
Abstract
Chronic kidney disease (CKD) is a common condition affecting a roughly estimated 400–850 million of the world’s population, primarily older adults. A variety of cardiovascular diseases (CVD) are common in this population, mostly due to similarity of risk factors, such as age, diabetes, hypertension, obesity, and dyslipidemia. But CKD also evokes a unique pathophysiology that contributes to the prevalence of CVD in this population. Primary prevention of CKD is possible and might contribute to a lower burden of CVD. Secondary prevention of progression of CKD to advanced stages, including end-stage kidney disease (ESKD), through early detection and aggressive management might also reduce the burden of CVD. Opportunities for primary and secondary prevention of the various forms of CVD seen in mild to moderate CKD will be the focus of this review, rather than treatment of CVD seen in association with advanced CKD (ESKD), treated by dialysis or transplantation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Chronic kidney disease
- Cardiovascular disease
- Estimated glomerular filtration rate
- Proteinuria
- Dyslipidemia
- Vascular calcification
- Sodium-glucose cotransporter-2 inhibitors
- Renin-angiotensin system inhibitors
- Hypoglycemic agents
- Anticoagulants
-
Chronic kidney disease (CKD) is conventionally defined, graded, and diagnosed using glomerular filtration rate (GFR) and albuminuria (or other features of kidney injury), along with persistence for 3 months or more.
-
CKD, so defined, is common, particularly in the elderly with comorbidities such as diabetes. Estimates of its global prevalence vary.
-
The etiopathogenesis of CKD is extremely varied. Major subdivisions are diabetes- and nondiabetes-related CKD.
-
Cardiovascular disease (CVD), in its many forms, commonly accompanies CKD, particularly in moderate to severe grades of CKD (GFR <45 mL/min/1.73 m2) in older adults. The pathophysiology underlying CVD in CKD is complex and shares many features of CVD occurring in patients without CKD.
-
Left ventricular hypertrophy and myocardial fibrosis are common with advancing grades of CKD contributing to risks of heart failure (HFrEF and HFpEF) and arrhythmias.
-
Risk stratification for CVD in CKD is complex and still evolving. Most CVD risk equations do not include CKD as a risk variable. Many experts regard CKD as a coronary disease risk equivalent, like some define diabetes.
-
Primary prevention of CKD (and thereby reducing CVD risk) is possible but difficult to prove without long-term randomized clinical trials. Screening of asymptomatic persons at risk for CKD may allow for early detection of CKD and better success for secondary prevention.
-
Secondary prevention of progression of CKD to higher grades will likely prevent CVD (in a primary or secondary way). Several successful strategies for secondary prevention of progressive CKD have also been shown to prevent CVD and its complications in randomized clinical trials.
1 Introduction
Chronic kidney disease (CKD) is most commonly defined in adults by a matrix of estimations or measurement of glomerular filtration rate (GFR) and signs of kidney injury (abnormalities of urinary albumin or protein excretion, urinalysis, imaging, or kidney biopsy) which persists for at least 3 months (see Fig. 1) [1]. The severity (and prognosis) of CKD is judged by categories of GFR and albuminuria. As such, CKD can be present with normal levels of GFR, but with increased albuminuria, and an abnormally low GFR can define CKD even in the absence of signs of kidney injury. So defined, CKD is relatively common (particularly in older adults), affects both genders and many ethnicities (preferentially racial minorities), and can in some cases progress to advanced kidney failure requiring dialysis or kidney transplantation. CKD is also associated with excess mortality and morbidity (especially that related to cardiovascular disease, CVD). It is crucial to recognize and appreciate that CKD is a “generic” term representing many individual diseases, often divided into diabetes-related and nondiabetic forms. Obviously, the nature of the disease underlying CKD has an important effect on the risks for and the kinds of CVD that develops before, concomitantly, or after development of CKD. The prognosis for “generic” CKD, illustrated by the colored “heat map” in Fig. 1, has been derived from large epidemiological studies that provide an “average” risk, which can vary considerably from specific disease to disease. For example, the risk of CVD for a given patient with type 2 diabetes or lupus nephritis with grade 3B CKD may not be the same, even after adjusting for age and other comorbidities as in a patient with the same grade of CKD due to IgA nephropathy or tubulointerstitial nephritis. It is not possible to structure this chapter around the specific diseases causing CKD, many of which are not preventable, so we will rely on the “generic” CKD concept, with full recognition of its limitations.

The categorization of CKD and its prognosis using a 2 × 2 matrix of glomerular filtration rate (GFR – measured or estimated) and albuminuria (uACR – urine albumin-to-creatinine ratio). Green, no CKD; yellow, orange, and red, increasing levels of risk for adverse events, including CVD. (Reprinted from Summary of Recommendations Statements [`]. With permission from Elsevier)
The cardiovascular diseases present in or developing after the recognition of “generic” CKD, so defined, are diverse and include coronary artery disease (CAD , also known as ischemic heart disease), congestive heart failure (either of the reduced or preserved ejection fraction varieties [HFrEF or HFpEF, respectively]), strokes (hemorrhagic, thrombotic, or embolic), peripheral artery disease, valvular heart disease, and arrhythmias (sudden cardiac death and non-valvular atrial fibrillation) (see Table 1) [2]. The general topic of coronary artery disease in CKD has been of great interest for decades. A state-of-the-art review commissioned by the Kidney Disease: Improving Global Outcomes (KDIDO) was recently published [3] and is an excellent source for contemporary information, unresolved issues, areas of controversy, and future research priorities.
The CVD events associated with CKD (co-incidentally or causally) can also be broadly divided into atherosclerotic and non-atherosclerotic forms. Death from CVD is a common event in patients with CKD, especially in the elderly, and commonly supervenes before CKD has progressed to an advanced stage requiring dialysis or transplantation for survival [4]. Cardiovascular mortality attributed to reduced GFR outnumbers deaths due to kidney failure (ESKD) globally [5].
The pathophysiology underlying the connections between CKD and CVD is complex and only partially understood [6]. Aging is one non-modifiable factor that underlies both CKD and CVD. The CKD-CVD connection involves accelerated atherogenesis, chronic extracellular volume expansion, intravascular pressure disturbances, dyslipidemia, accumulation of “uremic” toxins, hyper-homocysteinemia, hyperuricemia, disordered endocrine and hematological functions, and others. It is likely that CKD itself promotes CVD and CVD can be a cause of CKD; disentangling this “two-way street” in individual patients can be difficult and challenging, particularly among the elderly. Observational data showing an association between these two disease categories are confounded by this phenomenon. Nevertheless, opportunities exist for both primary and secondary prevention of CVD and its morbidity and mortality in patients with established CKD having a propensity for progression to ESKD.
This chapter will summarize the present state of these opportunities, with a focus on patients with mild to moderate CKD rather than very advanced CKD, requiring dialysis or transplantation. This chapter is not intended to be comprehensive but rather a pragmatic discussion of the topic.
2 Epidemiology of CKD and Its Association with CVD
2.1 General CKD and CV Mortality
In the 2019 US Medicare population (mostly over age 65 years), the prevalence of chronic kidney disease (CKD), using the Kidney Disease Improving Global Outcomes (KDIGO) definition specified above, was found to be 14.5%. In this same population, 67.5% of these CKD patients also shared a comorbidity of cardiovascular disease (CVD). In comparison, 35.5% of non-CKD patients were diagnosed with CVD [7]. The 2018 US Medicare dataset was further broken down into specific cardiovascular comorbidities. Coronary artery disease/acute myocardial infarction (CAD/AMI; 47.2%) was the most common CVD morbidity found among these CKD patients, followed by heart failure (HF; 25.9%), peripheral artery disease (PAD; 25.2%), atrial fibrillation (AF; 23.8%), cerebrovascular accident/transient ischemic attack (CVA/TIA; 16.1%), valvular heart disease (VHD; 12.8%), and then sudden cardiac arrest/ventricular arrhythmias (SCA/VA; 4.1%) (see Table 1) [8]. Worldwide, the prevalence of CKD in adults in a meta-analysis performed in 2016 by Hill et al. was found to be 13.4% (95% CI 11.7–15.1%), the majority of which was grade 3 CKD (7.6%; 95% CI 6.4–8.9%) [9]. One study estimates the global burden of cardiovascular disease attributable to impaired kidney function to be 25.3 million disability-adjusted life years [10]. Grade 3 CKD is found in about 0.7% in those 20–39 years of age and rises to 38% in those >70 years of age according to a national survey in the USA conducted in 1999–2004 [11]. (Note the definitions of CKD used in this survey may overestimate the prevalence of CKD in the elderly adult) [12].
Most recently, the Global Burden of Disease-CKD Collaboration has indicated a global prevalence of CKD in adults (all ages) to be about 9.1% or about 700,000,000 persons and the change of age-standardized prevalence over the past 27 years (1990–2017) to be about +2.8% – essentially unchanged. However, the prevalence of CKD varies quite widely from country to country. The global prevalence of end-stage kidney disease treated by dialysis or transplantation continues to rise, largely due to improved access to such treatment in less developed countries [9, 10].
Of note, several factors make the true prevalence of CKD difficult to ascertain in such epidemiological studies. Mild to moderate CKD is likely underestimated due to the asymptomatic nature of the disease, in studies examining volunteers or health records. This ascertainment bias is much less likely when population-based studies are used to estimate prevalence. Furthermore, estimates of prevalence are affected by choices and accuracy of biomarkers and formulas used to estimate glomerular filtration rate (GFR) or assess urinary albumin excretion rate. Using estimated rather than measured GFR itself, inter-assay reliability, failure to fully assess disease duration versus “one-off” testing, and using an absolute rather than age-adjusted threshold to diagnosis CKD all tend to overestimate CKD prevalence in the elderly (the same individuals who are at increased risk for CVD) and underestimate the prevalence of CKD in younger adults [12,13,14]. Thus, the true global prevalence of non-dialysis-treated CKD may be overestimated, perhaps by a factor of 2.
In summary, CKD is a common disorder, particularly in the older adult, and its age-standardized prevalence in the population of the world is relatively stable but variable between countries. As currently defined, CKD is also commonly associated with CVD, predominantly because of the shared predilection of both CKD and CVD to affect older and elder adults. Nevertheless, CVD is a significant contributor to overall causes of morbidity and mortality in CKD patients. CVD and cancer comprise the majority of the etiologies for death in overall CKD patients, at 30.2% and 31.9%, respectively. Among those with a GFR <60 mL/min/1.73 m2 and grade 3 CKD patients specifically, CVD was the leading cause of mortality and only behind cancer and infection in grade 1–2 CKD patients [15]. The risk of cardiovascular events increases directly with albuminuria and inversely to GFR, with both albuminuria and GFR conferring independent risk to CV death relative to each other as well as to other traditional risk factors [16, 17]. In grade 3 CKD patients, CVD mortality was found to be about twice as high compared to individuals with normal kidney function (Tables 2 and 3) [16]. A further breakdown of CVD mortality showed ischemic heart disease to be leading cause of mortality, followed by strokes, heart failure, valvular heart disease, and then arrhythmia in descending order. Stroke mortality was more prevalent among mild stages of CKD, whereas HF and valvular heart disease mortality increased with more severe stages of CKD [15]. Sudden cardiac death is the leading cause of mortality in patients with dialysis-treated ESKD [18].
2.2 CKD and Coronary Artery Disease (CAD)
Several clinical studies have found reduced kidney function to be independently associated with an increased risk of CAD. In fact, the risk of myocardial infarction in patients with advanced CKD is similar to or greater than the risk in patients with diabetes, such that some authors suggest CKD should also be considered a CAD risk equivalent [19, 20].
The Atherosclerosis Risk in Communities (ARIC) study examined a population of 14,971 men and women in the USA with grade 1–3 CKD over 12 years for de novo and recurrent events of coronary heart disease defined as myocardial infarction or coronary revascularization procedures. People with GFR equivalent to grade 3 CKD compared to no CKD had hazard ratios of 1.26 and 1.30 for de novo and recurrent events of coronary heart disease, respectively, and a hazard ratio of 2.4 for CAD mortality. Notably, the concurrence of anemia with grade 3 CKD greatly increased the risk for recurrent coronary heart disease up to a hazard ratio of 8.01 [21].
The Chronic Renal Insufficiency Cohort (CRIC) study examined a population of 1123 men and women in the USA with mild to moderate CKD (GFR 20–70 mL/min/1.73 m2) for coronary artery calcification using electron beam or multi-detector computed tomography and found that 25.1% of patients had de novo calcification and 18.0% of patients had progression of calcification at the end of an average of 3.3-year follow-up [22]. The Assessing Diagnostic Value of Noninvasive Computerized Tomography-Derived Fractional Flow Reserve (FFRCT) in Coronary Care (ADVANCE) study also found differences in presentation of acute coronary syndrome in CKD patients, with those individuals with lower GFR tending to present more often with acute myocardial infarction than with stable angina (especially GFR < 45 mL/min/1.73 m2, HR 3.82, CI 1.55–9.46) [23].
2.3 CKD and Congestive Heart Failure (CHF)
CKD and CHF are intimately related chronic disease epidemics, and determining which disease is primary versus secondary can often be difficult. The Atherosclerosis Risk in Communities study found the incidence rate of de novo HF in their CKD population to be 17–21%, with increasing incidence correlating with increasingly severe CKD [24]. An analysis of the Chronic Renal Insufficiency Cohort population demonstrated similar findings, although the correlation of CHF incidence and CKD was stronger using urine albuminuria and cystatin C-based GFR rather than creatinine-based GFR [25]. Multiple studies have found that reduced renal function is independently associated with increased overall mortality, cardiovascular mortality, and hospitalization in patients with CHF, regardless of preserved versus reduced ejection fraction status [26, 27].
2.4 CKD and Valvular Heart Disease
Valvular heart disease is more prevalent in the CKD population versus the general population, with mitral regurgitation being the most prevalent (43% vs. 24%), followed by aortic stenosis (9.5% vs. 3.5%), aortic regurgitation (19% vs. 10%), and then mitral stenosis (2% vs. 1%). CKD patients demonstrated greater degrees of left atrial/ventricular dilation, left ventricular hypertrophy, and right ventricular systolic pressures on echocardiogram compared to the general population [28, 29]. Several studies have shown an independent association with increasing aortic valve calcification and decreasing GFR [28, 30, 31]; however, associations of mitral annular calcification and GFR were only observed with comorbid diabetes [31]. At every level of increasing severity of aortic stenosis and mitral regurgitation, CKD patients suffered greater mortality relative to their non-CKD counterparts [29].
2.5 CKD and Stroke
Kidney function is further inversely related to the incidence of stroke (including both ischemic and hemorrhagic forms), with a 43% higher risk of stroke for eGFR <60 mL/min/1.73 m2. Hypertension, a crucial modifiable risk factor for stroke, is commonly associated with CKD and worsens with advancing disease, likely compounding the risk for stroke in CKD patients [32]. Among the measures of serum creatinine, cystatin C, and urine albumin for kidney function, increasing urine albumin has been demonstrated by several studies to have the strongest independent relationship with stroke risk [33, 34]. A nearly twofold increase risk of incident stroke has been demonstrated in individuals with moderate albuminuria (urinary albumin-creatinine ratio 30–300 mg/g) [32]. In one meta-analysis, the risk of hemorrhagic stroke was elevated even with small elevations in urinary albumin-creatinine ratio <30 mg/g, although this may not have been sufficiently powered due to the lower incidence of hemorrhagic strokes versus ischemic strokes (81% vs. 12%) [33]. The ARIC study additionally noted a marked increase of stroke risk in CKD patients comorbid with anemia, with a hazard ratio of 5.43 (95% CI 2.04–14.41) compared to CKD patients without anemia [34]. An increased risk of embolic stroke is associated with atrial fibrillation (see below).
2.6 CKD and Peripheral Arterial Disease (PAD)
Prevalence and incidence of PAD are higher in CKD populations compared to the general population. An analysis of the National Health and Nutrition Examination Survey (NHANES) estimated a prevalence of 24% of persons with ankle-brachial index <0.9 among those with creatinine clearance <60 mL/min/1.73 m2 compared to 3.7% among those with creatinine clearance ≥60 mL/min/1.73 m2 [35]. Similarly, the ARIC study observed a multivariable adjusted relative risk of 1.56 (95% CI 1.13–2.14) for incident PAD in CKD patients [36]. Women with CKD in particular have been found to have a higher incident risk of PAD compared to men, especially at younger ages (age <40 years, HR 2.57, 95% CI 1.27–5.20) [37]. Albuminuria itself, independent of decreased GFR, has also been found to be associated with an increased risk of developing PAD [38], although there remains debate as to whether this association holds true for nondiabetic patients [39].
2.7 CKD and Non-valvular Atrial Fibrillation (AF)
Atrial fibrillation is the most common cardiac arrhythmia, constitutes a risk for embolic stroke, and has been shown by several studies to be associated with CKD. The CRIC study estimates that non-valvular AF is prevalent in one-fifth of the CKD population, a number replicated by the US Renal dataset Medicare population and which is about two- to threefold of the prevalence in the general population [40]. Furthermore, two prospective cohort studies further showed that the incidence of AF was independently increased in CKD populations with lower cystatin C-based GFR and higher urine albuminuria [41, 42]. The risk of embolic stroke from AF is further enhanced by the presence of CKD, with one study estimating a nearly 50% increase in the risk of ischemic (embolic) stroke or systemic thromboembolism in AF accompanied by CKD (HR = 1.49; 95% CI = 1.38–1.59) [43]. In addition, another study shows a higher stroke risk in CKD patients that develop incident AF versus CKD patients without AF (HR = 2.00; 95% CI = 1.88–2.14) [44]. The risk of total , ischemic, and hemorrhagic stroke is highest at the lowest eGFR and highest urinary albumin-to-creatinine ratio (uACR) with CKD, and the type of stroke differs by degree of decline in eGFR and uACR [45].
2.8 CKD and Sudden Cardiac Death (SCD)
The risk of SCD, normally defined as an unexpected circulatory arrest occurring within 1 hour of acute change of clinical status or unwitnessed death without an obvious noncardiac cause in a patient known otherwise to be well in the past 24 hours, has been shown to increase with declining kidney function [18, 46]. Sudden cardiac death is the most common cause of mortality in dialysis-treated ESKD, probably linked to a high prevalence of left ventricular hypertrophy in this population [18]. An analysis of the Multicenter Automatic Defibrillator Implantation Trial-II (MADIT-II) study described that for each 10 unit reduction in eGFR, there was an associated increase of risk of SCD by 17%. Interestingly, the study found that a survival benefit conferred by implanted cardioverter defibrillator (ICD) therapy was only demonstrated among patients with eGFR ≥35 mL/min/1.73 m2, with no such survival benefit among patients with eGFR <35 mL/min/1.73 m2 despite increased prevalence of SCD , suggesting increased resistance to ICD therapy with declining renal function [47].
3 The Pathophysiology of CVD in CKD
The interrelationships between CVD and CKD are complex and multifactorial. Figure 2 graphically displays the major players. Not all of these will be discussed here. The pathophysiology can be broadly subdivided into proatherogenic factors and non-atherogenic factors, although there is overlap between these two categories (see Table 4). Diabetes, particularly type 2 with obesity or the metabolic syndrome, is a very important cause of the coexistence of CVD and CKD. Heart failure and ischemic heart disease are quite common in patients with CKD due to diabetes.

Factors that operate in the linkage between CKD and CVD. (CKD chronic kidney disease, CVD cardiovascular disease, LV left ventricular hypertrophy, PTH parathyroid hormone, FGF23 fibroblast growth factor-23)
Dyslipidemia
Among the proatherogenic factors, dyslipidemia is very important [48]. Dyslipidemia is quite common in CKD and relates to underlying diabetes in many cases and due to nephrotic syndrome or other nondiabetic forms of CKD in others. The patterns of dyslipidemia seen in patients with CKD depend on grade of disease (as assessed by estimated GFR), the degree of proteinuria (albuminuria) concomitantly present, and the existence of complicating inflammation/malnutrition and the presence or absence of diabetes [49]. In patients with advanced CKD and no or only mild proteinuria, the pattern is one of elevated triglycerides, increased very-low-density lipoprotein (VLDL), increased intermediate-density lipoproteins (IDL), increased oxidized lipids, elevated non-high-density lipoproteins (non-HDL), variable high-density lipoprotein (HDL), and an increase in highly atherogenic small dense low-density lipoproteins (LDL) [48,49,50,51]. In patients with CKD accompanied by substantial proteinuria (including nephrotic syndrome), the pattern is one of elevated total cholesterol, increased LDL, and variable HDL levels. Hypertriglyceridemia and hyperchylomicronemia can be seen in severe nephrotic syndrome [51, 52]. The molecular and metabolic disturbances underlying these patterns of dyslipidemia in CKD have been extensively reviewed by Moradi and Vaziri [50] and will not be recounted in detail here. However, the dyslipidemia seen in CKD contributes to the excess of atherosclerotic CVD observed in patients with CKD, of diverse etiology. Paradoxically, decrements in non-HDL and non-HDL/HDL ratio in advanced CKD treated by dialysis are associated with an increased CVD mortality rather than the converse seen in the general population [53], perhaps due to complicating malnutrition/inflammation.
Hypertension and Hypervolemia
Elevations of systolic (and diastolic) blood pressure and pulse pressure are commonly seen in various forms of progressive CKD (except those characterized by salt-losing states) [54]. A progressive increase in extracellular volume accompanied by incomplete suppression of the renin-angiotensin-aldosterone axis is likely the cause of CKD-associated hypertension [55]. An increase in centrally driven sympathetic nervous system activity also contributes to elevated arterial pressure and peripheral resistance in CKD [56]. Systolic arterial hypertension is also abetted by a decrease in vascular compliance, perhaps related to collagen cross-linking and calcification of the media seen in progressive CKD (see below) [57]. The increased systemic arterial blood pressure and expanded extracellular fluid volume promote both atherogenic CVD (ischemic heart disease, peripheral arterial disease, and thrombotic stroke) and left ventricular hypertrophy, leading to congestive heart failure with reduced ejection (HFrEF) fraction and arrhythmias, such as atrial fibrillation. Cardiac fibrosis is augmented by prolonged hypervolemia, especially in the presence of poorly suppressed aldosterone, and this can lead to heart failure with a preserved ejection fraction (HFpEF) [58], more commonly seen in CKD than in the general population. Prolonged hypertension in CKD is also responsible for an increase in risk of hemorrhagic stroke. The anemia of advanced CKD also contributes to left ventricular remodeling in CKD [59].
Uremic Toxins and Hormonal Factors
A panoply of “uremic toxins” accumulates in advancing CKD, such as asymmetric dimethyl arginine (ADMA), advanced glycation end products (AGEP), trimethylamine N-oxide (TMAO), and others (such as indoxyl sulfate, hyper-homocysteinemia, hyperphosphatemia) [60,61,62]. These substances can lead to myocardial and vascular injury (endothelial damage). The hormonal profile is altered in CKD, with increases in parathyroid hormone and fibroblast growth factor 23 and reduced α-Klotho generation, which collectively can have adverse direct effects on the myocardium and vessels [63,64,65]. α-Klotho is a novel glucuronidase transmembrane enzymatic protein with important “anti-aging” properties. It also serves as a cofactor for FGF-23 action. The reduction of serum α-Klotho levels seen in CKD might contribute to “premature aging” and accelerated arteriosclerosis/atherosclerosis. Marinobufagenin levels are increased in CKD and can promote cardiac fibrosis [66]. Disturbances leading to impaired Klotho generation in CKD can promote cardiac TGF-β signaling and cardiac fibrosis [67]. Decreases in active vitamin D (1,25-dihydroxyvitamin D) in CKD can have adverse effects on the coronary circulation and myocardium [68]. Loss of endogenous erythropoietin participates in the development of anemia in CKD, which can have adverse effects on the heart and circulation in general [69]. Hyperuricemia is another factor that can contribute to CVD accompanying CKD (see below).
Vascular Calcification
Patients with progressive CKD, particularly its later stages, can be affected by a process of vascular (arterial) calcification , involving large- and medium-sized arteries (including coronary arteries) and heart valves (mitral and aortic) [57]. This process is an active one, involving modifications in arterial smooth muscle biology [57]. It predominantly affects the tunica media (Monckeberg’s sclerosis) and leads to impaired relaxation and reduced vascular compliance. In advanced forms, it can produce a calcific uremic arteriopathy with ischemia and necrosis of the skin (calciphylaxis) [70]. The calcific deposits in the media have a chemical composition resembling bone (hydroxyapatite). The calcific deposits in atherosclerotic plaques have a different composition and clinical significance (see below).
Chronic Inflammation and Enhanced Oxidative Stress
For poorly understood reasons, most forms of CKD (diabetic and nondiabetic) are associated with features of chronic inflammation (such as manifested by increased C-reactive protein and/or Il-6 serum levels) and increased oxidative stress [71, 72]. The cytokine milieu and/or uremic toxin burden (e.g., indoxyl sulfate levels) underlying this phenomenon can have profound effects on atherogenesis, by causing proatherogenic changes in blood lipids (such as oxidized LDL and HDL transformation to an atherogenic lipid) [73]. These changes may account in part for the enhanced risk of CVD in CKD.
4 Risk Stratification for CVD in CKD
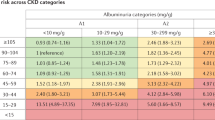
There is little doubt that CKD is associated with an excess risk of morbidity and mortality from CVD. The factors relevant for risk stratification in CKD are summarized in Table 4. The risk of coronary artery disease (and heart failure) increases as CKD progresses to more advanced grades, despite correction for traditional CVD risk factors [74]. Go and colleagues were among the first to quantify the risk of CVD events (mortality and hospitalization) in a large cohort (1,120,295 subjects; mean age 52 years, 55% women) reported in 2004 [17]. There was a graded increase in CVD risk when eGFR fell below 60 mL/min/1.73 m2, but the most significant increases in risk were seen when eGFR fell below 45 mL/min/1.73 m2. Any increase in CVD risk in grade 1 or 2 CKD (and possibly grade 3 CKD) is largely related to proteinuria (albuminuria), not GFR. Subsequently, many other studies showed an excess risk of CVD and all-cause mortality in older adults when eGFR fell below 45 mL/min/1.73 m2 (see Fig. 3), only a few of which are cited here [75, 76]. This association was particularly evident when albuminuria was present. Brantsma et al. using data from the PREVEND study in the Netherlands found that stage 1 and 2 CKD (characterized chiefly by abnormal albuminuria) have a greater risk of CVD than stage 3 CKD (chiefly characterized by abnormal GFR) [77]. Increased urinary albumin excretion, even close to the high normal range (10–30 mg/day), has been repeatedly shown to augment CVD risk [78]. Prediction of CVD risk in community-dwelling older adults without clinical evidence of CVD using combinations of eGFR and albuminuria was studied by Nerpin et al. in the USLAM study in Sweden [79]. They found that both uAER >8.6 mg/d and an eGFR <45 mL/min/1.73 m2 improved the integrated discrimination index for CVD mortality prediction. Interestingly, the eGFR prediction was only significant when it was based on cystatin C but not creatinine-based formulas [79]. This is most likely due to the impact of micro-inflammation (see above) elevating serum cystatin C levels rather than greater accuracy of eGFR-cystatin C for assessment of true measured GFR [80]. The conclusion is that the presence and magnitude of albuminuria is more important for risk prediction of CVD in CKD and that the risk of CVD events is mostly associated with eGFR creatinine levels below 45 mL/min/1.73 m2 in older adults. The rate of decline of GFR over time is another factor to consider in risk stratification for CVD in patients with CKD. Monitoring the change in eGFR over time seems to improve CVD prognostication [81].

The association of CKD (according to eGFR and albuminuria) and all-cause mortality (predominantly CVD – related to eGFR and albuminuria uACR) in various age groups. Values shown are incidence rate ratios for all-cause mortality. (Green, <1.5; yellow, >1.5 < 2.5; orange, >2.5 < 4.0; red, >4.0). (Reprinted from Warnock et al. [75]. With permission from Karger Publishers)
As stated above, most (but not all) of the excess risk for CVD in CKD is captured by traditional approaches to quantifying risk according to multivariable risk equations (such as Framingham or the ACC/AHA pooled risk scoring formulas) [74]. Indeed, Clase and coworkers found that the addition of uACR or eGFR values to traditional risk scoring led to no meaningful change in the proportion of patients assigned to an intermediate-risk category among a cohort of patients older than 55 years with documented CVD [82]. On the other hand, addition of eGFR and uACR has a profound impact on classification of risk for ESKD [83], irrespective of age, when the competing risk of mortality is taken into consideration. Di Angelantonio et al., in a prospective population-based cohort study (n = 16,958, ages 31–81 years) without known CVD, found that the addition of CKD information to traditional CVD risk assessment had only a modest effect on reclassification of risk [84]. The incremental gain provided by adding CKD to risk assessment was less than that provided by diabetes or smoking status. Importantly, most of the CVD risk prediction algorithms in common use do not include eGFR, albuminuria, or CKD. Only the UK QRISK-2® includes CKD (grades 4 and 5 only; eGFR <45 mL/min/1.72 m2) [85].
The controllable traditional factors associated with CKD that have a powerful impact on CVD risk (including ASCVD, stroke, heart failure, and arrhythmias) include hypertension, dyslipidemia, obesity (and metabolic syndrome), diabetes (and glycemic control), and smoking. Age, gender, family history, and ancestry also contribute to CVD risk but mostly independent of CKD status. Of course, both CKD and CVD are diseases that preferentially affect older adults, and these traditional risk factors are operative in non-CKD-associated CVD covered by other chapters in this manual.
Nontraditional CVD risk factors observed in subjects with CKD include high-sensitivity C-reactive protein (hsCRP) and interleukin 6 levels (as a feature of chronic inflammation), volume overload, anemia, vascular calcification, vitamin D deficiency, hyper-homocysteinemia, hyperuricemia, vitamin K deficiency, oxidative stress, uremic toxins (such as ADMA and TMAO levels), parathyroid hormone (PTH), fibroblast growth factor-23 (FGF-23) levels, and Klotho deficiency [63, 86,87,88,89]. These toxins and other molecules may bias the results of estimating GFR [86]. Paradoxically, some reports suggest that an increase in eGFR, seen in early diabetes and in excessive protein intake, may be associated with increased risk of CKD/CVD [89], but the mechanisms underlying this association are unclear. Cardiac biomarkers, such as cardiac troponin-T and NT-proBNP, may have application for better risk classification in patients with CKD [90]. Many of these nontraditional risk factors for CVD in CKD are the subject of ongoing research aimed at improving the accuracy of prediction of CVD risk in CKD. Some of these may have obvious preventative strategic importance in the future.
Coronary artery calcification (CAC) is common in CKD and increased in frequency and severity as CKD progresses [91]. Patients on long-term dialysis (survivors) tend to show progressively increasing degrees of CAC, which, paradoxically, might suggest a “protective effect” of such calcification [92]. Assessment of the coronary arterial calcium (CAC) score may play a useful role in assessing overall CVD risk in selected patients with CKD, perhaps in helping to inform on decisions for certain therapies (e.g., statins) [93], but it is unknown if treatments designed to prevent or cause regression of vascular calcification are beneficial, and there are no guidelines recommending repeating CAC scoring to evaluate the effects of therapy. Other nontraditional risk factors for CVD have not been adequately studied prospectively in CKD.
Left ventricular hypertrophy (LVH) is common in CKD and tends to increase in frequency and severity as CKD progress, mediated by volume expansion and poorly controlled hypertension [94, 95]. Such LVH increases the risk of heart failure, sudden cardiac death, and atrial fibrillation. Assessment of LVH by cardiac ultrasound or MRI can be a useful tool in evaluating non-atherogenic CVD risk [94]. Standard EKG assessment of LVH may be too insensitive for this purpose but is required for accurate diagnosis of atrial fibrillation and embolic stroke risk assessment.
5 Strategies for Prevention of CVD in Non-dialysis CKD
Primary Prevention of CKD
In an ideal world, the best strategy to reduce the burden of CVD associated with CKD is to prevent the development of CKD in the first place (primary prevention). This is easier said than done. It seems reasonable to postulate that a reduction in the prevalence of visceral obesity and the incidence of type 2 diabetes mellitus as well as earlier detection and better management of hypertension and diabetes in the general population will ultimately reduce the incidence and prevalence of CKD.
Moderate exercise, caloric moderation, lower salt intake, smoking cessation, and perhaps a diet rich in plants and fiber might accomplish this goal, but this requires a commitment of society to move away from Western diets, high in processed foods, refined sugars, salt, and animal-based protein, particularly processed or unprocessed red meat [96, 97]. Avoidance of high protein intake might have salutary effects on the incidence of CKD, particularly in individuals born with a nephron deficiency consequent to low birth weight, due to fetal dysmaturity, or who have congenital or acquired single kidneys (see also below) [98]. The frequency of low birth weight and nephron deficiency varies widely, largely due to differences in prenatal care and maternal nutrition. The impact of long-term high protein intake on incident CKD is controversial (see above) [99]. Unfortunately, long-term randomized trials have seldom been conducted with incident CKD as an endpoint, so prevention of CKD by means of lifestyle changes, while challenging, should not be dismissed. Elimination of smoking would also likely have a beneficial impact on both CVD and CKD [100].
Detection and control of elevated blood pressure is commonly touted as a tool for reducing the incidence of CKD and its progression to kidney failure [101, 102]. This proposal assumes that increased BP above some arbitrary threshold is causally related to the development of CKD. While this may be true for a subset of patients with very severe (“malignant”) hypertension, evidence exists to support the notion that CKD, often in subtle difficult-to-detect forms, causally underlies most forms of primary hypertension. Hypertension and its control appears to be an important player in the progression of established CKD, although it is difficult to tease apart the direct (non-antihypertensive) effects from the blood pressure-lowering effects of commonly used antihypertensive drugs on progression of CKD. Nevertheless, blood pressure above the normal range is an important causal factor in the generation of ASCVD and heart failure, with or without CKD [102].
The Systolic Blood Pressure Intervention Trial (SPRINT) of hypertension treatment in older, nondiabetic adults at moderate to high CVD risk is quite informative [103]. Intensive systolic blood pressure control (to <120 mmHg) did not prevent incident CKD (according to new-onset eGFR <60 mL/min/1.73 m2 or new-onset albuminuria); instead, it was associated with acute reductions in eGFR that were largely reversible upon discontinuation of therapy. Unfortunately, the follow-up was short (only 3.26 years), and severe hypertension (systolic blood pressure > 180 mmHg) was an exclusion criterion. The benefits of intensive blood pressure control on CVD were attenuated in those subjects with CKD at baseline, which comprised 28% of the randomized subjects and was usually grade 3 or less. Abnormal albuminuria was modest or absent in the patients randomized (uACR = 44 ± 160 mg/gm). The HR for the primary outcome in patients with CKD at baseline was 0.82 (95% CI = 0.63–1.07), however, demonstrating the benefit of intensive BP control in such patients for reducing CVD events. Additionally, recent very large observational epidemiological studies have shown that higher systolic blood pressure (>130 mmHg) are associated with (but not necessarily causal for) a higher risk of incident grade 3–5 CKD [104].
In summary, many CVD benefits (largely due to the avoidance of the primary outcomes of stroke and heart failure) accrue when blood pressure is strictly controlled in the absence of overt CKD, but whether control of hypertension per se will reduce incident CKD remains uncertain. The impact of aggressive blood pressure control on CVD in CKD remains controversial, but reduced stroke burden is one possible favorable outcome. The exact target blood pressure appropriate for patients with CKD for secondary prevention of CVD is not fully agreed upon, but a systolic pressure somewhere between 120 and 130 mmHg systolic seems reasonable [101, 105,106,107]. The selected values may depend on the method of measuring blood pressure (office, home, ambulatory monitoring) [101, 107]. The J-shaped relationship of blood pressure and CV morbidity and mortality seen in CKD patients (particularly in advanced grades of CKD) is in part explained by the concomitant malnutrition/micro-inflammation commonly observed in CKD [104, 106].
Angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARB), also known as renin-angiotensin system inhibition (RASi), are effective in slowing progression of established CKD, when abnormal albuminuria is present [108, 109], especially in diabetic subjects, but their effectiveness in primary prevention of CKD is unknown.
Many forms of nondiabetic CKD have a low potential for primary prevention, particularly when genetic mutations or autoimmunity is the underlying cause. Forms of CKD due to environmental factors, such as nephrotoxins or infections, are potentially preventable. Avoidance, treatment, or prophylaxis of infections known to induce CKD and avoidance of nephrotoxins (like adulterants in herbal medicines, toxic pesticides, air pollution, drugs, cigarette smoke) that can injure the kidneys [97,98,99,100, 110,111,112] can be an important feature of CKD prevention. These precepts are especially true in the neonate and infant and in the elderly population. The issues surrounding prevention and control of CKD are different for developed nations compared to low- to medium-income countries [111, 112]. Adequate maternal health and nutrition are commonly overlooked aspects of CKD prevention [111]. Poor maternal health and nutrition can be a cause of fetal dysmaturity leading to low birth weight and prematurity, both of which predispose to low nephron endowment (congenital nephropenia) (see above) [111]. Nephropenia at birth is an important and under-appreciated preventable cause of the later development of CKD. Improved prenatal care and adequate maternal nutrition can reduce the prevalence of low birth weight and prematurity and thus avoid congenital nephropenia and its expected adverse effect on CKD later in life. Acute kidney injury (AKI) can be an antecedent to incident CKD, so avoidance of all kinds of AKI, such as by minimization of nephrotoxins, and meticulous postoperative management will likely have a salutary effect on new-onset CKD [113]. A healthy lifestyle in general can have potential for reducing the rate of incident CKD [100].
Screening for CKD
By definition, screening for CKD in the general (apparently healthy) population by assessment of eGFR and/or albuminuria will have no impact on primary prevention of CKD; however, it might have a beneficial impact on secondary prevention of CKD progression or primary/secondary prevention of CVD, if early detection can be translated into effective treatment for CKD that delays its progression or leads to effective or even curative treatment [114] for underlying CKD that decreases morbidity and mortality directly related to CVD. Screening for disorders that increase risk of developing CKD, such as diabetes and obesity, might help in the primary prevention of CKD (and thereby CVS), but unfortunately we lack the long-term randomized controlled data to evaluate the utility of such population-based screening. Thus, most preventative disease organizations do not currently recommend population-based screening for CKD [115, 116]. Targeted screening of those at highest risk for CKD (diabetes, obesity, hypertension, and family history of kidney diseases) is presently advocated by many kidney disease organizations, but formal proof of the long-term benefits and lack of harms of such targeted screening is still lacking [115, 116]. Early detection and increased societal awareness of CKD were prominent themes of the 2020 World Kidney Day, endorsed by numerous nephrology organizations.
Secondary Prevention of Progression in established CKD
As described previously, patients with established diabetic or nondiabetic CKD have a tendency to progress to kidney failure (grade 5 CKD; previously known as ESKD) at variable rates, and they may present with no obvious clinical features of underlying CVD, atherosclerotic or non-atherosclerotic. There is great potential for both secondary prevention of progressive CKD and primary/secondary prevention of CVD in such patients [4]. Since advanced forms of CKD are often regarded as a “coronary artery disease risk equivalent” [117, 118] like certain people with diabetes, the characterization of interventions directed at CVD as primary or secondary in nature is often blurred (see Table 5 for a summary of the status of pharmacological interventions in patients with CKD designed to prevent CVD).
In general, strategies that slow or prevent the progression of CKD to higher grades or kidney failure also lower morbidity and mortality of CVD. The following paragraphs summarize the current status of pharmacologic and non-pharmacologic interventions in patients with established CKD to slow progression and/or reduce the risk of CVD morbidity or mortality.
5.1 Interventions in Established CKD That Slow Progression or Reduce CVD Risk or Both
RAS Inhibition
As a result of the Captopril, Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL), and Irbesartan in Diabetic Nephropathy (IDNT) Trials, among others, we are quite confident that intervention with RASi in established diabetic CKD (both type 1 and type 2 diabetes) can both slow progression of CKD (decreasing the rate of doubling of serum creatinine or developing kidney failure) and reduce CVD complications [108, 109, 119, 120]. Similar data that exist for nondiabetic CKD are also present, but the impact of RASi on progression of CKD may be disease dependent and highly variable [109]. Importantly, the extent of benefit is related both to persistent lowering of blood pressure and independently to the persistent reduction of albuminuria. The use of these agents for “reno-protection” and “cardio-protection” may also be applicable to many cases of nondiabetic CKD, when moderate to severe proteinuria (albuminuria) is present but the controlled trial evidence is much weaker.
In the SPRINT trial [103] mentioned above (where most patients were given RASi for blood pressure control), there were no reno-protective effects of intensive blood pressure control in patents with CKD at baseline, and, as stated previously, the cardio-protective effects of intensive blood pressure management were blunted considerably in patients with CKD at baseline. Combinations of RASi with dihydropyridine calcium channel blockers (CCB) are particularly effective and well tolerated for slowing CKD progression and reducing CVD incident events as shown by the ACCOMPLISH trial, despite a paradoxical tendency for increased urinary albumin excretion with such regimens [121, 122]. Direct renin inhibitors may have safety issues, such as hyperkalemia [123]. The safety profile of ACEi and ARB is quite favorable, but patients may initially manifest a decrement of GFR which is an expected consequence of their hemodynamic effects. Hyperkalemia may become an issue in more advanced CKD, but this can often be managed by concomitant oral administration of potassium-binding resins such as kayexalate [124]. A rise in serum creatinine levels (up to about 15% from baseline) can frequently be seen during the early phases of treatment with RASi. This is a reversible hemodynamic effect that usually indicates a favorable long-term response to treatment with this class of agents.
The combination of a neprilysin inhibitor (sacubitril) to an angiotensin receptor blocker (valsartan) has been shown to have clinical efficacy (compared to valsartan alone) in NYHA class II–IV heart failure for secondary prevention of heart failure events in HFrEF but not in HFpEF [125, 126]. About 36% of the subjects randomized to the HFrEF trial had preexisting CKD, and worsening of eGFR occurred less commonly with the sacubitril-valsartan combinations than valsartan alone. A preliminary analysis of this data shows that the sacubitril-valsartan combination slows the rate of progression of CKD compared to valsartan alone (presented at ASN meeting in 2019). The effects of the combination agent on heart failure-related events were not different in those with or without CKD at baseline. Thus, this combination may have beneficial effects on “progression” of CKD, but this has not yet been formally tested in a prospectively designed trial with “hard” CKD endpoints (doubling of serum creatinine or kidney failure). The effects of the sacubitril-valsartan combination on albuminuria needs further study. The combination of sacubitril and valsartan had no different effects on albuminuria compared to irbesartan [127]. To date, there have been no “head-to-head” trials of the sacubitril-valsartan combination versus SGLT2 inhibitors in patients with CKD with or without diabetes.
The target blood pressure associated with maximum benefit (all-cause mortality and/or reduction in CVD events) and safety in patients with established CKD is not well understood. Aggarwal and coworkers conducted a systematic analysis of pooled data from four randomized clinical trials (AASK, ACCORD, SPRINT, and MDRD) that included subjects with CKD (diabetic or nondiabetic). An intensive target of <130 mmHg systolic was associated with a reduction in all-cause mortality when compared to a target of <140 mmHg but only in those with grade 3 or greater CKD who were not undergoing intensive glycemic control as an aspect of management of comorbid type 2 diabetes [128]. However, the ACC/AHA blood pressure guidelines call for a target BP of <130/80 mmHg in persons with CKD [129].
Beta-Blockers for Congestive Heart Failure
Moderate to severely reduced GFRs are commonly found in patients with congestive heart failure, both HFrEF and HFpEF types. A comprehensive meta-analysis of RCTs examining beta-blockers for HFrEF (with normal sinus rhythm) has shown a benefit of these agents in terms of improved mortality rates in subjects with eGFRs of 30–59 mL/min/1.73 m2 [130]. Too few subjects with eGFR <30 mL/min/1.73 m2 were enrolled in the included trials for analysis. Mortality was not affected by the use of beta-blockers in HFrEF when atrial fibrillation was present, regardless of the level of eGFR (see below).
Statins and Other Hypolipidemic Agents
Statins generally have little or no impact on rates of progression of established CKD, although some studies with atorvastatin have shown some improvement in the rate of decline in eGFR [131]. Statin therapy is useful for prevention of ASCVD in non-dialysis-dependent CKD [132,133,134]. Statin therapy, when begun after dialysis therapy is required for ESKD, has no beneficial effects on CVD, despite substantial (35–40%) decline in LDL cholesterol (LDL-C) levels from baseline as shown by the 4D (atorvastatin) and AURORA (rosuvastatin) trials [135, 136]. The reason for the failure of stains to modify risk of ASCVD in kidney failure treated by dialysis is unknown but might have been due to the unique nature of the dyslipidemia in advanced CKD [134] or to the requirement for much lower levels of LDL-C to show a benefit [137]. In addition, vascular calcification in the media in CKD rather than atherosclerosis per se might be a partial explanation for the limited efficacy of statins in more advanced CKD, including ESKD (see “Pathophysiology” above).
However, the Study of Heart and Renal Protection (SHARP) trial involving 3023 subjects with dialysis-dependent CKD and 6247 with non-dialysis-dependent CKD (all with eGFR <60 mL/min/1.73 m2) allocated to a placebo or a simvastatin-ezetimibe combination showed beneficial effects on a composite CVD endpoint after a follow-up of 4 years [138]. The serum LDL cholesterol level decreased from 109 to 70 mg/dL in the active treatment group (a 36% decrease). The relative risk of a composite of major nonfatal ASCVD events decreased by 17% in the active compared to the placebo group overall, but no benefits were seen in the dialysis-dependent group. There was a (nonsignificant) trend toward greater benefit with higher eGFR and/or albuminuria at baseline. No benefits were seen in CVD or all-cause mortality. The treatment was generally well tolerated. The main benefits were a reduction in nonhemorrhagic stroke (risk ratio = 0.71; 95% CI = 0.57–0.92) and in coronary revascularization procedures (risk ratio = 0.71; 95% CI = 0.59–0.90). There was no evidence of a slower rate of CKD progression in the actively treated group. This and other studies have led to the general recommendation, further endorsed by the ACC/AHA 2018 cholesterol management guideline [139] that patients with non-dialysis CKD may receive statin therapy, regardless of the level of plasma LDL-C. The consensus is that patients receiving dialysis should not start statins, but if they are receiving statins, they may be continued, if tolerated. The specific question of whether adding a statin in patients with kidney failure (ESKD) who experience a new acute myocardial infarction or nonhemorrhagic or embolic stroke would lead to clinically meaningful benefits was not addressed by the SHARP trial. This requires further study, but many experienced clinicians would begin statin therapy in these circumstances, even in subjects on dialysis.
The impact of other hypolipidemic agents on CVD in patients with pro-protein convertase subtilisin/kexin 9 (PCSK9) inhibitors, omega-3 fatty acids, fibric acid derivatives, and novel lipid-lowering agents (bempedoic acid, lomitapide, apabetalone) has not been sufficiently studied in large well-powered RCTs of long duration in patients with CKD [140,141,142,143]. The ability of PCSK9 inhibitors to lower LDL-C levels needs further study in CKD, but the results from the Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk (FOURIER) trial are highly encouraging [144]. Fibric acid derivatives (such as fenofibrate) can increase PCSK9 production and can also cause a dose-dependent, but reversible, decrease in GFR by a direct effect on the kidney. However, in diabetic patients, fenofibrate may reduce total CV events (mainly fewer nonfatal myocardial infarctions), reduce albuminuria, decrease retinopathy, and possibly slow progression of CKD [145, 146]. The effects on proteinuria and progression of CKD have not been adequately studied in nondiabetic CKD.
Sodium-Glucose Transporter 2 Inhibitors
The dramatic emergence of sodium-glucose transporter 2 inhibitors (SGLT2i), causing an acquired form of renal glycosuria, as effective and reasonably safe agents for slowing progression of established CKD (eGFR 30–59 mL/minj/1.73 m2) and avoiding hospitalization for heart failure (mainly HFrEF) in patients with type 2 diabetes mellitus (and perhaps nondiabetic kidney disease as well) has altered the landscape of secondary prevention of CKD and also primary and secondary prevention of CVD in T2DM [147,148,149,150,151,152,153]. Data from large randomized controlled trials (such as Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Patients [EMPA-REG], Canagliflozin Cardiovascular Assessment Program [CANVAS], Canagliflozin and Renal Endpoint Diabetes with Established Nephropathy Clinical trial [CREDENCE], and Dapagliflozin Effect on Cardiovascular Event Trial [DECLARE-TIMI 58]) (see [145,146,147,148,149,150,151] for reviews) have very convincingly shown efficacy for slowing progression of CKD (in type 2 diabetes) and for reduction of CVD events , primarily heart failure. Most of the subjects randomized in these trials had overt CVD prior to randomization. However, only canagliflozin is approved by the FDA for slowing progression of CKD (in patients with diabetic kidney disease and albuminuria of >300 mg/day) and reducing the risk of hospitalization for CHF (usually HFrEF), largely the result of the CANVAS and CREDENCE trials. A meta-analysis of these trials involving 38,723 subjects followed for a mean of 2.9 years with 20% having established CKD (grades 1–3B) and 59% with known CVD , including HF, Showed that the use of SGLT2i (usually added to stable doses of RASi) reduced the HR of a composite of major adverse CV events (MACE) to 0.88 (95% CI = 0.82–0.94) and significantly reduced the occurrence of hospitalization for CHF (HR = 0.66; 95% CI = 0.60–0.76), CV death (HR = 0.83; 95%CI = 0.75–0.92), and all-cause death (HR = 0.85; 95% CI = 0.79–0.92) [147]. There was no overall benefit on stroke. These benefits were observed irrespective of CKD status (except for stroke which was decreased only in those with CKD at baseline). The rate of progression of CKD was reduced (HR 0.66; 95 CI = 0.53–0.81) often in association with a reduction in albuminuria in the CREDENCE trial [148]. The beneficial effect on slowing rates of progression in CKD is much greater in those subjects with higher degrees of baseline albuminuria, especially if >300 mg/day. The beneficial effects on MACE were seen largely when these agents were used for primary prevention. Additional systematic reviews and meta-analyses have shown that SGLT2i are primarily effective for secondary prevention of CVD in diabetic patients, mostly for reducing hospitalization for HFrEF and slowing progressions of CKD, with less robust effects on ASCVD. The extent of benefit varies with baseline eGFR – greater benefit for HFrEF and lesser benefit for CKD progression in patients with more severe grades of CKD [153].
These beneficial cardio- and reno-protective effects of SGLT2i cannot be easily explained by the modest reduction in HbA1c and systolic blood pressure, so they seem to be manifestations of direct effects on the heart and kidney or systemic effects independent of glycemia and blood pressure control. The mechanism of action of these agents upon these outcomes is not presently fully understood and may not be a class effect but one that varies between agents within the class. Afferent arteriolar constriction reducing maladaptive glomerular capillary pressure seems to be involved in reno-protection with all agents in the class [152]. An augmentation of tubulo-glomerular feedback is a popular hypothesis [154]. Basically, this hypothesis advances the idea that increased delivery of NaCl to the distal nephron (by virtue of a proximal nephron reduction of both glucose and NaCl reabsorption) activates a process located at the macula densa and juxtaglomerular axis of the same nephron to constrict the afferent arteriole and thus reduce glomerular capillary pressure (and single nephron GFR). However, these agents also affect volume excess (via natriuresis), reduce inflammation , lower body weight, lower plasma uric acid levels, reduce oxidative stress, impair fibrosis, and impact Na:H+ exchange in myocardium, among other effects [152, 154]. These pleiotropic effects of SGLT2i beyond their rather mild hypoglycemic effect (absent in patients with more advanced CKD) make these agents attractive candidates for treating patients with nondiabetic CKD with or without CVD (such as is being studied in Dapagliflozin in CKD trial [DAPA-CKD]). The preliminary results of this latter trial seem to indicate a favorable effect on CKD progression and CHF, even in subjects without diabetes [151, 155, 156]. An increase in serum ketone bodies and their influence on organ bioenergetics and inflammatory mediators might provide a potential unifying mechanism for the salutary effects of SGLT2i on the heart and kidney [157]. In addition, an exploratory analysis of the DAPA-HF trial has demonstrated a beneficial effect on worsening heart failure and CV mortality when dapagliflozin is added to recommended therapy in both diabetic and nondiabetic patients [158].
While these agents appear to have a reasonable safety profile, non-hyperglycemic ketoacidosis, acute kidney injury, severe perineal infections (Fournier’s gangrene), and in some studies (mainly CANVAS) an excess of lower limb amputations have been observed so caution and close surveillance is indicated.
The aforementioned trials limited randomization to those subjects with an eGFR >30 mL/min/1.73 m2. The safety and efficacy of these agents in more advanced CKD is not yet known. Most patients studied so far have utilized SGLT2i added to a baseline of optimal RASi, so we are not yet sure of the effect of these agents when used as monotherapy, but there are important interactions between SGLT2i and RASi in diabetic subjects, particularly in relation to volume control [159, 160]. The effect of these agents on HFrEF (see also Reference [159] for update on heart failure in CKD) is very impressive. The effect of SGLT2i on HFpEF is under study (e.g., PRESERVED-HF, EMPEROR-Preserved, EMPERIAL-Preserved). The beneficial effects of sacubitril-valsartan combinations have not yet been directly compared to SGLT2i in CKD with HFrEF.
Because of their weak hypoglycemic effects (especially in CKD with reduced eGFR), they are best combined with other hypoglycemic agents, especially metformin or a glucagon-like peptide 1 receptor agonist (GLP1), in T2DM to maintain HBA1c within recommended ranges (see below) [160,161,163]. Hypoglycemia is rare with these agents. Concomitant use of diuretics is not contraindicated, but such patients need careful follow-up to avoid iatrogenic volume depletion and acute kidney injury. Patients with CHF in T2DM are good candidates for SGLT2 inhibitor therapy, even without CKD. SGLT2 inhibitors have now become “standard of care” for patients with CKD (grades 1–3B) and T2DM, especially if HFrEF is present. SGLT2 inhibitors might also reduce major atherosclerotic events, if HBA1c is decreased.
Glycemic Control (in Patients with Diabetes and CKD)
Adequate standard glycemic control is a well-established goal in prevention of microvascular disease (diabetic nephropathy and retinopathy) and macrovascular ASCVD in patients with T1DM and T2DM [161, 163]. In T2DM patients with CKD, with or without overt CVD, the use of metformin (only if the eGFR is >30 mL/min/1.73 m2), GLP1 receptor agonists (such as dulaglutide, exenatide, lixisenatide, liraglutide, semaglutide), and/or SGLT2i (if eGFR is >30 mL/min/1.73 m2) is preferred in patients with CKD or without CHF or overt ASCVD [163,164,166]. Very recently, a comprehensive decision algorithm for prescribing SGLT2 inhibitors and GLKP-1 receptor agonists for diabetic kidney disease has been published [167]. This is a very useful approach for CVD and kidney failure risk stratification. Sulfonylureas and dipeptidyl-peptidase 4 inhibitors (DPP-4i, gliptins) have little if any beneficial effects on CVD in T2DM [162]. Insulin therapy is necessary in many T1DM and some T2DM patients, but it should be avoided in moderately advanced CKD if possible due to an enhanced risk for hypoglycemia. A goal of achieving a HbA1c of 6.5–8.0% is reasonable, depending on the grade of CKD (see [162, 163]).
Whether intensive glycemic control has any advantage in patients with CKD is doubtful. The Action to Control Cardiovascular Risk in Diabetes (ACCORD) targeted a HbA1c of <6.5% reduced risk for nonfatal myocardial infarction but increased all-cause mortality (mostly due to CV event) [168], especially in those with mild to moderate CKD [169]. Older, frail subjects and those with advanced kidney disease are likely to fare poorly with intensive programs of glycemia control [170]. The Veterans Affairs Diabetes Trial (VADT) showed some benefits on CVD events of intensive glycemia control over the first 5.6 years of follow-up, but this effect was not sustained on prolonged follow-up totaling 15 years (active treatment + posttrial observation) [171]. No legacy effect of intensive treatment on CV event rate was observed. However, after 11 years of follow-up (with 5.6 years of intensive glycemic control), the patients in the intensive therapy group had a 34% higher odds of maintaining an eGFR of >60 mL/min/1.73 m2 compared to the standard therapy group, suggesting that a legacy effect is seen with CKD outcomes [172].
Peroxisome proliferator-activated receptor gamma agonists (thiazolidinediones/glitazones such as pioglitazone) can improve glycemic control in T2DM and may slow progression of kidney disease, reduce proteinuria, and improve secondary CV outcomes [172,173,175]. But CHF can be aggravated, and they can cause edema, somewhat limiting their overall usefulness for secondary prevention of CVD in CKD.
Volume Control
While not extensively studied , the use of salt restriction and diuretics is commonly advised in CKD to minimize the effect of chronic volume expansion on hypertension and LVH and the undesirable effects in CVD including CHF. In the initial stages of CKD, thiazide diuretics may be effective, but in later stages (eGFR <30 mL/min/1.73 m2) they lose their natriuretic efficacy , even though they may retain some antihypertensive effect [176]. Loop-acting diuretics (furosemide, bumetanide, torsemide) may be preferred in such patients. Mineralocorticoid receptor antagonists (MRA: spironolactone, eplerenone, finerenone) can be used to improve blood pressure control in CKD when hypertension is resistant to two or more agents, and such treatment may have additional CV benefits such as improving CHF [177, 178]. However, hyperkalemia is a risk, particularly when patients with advanced CKD are concomitantly receiving RASi. This risk can be attenuated by coadministration of a potassium-binding resin such a patiromer or sodium zirconium cyclosilicate [124]. Mineralocorticoid receptor antagonism might improve outcomes in advanced dialysis-requiring kidney failure with an acceptable margin of safety, but this will only be proven by ongoing clinical trials [178, 179].
Diet and Other Non-pharmacologic Approaches
The use of dietary intervention for prevention of progression of CKD and for primary or secondary prevention of CVD in patients with established CVD has a long and checkered history. The difficult in doing rigorously controlled, well-powered RCTs has limited the development of evidence-based recommendations. Population-wide observational studies have suggested that a “healthy” eating style, in addition to avoiding obesity, smoking, and obtaining moderate exercise, can lower risk of CVD. However, this benefit of primary prevention of CKD has never been confirmed in an RCT. A large body of observational data support a beneficial effect of a low-protein diet on progression of CKD (secondary prevention), but this has also not been unequivocally confirmed in an RCT [180, 181]. Whether such low-protein diets are also beneficial for CVD prevention in such CKD patients remains uncertain. Also, it remains uncertain if high-protein diet causes CKD or accelerates its progression [96, 97], but consumption of increased amounts of processed or unprocessed red meat may have deleterious effects on CVD risk in CKD [96, 97].
A diet rich in plant-based foods, a Mediterranean style diet, and/or a DASH-type diet rich in fruits and vegetables and low in salt and red meat [182, 183] seem to have cardio-protective properties and perhaps a reno-protective effect [183, 184], perhaps via better control of ideal weight, blood pressure, avoidance of excess sodium salt, and improvement in potassium intake. A prudent, healthy style diet of a DASH, Mediterranean, or plant-based forms and avoiding saturated fat by replacing it with poly- or monounsaturated fats and vegetable sources of protein should be advised for all patients with CKD, with or without CVD. Avoiding sources of dietary cholesterol does not seem to be necessary in patients with CKD, with or without CVD. The value of prebiotics and/or probiotics for primary or secondary prevention of CVD in CKD remains largely unknown [185].
Anemia Management
Moderate to severe anemia (hemoglobin of 9–10 gm/dL) is fairly common in more advanced CKD (eGFR <45 mL/min/1.73 m2). This is due to a combination of relative iron deficiency and inadequate endogenous erythropoietin production. Anemia of this degree can contribute to LV remodeling and LVH [83]. Treatment of iron deficiency by oral or parenteral iron is indicated. Treatment with exogenous erythropoietin is not advised in pre-ESKD forms of CKD as these agents may promote CVD, especially stroke [186]. Patients with CKD and a history of stroke should avoid exogenous erythropoietin unless the anemia is severe (hemoglobin <9 gm/dL and nonresponsive to iron repletion therapy).
Vascular Calcification
Only very limited information is available concerning interventions to reduce vascular CAC for secondary prevention of CVD in CKD. Very recently, denosumab (a monoclonal antibody inhibitor of the bone resorption mediator – RANKL) has been shown to slow or stop progressive CAC artery calcification in advanced dialysis-dependent kidney failure, but whether this has any effect on CVD events is unknown [187]. Non-calcium-containing phosphate binders in patients with moderate non-dialysis-requiring CKD may actually increase the frequency of CAC [188]. The use of cinacalcet to reduce PTH levels has not been shown to reduce the risk of ASCVD events in kidney failure treated by dialysis [189]. A role of oral vitamin K supplementation or sodium thiosulfate for prevention or treatment of vascular calcification is unknown but is being studied.
Antiplatelet Treatment for Prevention of CVD in Patients with CKD
Antiplatelet therapy using aspirin or other agents appears to reduce the risk of CVD events in patients with CKD while having no effect on progression of CKD [190]. The risk of adverse bleeding events from these agents is increased in CKD. One systematic review and meta-analysis of RCTs involving 27,773 patients with CKD showed that for every 1000 patients with CKD treated for 12 months with antiplatelet agents, 23 major CVD events will be prevented and 9 major bleeding events will occur [190]. Another study using propensity matching came to opposite conclusions, with increased risks of ASCVD events and progression of CKD with the use of low-dose aspirin [191]. Aspirin, if it is used at all in CKD, is not effective for primary prevention (if you believe that CKD is a coronary risk equivalent), but it may be useful for secondary prevention of ASCVD but with some level of bleeding risk.
Anticoagulants for Atrial Fibrillation
Non-valvular atrial fibrillation (NVAFib) is common in CKD (see above), thought to be due to LVH, underlying HFpEF or HFrEF, and an enlarged left atrium. Such patients are at risk for embolic stroke. Prophylactic anticoagulation using warfarin or a novel oral anticoagulant (NOAC; apixaban, rivaroxaban, dabigatran, edoxaban) may be indicated [192]. The bleeding risk is increased in advanced CKD, so the balance between efficacy and safety is altered in CKD. In addition, warfarin and the vitamin K deficiency it produces can have unfavorable effects on vascular calcification in CKD , including calciphylaxis [193]. In addition, anticoagulation in CKD may predispose to anticoagulant-related nephropathy, as the cause of AKI superimposed on CKD, probably due to large amounts of hemoglobin in the tubular lumina provoking oxidant-induced cellular injury [194]. At present, only limited trials of prophylaxis of embolic stroke in CKD with have been conducted, as advanced CKD has been an exclusion factor in many trials. A recent systematic review and meta-analysis [195] have shown that warfarin is largely ineffective in prevention of ischemic stroke in patients with kidney failure (grade 5 CKD, ESKD). The risk of hemorrhagic stroke was increased (HR = 1.49; 95% CI = 1.03–1.94), but there was no added risk of major bleeding or increased mortality. Apixaban appears to be preferred in moderately advanced kidney failure because of its favorable pharmacokinetic profile in patients with reduced eGFR [196]. As stated previously, treatment of HFrEF in patients with NVAF using beta-blockers does not appear to reduce mortality in patients with CKD regardless of the extent of renal impairment [130].
Hypouricemic Agents
Asymptomatic hyperuricemia (plasma uric acid levels usually between 7 and 9 mg/dL) is fairly common in CKD, mainly in those with grade 3–5 CKD. A large body of observational and experimental data strongly suggests that this hyperuricemia in an independent risk factor for CVD and for progression of CVD, mainly ASCVD [196,197,199]. Cutoff values for serum uric acid levels identifying risk for acute myocardial infarction have been established in women but not in men [198]. Controlled trials of hypouricemic agents (mainly allopurinol) have had mixed results both for reno- and cardio-protection [197]. Due to a well-known but uncommon propensity for allopurinol to produce devastating side effects (exfoliative dermatitis, vasculitis) which are hard to predict in individual patients and uncertainty concerning its beneficial effects, it is not generally recommended for treatment of asymptomatic hyperuricemia in CKD. This is a very controversial area, and many experts do not recommend the use of hypouricemic agents in asymptomatic hyperuricemia for the purpose of slowing the rate of progression of CKD [200]. In the view of some, febuxostat is not recommended for this indication, as it has been associated with an increased risk for CVD [201]. However, the association of febuxostat with enhanced CVD risk has been challenged by recent observations, including the febuxostat for Cerebral and Cardiovascular Events Prevention Study from Japan [202]. This open label RCT including 1070 patients with or at risk of cerebral, CV, or renal disease showed that febuxostat reduced serum uric acid and decreased the primary composite event rate of cerebral, CV, and renal events (HR = 0.75; 95% CI = −0.59–0.95). There was no increase in CVD events in the febuxostat-treated group, and renal impairment was marginally less in the febuxostat group (HR = 0.745; 95% CI = 0.56–0.99). Clearly, this field is in a dynamic state, and further studies may help to clarify the uncertainties that exist concerning the risk/benefit ratio for the use of either allopurinol or febuxostat for cardio-renal protection in CKD with asymptomatic hyperuricemia. These agents have a clear and unequivocal role for treatment of symptomatic gout with or without CKD or CVD.
Revascularization Procedures
A comprehensive discussion of this complex topic is beyond the scope of this chapter. Such procedures are generally used to treat underlying, overt, often acute, ischemic heart disease. They may not be indicated in patients with stable angina, including patients with advanced CKD, as studied in the ISCHEMIA-CKD trial [203, 204].
Implantable Defibrillators
This topic is also beyond the scope of this discussion. Implantable electrical defibrillators are used to prevent a recurrence of ventricular fibrillation (VF) in patients who survive an episode of VF and “sudden cardiac death” or in patients deemed to be at high risk for fatal ventricular arrhythmias (such as patients with HFrEF and EF <35%) [205]. The benefits conferred by implantable electrical defibrillators measured in terms of prolonged survival appear to be limited in patients with CKD, especially those with advanced CKD or ESRD treated by dialysis.
6 Conclusions
Chronic kidney disease is a common problem that is frequently accompanied by covert or overt cardiovascular disease that takes many forms, both atherosclerotic and non-atherosclerotic in origin. The association of CKD and CVD is at least in part due to risk factors held in common, such as advancing. Age, diabetes, obesity, hypertension, and dyslipidemia but CVD-promoting factors unique to CKD also contribute. The added burden of CVD seen in CKD contributes to a very great extent to the morbidity and mortality of CKD. At least to some extent, these adverse consequences are preventable. Primary prevention of CKD is at least feasible, though not proven, by better control of high blood pressure, avoidance of obesity and diabetes, minimizing exposure to nephrotoxic agents (including drugs, pesticides, air pollution, and cigarette smoking), and better maternal health, thus reducing the prevalence of low birth weight and congenital nephropenia. But secondary prevention of progression of CKD to ESKD and management of overt or covert CVD using strategies to minimize the adverse consequences of dyslipidemia, reducing chronic volume expansion, improving glycemic control (in diabetics), improving nutrition, safely treating anemia, controlling the accumulation of “uremic” toxins, inhibiting vascular calcification, preventing heart failure and left ventricular hypertrophy, and reducing the prevalence of cardiac arrhythmias are all part of CVD prevention in CKD. Many gaps exist in our knowledge of how best to safely and effectively prevent CVD in patients with CKD, in part because of limitations for entry of patients with overt CKD into CVD prevention trials. Nevertheless, the recent upsurge of RCTs examining the effects of novel agents (e.g., SGLT2 inhibitors, hypouricemic agents, hypolipidemic agents, drugs for optimal glycemic control) in patients with both CKD and overt or covert CVD augurs a favorable future for this important objective.
References
Kidney Disease Improving Global Outcomes (KDIGO) 2012 Clinical Practice Guidelines for the evaluation and management of chronic kidney diseases. Kidney Int Suppl. 2013; 3:1–150.
Vallianou NG, Mitesh S, Gkogkou A, et al. Chronic kidney disease and cardiovascular disease: is there any relationship? Curr Cardiol Rev. 2019;15:55–63.
Sarnak MJ, Amann K, Bangalore S, Cavalcante JL, Charytan DM, Craig JC, Gill JS, Hlatky MA, Jardine AG, Landmesser U, Newby LK, Herzog CA, Cheung M, Wheeler DC, Winkelmayer WC, Marwick TH, Conference Participants. Chronic kidney disease and coronary artery disease: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019;74:1823–38.
Ali S, Dave N, Virani SS, Navaneethan SD. Primary and secondary prevention of cardiovascular disease in patients with chronic kidney disease. Curr Atheroscler Rep. 2019;21:32.
Thomas B, Matsushita K, Abate KH, Al-Aly Z, Ärnlöv J, Asayama K, Atkins R, Badawi A, Ballew SH, Banerjee A, Barregård L, Barrett-Connor E, Basu S, Bello AK, Bensenor I, Bergstrom J, Bikbov B, Blosser C, Brenner H, Carrero JJ, Chadban S, Cirillo M, Cortinovis M, Courville K, Dandona L, Dandona R, Estep K, Fernandes J, Fischer F, Fox C, Gansevoort RT, Gona PN, Gutierrez OM, Hamidi S, Hanson SW, Himmelfarb J, Jassal SK, Jee SH, Jha V, Jimenez-Corona A, Jonas JB, Kengne AP, Khader Y, Khang YH, Kim YJ, Klein B, Klein R, Kokubo Y, Kolte D, Lee K, Levey AS, Li Y, Lotufo P, El Razek HMA, Mendoza W, Metoki H, Mok Y, Muraki I, Muntner PM, Noda H, Ohkubo T, Ortiz A, Perico N, Polkinghorne K, Al-Radaddi R, Remuzzi G, Roth G, Rothenbacher D, Satoh M, Saum KU, Sawhney M, Schöttker B, Shankar A, Shlipak M, Silva DAS, Toyoshima H, Ukwaja K, Umesawa M, Vollset SE, Warnock DG, Werdecker A, Yamagishi K, Yano Y, Yonemoto N, Zaki MES, Naghavi M, Forouzanfar MH, Murray CJL, Coresh J, Vos T, Global Burden of Disease 2013 GFR Collaborators, CKD Prognosis Consortium, Global Burden of Disease Genitourinary Expert Group. Global cardiovascular and renal outcomes of reduced GFR. J Am Soc Nephrol. 2017;28:2167–79.
Marx N, Noels H, Jankowski J, Floege J, Fliser D, Böhm M. Mechanisms of cardiovascular complications in chronic kidney disease: research focus of the Transregional Research Consortium SFB TRR219 of the University Hospital Aachen (RWTH) and the Saarland University. Clin Res Cardiol. 2018;107(Suppl 2):120–6.
United States Renal Data System. 2019 annual data report: Atlas of chronic kidney disease and end-stage renal failure in the United States. Bethesda: National Institutes of Health, National Institute of Diabetes, Digestive and Kidney Disease; 2019.
United States Renal Data System. 2018 Annual Data Report: Atlas of chronic kidney disease and end-stage renal disease in the United States. Chapter 4: Cardiovascular disease in patients with CKD. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2018.
Hill NR, Fatoba ST, Oke JL, Hirst JA, O’Callaghan CA, Lasserson DS, et al. Global prevalence of chronic kidney disease—a systematic review and meta-analysis. PLoS One. 2016;11(7):e158765.
Bikbov B, Purcell CA, Levey AS, et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395:709–33.
Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298:2038–47.
Delanaye P, Jager KJ, Bökenkamp A, Christensson A, Dubourg L, Eriksen BO, Gaillard F, Gambaro G, van der Giet M, Glassock RJ, Indridason OS, van Londen M, Mariat C, Melsom T, Moranne O, Nordin G, Palsson R, Pottel H, Rule AD, Schaeffner E, Taal MW, White C, Grubb A, van den Brand JAJG. CKD: a call for an age-adapted definition. J Am Soc Nephrol. 2019;30:1785–805.
Delanaye P, Glassock RJ, De Broe ME. Epidemiology of chronic kidney disease: think (at least) twice! Clin Kidney J. 2017;10:370–4.
Glassock RJ, Warnock DG, Delanaye P. The global burden of chronic kidney disease: estimates, variability and pitfalls. Nat Rev Nephrol. 2017;13:104–14.
Thompson S, James M, Wiebe N, Hemmelgarn B, Manns B, Klarenbach S, et al. Cause of death in patients with reduced kidney function. J Am Soc Nephrol. 2015;26(10):2504–11.
Matsushita K, van der Velde M, Astor BC, et al, for the CKD Prognosis Consortium. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375:2073–81.
Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–305.
Pun PH, et al. The interplay between chronic kidney disease, sudden cardiac death, and ventricular arrhythmias. Adv Chronic Kidney Dis. 2014;21(6):480–8.
Briasoulis A, Bakris GL. Chronic kidney disease as a coronary artery disease risk equivalent. Curr Cardiol Rep. 2013;15:340.
Tonelli M, Muntner P, Lloyd A, et al. Risk of coronary events in people with chronic kidney disease compared with those with diabetes: a population-level cohort study. Lancet. 2012;380(9844):807–14.
Astor BC, Coresh J, Heiss G, Pettitt D, Sarnak MJ. Kidney function and anemia as risk factors for coronary heart disease and mortality: the Atherosclerosis Risk In Communities (ARIC) study. Am Heart J. 2006;151:492–500.
Bundy JD, Chen J, Yang W, et al., for the CRIC Study Investigators. Risk factors for progression of coronary artery calcification in patients with chronic kidney disease: the CRIC study. Atherosclerosis. 2018;271:53–60.
Go AS, Bansal N, Chandra M, et al., for the ADVANCE Study Investigators. Chronic kidney disease and risk for presenting with acute myocardial infarction versus stable exertional angina in adults with coronary heart disease. J Am Coll Cardiol. 2011;58:1600–7.
Kottgen A, Russell SD, Loehr LR, et al. Reduced kidney function as a risk factor for incident heart failure: the Atherosclerosis Risk In Communities (ARIC) study. J Am Soc Nephrol. 2007;18:1307–15.
He J, Shlipak M, Anderson A, et al. Risk factors for heart failure in patients with chronic kidney disease: the CRIC (Chronic Renal Insufficiency Cohort) study. J Am Heart Assoc. 2017;6. pii: e005336.
Smith DH, Thorp ML, Gurwitz JH, Mcmanus DD, Goldberg RJ, Allen LA, et al. Chronic kidney disease and outcomes in heart failure with preserved versus reduced ejection fraction: the Cardiovascular Research Network PRESERVE Study. Circ Cardiovasc Qual Outcomes. 2013;6:333–42.
Hillege HL, Nitsch D, Pfeffer MA, et al. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation. 2006;113:671–8.
Marwick TH, Amann K, et al. Chronic kidney disease and valvular heart disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019;96:836–49.
Samad Z, Sivak JA, Phelan M, et al. Prevalence and outcomes of left-sided valvular heart disease associated with chronic kidney disease. J Am Heart Assoc. 2017;6(10): pii: e006044.
Guerraty MA, Chai B, Hsu JY, et al. Relation of aortic valve calcium to chronic kidney disease (from the Chronic Renal Insufficiency Cohort Study). Am J Cardiol. 2015;115:1281–6.
Ix JH, Shlipak MG, Katz R, et al. Kidney function and aortic valve and mitral annular calcification in the Multi-Ethnic Study of Atherosclerosis (MESA). Am J Kidney Dis. 2007;50:412–20.
Lee M, Saver JL, Chang KH, Liao HW, Chang SC, Ovbiagele B. Low glomerular filtration rate and risk of stroke: meta-analysis. BMJ. 2010;341:c4249.
Lee M, Saver JL, Chang KH, Ovbiagele B. Level of albuminuria and risk of stroke: systematic review and meta-analysis. Cerebrovasc Dis. 2010;30:464–9.
Abramson JL, Jurkovitz CT, Vaccarino V, Weintraub WS, McClellan W. Chronic kidney disease, anemia, and incident stroke in a middle-aged, community-based population: the ARIC study. Kidney Int. 2003;64:610–5.
O’Hare AM, Glidden DV, Fox CS, Hsu CY. High prevalence of peripheral arterial disease in persons with renal insufficiency: results from the National Health and Nutrition Examination Survey 1999-2000. Circulation. 2004;109(3):320–3.
Wattanakit K, Folsom AR, Selvin E, Coresh J, Hirsch AT, Weatherley BD. Kidney function and risk of peripheral arterial disease: results from the Atherosclerosis Risk In Communities (ARIC) study. J Am Soc Nephrol. 2007;18:629–36.
Wang GJ, Shaw PA, Townsend RR, Anderson AH, Xie D, Wang X, Nessel LC, Mohler ER, Sozio SM, Jaar BG, et al; for the CRIC Study Investigators. Sex differences in the incidence of peripheral artery disease in the Chronic Renal Insufficiency Cohort. Circ Cardiovasc Qual Outcomes. 2016;9:S86–93.
Wu CK, Yang CY, Tsai CT, et al. Association of low glomerular filtration rate and albuminuria with peripheral arterial disease: the National Health and Nutrition Examination Survey, 1999-2004. Atherosclerosis. 2009;209(1):230–4.
Wattanakit K, Folsom AR, Criqui MH, et al. Albuminuria and peripheral arterial disease: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis. 2008;201(1):212–6.
Soliman EZ, Prineas RJ, Go AS, Xie D, Lash JP, Rahman M, Ojo A, Teal VL, Jensvold NG, Robinson NL, Dries DL, Bazzano L, Mohler ER, Wright JT, Feldman HI, Chronic Renal Insufficiency Cohort (CRIC) Study Group. Chronic kidney disease and prevalent atrial fibrillation: the Chronic Renal Insufficiency Cohort (CRIC). Am Heart J. 2010;159:1102–7.
Alonso A, Lopez FL, Matsushita K, et al. Chronic kidney disease is associated with the incidence of atrial fibrillation: the Atherosclerosis Risk In Communities (ARIC) study. Circulation. 2011;123:2946–53.
McManus DD, Corteville DCM, Shlipak MG, Whooley MA, Ix JH. Relation of kidney function and albuminuria with atrial fibrillation (from the Heart and Soul Study). Am J Cardiol. 2009;104:1551–5.
Olesen JB, Lip GY, Kamper AL, Hommel K, Køber L, Lane DA, Lindhardsen J, Gislason GH, Torp-Pedersen C. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med. 2012;367:625–35.
Carrero JJ, Trevisan M, Sood MM, Bárány P, Xu H, Evans M, Friberg L, Szummer K. Incident atrial fibrillation and the risk of stroke in adults with chronic kidney disease: the Stockholm CREAtinine Measurements (SCREAM) project. Clin J Am Soc Nephrol. 2018;13(9):1314–20.
Mace-Brickman T, Eddeen AB, Carrero JJ, Mark PB, Molnar AO, Lam NN, Zimmerman D, Harel Z, Sood MM. The risk of stroke and stroke type in patients with atrial fibrillation and chronic kidney disease. Can J Kidney Health Dis. 2019;6:1–9.
Whitman IR, Feldman HI, Deo R. CKD and sudden cardiac death: epidemiology, mechanisms, and therapeutic approaches. J Am Soc Nephrol. 2012;23:1929–39.
Goldenberg I, Moss AJ, McNitt S, et al. Relations among renal function, risk of sudden cardiac death, and benefit of the implanted cardiac defibrillator in patients with ischemic left ventricular dysfunction. Am J Cardiol. 2006;98:485–90.
Afshinnia F, Pennathur S. Lipids and cardiovascular risk with CKD. Clin J Am Soc Nephrol. 2020;15(1):5–7.
Contreras G, Hu B, Astor BC, Greene T, Erlinger T, Kusek JW, Lipkowitz M, Lewis JA, Randall OS, Hebert L, Wright JT Jr, Kendrick CA, Gassman J, Bakris G, Kopple JD, Appel LJ, African-American Study of Kidney Disease, and Hypertension Study Group. Malnutrition-inflammation modifies the relationship of cholesterol with cardiovascular disease. J Am Soc Nephrol. 2010;21:2131–42.
Moradi H, Vaziri ND. Molecular mechanisms of disorders of lipid metabolism in chronic kidney disease. Front Biosci (Landmark Ed). 2018;23:146–61.
Lamprea-Montealegre JA, Staplin N, Herrington WG, Haynes R, Emberson J, Baigent C, de Boer IH, SHARP Collaborative Group. Apolipoprotein B, triglyceride-rich lipoproteins, and risk of cardiovascular events in persons with CKD. Clin J Am Soc Nephrol. 2020;15(1):47–60.
Vaziri ND. Disorders of lipid metabolism in nephrotic syndrome: mechanisms and consequences. Kidney Int. 2016;90(1):41–52.
Chang TI, Streja E, Ko GJ, Naderi N, Rhee CM, Kovesdy CP, Kashyap ML, Vaziri ND, Kalantar-Zadeh K, Moradi H. Inverse association between serum non-high-density lipoprotein cholesterol levels and mortality in patients undergoing incident hemodialysis. J Am Heart Assoc. 2018;7(12):e009096.
Ku E, Lee BJ, Wei J, Weir MR. Hypertension in CKD: core curriculum 2019. Am J Kidney Dis. 2019;74(1):120–31.
Qian Q. Salt, water and nephron: mechanisms of action and link to hypertension and chronic kidney disease. Nephrology (Carlton). 2018;23 Suppl 4:44–9.
Campese VM. Pathophysiology of resistant hypertension in chronic kidney disease. Semin Nephrol. 2014;34:571–6.
Zoccali C, London G. Con: vascular calcification is a surrogate marker, but not the cause of ongoing vascular disease, and it is not a treatment target in chronic kidney disease. Nephrol Dial Transplant. 2015;3:352–7.
Kassem H, Chatila K. Mineralocorticoid receptor antagonists in heart failure patients with chronic kidney disease: why, when, and how? Curr Opin Nephrol Hypertens. 2020;29:258–63.
Parfrey PS, Lauve M, Latremouille-Viau D, Lefebvre P. Erythropoietin therapy and left ventricular mass index in CKD and ESRD patients: a meta-analysis. Clin J Am Soc Nephrol. 2009;4:755–62.
Zoccali C, Mallamaci F, Tripepi G. Novel cardiovascular risk factors in end-stage renal disease. J Am Soc Nephrol. 2004;15 Suppl 1:S77–80.
Kim RB, Morse BL, Djurdjev O, Tang M, Muirhead N, Barrett B, Holmes DT, Madore F, Clase CM, Rigatto C, Levin A, CanPREDDICT Investigators. Advanced chronic kidney disease populations have elevated trimethylamine N-oxide levels associated with increased cardiovascular events. Kidney Int. 2016;89:1144–52.
Vanholder R, Pletinck A, Schepers E, Glorieux G. Biochemical and clinical impact of organic uremic retention solutes: a comprehensive update. Toxins (Basel). 2018;10(1). pii: E33.
Gao S, Xu J, Zhang S, Jin J. Meta-analysis of the association between fibroblast growth factor 23 and mortality and cardiovascular events in hemodialysis patients. Blood Purif. 2019;47 Suppl 1:24–30.
Liu Q, Zhu LJ, Waaga-Gasser AM, Ding Y, Cao M, Jadhav SJ, Kirollos S, Shekar PS, Padera RF, Chang YC, Xu X, Zeisberg EM, Charytan DM, Hsiao LL. The axis of local cardiac endogenous Klotho-TGF-β1-Wnt signaling mediates cardiac fibrosis in human. J Mol Cell Cardiol. 2019;136:113–24.
Böckmann I, Lischka J, Richter B, Deppe J, Rahn A, Fischer DC, Heineke J, Haffner D, Leifheit-Nestler M. FGF23-mediated activation of local RAAS promotes cardiac hypertrophy and fibrosis. Int J Mol Sci. 2019;20(18). pii: E4634.
Tomaschitz A, Piecha G, Ritz E, Meinitzer A, Haas J, Pieske B, Wiecek A, Rus-Machan J, Toplak H, März W, Verheyen N, Gaksch M, Amrein K, Kraigher-Krainer E, Fahrleitner-Pammer A, Pilz S. Marinobufagenin in essential hypertension and primary aldosteronism: a cardiotonic steroid with clinical and diagnostic implications. Clin Exp Hypertens. 2015;37(2):108–15.
Yue Y, Meng K, Pu Y, Zhang X. Transforming growth factor beta (TGF-β) mediates cardiac fibrosis and induces diabetic cardiomyopathy. Diabetes Res Clin Pract. 2017;133:124–30.
Bonakdaran S, Nejad AF, Abdol-Reza V, Hatefi A, Shakeri M. Impact of oral 1,25-dihydroxy vitamin D (calcitriol) replacement therapy on coronary artery risk factors in type 2 diabetic patients. Endocr Metab Immune Disord Drug Targets. 2013;13(4):295–300.
Charytan DM, Fishbane S, Malyszko J, McCullough PA, Goldsmith D. Cardiorenal syndrome and the role of the bone-mineral axis and anemia. Am J Kidney Dis. 2015;66:196–205.
Nigwekar SU, Thadhani R, Brandenburg VM. Calciphylaxis. N Engl J Med. 2018;378(18):1704–14.
Mihai S, Codrici E, Popescu ID, Enciu AM, Albulescu L, Necula LG, Mambet C, Anton G, Tanase C. Inflammation-related mechanisms in chronic kidney disease prediction, progression, and outcome. J Immunol Res. 2018;2018:2180373.
Wada J, Makino H. Inflammation and the pathogenesis of diabetic nephropathy. Clin Sci (Lond). 2013;124:139–52.
Feingold KR, Grunfeld C. Effect of inflammation on HDL structure and function. Curr Opin Lipidol. 2016;27:521–30.
Edmonston DL, Pun PH. Coronary artery disease in chronic kidney disease: highlights for a Kidney Disease Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2020;97:642–4.
Warnock DG, Delanaye P, Glassock RJ. Risks for all-cause mortality: stratified by age, estimated glomerular filtration rate and albuminuria. Nephron. 2017;136(4):292–7.
Malmgren L, McGuigan FE, Berglundh S, Westman K, Christensson A, Åkesson K. Declining estimated glomerular filtration rate and its association with mortality and comorbidity over 10 years in elderly women. Nephron. 2015;130:245–55.
Brantsma AH, Bakker SJ, Hillege HL, de Zeeuw D, de Jong PE, Gansevoort RT, PREVEND Study Group. Cardiovascular and renal outcome in subjects with K/DOQI stage 1-3 chronic kidney disease: the importance of urinary albumin excretion. Nephrol Dial Transplant. 2008;23:3851–8.
Diercks GF, van Boven AJ, Hillege JL, de Jong PE, Rouleau JL, van Gilst WH. The importance of microalbuminuria as a cardiovascular risk indicator: a review. Can J Cardiol. 2002;18(5):525–35.
Nerpin E, Ingelsson E, Risérus U, Sundström J, Larsson A, Jobs E, Jobs M, Hallan S, Zethelius B, Berglund L, Basu S, Arnlöv J. The combined contribution of albuminuria and glomerular filtration rate to the prediction of cardiovascular mortality in elderly men. Nephrol Dial Transplant. 2011;26(9):2820–7.
Rule AD, Lieske JC. Cystatin C is more than GFR, and this may be a good thing. J Am Soc Nephrol. 2011;22:795–7.
Turin TC, Jun M, James MT, Tonelli M, Coresh J, Manns BJ, Hemmelgarn BR. Magnitude of rate of change in kidney function and future risk of cardiovascular events. Int J Cardiol. 2016;202:657–65.
Clase CM, Gao P, Tobe SW, McQueen MJ, Grosshennig A, Teo KK, Yusuf S, Mann JF, ONTARGET (ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial) and TRANSCEND (Telmisartan Randomized Assessment Study in Angiotensin-Converting-Enzyme-Inhibitor Intolerant Subjects with Cardiovascular Disease). Estimated glomerular filtration rate and albuminuria as predictors of outcomes in patients with high cardiovascular risk: a cohort study. Ann Intern Med. 2011;154:310–8.
Hallan SI, Matsushita K, Sang Y, Mahmoodi BK, Black C, Ishani A, Kleefstra N, Naimark D, Roderick P, Tonelli M, Wetzels JF, Astor BC, Gansevoort RT, Levin A, Wen CP, Coresh J, Chronic Kidney Disease Prognosis Consortium. Age and association of kidney measures with mortality and end-stage renal disease. JAMA. 2012;308(22):2349–60.
Di Angelantonio E, Chowdhury R, Sarwar N, Aspelund T, Danesh J, Gudnason V. Chronic kidney disease and risk of major cardiovascular disease and non-vascular mortality: prospective population based cohort study. BMJ. 2010;341:c4986.
van Staa TP, Gulliford M, Ng ES, Goldacre B, Smeeth L. Prediction of cardiovascular risk using Framingham, ASSIGN and QRISK2: how well do they predict individual rather than population risk? PLoS One. 2014;9(10):e106455.
Melsom T, Fuskevåg OM, Mathisen UD, Strand H, Schei J, Jenssen T, Solbu M, Eriksen BO. Estimated GFR is biased by non-traditional cardiovascular risk factors. Am J Nephrol. 2015;41(1):7–15.
Shah DS, Polkinghorne KR, Pellicano R, Kerr PG. Are traditional risk factors valid for assessing cardiovascular risk in end-stage renal failure patients? Nephrology (Carlton). 2008;13(8):667–71.
Balla S, Nusair MB, Alpert MA. Risk factors for atherosclerosis in patients with chronic kidney disease: recognition and management. Curr Opin Pharmacol. 2013;13(2):192–9.
Inrig JK, Gillespie BS, Patel UD, Briley LP, She L, Easton JD, Topol E, Szczech LA. Risk for cardiovascular outcomes among subjects with atherosclerotic cardiovascular disease and greater-than-normal estimated glomerular filtration rate. Clin J Am Soc Nephrol. 2007;2:1215–22.
Matsushita K, Sang Y, Ballew SH, Astor BC, Hoogeveen RC, Solomon SD, Ballantyne CM, Woodward M, Coresh J. Cardiac and kidney markers for cardiovascular prediction in individuals with chronic kidney disease: the Atherosclerosis Risk in Communities study. Arterioscler Thromb Vasc Biol. 2014;34:1770–7.
Chen J, Budoff MJ, Reilly MP, Yang W, Rosas SE, Rahman M, Zhang X, Roy JA, Lustigova E, Nessel L, Ford V, Raj D, Porter AC, Soliman EZ, Wright JT Jr, Wolf M, He J, CRIC Investigators. Coronary artery calcification and risk of cardiovascular disease and death among patients with chronic kidney disease. JAMA Cardiol. 2017;2:635–43.
Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, Wang Y, Chung J, Emerick A, Greaser L, Elashoff RM, Salusky IB. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med. 2000;342:1478–83.
Cano-Megías M, Guisado-Vasco P, Bouarich H, de Arriba-de la Fuente G, de Sequera-Ortiz P, Álvarez-Sanz C, Rodríguez-Puyol D. Coronary calcification as a predictor of cardiovascular mortality in advanced chronic kidney disease: a prospective long-term follow-up study. BMC Nephrol. 2019;20:188.
Glassock RJ, Pecoits-Filho R, Barberato SH. Left ventricular mass in chronic kidney disease and ESRD. Clin J Am Soc Nephrol. 2009;4 Suppl 1:S79–91.
Tripepi G, D’Arrigo G, Mallamaci F, London G, Tangri N, Hsu JY, Feldman H, Zoccali C. Nephrol dial transplant. Prognostic values of left ventricular mass index in chronic kidney disease patients. 2019. [Epub ahead of print].
Kalantar-Zadeh K, Fouque D. Nutritional management of chronic kidney disease. N Engl J Med. 2017;377:1765–76.
Qian F, Riddle MC, Wylie-Rosett J, Hu FB. Red and processed meats and health risks: how strong is the evidence? Diabetes Care. 2020;43:265–71.
Tantisattamo E, Dafoe DC, Reddy UG, Ichii H, Rhee CM, Streja E, Landman J, Kalantar-Zadeh K. Current management of patients with acquired solitary kidney. Kidney Int Rep. 2019;4(9):1205–18.
Kamper AL, Strandgaard S. Long-term effects of high-protein diets on renal function. Annu Rev Nutr. 2017;37:347–69.
Wakasugi M, Kazama JJ, Yamamoto S, Kawamura K, Narita I. A combination of healthy lifestyle factors is associated with a decreased incidence of chronic kidney disease: a population-based cohort study. Hypertens Res. 2013;36(4):328–33.
Chang AR, Lóser M, Malhotra R, Appel LJ. Blood pressure goals in patients with CKD: a review of evidence and guidelines. Clin J Am Soc Nephrol. 2019;14(1):161–9.
Briasoulis A, Bakris GL. The OSCAR for cardiovascular disease prevention in chronic kidney disease goes to blood pressure control. Kidney Int. 2013;83(1):20–2.
SPRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, Reboussin DM, Rahman M, Oparil S, Lewis CE, Kimmel PL, Johnson KC, Goff DC Jr, Fine LJ, Cutler JA, Cushman WC, Cheung AK, Ambrosius WT. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103–16.
Chang TI, Lim H, Park CH, Rhee CM, Moradi H, Kalantar-Zadeh K, Kang EW, Kang SW, Han SH. Associations of systolic blood pressure with incident CKD G3-G5: a Cohort Study of South Korean adults. Am J Kidney Dis. 2020;15. [EPub ahead of print].
Guerrot D, Humalda JK. Blood pressure targets in chronic kidney disease: an update on the evidence. Curr Opin Nephrol Hypertens. 2020;29(3):327–32.
Chiang HP, Chiu YW, Lee JJ, Hung CC, Hwang SJ, Chen HC. Blood pressure modifies outcomes in patients with stage 3 to 5 chronic kidney disease. Kidney Int. 2020;97(2):402–13.
Covic A, Apetrii M, Goldsmith D, Kanbay M. SPRINT: the study nephrologists might take with a grain of salt. J Clin Hypertens (Greenwich). 2016;18(11):1185–8.
Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S, RENAAL Study Investigators. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345:861–9.
Ruggenenti P, Perna A, Loriga G, Ganeva M, Ene-Iordache B, Turturro M, Lesti M, Perticucci E, Chakarski IN, Leonardis D, Garini G, Sessa A, Basile C, Alpa M, Scanziani R, Sorba G, Zoccali C, Remuzzi G, REIN-2 Study Group. Blood-pressure control for renoprotection in patients with non-diabetic chronic renal disease (REIN-2): multicentre, randomised controlled trial. Lancet. 2005;365(9463):939–46.
Ameh OI, Ekrikpo UE, Kengne AP. Preventing CKD in low- and middle-income countries: a call for urgent action. Kidney Int Rep. 2020;5:255–62.
Luyckx VA, Cherney DZI, Bello AK. Preventing CKD in developed countries. Kidney Int Rep. 2020;5:263–77.
Blum MF, Surapaneni A, Stewart JD, Liao D, Yanosky JD, Whitsel EA, Power MC, Grams ME. Particulate matter and albuminuria, glomerular filtration rate, and incident CKD. Clin J Am Soc Nephrol. 2020;15:311–9.
Ferenbach DA, Bonventre JV. Mechanisms of maladaptive repair after AKI leading to accelerated kidney ageing and CKD. Nat Rev Nephrol. 2015;11:264–76.
Glassock RJ, Winearls C. Screening for CKD with eGFR: doubts and dangers. Clin J Am Soc Nephrol. 2008;3:1563–8.
Fink HA, Ishani A, Taylor BC, Greer NL, MacDonald R, Rossini D, Sadiq S, Lankireddy S, Kane RL, Wilt TJ. Screening for, monitoring, and treatment of chronic kidney disease stages 1 to 3: a systematic review for the U.S. Preventive Services Task Force and for an American College of Physicians Clinical Practice Guideline. Ann Intern Med. 2012;156:570–81.
Moyer VA, U.S. Preventive Services Task Force. Screening for chronic kidney disease: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157:567–70.
Katsiki N, Banach M, Mikhailidis DP. Is type 2 diabetes mellitus a coronary heart disease equivalent or not? Do not just enjoy the debate and forget the patient! Arch Med Sci. 2019;15:1357–64.
Polonsky TS, Bakris GL. Chronic kidney disease: a coronary heart disease equivalent? Lancet. 2012;380:783–5.
Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, Ritz E, Atkins RC, Rohde R, Raz I, Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851–60.
Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J Med. 1993;329:1456–62.
Bakris GL, Sarafidis PA, Weir MR, Dahlöf B, Pitt B, Jamerson K, Velazquez EJ, Staikos-Byrne L, Kelly RY, Shi V, Chiang YT, Weber MA, ACCOMPLISH Trial Investigators. Renal outcomes with different fixed-dose combination therapies in patients with hypertension at high risk for cardiovascular events (ACCOMPLISH): a prespecified secondary analysis of a randomised controlled trial. Lancet. 2010;375:1173–8.
Jamerson K, Weber MA, Bakris GL, Dahlöf B, Pitt B, Shi V, Hester A, Gupte J, Gatlin M, Velazquez EJ, ACCOMPLISH Trial Investigators. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N Engl J Med. 2008;359:2417–28.
Parving HH, Brenner BM, McMurray JJ, de Zeeuw D, Haffner SM, Solomon SD, Chaturvedi N, Persson F, Desai AS, Nicolaides M, Richard A, Xiang Z, Brunel P, Pfeffer MA, ALTITUDE Investigators. Cardiorenal end points in a trial of aliskiren for type 2 diabetes. N Engl J Med. 2012;367:2204–13.
Meaney CJ, Beccari MV, Yang Y, Zhao J. Systematic review and meta-analysis of patiromer and sodium zirconium cyclosilicate: a new armamentarium for the treatment of hyperkalemia. Pharmacotherapy. 2017;37:401–11.
Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP, Maggioni AP, Martinez F, Packer M, Pfeffer MA, Pieske B, Redfield MM, Rouleau JL, van Veldhuisen DJ, Zannad F, Zile MR, Desai AS, Claggett B, Jhund PS, Boytsov SA, Comin-Colet J, Cleland J, Düngen HD, Goncalvesova E, Katova T, Kerr Saraiva JF, Lelonek M, Merkely B, Senni M, Shah SJ, Zhou J, Rizkala AR, Gong J, Shi VC, Lefkowitz MP, PARAGON-HF Investigators and Committees. Angiotensin-neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med. 2019;381:1609–20.
McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, Rouleau JL, Shi VC, Solomon SD, Swedberg K, Zile MR, PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371:993–1004.
Haynes R, Judge PK, Staplin N, Herrington WG, Storey BC, Bethel A, Bowman L, Brunskill N, Cockwell P, Hill M, Kalra PA, McMurray JJV, Taal M, Wheeler DC, Landray MJ, Baigent C. Effects of sacubitril/valsartan versus irbesartan in patients with chronic kidney disease. Circulation. 2018;138:1505–14.
Aggarwal R, Steinkamp J, Chiu N, Petrie B, Mirzan H. Intensive blood pressure targets for diabetic and other high-risk populations: a pooled individual patient data analysis. Hypertension. 2018;71:833–9.
Whelton PK, et al. ACC/AHA guidelines for prevention, detection, evaluation, management of high blood pressure in adults. Circulation. 2018;138:e489–594.
Kotecha D, Gill SK, Flather MD, Holmes J, Packer M, Rosano G, Böhm M, McMurray JJV, Wikstrand J, Anker SD, van Veldhuisen DJ, Manzano L, von Lueder TG, Rigby AS, Andersson B, Kjekshus J, Wedel H, Ruschitzka F, Cleland JGF, Damman K, Redon J, Coats AJS, Beta-Blockers in Heart Failure Collaborative Group. Impact of renal impairment on beta-blocker efficacy in patients with heart failure. J Am Coll Cardiol. 2019;74:2893–904.
Vogt L, Bangalore S, Fayyad R, Melamed S, Hovingh GK, DeMicco DA, Waters DD. Atorvastatin has a dose-dependent beneficial effect on kidney function and associated cardiovascular outcomes: post hoc analysis of 6 double-blind randomized controlled trials. J Am Heart Assoc. 2019;8(9):e010827.
Michos ED, McEvoy JW, Blumenthal RS. Lipid management for the prevention of atherosclerotic cardiovascular disease. N Engl J Med. 2019;381:1557–67.
Katsiki N, Mikhailidis DP, Banach M. Lipid-lowering agents for concurrent cardiovascular and chronic kidney disease. Expert Opin Pharmacother. 2019;20:2007–17.
Moradi H, Streja E, Vaziri ND. ESRD-induced dyslipidemia-Should management of lipid disorders differ in dialysis patients? Semin Dial. 2018;31(4):398–405.
Wanner C, Krane V, März W, Olschewski M, Mann JF, Ruf G, Ritz E, German Diabetes and Dialysis Study Investigators. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N Engl J Med. 2005;353:238–48.
Fellström BC, Jardine AG, Schmieder RE, Holdaas H, Bannister K, Beutler J, Chae DW, Chevaile A, Cobbe SM, Grönhagen-Riska C, De Lima JJ, Lins R, Mayer G, McMahon AW, Parving HH, Remuzzi G, Samuelsson O, Sonkodi S, Sci D, Süleymanlar G, Tsakiris D, Tesar V, Todorov V, Wiecek A, Wüthrich RP, Gottlow M, Johnsson E, Zannad F, AURORA Study Group. Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N Engl J Med. 2009;360:1395–407.
Giugliano RP, Wiviott SD, Blazing MA, De Ferrari GM, Park JG, Murphy SA, White JA, Tershakovec AM, Cannon CP, Braunwald E. Long-term safety and efficacy of achieving very low levels of low-density lipoprotein cholesterol: a prespecified analysis of the IMPROVE-IT trial. JAMA Cardiol. 2017;2:547–55.
Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, Levin A, Agodoa L, Gaziano M, Kasiske B, Walker R, Massy ZA, Feldt-Rasmussen B, Krairittichai U, Ophascharoensuk V, Fellström B, Holdaas H, Tesar V, Wiecek A, Grobbee D, de Zeeuw D, Grönhagen-Riska C, Dasgupta T, Lewis D, Herrington W, Mafham M, Majoni W, Wallendszus K, Grimm R, Pedersen T, Tobert J, Armitage J, Baxter A, Bray C, Chen Y, Chen Z, Hill M, Knott C, Parish S, Simpson D, Sleight P, Young A, Collins R, SHARP Investigators. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet. 2011;377:2181–92.
Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella-Tommasino J, Forman DE, Goldberg R, Heidenreich PA, Hlatky MA, Jones DW, Lloyd-Jones D, Lopez-Pajares N, Ndumele CE, Orringer CE, Peralta CA, Saseen JJ, Smith SC Jr, Sperling L, Virani SS, Yeboah J. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139:e1082–143.
Giugliano RP, Pedersen TR, Park JG, De Ferrari GM, Gaciong ZA, Ceska R, Toth K, Gouni-Berthold I, Lopez-Miranda J, Schiele F, Mach F, Ott BR, Kanevsky E, Pineda AL, Somaratne R, Wasserman SM, Keech AC, Sever PS, Sabatine MS, FOURIER Investigators. Clinical efficacy and safety of achieving very low LDL-cholesterol concentrations with the PCSK9 inhibitor evolocumab: a prespecified secondary analysis of the FOURIER trial. Lancet. 2017;390:1962–71.
Elewa U, Fernández-Fernández B, Mahillo-Fernández I, Martin-Cleary C, Sanz AB, Sanchez-Niño MD, Ortiz A. PCSK9 in diabetic kidney disease. Eur J Clin Investig. 2016;46:779–86.
Jukema JW, Zijlstra LE, Bhatt DL, Bittner VA, Diaz R, Drexel H, Goodman SG, Kim YU, Pordy R, Reiner Ž, Roe MT, Tse HF, Montenegro Valdovinos PC, White HD, Zeiher AM, Szarek M, Schwartz GG, Steg PG, ODYSSEY OUTCOMES Investigators. Effect of alirocumab on stroke in ODYSSEY OUTCOMES. Circulation. 2019;140:2054–62.
Bhatt DL, Miller M, Brinton EA, Jacobson TA, Steg PG, Ketchum SB, Doyle RT Jr, Juliano RA, Jiao L, Granowitz C, Tardif JC, Olshansky B, Chung MK, Gibson CM, Giugliano RP, Budoff MJ, Ballantyne CM, REDUCE-IT Investigators. REDUCE-IT USA: results from the 3146 patients randomized in the United States. Circulation. 2020;141:367–75.
Charytan DM, Sabatine MS, Pedersen TR, Im K, Park JG, Pineda AL, Wasserman SM, Deedwania P, Olsson AG, Sever PS, Keech AC, Giugliano RP, FOURIER Steering Committee and Investigators. Efficacy and safety of evolocumab in chronic kidney disease in the FOURIER trial. J Am Coll Cardiol. 2019;73:2961–70.
Davis TM, Ting R, Best JD, Donoghoe MW, Drury PL, Sullivan DR, Jenkins AJ, O’Connell RL, Whiting MJ, Glasziou PP, Simes RJ, Kesäniemi YA, Gebski VJ, Scott RS, Keech AC, Fenofibrate Intervention and Event Lowering in Diabetes Study investigators. Effects of fenofibrate on renal function in patients with type 2 diabetes mellitus: the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) Study. Diabetologia. 2011;54(2):280–90.
Keech A, Simes RJ, Barter P, Best J, Scott R, Taskinen MR, Forder P, Pillai A, Davis T, Glasziou P, Drury P, Kesäniemi YA, Sullivan D, Hunt D, Colman P, d’Emden M, Whiting M, Ehnholm C, Laakso M, FIELD study investigators. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005;366:1849–61.
Arnott C, Li Q, Kang A, Neuen BL, Bompoint S, Lam CSP, Rodgers A, Mahaffey KW, Cannon CP, Perkovic V, Jardine MJ, Neal B. Sodium-glucose cotransporter 2 inhibition for the prevention of cardiovascular events in patients with Type 2 diabetes mellitus: a systematic review and meta-analysis. J Am Heart Assoc. 2020;9:e014908.
Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, Edwards R, Agarwal R, Bakris G, Bull S, Cannon CP, Capuano G, Chu PL, de Zeeuw D, Greene T, Levin A, Pollock C, Wheeler DC, Yavin Y, Zhang H, Zinman B, Meininger G, Brenner BM, Mahaffey KW, CREDENCE Trial Investigators. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–306.
Heerspink HJL. Sodium glucose co-transporter 2 inhibition: a new avenue to protect the kidney. Nephrol Dial Transplant. 2019;34(12):2015–7.
Lam CSP, Chandramouli C, Ahooja V, Verma S. SGLT-2 inhibitors in heart failure: current management, unmet needs, and therapeutic prospects. J Am Heart Assoc. 2019;8:e013389.
Dekkers CCJ, Gansevoort RT. Sodium-glucose cotransporter 2 inhibitors: extending the indication to non-diabetic kidney disease? Nephrol Dial Transplant. 2020;35(Supplement_1):i33–42.
Tsimihodimos V, Filippatos TD, Elisaf MS. SGLT2 inhibitors and the kidney: effects and mechanisms. Diabetes Metab Syndr. 2018;12:1117–23.
Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Furtado RHM, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Sabatine MS. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393:31–9.
Verma S, McMurray JJV. SGLT2 inhibitors and mechanisms of cardiovascular benefit: a state-of-the-art review. Diabetologia. 2018;61:2108–17.
Heerspink HJL, Stefansson BV, Chertow GM, Correa-Rotter R, Greene T, Hou FF, Lindberg M, McMurray J, Rossing P, Toto R, Langkilde AM, Wheeler DC, DAPA-CKD Investigators. Rationale and protocol of the Dapagliflozin And Prevention of Adverse outcomes in Chronic Kidney Disease (DAPA-CKD) randomized controlled trial. Nephrol Dial Transplant. 2020;35(2):274–82.
AstraZeneca Press Release 30 March, 2020. www.astrazeneca.com/media-central/press-release/2020/farxiga-phase-iii-dapa-ckd-trial-will-be stopped-early. Accessed 30 Mar 2020.
Prattichizzo F, De Nigris V, Micheloni S, La Sala L, Ceriello A. Increases in circulating levels of ketone bodies and cardiovascular protection with SGLT2 inhibitors: is low-grade inflammation the neglected component? Diabetes Obes Metab. 2018;20(11):2515–22.
Petrie MC, Verma S, Docherty KF, Inzucchi SE, Anand I, Belohlávek J, Böhm M, Chiang CE, Chopra VK, de Boer RA, Desai AS, Diez M, Drozdz J, Dukát A, Ge J, Howlett J, Katova T, Kitakaze M, Ljungman CEA, Merkely B, Nicolau JC, O’Meara E, Vinh PN, Schou M, Tereshchenko S, Køber L, Kosiborod MN, Langkilde AM, Martinez FA, Ponikowski P, Sabatine MS, Sjöstrand M, Solomon SD, Johanson P, Greasley PJ, Boulton D, Bengtsson O, Jhund PS, McMurray JJV. Effect of dapagliflozin on worsening heart failure and cardiovascular death in patients with heart failure with and without diabetes. JAMA. 2020;323(14):1353–68.
Eickhoff MK, Dekkers CCJ, Kramers BJ, Laverman GD, Frimodt-Møller M, Jørgensen NR, Faber J, Danser AHJ, Gansevoort RT, Rossing P, Persson F, Heerspink HJL. Effects of dapagliflozin on volume status when added to renin-angiotensin system inhibitors. Clin Med. 2019;8(6). pii: E779.
House AA, Wanner C, Sarnak MJ, Piña IL, McIntyre CW, Komenda P, Kasiske BL, Deswal A, deFilippi CR, Cleland JGF, Anker SD, Herzog CA, Cheung M, Wheeler DC, Winkelmayer WC, McCullough PA; Conference Participants. Heart failure in chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019;95:1304–17.
Giugliano D, Maiorino MI, Bellastella G, Chiodini P, Esposito K. Glycemic control, preexisting cardiovascular disease, and risk of major cardiovascular events in patients with type 2 diabetes mellitus: systematic review with meta-analysis of cardiovascular outcome trials and intensive glucose control trials. J Am Heart Assoc. 2019;8:e012356.
KDIGO Clinical practice guidelines on diabetes management in chronic kidney disease. (In press, 2020).
Tuttle KR, Bakris GL, Bilous RW, Chiang JL, de Boer IH, Goldstein-Fuchs J, Hirsch IB, Kalantar-Zadeh K, Narva AS, Navaneethan SD, Neumiller JJ, Patel UD, Ratner RE, Whaley-Connell AT, Molitch ME. Diabetic kidney disease: a report from an ADA Consensus Conference. Diabetes Care. 2014;37:2864–83.
Mann JFE, Fonseca VA, Poulter NR, Raz I, Idorn T, Rasmussen S, von Scholten BJ, Mosenzon O, LEADER Trial Investigators. Safety of liraglutide in type 2 diabetes and chronic kidney disease. Clin J Am Soc Nephrol. 2020;15(4):465–73.
Cherney DZ, Tuttle KR. Liraglutide for the treatment of type 2 diabetes and safety in diabetic kidney disease: liraglutide and diabetic kidney disease. Clin J Am Soc Nephrol. 2020;15(4):444–6.
Marso SP, Baeres FMM, Bain SC, Goldman B, Husain M, Nauck MA, Poulter NR, Pratley RE, Thomsen AB, Buse JB, LEADER Trial Investigators. Effects of liraglutide on cardiovascular outcomes in patients with diabetes with or without heart failure. J Am Coll Cardiol. 2020;75:1128–41.
Li J, Albajrami O, Zhuo M, Hawley CF, Paik JM. Decision algorithm for prescribing SGLT2 inhibitors and GLP-1 receptor agonists for diabetic kidney disease. Clin J Am Soc Nephrol. 2020 June 9- [ePUB ahead of print].
The ACCORD Study Group. Long-term effects of intensive glucose lowering on cardiovascular outcomes. N Engl J Med. 2011;364:818–28.
Papademetriou V, Lovato L, Doumas M, Nylen E, Mottl A, Cohen RM, Applegate WB, Puntakee Z, Yale JF, Cushman WC, ACCORD Study Group. Chronic kidney disease and intensive glycemic control increase cardiovascular risk in patients with type 2 diabetes. Kidney Int. 2015;87:649–59.
Panduru NM, Nistor I, Groop PH, Van Biesen W, Farrington K, Covic A. Considerations on glycaemic control in older and/or frail individuals with diabetes and advanced kidney disease. Nephrol Dial Transplant. 2017;32:591–7.
Reaven PD, Emanuele NV, Wiitala WL, Bahn GD, Reda DJ, McCarren M, Duckworth WC, Hayward RA, VADT Investigators. Intensive glucose control in patients with type 2 diabetes - 15-year follow-up. N Engl J Med. 2019;380:2215–24.
Agrawal L, Azad N, Bahn GD, Ge L, Reaven PD, Hayward RA, Reda DJ, Emanuele NV, VADT Study Group. Long-term follow-up of intensive glycaemic control on renal outcomes in the Veterans Affairs Diabetes Trial (VADT). Diabetologia. 2018;61(2):295–9.
Stafylas PC, Sarafidis PA, Lasaridis AN. The controversial effects of thiazolidinediones on cardiovascular morbidity and mortality. Int J Cardiol. 2009;24(131):298–304.
de Jong M, van der Worp HB, van der Graaf Y, Visseren FLJ, Westerink J. Pioglitazone and the secondary prevention of cardiovascular disease. A meta-analysis of randomized-controlled trials. Cardiovasc Diabetol. 2017;16:134.
Zhou Y, Huang Y, Ji X, Wang X, Shen L, Wang Y. Pioglitazone for the primary and secondary prevention of cardiovascular and renal outcomes in patients with or at high risk of type 2 diabetes mellitus: a meta-analysis. J Clin Endocrinol Metab. 2020;105(5):dgz252.
Sinha AD, Agarwal R. Thiazide diuretics in chronic kidney disease. Curr Hypertens Rep. 2015;17:13.
Bramlage P, Swift SL, Thoenes M, Minguet J, Ferrero C, Schmieder RE. Non-steroidal mineralocorticoid receptor antagonism for the treatment of cardiovascular and renal disease. Eur J Heart Fail. 2016;18:28–37.
Dhaybi OA, Bakris G. Mineralocorticoid antagonists in chronic kidney disease. Curr Opin Nephrol Hypertens. 2017;26(1):50–5.
Agarwal A, Cheung AK. Mineralocorticoid receptor antagonists in ESKD. Clin J Am Soc Nephrol. 2020;15(7):1047–9.
Ko GJ, Kalantar-Zadeh K, Goldstein-Fuchs J, Rhee CM. Dietary approaches in the management of diabetic patients with kidney disease. Nutrients. 2017;9: Pii. E824.
Kramer H. Diet and chronic kidney disease. Adv Nutr. 2019;10(Suppl_4):S367–79.
Turner-McGrievy G, Mandes T, Crimarco A. A plant-based diet for overweight and obesity prevention and treatment. J Geriatr Cardiol. 2017;14:369–74.
Kim H, Caulfield LE, Garcia-Larsen V, Steffen LM, Grams ME, Coresh J, Rebholz CM. Plant-based diets and incident CKD and kidney function. Clin J Am Soc Nephrol. 2019;14:682–91.
Kim H, Caulfield LE, Garcia-Larsen V, Steffen LM, Coresh J, Rebholz CM. Plant-based diets are associated with a lower risk of incident cardiovascular disease, cardiovascular disease mortality, and all-cause mortality in a general population of middle-aged adults. J Am Heart Assoc. 2019;8:e012865.
Jia L, Jia Q, Yang J, Jia R, Zhang H. Efficacy of probiotics supplementation on chronic kidney disease: a systematic review and meta-analysis. Kidney Blood Press Res. 2018;43:1623–35.
Mc Causland FR, Claggett B, Burdmann EA, Chertow GM, Cooper ME, Eckardt KU, Ivanovich P, Levey AS, Lewis EF, McGill JB, McMurray JJV, Parfrey P, Parving HH, Remuzzi G, Singh AK, Solomon SD, Toto RD, Pfeffer MA. Treatment of anemia with darbepoetin prior to dialysis initiation and clinical outcomes: analyses from the Trial to Reduce Cardiovascular Events With Aranesp Therapy (TREAT). Am J Kidney Dis. 2019;73:309–15.
Chen CL, Chen NC, Wu FZ, Wu MT. Impact of denosumab on cardiovascular calcification in patients with secondary hyperparathyroidism undergoing dialysis: a pilot study. Osteoporos Int. 2020;31(8):1507–16.
Block GA, Wheeler DC, Persky MS, Kestenbaum B, Ketteler M, Spiegel DM, Allison MA, Asplin J, Smits G, Hoofnagle AN, Kooienga L, Thadhani R, Mannstadt M, Wolf M, Chertow GM. Effects of phosphate binders in moderate CKD. J Am Soc Nephrol. 2012;23:1407–15.
EVOLVE Trial Investigators, Chertow GM, Block GA, Correa-Rotter R, Drüeke TB, Floege J, Goodman WG, Herzog CA, Kubo Y, London GM, Mahaffey KW, Mix TC, Moe SM, Trotman ML, Wheeler DC, Parfrey PS. Effect of cinacalcet on cardiovascular disease in patients undergoing dialysis. N Engl J Med. 2012;367(26):2482–94.
Su X, Yan B, Wang L, Lv J, Cheng H, Chen Y. Effect of antiplatelet therapy on cardiovascular and kidney outcomes in patients with chronic kidney disease: a systematic review and meta-analysis. BMC Nephrol. 2019;20:309.
Kim AJ, Lim HJ, Ro H, Ko KP, Han SY, Chang JH, Lee HH, Chung W, Jung JY. Low-dose aspirin for prevention of cardiovascular disease in patients with chronic kidney disease. PLoS One. 2014;9:e104179.
Stamellou E, Floege J. Novel oral anticoagulants in patients with chronic kidney disease and atrial fibrillation. Nephrol Dial Transplant. 2018;33:1683–9.
Krüger T, Floege J. Vitamin K antagonists: beyond bleeding. Semin Dial. 2014;27:37–41.
Glassock RJ. Anticoagulant-related nephropathy: it’s the real McCoy. Clin J Am Soc Nephrol. 2019;14:935–7.
Randhawa MS, Vishwanath R, Rai MP, Wang L, Randhawa AK, Abela G, Dhar G. Association between use of warfarin for atrial fibrillation and outcomes among patients with end-stage renal disease: a systematic review and meta-analysis. JAMA Netw Open. 2020;3:e202175.
Stanifer JW, Pokorney SD, Chertow GM, Hohnloser SH, Wojdyla DM, Garonzik S, Byon W, Hijazi Z, Lopes RD, Alexander JH, Wallentin L, Granger CB. Apixaban versus warfarin in patients with atrial fibrillation and advanced chronic kidney disease. Circulation. 2020;141(17):1384–92.
Sato Y, Feig DI, Stack AG, Kang DH, Lanaspa MA, Ejaz AA, Sánchez-Lozada LG, Kuwabara M, Borghi C, Johnson RJ. The case for uric acid-lowering treatment in patients with hyperuricaemia and CKD. Nat Rev Nephrol. 2019;15:767–75.
Maloberti A, Giannattasio C, Bombelli M, Desideri G, Cicero AFG, Muiesan ML, Rosei EA, Salvetti M, Ungar A, Rivasi G, Pontremoli R, Viazzi F, Facchetti R, Ferri C, Bernardino B, Galletti F, D’Elia L, Palatini P, Casiglia E, Tikhonoff V, Barbagallo CM, Verdecchia P, Masi S, Mallamaci F, Cirillo M, Rattazzi M, Pauletto P, Cirillo P, Gesualdo L, Mazza A, Volpe M, Tocci G, Iaccarino G, Nazzaro P, Lippa L, Parati G, Dell’Oro R, Quarti-Trevano F, Grassi G, Virdis A, Borghi C, Working Group on Uric Acid and Cardiovascular Risk of the Italian Society of Hypertension (SIIA). Hyperuricemia and risk of cardiovascular outcomes: the experience of the URRAH (Uric Acid Right for Heart Health) project. High Blood Press Cardiovasc Prev. 2020;27(2):121–8.
Casiglia E, Tikhonoff V, Virdis A, Masi S, Barbagallo CM, Bombelli M, Bruno B, Cicero AFG, Cirillo M, Cirillo P, Desideri G, D’Elia L, Ferri C, Galletti F, Gesualdo L, Giannattasio C, Iaccarino G, Lippa L, Mallamaci F, Maloberti A, Mazza A, Muiesan ML, Nazzaro P, Palatini P, Parati G, Pontremoli R, Quarti-Trevano F, Rattazzi M, Rivasi G, Salvetti M, Tocci G, Ungar A, Verdecchia P, Viazzi F, Volpe M, Grassi G, Borghi C, Working Group on Uric Acid and Cardiovascular Risk of the Italian Society of Hypertension (SIIA). Serum uric acid and fatal myocardial infarction: detection of prognostic cut-off values: the URRAH (Uric Acid Right for Heart Health) study. J Hypertens. 2020;38:412–9.
Steiger S, Ma Q, Anders HJ. The case for evidence-based medicine for the association between hyperuricaemia and CKD. Nat Rev Nephrol. 2020;16(7):422.
Su CY, Shen LJ, Hsieh S, Lin LY, Lin FJ. Comparing cardiovascular safety of febuxostat and allopurinol in the real world: a population-based cohort study. Mayo Clin Proc. 2019;94:1147–57.
Kojima S, Matsui K, Hiramitsu S, Hisatome I, Waki M, Uchiyama K, Yokota N, Tokutake E, Wakasa Y, Jinnouchi H, Kakuda H, Hayashi T, Kawai N, Mori H, Sugawara M, Ohya Y, Kimura K, Saito Y, Ogawa H. Febuxostat for cerebral and CaRdiorenovascular Events PrEvEntion StuDy. Eur Heart J. 2019;40:1778–86.
Spertus JA, Jones PG, Maron DJ, O’Brien SM, Reynolds HR, Rosenberg Y, Stone GW, Harrell FE Jr, Boden WE, Weintraub WS, Baloch K, Mavromatis K, Diaz A, Gosselin G, Newman JD, Mavromichalis S, Alexander KP, Cohen DJ, Bangalore S, Hochman JS, Mark DB, ISCHEMIA Research Group. Health-status outcomes with invasive or conservative care in coronary disease. N Engl J Med. 2020;382(15):1408–19. https://doi.org/10.1056/NEJMoa1916370.
Bangalore S, Maron DJ, O’Brien SM, Fleg JL, Kretov EI, Briguori C, Kaul U, Reynolds HR, Mazurek T, Sidhu MS, Berger JS, Mathew RO, Bockeria O, Broderick S, Pracon R, Herzog CA, Huang Z, Stone GW, Boden WE, Newman JD, Ali ZA, Mark DB, Spertus JA, Alexander KP, Chaitman BR, Chertow GM, Hochman JS, ISCHEMIA-CKD Research Group. Management of coronary disease in patients with advanced kidney disease. N Engl J Med. 2020;382(17):1608–18.
Turakhia MP, Blankestijn PJ, Carrero JJ, Clase CM, Deo R, Herzog CA, Kasner SE, Passman RS, Pecoits-Filho R, Reinecke H, Shroff GR, Zareba W, Cheung M, Wheeler DC, Winkelmayer WC, Wanner C, Conference Participants. Chronic kidney disease and arrhythmias: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Eur Heart J. 2018;39:2314–25.
KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:5–14.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Lo, R.H., Glassock, R.J. (2021). Prevention of Cardiovascular Disease in Patients with Chronic Kidney Disease. In: Wong, N.D., Amsterdam, E.A., Toth, P.P. (eds) ASPC Manual of Preventive Cardiology. Contemporary Cardiology. Springer, Cham. https://doi.org/10.1007/978-3-030-56279-3_25
Download citation
DOI: https://doi.org/10.1007/978-3-030-56279-3_25
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-56278-6
Online ISBN: 978-3-030-56279-3
eBook Packages: MedicineMedicine (R0)