
Abstract
Many common misconceptions about simulated/ standardized patient (SP) methodology have emerged over the past few decades. While some of these ideas may appear to be humorous or benign, others can have an undesireable impact on a simulation session. Collected from the reports of a wide range of SP educators (SPEs) from around the world, we address these misperceptions in an evidence-based manner. Topics include authenticity, acting, general considerations for working with SPs, training, assessment, the Association of Standardized Patient Educators (ASPE) Standards of Best Practice (SOBP) (Lewis et al., Adv Simul 2(1):10, 2017) and the role of SPEs. We draw on evidence and practice for clarifying these misunderstandings and provide strategies that can be shared with stakeholders such as faculty, other SPEs or SPs, to promote the implementation of SP methodology in a knowledgeable, safe and effective manner.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- SP methodology
- Misconceptions
- Evidence
- SP educators
- Standards of Practice
- Simulated Patient
- Standardized Patient
- Strategies
- Practice
You have a message waiting for you on your phone. One of the faculty members you work with has called to request an SP for a class on giving bad news. The SP is needed in 2 hours. All you can imagine is that this person must think that you store your SPs in a dark room somewhere, already pre-trained for this role, waiting until they’re needed. You smile to yourself as you think of it as the “put money into a vending machine and out pops a ready-to-consume SP” misconception.
Introduction
A misconception is “a belief or an idea that is not based on correct information” [1]. Over the past 50 years, many common misconceptions about simulated/standardized patient (SP) methodology have emerged. While some of these ideas may appear to be humorous or benign, others can have an undesirable impact on a simulation session. We have collected these reports from an international community of SP educators (SPEs) in interviews for this book and through personal correspondence, as well as drawing on our own experiences. These misperceptions relate to many topics including authenticity, acting, general considerations for working with SPs, training, assessment, the Association of Standardized Patient Educators (ASPE) Standards of Best Practice (SOBP) [2] and the role of SPEs. We draw on evidence and practice to provide strategies for SPEs to address these misconceptions with stakeholders and promote the implementation of SP methodology in an informed, safe and effective manner.
SPs and Authenticity
Misconception:
SPs aren’t real.
The Evidence:
Barrows [3] noted that “students rapidly forget they are dealing with an ‘artificial’ patient and relate to the simulator [SP] as a real patient”. [3 p12] In addition, studies have shown that experienced physicians are unable to differentiate real patients from well-trained SPs when sent unannounced into their offices. Rethans et al. [4] and Siminoff et al. [5] both reported a zero detection rate in unannounced SP (USP) visits to physician offices. Siminoff et al. sent post-visit evaluations to the physicians to assess the believability of the USP role portrayals. On a scale of 1–7, with 7 indicating the most convincing portrayal, ratings ranged from 6.7 to 6.9 for believability, convincingness of portrayal and frequency of maintaining role. The conclusion was that carefully trained “USPs portrayed their roles authentically within the context of the patient-physician encounter”. [5 p8].
Misconception:
When working with SPs, learners sometimes state that they would act differently if the SP were a real patient.
The Evidence:
This type of response can indicate a lack of buy-in and engagement from a learner and can be the result of anxiety or uncertainty brought about by such factors as not understanding how to work with SPs, not being briefed properly before a simulation session or having had unhelpful previous encounters with SPs. Rudolph et al. [6] address how to create a safe container for a simulation to occur and increase the potential of learner buy-in and engagement by briefing learners before the simulation event. One of the techniques they endorse in the briefing is establishing a fiction contract, as articulated by Dieckmann et al. [7] When working with SPs, this contract would translate into acknowledging to the learner that yes, the SP is not a real patient and the encounter with the SP is in a constructed, fictional environment. Learners are asked to commit to this fiction, to suspend their disbelief and engage with the SP ‘as if’ the situation were real, and ‘as if’ the SP were the actual person they are representing. In turn, the facilitator is asked to commit to making the situation as real as possible by making sure that learners have all the resources that they need for an encounter. SPEs must work with faculty to create this fiction contract with their learners. For example, SPEs need to make sure that the SPs recruited fit the demographic profile of the people they are representing and fully train the SPs to respond authentically to many different kinds of learner encounters [8].
Misconception:
You can just send any SP over to portray our case. It doesn’t matter how old they are or what gender they are.
The Evidence:
SPs should be reflective of the people they are representing [9]. If the case centers on a 25-year-old pregnant woman and a 70-year-old man arrives to portray the role, the authenticity and integrity of the learning situation are completely undermined. It’s difficult for anyone to buy-in to this situation, let alone expect learners to perceive that a 70-year-old man could represent a 25-year-old pregnant woman. This example illustrates a fiction contract broken by both the faculty member and the SPE long before the SP encounters the learner.
Misconception:
There is a difference in learner/physician performances with SPs verses real patients.
The Evidence:
Early studies showed that the clinical performances of medical residents were similar between encounters with real patients or with SPs who were trained from a real patient case [10].
Misconception:
SPs are standardized.
The Evidence:
SPs are human beings and human beings cannot be standardized. However, as the ASPE SOBP [2] note, SP behaviors can be standardized along a spectrum depending on the purpose of what the SP is doing. At one end of the spectrum, in formative, educational settings, SPs have a great deal of flexibility in how they interact with learners while on the other end of the spectrum, in summative contexts, SP behaviors are honed to be more repeatable (consistent and accurate) in response to behaviors by learners. The onus is on the SPE to advocate for case development and training that supports SPs to perform in an authentic manner no matter the degree of standardization [11].
Misconception:
SPs react the same way to every learner.
The Evidence:
The key word in this misconception is ‘same’. Effectively trained SPs will react to each learner’s unique behavior in a flexible and authentic manner within the parameters of the degree of required standardization for the role they have been trained to portray [8, 12,13,14,15].
Misconception:
SPs aren’t as high fidelity as mannequins.
The Evidence:
The Society for Simulation’s Healthcare Simulation Dictionary [16] defines fidelity as “the degree to which the simulation replicates the real event ... the ability of the simulation to reproduce the reactions, interactions and responses of the real-world counterpart”. [16 p12] We must therefore argue the SP, who is portraying the human being, is the closest replication of a real patient in the real-world setting and therefore the highest fidelity simulation modality. Mannequins can be described as high technology. One modality is not better than another. The important thing is to match the right simulation modality with the right learning objectives.
Misconception:
We must use a mannequin because an SP cannot produce the signs and symptoms needed for this case.
The Evidence:
Barrows [17] noted that there are 49 signs and symptoms that an SP can portray. Increasingly, hybrid simulation is allowing for SPs, in combination with various pieces of wearable or adjunct technology, to be involved in cases that combine competencies related to the integration of communication and psychomotor skills, clinical decision-making and professionalism [18].
SPs and Actors
Misconception:
You must be an actor to be an SP.
The Evidence:
SPs are drawn from a diverse group of individuals including laypersons, learners, faculty, retired alumni and actors. However, there is no evidence to suggest that actors make better SPs than those who have no previous performance training or vice versa [14]. Actors may have the training, ability and experience to effectively portray strong emotions and learn detailed, complex information, and therefore may require less training in these aspects of SP role portrayal [19]. However, many of these skills also can be trained and developed with non- actors.
Misconception:
Human role players in simulation should be called actors rather than SPs.
The Evidence:
As long as there have been SPs, this use of terminology has been debated. Many SPs have an acting background and make excellent SPs. As discussed in the ASPE SOBP [2] actors and SPs are both performing, but have different functions or scopes of practice. Actors fulfill the objectives of the playwright and director and, for the most part, provide entertainment. SPs are part of the educational team and are in service to the learning objectives of the simulation case and the learners. And, acting practices can greatly inform the work of SPs [20,21,22,23,24,25,26,27]. Addressing this use of terminology provides an opportunity for the SPE to point out the unique role of SPs and that the nature of the SP’s performance is an application of role play in a learning or assessment setting.
Misconception:
SPs who have an acting background are not as accurate as SPs without an acting background at filling in assessment instruments.
The Evidence:
In a study of 1,972 encounters of SPs portraying a role and then filling in an assessment instrument for a high stakes licensing OSCE, Langenau et al. [28] reported there was no statistical differences in SP recording accuracy on history and physical examination checklists related to acting experience. The study concluded that “SPs with and without performing arts experience can be recruited for high-stakes SP-based clinical skills examinations without sacrificing examination integrity or scoring accuracy”. [28 p150]
Misconception:
I can save money if I hire actors because I don’t need to train them.
The Evidence:
If actors are recruited to be SPs, they need be orientated to SP work and then trained for specific contexts, as is the case with all SPs. Actors may need less training for roles that are highly affective or complicated, but not always [2].
Misconception:
Being an SP is just like any other acting job.
The Evidence:
The recruitment process offers an opportunity for SPEs to clarify the differences between SP and actor performance. SPEs should explain the multi-faceted components of SP work that may include providing feedback and/or assessing learners, in addition to role portrayal [2].
General Considerations for Working with SPs
Misconception:
SPs only portray patients.
The Evidence:
The scope of contemporary SP practice is continually evolving in health care and beyond. While SPs initially portrayed patients, they now portray an increasingly diverse array of individuals, such as family members, health care and other providers/professionals, (e.g. embedded participants). SP methodology is now employed in fields as diverse as law, architecture, chaplaincy, law enforcement, business, the military, veterinary medicine and human resources. To reflect this shift and to be inclusive of all professionals and disciplines that work with human role players, the term SP is increasingly seen in the literature to mean simulated participant [29].
Misconception:
SPs are ‘tools’ that are used.
The Evidence:
SPs are human beings , and part of the educational team. McNaughton and Anderson [30] remind us of the importance of the language we use to describe them, our relationship to them, and that their role in the process matters. Nestel et al. [31] advocate for “reconsidering this phrase [using SPs] to the more positive ‘working with SPs.’ Rather than regarding SPs as tools or objects of use, this small but significant statement emphasizes the crucial contributions that simulated participants make in supporting learning”. [31 p2]
Misconception:
SPs cost too much.
The Evidence:
The cost of working with SPs should not be the first consideration as to whether to employ SP methodology. The first consideration should be to determine the learning objectives and then to match the appropriate simulation modality to the learning objectives. If the learning objectives relate to diverse competencies such as communication and the integration of psychomotor skills, clinical decision-making and professionalism, SPs are probably a more appropriate simulation modality than mannequins [29]. Of course, cost is always an important consideration but to automatically dismiss working with SPs because of the cost overlooks the fact that all simulation modalities have associated costs. For example, mannequins have costs associated with purchasing, running and maintaining them [32,33,34,35].
Misconception:
SP work is easy and fun – it’s not a real job.
The Evidence:
SP work can be fun, and it is also a highly demanding job. Depending on the learning objectives and context, the SP may perform up to three tasks simultaneously: recollect details to authentically portray a role; remember what was discussed to document performance on assessment forms; and, provide verbal or written feedback about their experience with the learner. The work may be physically and mentally demanding in a variety of ways including long testing days that require stamina and intense concentration. Certain cases require repeated physical exams which may cause some discomfort [36,37,38,39,40].
Misconception:
Working with volunteer SPs will save my program a lot of money.
The Evidence:
Working with volunteer SPs will still require a budget line. Someone with expertise in SP methodology must recruit these volunteers, screen them, prepare them and ensure their quality and wellness [35, 41,42,43,44,45].
Misconception:
Volunteer SPs are not as effective as paid SPs.
The Evidence:
There is no evidence to suggest that volunteer SPs are more or less effective than paid SPs [14, 42, 46,47,48,49,50,51].
Misconception:
It is too expensive to train and hire SPs as physical exam instructors.
The Evidence:
Allen et al. [52] report working with SPs who are carefully trained to teach physical examinations and are also known as Physical Examination Teaching Associates (PETAs) or Patient Instructors (PI) is cost-effective, actually saves money, and is very popular with learners.
Misconception:
Some SP applicants think that being an SP means that they will be involved in medical experiments or undergo medical procedures.
The Evidence:
SPs do not have medical experimentation or medical procedures done on them. There is a strong ethical component to SP work, and to simulation in general, that would not allow for this kind of situation to happen [2, 53].
Misconception:
When I tell someone in a social setting about our program they say “Oh I have relative who would be perfect for this work. She’s such a character”. (e-mail to Gayle Gliva-McConvey from Nancy McNaughton, 25 June 2019; unreferenced).
The Evidence:
SPs portray ‘characters’, or someone other than themselves, but it is generally not a prerequisite and can sometimes be as a hindrance if they are ‘characters.’ To be a character implies someone with unique or quirky traits that are sometimes larger than life. The behavior of ‘characters’ can often pull a group training off track and frustrate other SPs. Additionally, ‘characters’ may engage in inappropriate interactions with learners (e.g. too much familiarity, inappropriate humor) and derail the learning activity from meeting the objectives. Clearly outlining the roles and responsibilities of the SP can help these individuals and yourself decide if SP work is the right fit for them [2].
Misconception:
Some people believe that there is no appreciable impact if last-minute changes are made to case materials (e-mail to Gayle Gliva-McConvey from Terry Summer, 23 January 2016; unreferenced).
The Evidence:
Flexibility is an important quality for SPEs and SPs [14]. Sometimes last-minute changes are inevitable but working habitually in a last-minute manner can be confusing and challenging for SPs and learners alike and erode the quality of the experience [54]. The ASPE SOBP offers guidance to help minimize these kinds of situations, such as creating explicit policies and procedures, allowing adequate time for the development of cases, and scheduling in a dry run or a pilot run to test the case prior to the actual simulation session, especially for a new case [2].
Misconception:
There is no impact on SPs if they play a complex case with a high emotional affect or complex physical maneuvers repeatedly over the day
The Evidence:
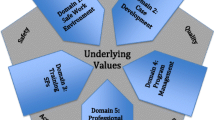
While SPs often feel that their SP work is among the most rewarding work they do, this work may come with emotional and physiological costs. Portraying highly emotional roles a single time a day can be draining. Portraying them multiple times can be overwhelming. McNaughton et al. [37] describe several residual psychophysiological effects after SP portrayal of emotionally intense roles and identify variables that are related to these residual effects. ASPE SOBP Domain 1 – Safe Work Practices [2] outllines the need to develop strategies to mitigate potential adverse effects to prevent SP injury or fatigue. McNaughton et al. [37] note that understanding the impact on SPs when portraying emotional roles, can lead to “improved recruitment, training, and performance”. [37 p135]
Misconception:
SPs have a hidden agenda and/or are trying to trick learners.
The Evidence:
SPs are not trained to have hidden agendas, and SP roles are not designed to trick learners. Rather, SP cases are carefully designed to support the learning objectives, and SPs are carefully trained according to the case details. For example, unless it is part of their role, SPs do not fill in gaps in the information, make assumptions, mislead or hold back information. However, if a learner only asks closed- ended questions then the SP will answer accordingly with short answers. If SPs suddenly say something that seems to be disconnected from the conversation, it is usually a prompt to get learners back on track rather than an attempt to trick them [12, 15, 55].
Training SPs
Misconception:
Only clinicians who are subject matter experts (SMEs) should train SPs.
The Evidence:
Having a clinical background can sometimes be helpful but is not essential to be an SPE. SPEs and SMEs bring different perspectives to the SP training process. SPEs are the experts in SP methodology. SMEs understand the clinical components of the SP’s task. Ideally, SMEs and SPEs are working together as a team to bring their respective areas of strength to the process of training SPs [56, 57].
Misconception:
SPs don’t need training.
The Evidence:
No matter what type of SPs on the Human Simulation Continuum (e.g. role player, structured role player, embedded participant, simulated patient, standardized patient or standardized patient for high stakes assessments) you work with, they must be prepared and/or trained, to a level deemed appropriate for a particular session, to ensure the safety and effectiveness of a simulation [2].
Misconception:
SPs can be trained to portray any person or work in any situation.
The Evidence:
It is important when selecting SPs, to consider many factors, including what Cleland et al. [14] refer to as their ability and suitability. SPs are not interchangeable widgets. Not all SPs can do all roles. Ability and skills are important to consider. A large part of the SPE’s task is to select the right SP for the right role. In addition, casting SPs in some roles can be unsuitable for various reasons. For example, there could be a conflict of interest (e.g. the SP is a close relative of the learner). Personal circumstances may also preclude a SP from being involved in a session. If an SP has had a recent death in the family, asking that SP to do a breaking bad news role could be devastating for both the SP and the learner if the SP becomes upset in the role. SPs should always be allowed to opt out of a role, even if they have been cast and trained, if they perceive that actually doing the simulation session would cause them distress [2]. As SPEs, we have an ethical imperative to screen for and ensure the psychological safety of all involved in the simulation [58].
Misconception:
At our site, we only work with confederates who are practicing clinicians. They don’t need any training because they already know what to do.
The Evidence:
Confederates, or embedded simulated participants are “individuals who commonly portray the role of healthcare professionals in mannequin -based simulations”. [58 p45] They may have subject matter expertise but may not understand how to work within a simulation. Sanko et al. [35] state: “simulation programs that lack training and assessment of ESPs [embedded simulated persons] do their learners and their programs an injustice, robbing them of the full spectrum of engagement and learning that can take place in a well-rehearsed, well-rounded and well-acted simulation experience”. [35 p213]
Misconception:
I only work with confederates or embedded simulated participants, so I can’t/don’t use SP methodology because it’s only relevant for training those who are going to portray patients.
The Evidence:
There are nuances in the different roles that SPs can take on [58, 59] but as the ASPE Standards of Best Practice [2] note, SP methodology can be employed for all human role players in simulation. For those educators just starting to work with human role players, it is helpful to know that the wheel does not have to be reinvented and there is an existing methodology in place to support and guide practice.
Misconception:
SPs don’t need /shouldn’t be provided with too many case details to portray a person in a case.
The Evidence:
SPs require enough detail to bring the person they are portraying to life in an authentic manner. They also need a common understanding of any additional information that they might he asked so they are able to interact with learners in a confident and consistent manner. Sometimes, requests for this kind of information from SPs are seen as being frivolous or unimportant, but SPs often gain valuable insights from their front-line interactions with learners to anticipate the kinds of questions that they will asked or to spot missing details or gaps in cases. If these gaps are not filled, SPs may start to make things up, or come out of role, thereby disrupting the integrity of the encounter and losing confidence [15]. SPE Elizabeth Kachur has observed that it can be very upsetting for SPs if they are portraying people with serious medical conditions and they are not given information about possible outcomes before the session. She reports that rationales for not wanting to provide knowledge of a diagnosis to the SPs can range from thinking that there is not enough training time to cover it or that it is not important, or that if SPs are naive, they will respond more authentically. Kachur reports that this practice has the potential to be psychologically unsafe for SPs and she has noted that it can cause them great distress during and long after the simulation is over [60]. Withholding this kind of information has the potential to contradict the practices and principles in Domain 1 of the ASPE SOBP, Safe Work Environment [2], particularity related to psychological safety.
Misconception:
SPs can use their personal histories. This will save time writing cases and training SPs.
The Evidence:
In certain contexts, SPs do use their own histories [14]. However, it is also important to be aware that if SPs use their own histories, they might introduce distracting or extraneous information or stray into territory that is upsetting for both them and/or the learners and that is not related to the learning objectives of the session [5, 58].
Misconception:
SPs do not need to be de-roled or debriefed.
The Evidence:
As outlined in the Phases of Simulation model developed by Nestel [29], de-roling SPs is an essential step and one that is often overlooked. De-roling is a technique derived from drama therapy and acting [61], through which SPs portraying roles, particularly ones that are intense or upsetting, can release or separate from the roles so they are not adversely affected. In addition, it is increasingly being recognized that, as with learners, debriefing SPs helps them to reflect and grow, allows for reflection and assessment of the quality of SP participation and attends to SP wellness [58, 62].
Misconception:
SPs don’t need to be trained to give feedback; rather, they should just provide an honest account of what an interaction was like for them.
The Evidence:
Sending SPs into a room without training in feedback delivery can result in unsafe situations and ineffective outcomes. Delivering feedback is a learned skill that must be practiced and continually refreshed. In addition, there are many different models of feedback and the SPE needs to be clear about which model is being required in a session so they can train their SPs appropriately. SPs also need to understand what the focus of their feedback is and that the focus can vary from session to session [63,64,65].
Misconception:
Physical examination techniques should only be taught to learners by clinicians.
The Evidence:
Several studies have proven that carefully trained SPs can train learners to conduct physical examination skills as effectively or more effectively than clinical faculty [52, 66, 67].
SPs and Assessments
Misconception:
There is no solid research base for evaluating SP-based assessments.
The Evidence:
Research started in the late 1970s to determine the reliability, validity and other psychometric criteria of assessments with SPs [68,69,70,71,72,73]. Colliver [10] notes that “a database prepared by the National Board of Medical Examiners (NBME) in 1991 listed 209 articles on SP assessments”. (p454) By the mid-1990s, the US-based National Board of Medical Examiners was satisfied with the research demonstrating the value of SPs in assessments and implemented the Step 2 clinical skills component of the licensing process in 2004 [74]. Although there are regional variations, SP-based summative assessments are now implemented around the world, including in the UK, Australia, New Zealand, United States, Canada, Switzerland and Taiwan, to name only a few countries.
Misconception:
SP scores aren’t reliable (reproducible).
The Evidence:
As Zabar et al. [75] note: “Many programs use SP raters since they can achieve a good level of reliability”. [75 p22] Swanson and Stillman [76] comment: “There is little difference in the reliability between SP and faculty raters, though the two may rate somewhat different skills depending on the study”. [76 p91]
Misconception:
Physical Exam Teaching Associates (PETA)/Patient Instructor (PI) scores aren’t as accurate as physician scores.
The Evidence:
A 1987 study by Elliot et al. [77] reported that “faculty observers reliably assessed 68% of physical examination skills. Patient Instructors provided an assessment that was comparable with faculty observers for 83% of these skills…even when SP training was low”. [77 p3408]
Misconception:
PETAs can’t teach the physical examination techniques as well as physicians.
The Evidence:
PETAs have effectively taught physical examination techniques as demonstrated in several studies [52, 78, 79]. Barley et al. [66] report that PETAs can teach physical examination techniques as well or sometimes better than clinical faculty.
Misconception:
SPs cannot assess communication skills.
The Evidence:
SPs can be trained to assess observable behaviors related to patient-centered communications skills (e.g. fostering the relationship, supporting emotions), such as in the United States Medical Licensing Examination (USMLE) [80, 81].
Misconception:
SPs cannot provide accurate ratings of a physician’s interpersonal skills.
The Evidence:
In a 2007 study of 37,000 international physicians completing the Educational Commission for Foreign Medical Graduates (ECFMG) certification examination, Van Zanten et al. [82] reported data from over 400,000 SP encounters. They analyzed four interpersonal dimensions: skills in interviewing and collecting data; counseling and delivering information; rapport; and, personal manner. Results indicated that “SPs, with proper training and a benchmarked scoring rubric, can provide accurate and defensible ratings of physician’s interpersonal skills”. [82 p195]
Misconception:
When students who have finished an assessment tell their peers who have not yet done the assessment about the cases, it is a threat to the validity of the assessment.
The Evidence:
Five studies conducted during 1991–1992 reported no consistent, systematic increasing (or decreasing) trend in scores throughout an examination period across 23 sites. Learners who were tested later in the examination period did not perform at a higher level. Additionally, just because the learner knows what the diagnosis is, it does not mean they can demonstrate the clinical and interpersonal skills. In fact, having this pre knowledge may even hamper their performance [83].
Misconception:
SPs are biased/not biased when scoring learners.
The Evidence:
We all have bias [84] and even the most rigorous training cannot prevent bias from creeping into an SP’s work [85]. SP educator Tony Errichetti notes that there are two types of bias: “statistical bias and personal bias, both of which are potential sources of SP/rater scoring errors” (e-mail to Cathy Smith from Tony Errichetti, 18 June 2019; unreferenced). There are many published strategies for dealing with statistical bias related to SP assessment [72, 86]. Personal bias, which refers to subjective beliefs and values of an individual [87], is increasingly being recognized as an important factor to consider in simulation and beyond and may best be addressed with the support of inclusion and diversity professionals.
Misconception:
SPs are not subject matter experts and therefore can’t/shouldn’t judge clinical content.
The Evidence:
It is true most SPs are not subject matter experts and therefore cannot judge clinical reasoning. However, with careful training, SPs can accurately document whether learners have addressed aspects of clinical content linked to a scoring tool they have been trained to use. Also, it is critical to design a checklist that has evidence-based clinically discriminating items to improve the reliability of the checklist scores of SPs [83].
The ASPE Standards of Best Practice (SOBP)
Misconception:
The ASPE SOBPs are only applicable to larger, well-resourced programs.
The Evidence:
The ASPE SOBP [2] were developed to be applicable to SP programs and practices with diverse characteristics, resources and cultures. These standards are designed to be both foundational and, depending on the context, aspirational. The SOBP provide precise and yet flexible guidelines that address the diversity of varying contexts of SP practice, and size of programs.
Misconception:
The ASPE SOBPs don’t apply to my SP work because my program doesn’t have high stakes exams.
The Evidence:
Training SPs for high stakes exams is just one aspect of SP methodology addressed in the ASPE SOBP. It is acknowledged in the document that because of the wide variety of work that SPs do, not all Domains and the accompanying Principles and Practices will be applicable to all programs [2].
Misconception
I’ve been getting along just fine in my SP program for many years doing it my own way, so I don’t need to follow the ASPE SOBP or any other standards.
The Evidence
Practice 5.1.1 of the ASPE SOBP Domain 5, Professional Development [2] notes that SPEs should “develop and promote expertise in knowledge, skills and attitudes related to SP-based simulation”. [2 p7] Therefore, as evidence emerges and standards are developed and refined related to both SP methodology and broader simulation practices, the SPE has a professional obligation to reflect on how to incorporate this new information into their practice.
The Role of the SPE
Misconception
SPEs are not necessary – SPs can train themselves.
The Evidence
SPEs and SPs have a symbiotic relationship. The ASPE SOBP [2] describes SPEs as “those who work to develop expertise in SP methodology and are responsible for training and/or administering SP-based simulation”. [2 p3] Emerging research and thought related to the evolving roles and responsibilities of the SPE and the SP indicates that the scope of SP practice continues to evolve and that SPEs and SPs have a relationship that shifts according to different contexts [11, 31, 88]. Nestel et al. [11] note: “All of this work is essentially collaborative … . Recognition that SPs are integral players providing educational input from a unique location and as part of an overarching learning plan means that the educational alliance can be turned into opportunities for rich learning. The role of SP practitioners [SPEs] is to position SPs to productively engage in these activities”. [11 p701]
Summary
By responding to misconceptions related to working with SPs, SPEs can maximize the potential for ensuring that the effectiveness and safety of an SP-based session is maintained. In addition, there is a valuable opportunity to engage with, educate, and learn from other stakeholders. Finally, addressing these misperceptions points out the importance of the SPE working in an evidence-based manner. Moving forward, we encourage open discussion about misconceptions related to SP methodology with the goal of strengthening and transforming the possibilities for working with SPs.
References
Oxford Learner’s Dictionary. Misconception, n. [Internet]. Oxford University Press; 2019 [cited 20 June 2019]. Available from https://www.oxfordlearnersdictionaries.com/definition/english/misconception.
Lewis KL, Bohnert CA, Gammon WL, Hölzer H, Lyman L, Smith C, et al. The association of standardized patient educators (ASPE) standards of best practice (SOBP). Adv Simul. 2017;2(1):10.
Barrows H. Simulated patients (programmed patients: the development and use of a new technique in medical education). Springfield, IL: Charles C Thomas; 1971.
Rethans J, Drop R, Sturmans F, van der Vleuten C. A method for introducing standardized (simulated) patients into general practice consultations. Br J Gen Pract. 1991;41(344):94–6.
Siminoff LA, Rogers HL, Waller AC, Harris-Haywood S, Esptein RM, Carrio FB, et al. The advantages and challenges of unannounced standardized patient methodology to assess healthcare communication. Patient Educ Couns. 2011;82(3):318–24.
Rudolph JW, Raemer DB, Simon R. Establishing a safe container for learning in simulation: the role of the presimulation briefing. Simul Healthc. 2014;9(6):339–49.
Dieckmann P, Manser T, Wehner T, Rall M. Reality and fiction cues in medical patient simulation: An interview study with anesthesiologists. J Cogn Eng Decis Mak. 2007;1(2):148–68.
Newlin-Canzone ET, Scerbo MW, Gliva-McConvey G, Wallace AM. The cognitive demands of standardized patients: Understanding limitations in attention and working memory with the decoding of nonverbal behavior during improvisations. Simul Healthc. 2013;8(4):207–14.
Nestel D, Krogh K, Kolbe M. Exploring realism in healthcare simulations. In: Nestel D, Kelly M, Jolly B, Watson M, editors. Healthcare simulation education: evidence, theory and practice. Oxford: Wiley-Blackwell; 2018. p. 23–8.
Colliver J, Williams RG. Technical issues: test application. AAMC Academic Medicine. 1993;68(6):454–60.
Nestel D, McNaughton N, Smith C, Schlegel C, Tierney T. Values and value in simulated participant methodology: a global perspective on contemporary practices. Med Teach. 2018;40(7):697–702.
Smith C, O’Byrne C, Nestel D. Simulated patient methodology and assessment. In: Nestel D, Bearman M, editors. Simulated patient methodology: theory, evidence and practice. Chichester: Wiley-Blackwell; 2015. p. 85–92.
Nestel D, Gough S. Designing simulation-based learning activities: a systematic approach. In: Nestel D, Kelly M, Jolly B, Watson M, editors. Healthcare simulation education: evidence, theory and practice. Oxford: Wiley-Blackwell; 2018. p. 135–42.
Cleland J, Abe K, Rethans J. The use of simulated patients in medical education: AMEE Guide No. 42. Med Teach. 2009;31:477–86.
Wallace P. Coaching standardized patients: for use in the assessment of clinical competence. New York: Springer; 2007.
Lopreiato J, Downing D, Gammon W, Lioce L, Sittner B, Slot V, et al. Healthcare simulation dictionary [Internet]. Society for Simulation in Heatlhcare. 2016 [cited 12 June 2019]. Available from http://www.ssih.org/Dictionary.
Barrows HS. Training standardized patients to have physical findings. Springfiled, IL.:Southern Illinois University School of Medicine; 1999.
Schocken D, Gammon W. Hybrid simulation. In: Palaganas J, Maxworthy J, Epps C, Mancini M, editors. Defining excellence in simulation programs. 1st ed. Philadelphia: Lippincott Williams & Wilkins; 2015. p. 235–40.
McNaughton N. The role of emotion and affect in the work of standardized patients: a critical theoretical analysis. Berlin: Lambert Academic Publishing Press; 2012.
Smith CM, Gephardt EG, Nestel D. Applying the theory of Stanislavski to simulation: stepping into role. Clin Simul Nurs. 2015;11(8):361–7.
Schweickerdt-Alker L. Revitalising the SP through authentication: the authentic portrayal. Med Teach. 2014;36(6):541–3.
Treadwell I, Schweickerdt-Alker L, Pretorius D, Hugo MD. The effect of characterisation training on the congruence of standardised patient portrayals. Afr J Health Prof Educ. 2014;6(1):56–9.
Liao C-S, Kao S-P, Liang S-Y, Hsieh M-C. Training actors as standardized patients. Tzu Chi Med J. 2015;27(2):96–7.
Nelles LJ. My body, their story: performing medicine. Can Theatr Rev. 2011;146(1):55–60.
Cowperthwait A, Saylor J, Carlsen A, Schmitt LA, Salam T, Melby MK, et al. Healthcare theatre and simulation: maximizing interprofessional partnerships. Clin Simul Nurs. 2015;11(9):411–20.
Cowperthwait A, Saylor J, Schell K. Healthcare theatre: a unique simulation partnership. Clin Simul Nurs. 2014;10(1):e41–e6.
Smith C, Edlington TL, Lawton R, Nestel D. The dramatic arts and simulated patient methodology. In: Nestel D, Bearman M, editors. Simulated patient methodology: theory, evidence and practice. Chichester: Wiley-Blackwell; 2015. p. 39–45.
Langenau EE, Dyer C, Roberts WL, De Champlain A, Montrey D, Sandella J. Relationship between standardized patient checklist item accuracy and performing arts experience. Simul Healthc. 2011;6(3):151–4.
Nestel D, Bearman M. Introduction to simulated patient methodology. In: Nestel D, Bearman M, editors. Simulated patient methodology: theory, evidence and practice. Chichester: Wiley-Blackwell; 2015. p. 1–4.
McNaughton N, Anderson M. Standardized patients: it’s all in the words. Clin Simul Nurs. 2017;13(7):293–4.
Nestel D, Roche J, Battista A. Creating a quality improvement culture in standardized/simulated patient methodology: the role of professional societies. Adv Simul. 2017;2(1):18.
Slone F, Lampotang S. Mannequins: terminology, selection, and usage. In: Palaganas JC, Maxworthy JC, Epps CA, Mancini ME, editors. Defining Excellence in Simulation Programs. 1st ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014. p.183–98
Motola I, Devine LA, Chung HS, Sullivan JE, Issenberg SB. Simulation in healthcare education: a best evidence practical guide. AMEE Guide No. 82. Med Teach. 2013;35(10):e1511–e30.
Fletcher J, Wind AP. Cost considerations in using simulations for medical training. Mil Med. 2013;178(suppl_10):37–46.
Sanko JS, Shekhter I, Kyle RR, Birnbach DJ. Using embedded simulated persons (aka “confederates”). In: Palaganas JC, Maxworthy JC, Epps CA, Mancini, ME, editors. Defining excellence in simulation programs. 1st ed. Philadelphia: Lippincott Williams & Wilkins; 2015. p. 213–26.
Schlegel C, Bonvin R, Rethans J-J, Van der Vleuten C. Standardized patients’ perspectives on workplace satisfaction and work-related relationships: a multicenter study. Simul Healthc. 2016;11(4):278–85.
McNaughton NL, Tiberius R, Hodges B. Effects of portraying psychologically and emotionally complex standardized patient roles. Teach Learn Med. 1999;11(3):135–41.
Plaksin J, Nicholson J, Kundrod S, Zabar S, Kalet A, Altshuler L. The benefits and risks of being a standardized patient: a narrative review of the literature. Patient-Patient-Centered Outcomes Res. 2016;9(1):15–25.
Nestel D, Clark S, Tabak D, Ashwell V, Muir E, Paraskevas P, et al. Defining responsibilities of simulated patients in medical education. Simul Healthc. 2010;5(3):161–8.
Abe K, Roter D, Erby LH, Ban N. A nationwide survey of standardized patients: who they are, what they do, and how they experience their work. Patient Educ Couns. 2011;84(2):261–4.
Smith C, Sokoloff S, Meyer R. Working with volunteers as standardized/simulated patients: everything you need to know to get started. Preconference workshop. Toronto: INACSL; 2018.
Nestel D, Calandra A, ElIiott RA. Using volunteer simulated patients in development of pre-registration pharmacists: learning from the experience. Pharm Educ: Int J Pharm Educ. 2007;7(1):35–42. PubMed PMID: 2007-06883-005. English
King MA, Ott J. Actors needed: clinical faculty get the call. Nurse Educ. 2012;37(3):105–7.
Husson N, Zulkosky KD. Recruiting and training volunteer standardized patients in the NCSBN national simulation study. Clin Simul Nurs. 2014;9(10):487–9.
Ker JS, Dowie A, Dowell J, Dewar G, Dent JA, Ramsay J, et al. Twelve tips for developing and maintaining a simulated patient bank. Med Teach. 2005;27(1):4–9.
Gallimore C, George AK, Brown MC. Pharmacy students’ preferences for various types of simulated patients. Am J Pharm Educ. 2008;72(1). English.
Collins JP, Harden RM. AMEE Medical Education Guide No. 13: real patients, simulated patients and simulators in clinical examinations. Med Teach. 1998;20(6):508–21.
Mavis B, Turner J, Lovell K, Wagner D. Developments: faculty, students, and actors as standardized patients: expanding opportunities for performance assessment. Teach Learn Med. 2006;18(2):130–6.
Murphy S, Imam B, MacIntyre DL. Standardized patients versus volunteer patients for physical therapy students’ interviewing practice: a pilot study. Physiother Can. 2015;67(4):378–84.
Bokken L, Rethans JJ, Jöbsis Q, Duvivier R, Scherpbier A, Van Der Vleuten C. Instructiveness of real patients and simulated patients in undergraduate medical education: a randomized experiment. Acad Med. 2010;85(1):148–54.
Luke K, Smith R. Communication skills training: a United Kingdom perspective. Acad Med. 2012;87(8):993. PubMed PMID: 2013-08954-001. English.
Allen SS, Miller J, Ratner E, Santilli J. The educational and financial impact of using patient educators to teach introductory physical exam skills. Med Teach. 2011;33(11):911–8.
Code of Ethics Working Group. The Healthcare Simulationist Code of Ethics [Internet]. Society for Simulation in Healthcare. 2018 [ cited 1 April 2019]. Available from https://www.ssih.org/SSH-Resources/Code-of-Ethics.
Nestel D, Fleishman C, Bearman M. Preparation: developing scenarios and training for role portrayal. In: Nestel D, Bearman M, editors. Simulated patient methodology: theory, evidence and practice. Chichester: Wiley-Blackwell; 2015. p. 63–70.
Owens T, Gliva-McConvey G. Standardized patients. In: Palaganas JC, Maxworthy JC, Epps CA, Mancini ME, editors. Defining excellence in simulation programs. 1st ed. Philadelphia: Lippincott Williams & Wilkins; 2014. p. 199–212.
Smith C, O’Byrne C. Using an exam-readiness tool to ensure quality of standardized/simulated patient role portrayal in high-stakes simulation assessments. Clear Exam Rev. 2017;27(1):17–24.
Furman GE. The role of standardized patient and trainer training in quality assurance for a high-stakes clinical skills examination. Kaohsiung J Med Sci. 2008;24(12):651–5.
Nestel D, Sanko J, McNaughton N. Simulated participant methodologies: maintaining humanism in practice. In: Nestel D, Kelly M, Jolly B, Watson M, editors. Healthcare simulation education: evidence, theory and practice. Oxford: Wiley-Blackwell; 2018. p. 45–53.
Nestel D, Mobley B, Hunt EA, Eppich WJ. Confederates in healthcare simulations: not as simple as it seems. Clin Simul Nurs. 2014;10:611–6.
Kachur E. Challenges of working with faculty – case writing & psychological safety. Presentation/discussion. Kansas City, M0: ASPE; 2018.
Kansas State University. ScienceDaily: How de-roling may help actors shed intense roles [Internet]. ScienceDaily. 5 June 2014 [cited 30 May 2019]. Available from: www.sciencedaily.com/releases/2014/06/140605140011.htm
Smith C. Debriefing SPs after simulation events (module 10) [Internet] 2012 [accessed 20 Oct 2019]. Available from www.simulatedpatientnetwork.org
Bokken L, Linssen T, Scherpbier A, Van Der Vleuten C, Rethans JJ. Feedback by simulated patients in undergraduate medical education: a systematic review of the literature. Med Educ. 2009;43(3):202–10.
Berenson LD, Goodill SW, Wenger S. Standardized patient feedback: making it work across disciplines. J Allied Health. 2012;41(1):27E–31E.
Nestel D, Bearman M, Fleishman C. Simulated patients as teachers: the role of feedback. In: Nestel D, Bearman M, editors. Simulated patient methodology: theory, evidence and practice. Chichester: Wiley-Blackwell; 2015. p. 71–8.
Barley GE, Fisher J, Dwinnell B, White K. Teaching foundational physical examination skills: study results comparing lay teaching associates and physician instructors. Acad Med. 2006;81(10):S95–S7.
Raj N, Badcock L, Brown G, Deighton C, O’reilly S. Undergraduate musculoskeletal examination teaching by trained patient educators—a comparison with doctor-led teaching. Rheumatology. 2006;45(11):1404–8.
Van der Vleuten CP, Swanson DB. Assessment of clinical skills with standardized patients: state of the art. Teach Learn Med. 1990;2(2):58–76.
Hodges B, Regehr G, Hanson M, McNaughton N. Validation of an objective structured clinical examination in psychiatry. Acad Med:J Assoc Am Med Coll. 1998;73(8):910–2.
Boulet JR, De Champlain AF, McKinley DW. Setting defensible performance standards on OSCEs and standardized patient examinations. Med Teach. 2003;25(3):245–9.
Vu NV, Barrows HS, Marcy ML, Verhulst SJ, Colliver J, Travis T. Six years of comprehensive, clinical, performance-based assessment using standardized patients at the Southern Illinois University School of Medicine. Acad Med. 1992;67(1):42–50.
Boulet JR, McKinley DW, Whelan GP, Hambleton RK. Quality assurance methods for performance-based assessments. Adv Health Sci Educ Theory Pract. 2003;8(1):27–47.
Boulet JR, Swanson DB. Psychometric challenges of using simulations for high-stakes assessment. In: Dunn W, editor. Simulators in critical care education and beyond. Des Plaines,IL: Society of Critical Care Medicine; 2004. p. 119–30.
Hawkins RE, Swanson D, Dillon G, Clauser B, King A, Scoles P, et al. The introduction of clinical skills assessment into the United States medical licensing examination (USMLE): a description of USMLE step 2 clinical skills (CS). J Med Licens Discip. 2005;91:22–5.
Zabar S, Kachur E, Kalet A, Hanley K. Objective structured clinical examinations: 10 steps to planning and implementing OSCEs and other standardized patient exercises. New York: Springer; 2013.
Swanson DB, Stillman PL. Use of Standardized Patients for Teaching and Assessing Clinical Skills. Eval Health Prof. 1990; 13(1): 79–103.
Elliot DL, Hickam DH. Evaluation of physical examination skills: reliability of faculty observers and patient instructors. JAMA. 1987;258(23):3405–8.
Aamodt CB, Virtue DW, Dobbie AE. Trained standardized patients can train their peers to provide well-rated, cost-effective physical exam skills training to first-year medical students. Fam Med-Kansas City. 2006;38(5):326.
Hasle JL, Anderson DS, Szerlip HM. Analysis of the costs and benefits of using standardized patients to help teach physical diagnosis. Acad Med: J Assoc Am Med Coll. 1994;69(7):567–70.
May W, Park JH, Lee JP. A ten-year review of the literature on the use of standardized patients in teaching and learning: 1996–2005. Med Teach. 2009;31(6):487–92.
The National Board of Medical Examiners. Step 2 CS (Clinical Skills) FAQ, Scores, Question 3 - Why does it take so long to score the Step 2 Clinical Skills exam? [Internet]. Federation of State Medical Boards and National Board of Medical Examiners. 2019 [cited 1 June 2019]. Available from: https://www.usmle.org/frequently-asked-questions/#scores
Van Zanten M, Boulet JR, McKinley D. Using standardized patients to assess the interpersonal skills of physicians: six years’ experience with a high-stakes certification examination. J Health Commun. 2007;22(3):195–205.
Daniels VJ, Bordage G, Gierl MJ, Yudkowsky R. Effect of clinically discriminating, evidence-based checklist items on the reliability of scores from an internal medicine residency OSCE. Adv Health Sci Educ. 2014;19(4):497–506.
Gladwell M. Blink: the power of thinking without thinking. New York: Little, Brown; 2005
Manciu M, Trevino R, Mulla ZD, Cortez C, Plavsic SK. Detection of biased rating of medical students by standardized patients: opportunity for improvement. Med Sci Educ. 2017;27(3):497–502.
Boulet JR, Errichetti A. Training and assessment with standardized patients. In Riley RH, editor. Manual of simulation in healthcare. 2nd ed. Oxford: OUP; 2106. p. 185–207
Northon L. Become aware of personal bias, and you’ll improve ethical practice [Internet]. SHRM;. 2016 [cited 30 June 2019]. Available from https://www.shrm.org/resourcesandtools/hr-topics/behavioral-competencies/ethical-practice/pages/become-aware-of-personal-bias-and-improve-ethical-practice-.aspx
Pritchard SA, Blackstock FC, Keating JL, Nestel D. The pillars of well-constructed simulated patient programs: a qualitative study with experienced educators. Med Teach. 2017;39(11):1159–67.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Smith, C.M., Gliva-McConvey, G. (2020). Misconceptions and the Evidence. In: Gliva-McConvey, G., Nicholas, C.F., Clark, L. (eds) Comprehensive Healthcare Simulation: Implementing Best Practices in Standardized Patient Methodology. Comprehensive Healthcare Simulation. Springer, Cham. https://doi.org/10.1007/978-3-030-43826-5_16
Download citation
DOI: https://doi.org/10.1007/978-3-030-43826-5_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-43825-8
Online ISBN: 978-3-030-43826-5
eBook Packages: MedicineMedicine (R0)