagnoses (Miller et al. 2011; Mitchell and Goldstein 2014; Dowlati et al. 2010; Enache et al. 2019). Similarly, immune mechanisms have been implicated in experimental studies on alcohol as well as psychostimulants and cannabis (Qin et al. 2008; Thomas et al. 2004; Crews and Vetreno 2016; Mecha et al. 2016). With regard to treatment, initial trials using anti-inflammatory medication in schizophrenia and depression have shown improvement in some cases (Sommer et al. 2012; Husain et al. 2017). However, in order to confirm an engagement of the brain immune system and thus pave the way for causative treatment, more direct methods to quantify the brain immune system are needed.
The 18-kD translocator protein (TSPO), previously known as the peripheral benzodiazepine receptor, is present in mitochondria of mostly glial cells in the brain as well as immune cells in the periphery (Braestrup et al. 1977; Canat et al. 1993). TSPO is expressed in normal conditions and has been shown to be involved in cholesterol transport, but the exact physiological role of the protein is not fully understood. Based on experimental data showing increases in TSPO expression in response to inflammatory stimuli (Venneti et al. 2013), TSPO has been viewed as a marker for immune activation; and therefore Positron Emission Tomography (PET) studies targeting this protein have been the most established method thus far to study brain immune function.
Initial TSPO PET studies were performed using the first-generation TSPO radioligand [11C]PK11195, which was developed in the 1990s. Due to the low signal-to-noise ratio of this tracer, much effort has been invested into the development of second-generation radioligands, with higher brain uptake and specific to nonspecific binding ratios (Imaizumi et al. 2008; Wilson et al. 2008). In early studies using second-generation TSPO radioligands, it was observed that a small proportion of the population did not show specific binding, which was attributed to different polymorphisms of the TSPO gene (Owen et al. 2012). Based on these different genotypes, the population can be classified as high-affinity binders (HABs), mixed-affinity binders (MABs), and low-affinity binders (LABs). Although effects of TSPO genotype had been shown also for [11C]PK11195 in peripheral tissue (Kreisl et al. 2010), the increased sensitivity of second-generation radioligands means that this factor has to be taken into account in the analysis, and also that LAB individuals, corresponding to around 9% of the (western) population, have to be excluded due to insufficient affinity for quantification for most radioligands (Owen et al. 2012).
To date, around 25 studies have been performed where TSPO levels have been directly compared between psychiatric patients and healthy control subjects, the results of which will be summarized in this chapter.
PET studies comparing TSPO binding in psychiatric patients to that of healthy control subjects
Publication | Population | Sample size (P/C) | Medication | Radioligand | Outcome measure | Kinetic model | TSPO genotyped | Statistically significant group differences | Comment (may remove this) |
|---|---|---|---|---|---|---|---|---|---|
Schizophrenia | 10/10 | Medicated | [11C]PK11195 | BPP | 2TCM | No | Total GM ↑ | ||
Schizophrenia | 10/7 | Medicated | [11C]PK11195 | BPND | 2TCM | No | Hippocampus ↑ | ||
Takano et al. (2010) | Schizophrenia | 14/14 | Medicated | [11C]DAA1106 | BPND | 2TCM | No | n.d. | |
Kenk et al. (2014) | Schizophrenia | 27/16 | Medicated | [18F]FEPPA | VT | 2TCM | Yes | n.d. | |
Bloomfield et al. (2016) | Schizophrenia | 14/14 | Medicated | [11C]PBR28 | DVRa/VT | 2TCM-1 | Yes | GM, FC, TC ↑/n.d.b | No difference in VT |
Ultra high risk | 14/14 | DN | [11C]PBR28 | DVRa/VT | 2TCM-1 | Yes | GM, FC, TC ↑/n.d. | ||
Coughlin et al. (2016) | Schizophrenia | 12/14 | Medicated | [11C]DPA713 | VT | 2TCM | Yes | n.d. | |
First episode psychosis | 19/20 | 14 DN, 5 DF | [18F]FEPPA | VT | 2TCM | Yes | n.d. | ||
Schizophrenia | 16/16 | 8 medicated, 6 DN, 2 DF | [11C]PK11195 | BPND | SRTM (CER) | No | n.d. | Increases in medicated patients | |
Van der Doef et al. (2016) | Psychotic disorder | 19/17 | Medicated | [11C]PK11195 | BPND | SRTM (SVCA4) | No | n.d. | |
First episode psychosis | 14/14 | DN | [11C]PBR28 | VT | 2TCM | Yes | GM, FC, TC, hip ↓ | ||
Di Biase et al. (2017) | Schizophrenia | 33/27 | Medicated | [11C]PK11195 | BPND | SRTM (CER) | No | n.d. | |
Ultra high risk | 10/27 | DN | [11C]PK11195 | BPND | SRTM (CER) | No | n.d. | ||
Clinical high risk | 24/23 | 22 DN 2 DF | [18F]FEPPA | VT | 2TCM | Yes | n.d. | ||
Ottoy et al. (2018) | Schizophrenia | 11/17 | Medicated | [11C]PBR111 | VT | 2TCM-1 k | Yes | n.d. | Interaction effect between age and patient status |
Hannestad et al. (2013) | Major depression | 10/10 | 8 medicated 2 DF | [11C]PBR28 | VT | 2TCM | Yes | n.d. | CRP > 3 was exclusion criterion |
Su et al. (2016) | Late-life depression | 5/13 | No data | [11C]PK11195 | BPND | SRTM (CER) | No | L subgenual ACC, R parahippocampus ↑c | No corrections for multiple comparisons |
Holmes et al. (2018) | Major depression | 14/13 | DF | [11C]PK11195 | BPND | SRTM (CER) | No | ACC ↑ | |
Major depression | 50/30d | 11 DN 19 DF? | [18F]FEPPA | VT | 2TCM | Yes | PFC, ACC, insula ↑ | ||
Richards et al. (2018) | Major depression | 28/20 | 16 medicated 12 DF | [11C]PBR28 | VT/fP | 2TCM | Yes | n.d. | Increases in DF |
Major depression | 50/30e | DN | [18F]FEPPA | VT | 2TCM | Yes | GM, WM, FC, TC, Hipp ↑ | ||
Sekine et al. (2008) | Methamphetamine users | 12/12 | N/A | [11C]PK11195 | BPND | SRTMf | No | N/Af | Method and results not valid |
Narendran et al. (2014) | Cocaine users | 15/17 | N/A | [11C]PBR28 | VT | T2CM | Yes | n.d. | |
Kalk et al. (2017) | Alcohol dependence | 9/20 | N/A | [11C]PBR28 | VT | T2CM | Yes | Hippocampus ↓ | |
Hillmer et al. (2017) | Alcohol dependence | 15/15 | N/A | [11C]PBR28 | VT | T2CM | Yes | Cerebellum, FC, striatum, hippocampus ↓ | |
Da Silva et al. (2019) | Cannabis users | 24/27 | N/A | [18F]FEPPA | 0 | T2CM | Yes | PFC, TC, ACC, cerebellum ↑ | |
Suzuki et al. (2013) | Autism | 20/20 | N/A | [11C]PK11195 | BPND | SRTMd | No | N/Af | Method and results not valid |
Haarman et al. (2014) | Bipolar disorder | 14/11 | 13 medicated 1 DF | [11C]PK11195 | BPND | 2TCM | No | R Hippocampus ↑ | |
Attwells et al. (2017) | OCD | 20/20 | DF | [18F]FEPPA | VT | 2TCM | Yes | Striatum, OFC, thalamus, ACC ↑ |
2 Psychotic Disorders
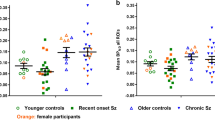
Schizophrenia and psychotic disorders are the psychiatric patient group that have been most extensively studied using TSPO PET, with in total 13 studies encompassing almost 250 patients or individuals at high risk for psychosis. In the first TSPO schizophrenia study by van Berckel et al. in 2008, [11C]PK11195 was used in a sample of ten medicated patients and ten control subjects (van Berckel et al. 2008a). Quantification was performed using a two-tissue compartment (2TCM) model with arterial input function and using the resulting microparameters to calculate binding potential in relation to plasma (BPP) (Innis et al. 2007a). An increase was observed in total gray matter, which was the only region studied. In a subsequent study in a similarly small sample of recent-onset schizophrenia, the same methodology was used, yielding binding potential in relation to non-displaceable binding (PBND). Increased binding was observed in hippocampus, although this effect became evident only after normalizing to total gray matter (Doorduin et al. 2009a).
In the first psychosis study employing a second-generation TSPO radioligand, 14 chronic schizophrenia patients and a corresponding number of control subjects were examined using [11C]DAA1106 (Takano et al. 2010). BPND as quantified using 2TCM showed no difference between groups. However, in this study the TSPO genotype was not known, significantly limiting the interpretability of the results. In another study, the second-generation TSPO radioligand [18F]FEPPA was used in a large group of 18 chronic schizophrenia patients compared to 27 volunteers. Using total distribution volume (VT) derived using 2TCM as outcome, corresponding to total binding in brain in relation to plasma, no difference was found compared to control subjects (Kenk et al. 2014). A subsequent study in high-risk individuals and chronic patients showed increased levels of binding in cortical gray matter regions compared to control subjects (Bloomfield et al. 2016). Here, the authors calculated binding as marginal means derived from a statistical model controlling for binding in whole brain, a relative approach that has been questioned (Narendran and Frankle 2016; Matheson et al. 2017). Notably, VT values in gray matter were numerically lower in both groups compared to control subjects, thus contradicting the conclusions drawn. This was the case both when using 2TCM and 2TCM-1k, a model which proposes to take an irreversible binding component into account.
Since antipsychotic compounds have been known to affect immune function (Drzyzga et al. 2006; Danovich et al. 2008), medication is a potential confounder in all the studies mentioned thus far. Addressing this shortcoming, a study with a combination of 5 untreated and 14 drug-naïve first episode psychosis patients was examined using [18F]FEPPA, finding no difference in VT (Hafizi et al. 2017a). In a following study in 14 antipsychotic-naïve patients using [11C]PBR28, significantly lower levels of VT in patients were observed (Collste et al. 2017a). Additional studies using both [11C]PK11195 and second-generation radioligands in different disease stages also failed to show increases in patients compared to control subjects (Coughlin et al. 2016; Van Der Doef et al. 2016; Holmes et al. 2016a; Di Biase et al. 2017; Ottoy et al. 2018), although one [11C]PK11195 study found elevated binding in a small subgroup of medicated patients (Holmes et al. 2016a). A study in a large group of high-risk individuals, using the second-generation TSPO radioligand [18F]FEPPA, found no differences in binding (Hafizi et al. 2017b), aligning to the results of Bloomfield et al. when using non-normalized binding measures (Bloomfield et al. 2016).
A common problem in PET research is the use of small sample sizes, yielding limited power to detect true differences, as well as increasing the risk for false positives. To address this limitation, individual participant TSPO data was combined from five studies using second-generation TSPO radioligands in schizophrenia or first episode psychosis patients. Strong evidence was obtained for a decrease in TSPO in gray matter regions, with effect sizes ranging from −0.47 to −0.63 (Plavén-Sigray et al. 2018a). No effect of antipsychotic medication on VT was observed. An additional meta-analysis using summary statistics found evidence of increases in binding in [11C]PK11195 studies and no difference in second-generation TSPO radioligand studies (Marques et al. 2019). However, due to methodological caveats of [11C]PK11195 discussed below, the evidential value of the [11C]PK11195 studies is limited (Plavén-Sigray and Cervenka 2019).
Taken together, the overall evidence is in favor of lower TSPO binding in psychosis patients. Although the underlying biology is unclear, this suggests altered function of brain glial cells in psychosis. It has been hypothesized that the causative role of immune factors in schizophrenia may be related to microglia-mediated excessive synaptic pruning, which may explain the cortical thinning and synaptic loss observed in MR and postmortem studies (Sekar et al. 2016; Cannon 2015; Sellgren et al. 2019; Glausier and Lewis 2013). Thus far, two studies have investigated the relationship between TSPO and brain structure in psychosis spectrum patients. Selvaraj et al. showed a relationship between TSPO binding and total cortical GM volume; however this was using the relative measure of TSPO binding which means that the interpretation of the findings is unclear (Selvaraj et al. 2018). In a much larger cohort of in total 90 clinical high-risk individuals, first episode psychosis patients and control subjects, associations were observed between TSPO binding and outward and inward morphological alterations in hippocampus, representing the first association between a brain immune marker and structural morphology (Hafizi et al. 2018).
3 Depression
During recent years, TSPO PET has been applied increasingly also in patients with major depressive disorder (MDD). In the first report published, Hannestad et al. used [11C]PBR28 to examine ten MDD patients and ten control subjects (Hannestad et al. 2013). No group difference was observed, either when using a one-tissue compartment (1TCM), 2TCM or the multilinear analysis MA1 to derive VT, or after correcting for free fraction. Apart from the limitation of a small sample size, in this study elevated C-reactive protein was used as an exclusion criterion, which may have influenced the results. Moreover, patients showed only mild-to-moderate symptom severity at time of scanning, which represented a reduction from screening. Subsequently, Setiawan et al. used [18F]FEPPA to study 20 medication-free patients with major depression (MD), compared to 20 control subjects (Setiawan et al. 2015). Increases in TCM-derived VT were shown in prefrontal cortex, anterior cingulate (ACC), and insula. Symptom scores were positively correlated to TSPO VT in the ACC, after correcting for genotype. The results of elevated TSPO were later confirmed when adding additional 30 patients and 5 controls to the same sample (Setiawan et al. 2018). In a study using [11C]PK11195 in 14 patients with depression and 13 controls, BPND was quantified using cerebellum as reference region in a simplified reference tissue model (Holmes et al. 2018). Significantly higher binding was found in ACC in patients, although the absolute difference in binding was low. Using similar methodology, increases in [11C]PK11195 was observed in five individuals with late-life depression, although the very small sample size as well as a lack of control for multiple comparisons limits the interpretability (Su et al. 2016). In an additional study using [11C]PBR28, in 28 patients and 20 controls, no significant difference between groups, using plasma fraction-corrected VT as outcome measure. However, a post hoc analysis revealed increased VT in a subgroup of 16 patients with ongoing antidepressant medication (Richards et al. 2018). Finally, in 2 publications based on overlapping samples, in cluding a total of 50 MDD patients and 30 HC were examined using [18F]FEPPA. Increases were observed in GM, WM, frontal and temporal cortices, as well as hippocampus (Li et al. 2018a, b).
Recently, results from TSPO PET studies in depression were analyzed in a summary statistics meta-analysis, showing increases in TSPO density in ACC, TC, FC, insula, and hippocampus with a standardized effect size of 0.71 (Enache et al. 2019). Interestingly, it was suggested that TSPO increases in depression may reflect increased recruitment of peripheral monocytes, which is in line with experimental data showing alterations in blood-brain barrier integrity in chronic social stress (Menard et al. 2017).
4 Substance Use Disorders
Based on animal studies showing an involvement of microglia in the neurotoxic effects of alcohol and psychostimulants, efforts have been made to investigate TSPO levels in individuals with substance use disorders. An initial study used [11C]PK11195 to examine 12 methamphetamine users and 12 healthy control subjects (Sekine et al. 2008). BPND was calculated using SRTM, with averaged TACs from cortical regions from the control group as reference input. BPND increases in patients ranged from 3- to 15-fold. Importantly, the unorthodox choice of reference region means that differences in delivery of radioligand to brain as well as nonspecific binding cannot be controlled for, severely limiting the interpretability of the results. In a subsequent study using [11C]PBR28, Narendran et al. investigated 15 chronic cocaine abusers in comparison with 17 control subjects (Narendran et al. 2014). VT was calculated using 2TCM, showing no difference between groups.
[11C]PBR28 has been used in two recent studies on alcohol dependence. Kalk et al. examined 9 patients within 1 month of withdrawal and 20 control subjects, showing significantly lower VT in hippocampus in patients (Kalk et al. 2017). In a similar study, 15 patients were examined within 1–4 days (n = 14) or 24 days (n = 1) after their last drink and compared to 15 control subjects (Hillmer et al. 2017). Again, contrary to the initial hypothesis, decreases in VT in patients were observed in hippocampus, striatum, frontal cortex, and cerebellum. In the latter study, PET data was paralleled by reduced cytokine expression in cultured monocytes after stimulation with lipopolysaccharide, in a subgroup of subjects.
Finally, following experimental data showing that the cannabinoid system can modulate immune responses, [18F]FEPPA and PET were very recently used to examine 24 chronic cannabis users and 27 controls (Da Silva et al. 2019). VT was higher across all regions examined a priori, with more prominent effects for individuals who met criteria for cannabis use disorder. TSPO levels were positively correlated with increased blood CRP levels as well as subjective measures of stress and anxiety.
5 Other Disorders
To date, one study investigated TSPO in developmental disorders. Suzuki et al. used [11C]PK11195 to examine 20 individuals with autism spectrum disorders and 20 matched controls. BPND was quantified using SRTM, with averaged cerebellar TACs from the control group as input function for both patients and control subjects. Increases in BPND were reported in all brain regions examined. As commented above, no clear conclusions can be drawn due to the use of this reference region approach.
Using the same radioligand, Haarman et al. examined 14 bipolar type I patients compared to 11 healthy controls (Haarman et al. 2014). All patients except one were euthymic, and 13 were taking mood stabilizers. BPND was quantified using 2TCM with an arterial input function, estimated as k3/k4. Binding in whole brain gray matter was used as a covariate to reduce variability. Hippocampus was selected as the main ROI and showed increases on the right side in patients. No other brain region reached statistical significance.
Finally, a recent study examined TSPO in a group of 20 patients with obsessive-compulsive disorder and 20 control subjects, using [18F]FEPPA (Attwells et al. 2017). None of the patients were on medication. VT as quantified using 2TCM was higher in striatum, orbitofrontal cortex, thalamus, as well as ACC. A correlation was observed between symptom severity and TSPO levels in orbitofrontal cortex, although this was not corrected for multiple comparisons.
6 Methodological Considerations
When interpreting the results from TSPO PET imaging, there are some methodological aspects to consider. In the field of psychosis and schizophrenia, apparent different results have been obtained using [11C]PK11195 compared to that of second-generation TSPO radioligands, necessitating a closer inspection of the differences in characteristics between these tracers. By performing PET experiments where the specific binding is blocked using a cold compound, the ratio between specific and non-displaceable (background) binding, referred to as non-displaceable binding potential (BPND) (Innis et al. 2007b), can be estimated. For [11C]PK11195, this approach has yielded BPND values in the range of 0.7–0.8 in healthy control subjects, suggesting that the background signal is proportionally larger than target signal (Kobayashi et al. 2017). This ratio is significantly lower than has been reported for the second-generation TSPO radioligands [11C]PBR28 (Plavén-Sigray et al. 2019; Owen et al. 2014), [11C]DPA713 (Kobayashi et al. 2017), and the more recently developed [11C]ER176 (Ikawa et al. 2017). Importantly, a consequence of lower signal-to-noise ratio means lower accuracy and reliability of the measurement.
A second caveat when interpreting TSPO PET results relates to the difference in quantification methods between studies. An important premise for TSPO quantification is that there is no reference region devoid of TSPO in the brain (Doble et al. 1987). This means that arterial blood sampling is necessary to establish the delivery of radioligand to brain, permitting kinetic modeling of the time activity curve data. Using this method, the gold standard outcome is considered to be the total distribution volume (VT), which is an estimate of radioligand binding in relation to plasma. Since arterial sampling can be cumbersome and technically difficult, attempts have been made to find simplified methods of analysis. For the majority of [11C]PK11195 studies in psychiatric disorders, reference tissue approaches have been used, either using the cerebellum as “pseudoreference” region (Di Biase et al. 2017; Holmes et al. 2016b, 2018; Su et al. 2016) or deriving an input function using cluster analysis (Van Der Doef et al. 2016; Di Biase et al. 2017). Using a test-retest dataset in healthy control subjects, these approaches showed intraclass correlation coefficient values in the range of 0.3–0.5 (Plavén-Sigray et al. 2018b), suggesting that at least half of the variability in BPND is due to measurement error. Moreover, there was a lack of correlation between BPND and BP calculated using microparameters, as employed in studies in psychosis and bipolar disorder (Haarman et al. 2014; van Berckel et al. 2008b; Doorduin et al. 2009b), and VT. Thus, in absence of clear increases in TSPO, the combination of low specific binding and suboptimal methods of quantification, we suggest that results from [11C]PK11195 studies should be interpreted with caution. As mentioned above, two [11C]PK11195 studies also used TACs from the control group as input function for the whole sample, creating further problems for interpretation (Sekine et al. 2008; Suzuki et al. 2013).
In studies using second-generation TSPO radioligands such as [11C]PBR28, one approach to reduce variability in the data has been to calculate ratios between binding in target region and reference region, using standardized uptake values (SUVR) or VT (DVR) (Lyoo et al. 2015). A drawback of this relative approach is that the resulting values are sensitive to changes in the normalizing region (Narendran and Frankle 2016). Moreover, a study in healthy controls suggested that in absence of clear increases, the high intercorrelation between binding in target and “normalizing” regions means that much of the biological signal is lost, leading to low reliability and low correlation to the gold standard VT measurement (Matheson et al. 2017). In one study in psychosis and ultra-high-risk individuals, yet another approach was used whereby VT in the normalizing region was entered as a covariate in the statistical model, and DVR was extracted as predicted values (Bloomfield et al. 2016). When the target region is included in the normalizing region, the regional intercorrelation is likely to increase, further reducing signal-to-noise.
One potential caveat that has been discussed when using arterial blood as input function for quantification is that peripheral inflammation may lead to biased results. Based on in vitro studies showing binding of [11C]PK11195 to acute phase proteins (Lockhart et al. 2003), it has been hypothesized that inflammation may lead to increased protein binding, such that the true input function is overestimated, leading to false low values of binding in brain. However, there is to date no study showing a clear effect of free fraction on VT. Instead, in a study by Sandiego and co-workers using the pro-inflammatory agent lipopolysaccharide (LPS) (Sandiego et al. 2015), there was no increase in radioligand binding to plasma proteins, despite a clear peripheral pro-inflammatory activation. The arterial input function was decreased, which is expected due to the increase in peripheral binding, whereas brain VT was increased. Similarly, at least three of the clinical studies reviewed above showed decreases in brain VT in patients in absence of changes in radioligand protein binding, despite previous research showing peripheral increases in pro-inflammatory markers in these populations (Kalk et al. 2017; Hillmer et al. 2017; Collste et al. 2017b). Further investigations into the effect of peripheral immune activation on central TSPO binding are warranted.
Considering the sometimes surprising findings of reduction in TSPO in clinical studies, additional work has been directed towards understanding the underlying biology. First, it has become clear that TSPO is not specific for microglial activation. The protein is expressed in astrocytes (Toth et al. 2016; Lavisse et al. 2012; Notter et al. 2018a) as well as in vascular cells (Veronese et al. 2017) and to some extent in neurons (Notter et al. 2018b). Second, animal and in vitro human data has challenged the view of TSPO as a specific pro-inflammatory marker. In a mouse model of low-grade immune activation, TSPO was found to be decreased, despite elevated levels of classical pro-inflammatory markers such as IL-1b and IL-6 (Notter et al. 2018a). In vitro assays of human cells have shown that TSPO may not increase upon stimulation with LPS (Narayan et al. 2017) and might even show decreased levels (Owen et al. 2017). Finally, the physiological role of TSPO may present yet another confounder. Recently, a large multicenter study of [11C]PBR28 in healthy control subjects (Tuisku et al. 2019) found that radioligand binding was associated to increasing age, confirming findings that were evident in some, but not all previous studies (Paul et al. 2019; Suridjan et al. 2014). Moreover, relationships were found also for BMI and sex results that may reflect the suggested role of TSPO in hormone production.
7 Conclusions
The increasing application of TSPO PET in psychiatric populations during recent years has led to the emergence of some patterns that appear to vary between disorders. The evidence is in favor of an increase in TSPO in depression, whereas psychosis patients and potentially also subjects with alcohol use disorder show decreases. Additional understanding of the underlying biology is now needed to fully interpret these findings. It is likely that new cell and activation-specific PET markers need to be developed in order to robustly assess pro-inflammatory brain immune activation.
The large interindividual variability in TSPO in combination with the small samples usually employed in PET research means that power is often lacking. For instance, for studies employing second-generation TSPO tracers to study psychosis patients, the power to detect a medium-size effect was 23–34% (Plavén-Sigray et al. 2018a). This may lead to the failure to detect clinically meaningful effects but equally increase the risk of false positives that are not replicated in subsequent studies (Button et al. 2013). Since larger samples may be unattainable for individual research centers, one important way forward is to further develop multicenter collaborations where data is pooled at the individual participant level. Apart from increasing power, this would also open up for investigations into subgroups of patients, also across diagnostic boundaries, possibly stratifying patients into different etiopathologies.
References
Attwells S, Setiawan E, Wilson AA, Rusjan PM, Mizrahi R et al (2017) Inflammation in the Neurocircuitry of Obsessive-Compulsive Disorder. JAMA Psychiatry. 74(8):833–840. https://doi.org/10.1001/jamapsychiatry.2017.1567. PMID: 28636705
Benros ME, Waltoft BL, Nordentoft M, Ostergaard SD, Eaton WW et al (2013) Autoimmune diseases and severe infections as risk factors for mood disorders: a nationwide study. JAMA Psychiatry [Internet] 70(8):812–820. [Cited 2015 Jun 23]. http://archpsyc.jamanetwork.com.proxy.kib.ki.se/article.aspx?articleid=1696348
Blomström Å, Karlsson H, Gardner R, Jörgensen L, Magnusson C, Dalman C (2016) Associations between maternal infection during pregnancy, childhood infections, and the risk of subsequent psychotic disorder—a Swedish cohort study of nearly 2 million individuals. Schizophr Bull 42(1):125–133
Bloomfield PS, Selvaraj S, Veronese M, Rizzo G, Bertoldo A et al (2016) Microglial activity in people at ultra high risk of psychosis and in schizophrenia: an [11C]PBR28 PET brain imaging study. Am J Psychiatry [Internet] 173(1):44–52. http://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2015.14101358
Braestrup C, Albrechtsen R, Squires RF (1977) High densities of benzodiazepine receptors in human cortical areas. Nature [Internet] 269(5630):702–704. [Cited 2019 May 9]. http://www.nature.com/articles/269702a0
Button KS, Ioannidis JPA, Mokrysz C, Nosek BA, Flint J et al (2013) Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci [Internet] 14(5):365–376. http://www.ncbi.nlm.nih.gov/pubmed/23571845
Canat X, Carayon P, Bouaboula M, Cahard D, Shire D et al (1993) Distribution profile and properties of peripheral-type benzodiazepine receptors on human hemopoietic cells. Life Sci 52(1):107–118
Cannon TD (2015) How schizophrenia develops: cognitive and brain mechanisms underlying onset of psychosis. Trends Cogn Sci [Internet] 19(12):744–756. https://doi.org/10.1016/j.tics.2015.09.009
Collste K, Plavén-Sigray P, Fatouros-Bergman H, Victorsson P, Schain M et al (2017a) Lower levels of the glial cell marker TSPO in drug-naive first-episode psychosis patients as measured using PET and [ 11 C]PBR28. Mol Psychiatry [Internet] 22(6):850–856. [Cited 2017 May 30]. http://www.ncbi.nlm.nih.gov/pubmed/28194003
Collste K, Plavén-Sigray P, Fatouros-Bergman H, Victorsson P, Schain M et al (2017b) Lower levels of the glial cell marker TSPO in drug-naive first-episode psychosis patients as measured using PET and [11C]PBR28. Mol Psychiatry [Internet] 22(6):850–856. [Cited 2019 May 1]. http://www.nature.com/doifinder/10.1038/mp.2016.247
Coughlin JM, Wang Y, Ambinder EB, Ward RE, Minn I et al (2016) In vivo markers of inflammatory response in recent-onset schizophrenia: a combined study using [ 11 C] DPA-713 PET and analysis of CSF and plasma. Transl Psychiatry 6(4):e777
Crews FT, Vetreno RP (2016) Mechanisms of neuroimmune gene induction in alcoholism. Psychopharmacology (Berl) 233(9):1543–1557
Da Silva T, Hafizi S, Watts JJ, Weickert CS, Meyer JH et al (2019) In vivo imaging of translocator protein in chronic cannabis users. JAMA Psychiatry 76(12):1305–1313
Danovich L, Veenman L, Leschiner S, Lahav M, Shuster V et al (2008) The influence of clozapine treatment and other antipsychotics on the 18 kDa translocator protein, formerly named the peripheral-type benzodiazepine receptor, and steroid production. Eur Neuropsychopharmacol 18(1):24–33
Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW (2008) From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci 9(1):46–56
Di Biase MA, Zalesky A, O’keefe G, Laskaris L, Baune BT et al (2017) PET imaging of putative microglial activation in individuals at ultra-high risk for psychosis, recently diagnosed and chronically ill with schizophrenia. Transl Psychiatry [Internet] 7(8):e1225. [Cited 2019 May 3]. http://www.nature.com/doifinder/10.1038/tp.2017.193
Doble A, Malgouris C, Daniel M, Daniel N, Imbault F et al (1987) Labelling of peripheral-type benzodiazepine binding sites in human brain with [3H]PK 11195: anatomical and subcellular distribution. Brain Res Bull [Internet] 18(1):49–61. http://www.ncbi.nlm.nih.gov/pubmed/3030512
Doorduin J, de Vries EFJ, Willemsen ATM, de Groot JC, Dierckx RA, Klein HC (2009a) Neuroinflammation in schizophrenia-related psychosis: a PET study. J Nucl Med [Internet] 50(11):1801–1807. [Cited 2012 Feb 9]. http://www.ncbi.nlm.nih.gov/pubmed/19837763
Doorduin J, de Vries EFJ, Willemsen ATM, de Groot JC, Dierckx RA, Klein HC (2009b) Neuroinflammation in schizophrenia-related psychosis: a PET study. J Nucl Med 50(11):1801–1807
Dowlati Y, Herrmann N, Swardfager W, Liu H, Sham L et al (2010) A meta-analysis of cytokines in major depression. Biol Psychiatry [Internet] 67(5):446–457. https://doi.org/10.1016/j.biopsych.2009.09.033
Drzyzga L, Obuchowicz E, Marcinowska A, Herman ZS (2006) Cytokines in schizophrenia and the effects of antipsychotic drugs. Brain Behav Immun 20:532–545
Enache D, Pariante CM, Mondelli V (2019) Markers of central inflammation in major depressive disorder: a systematic review and meta-analysis of studies examining cerebrospinal fluid, positron emission tomography and post-mortem brain tissue. Brain Behav Immun 81:24–40
Felgenhauer K (1990) Psychiatric disorders in the encephalitic form of multiple sclerosis. J Neurol [Internet] 237(1):11–18. [Cited 2015 Jul 2]. http://www.ncbi.nlm.nih.gov/pubmed/2156956
Glausier JR, Lewis DA (2013) Dendritic spine pathology in schizophrenia. Neuroscience 251:90–107
Haarman BBCM, Riemersma-Van der Lek RF, Burger H, Netkova M, Drexhage RC et al (2014) Relationship between clinical features and inflammation-related monocyte gene expression in bipolar disorder—towards a better understanding of psychoimmunological interactions. Bipolar Disord 16(2):137–150
Hafizi S, Tseng H-H, Rao N, Selvanathan T, Kenk M et al (2017a) Imaging microglial activation in untreated first-episode psychosis: a pet study with [18F]FEPPA. Am J Psychiatry [Internet] 174(2):118–124. http://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2016.16020171
Hafizi S, Gerritsen C, Kiang M, Michael R, Prce I et al (2017b) Imaging microglial activation in individuals at clinical high risk for psychosis: an in-vivo PET study with [ 18 F]FEPPA. Running title: Microglial activation in clinical high risk. Neuropsychopharmacology 42(13):2474–2481
Hafizi S, Guma E, Koppel A, Da Silva T, Kiang M et al (2018) TSPO expression and brain structure in the psychosis spectrum. Brain Behav Immun [Internet] 74:79–85. [Cited 2018 Jul 20]. http://www.ncbi.nlm.nih.gov/pubmed/29906515
Hannestad J, DellaGioia N, Gallezot JD, Lim K, Nabulsi N et al (2013) The neuroinflammation marker translocator protein is not elevated in individuals with mild-to-moderate depression: a [11C]PBR28 PET study. Brain Behav Immun 33:131–138
Hillmer AT, Sandiego CM, Hannestad J, Angarita GA, Kumar A et al (2017) In vivo imaging of translocator protein, a marker of activated microglia, in alcohol dependence. Mol Psychiatry [Internet] 22(12):1759–1766. http://www.nature.com/doifinder/10.1038/mp.2017.10
Holmes SE, Hinz R, Drake RJ, Gregory CJ, Conen S et al (2016a) In vivo imaging of brain microglial activity in antipsychotic-free and medicated schizophrenia: a [ 11 C](R)-PK11195 positron emission tomography study. Mol Psychiatry [Internet] 21(12):1672–1679. http://www.nature.com/doifinder/10.1038/mp.2016.180
Holmes SE, Hinz R, Drake RJ, Gregory CJ, Conen S et al (2016b) In vivo imaging of brain microglial activity in antipsychotic-free and medicated schizophrenia: a [11C](R)-PK11195 positron emission tomography study. Mol Psychiatry [Internet] 21(12):1672–1679. [Cited 2019 May 3]. http://www.nature.com/articles/mp2016180
Holmes SE, Conen S, Gregory CJ, Gerhard A, Talbot PS et al (2018) Elevated translocator protein in anterior cingulate in major depression and a role for inflammation in suicidal thinking: a positron emission tomography study. Biol Psychiatry 83(1):61–69
Husain MI, Strawbridge R, Stokes PR, Young AH (2017) Anti-inflammatory treatments for mood disorders: systematic review and meta-analysis. J Psychopharmacol 31(9):1137–1148
Ikawa M, Lohith TG, Shrestha S, Telu S, Zoghbi SS, Castellano S (2017) 11C-ER176, a radioligand for 18-kDa translocator protein, has adequate sensitivity to robustly image all three affinity genotypes in human brain. J Nucl Med 58(2):320–325
Imaizumi M, Briard E, Zoghbi SS, Gourley JP, Hong J et al (2008) Brain and whole-body imaging in nonhuman primates of [ 11 C]PBR28, a promising PET radioligand for peripheral benzodiazepine receptors. Neuroimage 39(3):1289–1298
Innis RB, Cunningham VJ, Delforge J, Fujita M, Gjedde A et al (2007a) Consensus nomenclature for in vivo imaging of reversibly binding radioligands. J Cereb Blood Flow Metab [Internet] 27(9):1533–1539. http://www.ncbi.nlm.nih.gov/pubmed/17519979
Innis RB, Cunningham VJ, Delforge J, Fujita M, Gjedde A et al (2007b) Consensus nomenclature for in vivo imaging of reversibly binding radioligands. J Cereb Blood Flow Metab 27(9):1533–1539
Kalk NJ, Guo Q, Owen D, Cherian R, Erritzoe D et al (2017) Decreased hippocampal translocator protein (18 kDa) expression in alcohol dependence: a [11C]PBR28 PET study. Transl Psychiatry [Internet] 7(1):e996. http://www.ncbi.nlm.nih.gov/pubmed/28072413%0A; http://www.nature.com/doifinder/10.1038/tp.2016.264
Kenk M, Selvanathan T, Rao N, Suridjan I, Rusjan P et al (2014) Imaging neuroinflammation in gray and white matter in schizophrenia: an in-vivo PET study with [18F]-FEPPA. Schizophr Bull 41(1):85–93
Kobayashi M, Jiang T, Telu S, Zoghbi SS, Gunn RN et al (2017) 11C-DPA-713 has much greater specific binding to translocator protein 18 kDa (TSPO) in human brain than 11C-(R)-PK11195. J Cereb Blood Flow Metab 38(3):393–403
Kreisl WC, Fujita M, Fujimura Y, Kimura N, Jenko KJ et al (2010) Comparison of [(11)C]-(R)-PK 11195 and [(11)C]PBR28, two radioligands for translocator protein (18 kDa) in human and monkey: implications for positron emission tomographic imaging of this inflammation biomarker. Neuroimage [Internet] 49(4):2924–2932. http://www.ncbi.nlm.nih.gov.proxy.kib.ki.se/pubmed/19948230
Lavisse S, Guillermier M, He A, Petit F, Delahaye M et al (2012) Reactive astrocytes overexpress TSPO and are detected by TSPO positron emission tomography imaging. J Neurosci 32(32):10809–10818
Li H, Sagar AP, Kéri S (2018a) Microglial markers in the frontal cortex are related to cognitive dysfunctions in major depressive disorder. J Affect Disord 241:305–310
Li H, Sagar AP, Kéri S (2018b) Translocator protein (18 kDa TSPO) binding, a marker of microglia, is reduced in major depression during cognitive-behavioral therapy. Prog Neuropsychopharmacology Biol Psychiatry 83:1–7
Lockhart A, Davis B, Matthews JC, Rahmoune H, Hong G et al (2003) The peripheral benzodiazepine receptor ligand PK11195 binds with high affinity to the acute phase reactant α1-acid glycoprotein: implications for the use of the ligand as a CNS inflammatory marker. Nucl Med Biol 30(2):199–206
Lyoo CH, Ikawa M, Liow J-S, Zoghbi SS, Morse CL et al (2015) Cerebellum can serve as a pseudo-reference region in Alzheimer disease to detect neuroinflammation measured with PET radioligand binding to translocator protein. J Nucl Med 56(5):701–706
Marques TR, Ashok AH, Pillinger T, Veronese M, Turkheimer FE et al (2019) Neuroinflammation in schizophrenia: meta-analysis of in vivo microglial imaging studies. Psychol Med [Internet] 49(13):2186–2196. https://www.cambridge.org/core/product/identifier/S0033291718003057/type/journal_article
Matheson GJ, Plavén-Sigray P, Forsberg A, Varrone A, Farde L, Cervenka S (2017) Assessment of simplified ratio-based approaches for quantification of PET [ 11 C]PBR28 data. EJNMMI Res 7:58
Mecha M, Carrillo-Salinas FJ, Feliú A, Mestre L, Guaza C (2016) Microglia activation states and cannabinoid system: therapeutic implications. Pharmacol Ther 166:40–55
Menard C, Pfau ML, Hodes GE, Kana V, Wang VX et al (2017) Social stress induces neurovascular pathology promoting depression. Nat Neurosci 20(12):1752–1760
Miller BJ, Buckley P, Seabolt W, Mellor A, Kirkpatrick B (2011) Meta-analysis of cytokine alterations in schizophrenia: clinical status and antipsychotic effects. Biol Psychiatry [Internet] 70(7):663–671. [Cited 2014 Oct 17]. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4071300&tool=pmcentrez&rendertype=abstract
Mitchell RHB, Goldstein BI (2014) Inflammation in children and adolescents with neuropsychiatric disorders: a systematic review. J Am Acad Child Adolesc Psychiatry [Internet] 53(3):274–296. https://doi.org/10.1016/j.jaac.2013.11.013
Narayan N, Mandhair H, Smyth E, Dakin SG, Kiriakidis S et al (2017) The macrophage marker translocator protein (TSPO) is down-regulated on pro-inflammatory ‘M1’ human macrophages. PLoS One 12(10):e0185767
Narendran R, Frankle WG (2016) Comment on analyses and conclusions of “microglial activity in people at ultra high risk of psychosis and in schizophrenia: an [11C]PBR28 PET brain imaging study”. Am J Psychiatry [Internet] 173(5):536–537. http://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2016.15111417
Narendran R, Lopresti BJ, Mason NS, Deuitch L, Paris J et al (2014) Cocaine abuse in humans is not associated with increased microglial activation: an 18-kDa translocator protein positron emission tomography imaging study with [11C]PBR28. J Neurosci 34(30):9945–9950
Network and Pathway Analysis Subgroup of Psychiatric Genomics Consortium (2015) Psychiatric genome-wide association study analyses implicate neuronal, immune and histone pathways. Nat Neurosci [Internet] 18(2):199–209. [Cited 2015 Jul 20]. http://www.nature.com.proxy.kib.ki.se/neuro/journal/v18/n2/full/nn.3922.html#ref22
Notter T, Coughlin JM, Gschwind T, Weber-Stadlbauer U, Wang Y et al (2018a) Translational evaluation of translocator protein as a marker of neuroinflammation in schizophrenia. Mol Psychiatry [Internet] 23(2):323–334. http://www.nature.com/doifinder/10.1038/mp.2016.248
Notter T, Coughlin JM, Sawa A, Meyer U (2018b) Reconceptualization of translocator protein as a biomarker of neuroinflammation in psychiatry. Mol Psychiatry 23(1):36
Odell D, Maciulis A, Cutler A, Warren L, McMahon WM et al (2005) Confirmation of the association of the C4B null allelle in autism. Hum Immunol [Internet] 66(2):140–145. [Cited 2015 Jul 2]. http://www.sciencedirect.com/science/article/pii/S0198885904006809
Oommen KJ, Johnson PC, Ray CG (1982) Herpes simplex type 2 virus encephalitis presenting as psychosis. Am J Med [Internet] 73(3):445–448. [Cited 2015 Jul 2]. http://www.ncbi.nlm.nih.gov/pubmed/7124772
Ottoy J, De Picker L, Verhaeghe J, Deleye S, Wyffels L et al (2018) 18 F-PBR111 PET imaging in healthy controls and schizophrenia: test–retest reproducibility and quantification of neuroinflammation. J Nucl Med [Internet] 59(8):1267–1274. [Cited 2019 May 12]. http://www.ncbi.nlm.nih.gov/pubmed/29326362
Owen DR, Yeo AJ, Gunn RN, Song K, Wadsworth G et al (2012) An 18-kDa translocator protein (TSPO) polymorphism explains differences in binding affinity of the PET radioligand PBR28. J Cereb Blood Flow Metab [Internet] 32(1):1–5. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3323305&tool=pmcentrez&rendertype=abstract
Owen DR, Guo Q, Kalk NJ, Colasanti A, Kalogiannopoulou D et al (2014) Determination of [11C]PBR28 binding potential in vivo: a first human TSPO blocking study. J Cereb Blood Flow Metab 34(6):989–994
Owen DR, Narayan N, Wells L, Healy L, Smyth E et al (2017) Pro-inflammatory activation of primary microglia and macrophages increases 18 kDa translocator protein expression in rodents but not humans. J Cereb Blood Flow Metab 37(8):2679–2690
Paul S, Gallagher E, Liow JS, Mabins S, Henry K et al (2019) Building a database for brain 18 kDa translocator protein imaged using [11C]PBR28 in healthy subjects. J Cereb Blood Flow Metab 39(6):1138–1147
Plavén-Sigray P, Cervenka S (2019) Meta-analytic studies of the glial cell marker TSPO in psychosis—a question of apples and pears? Psychol Med 49(10):1624–1628
Plavén-Sigray P, Matheson GJ, Collste K, Ashok AH, Coughlin JM et al (2018a) Positron emission tomography studies of the glial cell marker translocator protein in patients with psychosis: a meta-analysis using individual participant data. Biol Psychiatry [Internet] 84(6):433–442. [Cited 2018 Aug 30]. https://linkinghub.elsevier.com/retrieve/pii/S0006322318312988
Plavén-Sigray P, Matheson GJ, Cselényi Z, Jučaite A, Farde L, Cervenka S (2018b) Test-retest reliability and convergent validity of (R)-[11C] PK11195 outcome measures without arterial input function. EJNMMI Res 8:102
Plavén-Sigray P, Schain M, Zanderigo F, Rabiner I, Gunn R et al (2019) Accuracy and reliability of [11C] PBR28 specific binding estimated without the use of a reference region. Neuroimage 188:102–110
Qin L, He J, Hanes RN, Pluzarev O, Hong J-S, Crews FT (2008) Increased systemic and brain cytokine production and neuroinflammation by endotoxin following ethanol treatment. J Neuroinflammation 5(1):10
Reichenberg A, Yirmiya R, Schuld A, Kraus T, Haack M et al (2001) Cytokine-associated emotional and cognitive disturbances in humans. Arch Gen Psychiatry [Internet] 58(5):445–452. http://www.ncbi.nlm.nih.gov/pubmed/11343523
Richards EM, Zanotti-Fregonara P, Fujita M, Newman L, Farmer C et al (2018) PET radioligand binding to translocator protein (TSPO) is increased in unmedicated depressed subjects. EJNMMI Res 8:57
Ripke S, Neale BM, Corvin A, Walters JTR, Farh K-H et al. Biological insights from 108 schizophrenia-associated genetic loci. Nature [Internet]. 2014. [Cited 2014 Jul 22]. http://www.nature.com/doifinder/10.1038/nature13595
Sandiego CM, Gallezot J-D, Pittman B, Nabulsi N, Lim K et al (2015) Imaging robust microglial activation after lipopolysaccharide administration in humans with PET. Proc Natl Acad Sci [Internet] 112(40):12468–12473. http://www.pnas.org/lookup/doi/10.1073/pnas.1511003112
Sekar A, Bialas AR, de Rivera H, Davis A, Hammond TR et al (2016) Schizophrenia risk from complex variation of complement component 4. Nature [Internet] 530(7589):177–183. http://www.ncbi.nlm.nih.gov/pubmed/26814963
Sekine Y, Ouchi Y, Sugihara G, Takei N, Yoshikawa E et al (2008) Methamphetamine causes microglial activation in the brains of human abusers. J Neurosci 28(22):5756–5761
Sellgren CM, Gracias J, Watmuff B, Biag JD, Thanos JM et al (2019) Increased synapse elimination by microglia in schizophrenia patient-derived models of synaptic pruning. Nat Neurosci [Internet] 22(3):374–385. http://www.nature.com/articles/s41593-018-0334-7
Selvaraj S, Bloomfield PS, Cao B, Veronese M, Turkheimer F, Howes OD (2018) Brain TSPO imaging and gray matter volume in schizophrenia patients and in people at ultra high risk of psychosis: an [ 11 C]PBR28 study. Schizophr Res [Internet] 195:206–214. https://www.ncbi.nlm.nih.gov/pubmed/28893493
Setiawan E, Wilson A, Mizrahi R, Rusjan PM, Miler L et al (2015) Role of translocator protein density, a marker of neuroinflammation, in the brain during major depressive episodes. JAMA Psychiatry 72(3):1–8
Setiawan E, Attwells S, Wilson AA, Mizrahi R, Rusjan PM et al (2018) Association of translocator protein total distribution volume with duration of untreated major depressive disorder: a cross-sectional study. Lancet Psychiatry 5(4):339–347
Sommer IE, de Witte L, Begemann M, Kahn RS (2012) Nonsteroidal anti-inflammatory drugs in schizophrenia: ready for practice or a good start? A meta-analysis. J Clin Psychiatry [Internet] 73(4):414–419. [Cited 2015 Jul 3]. http://www.ncbi.nlm.nih.gov/pubmed/22225599
Su L, Faluyi YO, Hong YT, Fryer TD, Mak E et al (2016) Neuroinflammatory and morphological changes in late-life depression: the NIMROD study. Br J Psychiatry 209(6):525–526
Suridjan I, Rusjan PM, Voineskos AN, Selvanathan T, Setiawan E et al (2014) Neuroinflammation in healthy aging: a PET study using a novel Translocator Protein 18kDa (TSPO) radioligand, [18F]-FEPPA. Neuroimage [Internet] 84:868–875. https://doi.org/10.1016/j.neuroimage.2013.09.021
Suzuki K, Sugihara G, Ouchi Y, Nakamura K, Futatsubashi M et al (2013) Microglial activation in young adults with autism spectrum disorder. JAMA Psychiatry [Internet] 70(1):49–58. http://www.ncbi.nlm.nih.gov/pubmed/23404112
Takano A, Arakawa R, Ito H, Tateno A, Takahashi H et al (2010) Peripheral benzodiazepine receptors in patients with chronic schizophrenia: a PET study with [ 11 C]DAA1106. Int J Neuropsychopharmacol [Internet] 13(07):943–950. [Cited 2019 May 3]. https://academic.oup.com/ijnp/article-lookup/doi/10.1017/S1461145710000313
Thomas DM, Dowgiert J, Geddes TJ, Francescutti-Verbeem D, Liu X, Kuhn DM (2004) Microglial activation is a pharmacologically specific marker for the neurotoxic amphetamines. Neurosci Lett 367(3):349–354
Toth M, Little P, Arnberg F, Mulder J, Halldin C et al (2016) Acute neuroinflammation in a clinically relevant focal cortical ischemic stroke model in rat: longitudinal positron emission tomography and immunofluorescent tracking. Brain Struct Funct 221(3):1279–1290
Tuisku J, Plavén-Sigray P, Gaiser EC, Airas L, Al-Abdulrasul H et al (2019) Effects of age, BMI and sex on the glial cell marker TSPO—a multicentre [11C]PBR28 HRRT PET study. Eur J Nucl Med Mol Imaging 46(11):2329–2338
van Berckel BN, Bossong MG, Boellaard R, Kloet R, Schuitemaker A et al (2008a) Microglia activation in recent-onset schizophrenia: a quantitative (R)-[ 11 C]PK11195 positron emission tomography study. Biol Psychiatry 64(9):820–822
van Berckel BN, Bossong MG, Boellaard R, Kloet R, Schuitemaker A et al (2008b) Microglia activation in recent-onset schizophrenia: a quantitative (R)-[11C]PK11195 positron emission tomography study. Biol Psychiatry [Internet] 64(9):820–822. [Cited 2019 May 3]. https://linkinghub.elsevier.com/retrieve/pii/S0006322308005039
Van Der Doef TF, De Witte LD, Sutterland AL, Jobse E, Yaqub M et al (2016) In vivo (R)-[ 11 C] PK11195 PET imaging of 18kDa translocator protein in recent onset psychosis. Npj Schizophr [Internet] 2:16031. https://doi.org/10.1038/npjschz.2016.31
Venneti S, Lopresti BJ, Wiley CA (2013) Molecular imaging of microglia/macrophages in the brain. Glia [Internet] 61(1):10–23. wiley.com/10.1002/glia.22357
Veronese M, Marques T, Bloomfield PS, Rizzo G, Singh N et al (2017) Kinetic modelling of [11C]PBR28 for 18kDa Translocator Protein PET data: a validation study of vascular modelling in the brain using XBD173 and tissue analysis. J Cereb Blood Flow Metab 38(7):1227–1242
Wilson AA, Garcia A, Parkes J, McCormick P, Stephenson KA et al (2008) Radiosynthesis and initial evaluation of [18F]-FEPPA for PET imaging of peripheral benzodiazepine receptors. Nucl Med Biol [Internet] 35(3):305–314. [Cited 2015 Jul 3]. http://www.ncbi.nlm.nih.gov/pubmed/18355686
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Cervenka, S., Mizrahi, R. (2021). TSPO Imaging in Psychiatric Disorders. In: Dierckx, R.A., Otte, A., de Vries, E.F.J., van Waarde, A., Sommer, I.E. (eds) PET and SPECT in Psychiatry. Springer, Cham. https://doi.org/10.1007/978-3-030-57231-0_18
Download citation
DOI: https://doi.org/10.1007/978-3-030-57231-0_18
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-57230-3
Online ISBN: 978-3-030-57231-0
eBook Packages: MedicineMedicine (R0)