
Abstract
In this paper we focus on patient flows inside Internal Medicine Departments, with the aim of supporting new organizational models taking into account the patient relevant characteristics such as complexity and frailty. The main contribution of this paper is to develop a Discrete Event Simulation model to describe in detail the pathways of complex patients through medical hospital wards. The model has been applied to reproduce a case study of an Italian middle size hospital. The objective is quantifying the impact on resource use and outcome of introducing a new organizational model for medical departments. The re-organization is mainly focused on changing the available beds assignment among the wards to better address the complexity of care of patients with comorbidities. Following a patient-centered approach, patients are segmented considering the clinical characteristics (i.e. the pathology, proxy of Diagnoses Related Groups classification) and sub-grouped considering other characteristics, such as comorbidities and ward of admission. Then, an optimization component embedded into the model chooses the best pooling strategy to reorganize medical wards, determining the corresponding number of beds able to improve process indicators, such as length of stay. The simulation model is presented, and preliminary results are analyzed and discussed.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keyword
- Simulation-optimization
- Internal Medicine Ward organization
- Clinical pathway
- Hospitalist-based model
- Data segmentation
1 Introduction and Problem Addressed
In the last few years with the fast progress of medical knowledge, the education of doctors has evolved towards greater specialization. Within the medical area, many sub-specializations, such as cardiology, pulmonology, gastroenterology, geriatrics, etc., gemmated from Internal Medicine [2]. The need to investigate each medical condition has led, from an organizational point of view to the birth of different medical wards, each corresponding to a specific specialization [12]. Consequently, patients are today admitted to different wards depending on the prevalent clinical problem that led to the need for the hospital admission.
The problem arises from the fact that, to the greater specialization of medical knowledge, an evolution of the patient’s conditions in the opposite sense is observed. The presence of multiple-pathologies and social frailty represent the epidemic of the third millennium, and they are mining the sustainability of national and worldwide health systems [17]. This problem affects mostly patients admitted in hospital that have an age over 65 year old, with an average of 2.7 chronic diseases, requiring medical care for an acute transient condition, i.e. an infection, that triggers a decompensation of chronic condition or acute decompensated heart failure, and/or a complication such as diabetes onset [8]. The clinical complexity is increased by functional and cognitive decline, adverse events given by the use of multiple drugs, socioeconomic deprivation and poor familiar support. These patients, often called frail, require urgent organizational changes to address their health needs appropriately [5].
The first change to be addressed concerns the professional education of medical specialists who should regain their main characteristics, being doctors of complexity capable of treating the patient following a holistic approach. The appropriate professional figure, already introduced 20 years ago in the US, could be the “Hospitalist”, a medical specialist, more often a specialist in Internal Medicine hat should have the clinical, organizational and relational skills needed to the integrated care of complex patients with multi-pathologies [18]. The introduction of this new figure in a specialty-based hospital, however, is not sufficient to meet patient requirements, even if it seems to produce performance gain as literature proves [16, 19] but, in our opinion, it is not enough.
A second change is essential to take full advantage of this new professional figure, i.e. the reorganization of medical wards from specialty-based care to a patient-centered one. This change requires a cultural shift and a complete re-thinking of medical Departments, or even the whole hospital, where the divisions among sub-specialties should disappear. This does not mean, of course, that specialized cardiologists, pulmonologists, geriatricians and other specialized clinicians should disappear, but that they should not be assigned a specific ward. Instead, they should work in multidisciplinary teams coordinated by the global approach of the hospitalist. Some specialized units should remain for particularly severe intensive care such as the ICU for cardiac disease. This reconfiguration is the only one able to face the needs of new patients in the most appropriate clinical way as recent studies show it is a reconfiguration based on the patient and not on the hospital supply [4, 11]. However, before the introduction of organizational innovation, an evaluation of the expected impact should be carried on.
Whether this patient-centered reconfiguration also brings some advantages in terms of resource use and outcome to the traditional specialty-based one, is the specific aim of this work. The resource use is a proxy of the number of ward beds needed and costs for laboratory and diagnostics, while the outcome is assessed by means of the average length of stay. The main contribution of this paper is to develop a Discrete Event Simulation (DES) model to firstly reproduce the traditional (specialty-based) organization of a real case study and to evaluate the impact on resource utilization (beds and costs) and outcome (average length of stay) of re-organizing the stay areas using a patient-centered model. In the patient-centered model the specialist wards are merged into a unique Internal Medicine Ward (IMW) to better address the complexity of care of patients. Besides, the optimization component embedded in the DES model is used to determine the optimal (minimum) number of beds necessary to manage the overall cohort of patients flowing in the hospital IMWs following the patient-centered organizational model.
The paper is organized as follows: In Sect. 2, the study motivation is presented together with a brief description of the organizational models to be tested. Section 3 reports the case study, data collection, and analysis. In Sect. 4 the simulation model development is introduced, and some details of the methodology and assumptions are reported. The results given by the simulation-optimization for the case study are analyzed in Sect. 5. Finally, in Sect. 6, conclusions and future direction of the research are reported.
2 Study Motivation
This study began from a collaboration with a group of internists involved in an advanced master level course titled “Hospitalist: managing complexity in Internal Medicine inpatients”. The aim of the course was forming these internists as Hospitalist, for the Italian hospital sector. As reported in Sect. 1, Literature shows that the introduction of hospitalists in IMWs could result in reduced costs, shortened lengths of stay, preserved or even enhanced the quality of care and patient satisfaction, in essence improving the “value of care” [16, 19]. However, the introduction of this figure poses additional issues on how healthcare services should be organized around acute multi-pathology patients. At least, to the authors’ knowledge and experience, no studies are dealing with the evaluation of the re-organization of the stay area connected to the introduction of this new figure.
The organizational models herein compared are referred to as the specialty-based and the patient-centred model, respectively. The first reproduces the current practice where patients are admitted in a ward following the main acute clinical problem. Specialty-based hospitals cannot assure global and efficient care for multi-pathology and frailty of patients [15]. Their hospital stay will likely be fragmented in more, isolated episodes of care with transfers from the emergency department to other wards (e.g. infectious disease, cardiologic and metabolic wards). Movements among wards are uncomfortable and risky for patients. Transitions of care are invariably associated with loss of clinical information, duplication of tests, unintentional pharmacological discrepancies and much more. In the re-organization that follows the patient-centered model, the patient is admitted in a unique IMW where the hospitalist organizes and takes in charge the patient hospital stay managing a multidisciplinary medical team and assuring a holistic vision of the care.
Thanks to the collaboration of the clinicians involved in this study, we had the opportunity of collecting a large amount of clinical historical data of patients admitted in hospital with a diagnosis among the most prevalent in the Internal Medicine area. The inclusion criteria and the resulting cohort of patients analyzed are reported in Sect. 3. The clinical pathways of all patients with the same health problem, age, comorbidity conditions, severity of illness are analyzed with a focus on the differences in terms of resource use and outcome depending only on the organizational model: specialty-based or patient-centered. Starting with the data collected, a discrete event simulation model evaluates the benefits of introducing a patient-centered reconfiguration of the stay area in terms of resource use and outcome.
3 Case Study: Data Collection and Analysis
The case study herein reported refers to a Ligurian Local Health Authority (ASL5) sited in La Spezia province (Italy). ASL5 is one of the Local Health Authorities of Liguria Region. It provides, directly or through accredited public and private subjects, the following services: (i) services provided on the Essential Health Care Levels (LEA) in the form of district assistance and hospital care health services, (ii) high social and health integrated assistance, and (iii) emergency health services. It provides health services to 217,507 inhabitants (which 27.4% is over 65 years old). About 8500 inhabitants are frail and at risk of disability, while 8300 have a disability.
Administrative data coming from the Hospital Discharge Episodes Database (HDED) and medical data coming from Electronic Patient Record (EPR) collected from January 2016 to December 2016 were analyzed. The Hospital Discharge Report includes administrative data, as well as the date of admission and discharge, the transfers of the patient between wards, the diagnosis, and the DRG assigned. Data from EPR include all the tests and consultations (blood transfusion, specialist visits, diagnostic tests, laboratory tests, and other tests) performed to the patient during the hospital stay. The cost of these specialist and diagnostics services were provided by the Italian National Health System official tariff list. Other data were collected by the Hospital management accounting service.
The analysis is focused on the six medical wards reported in Table1, two of them (General Medicine 1 and General Medicine 2) are generic, and the other four are specialist wards. With reference to the pathologies to be included, as suggested by the hospital physicians involved in our study, the analysis focused on five Diagnosis Related Groups (DRGs) covering on average 70% of the total cases (DRG 087: Pulmonary edema and respiratory failure, DRG 089: Pneumonia and pleuritis with complications, DRG 090: Pneumonia and pleuritis >17 year old, DRG 127: Heart failure and shock, DRG 576: Sepsis without medical ventilation).
All DRGs are treated within each of the six wards. The total number of patients admitted by each ward depends on the different ward capacity in terms of resource, but they are not distributed exclusively following the prevalent condition. For instance, specialist wards, as cardiology and infectious diseases, admit patients with heart failure and sepsis, respectively, but also with respiratory problems.
As a consequence, patients with heart failure are almost equally distributed among cardiology, geriatrics and general medicine wards, while patients with pulmonary edema and respiratory failure are mostly managed by respiratory medicine and general medicine wards. This situation however, engenders different organizational processes leading to a different length of stay and an average cost of treatment for each patient at the parity of DRG, as pointed in Tables 2 and 3. For instance, the same condition Heart failure has a LOS ranging from 5.9 in the specialist ward Cardiology to 9.4 in General Medicine 2. There is a large variability also across wards about all wards: sometimes the difference is due to the specific treatment—this seems to be the case for the Infectious disease ward. However, in other cases, differences appear to be unjustified: for instance, General Medicine 1 has a larger average LOS for all the DRGs, while General Medicine 2 has on average three days less.
Large variability is also observed with regards to the average cost for each DRG (see Table 3). The average cost for each ward is given by the sum of different items: average utilization of diagnostics and laboratory and the average daily cost times the number of days.
The variability of the average cost depends, of course, by the clinical pathway (DRGs) requiring different bundle of services (diagnostics and so on), for instance in the case of Respiratory Medicine and Infectious Diseases. However, in other cases, as between General Medicine 1 and General Medicine 2, for the same DRG, the detected lower LOS seems to be justified by a different organizational model able to achieve larger productivity of the given beds and resources.
The comparison between the different organizational models for the same DRG, however, is correct only if patient complexity for each DRG is similar among the different wards. The analysis of the demographic and clinical data summarized in Tables 4 and 5 show large variability among the complexity of patients addressing different wards. Complexity is assessed by three characteristics drawn from administrative data (HDED): (i) demographic characteristics (age, sex); (ii) comorbidity status (measured by the Charlson Comorbidity Index; (iii) severity condition and mortality risk (APR-DRG classes).
The Charlson Comorbidity Index (CCI) was computed following the specific criteria reported in Deyo et al. [7]. The CCI is a method of categorizing comorbidities of patients based on the International Classification of Diseases (ICD) diagnosis codes reported in administrative data, such as electronic patient records. Seventeen comorbidity categories are included with associated weight (from 1 to 6), based on the adjusted risk of mortality or resource use, and the sum of all the weights provides a final comorbidity score for the patient. A score of zero indicates no comorbidities. The higher is the score, the more likely the predicted outcome will result in mortality or higher resource use. In this study, we use four classes of comorbidity with score values of 0, 1–2, 3–4 and more than 5 respectively.
The Patient Refined Diagnosis Related Group (APR-DRG), is an inpatient classification system that assigns a Diagnostic Related Group value, a Risk of Mortality subclass and a Severity of Illness subclass ranging from 1 to 4 in ascendant order of risk and severity [13]. Regarding the Clinical pathways, we mean the main disease condition causing hospitalization (proxy of DRG, coded using ICD9-CM v.24). In Table 4 for each ward are reported the demographic characteristics and the comorbidity status while in Table 5 the severity conditions, i.e. severity class and mortality risk.
General Medicine wards have the largest quantity of patients covering about 70% of the overall sample, while the smallest units in terms of patient treated are Cardiology and Infection diseases wards. More than half (63%) of overall patients are older than 80 years old, while the patients between 65 and 80 years old and the patients with less than 65 years old represent 27% and 10% of the cohort, respectively. Most of the patients have a CCI of 1–2 (48%) and 0 (42%). Patients with a CCI of 3–4 and larger than 5, are 8% and 2%, respectively A larger quantity of CCI 3–4 is present in the Geriatric unit (14%).
The most frequent APR severity class is 2 (60%), where in General Medicine 1 and Respiratory Medicine has a maximum of 67% and 77%, respectively. The 16% and 22% of patients have a severity class of 1 and 3, respectively, while only the 2% has a severity class of 4. The most frequent APR mortality risk is 2 (43%), where in Cardiology and Geriatric units has a maximum of 67% and 49%, respectively. The 17% and 35% of patients have a mortality risk of 1 and 3, respectively, while only the 5% has a mortality risk of 4. Infection and Immunology ward treat patients with higher APR values (both severity class and mortality risk). Geriatrics, Immunology and General Medicine 1 and 2 have at least the 30% of patients with a high risk of mortality (3 or 4). Different combinations of complexity characteristics for each Clinical Pathway (represented by the DRG) define groups of patients that should be homogeneous with respect to the resource use and cost. After this adjustment, the residual variability among wards is due only to different organizational models.
In the next section a simulation model is developed to evaluate the impact on resource utilization (beds and costs) and outcome (average length of stay) of merging all IMW into a unique ward following the best model.
4 Simulation Model Development
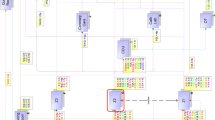
The adoption of simulation modeling in the healthcare context derives from the need to reproduce the system reality and to provide to the decision maker a good or optimal solution for health policies. Since the 1970s were published several scientific articles where simulation techniques were applied to analyze healthcare services [3, 9, 10]. DES is a simulation technique that was used widely in health care to provide evidence of “what-if” and scenario analysis before implementation in reality [20]. DES is an effective modeling technique to represent the care pathways structures, it can include inside its structure resource constraints and health outcomes. “What-if” scenarios analyses and determines the effect of implementing changes and process re-organization in the whole system performance [6, 14]. The adoption of solutions provided by “what if” analysis through simulation models, enables to understand the system behavior and the implication of a process re-organization before their implementation [1]. In this paper, a DES model has been developed and implemented using the simulation software WITNESS to assess the impact of introducing a patient-centered reconfiguration of the medical wards stay area. The schematic flow chart of the resulting DES model is reported in Fig. 1.

Schematic flow chart of the system under study
Following a patient-centered perspective, new patients enter the system belonging to a Pathology-related Clinical Pathway, represented by the DRG. Note that, all patients arrive as urgent and are directly admitted from the Emergency Department. The number and time of arrivals of patients for each DRG are taken from the data collection as well as the main characteristics associated. To consider the current occupation of beds at the beginning of the planning horizon, the number and LOS of patients already in the hospital are generated using retrospective data and pushed into the stay area. Note that, using the real data to feed the system with the patients already present at the beginning of the simulation run, we do not need to perform a warm-up to reach steady-state simulation. In fact, in our analysis, we want to simulate the flows of the cohort of patients as collected by real data verifying the impact of different organizational settings.
During the simulation run, new patient arrivals are managed using an arrival profile input data. Patients arriving in the system are segmented using demographic and clinical characteristics, as reported in Tables 4 and 5, DRG and ward of admission. Different combinations of these characteristics define groups of patients homogenous with respect to the resource use and cost. Each identified group is then associated with a LOS and cost distribution function. After hospital admission, patients flow in the system depending on the clinical pathway and organizational model of the stay area used.
As introduced in Sect. 2, the organizational model refers to how the stay areas are organized, i.e. specialty-based versus patient-centered hospital organization. The first reproduces the current practice where patients are admitted in the ward collected by real data. Instead, in the re-organization that follows the patient-centered model, all patients are accepted into a generic ward, where the multidisciplinary team organizes and takes in charge the patient hospital stay and providing a holistic vision of the care process. Dealing with multi-pathologies patients recovered in medical wards, the main resources in the care process are beds and clinical staff. Assuming that the number of clinicians and nurses are fixed, the main question herein addressed is determining how many beds are needed for each ward to treat the considered cohort of patients in both scenarios. To answer this question, we used the optimization module integrated into the simulation environment. We use as constraints the overall capacity in terms of the number of beds for each ward, as collected from real data. The objective function aims at defining the optimal number of beds to avoid cancellations and delayed admissions. Obviously, in the best scenario the objective function must reach the null value, guaranteeing that all patients arriving in the system in the exact timing of the real data (real arrival profile) are admitted.
5 Preliminary Results
The data-driven simulation model has been used to exactly reproduce the cohort of patients under study with their characteristics and their flow rules validated with the clinicians involved in our study to ensure its ability to represent the real system under investigation. Two scenarios are tested to evaluate the effect of re-organizing the “traditional”, specialty-based, stay area (each medical ward has its available beds) into a new patient-centered organization (beds are shared among all medical wards and patients are all treated as they are in an IMW).
In Table 6, the number of beds needed and the average length of stay in the three scenarios are reported. Note that, concerning the patient-centered model, two configurations are tested using for each patient group the LOS distributions and costs of the data collected in General Medicine 1 and General Medicine 2, respectively.
In both patient-centered scenarios, a reduction of the total number of beds needed is shown passing from 119 beds, in the current scenario (Specialty-based), to 115 and 98, respectively, in Patient-centered configuration (1) and (2), with a percentage reduction of beds of 3.4% and 17.6%. The outcome, measured by the average length of stay, shows improvement only in the Patient-centered model (2), where it reduces from 9.4 days to 8.3 days on average with a percentage reduction of 11.7%.
In Table 7 the average cost for each DRG and the total cost of the cohort is reported for the two scenarios. For both configurations of the patient-centered model a cost reduction is observed for all DRGs. Note that the average cost herein reported is weighted for the number of the patient in the segment and reflects the differences among the number and types of tests performed to the patients belonging to the segment analysed. Shifting from a specialty-based model to a patient-centered one, a total average reduction of 3% and 28% is obtained in configuration (1) and (2) respectively.
The better results of configuration (2) can be explained by the different skills of the clinicians of the two wards that affect the clinical pathways and outcomes of patients treated. In particular, in General Medicine 2 ward, the skills and abilities of the physicians are similar to the hospitalist, as described by literature: they perform ultrasounds on their own, as well as most invasive procedures such as positioning of central venous catheters, they plan the controls themselves or some changes in therapies such as insulin or laxative, helping to anticipate the controls, identify early or prevent complications, and thus shorten the stay and reduce the costs accordingly.
6 Conclusions and Future Works
This study focuses on the analysis of the impact of the adoption of a new organizational model for medical wards (Patient-centered model) with respect to the standard organization currently in use (Specialty-based model), considering both resources use and outcomes. The flow of patients within the hospital wards was modeled including patient-relevant characteristics such as severity, comorbidities, age, and sex. A Discrete Event Simulation model was developed to represent the pathways of complex patients through medical hospital wards. The model evaluates the length of stay of patients and the resource use (consultations, blood transfusions and diagnostic, cardiology, imaging and laboratory tests), using two organizational models. A real case study based on a medium hospital setting was analyzed. The results show that the patient-centered model provides an improvement in terms of beds needed and length of stay reduction of about 17% and 12%, respectively. The reduction of costs provided by the patient-centered models of 3% and 28%, respectively.
This study presents two main limitations: the first consists in the limited use of outcome indicators, where other outcomes should be included such as 90-days patient readmission and in-hospital mortality; the second derives from the hospital data which the model is based, a sensitivity analysis should be provided in order to verify the robustness of the results. Future work will be directed to test the model on a larger dataset, made up of three years of hospital data records also distinguishing in detail the results with respect to different DRGs. Indeed, we will use Machine unsupervised learning techniques, such as K-means clustering to identify the main characteristics able to create representative clusters of patients, with similar characteristics in terms of the intensity level of care and corresponding costs.
References
Abuhay, T.M., Krikunov, A.V., Bolgova, E.V., Ratova, L.G., Kovalchuka. S.V.: Simulation of patient flow and load of departments in a Specialized Medical Center. Procedia Comput. Sci. 101, 143–151 (2016)
Bauer, W., Schumm-Draeger, P.M., Koebberling, J., Gjoerup, T., Garcia Alegria, J.J., Ferreira, F., Higgens, C., Kramer, M., Licata, G., Mittelman, M., O’hare, J., Unal, S.: Political issues in internal medicine in Europe. A position paper. Eur. J. Intern. Med. 16(3), 214–217 (2005)
Brailsford, S.C., Harper, P.R., Patel, B., Pitt, M.: An analysis of the academic literature on simulation and modelling in health care. J. Simul. 3(3), 130–140 (2009)
Bruzzi, S., Landa, P., Tànfani, E., Testi, A.: Conceptual modelling of the flow of frail elderly through acute-care hospitals: an evidence-based management approach. Manag. Decis. 56(10), 2101–2124 (2018)
Clegg, A., Young, J., Iliffe, S., Rikkert, M.O., Rockwood, K.: Frailty in elderly people. The Lancet 381, 752–762 (2013)
Demir, E., Southern, D., Rashid, S., Lebcir, R.: A discrete event simulation model to evaluate the treatment pathways of patients with cataract in the United Kingdom. BMC Health Serv. Res. 18, 933 (2018)
Deyo, R.A., Cherkin, D.C., Ciol, M.A.: Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45(6), 613–619 (1992)
Duckitt, R., Palsson, R., Bosanska, L., Dagna, L., Durusu, T.M., Vardi M.: CDIME group. Common diagnoses in internal medicine in Europe 2009: a pan-European, multi-centre survey. Eur. J. Intern. Med. 21(5), 449–452 (2010)
Günal, M.M., Pidd, M.: Discrete event simulation for performance modelling in health care: a review of the literature. J. Simul. 4(1), 42–51 (2010)
Katsaliaki, K., Mustafee, N.: Applications of simulation within the healthcare context. J. Oper. Res. Soc. 62(8), 1431–1451 (2011)
La Regina, M., Guarneri, F., Romano, E., Orlandini, F., Nardi, R., Mazzone, A., Fontanella, A., Campanini, M., Manfellotto, D., Bellandi, T., Gussoni, G., Tartaglia, R., Squizzato, A.: What quality and safety of care for patients admitted to clinically inappropriate wards: a systematic review. J. Gen. Int. Med. (2019)
Malone, T.W., Laubacher, R., Johns, T.: The big idea: the age of hyprspecialization. Harvard Business Review 2011; available at https://hbr.org/2011/07/the-big-idea-the-age-of-hyperspecialization, last consultation on 18th march 2019
McCormick, P.J., Lin, H., Deiner, S.G., Levin, M.A.: Validation of the all patient refined diagnosis related group (APR-DRG) risk of mortality and severity of illness modifiers as a measure of perioperative risk. J. Med. Syst. 42, 81 (2018)
Ozcan, Y.A., Tànfani, E., Testi, A.: Improving the performance of surgery-based clinical pathways: a simulation-optimization approach. Health Care Manag. Sci. 20(1), 1–15 (2017)
Pietrantonio, F., Orlandini, F., Moriconi, L., La Regina, M.: Acute Complex Care Model: an organizational approach for the medical care of hospitalized acute complex patients. Eur. J. Intern. Med. 26(10), 759–765 (2015)
Rachoin, J.S., Skaf, J., Cerceo, E., Fitzpatrick, E., Milcarek, B., Kupersmith, E., Scheurer, D.B.: The impact of hospitalists on length of stay and costs: systematic review and meta-analysis. Am. J. Manag. Care 18(1), e23–e30 (2012)
Salive, M.E.: Multimorbidity in older adults. Epidemiol. Rev. 35(1), 75–83 (2013)
Wachter, R.M., Goldman, L.: The emerging role of “hospitalists” in the American health care system. New England J. Med. 335, 514–517 (1996)
Wachter, R.M., Goldman, L.: Zero to 50,000—the 20th Anniversary of the Hospitalist. New England J. Med. 375, 1009–1011 (2016)
Zhang, X: Application of discrete event simulation in health care: a systematic review. BMC Health Serv. Res. 18(1), 687 (2018)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this paper

Cite this paper
Landa, P. et al. (2020). Modelling Hospital Medical Wards to Address Patient Complexity: A Case-Based Simulation-Optimization Approach. In: Bélanger, V., Lahrichi, N., Lanzarone, E., Yalçındağ, S. (eds) Health Care Systems Engineering. ICHCSE 2019. Springer Proceedings in Mathematics & Statistics, vol 316. Springer, Cham. https://doi.org/10.1007/978-3-030-39694-7_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-39694-7_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-39693-0
Online ISBN: 978-3-030-39694-7
eBook Packages: Mathematics and StatisticsMathematics and Statistics (R0)