
Abstract
Restricted and repetitive behaviors (RRBs) in ASD include stereotyped movement, repetitive use of objects and speech, restricted interests, insistence on sameness, and atypical sensory responses. The way these symptoms present vary across children and development, but often cause significant challenges for individuals and families. Although comprehensive treatment approaches have shown limited effect on RRBs in young children, there are effective strategies to reduce RRBs and/or their effect on children and families. These include a range of behavioral and cognitive behavioral strategies such as functional communication training, use of visual schedules and cues, interruption and redirection, physical exercise, differential reinforcement, and exposure and response prevention, all to be discussed in this chapter.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
“In his second year he ‘developed a mania for spinning blocks and pans and other round objects.’”
—Kanner, 1943
Introduction
In 1943, Leo Kanner detailed the rigidity and repetitious behaviors of 11 case studies of children who he assumed to have “inborn autistic disturbances of affective contact.” One link between Kanner’s cases was rigid behaviors and a “strong urge for sameness.”Today, an observation of repetitive behaviors in a young child, such as the ones described by Kanner in the quote above, would cause suspicion for the presence of autism spectrum disorder (ASD). Restrictive and repetitive behaviors (RRBs) are key attributes of diagnosis of ASD. The Diagnostic and Statistical Manual 5th Edition (DSM-5) divides RRBs into four groups (1) repetitive movements, use of objects, or speech; (2) insistence on sameness, inflexible routines, or ritualized patterns of verbal or nonverbal behaviors; (3) highly restricted interests; and (4) hyper- or hyporeactivity to sensory input or unusual interests (American Psychiatric Association, 2013). RRBs are often further grouped into two categories: low-order behaviors, which include repetitive movements of body and objects and high-order behaviors, which include restricted interests, insistence of sameness, and ritualized verbal patterns (Turner, 1999). Much of the literature around young children and RRBs focuses on repetitive sensory motor (RSM) behaviors when discussing low-order behaviors and “insistence on sameness” behaviors when discussing high-order behaviors (Bishop et al., 2013; Richler, Huerta, Bishop, & Lord, 2010). Below, we characterize each of these symptoms and how they may present themselves in young children with ASD.
Characterizing RRB Symptoms
RRBs can occur in typical toddler development; therefore, distinguishing between typicality and atypicality relies on categorizing the type, frequency, and intensity of the behavior (American Psychiatric Association, 2013). Differences begin to emerge in the second year of life between the RRBs of typical infants and infants with ASD (Elison et al., 2014; Wolff et al., 2014), and between infants with other developmental delays and those with ASD (Morgan, Wetherby, & Barber, 2008; Watt et al., 2008). RRB symptoms are complex in part because they may interfere with development and also may serve as areas of strength and interest that can facilitate learning in other areas. Below, we describe each symptom in this domain.
Repetitive Movements, Use of Objects, or Speech
Repetitive body movements are characteristic of typical infant development in the first 2 years of life. Babies flap their arms to balance and when expecting an action. In typical development, these repetitive movements decrease significantly by 2 years of age (Shafer, Newell, Lewis, & Bodfish, 2017). However, in young children with ASD, and in children with global developmental delays, they might continue. In addition to flapping, repetitive body movements may also include spinning or pacing, posturing hands or fingers, or full body movements like rocking. These movements may be adaptive during typical infancy by allowing infants to explore their environment and functionally change their behavior as a result. In contrast, children with ASD may not integrate sensory feedback to adapt their movements to environment. Thus, these behaviors become maladaptive and can interfere with learning and play (Shafer et al., 2017). For example, a child who rocks his body as he is learning to crawl may no longer engage in rocking once he has mastered the skill of crawling. In contrast, consider an infant who already knows how to crawl, and while crawling toward a caregiver who has called his name, pauses and rocks back and forth repetitively. This behavior no longer promotes the development of a skill and interferes with the child responding to his parent.
Repetitive use of objects in young children can present itself as simply playing with a toy repeatedly in the same manner. For example, a child might roll a car back and forth on the floor without ever moving outside of a specific area. Another child might hold a spoon and shake it up and down repetitively. In young children, repetition is a learning strategy, so deciding what makes the repetitive use of an object a symptom rather than a strategy is determined through the observation of patterns over time. While a typically developing toddler may open and close the door on a play house multiple times, she or he will move on to other actions after figuring out how the doors and windows work. In contrast, a child with ASD may continue to open and close the doors to the exclusion of other actions with that toy.
Finally, repetitive speech includes echolalia (repeating words others have said) and idiosyncratic phrases. Echolalia can be immediate or delayed. Immediate echolalia may present itself as repeating the question a person has asked (e.g., Mom says, “do you want some juice?” and the child responds, “you want some juice”). Delayed echolalia often presents as a child reciting a phrase she has heard before, either from a person in her environment or a cartoon or commercial he or she watched. For example, upon entering a tunnel on his ride to preschool in the morning, a child always says, “would you could you in the dark?” echoing his parents’ reading of a Dr. Seuss book Green Eggs and Ham. Some children reverse their pronouns as part of this echolalia, asking for a snack by saying, “you want cracker.” Intonation patterns of this speech in young children with ASD stands out as children often echo not only the words, but the exact intonation of the previous speaker each time.
Insistence on Sameness, Inflexible Adherence to Routines, or Ritualistic Behavior
Although insistence on sameness and ritualistic behavior can appear later in life, symptoms may be present in early childhood. For example, a child might insist on eating a particular food (e.g., chips) using a particular plate (e.g., the green one), sitting in a particular chair (e.g., the red one) at each meal. This behavior, by itself, is common in typically developing children between ages 2 and 4 years, when most children become increasingly inflexible as part of normative development (Evans et al., 1997). What distinguishes the behavior in children with ASD is the level of adherence, the degree to which the child becomes upset when the routine is interrupted, and, at times, the idiosyncrasies associated with the routine. To take the same example above, a child with ASD might also only eat one brand of chips and associate a different color plate with a different food s/he eats.
Restricted Interests
Highly restricted interests are often what stand out when meeting an older child or adult with ASD, as they may be able to describe in detail numerous facts about unusual topics such as train schedules or car models. In early childhood, when many children with ASD have not yet developed functional speech, these interests present themselves a bit differently. Rather than talking excessively about a topic, children may play exclusively with one toy (e.g., a toy train) or carry around a particular object (e.g., spoons). At times, these interests can be avenues toward engagement, and highlight strengths of a child with ASD. For example, a child who loves trains may learn to count, distinguish colors, and play creatively through train activities. Parents often see these interests as ways to highlight their child’s strengths and interests. For example, a child with a strong interest in dinosaurs may develop this vocabulary for types of dinosaurs ahead of his peers and beyond parents’ knowledge. At other times, these interests can interfere with development. For example, a child with restricted interests in trains may become aggressive toward a peer who tries to play with them and may miss other activities in preschool such as singing and art because of exclusive play with trains. Challenging behaviors may result when a child needs to transition away from a preferred toy or when a parent does not bring along the favorite block the child likes to carry.
Hyper- or Hyporeactivity to Sensory Input or Unusual Interests
Atypical sensory reactions and interests are the final symptoms in this category and include both overreaction (hyperreactivity) and underreaction (hyporeactivity). Examples of hyperreactivity include a child covering her ears when she hears loud sounds or refusing to eat foods with certain textures. Examples of hyporeactivity include a child who does not respond when his name is called or does not seem to notice when he is hurt. Along with these types of reactivity, children with ASD might seek sensory input in unusual ways, such as rubbing a fabric in their hands, squeezing objects, mouthing, or chewing beyond the stage when it is developmentally appropriate. While children with a range of developmental disabilities often show hyperreactivity, it is the combination of hyperreactivity with hyporeactivity that is often indicative of a diagnosis of ASD (Ausderau et al., 2014).
In contrast to OCD symptoms, RRBs in ASD frequently do not cause distress, but rather reflect preferred and/or comforting activities. Despite the positive valence, RRBs can lead to distress and even tantrums and aggression when the individual is interrupted or asked to stop the behavior (Klin, Danovitch, Merz, & Volkmar, 2007; Postorino et al., 2017)
Correlates of RRBs
Ability
Some RRB features are associated with ability level. Children who have more significant intellectual disability often display increased RSM such as stereotypies or sensory interests (Bishop, Richler, & Lord, 2006; Lam, Bodfish, & Piven, 2008; Richler et al., 2010). However, this association is less clear in younger children (e.g., under 3 years)—regardless of intellectual ability, many young children with ASD engage in RSM (Bishop et al., 2006). In contrast, insistence on sameness has been shown to be associated with intelligence in the opposite way, with individuals who have higher ability showing higher challenges with insistence on sameness (Bishop et al., 2006; Lam et al., 2008; Richler et al., 2010). In very young children with or at risk for ASD, RRB symptoms are strongly associated, as a whole, with socialization and adaptive behavior abilities (Schertz, Odom, Baggett, & Sideris, 2016; Wolff, Boyd, & Elison, 2016). In addition, there is some evidence that early presence of significantly impairing RRBs is predictive of less optimal outcomes in children with ASD (Troyb et al., 2016).
Age
Before age 2 or 3, it can be challenging to distinguish children with ASD from children with other developmental delays based on the presence of RRBs (Lord, 1995; Stone et al., 1999), especially when observing a child in one setting or asking parents about RRBs. With recorded videos, detailed coding, or specific screening of these behaviors researchers have found that children who develop ASD show more RRBs than their typically developing peers even in the first 2 years of life (Elison et al., 2014; Morgan et al., 2008; Turner-Brown, Baranek, Reznick, Watson, & Crais, 2013; Watt et al., 2008). Thus, the symptoms are present early in life; RSM behaviors seem to decrease over time while insistence on sameness behaviors may increase over time (Richler et al., 2010; Watt et al., 2008).
Sleep
Many children with ASD have some kind of difficulty with sleep, whether it is difficulty falling asleep, staying asleep, or waking (Hollway & Aman, 2011). Decreased sleep is associated with a range of symptoms, including RRBs in children with ASD. In some cases, RRBs may interfere with the process of going to sleep (Richdale & Schreck, 2009). For example, a child may have ritualistic behavior around bedtime that is hard to interrupt. Or, the relationship could go the other way, with decreased sleep leading to increased RRBs (Abel, Schwichtenberg, Brodhead, & Christ, 2018). Some research suggests that decreased sleep is particularly associated with increases in repetitive and stereotyped movements (Hundley, Shui, & Malow, 2016). It is likely that the relationship between RRB and sleep is bidirectional—suggesting that changes in either area may affect the other (Hollway & Aman, 2011).
Gender
In young children with ASD, there do not seem to be differences between males and females and severity of RRB. At older ages findings are mixed, but there is preliminary evidence that RRB symptoms may be worse in males than females (Harrop, Gulsrud, & Kasari, 2015; Knutsen, Crossman, Perrin, Shui, & Kuhlthau, 2019; Van Wijngaarden-Cremers et al., 2014).
Family Well-Being
Many families become involved in their child’s ritualistic behavior—imagine the child who screams whenever he arrives at the park to discover he does not have his train to carry around with him. His caregiver must decide whether to return home to retrieve the train (and prevent screaming in public) or to allow and manage the screaming in hope that the child will calm down quickly. These decisions are challenging in the moment as both have immediate negative consequences for the parent (e.g., screaming or added driving). Making decisions to prevent screaming may inadvertently increase the rigidity the child has around having access to that object. It is not surprising, then, that high levels of parent stress have been documented for children with ASD in numerous studies (see Hayes & Watson, 2013, for a review) and that parent stress is frequently associated with challenging and/or RRBs. Parents find RRBs particularly difficult to manage in their daily lives, even more challenging than communication symptoms (Bishop, Richler, Cain, & Lord, 2007; Lecavalier, Leone, & Wiltz, 2006). When RRBs increase, parent stress may increase (Harrop, McBee, & Boyd, 2016). In addition, increased parent stress can negatively impact outcomes of early intervention (Osborne, McHugh, Saunders, & Reed, 2008).
In sum, RRBs are observable early in a child’s life, with atypicalities present as early as 12 months. Some of these behaviors decrease across development, such as RSM behaviors, while insistence on sameness behaviors tends to increase over time, particularly during early childhood (Richler et al., 2010). These changes in patterns of the display of RRBs are mirrored by changes in parent stress; as RRBs decrease, so do parenting stress ratings (Harrop, McBee, et al., 2016). Sleep may play a significant role in RRBs.
Why Do Children Engage in RRBs?
Consider a 2-year-old child who is repetitively lining up his crayons in a precise way. When his brother suggests they play with blocks, he does not look over to see what is going on because the crayons are holding his attention. Thus, he misses the opportunity to engage with his brother and play with something different. When it is time to clean up and move to meal time, he becomes upset because he does not have his line of crayons perfect yet. So, he misses the family meal. Finally, because he is so focused on color arrangement of his crayons, he resists when his mother tries to teach him to color with them. These three examples of missed opportunities highlight some of the negative consequences of RRBs on child learning and development. When asked, his parents might describe this behavior differently, however. They may see this behavior as a strength, as their son knows all the colors in a 128-pack of crayons and can count to 128 at a really early age.
Why do children with ASD engage in RRBs? Do individuals with ASD have lower social motivation and higher motivation to engage with objects? Or, is their entire brain circuitry dysregulated such that reward is processed differently for both social interaction and engagement with objects? Do children with autism have difficulty shifting their attention from one thing to another leading to extended focus on one activity? Researchers have explored these theories, and found some support for many of them along with differences in both the brain size and function that may contribute to development and maintenance of RRBs (Bodfish, Symons, Parker, & Lewis, 2000; Boyd, McDonough, Rupp, Khan, & Bodfish, 2011; Dichter et al., 2012; Klin, Jones, Schultz, Volkmar, & Cohen, 2002; Pierce, Glad, & Schreibman, 1997; Troyb et al., 2016; Turner, 1999).
While there is no one answer to explain the myriad of RRB manifestations, engagement in RRBs can cause a child to miss potential learning opportunities starting early in development. Thus, early intervention has the potential to increase learning opportunities by addressing RRBs and expanding the range of adaptive skills a child develops.
Effects of Early Intervention on RRBs
A majority of early intervention research has focused on promoting early social communication skills rather than on reducing RRBs. Yet there are several focused interventions that specifically target reduction of RRBs, and a range of comprehensive treatment approaches that aim to reduce RRB among a wide range of other treatment targets (e.g., increase communication). We review findings from both below.
Comprehensive Treatment Models
Despite the growing number of comprehensive treatment models (Lee, Odom, & Loftin, 2007) demonstrating positive effects on cognitive, communication, and adaptive skills, there is less evidence of their effects on RRBs. For example, research on Early Intensive Behavioral intervention (EIBI; see Chap. 5), TEACCH (see Chap. 7), Early Start Denver Model (ESDM; see Chap. 6), and Learning Experiences and Alternate Program for Preschoolers and their Parents (LEAP) has shown limited immediate effects on RRBs, despite positive changes in other areas (e.g., Boyd et al., 2014; Dawson et al., 2010; Reichow, Hume, Barton, & Boyd, 2018). There are many possible reasons for these findings. First, high-quality studies of comprehensive treatment models often measure symptom change in a global way. For example, parents might complete a symptom inventory of all types of RRBs, before and after treatment. If the total score increases, it means there are more behaviors and/or the behaviors are more problematic. If the score decreases, it means that there are fewer behaviors and/or the behaviors are less problematic. While this measure tells a lot about overall severity of RRBs, it may be too broad to detect slight changes in specific RRBs that result from intervention.
A second reason why comprehensive treatment models may not have shown positive effects on RRBs in early childhood is the natural progression of these behaviors. Research has shown that RSM often decreases across early childhood. Thus, detecting a treatment effect on top of natural decreases is challenging. In contrast, insistence on sameness or higher-order RRBs may increase during these years, making it even more challenging to show improvement.
Finally, many comprehensive treatment models are designed to focus primarily on social communication and adaptive functioning. Theoretically, as adaptive skills increase (e.g., a child learns to play with more toys or ask for help), RRBs would decrease as a result. If this theory is valid, it might be the case that RRBs would show a decrease long after an intervention is complete rather than immediately after it ends. Some evidence supports this theory, as a 2-year follow up study of ESDM showed more effects of ESDM on RRB 2 years later than immediately after ESDM was implemented (Estes et al., 2015).
In sum, while the evidence of effects of comprehensive treatment models on RRB is limited, research is ongoing. As stated, these models often emphasize building skills rather than reducing symptoms. Where research has shown more positive effects is when examining focused intervention practices whose specific target is reduction of a specific behavior. We review these below.
Focused Intervention Practices
The principles of applied behavior analysis (ABA) and cognitive behavioral therapy (CBT) underlie the focused approaches shown to reduce RRBs. ABA techniques aim to reduce or increase a specific behavior by changing the contingencies under which the behavior occurs. Behaviors occur in an antecedent–behavior–consequence context (ABC; see Chaps. 1 and 5), and efforts to change behavior focus on modifying either the antecedent or the consequence associated with the behavior. Imagine the situation of a child entering a loud preschool classroom. Upon entering, the child covers his ears and rocks his body. His parent then takes his hands off his ears and says, “hands down.” The behavior is covering ears, the antecedent is the loudness in the classroom setting, and the consequence is the physical movement of the child’s hands and verbal direction. ABA techniques to reduce these behaviors focus on changing antecedents or consequences. CBT techniques are similar to ABA, but also consider internal states (e.g., thoughts and feelings) in addition to the ABCs of behavior.
In their review of interventions targeting RRBs, Boyd and colleagues organized successful approaches to reducing RRBs into three categories: consequence-based interventions that interrupt the reinforcement provided by an RRB, antecedent-based interventions that reduce the likelihood of the occurrence of an RRB by altering the environment, and antecedent-based interventions that enrich skills or the environment that may consequently affect the presence of RRBs (Boyd, McDonough, & Bodfish, 2012). For simplicity, we group these as (1) preventing RRBs and (2) changing consequences to RRBs below.
Preventing RRB
Several practices have effectively reduced RRBs by aiming to prevent their occurrence; if we know the contexts in which the behavior occurs, we can change the environment to prevent the behavior and/or teach alternative skills to use instead of an RRB. As illustrated in the following sections, using visual schedules and cues, schedule variation, exercise, and functional communication training are all research-supported approaches for reducing RRBs in this way.
Functional communication training (FCT; Kennedy, Meyer, Knowles, & Shukla, 2000) and similar approaches involve teaching an individual a more appropriate skill, such as a communication or play skill that may serve the same function as an RRB. Consider this scenario. A young child flaps his hands often at school. A functional analysis determined that this behavior occurs most often when a teacher gives a demand, such as “time to clean up,” suggesting that the function of this stereotyped behavior is avoiding a demand. FCT would then teach this child a more appropriate way to get the same result. For example, a therapist might teach a communicative behavior such as signing “break” to request a break from the demand. Teaching more adaptive skills is effective for reducing stereotypies and self-injurious behavior (Kennedy et al., 2000; Lee et al., 2007; Loftin, Odom, & Lantz, 2008; Rispoli, Camargo, Machalicek, Lang, & Sigafoos, 2014; Tiger, Hanley, & Bruzek, 2008).
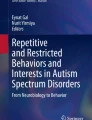
A second strategy for preventing RRB is using visual schedules and cues. Visual schedules are a component of the TEACCH Approach (Mesibov, Shea, & Schopler, 2006; see Chap. 7) and involve providing visual cues at the developmental level of the child to let the child know what will happen next. Schedules vary in form (e.g., objects, pictures, and written lists) and length (e.g., what is next, two-step, part day, full day). In the context of RRBs, it can be useful to schedule time for when a child can engage in RRB. For example, showing the child that first he must play outside and then he can play on his tablet with picture cues may reduce attempts to bring the iPad to outdoor play (see Lequia, Machalicek, & Rispoli, 2012, for a review, and see Fig. 4.1 for an example of this type of schedule). Using visual cues about upcoming changes in an activity or routine (Horner, Day, & Day, 2006) may also reduce RRBs. This approach may help a child who asks repeated questions about the weather. Placing a time on the schedule when it is appropriate to discuss the weather may reduce weather-talk at other times of day.

Examples of visual schedules
Engaging in physical exercise can also reduce RRB (Bahrami, Movahedi, Marandi, & Abedi, 2012; Kasner, Reid, & MacDonald, 2012; Schmitz Olin et al., 2017). Some research shows an immediate effect, with RRB reduced immediately after a period of exercise. Other studies show more global reductions in RRB after a period of exercise training.
Finally, treatment of sleep problems can lead to reduced RRBs (Malow et al., 2012, 2014; Reed et al., 2009). Approaches including educating parents about sleep hygiene, behavioral interventions to decrease insomnia, and melatonin have all shown promise as ways to improve sleep that also lead to decreases in repetitive and other challenging behavior.
Changing Consequences to RRB
Many studies have explored how to change the consequences associated with RRBs. Harrop and colleagues (2016) studied family reactions to RRB in the home and found that caregivers respond to about half of the RRB their children displayed. These caregivers were more likely to redirect behaviors that involved objects (e.g., visually inspecting objects and shaking objects) than to motor or verbal behaviors (e.g., flapping hands or repetitive sounds). Parents’ physical and verbal strategies to stop the child from engagement in the behaviors were rated as the most effective in stopping RRBs (Harrop, Gulsrud, Shih, Hovsepyan, & Kasari, 2016). Examples of approaches that aim to reduce RRB by changing consequences include blocking or response interruption and redirection, differential reinforcement, as well as exposure and response prevention. These are each described below.
Response interruption and redirection involves interrupting an RRB and redirecting the child to a different action (Ahearn, Clark, MacDonald, & In Chung, 2007; Boyd et al., 2011; Koegel, Firestone, Kramme, & Dunlap, 1974; Liu-gitz & Banda, 2010). For example, a father sees his daughter holding a block close to her eye. He then physically interrupts this behavior by placing his hands over her hand and the object, and redirects her to a different behavior, such as placing the block on another to begin making a tower. This approach can both reduce stereotyped behavior and increase more adaptive behavior.
Differential reinforcement entails reinforcement of certain behaviors (e.g., adaptive skills and varying play skills) while not reinforcing other behaviors (e.g., RRB). It can target a range of goals, such as increasing flexible and novel engagement with routines and toys (Azrin, Besalel, Jamner, & Caputo, 1988; Boyd et al., 2011; Miller & Neuringer, 2000). For example, a teacher responds with specific verbal praise whenever seeing a child using a toy in a new way while ignoring repetitive use of the toy.
Finally, exposure and response prevention (ERP; (Huppert & Franklin, 2005) is a CBT approach to reducing symptoms in people with obsessive compulsive disorder (OCD). This approach has been evaluated in children with ASD because of the partial overlap in symptoms between ASD and OCD (e.g., individuals with both conditions can be observed engaging in repetitive behavior such as opening and closing doors; see Klin et al., 2007; Postorino et al., 2017; Scahill & Challa, 2016 for reviews on the similarities and differences between RRBs and OCD symptoms). ERP involves building up skills to handle challenging or fearful situations, and then gradually exposing the child step-by-step to that situation. Thus, the specific RRB characteristics targeted for children with ASD have been rigidity and need for sameness. Consider a child who gets upset when he wants to complete a jigsaw puzzle in a particular order and becomes upset when he is unable to complete it that way. This intervention would entail step-by-step exposure to completing a puzzle in a different way. Results have shown that these approaches reduce rigidity and accompanying anxiety in children with ASD (Boyd, Woodard, & Bodfish, 2013; Eilers & Hayes, 2015; Reaven & Hepburn, 2003), though they have only been tested with older children to date.
Parent Training
RRBs can be difficult for parents to deal with in daily life (Harrop, McBee, et al., 2016). Thus, it is important to ensure parents and caregivers are equipped with a strong understanding of these symptoms as well as approaches that can be useful to daily life. Teaching parents about behavioral inflexibility in ASD, providing parent to parent support, and teaching parents evidence-supported strategies to prevent and respond to RRBs can be helpful (Boyd et al., 2011; Grahame et al., 2015; Lin & Koegel, 2018).
Incorporating Child RRBs in Learning Activities
A common strategy across a range of intervention approaches entails using one RRB characteristic, circumscribed interests, as a way to engage and reward children with ASD. For example, a 4-year-old child in a preschool class loves to play with blocks and cars but refuses to participate in art activities. One strategy to increase his participation in art might be to include cars in the art activity by dipping wheels in paint and rolling the cars on paper to make a pattern. By using this child’s special interest in cars, the teacher increases his engagement in art and provides more opportunities for peer interaction as the child is able to participate in a group activity. Research supports this strategy (Boyd, Conroy, Mancil, Nakao, & Alter, 2007; Gunn & Delafield-Butt, 2016). This approach also reflects the notion that the talents that may develop from these interests (e.g., a strong vocabulary of dinosaur names or states and capitals) are valuable, positive, and a true strength for the individual with ASD.
Pharmacotherapies
Despite considerable research on the efficacy of a range of medications on RRBs, only buspirone currently shows promise to reduce these symptoms in children with ASD. Buspirone is a serotonin agonist generally used to treat anxiety in children and has been associated with improvement in RRBs (Chugani et al., 2016). Other medications have not led to reduction in RRB symptoms, including serotonin receptor inhibitors (Accordino, Kidd, Politte, Henry, & Mcdougle, 2016; Carrasco, Volkmar, & Bloch, 2012).
Conclusion
RRBs are present early in life and can cause significant impairment in development and lead to increase in parent stress and other mental health challenges in children with ASD. Several focused intervention practices including prevention of RRB and changing consequences to RRB are effective for reducing RRB, and supporting parents may have lasting positive effects on the child and family. In addition, some RRBs, such as circumscribed interests provide a way to reach and engage with a child who may be challenging to engage in typical ways. These interests may also develop into strengths to be promoted throughout life.
Change history
24 December 2020
Mary Kate Frisch provided her valuable contribution to chapter 4 “Understanding and Addressing Restricted and Repetitive Behaviors in Children with Autism” of this book.
References
Abel, E. A., Schwichtenberg, A. J., Brodhead, M. T., & Christ, S. L. (2018). Sleep and challenging behaviors in the context of intensive behavioral intervention for children with autism. Journal of Autism and Developmental Disorders, 48(11), 3871–3884. https://doi.org/10.1007/s10803-018-3648-0
Accordino, R. E., Kidd, C., Politte, L. C., Henry, C. A., & Mcdougle, C. J. (2016). Expert opinion on pharmacotherapy psychopharmacological interventions in autism spectrum disorder Psychopharmacological interventions in autism spectrum disorder. Expert Opinion on Pharmacotherapy, 17(7), 937–952. https://doi.org/10.1517/14656566.2016.1154536
Ahearn, W. H., Clark, K. M., MacDonald, R. P., & In Chung, B. (2007). Assessing and treating vocal stereotypy in children with autism. Journal of Applied Behavior Analysis, 40(2), 263–275. https://doi.org/10.1901/jaba.2007.30-06
American Psychiatric Association. (2013). Diagnostic and statistical manual or mental disorders (5th ed.). doi: https://doi.org/10.1176/appi.books.9780890425596.744053.
Ausderau, K. K., Furlong, M., Sideris, J., Bulluck, J., Little, L. M., Watson, L. R., … Baranek, G. T. (2014). Sensory subtypes in children with autism spectrum disorder: Latent profile transition analysis using a national survey of sensory features. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 55(8), 935–944. https://doi.org/10.1111/jcpp.12219
Azrin, N. H., Besalel, V. A., Jamner, J. P., & Caputo, J. N. (1988). Comparative study of behavioral methods of treating severe self-injury. Behavioral Residential Treatment, 3(2), 119–152.
Bahrami, F., Movahedi, A., Marandi, S. M., & Abedi, A. (2012). Kata techniques training consistently decreases stereotypy in children with autism spectrum disorder. Research in Developmental Disabilities, 33(4), 1183–1193. https://doi.org/10.1016/j.ridd.2012.01.018
Bishop, S. L., Hus, V., Duncan, A., Huerta, M., Gotham, K., Pickles, A., … Lord, C. (2013). Subcategories of restricted and repetitive behaviors in children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 43(6), 1287–1297. https://doi.org/10.1007/s10803-012-1671-0
Bishop, S. L., Richler, J., Cain, A. C., & Lord, C. (2007). Predictors of perceived negative impact in mothers of children with autism spectrum disorder. American Journal of Mental Retardation: AJMR, 112(6), 450–461. https://doi.org/10.1352/0895-8017(2007)112[450:POPNII]2.0.CO;2
Bishop, S. L., Richler, J., & Lord, C. (2006). Association between restricted and repetitive behaviors and nonverbal IQ in children with autism spectrum disorders. Child Neuropsychology, 12(4–5), 247–267. https://doi.org/10.1080/09297040600630288
Bodfish, J. W., Symons, F. J., Parker, D. E., & Lewis, M. H. (2000). Varieties of repetitive behavior in autism: Comparisons to mental retardation. Journal of Autism and Developmental Disorders, 30(3), 237–243.
Boyd, B. A., Conroy, M. A., Mancil, G. R., Nakao, T., & Alter, P. J. (2007). Effects of circumscribed interests on the social behaviors of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37(8), 1550–1561. https://doi.org/10.1007/s10803-006-0286-8
Boyd, B. A., Hume, K., McBee, M. T., Alessandri, M., Gutierrez, A., Johnson, L. A., … Odom, S. L. (2014). Comparative efficacy of LEAP, TEACCH and non-model-specific special education programs for preschoolers with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(2), 366–380. https://doi.org/10.1007/s10803-013-1877-9
Boyd, B. A., McDonough, S. G., & Bodfish, J. W. (2012). Evidence-based behavioral interventions for repetitive behaviors in autism. Journal of Autism and Developmental Disorders, 42(6), 1236–1248. https://doi.org/10.1007/s10803-011-1284-z
Boyd, B. A., McDonough, S. G., Rupp, B., Khan, F., & Bodfish, J. W. (2011). Effects of a family-implemented treatment on the repetitive behaviors of children with autism. Journal of Autism and Developmental Disorders, 41(10), 1330–1341. https://doi.org/10.1007/s10803-010-1156-y
Boyd, B. A., Woodard, C. R., & Bodfish, J. W. (2013). Feasibility of exposure response prevention to treat repetitive behaviors of children with autism and an intellectual disability: A brief report. Autism: The International Journal of Research and Practice, 17(2), 196–204. https://doi.org/10.1177/1362361311414066
Carrasco, M., Volkmar, F. R., & Bloch, M. H. (2012). Pharmacologic treatment of repetitive behaviors in autism spectrum disorders: Evidence of publication bias. Pediatrics, 129(5), e1301–e1310. https://doi.org/10.1542/peds.2011-3285
Chugani, D. C., Chugani, H. T., Wiznitzer, M., Parikh, S., Evans, P. A., Hansen, R. L., … Hirtz, D. (2016). Efficacy of low-dose buspirone for restricted and repetitive behavior in young children with autism spectrum disorder: A randomized trial. Journal of Pediatrics, 170, 45–53e4. https://doi.org/10.1016/j.jpeds.2015.11.033
Dawson, G., Rogers, S., Munson, J., Smith, M., Winter, J., Greenson, J., … Varley, J. (2010). Randomized, controlled trial of an intervention for toddlers with autism: The early start denver model. Pediatrics, 125(1), e17–e23. https://doi.org/10.1542/peds.2009-0958
Dichter, G. S., Felder, J. N., Green, S. R., Rittenberg, A. M., Sasson, N. J., & Bodfish, J. W. (2012). Reward circuitry function in autism spectrum disorders. Social Cognitive and Affective Neuroscience, 7(2), 160–172. https://doi.org/10.1093/scan/nsq095
Eilers, H. J., & Hayes, S. C. (2015). Exposure and response prevention therapy with cognitive defusion exercises to reduce repetitive and restrictive behaviors displayed by children with autism spectrum disorder. Research in Autism Spectrum Disorders, 19, 18–31. https://doi.org/10.1016/j.rasd.2014.12.014
Elison, J. T., Wolff, J. J., Reznick, J. S., Botteron, K. N., Estes, A. M., Gu, H., … Piven, J. (2014). Repetitive behavior in 12-month-olds later classified with autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 53(11), 1216–1224. https://doi.org/10.1016/j.jaac.2014.08.004
Estes, A., Munson, J., Rogers, S. J., Greenson, J., Winter, J., & Dawson, G. (2015). Long-term outcomes of early intervention in 6-year-old children with autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 54(7), 580–587. https://doi.org/10.1016/j.jaac.2015.04.005
Evans, D. W., Leckman, J. F., Carter, A., Reznick, S. J., Henshaw, D., King, R. A., & Pauls, D. (1997). Ritual, habit, and perfectionism: The prevalence and development of compulsive-like behavior in normal young children. Child Development, 68(1), 58–68.
Grahame, V., Brett, D., Dixon, L., McConachie, H., Lowry, J., Rodgers, J., … Le Couteur, A. (2015). Managing repetitive behaviours in young children with autism spectrum disorder (ASD): Pilot randomised controlled trial of a new parent group intervention. Journal of Autism and Developmental Disorders, 45(10), 3168–3182. https://doi.org/10.1007/s10803-015-2474-x
Gunn, K. C. M., & Delafield-Butt, J. T. (2016). Teaching children with autism spectrum disorder with restricted interests. Review of Educational Research, 86(2), 408–430. https://doi.org/10.3102/0034654315604027
Harrop, C., Gulsrud, A., & Kasari, C. (2015). Does gender moderate core deficits in ASD? An investigation into restricted and repetitive behaviors in girls and boys with ASD. Journal of Autism and Developmental Disorders, 45(11), 3644–3655. https://doi.org/10.1007/s10803-015-2511-9
Harrop, C., Gulsrud, A., Shih, W., Hovsepyan, L., & Kasari, C. (2016). Characterizing caregiver responses to restricted and repetitive behaviors in toddlers with autism spectrum disorder. Autism, 20(3), 330–342. https://doi.org/10.1177/1362361315580443
Harrop, C., McBee, M., & Boyd, B. A. (2016). How are child restricted and repetitive behaviors associated with caregiver stress over time? A parallel process multilevel growth model. Journal of Autism and Developmental Disorders, 46(5), 1773–1783. https://doi.org/10.1007/s10803-016-2707-7
Hayes, S. A., & Watson, S. L. (2013). The impact of parenting stress: A meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. Journal of Autism and Developmental Disorders, 43(3), 629–642. https://doi.org/10.1007/s10803-012-1604-y
Hollway, J. A., & Aman, M. G. (2011). Sleep correlates of pervasive developmental disorders: A review of the literature. Research in Developmental Disabilities, 32(5), 1399–1421. https://doi.org/10.1016/j.ridd.2011.04.001
Horner, R. H., Day, H. M., & Day, J. R. (2006). Using neutralizing routines to reduce problem behaviors. Journal of Applied Behavior Analysis, 30(4), 601–614. https://doi.org/10.1901/jaba.1997.30-601
Hundley, R. J., Shui, A., & Malow, B. A. (2016). Relationship between subtypes of restricted and repetitive behaviors and sleep disturbance in autism spectrum disorder. Journal of Autism and Developmental Disorders, 46(11), 3448–3457. https://doi.org/10.1007/s10803-016-2884-4
Huppert, J. D., & Franklin, M. E. (2005). Cognitive behavioral therapy for obsessive-compulsive disorder: An update. Current Psychiatry Reports, 7(4), 268–273. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/16098280.
Kanner, L. (1943). Autistic disturbances of affective contact. The Nervous Child, 2, 217–250.
Kasner, M., Reid, G., & MacDonald, C. (2012). Evidence-based practice: Quality indicator analysis of antecedent exercise in autism spectrum disorders. Research in Autism Spectrum Disorders, 6(4), 1418–1425. https://doi.org/10.1016/j.rasd.2012.02.001
Kennedy, C. H., Meyer, K. A., Knowles, T., & Shukla, S. (2000). Analyzing the multiple functions of stereotypical behavior for students with autism: Implications for assessment and treatment. Journal of Applied Behavior Analysis, 33(4), 559–571.
Klin, A., Danovitch, J. H., Merz, A. B., & Volkmar, F. R. (2007). Circumscribed interests in higher functioning individuals with autism spectrum disorders: An exploratory study. Research and Practice for Persons with Severe Disabilities, 32(2), 89–100. https://doi.org/10.2511/rpsd.32.2.89
Klin, A., Jones, W., Schultz, R., Volkmar, F., & Cohen, D. (2002). Visual fixation patterns during viewing of naturalistic social situations as predictors of social competence in individuals with autism. Archives of General Psychiatry, 59(9), 809. https://doi.org/10.1001/archpsyc.59.9.809
Knutsen, J., Crossman, M., Perrin, J., Shui, A., & Kuhlthau, K. (2019). Sex differences in restricted repetitive behaviors and interests in children with autism spectrum disorder: An Autism Treatment Network study. Autism, 23(4), 858–868. https://doi.org/10.1177/1362361318786490
Koegel, R. L., Firestone, P. B., Kramme, K. W., & Dunlap, G. (1974). Increasing spontaneous play by suppressing sel-stimulation in autistic children. Journal of Applied Behavior Analysis, 7(4), 521–528.
Lam, K. S. L., Bodfish, J. W., & Piven, J. (2008). Evidence for three subtypes of repetitive behavior in autism that differ in familiality and association with other symptoms. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 49(11), 1193–1200. https://doi.org/10.1111/j.1469-7610.2008.01944.x
Lecavalier, L., Leone, S., & Wiltz, J. (2006). The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. Journal of Intellectual Disability Research, 50(3), 172–183. https://doi.org/10.1111/j.1365-2788.2005.00732.x
Lee, S., Odom, S. L., & Loftin, R. (2007). Social engagement with peers and stereotypic behavior of children with autism. Journal of Positive Behavior Interventions, 9(2), 67–79.
Lequia, J., Machalicek, W., & Rispoli, M. J. (2012). Effects of activity schedules on challenging behavior exhibited in children with autism spectrum disorders: A systematic review. Research in Autism Spectrum Disorders, 6(1), 480–492. https://doi.org/10.1016/j.rasd.2011.07.008
Lin, C. E., & Koegel, R. (2018). Treatment for higher-order restricted repetitive behaviors (H-RRB) in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 48(11), 3831–3845. https://doi.org/10.1007/s10803-018-3637-3
Liu-gitz, L., & Banda, D. R. (2010). A replication of the rird strategy to decrease vocal stereotypy in a student with autism. Behavioral Interventions, 25, 77–87. https://doi.org/10.1002/bin
Loftin, R. L., Odom, S. L., & Lantz, J. F. (2008). Social interaction and repetitive motor behaviors. Journal of Autism and Developmental Disorders, 38, 1124–1135. https://doi.org/10.1007/s10803-007-0499-5
Lord, C. (1995). Follow-up of two-year-olds referred for possible autism. Journal of Child Psychology and Psychiatry, 36(8), 1365–1382. https://doi.org/10.1111/j.1469-7610.1995.tb01669.x
Malow, B., Adkins, K. W., McGrew, S. G., Wang, L., Goldman, S. E., Fawkes, D., & Burnette, C. (2012). Melatonin for sleep in children with autism: A controlled trial examining dose, tolerability, and outcomes. Journal of Autism and Developmental Disorders, 42(8), 1729–1737; author reply 1738. https://doi.org/10.1007/s10803-011-1418-3
Malow, B., Adkins, K. W., Reynolds, A., Weiss, S. K., Loh, A., Fawkes, D., … Clemons, T. (2014). Parent-based sleep education for children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(1), 216–228. https://doi.org/10.1007/s10803-013-1866-z
Mesibov, G. B., Shea, V., & Schopler, E. (2006). The TEACCH approach to autism spectrum disorders. New York, NY: Springer.
Miller, N., & Neuringer, A. (2000). Reinforcing variability in adolescents with autism. Journal of Applied Behavior Analysis, 33(2), 151–165. https://doi.org/10.1901/jaba.2000.33-151
Morgan, L., Wetherby, A. M., & Barber, A. (2008). Repetitive and stereotyped movements in children with autism spectrum disorders late in the second year of life. Journal of Child Psychology and Psychiatry, 49(8), 826–837. https://doi.org/10.1111/j.1469-7610.2008.01904.x
Osborne, L. A., McHugh, L., Saunders, J., & Reed, P. (2008). Parenting stress reduces the effectiveness of early teaching interventions for autistic spectrum disorders. Journal of Autism and Developmental Disorders, 38(6), 1092–1103. https://doi.org/10.1007/s10803-007-0497-7
Pierce, K., Glad, K. S., & Schreibman, L. (1997). Social perception in children with autism: An attentional deficit? Journal of Autism and Developmental Disorders, 27(3), 265–282. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9229258.
Postorino, V., Kerns, C. M., Vivanti, G., Bradshaw, J., Siracusano, M., & Mazzone, L. (2017). Anxiety disorders and obsessive-compulsive disorder in individuals with autism spectrum disorder. Current Psychiatry Reports, 19(12), 92. https://doi.org/10.1007/s11920-017-0846-y
Reaven, J., & Hepburn, S. (2003). Cognitive-behavioral treatment of obsessive-compulsive disorder in a child with Asperger syndrome: A case report. Autism, 7(2), 145–164.
Reed, H. E., McGrew, S. G., Artibee, K., Surdkya, K., Goldman, S. E., Frank, K., … Malow, B. (2009). Parent-based sleep education workshops in autism. Journal of Child Neurology, 24(8), 936–945. https://doi.org/10.1177/0883073808331348
Reichow, B., Hume, K., Barton, E. E., & Boyd, B. A. (2018). Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). The Cochrane Database of Systematic Reviews, 5, CD009260. https://doi.org/10.1002/14651858.CD009260.pub3
Richdale, A. L., & Schreck, K. A. (2009). Sleep problems in autism spectrum disorders: Prevalence, nature, & possible biopsychosocial aetiologies. Sleep Medicine Reviews, 13(6), 403–411. https://doi.org/10.1016/j.smrv.2009.02.003
Richler, J., Huerta, M., Bishop, S. L., & Lord, C. (2010). Developmental trajectories of restricted and repetitive behaviors and interests in children with autism spectrum disorders. Development and Psychopathology, 22(1), 55–69. https://doi.org/10.1017/S0954579409990265
Rispoli, M., Camargo, S., Machalicek, W., Lang, R., & Sigafoos, J. (2014). Functional communication training in the treatment of problem behavior maintained by access to rituals. Journal of Applied Behavior Analysis, 47(3), 580–593. https://doi.org/10.1002/jaba.130
Scahill, L., & Challa, S. A. (2016). Repetitive behavior in children with autism spectrum disorder: Similarities and differences with obsessive-compulsive disorder. In L. Mazzone & B. Vitiello (Eds.), Psychiatric symptoms and comorbidities in autism spectrum disorders. Berlin: Springer.
Schertz, H. H., Odom, S. L., Baggett, K. M., & Sideris, J. H. (2016). Parent-reported repetitive behavior in toddlers on the autism spectrum. Journal of Autism and Developmental Disorders, 46(10), 3308–3316. https://doi.org/10.1007/s10803-016-2870-x
Schmitz Olin, S., McFadden, B. A., Golem, D. L., Pellegrino, J. K., Walker, A. J., Sanders, D. J., & Arent, S. M. (2017). The effects of exercise dose on stereotypical behavior in children with autism. Medicine and Science in Sports and Exercise, 49(5), 983–990. https://doi.org/10.1249/MSS.0000000000001197
Shafer, R. L., Newell, K. M., Lewis, M. H., & Bodfish, J. W. (2017). A cohesive framework for motor stereotypy in typical and atypical development: The role of sensorimotor integration. Frontiers in Integrative Neuroscience, 11, 1–8. https://doi.org/10.3389/fnint.2017.00019
Stone, W. L., Lee, E. B., Ashford, L., Brissie, J., Hepburn, S. L., Coonrod, E. E., & Weiss, B. H. (1999). Can autism be diagnosed accurately in children under 3 years? Journal of Child Psychology and Psychiatry, and Allied Disciplines, 40(2), 219–226. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/10188704.
Tiger, J. H., Hanley, G. P., & Bruzek, J. (2008). Functional communication training: A review and practical guide. Behavior Analysis in Practice, 1(1), 16–23. Retrieved from www.abainternational.
Troyb, E., Knoch, K., Herlihy, L., Stevens, M. C., Chen, C. M., Barton, M., … Fein, D. (2016). Restricted and repetitive behaviors as predictors of outcome in autism spectrum disorders. Journal of Autism and Developmental Disorders, 46(4), 1282–1296. https://doi.org/10.1007/s10803-015-2668-2
Turner, M. (1999). Annotation: Repetitive behaviour in autism: A review of psychological research. Journal of Child Psychology and Psychiatry, 40(6), 839–849. https://doi.org/10.1111/1469-7610.00502
Turner-Brown, L. M., Baranek, G. T., Reznick, J. S., Watson, L. R., & Crais, E. R. (2013). The first year inventory: A longitudinal follow-up of 12-month-old to 3-year-old children. Autism, 17(5), 527–540. https://doi.org/10.1177/1362361312439633
Van Wijngaarden-Cremers, P. J. M., Van Eeten, E., Groen, W. B., Van Deurzen, P. A., Oosterling, I. J., & Van Der Gaag, R. J. (2014). Gender and age differences in the core triad of impairments in autism spectrum disorders: A systematic review and meta-analysis. Journal of Autism and Developmental Disorders, 44(3), 627–635. https://doi.org/10.1007/s10803-013-1913-9
Watt, N., Wetherby, A. M., Barber, A., & Morgan, L. (2008). Repetitive and stereotyped behaviors in children with autism spectrum disorders in the second year of life. Journal of Autism and Developmental Disorders, 38(8), 1518–1533. https://doi.org/10.1007/s10803-007-0532-8
Wolff, J. J., Botteron, K. N., Dager, S. R., Elison, J. T., Estes, A. M., Gu, H., … Piven, J. (2014). Longitudinal patterns of repetitive behavior in toddlers with autism. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 55(8), 945–953. https://doi.org/10.1111/jcpp.12207
Wolff, J. J., Boyd, B. A., & Elison, J. T. (2016). A quantitative measure of restricted and repetitive behaviors for early childhood. Journal of Neurodevelopmental Disorders, 8(1), 1–10. https://doi.org/10.1186/s11689-016-9161-x
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Turner-Brown, L., Frisch, M. (2020). Understanding and Addressing Restricted and Repetitive Behaviors in Children with Autism. In: Vivanti, G., Bottema-Beutel, K., Turner-Brown, L. (eds) Clinical Guide to Early Interventions for Children with Autism. Best Practices in Child and Adolescent Behavioral Health Care. Springer, Cham. https://doi.org/10.1007/978-3-030-41160-2_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-41160-2_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-41159-6
Online ISBN: 978-3-030-41160-2
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)