
Abstract
After Botulinum injections and dermal fillers, laser and light assisted hair removal is the third most common non-surgical cosmetic procedure requested worldwide, with the global market set to reach $1.5 billion by 2025. The procedure is routinely performed throughout the world and has been demonstrated to be a safe and effective method of epilation of dark hairs, in all skin types.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Photoepilation
- Laser hair removal
- Permanent hair reduction
- Long-lasting hair removal
- Light-assisted hair removal
Introduction
Cultural norms in many countries dictate that excessive or visible hair on certain areas of the body is problematic at worst and unattractive at best. With a global hair removal market predicted to grow to $1.5 billion by 2025 [1], the drive to rid ourselves of facial and body hair shows no signs of abating.
Laser and light-assisted hair removal is increasingly considered the treatment of choice for long term reduction of unwanted hair. In 1997, the FDA approved the use of the first laser for cosmetic hair reduction, and since then, it has been widely used in clinical practice and is considered to be a safe and effective alternative to other methods of hair removal. Despite this, a 2009 Cochrane Review concluded that the lack of high-quality studies meant that data were insufficient to support long-term hair clearance from laser and IPL [2].
Although initially promoted as a means of achieving permanent hair removal for all skin types, many clinicians have revised this claim and now hold more realistic expectations. Depending on factors such as the colour, texture and location of the hair, as well as a patient’s skin type and hormonal status, it is now generally accepted that complete hair removal may not be achieved. Rather, the absence of hair growth in a 12-month period is classed as “permanent hair reduction ” with any regrowth generally being lighter in colour, finer in texture and reduced in number.
The Ruby laser was the first laser to be demonstrated in 1960. Although some early studies looked at using lasers on the skin to remove tattoos, it wasn’t until 1996 that Grossman et al. showed that the Ruby laser could be used for successful long-term hair reduction for cosmetic applications. Since then, long-pulsed Alexandrite, Diode, and Nd:YAG lasers have all been cultivated for use in hair removal. In the late 1990s, the first Intense Pulsed Light (IPL) system was introduced, and since then countless other IPL systems have come to market, and these Intense Light Sources (ILS) are also commonly used for hair removal.
Mode of Action
Most lasers and light sources use the principle of Selective Photothermolysis, which describes how light can be delivered to the skin, such that it can selectively destroy certain biological targets, whilst avoiding damage to the surrounding areas. In order for long-term hair loss to occur, the cells that make up the hair follicle must be irreversibly damaged. Following this damage to the follicle, the cells responsible for hair growth are destroyed and long-term hair reduction is achieved. This damage to the hair follicle can be achieved using laser or light systems due to the absorption of light by the chromophore melanin, which is present in the hair shaft and skin.
In order to achieve this damage, the light must be delivered over a time period matching the approximate Thermal Relaxation Time (TRT), or Cooling Time, of the target. In the case of the hair, the TRT is of the order of 10–100 ms, so for laser hair removal, long-pulsed lasers (rather than Q-Switched lasers) are used.
Light of the correct pulse duration (approximately tens of milliseconds), is directed at the skin and absorbed by the melanin in the hair shaft producing heat (photothermal reaction). This heat is conducted down the shaft and outwards into the surrounding follicle—the hair is in fact acting as an ‘intermediary’ for the transmission of heat into the follicle. The hair must therefore always be present in the follicle for laser hair removal to work—hair that has been plucked or waxed or otherwise removed from the follicle is not suitable for treatment.
If the heating effect is sufficient, the follicular cells within the matrix and hair bulge that are responsible for re-growth are damaged to the extent that re-growth is inhibited and long term hair reduction is achieved.
This can be summarized as follows:
-
1.
The light is selectively absorbed by the melanin within the hair shaft.
-
2.
This light causes the hair to heat rapidly and conducts heat to the follicle and the neighbouring cells.
-
3.
The cells responsible for re-growth of the hair are heated and damaged, resulting in either the complete destruction of the hair or a transition to a finer, fairer hair.
-
4.
New hair growth appears as surrounding hairs enter the anagen (growing) phase.
-
5.
New hair growth is treated and the percentage of re-growth decreases with each subsequent treatment.
When considering the mechanisms involved using light sources for hair removal, it is crucial to consider the effect of wavelength selection. In order to effectively remove hair with lasers or light it is necessary to target the melanin contained within the hair shaft. Hair lacking in melanin (i.e. grey or white hair) will show limited light absorption and heat production, so it is therefore difficult to treat this type of hair with any laser or light system. According to the principle of Selective Photothermolysis , to target the pigment in hair it is necessary to use a wavelength that will be selectively absorbed by melanin. The ideal wavelength should be readily absorbed in melanin but not well absorbed in other chromophores such as water or blood.
The commonly used hair removal lasers all use wavelengths within the ‘Optical Window for Melanin’ which stretches from approximately 650–1200 nm. This region contains wavelengths which are readily absorbed by melanin, but avoids the main absorption peaks of blood, minimizing the possibility of vascular damage, and avoiding the longer infrared wavelengths that will cause heating of water present in the tissue.
In order for hair to be treated without damaging the surrounding tissue, Laser and IPL hair removal relies on the absorption of light by the melanin contained in the hair shaft in preference to absorption by melanin in the skin. As it is usual for melanin to exist in the epidermis, at the junction between the epidermis and the dermis, within the dermis, as well as within the hair, the process can become quite complex. It is essential however, that the hair is darker than the skin for preferential absorption to occur. The best results will normally be seen for people with dark hair and fair skin. The treatment is effective when the hair follicle reaches a temperature high enough to destroy the follicle whilst the epidermis remains below the damage threshold temperature.
Cooling the skin before, during and after treatment can reduce damage to the epidermis. Thermal damage can occur if skin temperatures reach more than 45 °C [3], so cooling the epidermis allows the use of higher fluences without increasing the risk of complications. Common cooling methods include ice packs, cold gel, forced air cooling, contact cooling or cryogen sprays.
Hair Structure
The hair follicles (bulb, papilla and surrounding connective tissue) develop before birth and cannot be replaced if they die. The total number of hair follicles for an adult human is estimated to be at least five million (with one million of these on the head).
Hair is made of keratin and nourished by blood supply from dermal papilla, with the hair epithelium being continuous with epidermis. The hair shaft grows from matrix cells within the hair bulb, but epithelial stem cells are also contained with the hair bulge, at the junction of the erector pili muscle.
A cross-section of a terminal hair consists of:
-
1.
Cuticle: the outermost layer, which is thin and colourless
-
2.
Cortex: the middle layer which accounts for greatest proportion of hair shaft
-
3.
Medulla: the central portion of the hair shaft which contains the hair pigment
Hair can be classified into two major types:
-
Terminal hairs are thick, long and pigmented with melanin
-
Vellus hairs are small in diameter, short and often non-pigmented
It is generally terminal hair that causes the greatest cosmetic concern, as fine vellus hair is often not immediately visible. Vellus hairs can be converted to terminal hairs by hormones (as happens during the onset of puberty) or by mechanical stimulation of the hair, such as that which arises from plucking the hair. Plucking, threading and waxing of unwanted hair should therefore be discouraged.
Hair Growth Cycle
Every hair has a cycle of growth—in fact it has a cycle of growing, resting and shedding. Not all of the hairs on our body are in the same stage at the same time. The three phases of growth are Anagen, Catagen and Telogen.
-
1.
Anagen —the stage at which hairs are in active growth and when melanin synthesis occurs. At this stage, melanocyte stem cells located in the bulge start to produce melanosomes which give the hair shaft its colour [4]. In addition, anagen hairs are attached to the papilla and at maximum depth within the dermis.
-
2.
Catagen —the stage at which hair growth is arrested but the hair continues to be nourished from the papilla
-
3.
Telogen —the stage at which hair growth ceases altogether, the hair detaches from the papilla and contracts to almost one-third its original depth. The hair then falls out and the process begins once more with the early anagen phase.
Probably the most important phase for laser or light assisted hair removal is anagen, as the hair is connected to, and nourished by the papilla, which is still relatively close to the surface. The hair follicle is also comparatively richer in melanin at this phase of growth. It therefore makes it easier to deposit sufficient energy into the hair shaft, the papilla and the hair bulb to cause permanent damage which will delay or prevent future hair re-growth. It is because of the need to treat hair in this early anagen phase that several treatments are always required to successfully target an entire anatomical area.
The duration of the anagen phase varies greatly depending upon age, season, anatomic region, sex and genetic disposition, and can be as long as 6 years on the scalp, with 80–90% of hair in the anagen phase. The catagen phase is relatively constant for most body sites, at around 3 weeks, whereas the telogen phase usually lasts approximately 3 months. Hair in the catagen or telogen phase is thought to be less susceptible to the effects of the light. This explains why legs or backs, which have only about 20% of hair in the anagen phase at any time, may take some time to show long term results as the majority of the hair is not actively growing at any one time.
In addition, the hair cycle is under the influence of a number of hormones: oestrogens, testosterone, adrenal glucocorticoids, prolactin and growth hormone. Testosterone and its active metabolite, dihydrotestosterone (present in conditions such as Polycystic Ovaries) exerts the strongest effect. Most people seeking hair removal generally are in good health but excess hair growth can also result from many inherited syndromes and it is useful to be aware of such cases.
Lasers and Light Sources Used for Photoepilation
The key properties of the light required for successful photo-epilation are:
-
Wavelength
-
Pulse duration
-
Fluence
Wavelength
The method utilized to heat the hair follicle relies on the absorption of light by the chromophore melanin. There are five different laser/light sources that are commonly used for hair removal. They all deliver ‘long-pulses’ in the millisecond range for a photothermal effect. They are:
-
1.
Ruby laser (694 nm)
-
2.
Alexandrite laser (755 nm)
-
3.
Diode laser (various wavelengths, usually 810 nm or 920 nm)
-
4.
Nd:YAG laser (1064 nm)
-
5.
IPL or ILS sources (filtered broadband light, typically 620–1200 nm)
Lasers at the shorter end of the wavelength spectrum show enhanced melanin absorption, making them particularly effective for the treatment of finer, lighter hairs. However, the high melanin affinity means that these shorter wavelengths are more likely to interact with pigment within the skin, and they are therefore not suitable for the treatment of skin of colour.
Fluence
The fluence , also known as Energy Density , is a measure of the amount of energy delivered in a given area, and is measured in Joules per centimeter square (J/cm2). In order to achieve destruction of the hair follicle, the fluence must be sufficient to obtain temperatures high enough to damage the follicular stem cells. For a fixed energy, fluence can be increased by using smaller spot sizes, but this will impact on treatment times and effective penetration depths.
The fluence required to achieve follicular damage is largely determined from experiment and will often vary significantly depending upon various factors. The skin type and the colour of hair are major factors in determining a suitable (safe but effective) fluence. However, there are also variations due to the parameters of a particular system, in general, systems with longer wavelengths (and reduced melanin affinity) require much higher fluences to achieve the same clinical results as those with shorter wavelengths.
Pulse Duration
The pulse duration (sometimes known as pulse width) represents the on-time of the light pulse. According to the Theory of Selective Photothermolysis, the pulse duration of the laser should match the Thermal Relaxation Time (TRT) of the target. The Thermal Relaxation Time is defined as the time taken for an object to lose 50% of its induced thermal energy to surrounding tissues through thermal diffusion. For a hair, the TRT is approximately 40–100 milliseconds [5], so lasers/light sources using pulse durations of this order can efficiently heat the hair follicle whilst the epidermis conducts heat to surrounding tissue.
Thicker hairs have longer TRT and can therefore be treated effectively with longer pulse durations, however, very fine hairs will need shorter pulses in order to achieve high peak temperatures within the follicle. Keeping all else equal, reducing pulse durations will make treatments more effective (and more aggressive), whilst increasing pulse durations will reduce peak powers delivered, therefore making treatments safer for skin of colour.
Hair Removal Lasers and Light Sources
Ruby Lasers
The ruby laser at 694 nm was the first selective laser to be used for hair removal. At the shorter end of the wavelength range, melanin absorption is high, resulting in effective heating of the hair follicle, but also resulting in undesirable heating of the melanin within the skin. Multiple studies have shown an increased incidence of side effects with this wavelength, such as superficial burns or pigment disruption [6, 7]. For this reason, the Ruby laser is only suitable for Fitzpatrick skin types 1 and 2.
Technological difficulties with long-pulsed Ruby lasers (the inefficient lasing process results in high operating temperatures within the laser cavity) mean that high repetition rates and high energies are difficult to reliably achieve, which has limited their use as hair removal systems in recent years.
Alexandrite Lasers
At 755 nm, the Alexandrite is often the preferred choice for the treatment of lighter skin types. The high melanin absorption means that it can effectively treat even fine and fair hairs (although some melanin is always required within the hair shaft, so blonde or white hair will not respond to any laser or light treatment). Short pulse durations are achievable with Alex lasers, increasing efficacy, however, they are not suitable for the treatment of skin types 5 and 6, and should be used with extreme caution in skin type 4.
Diode Lasers
Diode lasers are increasingly popular due to their ability to treat a wide range of skin types (1 to 5). They were also the first lasers to be used for in-motion or ‘pain-free’ treatments, and are delivered to the skin directly, via a laser handpiece. Some diode systems struggle to deliver sufficient energy in short pulse durations, which may affect the efficacy of the treatment of finer hairs.
Neodymium YAG Lasers
The long pulsed Nd:YAG laser has the longest wavelength (1064 nm) of all the lasers commonly used for hair removal and as such shows a decreased affinity for absorption in the epidermal melanin. This reduced absorption results in less skin heating in comparison to other hair removal laser systems. Therefore there is a lower associated risk of epidermal damage and the Nd:YAG is considered to be the safest laser for skin of colour, especially for the treatment of skin type VI. The reduced melanin absorption also means that skin penetration depths are relatively high. This enables the laser energy to easily reach the hair bulb and bulge region and cause lethal follicular damage, resulting in long-lasting hair reduction, however this increased penetration can make treatment more painful than with other laser systems, and results can be limited on fine and fair hair.
Intense Light Sources
Intense Light Sources (ILS) , often known as Intense Pulsed Light (IPL) are now perhaps the most common method of light-assisted hair removal on the high-street. Their relative simplicity means that they are generally lower priced than lasers, and the ability to use filters to target additional skin chromophores mean that these can be very versatile systems, also being used for the treatment of superficial vascular lesions and rosacea, lentigines and photo-damaged skin (see Chap. 9 for further details).
ILS are generally comprised of a Xenon flashlamp which produces a wide spectrum of wavelengths ranging from ultra violet to near infrared. The output therefore requires some form of filtration, and for hair removal treatments, a cut-off filter is usually employed to remove all wavelengths below approximately 650 nm. This results in an emitted wavelength range from about 650 nm to 1200 nm. These wavelengths are readily absorbed in melanin but avoid the main absorption peaks of blood, therefore avoiding the possibility of vascular damage.
The treatment outcomes are very dependent on pulse duration and peak powers achievable, and there is a wide range of pulsing profiles available from different systems, which are not always easy to decipher from the manufacturers’ specifications. This means there tends to be much more variation in technical specification and price with IPL systems than is commonly seen with lasers, with a resultant variation in treatment outcomes.
A comparison of different devices for LHR is shown in Table 4.1.
Pre-Treatment Preparation and Precautions
Prior to treatment, each patient should undergo a thorough consultation, informed consent should be obtained, and a test patch should be carried out. During the consultation a full medical history will be taken and the treatment will be fully explained. Generally, the following circumstances would contraindicate treatment:
Contraindications
-
Recently UV-exposed or tanned skin (real or fake, including tanning injections)
-
Skin pigmentation problems such as melasma (in or near the treatment area)
-
A history of keloid scarring
-
Pregnancy/Breastfeeding
-
Severely photosensitive skin or photosensitising conditions such as porphyria
-
Epilepsy within the last 12 months
-
Skin Cancer or other malignant disease
-
Any active inflammatory skin condition e.g. eczema, psoriasis, Herpes Simplex in the treatment area
-
Healing disorders such as those caused by Diabetes Mellitus, connective tissue disease (e.g. lupus), radiation therapy or chemotherapy
-
Patients with unrealistic expectations, or those who are unlikely to follow post treatment guidelines
-
Do not treat over any tattoos, semi-permanent make-up or moles.
-
Use of St John’s Wort, minocycline or amiodarone in the past month
-
Use of Isotretinoin (Roaccutane) or any drugs for Photodynamic Therapy (PDT) in the previous 6 months
-
Use of topical retinoids such as Tretinoin, (Retin-A, Aknemycin Plus,) Isotretinoin (Isotrexin), Adapalene (Differin) in the last 2 weeks on the area to be treated
-
Use of high dose systemic (oral or injectable) steroids in the past month
-
Use of topical steroids in the past week (in or near the treatment area)
After a medical history is obtained it is important to also:
-
Assess the condition to be treated. For example, hair thickness and colour. If there is a possibility of an underlying endocrine disorder, then explain that the cause of the hair growth is not being treated, so maintenance treatments may be necessary.
-
Show examples to the patient of the likely results of treatment. Answer any questions the patient has regarding treatment and make sure the patient has realistic expectations of the outcome of the treatment. The patient should be informed that 100% clearance can not be guaranteed and results may not be permanent, and the effectiveness of treatment is related to skin/hair type.
-
Explain that treatment efficacy is related to patient skin and hair colour so results may vary. Dark hair with light skin responds best, whilst white, blonde and red hair rarely responds.
-
Ensure the patient knows that multiple treatments will be required because hair grows in cycles and can only be treated effectively in the growing phase. Explain that alternative methods of hair removal exist, include waxing, shaving, threading and depilatory creams, but prior to laser/IPL hair removal, the hair must be shaven.
-
Explain the treatment process to the patient. Discuss pain control and aftercare. Possible side effects of treatment should be discussed in detail.
-
Explain the hazards of Intense Pulsed Light/laser radiation and the need for appropriate goggles to be worn at all times.
-
Carefully record the patient’s reaction to sun exposure and assign skin type using the Fitzpatrick Scale.
-
Provide estimates of the total cost of treatment and methods of payment.
-
Photograph the treatment site for the patient’s records.
-
Answer any questions that the patient might have and record patient comments. Each patient should be provided with written information about the treatment
-
Ask the patient to read, sign and date the consent form if he/she has understood its contents. Countersign the consent form and give the patient a copy if requested.
Informed Consent
Prior to any examination, skin test patch or treatment, every patient is required to provide informed consent to LASER or ILS treatment. Patients need sufficient information concerning the benefits, risks, alternative treatments, expected outcomes and fees before they can decide whether to give their consent. If the patient is not offered as much information as they reasonably need to make their decision, and in language they can understand, their consent may not be valid. If the patient is suitable for treatment, continue with patch-testing. A patch test must be performed on or as near as possible to the area prior to any course of treatment.
Test-Patching
Once eligibility has been established, it is recommended that a test patch is completed for all patients before treatment commences. The aim of the test patch is to determine the most effective treatment parameters for the patient’s skin and hair type and lesion type, and to judge how the skin will respond to treatment. The test patch should always be carried out in a small area, in or near the area for treatment, and if other body sites are to be treated subsequently, then a test patch must be carried out in the new treatment area.
Select the lowest recommended settings, taking into account skin type, body site and density and thickness of hair in the area. Observe the skin response and patient’s tolerance to treatment, settings can be increased if an appropriate skin reaction is not observed, but keep in mind that reactions may not always be obvious on test patch. The presence of follicular erythema and oedema, and a smell of burning hair are good indicators that the treatment settings are suitable. Very pronounced erythema is not expected following most hair removal treatments and may be a sign of over-treatment. Typically, a test patch consists of a few shots only. Complete patient records, noting observed skin and patient reaction, sign, date and schedule an appointment for treatment.
An appropriate amount of time should pass before proceeding with treatment—this might be as short as 24 h, but more often will be approximately 7 days, especially for darker skin types. Subsequent treatment intervals will typically be around 4–8 weeks.
Typical Skin Reactions and End Points of Treatment
Patients should be made aware of likely effects following treatment including:
-
Redness and/or tenderness of the treatment area.
-
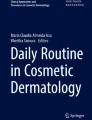
Itchiness, mild irritation or swelling of the follicles which normally subsides within 48 h (see Fig. 4.1)
-
Hair should fall out within approximately 2 weeks
-
Some hair may regrow thinner and lighter than before
-
Shaving of the area may be restarted as soon as hair growth becomes apparent.
-
Folliculitis and/or histamine reactions can occur on occasion, and can be reduced by increased personal hygiene (new razor, fresh towels and face cloths) and by using anti-inflammatory/antibacterial and skin-calming lotions

Pronounced follicular erythema following treatment with a low-fluence, high rep-rate Alexandrite laser (Motus AY, DEKA lasers). Although not always seen, when present, it’s a good indicator of a successful treatment
Epilation Laser Medical Indications
-
Hirsutism
-
Polycystic Ovarian Syndrome
-
Limb Prosthesis in Amputees
-
Reduction of Body Odour
-
Pilonidal Sinus
-
Hidradenitis Suppurativa
-
Dissecting Folliculitis of the Scalp
-
Trichostasis Spinulosa
-
Pseudofolliculitis Barbae
-
Hairy Intraoral flaps
-
Transgender laser hair removal and Genital Gender reaffirming surgery
-
Peristomal hair growth
-
Hair restoration surgery to redesign frontal hairline in women
Hirsuitism
Hirsutism is often defined as excessive hair in an androgen dependent distribution e.g. beard area, lower abdomen in females. The prevalence of hirsutism varies from 5% to 32% in different population groups. It is recognized that hirsutism is a distressing symptom with a negative impact on psychosocial aspects and quality of life [8].
It is important to recognize patient’s perceptions of the severity of their hirsutism can differ greatly from doctors, nurses and the wider population. One study showed a significant reduction in the hirsutism related Disability Life Quality Index score (DLQI ) after treatment with an Alexandrite laser. The same study also showed that LHR led to an increase in social and interpersonal activities [8].
Many women choose LHR over alternative methods of hair removal for axillary, legs, bikini line hair. Alternative methods such as depilatory creams and electrolysis are becoming less popular. Depilatory creams can often cause an irritant reaction and plucking can result in folliculitis and post inflammatory pigmentation. Waxing can cause similar problems. Electrolysis is an effective method, and can lead to permanent hair reduction, but the process is slow and painful, and results and side effect profile are very operator dependent.
On the basis of this, LHR has become a popular option, despite the fact that original reports of permanent hair removal have now been revised to longer periods of remission and delayed hair growth (Fig. 4.2). However, many people, especially women with facial hirsutism, find that having several months of remission is more acceptable than daily treatments such as shaving or plucking.

Female patient before and after nine treatments with Long pulsed ND Yag 20–30 J/cm2 12 mm spot size 3 ms pulse duration for Laser Hair reduction
Non androgen dependent hair growth in areas such as the forearms or back is termed hypertrichosis. Patients with hirsutism require a full evaluation to exclude treatable causes of androgen excess, including some tumours. Other causes of hypertrichosis include drug induced hair growth, congenital hair and hair growth from grafted donor sites [9].
There are also an increasing number of men who are having laser hair removal in areas such as the chest and back. It is becoming increasingly commonplace for men, particularly under 30s to remove hair from their body. 19% of men claim they feel expected to remove hair from their torso [10].
Poly Cystic Ovarian Syndrome
Polycystic ovarian syndrome (PCOS) is a condition affecting 4–8% of women of reproductive age. Characteristic features include polycystic ovaries, menstrual disturbances and hyperandrogenism. Up to 70% of women with hyperandrogenism present with hirsutism. Suppression of ovarian androgen production using oral contraceptives, androgen receptor blockers are often tried to reduce hirsutism but results are variable [11].
Laser hair removal has been a significant advance of treatment for these individuals as medical treatment has provided limited results. Compared with idiopathic hirsutism, PCOS patients require more treatment sessions and ‘top up’ sessions to achieve hair reduction.
Limb Prosthetics in Amputees
Hair growth at the residual limb-prosthetic interface in individuals with traumatic lower limb amputation can lead to a folliculitis. This can cause significant irritation and limit the time the prosthesis can be worn. Laser hair removal in this area can lead to reduction in the folliculitis and improve symptoms which can lead to a significant improvement in quality of life due to the improved comfort in wearing a prosthesis (Fig. 4.3) [12]. Studies have shown a marked decrease in hair density and disease exacerbations at follow-up were noted after Alexandrite LHR for below knee amputation stump [13].

Lower leg amputee presenting with folliculitis which showed marked improvement after 4 Alexandrite laser treatments 755 nm 18 mm 3 ms 16–20 J/cm2
Use of Laser Hair Removal in the Axillae to Reduce Body Odour
Body odour, in particular axillary odour, is perceived as unpleasant by many cultures worldwide. Reducing or eliminating body odour is an important part of the daily personal care routine for many individuals. Over the last decade, removal of underarm hair has become more commonplace for hygiene as well as aesthetic reasons [14].
Hair Follicle Pathology
A number of dermatological conditions associated with hair follicular pathology as the primary dysfunction have been treated with LHR. These include chronic inflammatory disorders such as pilonidal sinus disease (PSD), hidradenitis suppurativa (HS), dissecting folliculitis, and pseudofolliculitis barbae (PFB). These diseases are thought to result from occlusion, rupture, and inflammation of the follicular unit [15]. Laser-induced damage and epilation of hair follicles has led to a significant improvement in these disorders, which is helpful where current medical treatment options often have limited results with frequent relapses.
Pilonidal Sinus
A pilonidal sinus (PNS) or sacrococcygeal fistula is a cyst or abscess on the natal cleft of the buttocks that often contains hair and skin debris (Fig. 4.4).

Pilonidal sinus in male before and after 7 treatments with Alexandrite laser 755 nm 18 mm spot size, 3 ms pulse duration 16–20 J/cm2
PNS of the natal cleft is painful and causes significant disability. Complete surgical excision of the sinus tract is the standard treatment but there is significant risk of recurrence. Due to the association with excessive hair in sacrococcygeal region, laser epilation has been reported to be beneficial as an additional treatment to surgery [16,17,18,19,20,21,22,23,24].
The conventional treatment of PNS involve use of depilatory creams, but with this recurrence is a common due to recurring hair growth at the site. However, with five to six sessions of LHR, chances of recurrence reduce [25, 26]. Diode, Nd:YAG and Alexandrite lasers as well as IPL systems have been used in different studies in this indication and all of these devices have shown promising results [27].
Jain et al. [28] treated three patients of PNS but the disease recurred. The patients were then treated with a combination of CO2 laser with 1064 nm Nd:YAG laser with the aim of deroofing with CO2 laser and use of long pulse Nd:YAG laser to destroy hair follicles in five patients with PNS with follow up of up to 3 years. Long Pulse Nd:YAG was repeated in all patients at a 2–3 month gap for four to five times. During this time, no recurrence was observed.
Relapse rates are high if fewer than four sessions are used; one study with mean of 2.7 sessions reported a recurrence rate of 13.3% over a follow-up period of 4.4 years [23]. LHR in PSD is usually well tolerated and without any major complications. A long-term follow-up study reported no recurrence in 86.6% of patients following LHR over a period of 5–7 years [13].
Hidradenitis Suppurativa (HS)
HS is a chronic disabling disorder, often affecting the axillae, inframammary areas and groin, characterized by exacerbations, recurrence, and progression despite medical and surgical treatment. There has been increasing evidence for a primary follicular pathogenesis, which has led to LHR being used in the treatment of HS.
Significant improvement of HS has been reported in this condition after LHR with diode and Nd:YAG lasers, and IPL devices [29,30,31].
Long pulse Nd:YAG laser has deeper tissue penetration than other lasers and due to this, has been considered to be the preferred laser for this indication. Histopathological changes in 20 patients of HS were followed using biopsy specimens obtained at specified intervals before and after treatment and this correlated with the degree of clinical improvement in them after treatment with a long-pulsed 1064-nm Nd:YAG laser. Patients received two treatments to an affected area; Laser parameters ranged from 25 to 50 J/cm2 with a 10-mm spot size and a 20- to 35-ms pulse duration. Double pulse stacking was used at the first treatment, and triple at the second treatment on all inflammatory lesions. By 1 month, inflammation had decreased and broken hair shafts were noted. At 2 months, the investigators found scarring, fibrosis, and minimal inflammation. As measured by a Lesion Area and Severity Index score modified for HS, a significant improvement of 32% in treated areas was noted 2 months after the second treatment [32].
Pseudofolliculitis Barbae
PFB is a common chronic disorder predominantly in those of African descent with tightly curled hairs curving back into the skin. Shaving is a predisposing factor because it results in sharp and short hairs, which re-enter the skin. LHR has been shown to be helpful by reducing the number and/or thickness of hair shafts. Greater than 50% improvement has been observed in long-standing PFB after LHR [33,34,35]. In PFB, LHR with Nd:YAG laser has been reported as a safe and effective option for reducing hair and subsequent papule formation. Papule counts performed 90 days after treatment in dark skins (type IV–VI) were significantly reduced in the laser-irradiated area as compared to the control [36]. Another study reported 56% mean reduction in PFB lesions after using three passes of Nd:YAG laser [37]. A low-fluence (12 J/cm2) laser treatment at 1064 nm at 5-week intervals also achieved significant temporary reduction in PFB on the neck which had been unresponsive to other treatments [38].
Dissecting Cellulitis
Dissecting cellulitis is an inflammatory condition of the scalp characterized by nodules, sinus tract formation, and scarring alopecia. A severe case of recalcitrant dissecting cellulitis of the scalp had no recurrence at 6-month follow-up after four treatment sessions of diode laser as monotherapy [39]. In addition, some patients have reported regrowth of terminal hairs in treatment sites, 1 year after initiating laser treatment [40].
Folliculitis Decalvans
Folliculitis decalvans (FD) is another inflammatory condition of the scalp characterized by follicular papules and pustules. It often leads to a scarring alopecia. The long pulse Nd:YAG laser was used in in several cases of FD with good results in a few studies [41,42,43].
Trichostasis Spinulosa
Trichostasis spinulosa is a disorder consisting of asymptomatic comedo-like lesions that contain keratin and multiple vellus hairs primarily on the face associated with dilated hair follicles. LHR therapy has been reported to be helpful, removing the hair responsible for the plugged appearance. The alexandrite laser has been reported as being effective [44, 45], with one study reporting no recurrence in 90% of the treated cases [46].
Hair-Bearing Skin Flaps and Grafts
Following surgical reconstruction hair-bearing skin flaps and grafts result in hair growth at sites where it is inappropriate. LHR has been used on the nose following basal cell carcinoma excision, after reconstruction in breast cancer, and other traumatic injuries requiring skin grafts [47, 48].
Hairy Intraoral Flaps
A variety of flaps used to reconstruct defects of the head and neck region following surgery for malignant disease contain hair follicles that may result in unwanted hair growth. This can lead to with irritation, pooling of saliva and trapping of food. Several lasers have been used to deal with this but the most common has been the long pulsed alexandrite laser [49]. The long pulsed Nd:YAG laser has also been used.
Shields et al. demonstrated that these lasers provided safe and effective treatment and improved patient quality of life following intraoral flap repair following excision of malignancy [50].
LHR is very difficult in such cases due to poor visibility and the bulky hand piece of laser in the confined oropharyngeal space. Marked symptom improvement was noted in a patient with reconstructed hypopharynx post laryngopharyngectomy using Alexandrite laser, with a 7-mm hand piece with 90° side-firing fiber-optic attachment passed through the lumen of a suspension laryngoscope [51].
Transgender Laser Hair Removal and Genital Gender Affirming Surgery
The trans gender community often desire hair removal and lasers provide an effective method of achieving this (Fig. 4.5).

Male to female gender reassignment patient. Alexandrite laser 755 nm. over 30 treatments 20 J/cm2–30 J/cm2 12 mm. In addition to eight electrolysis sessions
Genital gender affirming surgery (GAS) involves reconstruction of the genitals to match the patients identified sex. The use of hair-bearing flaps can result in postoperative intravaginal and intraurethral growth hair growth and associated complications [52, 53]. Electrolysis has been used for hair removal prior to GAS but LHR has been shown to be superior [54, 55]. It is best to wait 3 months after the last planned hair removal treatment before proceeding with surgery, in order to confirm that no further hair regrowth will occur [56].
Peristomal Hair Growth
Peristomal hair growth following an ileostomy can cause difficulty for adhesion of the stomal appliance to the skin. LHR has resulted in effective epilation, resulting in improved stoma appliance adhesion and reduced risk of trauma and infection [57, 58].
Redesign Frontal Hairline in Women in Hair Restoration Surgery
Hair transplantation in women for hairline correction can be associated with an unnatural appearance due to thicker donor hair from occipital region. LHR has been used as a nonsurgical method for revising hairline following hair transplantation in women. Study carried out by Park et al. [59], resulted in subjective improvement in 87.5% of the cases as well as significant reduction in hair diameter.
Complications of Hair Removal Laser Treatments and How to Treat and Avoid Them
Typical end points following hair removal treatment are usually restricted to mild erythema, peri-follicular swelling and smell of burning hair. Laser and light-assisted hair removal is generally a low-risk procedure and when complications do arise they are generally transient, with permanent sequalae being very uncommon. Good clinical practice and sensible precautionary measures can minimize this risk, and most importantly, it’s essential that patients are treated with the laser most appropriate for their skin type.
During the consultation procedures, it is important to be clear on possible risks of treatment. These are outlined below:
Burning, Blistering and Scarring
If inappropriate settings are used (fluence too high, incorrect wavelength for skin type etc.), cooling is not adequate or tanned skin is treated, then thermal damage can occur to the skin, presenting as pronounced erythema, grazing or even blistering (Figs. 4.6 and 4.7).

Adverse skin reactions due to excessive overlapping and incomplete removal of make-up. Figure courtesy Dr. Vishal Madan

Adverse skin reactions due to excessive overlapping and incomplete removal of make-up. Figure courtesy Dr. Vishal Madan
It is essential that any blisters or grazes which form following the treatment are not popped, picked, or scratched and the area kept clean and dry. Once the blister subsides, the skin may be dry and flaky, do not exfoliate and let the skin flake at its own speed. Sun avoidance is essential, and once the area has healed, a high-factor sunscreen should be applied daily for up to 12 months to reduce the risk of pigmentation changes occurring.
Generally IPL/Laser burns are superficial and will heal without issue, but if infection is suspected, immediate treatment is required to minimize the risk of scarring or permanent pigmentation change.
Pigmentation Changes
Hyper and hypo pigmentation may arise either following the presence of a burn or just occur spontaneously after treatment (Figs. 4.8, 4.9, and 4.10). Avoidance of sun exposure before and after treatment can lessen the risk of pigmentary changes occurring. Permanent pigmentary alteration is rare, but is more common in darker skins. The presence of melasma appears to increase the risk of post-inflammatory hyperpigmentation occurring, so facial hair removal should proceed with caution in patients with this condition, and pigment suppressants are recommended prior to treatment.

Transient hyperpigmentation following IPL treatment, due to presence of tan or inappropriate settings for skin type. Figure courtesy Dr. Vishal Madan

Pronounced skin reaction following treatment due to excessive fluence. Figure Courtesy Dr. Vishal Madan

Hypopigmentation on a skin type 2 following LHR. Figure courtesy Dr. Vishal Madan
Hyperpigmentation should be treated with daily use of sunscreen in the first instance. Topical products containing hydroquinone and retinoids can be used to expedite improvement.
Paradoxical Hypertrichosis
A rare but distressing adverse effect of laser hair removal is an increase in hair growth on, or adjacent to, the LASER or IPL treatment site (Fig. 4.11). This is called ‘paradoxical hair growth’ and is thought to affect 0.6–10% of all patients having treatment [60]. Paradoxical growth has been reported with all types of laser and IPL [61], and the aetiology is unclear. Many mechanisms have been proposed, including sub-therapeutic thermal injury affecting the follicular cycling so that terminal hair growth is induced whilst other studies indicate that it is the thermally-induced inflammatory response which induces activation of dormant hair follicles in untreated areas close to hirsute-treated areas [62]. Another hypothesis is that hair removal simply synchronizes the cycling of hairs growing within the laser treatment, thereby causing the overall hair density to appear to be greater [63].

Reactive hair growth on shoulder before and after five treatments with an Alexandrite laser
It is certainly the case that this affect appears to be more prevalent in patients of Mediterranean, Middle-Eastern and Asian descent (skin types 3 to 5 [64]), and one study reported that it was more common in patients suffering from underlying hormonal conditions such as Poly Cystic Ovarian Syndrome and associated ovarian hyperandrogenism [65]. It generally occurs when treating fine, vellus hair on the neck and jawline in women, but it has also been reported in men, usually on the back and shoulders, although it is unclear whether this predominance is simply due to those areas being treated more commonly in men than other body sites.
The increased hair growth can be treated with further laser/IPL treatments, with the use of higher laser fluences widely recommended. Wiley et al. [66] suggest actively cooling the neighbouring (non-treated) areas to prevent stimulation of the follicles by sub-therapeutic light. They also recommend double passing over the treatment area, although caution is advised with this method, especially when treating darker skin types.
Other Unusual Side Effects
Leukotrichia has been reported following treatment with IPL [67] and other lasers [68]. This seems to occur when fluences are used that are insufficient to damage the germinative hair follicle, but sufficient to damage the melanocytes either permanently or temporarily. It appears to be more common in patients who already have some white or grey hair.
Folliculitis can arise following treatment—this may be as a result of shaving the area prior to treatment, or may be due to the hair shaft burning and causing orificial oedema which may occlude the follicular canal.
Common Causes of Adverse Reactions
-
1.
Treating tanned or recently UV exposed skin—Perhaps the most common cause of unwanted skin reactions is treatment of tanned skin. Skin that has been recently exposed to UV, or self-tanning products, should not be treated, and exposure to UV should also be avoided for 4 weeks after treatment. Some lasers, such as the Nd:YAG or pain-free lasers, are less likely to cause problems when treating tanned skin. Nonetheless, lower fluences will have to be used, so general advice is to avoid tanning where possible, even with systems suitable for tanned skins.
In recent years, a number of tanning supplements have become available such as tanning injections, melonotan, tanning oral supplements and tanning nasal sprays. Many of these are unlicensed and untested, so although it’s probable that they will also increase the risk of epidermal damage, we do not know how long they will have an effect—some anecdotal evidence suggests tanning injections in particular can be very long-lasting. Their use is therefore a contraindication for LHR.
-
2.
Inappropriate wavelength selection—unwanted reaction incidence is higher when using shorter wavelengths, especially on darker skins. The Ruby and Alexandrite lasers are particularly inappropriate for use in darker skin types.
-
3.
Treating unshaven hair—reactions can occur when hair has not been shaved sufficiently. Although it can be useful for visualization for the hair to protrude from the follicle by a millimeter or so, if it is any longer than this, absorption by the hair shaft can cause frazzling of the hair and subsequent epidermal damage.
-
4.
Treating over thin skin—Settings should be reduced when treating over bony prominences or thin skin, for example, when treating the neck and décolleté, over shins or elderly patients.
-
5.
Treating thick, coarse hair—when treating over very concentrated target (for example pubic hair or facial hair in men) more absorption will occur, and settings will therefore need to be adjusted to account for this.
-
6.
Inadequate cooling—most hair removal systems will require some form of cooling. Some are built into the system, such as contact cooling handpieces or cryogen cooling, others recommend the use of separate devices such as forced air cooling or even just ice-packs. Too much cooling can limit efficacy but some cooling is generally recommended, especially when treating darker skin types.
Latest Advances
Pain-Free Hair Removal
A factor in many people’s decision not to continue with LHR is the discomfort associated with treatment, especially for those with thick, dense hair, or darker skin. Although different cooling methods are employed to protect the epidermis and lessen discomfort, the traditional single-shot method of treatment, delivers high fluences in one pulse, resulting in high-peak temperatures within the skin. This can make treatment uncomfortable, and even intolerable, for people with thick, dark hair.
In recent years a different technique, known variously as ‘in-motion’ or ‘high rep-rate’ method, has been introduced with the aim of offering effective, ‘pain-free’ treatment. These systems use a contact-cooling handpiece, delivering light at lower fluences than the traditional methods, but at very high repetition rates. Rather than stamping single shots over the treatment area, the light is administered by sliding the handpiece across the skin in a series of continuous circular or linear movements, aiming to pass several times over the same area. Delivering multiple passes over a given area (usually 100 cm2) in this fashion, causes cause gradual heating of the vital parts of the hair follicle, leading to its destruction with significantly less discomfort and with a very low incidence of side effects [69, 70]. These treatments are typically delivered with a Diode laser at a 800–810 nm wavelength, but more recently Alexandrite and Nd:YAG lasers with similar technology have also been launched on the market [69].
In general, more treatments may be required in pain-free modes, and many manufacturers suggest moving to standard emission for the final treatments for residual finer hair. Nonetheless, studies show that results are comparable to traditional lasers, with fewer side effects and high patient satisfaction [71].
Home-Use Devices
A number of laser/light sources are now available for home-use. These generally use diode or IPL technology and operate at fluences lower than those of professional devices. They usually have an in-built contact sensor to stop the system firing unless it is in contact with the skin, thereby making them eye safe and avoiding the requirement for safety eyewear [72]. However, it is more difficult to ensure that these systems are only used by people of appropriate skin type, or those without an active tan. The lack of training of the users means that there is also a real risk of people mis-judging skin type and therefore using inappropriate settings that may result either in reduced efficacy or unwanted skin reactions.
Several studies report hair reduction with light-based home use devices [73, 74], however, there is some evidence that the low fluences used are only damaging the hair follicles to the extent that the hair is moved into catagen or telogen phase, thus delaying regrowth rather than causing permanent hair reduction [75].
Case Studies

Case Study 1: A 29 year old lady, Fitzpatrick skin type 5 presented with coarse hair on her top lip, previously managed by threading. Before and after four treatments with Lumina IPL system (Lynton Lasers). Fluence 14–18 J/cm2. Note remaining hair is much finer.

Case Study 2: A 36 year old man requested hair removal for dense hair growth on his back. Before and after four treatments with Lumina IPL system (Lynton Lasers). Skin Type 2, Fluence 20–26 J/cm2. Note that in cases such as this, consideration is required to determine whereabouts on the arms to terminate treatment. In this case, the upper arms were treated every other treatment to avoid an abrupt change in growth. Due to the long hair growth cycle on the back, treatments should be spaced no less than 8 weeks apart.

Case Study 3: Facial hair removal in a 32 year old man, before and after six treatments with Lumina IPL system (Lynton Lasers). Skin Type 2, Fluence 20–26 J/cm2.

Case Study 4: A 27 year old woman presented for hair removal on her lower legs. This had preciously been managed with waxing, but had resulted in unsightly ingrowing hairs. Before and after nine treatments with Lumina IPL system (Lynton Lasers). Skin Type 4, Fluence 16–20 J/cm2, 4–5 pulses with a 40–50 ms delay. Note the improvement in in-grown hairs and skin tone.

Case Study 5:
A 36 year old woman was looking for a more effective, longer-lasting method for keeping her bikini line in check. She had previously tried shaving, waxing and sugaring and was only happy with the bikini line immediately after waxing or shaving. If shaved, she would have regrowth the following day, which would make the area itchy and uncomfortable. She found that waxing and sugaring provided a longer-lasting result, but the actual process was time consuming and painful. She would be happy with the results for a couple of weeks, but then suffered with ingrown hairs.
So her aim was to find a more permanent solution to maintain her bikini line—that wouldn’t result in ingrown hairs or a shaving rash.
She was treated with Alexandrite laser , 12 mm spot size commencing at 20 J with a pulse width of 3 ms.
Patient noted a 75% reduction in hair growth after six treatments and complete resolution of ingrown hair.
References
Global Laser Hair Removal Market Report, https://www.marketwatch.com/press-release/at-170-cagr-laser-hair-removal-market-size-set-to-register-15468-million-usd-by-the-end-of-2025-2019-05-08
Haedersdal M, Wulf HC. Evidence-based review of hair removal using lasers and light sources. J Eur Acad Dermatol Venereol. 2006;20(1):9–20.
Zandi H, Lui H. Long-term removal of unwanted hair using light. Derm Clinics. 2013;31:179.
Slominski A, et al. Hair Foolical Pigmentation. J Invest Dermatol. 2005;124(1):13–21.
Caerwyn Ash et al Mathematical modeling of the optimum pulse structure for safe and effective photo epilation using broadband pulsed light, Journal of applied clinical medical physics, volume 13, number 5, 2012.
Lanigan SW. Incidence of side effects after laser hair removal. J Am Acad Dermatol. 2003;49:882–6.
Lim SP, Lannigan S. A review of the adverse effects of laser hair removal. Lasers Med Sci. 2006;21:121–5.
Alizadeh N, Aryoubi S, Naghipour R, et al. Can laser treatment improve quality of life of hirsute women. Int J Womans Health. n.d.;2017(9):777–80.
Lanigan S. Lasers in dermatology. London: Springer; 2000. p. 87.
Mintel. 2014. “The only way is smooth: half of Britains men feel the pressure to remove or groom their body hair.” www.mitel.com . Accessed April 2015, 2015. www.mintel.com/press-centre/beauty-and-personal-care/the-only-way-is-smooth-half-of-britains-men-feel-the-pressure-to-remove-or-groom-their-body-hair.
Toosy S, Sodi R, Pappachan M. Lean polycystic ovary syndrome. J Diabetes Metabolic Disorders (Springer Nature). 2018;17:371.
Miletta NR, KIm S, Lezanski-Guida A, et al. Improving health related quality of life in wounded warriors: the promising benefits of laser hair removal to the residual limg-prosthetic ineterface. Dermatol Surg. 2016;42(10):1182–7.
Koch D, Pratsou P, Szczecinska W, Lanigan S, Abdullah A. The diverse application of laser hair removal therapy: a tertiary laser unit’s experience with less common indications and a literature overview. Lasers Med Sci. 2015;30:453–67.
Lanzalaco A, Vanoosthuyze K, Stark C. A comparative clinical Study of diferent hair removal procedures and their impact on asillary odor reduction in men. J Cosmet Dermatol. 2016;15:58–65.
Chicarilli ZN. Follicular occlusion triad: hidradenitis suppurativa, acne conglobata, and dissecting cellulitis of the scalp. Ann Plast Surg. 1987;18:230–4.
Schulze SM, Patel N, Hertzog D, Fares LG. 2nd Treatment of pilonidal disease with laser epilation. Am Surg. 2006;72:534–7.
Conroy FJ, Kandamany N, Mahaffey PJ. Laser depilation and hygiene: preventing recurrent pilonidal sinus disease. J Plast Reconstr Aesthet Surg. 2008;61:1069–72.
Benedetto AV, Lewis AT. Pilonidal sinus disease treated by depilation using an 800nm diode laser and review of the literature. Dermatol Surg. 2005;31:587–91.
Lavelle M, Jafri Z, Town G. Recurrent pilonidal sinus treated with epilation using a ruby laser. J Cosmet Laser Ther. 2002;4:45–7.
Downs AM, Palmer J. Laser hair removal for recurrent pilonidal sinus disease. J Cosmet Laser Ther. 2002;4:91.
Odili J, Gault D. Laser depilation of the natal cleft–an aid to healing the pilonidal sinus. Ann R Coll Surg Engl. 2002;84:29–32.
Landa N, Aller O, Landa-Gundin N, Torrontegui J, Azpiazu JL. Successful treatment of recurrent pilonidal sinus with laser epilation. Dermatol Surg. 2005;31:726–8.
Lukish JR, Kindelan T, Marmon LM, Pennington M, Norwood C. Laser epilation is a safe and effective therapy for teenagers with pilonidal disease. J Pediatr Surg. 2009;44:282–5.
Lukish JR, Kindelan T, Marmon LM, Pennington M, Norwood C. Laser epilation is a safe and effective therapy for teenagers with pilonidal disease. J Pediatr Surg. 2009;44:282–5.
Ghnnam WM, Hafez DM. Laser hair removal as adjunct to surgery for pilonidal sinus: our initial experience. J Cutan Aesthet Surg. 2011;4:192–5.
Ganjoo A. Laser hair reduction for pilonidal sinus-My experience. J Cutan Aesthet Surg. 2011;4:196.
Aleem S, Majid I. Unconventional uses of laser hair removal: a review. J Cutan Aesthet Surg. 2019;12(1):8–16.
Jain V, Jain A. Use of lasers for the management of refractory cases of hidradenitis suppurativa and pilonidal sinus. Cutan Aesthet Surg. 2012;5(3):190–2.
Tierney E, Mahmoud BH, Srivastava D, Ozog D, Kouba DJ. Treatment of surgical scars with nonablative fractional laser versus pulsed dye laser: a randomized controlled trial. Dermatol Surg. 2009;35:1172–80. [PubMed] [Google Scholar].
Highton L, Chan WY, Khwaja N, Laitung JK. Treatment of hidradenitis suppurativa with intense pulsed light: a prospective study. Plast Reconstr Surg. 2011;128:459–65.
Downs A. Smoothbeam laser treatment may help improve hidradenitis suppurativa but not hailey-hailey disease. J Cosmet Laser Ther. 2004;6:163–4.
Xu LY, Wright DR, Mahmoud BH, Ozog DM, Mehregan DA, Hamzavi IH. Histopathologic study of hidradenitis suppurativa following long-pulsed 1064-nm nd:YAG laser treatment. Arch Dermatol. 2011;147:21–8.
Yamauchi PS, Kelly AP, Lask GP. Treatment of pseudofolliculitis barbae with the diode laser. J Cutan Laser Ther. 1999;1:109–11. [PubMed] [Google Scholar].
Leheta TM. Comparative evaluation of long pulse Alexandrite laser and intense pulsed light systems for pseudofolliculitis barbae treatment with one year of follow up. Indian J Dermatol. 2009;54:364–8.
Smith EP, Winstanley D, Ross EV. Modified superlong pulse 810nm diode laser in the treatment of pseudofolliculitis barbae in skin types V and VI. Dermatol Surg. 2005;31:297–301.
Ross EV, Cooke LM, Overstreet KA, Buttolph GD, Blair MA. Treatment of pseudofolliculitis barbae in very dark skin with a long pulse nd:YAG laser. J Natl Med Assoc. 2002;94:888–93.
Rogers CJ, Glaser DA. Treatment of pseudofolliculitis barbae using the Q-switched nd:YAG laser with topical carbon suspension. Dermatol Surg. 2000;26:737–42.
Schulze R, Meehan KJ, Lopez A, Sweeney K, Winstanley D, Apruzzese W, et al. Low-fluence 1,064-nm laser hair reduction for pseudofolliculitis barbae in skin types IV, V, and VI. Dermatol Surg. 2009;35:98–107.
Boyd AS, Binhlam JQ. Use of an 800-nm pulsed-diode laser in the treatment of recalcitrant dissecting cellulitis of the scalp. Arch Dermatol. 2002;138:1291–3. [PubMed] [Google Scholar].
Krasner BD, Hamzavi FH, Murakawa GJ, Hamzavi IH. Dissecting cellulitis treated with the long-pulsed Nd:YAG Laser. Dermatol Surg. 2006;32:1039–44.
Parlette EC, Kroeger N, Ross EV. Nd:YAG laser treatment of recalcitrant folliculitis decalvans. Dermatol Surg. 2004;30: 1152–4. [PubMed] [Google Scholar].
Meesters AA, Van der Veen JP, Wolkerstorfer A. Long-term remission of folliculitis decalvans after treatment with the long-pulsed nd:YAG laser. J Dermatolog Treat. 2014;25:167–8.
Harowitz MR. Treatment of folliculitis decalvans with Nd: YAG laser. Surgical Cosmetic Dermatol. 2013;5:170–2.
Toosi S, Ehsani AH, Noormohammadpoor P, Esmaili N, Mirshams-Shahshahani M, Moineddin F. Treatment of trichostasis spinulosa with a 755-nm long-pulsed alexandrite laser. J Eur Acad Dermatol Venereol. 2010;24:470–3.
Badawi A, Kashmar M. Treatment of trichostasis spinulosa with 0.5-millisecond pulsed 755-nm Alexandrite laser. Lasers Med Sci. 2011;26:825–9.
Chavan DK, Chavan DD, Nikam BP, Kale MS, Jamale VP, Chavan SD. Efficacy of 800 nm diode laser to treat trichostasis spinulosa in Asian patients. Int J Trichol. 2018;10:21–3.
Moreno-Arias GA, Vilalta-Solsona A, Serra-Renom JM, Benito-Ruiz J, Ferrando J. Intense pulsed light for hairy grafts and flaps. Dermatol Surg. 2002;28:402–4.
Thomson KF, Sommer S, Sheehan-Dare RA. Terminal hair growth after full thickness skin graft: treatment with normal mode ruby laser. Lasers Surg Med. 2001;28:156–8.
Shim TN, Abdullah A, Lanigan S, Avery C. Hairy intraoral flap- an unusual indication for laser epilation. as series of 5 cases and review of the literature. Br J Oral Maxillofac Surg. 2011;49(7):50–2.
Shields BE, Moya MS, Bayon R, et al. A hairy siutation:laser hair removal after oral construction. Ann Otol Rhino Laryngol. 2018;127(3):205–8.
Toft K, Keller GS, Blackwell KE. Ectopic hair growth after flap reconstruction of the head and neck. Arch Facial Plast Surg. 2000;2:148–50.
Selvaggi G, Bellringer J. Gender reassignment surgery: an overview. Nat Rev Urol. 2011;8:274–82.
Bowman C, Goldberg JM. Care of the patient undergoing sex reassignment surgery. Int J Transgend. 2006;9:135–65.
Haedersdal M, Gøtzsche PC. Laser and photoepilation for unwanted hair growth. Cochrane Database Syst Rev. 2006:CD004684.
Görgü M, Aslan G, Aköz T, Erdoğan B. Comparison of alexandrite laser and electrolysis for hair removal. Dermatol Surg. 2000;26:37–41.
Zhang WR, Garrett GL, Arron ST, Garcia MM. Laser hair removal for genital gender affirming surgery. Transl Androl Urol. 2016;5:381–7.
Royston SL, Cole RP, Wright PA. Peristomal hair removal with an alexandrite laser. Colorectal Dis. 2013;15:1043–4. [PubMed] [Google Scholar.
Preston PW, Williams G, Abdullah A. Laser hair removal for peristomal skin. Clin Exp Dermatol. 2006;31:458.
Park HS, Kim JY, Choe YS, Han W, An JS, Seo KK. Alternative method for creating fine hairs with hair removal laser in hair transplantation for hairline correction. Ann Dermatol. 2015;27:21–5.
Desai S, Mahmoud BH, Bhatia AC, Hamzavi IH. Paradoxical hypertrichosis after laser therapy: a review. Dermatol Surg. 2010;36:291–8.
Moreno-Arias GA, Castelo-Branco C, Ferrando J. Side-effects after IPL photodepilation. Dermatol Surg. 2002;28(12):1131–4.
Town G, Bjerring P. Is paradoxical hair growth caused by low-level radiant exposure by home-use laser and intense pulsed light devices? J Cosmet Laser Ther. 2016;18(6):355–62.
Lolis MS, Marmur ES. Paradoxical effects of hair removal systems: a review. J Cosmet Dermatol. 2006;5:274–46.
Alajlan A, et al. Paradoxical hypertrichosis after laser epilation. J Am Acad Dermatol. 2005;53:85–8.
Moreno-Arias GA, Castel-Branco C, Ferrando J. Paradoxical effect after IPL photoepilation. Dermatol Surg. 2002;28:1013–6.
Willey A, Torrontegui J, Azpiazu J, et al. Hair stimulation following laser and intense pulsed light photo-epilation: review of 543 cases and ways to manage it. Lasers Surg Med. 2007;39:297–301.
Radmanesh M, Azar-Beig M, Abtahian A, Naderi AH. Burning, paradoxical hypertrichosis, leukotrichia and folliculitis are four major complications of intense pulsed light hair removal therapy. J Dermatolog Treat. 2008;19(6):360–3.
Hélou J, Soutou B, Jamous R, Tomb R. Novel adverse effects of laser-assisted axillary hair removal. Annales de Dermatologie et de Venereologie. 2009;136(6-7):495–500.
Removal of unwanted hair: efficacy, tolerability, and safety of long-pulsed 755-nm alexandrite laser equipped with a sapphire handpiece. Lasers Med Sci. 2018, https://doi.org/10.1007/s10103-018-2503-z
Braun M. Comparison of high-fluence, single-pass diode laser to low-fluence, multiple-pass diode laser for aser hair reduction with 18 months of follow up. J Drugs Dermatol. 2011;10:62–5.
Barolet D. Low fluence–high repetition rate diode laser hair removal 12-month evaluation: reducing pain and risks while keeping clinical efficacy. Lasers Surg Med. 44:227–81.
Town G, Ash C. Are home-use intense pulsed light (IPL) devices safe? Lasers Med Sci. 2010; https://doi.org/10.1007/s10103-010-0809-6.
Alster TS, Tanzi EL. Effect of a novel, low-energy pulsed light device for home-use hair removal. Dermatol Surg. 2009;35:483–9.
Emerson R, Town G. Hair removal with a novel, low fluence, home-use intense pulsed light device: preliminary Results. J Cosmet Laser Ther. 2009;11(2):98–105.
Roosen G, Westgate G, Philpott M, Berretty P, Nuijs T, Bjerring P. Temporary hair removal by low fluence photoepilation: histological study on biopsies and cultured human hair follicles. Lasers Surg Med. 2008;40:520–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Hills, S., Seukeran, D. (2020). Epilation Lasers. In: Madan, V. (eds) Practical Introduction to Laser Dermatology. Springer, Cham. https://doi.org/10.1007/978-3-030-46451-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-46451-6_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-46450-9
Online ISBN: 978-3-030-46451-6
eBook Packages: MedicineMedicine (R0)