
Abstract
While majority of previous research focus on reviewing mobile health (mHealth) apps targeting specific health domain, this paper provides a comparative systematic review of mHealth apps across multiple health domains with the aim of deconstructing the persuasive strategies employed and their implementation. Specifically, we targeted four health domains (i.e., physical activity and fitness, diet, emotional and mental health, and health assessment and healthcare). We retrieved a total of 639 apps from Google Play out of which 80 popular apps were extracted (20 apps in each category). Three expert reviewers coded the apps using 32 persuasive strategies (PSs) based on Persuasive System Design (PSD) Model and Cialdini’s Principles of Persuasion. Overall, out of the 80 mHealth apps reviewed, personalization is the most commonly employed PS (n = 77), followed by surface credibility (n = 69), trustworthiness (n = 66) and self-monitoring (n = 64). How the apps are implemented varies depending on the domain. Based on our findings, we offer suggestions for designing mHealth apps to improve their persuasiveness.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
The proliferation of smartphones has made it possible to share millions of life-enriching mobile apps to billions of people worldwide [1]. Many of these apps are health-related and help in managing chronic or mild health conditions [2], supporting the adoption of a healthy lifestyle or promoting healthy behaviours [3]. Specifically, these mobile health (mHealth) apps are effective in promoting physical activity [3, 4], weight management [5], dietary interventions [3], disease management [2], mental well-being [6], and so on. However, for behaviour change to occur, developers of mHealth apps need to employ persuasive principles or strategies [7, 8].
While previous research has conducted literature review on the persuasiveness of mHealth apps [9, 10] or review apps targeting specific health domain [11,12,13,14], existing work has not conducted a comparative systematic review of mHealth apps (on Google Play or App Store) across multiple health domains (such as fitness, diet, mental health, etc.) at the same time to the best of our knowledge.
To fill this gap, we conduct a comparative systematic review of 80 mHealth apps across four different categories with each category having 20 popular apps. The categories include physical activity and fitness, diet, emotional and mental health, and health assessment and healthcare. The goal of this review is to identify and compare the persuasive strategies employed by the apps and how they were implemented. Three expert reviewers coded the apps using 32 persuasive strategies (PSs) based on the Persuasive System Design (PSD) Model [7] and Cialdini’s Principles of Persuasion [8].
Our findings show that for the Physical Activity and Fitness category, personalization (n = 20) and trustworthiness (n = 20) PSs are the most commonly employed, followed by self-monitoring (n = 19). For the Diet category, personalization (n = 20), commitment/consistency (n = 20) and suggestion (n = 20) PSs emerged as the most commonly employed, followed by reminders (n = 19). Moreover, under the Emotional and Mental Health category, personalization (n = 19) and surface credibility (n = 19) PSs are the most commonly employed, followed by liking (n = 17). For the Health Assessment and Healthcare category, personalization (n = 18) is the most commonly employed PS, followed by surface credibility (n = 16), and self-monitoring (n = 15). Overall, out of the 80 mHealth apps reviewed, personalization emerged as the most commonly employed PS (n = 77), followed by surface credibility (n = 69), trustworthiness (n = 66), and self-monitoring (n = 64). Based on our findings, we offer suggestions for designing mHealth apps to improve their persuasiveness.
2 Related Work
Existing research has evaluated mobile health apps to determine the persuasive features they provide. For instance, Langrial et al. [15] conducted a review to identify the persuasive features in twelve mobile apps for personal well-being using the PSD model. Similarly, Chang et al. [6] evaluated twelve mobile apps for mental well-being using the 28 principles of the PSD model. They reviewed the apps based on user acceptance of mobile services, mobile intervention design, and persuasive design. Furthermore, Azar et al. [16] assessed the intervention strategies present in 23 weight management mobile apps using four behavioural theories or models, which are the health belief model, transtheoretical model, theory of reasoned action/planned behaviour, and the social cognitive or social learning theory. They also assessed the persuasive nature of the applications using the Fogg Behavioural Model (FBM).
Rather than targeting a specific health domain, our work provides a comparative systematic review of 80 mHealth apps across multiple health domains using both the PSD model and Cialdini’s Principles of Persuasion. Specifically, we targeted four health domains: physical activity and fitness, diet, emotional and mental health, and health assessment and healthcare to uncover new insights and enrich the literature.
3 Methodology
In this section, we discussed the app selection criteria and coding process.
3.1 Selection of MHealth Apps
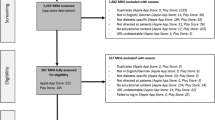
We developed a Python script to automate the app selection process which involves two stages. First, we searched for health-related apps that are free or free with in-app purchases on Google Play using keywords appropriate for each category, as defined in Table 1. We filtered our search results by selecting apps that belong to at least one of the following relevant Google Play groups: health and fitness, medical, social, and lifestyle. Second, we selected 20 most popular apps after sorting the total apps in each category in descending order of number of installations, followed by average ratings and number of reviews. Table 2 shows the apps summary per category based on number of installations, average ratings and number of reviews. We ensure that none of the 20 apps in a category is repeated in another category. In other words, we selected 80 unique apps in total for coding and analysis. 92.5% of the 80 apps were updated in 2019.
3.2 Coding and Analysis of Selected Apps
In the coding phase, we identified the persuasive strategies (PSs) employed in designing each of the 80 mHealth apps including how the strategies were implemented using the PSD model [7] and Cialdini’s Principles of Persuasion [8]. Both frameworks have been widely used in deconstructing persuasive technologies over the years. From the PSD model, we used all the PSs under the primary task support, dialogue support, system credibility support and social support categories for coding purposes. From the Cialdini’s Principles of Persuasion, we selected four out of the six available PSs since two strategies (i.e., authority and liking) already exist in the PSD model. Table 3 shows the 32 persuasive strategies and their categories.
Figure 1 describes the coding process. Three expert reviewers installed the apps on their Android smartphones and used the app features to perform various tasks while taking note of the PSs and how they were implemented in their coding sheets. Afterwards, the reviewers discussed the information captured on the coding sheets.

The Process of Coding Apps
4 Results
In this section, we present the apps review results. We discussed the persuasive strategies identified in the apps and how they were implemented.
4.1 Persuasive Strategies Employed by Apps in Various Health Domains
Figure 2 shows the primary task support PSs employed by apps in the four health domains or categories (i.e., Physical Activity and Fitness, Diet, Emotional and Mental Health, and Health Assessment and Healthcare). Of the seven primary task support PSs, personalization is the most commonly employed strategy in all four categories, followed by self-monitoring. Specifically, for Physical Activity and Fitness category, personalization is the most commonly employed strategy (n = 20), followed by self-monitoring (n = 19) and reduction (n = 18). For Diet category, personalization is the most commonly employed strategy (n = 20), followed by self-monitoring (n = 19) and reduction (n = 19). However, for Emotional and Mental Health category, personalization is the most commonly implemented strategy (n = 19), followed by self-monitoring (n = 11) and tunneling (n = 11). For Health Assessment and Healthcare category, personalization is the most commonly implemented strategy (n = 18), followed by self-monitoring (n = 15) and tunneling (n = 11).

Primary Task Support PSs employed in Physical Activity and Fitness, Diet, Emotional and Mental Health, and Health Assessment and Healthcare categories
Furthermore, Fig. 3 shows the dialogue support PSs employed by apps in the four categories. For Physical Activity and Fitness category, reminders (n = 17) is the most commonly employed, followed by suggestion (n = 15) and liking (n = 12). However, for Diet category, suggestion (n = 20) is the most commonly employed, followed by reminders (n = 19) and liking (n = 10). For Emotional and Mental Health category, liking (n = 17) is the most commonly employed, followed by reminders (n = 14) and suggestion (n = 9). Finally, for Health Assessment and Healthcare category, liking (n = 13) is the most commonly employed, followed by suggestion (n = 12) and social role (n = 9).

Dialogue Support PSs employed in Physical Activity and Fitness, Diet, Emotional and Mental Health, and Health Assessment and Healthcare categories
Moreover, Fig. 4 revealed the system credibility PSs employed by apps in the four categories. For Physical Activity and Fitness category, trustworthiness (n = 20) is the most commonly employed PS, followed by real-world feel (n = 17), surface credibility (n = 16) and expertise (n = 16). For Diet category, trustworthiness (n = 19) and expertise (n = 19) are the most commonly employed PSs, followed by surface credibility (n = 18). For Emotional and Mental Health category, surface credibility (n = 19) is the most commonly employed, followed by trustworthiness (n = 13) and real-world feel (n = 12). Finally, for Health Assessment and Healthcare category, surface credibility (n = 16) is the most commonly employed, followed by real-world feel (n = 15) and trustworthiness (n = 14).

System Credibility Support PSs employed in Physical Activity and Fitness, Diet, Emotional and Mental Health, and Health Assessment and Healthcare categories
Furthermore, Fig. 5 shows the social support PSs employed by apps in the four categories. For Physical Activity and Fitness category, competition is most commonly employed (n = 10), followed by social learning (n = 5) and recognition (n = 5). For Diet category, normative influence is most commonly employed (n = 8), followed by social learning (n = 7) and competition (n = 7). For Emotional and Mental Health category, only social facilitation (n = 1) and social learning (n = 1) were employed. Interestingly, for Health Assessment and Healthcare category, none of the apps employed the social support PSs. Also, none of the four categories employed the cooperation PS.

Social Support PSs employed in Physical Activity and Fitness, Diet, Emotional and Mental Health, and Health Assessment and Healthcare categories
Finally, Fig. 6 revealed the Cialdini’s Principles of Persuasion employed by apps in the four categories. For commitment/consistency (n = 18) is the most commonly employed, followed by reciprocity (n = 9) and social proof (n = 6). For Diet category, commitment/consistency (n = 20) is the most commonly employed, followed by social proof (n = 10) and scarcity (n = 7). For Emotional and Mental Health category, reciprocity (n = 6) is the most commonly employed, followed by commitment/consistency (n = 5) and social proof (n = 3). Interestingly, for Health Assessment and Healthcare category, commitment/consistency (n = 4) is the only strategy employed.

Cialdini’s Principles of Persuasion employed in Physical Activity and Fitness, Diet, Emotional and Mental Health, and Health Assessment and Healthcare categories
4.2 Persuasive Strategies Implementation in the Apps
Table 4 presents how the various persuasive strategies are implemented in the apps.
4.3 Persuasive Strategies and App Effectiveness
For each category, we performed a bivariate Pearson Correlation (using SPSS version 25) to determine whether a relationship exists between the number of persuasive strategies implemented in an app and the perceived app effectiveness (based on average ratings). We also performed the same computation for all apps combined. The results, as shown in Table 5, revealed that for each category, there is no correlation (though not significant) between the number of strategies employed and app effectiveness. Overall, no relationship exists between the number of persuasive strategies employed in an app and its effectiveness.
5 Discussion
We conducted a comparative systematic review of 80 mHealth apps across four categories (see Table 1) with the aim of deconstructing the persuasive strategies employed and their implementation, and then provide suggestions on how the persuasiveness of mHealth apps can be further improved using the insights.
5.1 Persuasive Strategies Employed Overall
Out of the 80 mHealth apps reviewed, personalization emerged as the most commonly employed PS (n = 77), followed by surface credibility (n = 69), trustworthiness (n = 66), self-monitoring (n = 64), real-world feel (n = 59), reminders (n = 57), suggestion (n = 56), liking (n = 52), expertise (n = 52), commitment/consistency (n = 47), reduction (n = 45) and tunneling (n = 40). Other strategies were employed by less than 23 apps. Research has shown that the personalization strategy was effective in promoting health-related behaviours [9, 17] which, in turn, explains why 96% of the total apps implemented it.
5.2 Persuasive Strategies for Physical Activity
Based on our findings, all the reviewed apps under the physical activity and fitness category employed both the personalization and trustworthiness PSs. Moreover, 95% of the apps employed self-monitoring, 90% employed commitment/consistency and reduction, 85% employed reminders and real-world feel, 80% employed surface credibility and expertise, and 75% employed suggestion. 65% or less employed other strategies. Existing research supported our findings. For instance, self-monitoring and reminders were found to be commonly implemented in physical activity apps by [18, 19]. Another study found that users are more persuaded by physical activity apps that implement primary task support and dialogue support PSs [20], including goal-setting [21] which correlates well with the commitment/consistency strategy [22].
5.3 Persuasive Strategies for Healthy Eating
Our findings revealed that personalization, commitment/consistency, and suggestion PSs were implemented in all the reviewed apps under the Diet category. 95% of the apps employed self-monitoring, reduction, reminders, expertise and trustworthiness PSs, while 90% and 75% of the apps employed surface credibility and real-world feel respectively. This shows that most mHealth apps rely on a mix of these strategies to promote healthy diets among users.
5.4 Persuasive Strategies for Emotional and Mental Health
Our findings showed that 95% of the reviewed apps employed the personalization and surface credibility PSs under emotional and mental health category, while 85% and 70% implemented the liking and reminders strategies respectively. This outcome is corroborated by previous research on persuasive mental health apps which shows that primary task support PSs are the most commonly implemented, followed by system credibility and dialogue support strategies [6].
5.5 Persuasive Strategies for Health Assessment and Healthcare Delivery
In health assessment and healthcare category, 90% and 80% of the reviewed apps implemented the personalization and surface credibility PSs respectively. However, 75% of the apps implemented real-world feel and self-monitoring, while 70% implemented the trustworthiness PS. Only 60% and 45% of the apps employed suggestions and social role PSs which are equally important to provide medical advice and facilitate doctor-patient conversations.
5.6 Comparative Analysis
Table 6 shows the three most dominant persuasive strategies and the least dominant strategies for each of the four categories.
In a world where precision medicine has become prominent, personalization is unarguably critical to tailor healthcare (such as treatment and prevention of diseases or ailments) to individual patient. It is therefore not surprising personalization is the most dominant in mHealth apps. Surface credibility is important for emotional and mental health, as well as health assessment and healthcare delivery, due to the sensitive nature of these issues. Users tend to be skeptical and critical of apps in these areas and that makes it really necessary that the apps must be professionally looking, responsive, and with visually appealing interface to be adopted. Any app that lacks these attributes may be deemed incredible. Hence, surface credibility is a popular strategy in these domains. Furthermore, self-monitoring is dominant in physical activity and fitness apps since technological advancements in these areas have made it possible to automatically track movements (while walking, running, cycling, etc.) in real-time through various sensors on smartphones or wearable devices. Same applies to health assessment and healthcare delivery apps, where various sensors can be used to track vital signs, such as heart rate, blood pressure, temperature, etc. However, it is difficult to monitor food intake and dietary levels in diet apps unless users supply this information manually, and that explains why self-monitoring is not among the top in the domain of dieting.
5.7 Design Suggestions
Research has shown that social interaction can motivate individuals to achieve their target behaviours [18, 23, 24]. However, only 21% of the 80 mHealth apps employed at least one of the social support PSs. Designers of persuasive mHealth apps should consider implementing social support strategies in their apps by providing features allowing users to: (1) invite their friends to perform the target behaviour together, (2) compare their performance with others performing the same activities, (3) be publicly recognized after achieving important milestones that move them closer to their health goals, (4) learn from other users’ experiences or success stories, (5) team up with (or join) other users in performing a common healthy activity.
Designers should also introduce praise in their apps such that users are praised or appreciated for every milestone achieved even if it seems small or trivial.
Finally, the relationship between the number of persuasive strategies employed in persuasive app design and their effectiveness is an open area of research. Although many existing persuasive apps employ multiple strategies, this analysis suggests that there is no relationship between the number of strategies employed in persuasive app for health design and app effectiveness as operationalized by the app rating. Hence, persuasive app developers could employ fewer strategies and still be effective. This will reduce the app complexity and reduce overall cognitive load on the user. This is in line with Orji et al. [25] which shows that persuasive apps employing a single strategy can be effective.
6 Conclusion and Future Work
We conducted a comparative systematic review of 80 mHealth apps across four categories with each category having 20 popular apps. The categories include physical activity and fitness, diet, emotional and mental health, and health assessment and healthcare. The goal of this review is to identify and compare the PSs employed and how they were implemented, and then offer design suggestions to improve persuasiveness of mHealth apps.
Our future work will be a broader review involving additional mHealth apps from both Google Play and App Store, spanning more health domains. In addition to PSs in PSD and Cialdini’s Principles of Persuasion frameworks, others such as punishment would be considered. We also plan to investigate the effectiveness of apps employing multiple strategies in comparison to those employing a single strategy in actual app.
References
Gu, T.: Insights into the World’s 3.2 Billion Smartphone Users, the Devices They Use & the Mobile Games They Play (2019). https://newzoo.com/insights/articles/newzoos-global-mobile-market-report-insights-into-the-worlds-3-2-billion-smartphone-users-the-devices-they-use-the-mobile-games-they-play/
Martínez-Pérez, B., et al.: Mobile health applications for the most prevalent conditions by the world health organization: review and analysis. J. Med. Internet Res. 15, e120 (2013)
Dute, D.J., et al.: Using mobile apps to promote a healthy lifestyle among adolescents and students. JMIR mHealth uHealth. 4, e39 (2016)
Dallinga, J.M., et al.: App use, physical activity and healthy lifestyle: a cross sectional study. BMC Public Health 15, 1–9 (2015)
Rivera, J., et al.: Mobile apps for weight management. JMIR mHealth 4, e87 (2016)
Chang, T.-R., Kaasinen, E., Kaipainen, K.: Persuasive design in mobile applications for mental well-being: multidisciplinary expert review. In: Godara, B., Nikita, K.S. (eds.) MobiHealth 2012. LNICST, vol. 61, pp. 154–162. Springer, Heidelberg (2013). https://doi.org/10.1007/978-3-642-37893-5_18
Harri, O., Marja, H.: Persuasive systems design: key issues, process model, and system features. Commun. Assoc. Inf. Syst. 24, 96 (2009)
Cialdini, R.B.: Harnessing the science of persuasion. Harvard Bus. Rev. 79(9), 72–81 (2001)
Nurcan, A., Duygu, F.: Use of Persuasion Strategies in Mobile Health Applications. Springer, Cham (2018). https://doi.org/10.1007/978-3-319-73135-3_2
Pinzon, O.E., Iyengar, M.S.: Persuasive technology and mobile health: a systematic review. In: Persuasive Technology, pp. 45–48, Linköping, Sweden (2012)
Meedya, S., Sheikh, M.K., Win, K.T., Halcomb, E.: Evaluation of breastfeeding mobile health applications based on the persuasive system design model. In: Oinas-Kukkonen, H., Win, K.T., Karapanos, E., Karppinen, P., Kyza, E. (eds.) PERSUASIVE 2019. LNCS, vol. 11433, pp. 189–201. Springer, Cham (2019). https://doi.org/10.1007/978-3-030-17287-9_16
Geuens, J., et al.: A review of persuasive principles in mobile apps for chronic arthritis patients: opportunities for improvement. JMIR mHealth 4, e118 (2016)
Thach, K.S., Phan, T.P.N.: Persuasive design principles in mental health apps. In: IEEE-RIVF International Conference on Computer and Communication Technology, pp. 1–6 (2019)
Tiffany, B., et al.: Mobile apps for oral health promotion. JMIR 6, e11432 (2018)
Langrial, S., et al.: Native mobile applications for personal well-being: a persuasive systems design evaluation. In: PACIS 2012 Proceedings (2012)
Azar, K.M., et al.: Mobile applications for weight management. Am. J. Prev. Med. 45, 583–589 (2013)
Orji, R., Moffatt, K.: Persuasive technology for health and wellness: state-of-the-art and emerging trends. Health Inform. J. 24, 66–91 (2018)
Matthews, J., et al.: Persuasive technology in mobile applications promoting physical activity: a systematic review. J. Med. Syst. 40, 1–13 (2016)
Wang, Y., et al.: Persuasive technology in reducing prolonged sedentary behavior at work: a systematic review. Smart Heal. 7–8, 19–30 (2018)
Bartlett, Y.K., et al.: Using persuasive technology to increase physical activity in people with chronic obstructive pulmonary disease by encouraging regular walking. J. Med. Internet Res. 19, 124 (2017)
Consolvo, S., et al.: Goal-setting considerations for persuasive technologies that encourage physical activity. In: ACM International Conference Proceeding Series, p. 350 (2009)
Cham, S., Algashami, A., McAlaney, J., Stefanidis, A., Phalp, K., Ali, R.: Goal setting for persuasive information systems: five reference checklists. In: Oinas-Kukkonen, H., Win, K.T., Karapanos, E., Karppinen, P., Kyza, E. (eds.) PERSUASIVE 2019. LNCS, vol. 11433, pp. 237–253. Springer, Cham (2019). https://doi.org/10.1007/978-3-030-17287-9_20
Orji, R., et al.: Socially-driven persuasive health intervention design: competition, social comparison, and cooperation. Health Inform. J. 25, 1451–1484 (2018)
Orji, R.: Why are persuasive strategies effective? Exploring the strengths and weaknesses of socially-oriented persuasive strategies. In: de Vries, P.W., Oinas-Kukkonen, H., Siemons, L., Beerlage-de Jong, N., van Gemert-Pijnen, L. (eds.) PERSUASIVE 2017. LNCS, vol. 10171, pp. 253–266. Springer, Cham (2017). https://doi.org/10.1007/978-3-319-55134-0_20
Orji, R., et al.: Improving the efficacy of games for change using personalization models. ACM Trans. Comput. Interact. 24, 32 (2017)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this paper

Cite this paper
Oyebode, O., Ndulue, C., Alhasani, M., Orji, R. (2020). Persuasive Mobile Apps for Health and Wellness: A Comparative Systematic Review. In: Gram-Hansen, S., Jonasen, T., Midden, C. (eds) Persuasive Technology. Designing for Future Change. PERSUASIVE 2020. Lecture Notes in Computer Science(), vol 12064. Springer, Cham. https://doi.org/10.1007/978-3-030-45712-9_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-45712-9_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-45711-2
Online ISBN: 978-3-030-45712-9
eBook Packages: Computer ScienceComputer Science (R0)