
Abstract
Non-alcoholic fatty liver disease (NAFLD) is the most common liver disease, with a worldwide prevalence of 25%. NAFLD represents a spectrum of liver disease severity from simple hepatic steatosis to non-alcoholic steatohepatitis, which is a potentially progressive liver condition with ongoing liver injury. It is strongly associated with obesity, insulin resistance, metabolic syndrome, genetic factors, and lifestyle factors. However, the exact pathophysiology of NAFLD remains to be established. Moreover, the diagnosis of NASH also represents a major challenge. The reference standard in the diagnosis of NASH is considered liver biopsy. Due to its invasive nature, there is a major effort to optimize biochemical and imaging methods in terms of replacing liver biopsy. To date, a combination of noninvasive tests based on blood tests with imaging methods is recommended. Although there is no consensus about the pharmacological therapy of NASH, the international guidelines recommend achieving significant weight loss and lifestyle modification. In conclusion, the combination of high prevalence and its high burden warrant further research in that area.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Non-alcoholic fatty liver disease
- Non-alcoholic steatohepatitis
- Fibrosis
- Liver failure
- Liver transplantation
Worldwide Growth of Non-alcoholic Fatty Liver Disease
Non-alcoholic fatty liver disease (NAFLD) represents an umbrella term of clinical and pathologic entities, which encompasses simple hepatic steatosis, non-alcoholic fatty liver (NAFL), to non-alcoholic steatohepatitis (NASH), which according to compelling evidence is associated with fibrosis, cirrhosis, and, in some cases, hepatocellular carcinoma (HCC), in the absence of significant alcohol ingestion or other secondary causes of hepatic fat accumulation (Chalasani et al. 2018; European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO) 2016; Kaya and Yılmaz 2019a; Yilmaz 2012a).
There are different NAFLD prevalence reported around the world, mainly due to different study populations, but also due to the heterogeneity of the methods used to diagnose NAFLD. There are numerous noninvasive methods such as conventional ultrasonography, computerized tomography, magnetic resonance imaging (MRI), controlled attenuation parameter (CAP) by transient elastography (TE), and MRI-derived proton density fat fraction (PDFF-MRI). Depending on the accuracy, they can lead to over- or under-diagnosis (Kaya and Yılmaz 2019b). In a comprehensive meta-analysis, NAFLD is recognized as the most common chronic liver disease, with a prevalence of 25% worldwide. The highest prevalence was reported from the Middle East and South America, reaching 32% and 30%, respectively, whereas the lowest corresponds to Africa with 13% (Younossi et al. 2016).
From those 25% of the adult world population, approximately 20% (one-fifth) were classified as NASH corresponding to 16.5 million people (Estes et al. 2018a). Considering the future progress, by 2030 NAFLD prevalence was projected at 33.5%. As a reflection of the ageing population and disease progression, NASH was expected to increase by 27%. In this scenario, NASH is predicted to increase the number of liver-related deaths until 2030 by 178%. Therefore, NAFLD represents a significant public health issue worldwide (Sayiner et al. 2019).
NASH, the more progressive subtype of NAFLD, has an increased risk of proceeding to decompensated liver cirrhosis, hepatocellular carcinoma (HCC), and finally liver failure. Moreover, NAFLD has been recognized as a major contributor to the global burden of HCC. In the coming future, considering the trends of increase in NAFLD prevalence, NAFLD is expected to become the leading cause of HCC (Younossi et al. 2019a). In addition to this, NASH is the most rapidly growing aetiology for liver transplantation (Estes et al. 2018b).
Correlations with Obesity, Diabetes, and Metabolic Syndrome
The prevalence of NAFLD has increased in many countries both in the paediatric and adult populations as a result of the spread of sedentary lifestyle and westernized diet (Golabi et al. 2018). NAFLD is mostly associated with increased visceral obesity and metabolic abnormalities such as insulin resistance, diabetes mellitus, and dyslipidaemia. It became increasingly clear that NASH is the hepatic manifestation of the metabolic syndrome. Additionally, the prevalence of NASH is higher among diabetic and obese individuals. The risk of developing NASH was also reported to be in line with an increased number of components of metabolic syndrome (Chalasani et al. 2018; Younossi et al. 2019a). Moreover, being female, age over 50 years, obesity, metabolic syndrome, hypertension, dyslipidaemia, and hypertriglyceridaemia were reported as risk factors for developing NASH (Povsic et al. 2019).
According to a recent meta-analysis, more than 80% of NASH patients were overweight or obese (Chalasani et al. 2018). Obesity is known to increase the risk of developing NAFLD (Younossi et al. 2018; Singh et al. 2015). In fact, the prevalence of NAFLD is directly proportional to the increase in body mass index (BMI) (Younossi et al. 2019b). Given that NAFLD is associated with visceral obesity, the mutual evaluation of BMI and waist circumference can be more accurate in the classification of obesity in terms of NAFLD (Mongraw-Chaffin et al. 2015). NAFLD appears to increase at the same rate as obesity (World Health Organization (WHO) 2020; Fan et al. 2017). Although the prevalence of NAFLD was estimated to be around 25%, it could reach 90% in morbidly obese individuals, making possible even further prevalence elevations of NAFLD and related comorbidities (Younossi et al. 2019b).
Obese and Nonobese NAFLD
The majority of the patients undergoing bariatric surgery due to severe obesity have NAFLD, with a prevalence of approximately 95% (Sasaki et al. 2015; Subichin et al. 2015). On the other hand, a subgroup of patients, so-called lean NAFLD, were also reported to have NAFLD, although the BMI is normal (Akyuz et al. 2015; Yılmaz et al. 2019). As known, overweight is defined as >23 kg/m2 for Asian and >25 kg/m2 for Caucasian ethnicities (Consultation WHOE; WHO Expert Consultation 2004). Epidemiological data show a prevalence of 5–26% in Asian and 7–20% in Western populations (Consultation WHOE; WHO Expert Consultation 2004). Recent studies showed that NAFLD without the presence of obesity implies added severity, with increased rates of diabetes mellitus, metabolic syndrome and cardiovascular disorders (Sung et al. 2009).
NAFLD and Diabetes
Type 2 diabetes mellitus appears to be a major driver in the development of NAFLD. Moreover, type 2 diabetes mellitus accelerates the progression of liver disease (Stefan et al. 2019). According to a recent meta-analysis, the global prevalence of NAFLD among patients with type 2 diabetes mellitus was estimated to be over 55%, which corresponds to 4.7% of the global population. The prevalence of NASH among the diabetic population is estimated to be around 37%. In the same study, among the biopsied diabetic patients with NAFLD, the prevalence of advanced fibrosis was reported as 17% (Younossi et al. 2019c). Therefore, noninvasive screening of diabetic patients for both NASH and liver fibrosis is recommended, with the use of available noninvasive tools (Arrese et al. 2019).
Additionally, those patients had higher rates of other metabolic comorbidities. The vast majority of diabetic patients with NAFLD met the criteria of metabolic syndrome. More than half of them had hyperlipidaemia and hypertension; approximately one-fourth had cardiovascular disease (Kalra et al. 2013; Targher and Byrne 2015; Firneisz 2014). In fact, NAFLD itself is significantly associated with an increased risk of cardiovascular events and cardiovascular-related deaths (Targher et al. 2016).
NAFLD is considered the hepatic manifestation of metabolic syndrome due to its frequent coexistence with metabolic syndrome. However, the presence of metabolic syndrome is not sufficient to explain the coexistence of NAFLD. Because neither all the patients with NAFLD fulfil the criteria of metabolic syndrome nor all metabolic syndrome patients have NAFLD (Yilmaz 2012b). In fact, 20–80% of the patients with NAFLD have sufficient criteria for metabolic syndrome (Green 2003). In a recent community-based study, NAFLD alone was not associated with mortality, but those NAFLD patients with metabolically abnormal profiles had an increased risk of mortality (Niriella et al. 2019).
The Natural Course of NAFLD
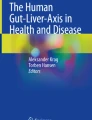
NAFLD is associated with increased all-cause mortality. However, isolated hepatic steatosis without hepatic inflammation behaves differently than NASH, exhibiting no increase in liver-related mortality and minimal risk for disease progression. Approximately 80% of the NAFLD patients remain as non-alcoholic fatty liver for life. The remaining 20% develop NASH, and from those, approximately 7% progress to HCC over 6.5 years (Torres DM1, Williams CD, Harrison SA. 2012). The annual development of HCC among NAFLD-associated cirrhosis patients was approximately 3% (Ascha et al. 2010). In another 8 years, 30% of those cirrhotic subjects are estimated to progress to hepatic decompensation (Torres DM1, Williams CD, Harrison SA. 2012). Patients with NASH showed progression to significant fibrosis at a rate of 13% in 17 years, to cirrhosis 2% in 20 years and without NASH to significant fibrosis at a rate of 10% in 19 years, to cirrhosis 3.1% in 7.6 years (Hagström et al. 2017a; Calzadilla Bertot and Adams 2016). The probability of developing cirrhosis is estimated to be annually 6% for F2 fibrosis and 8% for F3 fibrosis (Singh et al. 2015; Argo et al. 2009; Singh et al. 2015). The natural course of NAFLD is schematized in Fig. 24.1.

Natural course of NAFLD
Based on a meta-analysis with 11 cohort studies including 411 biopsy-proven NAFLD patients, and over 2145.5 person-years of follow-up evaluation, 33.6% of the subjects showed progression in fibrosis, 43.1% remained stable, and 22.3% had improvement regarding fibrosis stage. Progression of fibrosis at stage 1 was determined as 14.3 years for patients with NAFL and 7.1 years with NASH. Among NASH patients, 20% had rapid progression rates in the fibrosis stage (Singh et al. 2015). In a meta-analysis of Dulai et al., fibrosis stage was found to be directly associated with all-cause mortality and liver-related mortality. This increase is more pronounced in patients with fibrosis stages of 3–4 (Dulai et al. 2017).
Liver-related mortality is not the leading cause of death among patients with NASH. In decreasing order, the most common aetiologies for mortality are cardiovascular disease, malignancies and then liver-related causes (Francque et al. 2011; Dam-Larsen et al. 2009; Söderberg et al. 2010). Diabetes mellitus, severe insulin resistance, increased BMI, significant weight gain (Adams et al. 2005), and cigarette smoking (Enc et al. 2019) are associated with disease severity. On the other hand, the effect of increased serum transaminases at disease severity remains controversial. Studies have shown that although increased serum aminotransferases indicate the probability of NAFLD, the absence of increased aminotransferases does not exclude NAFLD (Mofrad et al. 2003). NAFLD patients with normal liver enzymes are characterized by a severe metabolic profile, however, similar rates of advanced fibrosis compared to subjects with elevated aminotransferases (Ulasoglu et al. 2019).
Coffee and Alcohol
Coffee consumption is considered a protective factor for NAFLD (Yesil and Yilmaz 2013). A meta-analysis showed a significantly decreased risk of NAFLD among coffee drinkers, including less risk of liver fibrosis among patients with NAFLD, who consumed coffee regularly, which can make coffee a preventive factor for NAFLD and NAFLD-related complications (Wijarnpreecha et al. 2017). There are also studies showing the benefits of low amounts of alcohol consumption. Up to 13 units per week were shown to be associated with a lower stage of fibrosis (Hagström et al. 2017b).
One unit (10 ml ethanol) roughly corresponds to 25 ml of distilled drinks, 80 ml of wine, and 170 ml of beer. However, there is insufficient evidence about the benefits of alcohol consumption. Heavy episodic drinking may accelerate fibrosis progression and increase the risk of hepatocellular carcinoma. Therefore, considering the overlap between the pathophysiological mechanisms of NAFLD and alcoholic fatty liver disease, alcohol consumption is discouraged (Ajmera et al. 2017). In parallel, recent data showed there is no safe level or beneficial level of alcohol consumption. The safe level must be no consumption at all (Burton and Sheron 2018).
Noninvasive Diagnostic Methods vs. Liver Biopsy
Liver biopsy is considered the gold standard in approach for identifying the presence of NASH and a histological classification of the disease in terms of fibrosis. However, due to major limitations such as high cost, sampling errors, patients’ discomfort, and the presence of procedure-related morbidity and even mortality, its use in the clinical practice remains questionable. Therefore, there has been significant interest in developing noninvasive methodologies to predict the severity of the disease (Musso et al. 2011). Risk factors for NAFLD are summarized in Table 24.1.
The fibrosis stage is specifically associated with the prognosis of the disease. Stages 3–4 increased the risk of liver-related mortality by 50–80%. In this context, noninvasive detection of the fibrosis stage has been a major focus. The most common noninvasive scores are NAFLD Fibrosis Score (NFS), the Fibrosis-4 Score (FIB-4), the AST to Platelet Ratio Index (APRI), and the BARD Score, which includes several clinical and biochemical parameters obtained by routine clinical examinations (Drescher et al. 2019). The NAFLD guideline of the American Association for the Study of Liver Diseases (AASLD) recommends FIB-4 and NFS as clinically useful tools for the prediction of advanced fibrosis (F≥3) (Chalasani et al. 2018), Kaya et al. 2020. However, those scores have a high negative predictive value rather than positive predictive value, which means they can be confidently used for exclusion of advanced fibrosis rather than detection of it as also recommended in the guideline of European Association for the Study of the Liver (EASL) (European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO) 2016; Kaya et al. 2019).
Single vs. Multiple Criteria
Moreover, those scores include a grey zone, in which NAFLD patients are classified as having an indeterminate risk for advanced fibrosis. Another clinically important question concerns the management of those patients. Therefore, noninvasive scores are useful in the first-line stratification of the disease. Owing to the high-negative predictive values of those tests, patients classified as low risk for advanced fibrosis are recommended to be managed in primary care, whereas those at high risk should be directly referred to secondary care. For the patients in the indeterminate zone, Fibroscan examination is recommended for detecting the future management strategy. A noninvasive fibrosis marker or score, a diagnostic test, or an algorithm incorporating a panel of biomarkers is not capable of making a comprehensive statement of the disease outcome. Therefore, the combined use of noninvasive scores with imaging methods has been advised to increase diagnostic accuracy (Jafarov et al. 2019; Zhou et al. 2019).
Imaging Tools
Conventional ultrasonography is recommended for the diagnosis of moderate-to-severe steatosis, with a sensitivity of 85% and a specificity of 94% (Hernaez et al. 2011). However, it is incapable of detecting steatosis lower than 20% or in morbidly obese patients (Chalasani et al. 2018). Computerized tomography is more effective for evaluating hepatic steatosis; however, it remains also limited by insufficient accuracy for mild-to-moderate hepatic steatosis, and it involves radiation exposure (Schwenzer et al. 2009). Alternatively, controlled attenuation parameter (CAP) by Fibroscan, which measures the hepatic fat quantity by attenuation of the shear waves, and magnetic resonance-derived proton density fat fraction (MRI-PDFF), are more accurate and up-to-date methods for detection of hepatic steatosis. MRI-PDFF is a robust noninvasive method to monitor the treatment effect by means of hepatic fat quantification (Caussy et al. 2018). It is considered more accurate, reproducible, and reliable than liver histology. However, its use remains limited due to high costs, need for expertise, and long examination duration (Dulai et al. 2016). In terms of quick accessibility and cost-effectiveness, CAP (Fibroscan) is preferred over MRI-PDFF in clinical routine (Leung et al. 2013).
First-line Liver Fibrosis Assessment
Vibration-controlled transient elastography (VCTE) is the first Food and Drug Administration-approved modality by FibroScan employing ultrasound-based technology, which measures the velocity of a shear wave that is emitted by a probe in the intercostal space into the liver (Leung et al. 2013). Magnetic Resonance Elastography (MRE) is an excellent method as well for assessment of fibrosis stage in NAFLD. According to recent information, MRE performs better than VCTE for the identification of significant fibrosis; on the other hand, it performed equally well for the quantification of advanced fibrosis (Loomba et al. 2014).
Pathophysiology
The development of NAFLD classically relies on the “multiple hit and organ theory,” in agreement with a large spectrum of metabolic dysfunctions caused by the interaction of genetic and environmental factors (Buzzetti et al. 2016). Liver fat accumulation, caused by obesity and insulin resistance, seems to represent the “first hit” (Fang et al. 2018). Hepatic fat accumulation in the liver is mainly comprised of triacylglycerol (TAG) derived from the esterification of glycerol and free fatty acids (FFA) (Buzzetti et al. 2016). TAG in hepatic fat is hydrolysed and secreted into the blood circulation as very-low-density lipoprotein particles. Disruption of those pathways can result in hepatic steatosis (Musso et al. 2013). Peroxisome proliferator-activated receptor-α (PPAR-α) plays a significant role in the regulation of β-oxidation in hepatocytes. The downregulation of PPAR-α was significantly associated with NAFLD and NASH (Tanaka et al. 2017). De novo lipogenesis in hepatocytes is mainly regulated by activation of transcriptional factor sterol regulatory element-binding protein 1c (SREBP-1c), which is enhanced by hyperglycaemia, and explains the close association between NAFLD and insulin resistance (Tanaka et al. 2019).
Subsequent Steps
Hepatic fat accumulation does not represent alone strong toxicity for the liver. There is no association between the degree of steatosis and NAFLD severity. However, TAG-derived molecules and its precursors such as palmitate, diacylglycerol (DAG), and ceramide are likely to be a detriment to hepatocytes. Palmitate increases oxidative stress leading to lipoapoptosis. DAG activates protein kinase C disrupting the insulin signalling pathway, and ceramide promotes the production of palmitate (Akazawa and Nakao 2018; Jiang et al. 2015; Gan et al. 2014). Furthermore, overloaded TAG storage creates metabolic distress and following this lipotoxicity, which increases together oxidative stress.
Normally, oxidation of FFAs ensues through α-, β-, and ω-oxidation. Mitochondrial β-oxidation and peroxisomal α-, β-oxidation are normal metabolic processes. However, if these metabolic pathways are impaired, ω-oxidation occurs in endoplasmic reticulum leading to reactive oxygen species production. It was observed that ω-oxidation and oxidation via NADPH oxidase in Kupffer cells are increased in NAFLD patients, causing inhibition of mitochondrial β-oxidation. All these metabolic processes lead to DNA damage in cell nucleus and mitochondria, and release of cytokines which promotes hepatocellular injury (Yao et al. 2019).
The Liver Damage Cascade
Hepatocellular injury causes the release of several pro-inflammatory mediators recruiting immune cells and activating Kupffer cells, which result in the release of bioactive molecules further damaging hepatocytes (Zhang et al. 2015). Chronic hepatocyte death or impaired hepatocyte regeneration leads to alternative replacement by fibres and extracellular matrix, resulting in significant scar tissue formation and remodelling of the normal structure of hepatic lobules. Fibrogenesis mainly in the perisinusoidal space is relatively specific to steatohepatitis (Lee et al. 2015).
The Microbiota and the Gut Barrier Function
There is increasing research interest on gut-liver axis dysfunction including intestinal dysbiosis, bacterial overgrowth, and alteration of gastrointestinal mucosa permeability. In the development of NAFLD, gastrointestinal microbiota play a significant role in maintaining barrier integrity and intestinal permeability. There are several mechanisms associated with alteration in gastrointestinal microbiota and development of NAFLD: Deterioration in microbiota can damage the intestinal epithelium and tight junction proteins in the gut, which allow harmful substances such as bacteria, ethanol, and endotoxins entering into the portal circulation. Furthermore, microbiota digest and ferment the excessive dietary energy into short-chain fatty acids and produces ethanol, affecting the liver similarly to chronic alcoholism (Doulberis et al. 2017).
According to the study of Zhu et al., there is a significantly increased population of alcohol-producing bacteria in patients with NASH compared to obese and healthy subjects. Furthermore, a significantly increased serum ethanol concentration was observed in NASH patients, although there was no difference between obese and healthy subjects (Zhu et al. 2013). In a more recent study, high alcohol-producing Klebsiella pneumonia was found to be associated with up to 60% of individuals of the study cohort. Moreover, clinical isolates of high alcohol-producing Klebsiella pneumonia transferred via oral gavage or faecal transplant also induced NAFLD in mice, supporting the strong association with NAFLD development (Yuan et al. 2019).
Disease-specific Variants
NAFLD is also associated with a genetic predisposition. Although only a minority of the genetic modifiers of NAFLD has been validated, there are several genetic associations to mention. The initial genome was identified as PNPLA3, which was validated in different ethnic groups as a modifier of NAFLD severity. In obese children and adolescents, the PNPLA3 rs738409 variant was also suspected to affect the histological severity in NAFLD (Valenti et al. 2010). Additionally, PNPLA3 has been accepted globally as a major determinant of not only steatosis but also the severity of NASH, fibrosis stage, and probability of HCC development (Anstee and Day 2013). Recently, the TM6SF2 gene has been reported as another disease modifier, which might be clinically useful in the future for estimating the disease progression severity (Dongiovanni et al. 2015).
TM6SF2 rs58542926 T-allele mediates hepatic accumulation of triglycerides and cholesterol creating a predisposition to NAFLD-related fibrosis, whereas C-allele carriage protects liver excreting VLDL from the liver, at a price of increased atherosclerosis and cardiovascular disease (Kahali et al. 2015). More recently, HSD17B13 was found to play role in the progression of liver disease from steatosis to later stages of non-alcoholic steatohepatitis, fibrosis, and cirrhosis, since the reduced activity of HSD17B13 was associated with a lower risk of progression from steatosis to steatohepatitis (Abul-Husn et al. 2018). MBOAT gene was also associated with disease severity in both NAFLD and alcoholic fatty liver disease (Caussy et al. 2019).
Lifestyle and Pharmacological Interventions
NAFLD has been associated with a diet of high caloric amount, which contains excessive saturated fats, refined carbohydrates, and high fructose (Barrera and George 2014), along with sedentary behaviour (Gerber et al. 2012). Therefore, lifestyle modification is the cornerstone treatment of NAFLD and has an important impact on the natural course of the disease (Kugelmas et al. 2003). Weight loss between 5 and 7% can diminish fat accumulation, whereas a 7–10% weight loss is significantly associated with improvement in NASH and fibrosis, with a chance of 64% and 50%, respectively. Weight loss of >10% was associated with up to 90% chance of NASH resolution and up to 81% of regression in fibrosis (Vilar-Gomez et al. 2015).
According to the recent studies and expert opinions, following a Mediterranean diet can reduce liver fat even without weight loss, which is characterized by reduced carbohydrate and increased monounsaturated and ω-3 fatty acid intake (Romero-Gomez et al. 2017). Therefore, it has been also recommended as the preferred diet type in the major guidelines (Chalasani et al. 2018; European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO) 2016). In addition to diet modifications, exercise should also be recommended. Aerobic exercise training of 150 min per week contributed to weight reduction and had an impact on intrahepatic fat (Hashida et al. 2017).
Zelber-Sagi et al. demonstrated that weight gain was a predictor of NAFLD development even among nonobese individuals. Loss of 5% of the initial body weight resulted in remission of NAFLD in 75% of those individuals (Zelber-Sagi et al. 2012). Both lean and obese individuals seem to similarly benefit from weight loss in terms of NAFLD remission (Varol Hamurcu et al. 2020).
Bariatric Interventions
In line with weight reduction, bariatric surgery is an excellent method to recommend for morbidly obese patients. After a one-year follow-up, in more than 85% of the patients, resolution of NASH has been observed. Moreover, in those patients, pathological features were also ameliorated (Laursen et al. 2019). In a meta-analysis, steatosis, inflammation, and ballooning mostly improved or completely resolved. An extensive review emphasizes that in most patients, liver fibrosis diminishes, whereas refractory cases exist in which both fibrosis and inflammation persist or progress (Laursen et al. 2019).
Drug Therapy
There is no specifically licensed pharmacological treatment for NAFLD. Yet, given the close association between NAFLD and type 2 diabetes mellitus, pioglitazone has been utilized in NASH targeting both adipose tissue metabolism and inflammation through PPAR-γ. Thus, it reduces hepatic steatosis, inflammation, and ballooning increasing uptake of fatty acid by adipocytes. However, because of its side effects such as weight gain and the conflict of its effect on the improvement of hepatic fibrosis, its use recommended only in selected diabetic patients (Cusi et al. 2016).
Although there is no convincing evidence about vitamin E and improvement of liver fibrosis, given the antioxidative and anti-inflammatory effect of vitamin E, it has been investigated as a therapeutic option in NASH. However, due to lack of further data, vitamin E is not recommended in NASH patients with diabetes, NAFLD without liver biopsy, NASH cirrhosis, or cryptogenic cirrhosis. The risks and benefits must be discussed for each patient individually (Chalasani et al. 2018).
There are several pharmaceutical agents with completed or ongoing phase III controlled trials. Obeticholic acid improves hepatic insulin sensitivity and decreases lipogenesis, inflammation, and fibrosis. The interim analysis of the phase 3 REGENERATE Study showed that obeticholic acid use resulted in fibrosis improvement without worsening of NASH (Younossi et al. 2019d). However, due to its side effects such as LDL increase and pruritus, its use in clinical routine remains limited considering that 13% discontinued therapy and 17% exhibited increased LDL levels (Younossi et al. 2019d). Another agent selonsertib inhibits apoptosis signal-regulating kinase 1, which reduces hepatocyte apoptosis and fibrosis. Still selonsertib failed to meet endpoint in STELLAR-3 and STELLAR-4 phase III clinical trials (Trial Site 2019; Clinical Trials 2019). Also Emricasan, an oral pan-caspase inhibitor, suppresses apoptosis failed to meet endpoint, also worsening liver histology (Shiffman et al. 2019). The ongoing phase III trials are with elafibranor, a PPARα and PPARδ agonist, which also improves insulin sensitivity and hepatic inflammation (Yuan et al. 2019), and cenicriviroc, a dual C-C chemokine receptor type 2 and 5 (CCR2/5) inhibitor (Yuan et al. 2019). The results of these trials are expected to be released through the midyear of 2020. In conclusion, diet and exercise remain still the cornerstone of NAFLD therapy.
References
Abul-Husn NS, Cheng X, Li AH, Xin Y, Schurmann C, Stevis P et al (2018) A protein-truncating HSD17B13 variant and protection from chronic liver disease. N Engl J Med 378(12):1096–1106
Adams LA, Sanderson S, Lindor KD, Angulo P (2005) The histological course of nonalcoholic fatty liver disease: a longitudinal study of 103 patients with sequential liver biopsies. Hepatology 42:132–138
Ajmera VH, Terrault NA, Harrison SA (2017) Is moderate alcohol use in nonalcoholic fatty liver disease good or bad? A critical review. Hepatology 65(6):2090–2099
Akazawa Y, Nakao K (2018) To die or not to die: death signaling in nonalcoholic fatty liver disease. J Gastroenterol 53:893–906
Akyuz U, Yesil A, Yilmaz Y (2015) Characterization of lean patients with nonalcoholic fatty liver disease: potential role of high hemoglobin levels. Scand J Gastroenterol 50(3):341–346
Anstee QM, Day CP (2013) The genetics of NAFLD. Nat Rev Gastroenterol Hepatol 10(11):645–655
Argo CK, Northup PG, Al-Osaimi AM, Caldwell SH (2009) Systematic review of risk factors for fibrosis progression in non-alcoholic steatohepatitis. J Hepatol 51(2):371–379
Arrese M, Barrera F, Triantafilo N, Arab JP (2019) Concurrent nonalcoholic fatty liver disease and type 2 diabetes: diagnostic and therapeutic considerations. Expert Rev Gastroenterol Hepatol 13(9):849–866
Ascha MS, Hanouneh IA, Lopez R, Tamimi TA, Feldstein AF, Zein NN (2010) The incidence and risk factors of hepatocellular carcinoma in patients with nonalcoholic steatohepatitis. Hepatology 51(6):1972–1978
Barrera F, George J (2014) The role of diet and nutritional intervention for the management of patients with NAFLD. Clin Liver Dis 18:91–112
Burton R, Sheron N (2018) No level of alcohol consumption improves health. Lancet 392(10152):987–988
Buzzetti E, Pinzani M, Tsochatzis EA (2016) The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism 65:1038–1048
Calzadilla Bertot L, Adams LA (2016) The natural course of non-alcoholic fatty liver disease. Int J Mol Sci 20:E774
Caussy C, Reeder SB, Sirlin CB, Loomba R (2018) Noninvasive, quantitative assessment of liver fat by MRIPDFF as an endpoint in NASH Trials. Hepatology 68:763–772
Caussy C, Bhargava M, Villesen IF, Gudmann NS, Leeming DJ, Karsdal MA et al (2019) Collagen formation assessed by N-terminal propeptide of type 3 procollagen is a heritable trait and is associated with liver fibrosis assessed by magnetic resonance elastography. Hepatology 70(1):127–141
Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M et al (2018) The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology 67:328–357
Clinical Trials (2019). https://www.clinicaltrialsarena.com/news/gileads-selonsertib-fails/. Accessed 23 Nov 2019
Consultation WHOE; WHO Expert Consultation (2004) Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363(9403):157–163
Cusi K, Orsak B, Bril F, Lomonaco R, Hecht J, Ortiz-Lopez C et al (2016) Long-term pioglitazone treatment for patients with nonalcoholic steatohepatitis and prediabetes or type 2 diabetes mellitus. Ann Intern Med 165:305–315
Dam-Larsen S, Becker U, Franzmann MG, Larsen K, Christoffersen P, Bendtsen F (2009) Final results of a long-term, clinical follow-up in fatty liver patients. Scand J Gastroenterol 44:1236–1243
Dongiovanni P, Petta S, Maglio C, Fracanzani AL, Pipitone R, Mozzi E et al (2015) Transmembrane 6 superfamily member 2 gene variant disentangles nonalcoholic steatohepatitis from cardiovascular disease. Hepatology 61:506–514
Doulberis M, Kotronis G, Gialamprinou D, Kountouras J, Katsinelos P (2017) Non-alcoholic fatty liver disease: An update with special focus on the role of gut microbiota. Metabolism 71:182–197
Drescher HK, Weiskirchen S, Weiskirchen R (2019) Current status in testing for nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH). Cell 8(8):E845. https://doi.org/10.3390/cells8080845
Dulai PS, Sirlin CB, Loomba R (2016) MRI and MRE for non-invasive quantitative assessment of hepatic steatosis and fibrosis in NAFLD and NASH: clinical trials to clinical practice. J Hepatol 65(5):1006–1016
Dulai PS, Singh S, Patel J, Soni M, Prokop LJ, Younossi Z et al (2017) Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: systematic review and meta-analysis. Hepatology 65(5):1557–1565
Enc FY, Ulasoglu C, Bakir A, Yilmaz Y (2019) The interaction between current smoking and hemoglobin on the risk of advanced fibrosis in patients with biopsy-proven nonalcoholic fatty liver disease. Eur J Gastroenterol Hepatol 32:597–600. https://doi.org/10.1097/MEG.0000000000001536
Estes C, Razavi H, Loomba R, Younossi Z, Sanyal AJ (2018a) Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 67:123–133
Estes C, Anstee QM, Arias-Loste MT, Bantel H, Bellentani S, Caballeria J et al (2018b) NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J Hepatol 69:896–904
European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO) (2016) EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. J Hepatol 64(6):1388–1402
Fan JG, Kim SU, Wong VW (2017) New trends on obesity and NAFLD in Asia. J Hepatol 67(4):862–873
Fang YL, Chen H, Wang CL, Liang L (2018) Pathogenesis of non-alcoholic fatty liver disease in children and adolescence: from “two hit theory” to “multiple hit model”. World J Gastroenterol 24(27):2974–2983
Firneisz G (2014) Non-alcoholic fatty liver disease and type 2 diabetes mellitus: the liver disease of our age? World J Gastroenterol 20:9072–9089
Francque S, De Maeght S, Adler M, Deltenre P, de Galocsy C, Orlent H et al (2011) High prevalence of advanced fibrosis in association with the metabolic syndrome in a Belgian prospective cohort of NAFLD patients with elevated ALT: results of the Belgian NAFLD registry. Acta Gastroenterol Belg 74:9–16
Gan LT, Van Rooyen DM, Koina ME, McCuskey RS, Teoh NC, Farrell GC (2014) Hepatocyte free cholesterol lipotoxicity results from JNK1-mediated mitochondrial injury and is HMGB1 and TLR4-dependent. J Hepatol 61:1376–1384
Gerber L, Otgonsuren M, Mishra A, Escheik C, Birerdinc A, Stepanova M et al (2012) Non-alcoholic fatty liver disease (NAFLD) is associated with low level of physical activity: a population-based study. Aliment Pharmacol Ther 36:772–781
Golabi P, Otgonsuren M, de Avila L, Sayiner M, Rafiq N, Younossi ZM (2018) Components of metabolic syndrome increase the risk of mortality in nonalcoholic fatty liver disease (NAFLD). Medicine (Baltimore) 97(13):e0214
Green RM (2003) NASH—hepatic metabolism and not simply the metabolic syndrome. Hepatology 38:14–17
Hagström H, Nasr P, Ekstedt M, Hammar U, Stål P, Hultcrantz R, Kechagias S (2017a) Fibrosis stage but not NASH predicts mortality and time to development of severe liver disease in biopsy-proven NAFLD. J Hepatol 67(6):1265–1273
Hagström H, Nasr P, Ekstedt M, Kechagias S, Önnerhag K, Nilsson E et al (2017b) Low to moderate lifetime alcohol consumption is associated with less advanced stages of fibrosis in non-alcoholic fatty liver disease. Scand J Gastroenterol 52(2):159–165
Hashida R, Kawaguchi T, Bekki M, Omoto M, Matsuse H, Nago T et al (2017) Aerobic vs. resistance exercise in non-alcoholic fatty liver disease: a systematic review. J Hepatol 66(1):142–152
Hernaez R, Lazo M, Bonekamp S, Kamel I, Brancati FL, Guallar E, Clark JM (2011) Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology 54:1082–1090
Jafarov F, Kaya E, Bakir A, Eren F, Yilmaz Y (2019) The diagnostic utility of fibrosis-4 or non-alcoholic fatty liver disease fibrosis score combined with liver stiffness measurement by Fibroscan in assessment of advanced liver fibrosis: a biopsy-proven nonalcoholic fatty liver disease study. Euro J Gastroent Hepatol 32:642–649. https://doi.org/10.1097/MEG.0000000000001573
Jiang C, Xie C, Li F, Zhang L, Nichols RG, Krausz KW, Cai J, Qi Y, Fang ZZ, Takahashi S, Tanaka N, Desai D, Amin SG, Albert I, Patterson AD, Gonzalez FJ (2015) Intestinal farnesoid X receptor signaling promotes nonalcoholic fatty liver disease. J Clin Invest 125:386–402
Kahali B, Liu YL, Daly AK, Day CP, Anstee QM, Speliotes EK (2015) TM6SF2: catch-22 in the fight against nonalcoholic fatty liver disease and cardiovascular disease? Gastroenterology 148(4):679–684
Kalra S, Vithalani M, Gulati G, Kulkarni CM, Kadam Y, Pallivathukkal J et al (2013) Study of prevalence of nonalcoholic fatty liver disease (NAFLD) in type 2 diabetes patients in India (SPRINT). J Assoc Physicians India 61:448–453
Kaya E, Yılmaz Y (2019a) Non-alcoholic fatty liver disease: a growing public health problem in Turkey. Turk J Gastroenterol 10:865–871
Kaya E, Yılmaz Y (2019b) Türkiye’de ve dünyada nonalkolik yağlı karaciğer hastalığı epidemiyolojisi. In: Sonsuz A (ed) Nonalkolik Yağlı Karaciğer Hastalığı, 1st edn. Türkiye Klinikleri, Ankara, pp 1–7
Kaya E, Bakir A, Kani HT, Demirtas CO, Keklikkiran C, Yilmaz Y (2019) Simple noninvasive scores are clinically useful to exclude, not predict, advanced fibrosis: a study in Turkish patients with biopsy-proven nonalcoholic fatty liver disease. Gut Liver 14:486–491. https://doi.org/10.5009/gnl19173
Kaya E, Bakir E, Eren F, Yilmaz Y (2020). The utility of noninvasive scores in non-alcoholic fatty liver disease patients with normal and elevated serum transaminases. Hepatol Forum 1(1):8–13
Kugelmas M, Hill DB, Vivian B, Marsano L, McClain CJ (2003) Cytokines and NASH: a pilot study of the effects of lifestyle modification and vitamin E. Hepatology 38:413–419
Laursen TL, Hagemann CA, Wei C, Kazankov K, Thomsen KL, Knop FK, Grønbæk H (2019) Bariatric surgery in patients with non-alcoholic fatty liver disease—from pathophysiology to clinical effects. World J Hepatol 11(2):138–149
Lee YA, Wallace MC, Friedman SL (2015) Pathobiology of liver fibrosis: a translational success story. Gut 64:830–841
Leung VY, Shen J, Wong VW, Abrigo J, Wong GL, Chim AM, Chu SH, Chan AW, Choi PC, Ahuja AT, Chan HL, Chu WC (2013) Quantitative elastography of liver fibrosis and spleen stiffness in chronic hepatitis B carriers: comparison of shear-wave elastography and transient elastography with liver biopsy correlation. Radiology 269:910–918
Loomba R, Wolfson T, Ang B, Hooker J, Behling C, Peterson M et al (2014) Magnetic resonance elastography predicts advanced fibrosis in patients with nonalcoholic fatty liver disease: a prospective study. Hepatology 60:1920–1928
Mofrad P, Contos MJ, Haque M, Sargeant C, Fisher RA, Luketic VA et al (2003) Clinical and histologic spectrum of nonalcoholic fatty liver disease associated with normal ALT values. Hepatology 37:1286–1292
Mongraw-Chaffin M, Golden SH, Allison MA, Ding J, Ouyang P, Schreiner PJ et al (2015) The sex and race specific relationship between anthropometry and body fat composition determined from computed tomography: evidence from the multi-ethnic study of atherosclerosis. PLoS One 10:e0139559
Musso G, Gambino R, Cassader M, Pagano G (2011) Meta-analysis: natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasive tests for liver disease severity. Ann Med 43:617–649
Musso G, Gambino R, Cassader M (2013) Cholesterol metabolism and the pathogenesis of non-alcoholic steatohepatitis. Prog Lipid Res 52:175–191
Niriella MA, Kasturiratne A, Beddage TU, Withanage SA, Goonatilleke DC, Abeysinghe CP et al (2019) Metabolic syndrome, but not non-alcoholic fatty liver disease, increases 10-year mortality: a prospective, community-cohort study. Liver Int 40:101–106. https://doi.org/10.1111/liv.14237
Povsic M, Wong OY, Perry R, Bottomley J (2019) A structured literature review of the epidemiology and disease burden of non-alcoholic steatohepatitis (NASH). Adv Ther 36:1574–1594
Romero-Gomez M, Zelber-Sagi S, Trenell M (2017) Treatment of NAFLD with diet, physical activity and exercise. J Hepatol 67(4):829–846
Sasaki A, Nitta H, Otsuka K, Umemura A, Baba S, Obuchi T et al (2015) Bariatric surgery and non-alcoholic fatty liver disease: current and potential future treatments. Front Endocrinol 5:164
Sayiner M, Golabi P, Younossi ZM (2019) Disease burden of hepatocellular carcinoma: a global perspective. Dig Dis Sci 64(4):910–917
Schwenzer NF, Springer F, Schraml C, Stefan N, Machann J, Schick F (2009) Non-invasive assessment and quantification of liver steatosis by ultrasound, computed tomography and magnetic resonance. J Hepatol 51:433–445
Shiffman M, Freilich B, Vuppalanchi R, Watt K, Chan JL, Spada A et al (2019) Randomised clinical trial: emricasan versus placebo significantly decreases ALT and caspase 3/7 activation in subjects with non-alcoholic fatty liver disease. Aliment Pharmacol Ther 49(1):64–73
Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R (2015) Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 13(4):643–654
Söderberg C, Stål P, Askling J, Lindberg G, Marmur J, Hultcrantz R (2010) Decreased survival of subjects with elevated liver function tests during a 28-year follow-up period. Hepatology 51:595–602
Stefan N, Haring HU, Cusi K (2019) Non-alcoholic fatty liver disease: causes, diagnosis, cardiometabolic consequences, and treatment strategies. Lancet Diabetes Endocrinol 7(4):313–324
Subichin M, Clanton J, Makuszewski M, Bohon A, Zografakis JG, Dan A (2015) Liver disease in the morbidly obese: a review of 1000 consecutive patients undergoing weight loss surgery. Surg Obes Relat Dis 11:137–141
Sung KC, Ryan MC, Wilson AM (2009) The severity of nonalcoholic fatty liver disease is associated with increased cardiovascular risk in a large cohort of non-obese Asian subjects. Atherosclerosis 203:581–586
Tanaka N, Aoyama T, Kimura S, Gonzalez FJ (2017) Targeting nuclear receptors for the treatment of fatty liver disease. Pharmacol Ther 179:142–157
Tanaka N, Kimura T, Fujimori N, Nagaya T, Komatsu M, Tanaka E (2019) Current status, problems, and perspectives of non-alcoholic fatty liver disease research. World J Gastroenterol 25(2):163–177
Targher G, Byrne CD (2015) A perspective on metabolic syndrome and nonalcoholic fatty liver disease. Metab Syndr Relat Disord 13:235–238
Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C (2016) Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol 65(3):589–600
Torres DM, Williams CD, Harrison SA (2012) Features, diagnosis, and treatment of nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 10(8):837–858
Trial Site (2019). https://www.trialsitenews.com/gilead-reports-phase-3-stellar-3-of-selonsertib-for-bridging-fibrosis-f3-due-to-nonalcoholic-steatohepatitis-fails-to-meet-endpoints/. Accessed 23 Nov 2019
Ulasoglu C, Enc Yilmaz F, Kaya E, Yilmaz Y (2019) Characterization of patients with biopsy-proven non-alcoholic fatty liver disease and normal aminotransferase levels. J Gastrointest Liver Dis 28(4):427–431
Valenti L, Alisi A, Galmozzi E, Bartuli A, Del Menico B, Alterio A et al (2010) I148M patatin-like phospholipase domain-containing 3 gene variant and severity of pediatric nonalcoholic fatty liver disease. Hepatology 52:1274–1280
Varol Hamurcu P, Kaya E, Alphan E, Yilmaz Y (2020) Role of intensive dietary and lifestyle interventions in the treatment of lean nonalcoholic fatty liver disease patients. Eur J Gastroenterol Hepatol 32:1352–1357
Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, Torres-Gonzalez A, Gra-Oramas B, Gonzalez-Fabian L et al (2015) Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology 149(2):367–378
Wijarnpreecha K, Thongprayoon C, Ungprasert P (2017) Coffee consumption and risk of nonalcoholic fatty liver disease: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol 29(2):e8–e12
World Health Organization (WHO) (2020) Obesity and overweight. Obtained from the world wide web. http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 23 Nov 2019
Yao Y, Cai J, She Z, Li H (2019) Insights into the epidemiology, pathogenesis, and therapeutics of nonalcoholic fatty liver diseases. Adv Sci (Weinh) 6(4):1801585
Yesil A, Yilmaz Y (2013) Review article: coffee consumption, the metabolic syndrome and non-alcoholic fatty liver disease. Aliment Pharmacol Ther 38(9):1038–1044
Yilmaz Y (2012a) Review article: is non-alcoholic fatty liver disease a spectrum, or are steatosis and non-alcoholic steatohepatitis distinct conditions? Aliment Pharmacol Ther 36(9):815–823
Yilmaz Y (2012b) Is nonalcoholic fatty liver disease the hepatic expression of the metabolic syndrome? World J Hepatol 4:332–334
Yılmaz Y, Kanı HT, Demirtaş CÖ, Kaya E, Sapmaz AF, Qutranji L et al (2019) Growing burden of nonalcoholic fatty liver disease in Turkey: a single-center experience. Turk J Gastroenterol 30(10):892–898
Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M (2016) Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 64:73–84
Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, George J, Bugianesi E (2018) Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol 15(1):11–20
Younossi Z, Stepanova M, Ong JP, Jacobson IM, Bugianesi E, Duseja A et al (2019a) Nonalcoholic steatohepatitis is the fastest growing cause of hepatocellular carcinoma in liver transplant candidates. Clin Gastroenterol Hepatol 17:748–755
Younossi Z, Tacke F, Arrese M, Sharma BC, Mostafa I, Bugianesi E, Wong VW, Yilmaz Y, George J, Fan J, Vos MB (2019b) Global perspectives on non-alcoholic fatty liver disease and non-alcoholic steatohepatitis. Hepatology 69(6):2672–2682
Younossi ZM, Golabi P, de Avila L, Paik JM, Srishord M, Fukui N, Qiu Y, Burns L, Afendy A, Nader F (2019c) The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol 71(4):793–801
Younossi Z, Ratziu V, Loomba R et al (2019d) Positive results from REGENERATE: a phase 3 international, randomized, placebo-controlled study evaluating obeticholic acid treatment for NASH. J Hepatol 70:e5. https://doi.org/10.1016/S0618-8278(19)30006-4
Yuan J, Chen C, Cui J, Lu J, Yan C, Wei X et al (2019) Fatty liver disease caused by high-alcohol-producing klebsiella pneumoniae. Cell Metab 30(4):675–688
Zelber-Sagi S, Lotan R, Shlomai A, Webb M, Harrari G, Buch A et al (2012) Predictors for incidence and remission of NAFLD in the general population during a seven-year prospective follow-up. J Hepatol 56:1145–1151
Zhang L, Nichols RG, Correll J, Murray IA, Tanaka N, Smith PB, Hubbard TD, Sebastian A, Albert I, Hatzakis E, Gonzalez FJ, Perdew GH, Patterson AD (2015) Persistent organic pollutants modify gut microbiota-host metabolic homeostasis in mice through aryl hydrocarbon receptor activation. Environ Health Perspect 123:679–688
Zhou JH, Cai JJ, She ZG, Li HL (2019) Noninvasive evaluation of nonalcoholic fatty liver disease: current evidence and practice. World J Gastroenterol 25(11):1307–1326
Zhu L, Baker SS, Gill C, Liu W, Alkhouri R, Baker RD, Gill SR (2013) Characterization of gut microbiomes in nonalcoholic steatohepatitis (NASH) patients: A connection between endogenous alcohol and NASH. Hepatology 57(2):601–609
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kaya, E., Yilmaz, Y. (2020). Non-alcoholic Fatty Liver Disease: A Global Public Health Issue. In: Faintuch, J., Faintuch, S. (eds) Obesity and Diabetes. Springer, Cham. https://doi.org/10.1007/978-3-030-53370-0_24
Download citation
DOI: https://doi.org/10.1007/978-3-030-53370-0_24
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-53369-4
Online ISBN: 978-3-030-53370-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)