
Abstract
Emergency general surgery patients are a unique subset of patients with higher rates of postoperative complications, mortality, re-admissions, and care discontinuity. Institutional cultural norms and poor operating room communication can be improved with a surgical safety checklist and team huddle strategies. A unique communication tool encouraged any member of the operative team to request a huddle for any patient safety concern in order to improve intraoperative communication.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Overview of Emergency General Surgery
The American Association for the Surgery of Trauma and the American College of Surgeons Committee on Trauma defined emergency general surgery (EGS) as a field in 2003. In the United States, EGS constitutes 7% of all hospital admissions and 850,000 EGS operations are performed every year [1, 2]. A recent study from the National Inpatient Sample defined seven emergency general surgery procedures, which account for 80% of the operative EGS burden [3]. These seven procedures include partial colectomy, small bowel resection, cholecystectomy, peptic ulcer disease, lysis of adhesions, appendectomy, and laparotomy. EGS patients are a unique subset of patients with higher rates of postoperative complications, mortality, re-admissions, and care discontinuity (Fig. 15.1) [4].

Summary of emergency general surgery outcomes. (Reference: PMID: 29657721)
Case Study
Case #1
A 70-year-old male presented to the emergency department (ED) with complaints of abdominal pain for 48 hours. A CT scan was obtained in the ED, which showed free air and fluid likely due to a small bowel perforation. The emergency general surgery (EGS) team was consulted. Upon evaluation, the patient was in septic shock with peritonitis on physical exam. The patient was taken to the operating room (OR) urgently for an exploratory laparotomy. A safety pause that included all of the team members in the operating room (surgery, anesthesia, scrub, circulator) was conducted before the surgical incision. The team was unable to tell whether the patient had received pre-operative antibiotics in the ED or not. A decision was therefore made to administer antibiotics. A laparotomy was performed and there was significant contamination of the abdomen due to a small bowel perforation. The patient continued to be hemodynamically unstable with escalating vasopressor requirements. This was not communicated clearly between the surgery and the anesthesia team. A bowel resection and anastomosis was performed. The patient received 4 units of packed red blood cells and 2 units of Fresh Frozen Plasma (FFP), even though blood loss was noted to be minimal by the surgery team. At the end of the surgery, the patient had improved clinically from a hemodynamic standpoint, but still had metabolic acidosis and a base deficit. It was determined that the patient needed to go to the intensive care unit (ICU) postoperatively. However, the circulating nurse did not anticipate this and had requested a floor bed instead of an ICU bed. The team waited in the OR for the next 60 minutes while an ICU bed was arranged, and the patient was then transferred to the ICU.
Analysis:
There was a lack of communication between the ED team and OR team regarding pre-operative antibiotics. Then the patient’s hemodynamic instability was attributed to blood loss and the surgery and anesthesia teams did not discuss the need for blood transfusions. The surgery team did not communicate the patient’s postoperative disposition to the circulating nurse causing a delay in transfer to the ICU.
Case #2
The EGS service was consulted on a patient with choledocholithiasis for cholecystectomy during hospital admission. The patient had already undergone an endoscopic retrograde cholangiopancreatography by the gastroenterology team, which revealed multiple stones in the common bile duct. The patient was evaluated and the surgery team recommended a cholecystectomy. An appropriate sign out was performed between the medicine and surgery team before proceeding to the operating room. This included discussion of the need for any additional work-up for pre-op risk stratification, timing of surgery to determine NPO status, and if and when prophylactic anticoagulation should be held. In the operating room, during the safety pause, the possibility of conversion to an open surgery was discussed as the patient had a history of a previous hysterectomy and right colectomy. The surgery team discussed the necessary surgical instruments and retractors that would be needed in the event of an open operation. The circulating nurse made arrangements for the open cholecystectomy tray to be in the operating room. The team also discussed that the patient will be transferring to the surgery service postoperatively and a bed request for a bed on the surgery floor was established. Intraoperatively, there were significant adhesions and the critical view of safety for laparoscopic cholecystectomy could not be obtained and the decision to convert to an open operation was made. The surgery team communicated this with the anesthesia team. All the necessary equipment for an open cholecystectomy was in the room. After the conclusion of the operation, the patient was extubated and transferred to the recovery area. The patient went to the surgical floor postoperatively.
Analysis:
Inpatient consultations require coordination and communication between the primary service and the EGS team for pre-op risk stratification, NPO status, and prophylactic anticoagulation. The surgery team discussed the plan for conversion to an open operation early and all the necessary equipment was present in the room. The disposition of the patient postoperatively was clarified and necessary arrangements were made.
Discussion of the Topic Including Human Factors
Institutional cultural norms and infrequent communication between the team members in the operating room can compromise a patient’s safety in the operating room [5]. Implementation of the World Health Organization Surgical Safety Checklist (WHO SSC) has improved multidisciplinary communication practices and reduced morbidity and mortality in surgical settings [6,7,8]. This concept is borrowed from principles studied in the airline industry. The role of the checklist is to improve the completion of critical tasks, which have the potential of increasing risk or be life threatening if missed, at points where the detection of missed task is still possible [8]. The WHO Surgical Safety Checklist has three components to it. The first part occurs before the induction of anesthesia and is initiated by the anesthesia team and includes confirmation of the patient’s identity, procedure, and consent and site marking. The second part occurs before skin incision and is initiated by the surgery team. It focuses on introduction of all team members by name and role, patient’s identity, procedure and site of incision, and prophylactic antibiotics. The surgery, anesthesia, and nursing teams voice any anticipated critical events at this stage. The third part occurs before the patient leaves the operating room and is initiated by the nursing team and includes confirmation of the name of the procedure, completion of count, and specimen labeling [9]. The WHO SCC should be implemented 100% of the time in the operating room.
In addition to the checklist tools, team huddle strategies in which everyone on the team pauses and focuses their attention on a common task has been shown to improve communication between the different team members [10]. None of these tools had previously been examined or tailored to the need of EGS.
Approximately 3 million patients are admitted to US hospitals each year for EGS diagnoses [2, 11]. EGS patients are a unique surgical population who are at higher risk of morbidity and mortality. Patients who undergo an EGS operation are more likely to die compared to patients who have the same operation on an elective basis [12,13,14]. Approximately 50% of the patients undergoing emergency general surgery develop a postoperative complication [15]. Additionally, 15% of the patients are readmitted to the hospital within 30 days of their index operation [16]. Identification of the seven procedures, which account for 80% of procedures, deaths, complications, and costs has been vital in establishing EGS benchmarks [3]. This work has enabled us to understand the factors causing high morbidity and mortality in EGS patients and develop interventions to improve them. We conducted a retrospective cohort study of all adult patients who underwent EGS at two tertiary academic hospitals using the American College of Surgeons-National Surgical Quality Improvement Project database. We demonstrated that emergency general surgery is independently associated with high rates of intraoperative blood product transfusion. EGS patients were twice as likely to receive high-intraoperative pRBC use and three times more likely to receive high-intraoperative FFP use [12]. This work enabled us to identify modifiable factors contributing to the excess morbidity in EGS patients.
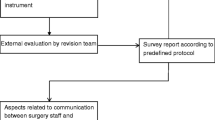
Based on this work, our division developed an evidence-based surgical safety tool aimed at encouraging the use of huddle strategies focused on modifiable factors unique to the EGS surgical subspecialty. The EGS communication tool works as an adjunct to the WHO SCC. Our communication tool was created through three phases: (1) identification of modifiable huddle points, (2) pilot testing, and (3) implementation of the tool in the OR. After demonstrating the feasibility of the EGS communication tool, we implemented it into all the operating rooms at our institution, and it is physically posted on the OR wall next to the WHO SCC in each OR [17] (Fig. 15.2).

The EGS communication tool (Reference: PMID 29907223)
In our practice, just before the surgical incision, in addition to the use of the standard WHO SCC, the EGS team acknowledges if the case is classified as an EGS procedure and verbalizes the anticipated postoperative disposition of the patient. Additionally, all the team members are encouraged to call a team huddle to discuss any concerns at any time. Use of the EGS communication tool in case #1 could have potentially prevented unnecessary blood transfusion in the patient by prompting the surgery and anesthesia team to have a conversation regarding the need for blood transfusion. Additionally, even though the postoperative disposition might have been obvious to the surgery team, this was not translated to the OR circulating nurse. Discussing the potential postoperative disposition of the patient at the beginning of the case would have prevented the delay in transfer to the ICU. Future work will identify the long-term effects of this tool implementation on EGS patient morbidity and mortality.
Lessons Learned
-
EGS patients are a vulnerable patient population. It is important to recognize that EGS patients are at increased risk of morbidity and mortality compared to patients undergoing the same operation on an elective basis.
-
An EGS communication tool can potentially improve intraoperative communication and patient safety in this population.
References
Becher RD, Davis KA, Rotondo MF, Coimbra R. Ongoing evolution of emergency general surgery as a surgical subspecialty. J Am Coll Surg. 2018;226:194–200. https://doi.org/10.1016/j.jamcollsurg.2017.10.014.
Gale SC, Shafi S, Dombrovskiy VY, Arumugam D, Crystal JS. The public health burden of emergency general surgery in the United States: a 10-year analysis of the Nationwide Inpatient Sample—2001 to 2010. J Trauma Acute Care Surg. 2014;77:202–8. https://doi.org/10.1097/TA.0000000000000362.
Scott JW, et al. Use of National Burden to define operative emergency general surgery. JAMA Surg. 2016;151:e160480. https://doi.org/10.1001/jamasurg.2016.0480.
Lyu HG, Najjar P, Havens JM. Past, present, and future of emergency general surgery in the USA. Acute Med Surg. 2018;5:119–22. https://doi.org/10.1002/ams2.327.
Kim FJ, et al. Current issues in patient safety in surgery: a review. Patient Saf Surg. 2015;9:26. https://doi.org/10.1186/s13037-015-0067-4.
Russ S, et al. Measuring variation in use of the WHO surgical safety checklist in the operating room: a multicenter prospective cross-sectional study. J Am Coll Surg. 2015;220:1–11.e14. https://doi.org/10.1016/j.jamcollsurg.2014.09.021.
Treadwell JR, Lucas S, Tsou AY. Surgical checklists: a systematic review of impacts and implementation. BMJ Qual Saf. 2014;23:299–318. https://doi.org/10.1136/bmjqs-2012-001797.
Haynes AB, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009;360:491–9. https://doi.org/10.1056/NEJMsa0810119.
Weiser TG, et al. Perspectives in quality: designing the WHO Surgical Safety Checklist. Int J Qual Health Care. 2010;22:365–70. https://doi.org/10.1093/intqhc/mzq039.
Glymph DC, et al. Healthcare utilizing deliberate discussion linking events (HUDDLE): a systematic review. AANA J. 2015;83:183–8.
Havens JM, et al. Explaining the excess morbidity of emergency general surgery: packed red blood cell and fresh frozen plasma transfusion practices are associated with major complications in nonmassively transfused patients. Am J Surg. 2016;211:656–663 e654. https://doi.org/10.1016/j.amjsurg.2015.11.031.
Havens JM, et al. The excess morbidity and mortality of emergency general surgery. J Trauma Acute Care Surg. 2015;78:306–11. https://doi.org/10.1097/TA.0000000000000517.
Ingraham AM, et al. Comparison of hospital performance in nonemergency versus emergency colorectal operations at 142 hospitals. J Am Coll Surg. 2010;210:155–65. https://doi.org/10.1016/j.jamcollsurg.2009.10.016.
Ingraham AM, Cohen ME, Raval MV, Ko CY, Nathens AB. Comparison of hospital performance in emergency versus elective general surgery operations at 198 hospitals. J Am Coll Surg. 2011;212:20–28.e21. https://doi.org/10.1016/j.jamcollsurg.2010.09.026.
Patel SS, et al. Elective versus emergency surgery for ulcerative colitis: a National Surgical Quality Improvement Program analysis. Am J Surg. 2013;205:333–7, discussion 337–338. https://doi.org/10.1016/j.amjsurg.2012.10.014.
Havens JM, et al. Defining rates and risk factors for readmissions following emergency general surgery. JAMA Surg. 2016;151:330–6. https://doi.org/10.1001/jamasurg.2015.4056.
Columbus AB, et al. An evidence-based intraoperative communication tool for emergency general surgery: a pilot study. J Surg Res. 2018;228:281–9. https://doi.org/10.1016/j.jss.2018.03.007.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kisat, M., Salim, A. (2020). Identifying Opportunities to Improve Processes in Emergency General Surgery. In: Cohen, T.N., Ley, E.J., Gewertz, B.L. (eds) Human Factors in Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-53127-0_15
Download citation
DOI: https://doi.org/10.1007/978-3-030-53127-0_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-53126-3
Online ISBN: 978-3-030-53127-0
eBook Packages: MedicineMedicine (R0)