
Abstract
Schizophrenia is a highly heritable disorder characterized by disruptions on the molecular, cellular, and neural circuit level that lead to the behaviors and cognitive impairments associated with the illness. This chapter evaluates how combining neuroimaging methods with genetic approaches such as studying single genes and polygenic risk scores, to genome-wide association study (GWAS) variants and gene expression networks, can provide valuable insight into both biomarkers of schizophrenia and underlying neural mechanisms. Discussions begin with the evolving focus on smaller studies and a few genetic variants to larger scale multi-variant initiatives, and the benefits and challenges of both. The implications of recent findings are explored from bottom-up studies investigating brain abnormalities associated with candidate and GWAS identified variants individually, as well as the utility of examining aggregated risk in the form of polygenic risk scores. Advancements with large collaborative efforts such as ENIGMA hold promise with their top-down work identifying genetic variants underlying variation in brain structure, function, and connectivity. However, further work is needed to clarify how this builds upon our knowledge of intermediate phenotypes and insight into schizophrenia pathology. Moving forward, this chapter highlights emerging work examining relationships between imaging phenotypes and gene expression patterns that take into account spatial variation across the brain. It also evaluates the importance and increasing prevalence of studies investigating schizophrenia from a neurodevelopmental standpoint, and provides a dimensional point of view by examining early and prodromal stages of psychosis. Finally, the overall limitations in imaging genetic research, including challenges, and the progress to overcome them are discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Schizophrenia
- Psychosis
- Neurodevelopmental
- Clinical high risk
- Imaging genetics
- GWAS
- eQTL
- Intermediate biomarkers
- Endophenotypes
- MRI
- Neuroimaging
- Polygenic risk scores
- SNPs
- Gene expression
- Genetic risk variants
- ENIGMA
1 Introduction
Schizophrenia is a complex disorder affecting approximately 1% of the population (McGrath et al. 2008) and found to have a heritability as high as 85% (Sullivan et al. 2003; Wray and Gottesman 2012). However, genetic underpinnings and the widespread polygenic contributions to risk are far from fully understood (Sullivan et al. 2012). Accumulating evidence demonstrates that individuals with schizophrenia have disruptions on the molecular, cellular, and neural circuit level that lead to the behaviors and cognitive impairments associated with the illness. Although a person’s genetic profile can predispose them to have increased vulnerability for developing schizophrenia, there are also environmental factors and external stressors that may be the tipping point for illness onset or symptom severity. Neuroimaging is an important tool to understand better the neurobiological and genetically mediated risk mechanisms associated with this debilitating brain disorder.
There has been an increased focus in the literature on identifying biomarkers of schizophrenia and indicators of vulnerability, instead of examining the illness only as a clinical phenotype (Schmitt et al. 2016). Studies integrating genetic and imaging approaches can aid in the identification of endophenotypes or intermediate biomarkers between genotype and risk for disorders, such as quantifiable brain measures. If intermediate phenotypes capture a middle point in the pathway towards pathology, and are closer biologically to mechanisms underlying schizophrenia than clinical measures, then focusing on them may increase power for genetic studies. However, this approach assumes that the genetic architecture underlying brain structures will be less complex than that involved in neuropsychiatric disorders. Despite initial hopes for increased effect sizes, recent larger studies show that effect sizes of SNPs on imaging phenotypes are quite small (<1%), and similar to those of schizophrenia risk variants (Hibar et al. 2017; Franke et al. 2016).
Two main approaches exist for studying genetic risk and imaging phenotypes. The first, and more bottom-up, is to examine the effect of a single or group of genetic risk variants on neural systems and circuitry. Alternatively, a top-down data-driven approach can be used to begin with an altered pattern of neural circuitry, and then find both novel genetic variants, as well as confirm existing knowledge of variants. Some challenges with beginning first with an imaging phenotype is that one to one mapping in relation to the presentation of symptoms is challenging. However, it is a less biased approach and has the potential for discovery regarding biological pathways associated with the illness.
A common strategy to understand the contribution of genetics to risk for schizophrenia is to study patients and their unaffected family members. Investigating brain structure and functional abnormalities in healthy family members allows for analyses of genetic contribution of risk, without complications introduced by confounds such as illness duration, treatment, or symptom severity. This approach however, cannot infer specificities of which risk variants contribute to associated brain alterations, or how such contributions are made. It does not take into account the heterogeneity in genetic risk factors that can lead to schizophrenia. Nevertheless, family and twin studies have importantly indicated high heritability across neuroimaging phenotypes in relation to schizophrenia and have been reviewed in depth elsewhere (Lancaster et al. 2016a, b; Blokland et al. 2012; Jansen et al. 2015; Polderman et al. 2015).
The field of imaging genetics is gaining momentum, specifically in psychiatry, as multimodal approaches are increasingly used to study elevated vulnerability and the underlying pathophysiology of mental health and illnesses (Arslan 2015, 2018a, b; Bogdan et al. 2017; Lancaster et al. 2016a, b; Dima and Breen 2015; Carter et al. 2017; Meyer-Lindenberg 2010). Advances in neuroimaging methodologies and the increasing number of publically available datasets with multimodal data are contributing factors. Sample sizes for psychiatric populations are growing exponentially through large-scale collaborative consortiums such as Enhancing Neuro Imaging Genetics through Meta-Analysis (ENIGMA, Chap. 21) (Thompson et al. 2014), the Cohorts for Heart and Aging Research in Genomics Epidemiology (CHARGE) (Psaty et al. 2009), IMAGEN (Schumann et al. 2010), Alzheimer’s Disease Neuroimaging Initiative (ADNI) (Petersen et al. 2010), and recently specifically targeted at schizophrenia Genetics of Endophenotypes of Neurofunction to Understand Schizophrenia (GENUS) (Blokland et al. 2018), and have become accessible to a wide range of researchers.
In this chapter, we will focus on studies combining the use of neuroimaging and genetic approaches to review what is currently known about the genetic architecture underlying imaging phenotypes of schizophrenia. Work that has been done in healthy subjects, schizophrenia patients, as well as youth at clinically high-risk for psychosis is included.
2 Types of Genetic Variation
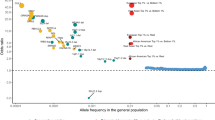
Genetic risk for schizophrenia is highly polygenic and heterogeneous, with no single factor associated with the guaranteed development of schizophrenia in an individual. The most well-known variations in the genome associated with schizophrenia are single nucleotide polymorphisms (SNPs), more rare mutations such as copy number variants (CNVs), and larger structural chromosomal abnormalities. The majority of rare mutations involve several genes and have greater functional and more deleterious effects as compared to common variants (Sebat et al. 2009; Sebat and Malhotra 2013). They also often are not inherited and occur de novo, perhaps explaining their enduring prevalence despite reduced fitness of carriers (Van Dongen and Boomsma 2013). There has been a surge in studies and shift towards focusing on rare variants and their contribution to genetic risk for schizophrenia, alongside the variance explained by common variants (Bustamante et al. 2017). Studies of effect sizes have shown that the 16p11.2 duplication has an Odds Ratio (OR) for psychosis of 14.4 (Giaroli et al. 2014), the 3q29 deletion is above 40 (Mulle 2015), and the 22q11.2 deletion increases risk for schizophrenia roughly 30-fold (Schneider et al. 2014). Implicated rare variants like 22q11.2 increase risk for multiple neural pathologies in addition to schizophrenia, such as Autism Spectrum Disorder and intellectual disability. Imaging genetic studies have begun determining brain structure and functional abnormalities associated with rare variants. Additionally, with the recent emergence of a 22q11.2 deletion ENGIMA working group, there is promise moving forward for large meta-analyses with the power to build on our understanding of developmental trajectories associated with this condition. However, further in-depth discussion of imaging studies focusing on rare mutations is beyond the scope of this chapter, and moving forward, the focus will be on studies involving common variants.
3 Moving from a Candidate Gene Approach to the Era of GWAS
A substantial portion of imaging-genetic studies thus far have been dominated by investigations of candidate genes pre-selected for studies based on a priori knowledge. These initial studies were important in creating neurobiological models of schizophrenia risk and validating hypotheses of the involvement of these genes in specific biological systems. Candidate genes such as catechol-O-methyltransferase (COMT; Witte and Flöel 2012; Gonzalez-Castro et al. 2016), brain-derived neurotrophic factor (BDNF; Hong et al. 2011; Harrisberger et al. 2015), dopamine 2-receptor (DRD2; Luykx et al. 2017), and 5-HTTLPR (Raab et al. 2016; Murphy et al. 2013). Their effects have been reviewed and found to be associated with a variety of brain changes from altered activation to structure (Arslan 2015; Hashimoto et al. 2015; Rasetti and Weinberger 2011). However, the strategy of investigating a single gene at a time has not been overly successful, as effects of single variants are quite small and statistical power is often low (Meyer-Lindenberg 2010; Farrell et al. 2015).
Recently, growth in sample sizes has provided the opportunity to use GWAS to study genetic risk variants associated with schizophrenia. The largest GWAS of risk for schizophrenia currently published by the PGC includes 36,989 cases and 113,075 controls, scanned for 9.5 million variants, and has identified 125 genetic loci (of which 108 are independent) associated with this mental disorder (Schizophrenia Working Group of the Psychiatric Genomics Consortium 2014).This un-biased data-driven alternative to studying candidate genes has been able to identify novel genetic variants and polymorphisms linked to schizophrenia because of the large study power. Although GWAS findings have increased support for some candidate risk variants such as zinc-finger protein 804A (ZNF804A), calcium voltage-gated channel subunit alpha1 C (CACNA1C), glutamate receptor mgluR3 (GRM3), and DRD2, they have also found unexpected negative results for others such as COMT and BDNF, and questioned previous effect size findings of others such as 5-HTTLPR (serotonin transporter–linked polymorphic region; Hariri et al. 2002; Flint and Munafò 2013).
There are many hypotheses about the mechanisms underlying schizophrenia development, such as the dysregulation of the dopamine (Howes et al. 2017; Meltzer and Stahl 1976), glutamate (Moghaddam and Javitt 2012), or GABAnergic systems (Nakazawa et al. 2012), disruption in myelin and axons (Stedehouder and Kushner 2017; Cassoli et al. 2015), calcium imbalance (Berridge 2014; Lidow 2003), or inflammation (Howes and Mccutcheon 2017). These have traditionally been investigated separately and as more is discovered about the genetic architecture and polygenic nature of schizophrenia through GWAS, evidence has emerged that supports each of these theories instead of narrowing down possible mechanisms or pathophysiological processes (Devor et al. 2017). However, recent analyses are converging on the involvement of biological pathways to unify many of these theories into a general hypothesis of disrupted intracellular signaling pathways, communication across fast (voltage-gated ionic channels) and slow (G-protein coupled receptors) neurotransmission (Devor et al. 2017), as well as on excitatory and inhibitory synaptic neurotransmission and plasticity (Hall et al. 2015).
4 Targeted GWAS Risk Variant Studies
As a result of GWAS findings, a great deal of work has been done to target identified risk genes or specific variants and to examine their relationship with imaging phenotypes. These structural and functional studies involving genes implicated in the schizophrenia GWAS have found associated alterations in brain volume, density, white and gray matter, cortical folding and thickness, as well as regional activation and connectivity during executive tasks (Gurung and Prata 2015; Harrison 2015).
Genes containing loci that were implicated in the most recent PGC GWAS include dopaminergic system related gene DRD2, glutamatergic transmission genes GRM3 and GRIN2A, and calcium signalling genes CACNA1C and NRG1, in addition to other genes of interest such as ZNF804A, DISC1, MIR137, and ANK3, to name a few.
GWAS have been important for the identification of novel variants to target for further investigation. Results have inspired follow up imaging and molecular studies to try to understand the relationship between common variants and effects on functioning that might be related to psychosis symptoms. These multimodal explorations are especially important for identifying the actual susceptibility gene and mechanism conferring risk. Only 10 of the identified variants exist in exonic regions of the genome and result in amino acid changes in proteins. Many of the others are most likely located in regulatory regions and lead to functional effects through changes in splicing, gene expression, or other molecules involved in these processes. Considering the high linkage disequilibrium that can occur across many variants and span regions that encompass multiple genes, it is also possible that identified risk variants are merely in high define with the actual variant that confers risk through altered functioning (Bray and Hill 2015).
A recent large study by Erk et al. (2017) examined all of the significant GWAS schizophrenia risk alleles (Schizophrenia Working Group of the Psychiatric Genomics Consortium 2014) and their effects across RDoC neurocognitive domains and brain activation. Only a single SNP rs9607782 near EP300 survived significance after correcting for multiple comparisons and was associated with amygdala activation during emotional processing, indicating that the schizophrenic risk may be mediated by amygdala functioning. There were also findings regarding ZNF804A and CACNA1C, but these only reached subthreshold significance and did not survive correction. It is possible that other meaningful links were lost because of the multiple tests and stringent corrections applied to address false positives. There have also been negative findings in another smaller study looking at associations between identified GWAS schizophrenia risk variants and both cortical thickness and white matter FA neuroimaging phenotypes across the lifespan (Voineskos et al. 2015).
However, significant progress has been made in smaller studies with more a narrowed focus on one or a few risk variants in elucidating functioning. A highly implicated risk allele and one of the first to be identified by GWAS is ZNF804A rs1344706, an intron of a zinc-finger gene coding for a transcription factor. This gene is thought to regulate other genes (Donohoe et al. 2011), including other candidate genes associated with schizophrenia: PRSS16, COMT, PDE4B and DRD2 (Girgenti et al. 2012), and to impact cell adhesion among other functions (Hill et al. 2012). The effect of ZNF804A on structural white matter fractional anisotropy (FA) remains unclear, with both positive (Mallas et al. 2017; Kuswanto et al. 2015; Ikuta et al. 2014) and negative findings (Voineskos et al. 2011; Fernandes et al. 2014; Sprooten et al. 2012; Wei et al. 2015). A recent study showed more widespread effects on white matter FA (Mallas et al. 2017). The ZNF804A risk allele also has mixed effects on gray matter volume in schizophrenia and healthy controls (Donohoe et al. 2011; Cousijn et al. 2012; Voineskos et al. 2011).
Functional imaging studies of the ZNF804A risk allele have replicated findings related to working memory and modulation of connectivity between the hippocampus and dorsolateral PFC (Esslinger et al. 2009, 2011; Rasetti and Weinberger 2011), as well as altered regional activity during social theory of mind tasks and emotional processing (Esslinger et al. 2011; Walter et al. 2011; Mohnke et al. 2014), as well as cognitive control (Thurin et al. 2013).
Investigations have shown that rs1344706 reduces the expression of ZNF804A during the fetal stage, a critical period in neurodevelopment (Hill and Bray 2012; Tao et al. 2014). However, the mechanism by which this risk variant alters expression remains unknown. There is also evidence from animal models that ZNF804A is involved in neurite growth and elongation in the hippocampus and frontal cortex, areas also implicated in imaging studies, and that the rs1344706 allele reduces dendritic spine density, which is consistent with the clinical presentation of schizophrenia (Deans et al. 2016). Overall, compelling findings indicate that this risk variant is a significant factor relating to the onset of schizophrenia that affects the brain early in life and may be involved in white matter structure, connectivity, and cognition (Chang et al. 2017).
It is clear that although GWAS studies have identified novel risk variants, the underlying functioning of these variants and their involvement in molecular pathways leading to their effect on the brain is far from understood. A combination of basic science and molecular genetic studies are needed to move forward in disentangling how genetics contribute to the risk for mental illnesses (Bogdan et al. 2017). A recent study by Sekar et al. (2016) investigated the possible mechanisms of C4 risk alleles located in the dense major histocompatibility complex (MHC), the area most highly associated with schizophrenia through GWAS. Through post-mortem, animal, and population studies, these investigators reported that structural variants altered C4A and C4B expression in the brain that were related to risk for schizophrenia. In combination with findings that C4 mediated synaptic pruning in mice during neuronal maturation, this research suggests that alterations in C4 expression may be related to the reduced number of synapses in the brains of individuals with schizophrenia. These findings have triggered studies of C4 expression and the complement system, although neuroimaging studies have not been done to elucidate how expression relates to imaging phenotypes in humans.
5 Polygenic Risk Scores and Imaging Phenotypes
Examining the role of each GWAS identified risk variant or groups of variants is important for understanding the specificities of how they are involved in schizophrenia risk. However, individual GWAS SNPs capture little of the phenotypic variance observed in schizophrenia (often much less than 1%) and do not address the possible polygenic, additive, or synergistic contributions thought to be involved in illness development. Using an accumulated polygenic risk score (PRS), created by aggregating the effects of many risk variants based on odds ratios, increases the amount of explained variance to as much as a third, and can be a useful tool for applying findings from large GWAS to small samples (Dima and Breen 2015). PRS is thus advantageous as it can incorporate the effects of all or a portion of SNPs, which can extend beyond the few that reach genome-wide significance as determined by a corrected statistical threshold. This approach most likely introduces false positives for the effects of some SNPs, but it also overcomes biases associated with a relatively arbitrary cut-off threshold for significance. Recently, studies have begun to investigate the overlap between polygenic risk for schizophrenia and brain abnormalities linked with the disorder as a complementary bottom-up approach to studying individual common variants. Effect sizes from the PGC GWAS are typically used to construct scores, although not universally (Ohi et al. 2014), and studies often use all SNPs under a certain p-value significance threshold. Importantly, even in healthy youth, an increased polygenic risk score (PRS) for schizophrenia has been found to be correlate with impairments in social cognition and verbal reasoning, demonstrating that relationships emerge early in development (Germine et al. 2016). Additionally, a higher PRS is linked to a family history of psychotic illnesses (Bigdeli et al. 2016). However, there are variations in how studies define PRS and the number of variants included, which has led to challenges related to comparing and replicating results.
As genetic testing of massive numbers of an individual’s SNPs continues to quickly become more inexpensive and accessible, it is increasingly becoming an attractive option for quickly determining an individual’s risk load for a mental illness that is consistent across a lifespan. A recent growth of studies examining PRS and their associations with cognition, behavior, and neuroimaging phenotypes are improving our understanding of the implications of this aggregated score and its possible utility in health care and clinical practice. As research accumulates to improve specificity and sensitivity, it is possible that one day a PRS may be used for more personalized and preventative medicine, resulting in early identification and more individually targeted interventions.
6 Findings from PRS Imaging Studies
Despite the well-established structural alterations prevalent in schizophrenia, larger studies examining overlap between PRS and these abnormalities have found mixed results. Some earlier studies identified direct relationships between PRS and total brain and white matter volume using a range of significance cut-offs for PRS (Terwisscha van Scheltinga et al. 2013), although this has not been consistently replicated and there have been predominantly negative findings for total GM volume (Papiol et al. 2014; Van der Auwera et al. 2015; Reus et al. 2017; Lancaster et al. 2018). One study did support an association between reductions in total white matter and PRS in psychosis, as well as familial genetic risk using a 7 SNP white matter targeted score (Oertel-knöchel et al. 2015).
Studies looking at regional volume differences associated with PRS have found a negative relationship with globus pallidus volume and a trending negative relationship with thalamic volume, both with a range of schizophrenia PRS and a shared PRS between schizophrenia and bipolar disorder (Caseras et al. 2015). This trending association with thalamic volume has been replicated (Reus et al. 2017). Additionally, when a range of PRS are examined using effect sizes from a Japanese GWAS (Ikeda et al. 2011), a negative relationship was found with the left superior temporal gyrus volume (Ohi et al. 2014).
Findings related to the hippocampus show that a higher PRS based on 108 loci is negatively associated with volume (Harrisberger et al. 2016). Additionally, higher scores for a range of PRS have been related to reduced neuroplasticity in response to an aerobic exercise intervention for schizophrenia, specifically in the left CA4/DG region of the hippocampus (Papiol et al. 2017). Another study with a discovery Chinese sample and European replication sample found negative results for hippocampus volumes, intracranial volume (ICV), and total volumes when both a mixture of GWAS significant and previously found variants associated with candidate genes were included in a PRS (Li et al. 2015). Additionally, when PRS scores based on the 108 identified variants were broken down into biological systems such as calcium signalling, neurodevelopment, and glutamatergic neurotransmission, findings of volume changes were negative across the brain (Van der Auwera et al. 2017). Further, there were no associations found between white matter tract measures FA and MD with a PRS based on the 108 loci (Voineskos et al. 2015), or a range of PRS (Reus et al. 2017). Of note, replicated findings show evidence for lower cortical gyrification in the inferior parietal lobes associated with a range of PRS (Liu et al. 2017). Global cortical thinning has also been associated with a range of higher PRS in individuals with schizophrenia (Neilson et al. 2017).
In a large study by French et al. (2015), a negative relationship was discovered between cannabis use and cortical thickness in adolescent boys with high PRS determined by the significant 108 loci. This relationship was replicated in three samples and was not present in any of the adolescent girls or the boys with low PRS, although a higher PRS in girls was associated with elevated cortical thinning. This finding demonstrates possible useful applications of PRS in elucidating neurobiological mechanisms of risk factors for schizophrenia development, such as cannabis use during adolescence (Manrique-Garcia et al. 2012).
There have been fewer functional neuroimaging studies involving PRS, but with more consistently positive results. A novel study by Erk et al. (2017) investigated schizophrenia risk PRS and its impact on brain activation during the five neurocognitive domains outlined by the RDoc in healthy controls using two thresholds from the PGC study—5 × 10−8 and 0.05. Findings showed activation of the perigenual anterior cingulate during an emotion recognition task, and posterior cingulate during a theory of mind task, which were both associated with PRS.
Altered activation and inefficiency of the dorsolateral and middle superior PFC during WM related tasks has been found to be related to a variety of differently chosen PRS (Walton et al. 2013, 2014; Kauppi et al. 2014). A recent study also showed a positive association between a PRS created from 418 genes from the CREBS and BDNF family, with deviation in the variability in resting-state networks and functional network connectivity predominantly related to the thalamus, parahippocampal gyrus, visual, and/or sensorimotor areas compared to cohort-common patterns (Chen et al. 2018).
Multiple studies have found a relationship between PRS and alterations in ventral striatal activity. The first examined a monetary incentive delay task and found that higher scores across a range of PRS thresholds were associated with lower IQ and striatal activity, indicating that it may be related to different reward processing in higher risk individuals (Lancaster et al. 2016b). The second study found increased BOLD signal in the ventral striatum, extended reward-related areas, and cortical networks, including posterior regions, occurred during a reversal learning task in individuals with a higher PRS thresholded at 0.05 (Lancaster et al. 2018).
These findings overall support a lack of genetic overlap between this disorder and subcortical volumes, but larger overlap with cognition and altered neural circuitry (Hubbard et al. 2016; Hagenaars et al. 2016). However, the success of studies focusing on specific variants and targeted PRS including variants previously implicated in structural abnormalities may indicate that a subgroup of variants are involved in structural changes related to risk, and that the use of more complex PRS dilute effects. Evidence points to the hypothesis that common genetic variants associated with schizophrenia are involved in altering cognition (especially emotion processing) and motivational circuitry predominantly, which may influence the volumetric abnormalities observed in schizophrenia. The varied findings may also be related to the fact that the relationships observed between neuroimaging phenotypes and a continuous PRS are not as linear as expected, especially in functional imaging (Birn and Bandettini 2005).
7 Successes and Failures of Collaborative Imaging Genetic Efforts
In the last decade, multiple large-scale consortiums have worked to combine impressive quantities of imaging and genetic data internationally into meta-analyses. One of the largest efforts has been by ENIGMA, which had as its initial aim to use GWAS to identify common variants underlying variation in brain structure, function, and connectivity. This work now extends to identifying factors that reliably affect brain features and can be used for individual prediction of risk and deviations from normal development (Thompson et al. 2014). Although individually common variants have small effects, collaborative efforts use the strategy of collecting large samples and increasing power to identify enough variants that, when aggregated, explain a substantial portion of imaging phenotype variance. This increase in power through meta-analysis can also be used to study diseased populations and build upon our knowledge of intermediate phenotypes to clarify mechanisms involved in how these abnormalities relate to the development of mental illnesses such as schizophrenia. Thus far, over 20 psychiatric, neurodegenerative and neurodevelopmental disorders have been studied as part of ENIGMA, and publications have followed from the largest structural MRI studies for multiple mental illnesses (Schmaal et al. 2015; Hibar et al. 2017; Boedhoe et al. 2017; Hoogman et al. 2017). Initiatives have also led to the identification of the first genome-wide variants associated with subcortical structures (Hibar et al. 2015, 2017; Stein et al. 2012). However, this large-scale approach has met with both successes and failures, and there are many challenges to offering insight into pathology related to schizophrenia.
Findings to date have shown that there is little overlap between GWAS identified risk variants for schizophrenia and those associated with subcortical volume (Hibar et al. 2015, 2017). A large population study by (Hibar et al. 2015), including both healthy and mentally ill individuals, examined ICV and seven subcortical volumes in 13,171 subjects of European ancestry, and a replication sample of 17,546. Findings showed significant and suggestive findings for ICV, hippocampus, putamen, amygdala and caudate, but not the nucleus accumbens, pallidum or thalamus. A single significant SNP rs2909457 is also associated with schizophrenia risk, and was found to be correlated with hippocampus volume. A similar correlation with a SNP in high LD emerged in a following study (Hibar et al. 2017). Contrary to what was expected based on changes commonly seen in schizophrenia (Adriano et al. 2012), hippocampal volume increased with increasing risk.
A study by Franke et al. (2016) examined the overlap between genetic variants related to these same structural measures and those associated with schizophrenia to further confirm null results. These results are perhaps even more surprising as the use of the same methodology has found large overlaps in common variants between schizophrenia and both bipolar disorder and major depressive disorder (Cross-Disorder Group of the PGC 2013a, b). Overall, converging evidence does not support the hypothesis that alterations in brain structure are causally associated with schizophrenia risk, or that there are pleiotropic effects of common variants on structural phenotypes and schizophrenia. Limited progress has forced the reassessment of the potential for this approach to assist with constructing new or improved hypotheses about how the brain is involved in the onset and course of schizophrenia.
Little overlap in associated common variants suggest that alternative hypotheses independent of genetic causes regarding structural abnormalities seen in schizophrenia may need to be considered. Other possible contributing factors are rare mutations, epigenetics (Cariaga-Martinez and Alelú-Paz 2017), gene interactions, environmental interactions (Davis et al. 2016), course of illness (Mathalon et al. 2001), or treatments (Ho et al. 2011). More consistent findings of altered cognitive and behavioral alterations associated with common variants may be related to downstream effects or reverse causation of volume changes (Owens et al. 2012; Toulopoulou et al. 2015).
Alternatively, it is possible that the effect sizes of genetic overlap between brain structure and schizophrenia are quite small and that GWAS are either underpowered or methodology is insufficient to find results. The higher the number of participants in a study, the larger the power to discover variants contributing small effects that may be overshadowed by heterogeneity within the sample. This is supported by a more recent focused study with increased power that examined only the overlap between schizophrenia and subcortical structures genetic risk, and had positive findings in loci such as FOXO3 and ITIH4, associated with ICV, SLC4A10 and SPATS2L with the hippocampus, as well as DCC, and DLG2 with the putamen (Smeland et al. 2017). Additionally, the use of a newer method called partitioning-based heritability analysis demonstrated that schizophrenia risk variants significantly modulate normal variation in cortical thickness and surface area in multiple brain regions (Lee et al. 2016).
8 Combining Gene Expression, Risk Variants and Imaging Phenotypes
A similar approach to beginning with imaging phenotypes as continuous quantitative traits and determining genetic associations is to begin with gene expression and discover genetic variation contributing to changes. Variants that affect expression levels are considered expression quantitative trait loci (eQTL) and provide a possible mechanism by which common variants may influence imaging phenotypes and confer risk for schizophrenia. Many genes have altered expression in schizophrenia, and a significant portion of variants associated with schizophrenia (Schizophrenia Working Group of the Psychiatric Genomics Consortium 2014) have been found to be eQTL and to alter the expression of at least one gene (Richards et al. 2012; Fromer et al. 2016).
However, another aspect not commonly captured is the wide-ranging effects these risk variants sometimes have spatially across the brain. It is known that the majority of gene expression varies both by brain region and temporally across the lifespan, as well as that SNPs can impact expression (Kang et al. 2012). Post-mortem studies have shown that gene expression disturbances in schizophrenia patients exist across and vary by brain region (Horváth et al. 2011). Recent studies are beginning to highlight the importance of regional expression of specifically schizophrenia related risk genes associated with abnormalities observed in the brain that may improve understanding of why brain changes are concentrated in certain areas or along specific pathways in schizophrenia. This strategy also provides the opportunity to study the relationships between genetic risk and more complex imaging phenotypes, such as network connectivity.
In the same way that similar co-expression networks of multiple genes indicate a common regulatory pathway (Weirauch 2011), overlapping gene expression and brain connectivity networks may indicate common underlying mechanisms and influence. Further, areas where risk variants have increased expression may indicate increased influence on neural functioning of that region and greater effect on local imaging phenotypes.
With increasing accessibility through publically available resources such as the Allen Human Brain Atlas, BrainCloud, BrainSpan, and CommonMind Consortium (providing maps of gene specific transcription across the brain), it is possible to examine genetic risk with regionally specific gene expression patterns throughout the brain. Examining the spatial expression of schizophrenia risk variants together with brain abnormalities may provide insight into the complex relationships between them and the pathogenic mechanisms involved in psychosis development (French et al. 2015).
9 Structural and Functional Connectivity Overlapping with Networks of Gene Expression
A recent study by Romme et al. (2016) cross-correlated connectivity networks determined using diffusion-weight imaging with spatial expression of schizophrenia GWAS identified genes (Schizophrenia Working Group of the Psychiatric Genomics Consortium 2014) from post-mortem microarray data in the Allen Human Brain Atlas (Hawrylycz et al. 2012). Results showed that increased differences in structural connectivity between schizophrenia and healthy controls across the brain overlapped with areas of the cortex where there was heightened expression of risk genes. Further breakdown of schizophrenia risk genes into classes of function, as specified by PGC, showed that genes involved in neuronal calcium signaling (including CACNA1C) were most closely associated with connectivity differences. Additionally, findings were specific to schizophrenia and there was no association between expression of schizophrenia risk genes and structural connectivity in individuals with bipolar disorder. This differentiation between these illnesses may be key, particularly given the strong overlaps in genetic risk of approximately 65% (Cross-Disorder Group of the Psychiatric Genomics Consortium 2013a, b) in brain abnormalities and symptomology that exist.
As well as investigating previously associated genes found through GWAS of schizophrenia, Romme et al. (2016) linked novel genes, as well as supported previous findings, in a data driven approach examining all available gene expression networks and the most highly correlated with networks of altered connectivity in schizophrenia. Many of the identified top 100 and 500 genes (the second most highly correlated being C4A) have already been associated with psychiatric disorders, and investigation of the remaining genes may assist with the identification of risk genes involved in pathophysiology specifically related to altered neural connectivity observed in schizophrenia.
Another study examined the relationship between white matter network organization and local gene expression across age in schizophrenia (Powell et al. 2017). Declining network integrity across age was delayed in individuals with schizophrenia compared to controls. Additionally, when the spatial expression of six top schizophrenia associated genes were examined, DISC1, DRD2, DTNBP1, and GRM3 were associated with age-dependent changes in white matter network modularity, with DISC1 additionally associated with local efficiency. There were no significant associations between white matter network measures and regional expression of the COMT and BDNF genes.
A study by Pergola et al. (2017) focused on the commonly implicated dopamine molecular pathway and DRD2 gene expression across the PFC. SNPs associated with co-expression of specifically the D2 long dopamine receptor were identified to create a Polygenic Co-expression Index (PCI). An increased PCI was found to predict working memory performance, greater BOLD signal in the PFC indicating inefficiency during this task, as well as a better clinical course. This approach demonstrates that investigating gene co-expression can be used to investigating gene co-expression can be used to better understand the role of risk genes in biological pathways that relate to behavioral and clinical phenotypes.
There is also evidence that resting-state networks are heritable (Glahn et al. 2010; Fu et al. 2015), signifying that genetic risk associated with schizophrenia may underlie alterations observed in the disorder. Furthermore, resting-state functional connectivity networks correspond with networks of correlated gene expression, and polymorphisms in these identified genes, which alters resting-state connectivity in healthy adolescents (Richiardi et al. 2015). It has also been shown that spatial patterns of gene expression have a high correspondence with cortico-striatal pathways involved in limbic and somatomotor functional networks (Anderson et al. 2018), which are pathways strongly associated with schizophrenia pathology.
10 At Risk Youth and Discovering Predictors for Psychosis
Schizophrenia is considered a neurodevelopmental disorder involving altered neural maturation and connectivity (Insel 2010; Marenco and Weinberger 2000). Numerous studies have examined and found alterations in brain circuitry and functioning in youth at all stages of psychosis development, from subthreshold symptoms (Satterthwaite et al. 2016) to clinically high-risk groups and genetic high-risk groups (Fusar-Poli et al. 2012), to the emergence of first-episode psychosis. There is support that increased genetic risk based on family history increases risk of transition and is associated with symptom severity and with brain abnormalities (Fusar-Poli et al. 2015; Seidman et al. 2010).
Imaging-genetic studies in neurodevelopmental samples as well as adult samples provide the opportunity to study changes across the emergence of symptoms and answer the question of when, in addition to how, genetic factors confer risk by affecting brain structure and function. The early detection and treatment of psychosis at prodromal stages is an important and widely accepted goal to move towards reducing the burden of schizophrenia (Pettersson-Yeo et al. 2013). If biomarkers are identified, they can be integrated into predictive models to distinguish better high risk youth that will later transition to full psychosis or schizophrenia so that they can be targeted for preventative early interventions (Millan et al. 2016).
Despite this surge in studies examining high-risk youth, the majority of imaging-genetics studies focus on neuroimaging phenotypes and increased risk in the context of familial or genetic risk, with fewer studies addressing specifics in the heterogeneity of genetic vulnerability (Fusar-Poli et al. 2015). Additionally, there are challenges with methodology and reporting of studies aimed at predicting transition to psychosis in CHR (Studerus and Ramyead 2017). For example, a study reviewing brain abnormalities in genetic high-risk groups and clinical high-risk groups found that clinical high risk groups had more severe structural and functional differences, including abnormalities associated with transition to psychosis. This is most likely related to the higher symptom severity seen in this high-risk group (Smieskova et al. 2013).
A promising finding from multiple studies is the association of risk variants in the 5′ region of neuroregulin 1 (NRG1) and rates of transition to schizophrenia in high-risk psychosis groups. This gene is involved in regulating myelination processes (Ortega et al. 2012; Wood et al. 2009) and is important for cortico-cortical myelination during neurodevelopment (Chen et al. 2016). It has been marginally associated with total brain FA, and together with other genes involved in myelination, it is significantly associated with schizophrenia and FA, perhaps indicating that it works by affecting oligodendrocyte-expressed specific genes (Chavarria-siles et al. 2015).
Studies have also found a 100% transition rate in both genetic and clinical high-risk cohorts associated with the NRG1 rs6994992 SNP (Hall et al. 2006; Keri et al. 2009). Another larger study by Bousman et al. (2013) did not replicate these findings, but did discover that nearby rs4281084 and rs12155594 risk alleles increased the risk for transition. A recent follow-up imaging-genetics study by Bousman et al. (2018), looked at the neurobiological effect of having a high allelic risk load based on these identified SNPs in the NRG1 gene. Individuals who had an early age of onset and developed schizophrenia before the age of 26 had increased left and right ventricles. Further, all carriers of high risk alleles had reduced FA, elevated RA, and stable AD in the frontal cortex, but no differences in cortical thickness, gray matter volume, and surface area.
In another study, higher schizophrenia PRS has been associated with decreasing hippocampal volume in at-risk mental state youth, and with a higher rate of transition to first episode psychosis (Harrisberger et al. 2016).
Recent initiatives, such as the publically available Philadelphia Neurodevelopmental Cohort (PNC), hold promise for improving our understanding of factors involved in psychosis risk. This large-scale population sample study began with just genetics data, but now has approximately 1600 participants aged 8–21 with multimodal neuroimaging, cognitive, and psychopathology data, with an enrichment for youth with psychosis spectrum symptoms. Further, a portion of the participants have data from multiple follow up assessments 2 years apart. Studies to date have shown structural and functional brain abnormalities associated with youth experiencing psychosis spectrum symptoms (Wolf et al. 2015; Satterthwaite et al. 2016). An investigation by Voineskos et al. (2015) examining the relationship between schizophrenia risk variants, cortical thickness, and white matter tract measures included PNC participants but showed negative findings. A recent paper by Cordova-Palomera et al. (2018) examined a wide range of PGR, as well as brain thickness, surface and volume in the PNC. A higher risk score was associated with reduced cortical surface area and thalamic volume. This study also found an apparent suppressing effect, in that altered brain features compensated for the effect of PGR on cognition. Although there are only a few PNC studies integrating imaging and genetics as of yet, this sample’s large numbers and range of data present exciting possibilities for elucidating mechanisms associated with psychosis development in adolescence.
There is also accumulating evidence that genetic factors and epigenetic mechanisms are involved in hormonal responses causing brain changes during adolescent development, and that these are linked to underlying pathophysiological mechanisms of psychosis development (Trotman et al. 2013; Walker et al. 2013). Further work is needed to better understand the relationship between hormones and their role during this key neurodevelopmental period when symptoms being to emerge. Revealing these mechanisms may also explain sex differences in cognition and brain abnormalities occurring in schizophrenia in adulthood that may be tied to hormonal divergences that begin in adolescence (Mendrek and Mancini-Marïe 2016).
11 The Challenge of High Dimensionality of Imaging and Genetic Data
Mixed findings of genetic overlap between schizophrenia risk and brain structure, but replicated positive findings from studies examining individual SNPs and neuroimaging phenotypes indicate that the problem may lie in the methodology for discovering GWAS common variants, and not that there truly is no overlap in genetic underpinnings. There are a number of evolving statistical methods to address the challenge of the high-dimensionality of imaging and genetic data (Schork et al. 2016). In GWAS, each SNP is independently tested using regression models for association with a scalar measure such as clinical diagnosis. This results in huge numbers of pairwise univariate tests that need to have statistical corrections applied to reduce the prevalence of false positives. The number of tests increases when multiple neuroimaging phenotypes, especially voxel-wise measures, are investigated, and leads to reductions in power and elevated computational costs. Additionally, applied corrections may be too stringent, ignoring the possibility that SNPs may have high LD and that regions of imaging phenotypes such as cortical thickness, FA, and volume tend to be highly co-varied across the brain, and not actually independent. Alternative strategies such as controlling for false discovery rate (FDR) instead of family-wise error rates, or prioritizing genes based on ontology in combination with stratified corrections have been proposed (Patel et al. 2016).
Other approaches such as set-based association tests can reduce the number of comparisons, as well as detect small effects from rare variants that GWAS currently does not have the power to take into account. By looking at whether a group of variants collectively affect a phenotype, their accumulated effect may be large enough to be identified. Different set-based association tests are more appropriate depending on whether or not genetic variants within a set are heterogeneous or homogeneous in their effects (Lee et al. 2014). This approach has been successfully extended for analyses of gene-environment interactions on neuroimaging phenotypes, taking into account both fixed and random effects (Wang et al. 2017). Bayesian approaches with mixed models have also been a sophisticated multivariate strategy to select variables and reduce dimensionality, while ensuring that variables are more likely to correspond to SNPs within the same gene and across different neuroimaging phenotypes (Greenlaw et al. 2016; Stingo et al. 2014; Chekouo et al. 2016). Parallel independent component analysis is also an option for a multivariate method to associate groups of common variants with neuroimaging phenotypes (Pearlson et al. 2015). Additionally, the use of machine learning is an important way forward with both approaches based on pre-selected risk variants and more data-driven analyses (Yang et al. 2010).
12 Other Limitations and Future Directions
Although, substantive progress has been made in understanding the pathology of schizophrenia and how risk is conferred genetically using imaging genetic studies, there are many limitations that need to be considered (Blokland et al. 2017). In general, there has been an overall lack of replication of many candidate findings and effect sizes in structural and functional imaging genetic studies (Button et al. 2013, Ioannidis from Thompson et al. 2014), including in the large meta-analyses that have been done by ENIGMA.
One of the reasons that there has been little success in linking imaging phenotypes such as subcortical structure to genetic risk for schizophrenia in meta-analyses may be that these simplistic phenotypes are not complex enough to capture relationships bridging genetic risk with a multifaceted illness such as schizophrenia. More promising progress may be made by examining networks of structure and function to represent the polygenic and clinical diversity of schizophrenia. Additionally, continuing to move towards combining multiple levels of data such as risk variants, gene expression, and more intricate brain features holds promise for disentangling convoluted causal mechanisms. Further, methodology is being developed to integrate factors such as gene-environment interactions and epistatic effects of genes into imaging genetic studies (Kang et al. 2015).
Some limitations on imaging genetic studies targeting a single or groups of variants often include small samples, inconsistencies choosing phenotypes, demographic differences, as well as a range of symptom severity, course of illness, comorbidities, medication confounds, and a publication bias that may lead to false positives (Nickl-Jockschat et al. 2015). However, smaller samples can provide the opportunity for more homogeneity to discern aspects of altered biological processes that affect subgroups of individuals with schizophrenia. In combination with larger studies, it is important to further dissect potentially meaningful differences in studies when findings are not uniform.
The GWAS and collaborative approach has and continues to contribute greatly to our understanding of genetic architecture. However, there are disadvantages and limitations to using simple phenotypes such as binary categorizations for cases and controls. This method relies on sample size to address heterogeneity within cases, as well as controls. It allows genetic variants with small effects to be identified, but it also forces the creation of national and sometimes international norms that may or may not exist. By grouping everyone together, signals from important risk factors that affect subgroups of the cases may be drowned out. This is important considering our knowledge of the heterogeneity in schizophrenia, as well as the effects from factors such as environment and ethnicity. It is becoming apparent that the same disorder, schizophrenia, can develop from a range of differently implicated genetic alterations and impaired biological systems, and that the key to moving towards meaningful understanding of this illness and the ability to aid in treatment is to acknowledge and accept these subtypes of pathophysiological mechanisms instead of studying the disorder as a whole. Moving forward we can take advantage of larger samples to find subgroups within meta-analyses, and instead of trying to remove the effect of influential factors, we can strive to integrate them meaningfully into the analytic models used.
There are also specific limitations associated with bringing together studies in large meta-analyses, such as the heterogeneity between samples in scanners, protocols, participant inclusion criteria, and recruitment location. Substantial work by groups such as ENIGMA are creating a shift towards standardized procedures of data collection and analysis to address these differences. A general challenge with collaborations though, is how to define accurate measurements and models that are both consistent and relevant across the studies being brought together. There are many confounds that interact with measurements and impact results. Additionally, many individuals have co-morbidities and potentially subtypes of illnesses that cause variation in their classification and inclusion in studies. As more information is gathered and modelling approaches are developed to take these variables and their complex interactions into account, predictive models relevant to an individual or cohort are likely to become more valuable in the variance they describe.
Another consideration is the timing of many studies in the context of brain maturation and development. Large changes in volume, cortical thickness, growth, and maturation occur across late childhood and adolescence (Sussman et al. 2016). Investigations using GWAS at earlier ages may better capture genetic underpinnings of structural function and development. The aspect of development across time is underutilized in imaging genetic studies, especially considering our knowledge of how temporally dependent gene expression, brain changes, and clinical presentation are. Studying younger samples may be particularly helpful for elucidating disease risk, as opposed to studying adults who may be more indicative of disease progression or course. The increasing number of large youth multimodal datasets such as the PNC hold promise for pursuing these key questions.
Additionally, longitudinal studies provide the opportunity to investigate timing of changes. Thus far, longitudinal imaging genetics findings in adults have varied results, although predominantly declines in gray matter are observed, but this may be partially explained by the genetic effect on variation (Olabi et al. 2011; Vita et al. 2012). A systematic review by Harari and Díaz-caneja (2017) uncovered the few studies analyzing the longitudinal structural changes associated with gene variants. Progressive brain changes were most commonly observed in frontal regions, with small or intermediate effect sizes. None of the findings were replicated, and for the two risk variants with multiple studies there were heterogeneous results, indicating that further work is needed for concrete conclusions.
A further limitation that may affect consistency of imaging genetic findings is that many studies were done with healthy controls, and not individuals with schizophrenia. Studying healthy samples has the advantage of minimizing confounding factors associated with clinical diagnoses. However, there is evidence that results can differ between these populations (Lett et al. 2013), and it is important to consider that effects might be observed only once vulnerability for schizophrenia development has progressed to full illness onset. Although there is support that disease risk lies along a continuum, there may still be a tipping point leading to illness onset and a cascade of risk mechanisms and emerging effects.
A final limitation of imaging genetic studies is that the use of MRI cannot capture whether genetic variants are influencing specific cell types within the brain, which may be contributing to a lessened signal strength for association with imaging phenotypes. The use of both imaging and genetics methods to study schizophrenia need to be interpreted within the context of their methodology and limitations.
13 Conclusion
As the field evolves rapidly in terms of technology, method development, collaborative initiatives, sample sizes, and statistical power, there is no doubt that new discoveries will continue to be made regarding the genetic risk and neural circuit disruptions underlying schizophrenia. Huge progress has been made that can inform new initiatives and redirect focus moving forward. A recent project, the Adolescent Brain Cognitive Development (ABCD), is a massive longitudinal study with well characterized phenotyping and multimodal assessments of a population sample (Casey et al. 2018). This rigorous multi-site study includes over 11,000 American children ages 9–10 who will receive follow up assessments every year for the next 10 years. As a publically available resource, there is immense potential for improving our understanding of the development of mental illnesses, cognition, and overall neurodevelopment across adolescence including the effect of environmental and genetic influences.
Another opportunity is the integration of multiple data types, such as structural and functional imaging, clinical, cognitive, and genetic risk measures into models that can capture complex patterns across individuals. Further, clustering algorithms able to integrate these diverse data, such as Similarity Network Fusion (Wang et al. 2014), can be used to group participants into more biologically and functionally homogeneous groups in a way that is agnostic to diagnostic labels. These subgroups within schizophrenia or psychosis may be useful for developing and targeting treatments and interventions in a more personalized way that takes into account specific biological alterations and genetic risk, instead of just inferences from symptomology.
Summary
-
Schizophrenia is highly heritable and has heterogeneous and polygenic contributions to risk.
-
Studies integrating genetic and imaging approaches can improve our understanding of pathophysiology and aid in the identification of endophenotypes or intermediate biomarkers between genotype and disorder risk.
-
Hypothesis driven studies focusing on single candidate genes complement data-driven GWAS that identify novel variants in improving our understanding of mechanisms underlying schizophrenia development.
-
Polygenic risk scores that aggregate the effects of many risk variants increases the amount of explained variance and has potential for an accessible, inexpensive, and effective method for determining individualized risk.
-
There has been a surge in collaborative efforts that increase sample sizes and power with meta-analyses, but results have been mixed in terms of overlapping with previous findings and hypotheses.
-
Examining genetic variants that affect gene expression levels (eQTL) and regional gene expression across the brain provide a possible mechanism by which variants may influence imaging phenotypes, confer risk for schizophrenia, and provide insight into why brain changes are concentrated in certain areas or along specific pathways in schizophrenia.
-
Studying youth at all stages of psychosis development provides the opportunity to evaluate changes across the emergence of symptoms and answer the question of when, in addition to how, genetic factors confer risk by affecting brain structure and function, in addition to aiding with early detection and treatment of psychosis at prodromal stages.
-
Although imaging genetic studies face challenges such as the high dimensionality of data, lack of findings replication, and heterogeneity in samples, there has been progress in developing strategies to overcome these obstacles.
References
Adriano F, Caltagirone C, Spalletta G. Hippocampal volume reduction in first-episode and chronic schizophrenia. Neuroscientist. 2012;18(2):180–200.
Anderson KM, Holmes AJ, Krienen FM, Choi EY, Reinen JM, Yeo BTT. Gene expression links functional networks across cortex and striatum. Nat Commun. 2018;9:1428. https://doi.org/10.1038/s41467-018-03811-x.
Arslan A. Genes, brains, and behavior: imaging genetics for neuropsychiatric disorders. J Neuropsychiatry Clin Neurosci. 2015;27:81–92. https://doi.org/10.1176/appi.neuropsych.13080185.
Arslan A. Progress in neuropsychopharmacology & biological psychiatry imaging genetics of schizophrenia in the post-GWAS era. Prog Neuropsychopharmacol Biol Psychiatry. 2018a;80:155–65. https://doi.org/10.1016/j.pnpbp.2017.06.018.
Arslan A. Mapping the schizophrenia genes by neuroimaging: the opportunities and the challenges. Int J Mol Sci. 2018b;19:E219. https://doi.org/10.3390/ijms19010219.
Berridge MJ. Calcium signalling and psychiatric disease: bipolar disorder and schizophrenia. Cell Tissue Res. 2014;357:477–92. https://doi.org/10.1007/s00441-014-1805-z.
Bigdeli TB, Ripke S, Bacanu SA, Lee SH, Wray NR, Gejman PV, et al. Genome-wide association study reveals greater polygenic loading for schizophrenia in cases with a family history of illness. Am J Med Genet. 2016;171B:276–89. https://doi.org/10.1002/ajmg.b.32402.
Birn RM, Bandettini PA. The effect of stimulus duty cycle and “off” duration on BOLD response linearity. Neuroimage. 2005;27:70–82. https://doi.org/10.1016/j.neuroimage.2005.03.040.
Blokland GA, Zubicaray GI, McMahon KL, Wright MJ. Genetic and environmental influences on neuroimaging phenotypes: a meta-analytical perspective on twin imaging studies. Twin Res Hum Genet. 2012;15:351–71. https://doi.org/10.1017/thg.2012.11.Genetic.
Blokland GAM, del Re EC, Mesholam-Gately RI, Jovicich J, Trampush JW, Keshavan MS, DeLisi LE, Walters JTR, Turner JA, Malhotra AK, Lencz T, Shenton ME, Voineskos AN, Rujescu D, Giegling I, Kahn RS, Roffman JL, Holt DJ, Ehrlich S, Kikinis Z, Dazzan P, Murray RM, Di Forti M, Lee J, Sim K, Lam M, Wolthusen RPF, de Zwarte SMC, Walton E, Cosgrove D, Kelly S, Maleki N, Osiecki L, Picchioni MM, Bramon E, Russo M, David AS, Mondelli V, Reinders AATS, Aurora Falcone M, Hartmann AM, Konte B, Morris DW, Gill M, Corvin AP, Cahn W, Ho NF, Liu JJ, Keefe RSE, Gollub RL, Manoach DS, Calhoun VD, Charles Schulz S, Sponheim SR, Goff DC, Buka SL, Cherkerzian S, Thermenos HW, Kubicki M, Nestor PG, Dickie EW, Vassos E, Ciufolini S, Marques TR, Crossley NA, Purcell SM, Smoller JW, van Haren NEM, Toulopoulou T, Donohoe G, Goldstein JM, Seidman LJ, McCarley RW, Petryshen TL. The genetics of endophenotypes of neurofunction to understand schizophrenia (GENUS) consortium: a collaborative cognitive and neuroimaging genetics project. Schizophr Res. 2018;195:306–17.
Boedhoe PS, Schmaal L, Abe Y, Ameis SH, Arnold PD, Batistuzzo MC, et al. Distinct subcortical volume alterations in pediatric and adult OCD: a worldwide meta- and mega-analysis. Am J Psychiatry. 2017;174:60–9. https://doi.org/10.1176/appi.ajp.2016.16020201.
Bogdan R, Salmeron BJ, Carey CE, Agrawal A, Calhoun VD, Garavan H, et al. Review imaging genetics and genomics in psychiatry: a critical review of progress and potential. Biol Psychiatry. 2017;82:165–75. https://doi.org/10.1016/j.biopsych.2016.12.030.
Bousman CA, Yung AR, Pantelis C, Ellis JA, Chavez RA, Nelson B, Lin A, Wood SJ, Amminger GP, Velakoulis D, Mcgorry PD, Everall IP, Foley DL. Effects of NRG1 and DAOA genetic variation on transition to psychosis in individuals at ultra-high risk for psychosis. Transl Psychiatry. 2013;3:e251. https://doi.org/10.1038/tp.2013.23.
Bousman CA, Cropley V, Klauser P, Hess JL, Pereira A, Idrizi R, Bruggemann J. Neuregulin-1 (NRG1) polymorphisms linked with psychosis transition are associated with enlarged lateral ventricles and white matter disruption in schizophrenia. Psychol Med. 2018;48:801–9. https://doi.org/10.1017/S0033291717002173.
Bray NJ, Hill MJ. Translating genetic risk loci into molecular risk mechanisms for schizophrenia. Schizophr Bull. 2015;42:5–8. https://doi.org/10.1093/schbul/sbv156.
Bustamante ML, Herrera L, Gaspar PA, Nieto R, Maturana A, Villar MJ, et al. Shifting the focus toward rare variants in schizophrenia to close the gap from genotype to phenotype. Am J Med Genet. 2017;174B:663–70. https://doi.org/10.1002/ajmg.b.32550.
Button KS, Ioannidis JP, Mokrysz C, Nosek BA, Flint J, Robinson ES, Munafò MR. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013;14(5):365–76. https://doi.org/10.1038/nrn3475.
Cariaga-Martinez A, Alelú-Paz R. Rethinking the epigenetic framework to unravel the molecular pathology of schizophrenia. Int J Mol Sci. 2017;18(4):790. https://doi.org/10.3390/ijms18040790.
Carter CS, Bearden CE, Bullmore ET, Geschwind DH, Glahn DC, Gur RE, et al. Review enhancing the informativeness and replicability of imaging genomics studies. Biol Psychiatry. 2017;82:157–64. https://doi.org/10.1016/j.biopsych.2016.08.019.
Caseras X, Tansey K, Foley S, Linden D. Association between genetic risk scoring for schizophrenia and bipolar disorder with regional subcortical volumes. Transl Psychiatry. 2015;5:e692. https://doi.org/10.1038/tp.2015.195.
Casey BJ, Cannonier T, Conley MI, Cohen AO, Barch DM, Heitzeg MM, et al. The Adolescent Brain Cognitive Development (ABCD) study: imaging acquisition across 21 sites. Dev Cogn Neurosci. 2018;32:43–54. https://doi.org/10.1016/j.dcn.2018.03.001.
Cassoli JS, Guest PC, Malchow B, Schmitt A, Falkai P, Martins-de-Souza D. Disturbed macro-connectivity in schizophrenia linked to oligodendrocyte dysfunction: from structural findings to molecules. NPJ Schizophr. 2015;1:15034. https://doi.org/10.1038/npjschz.2015.34.
Chang H, Xiao X, Li M. The schizophrenia risk gene ZNF804A: clinical associations, biological mechanisms and neuronal functions. Mol Psychiatry. 2017;22(7):944–53.
Chavarria-siles I, White T, De Leeuw C, Goudriaan A, Lips E, Ehrlich S, et al. Myelination-related genes are associated with decreased white matter integrity in schizophrenia. Eur J Hum Genet. 2015;24(3):381–6. https://doi.org/10.1038/ejhg.2015.120.
Chekouo T, Stingo FC, Guindani M, Do K-A. A Bayesian predictive model for imaging genetics with application to schizophrenia. Ann Appl Stat. 2016;10(3):1547–71. https://doi.org/10.1214/16-AOAS948.
Chen S, Velardez MO, Warot X, Yu ZX, Miller SJ, Cros D, Corfas G. Neuregulin 1-erbB signaling is necessary for normal myeli- nation and sensory function. J Neurosci. 2016;26:3079–86. https://doi.org/10.1523/JNEUROSCI.3785-05.2006.
Chen J, Rashid B, Yu Q, Liu J, Lin D, Du Y. Variability in resting state network and functional network connectivity associated with schizophrenia genetic risk: a pilot study. Front Neurosci. 2018;12:114. https://doi.org/10.3389/fnins.2018.00114.
Cordova-Palomera A, Kaufmann T, Bettella F, Wang Y, Doan NT, Van Der Meer D, Westlye LT, et al. Effects of autozygosity and schizophrenia polygenic risk on cognitive and brain developmental trajectories. Eur J Hum Genet. 2018;26:1049–59. https://doi.org/10.1101/159939.
Cousijn H, Rijpkema M, Harteveld A, et al. Schizophrenia risk gene ZNF804A does not influence macroscopic brain structure: an MRI study in 892 volunteers. Mol Psychiatry. 2012;17(12):1155–7. https://doi.org/10.1038/mp.2011.181.
Cross-Disorder Group of the Psychiatric Genomics Consortium. Genetic relationship between five psychiatric disorders estimated from genome-wide ANPs. Nat Genet. 2013a;45:984–94. https://doi.org/10.1038/ng.2711.
Cross-Disorder Group of the Psychiatric Genomics Consortium. Identification of risk loci with shared effects on five major psychiatric disorders: a genome-wide analysis. Lancet. 2013b;381(9875):1371–9. https://doi.org/10.1016/S0140-6736(12)62129-1.
Davis J, Eyre H, Jacka FN, Dodd S, Dean O, McEwen S, et al. A review of vulnerability and risks for schizophrenia: beyond the two hit hypothesis. Neurosci Biobehav Rev. 2016;65:185–94. https://doi.org/10.1016/j.neubiorev.2016.03.017.
Deans MPJ, Raval P, Sellers JK, Gatford JFN, Halai S, Duarte RRR, et al. Psychosis risk candidate ZNF804A localizes to synapses and regulates neurite formation and dendritic spine structure. Biol Psychiatry. 2016;82(1):49–61. https://doi.org/10.1016/j.biopsych.2016.08.038.
Devor A, Andreassen O, Wang Y, Mäki-Marttunen T, Smeland O, Fan C-C, et al. Genetic evidence for role of integration of fast and slow neurotransmission in schizophrenia. Mol Psychiatry. 2017;22(6):792–801. https://doi.org/10.1038/mp.2017.33.
Dima D, Breen G. Polygenic risk scores in imaging genetics: usefulness and applications. J Psychopharmacol. 2015;29(8):867–71. https://doi.org/10.1177/0269881115584470.
Donohoe G, Rose E, Frodl T, et al. ZNF804A risk allele is associated with relatively intact gray matter volume in patients with schizophrenia. Neuroimage. 2011;54(3):2132–7. https://doi.org/10.1016/j.neuroimage.2010.09.089.
Erk S, Mohnke S, Ripke S, Lett TA, Veer IM, Wackerhagen C, et al. Functional neuroimaging effects of recently discovered genetic risk loci for schizophrenia and polygenic risk profile in five RDoC subdomains. Transl Psychiatry. 2017;27(1):e997. https://doi.org/10.1038/tp.2016.272.
Esslinger C, Walter H, Kirsch P, Erk S, Schnell K, Arnold C, et al. Neural mechanisms of a genome-wide supported psychosis variant. Science. 2009;324:605. https://doi.org/10.1126/science.1167768.
Esslinger C, Kirsch P, Haddad L, Mier D, Sauer C, Erk S, et al. NeuroImage cognitive state and connectivity effects of the genome-wide significant psychosis variant in ZNF804A. Neuroimage. 2011;54(3):2514–23. https://doi.org/10.1016/j.neuroimage.2010.10.012.
Farrell MS, Werge T, Sklar P, Owen MJ, Ophoff RA, O’Donovan MC, Corvin A, Cichon S, Sullivan PF. Evaluating historical candidate genes for schizophrenia. Mol Psychiatry. 2015;20:555–62. https://doi.org/10.1038/mp.2015.16.
Fernandes CP, Westlye LT, Giddaluru S, Christoforou A, Kauppi K, Adolfsson R, Nilsson LG, Nyberg L, Lundervold AJ, Reinvang I, Steen VM, Le Hellard S, Espeseth T. Lack of association of the rs1344706 ZNF804A variant with cognitive functions and DTI indices of white matter microstructure in two in- dependent healthy populations. Psychiatry Res. 2014;222(1–2):60–6. https://doi.org/10.1016/j.pscychresns.2014.02.009.
Flint J, Munafò MR. Candidate and non-candidate genes in behavior genetics. Curr Opin Neurobiol. 2013;23:57–61. https://doi.org/10.1016/j.conb.2012.07.005.
Franke B, Stein JL, Ripke S, Anttila V, Hibar DP, van Hulzen KJ, et al. Genetic influences on schizophrenia and subcortical brain volumes: large-scale proof of concept. Nat Neurosci. 2016;19:420–31. https://doi.org/10.1038/nn.4228.
French L, Gray C, Leonard G, et al. Early cannabis use, polygenic risk score for schizophrenia and brain maturation in adolescence. JAMA Psychiat. 2015;72:1002–11. https://doi.org/10.1001/jamapsychiatry.2015.1131.
Fromer M, Roussos P, Sieberts SK, Johnson JS, Kavanagh DH, Perumal TM, et al. Gene expression elucidates functional impact of polygenic risk for schizophrenia. Nat Neurosci. 2016;19(11):1442–53. https://doi.org/10.1038/nn.4399.
Fu Y, Ma Z, Hamilton C, Liang Z, Hou X, Ma X, et al. Genetic influences on resting-state functional networks: a twin study. Hum Brain Mapp. 2015;36:3959–72. https://doi.org/10.1002/hbm.22890.
Fusar-Poli P, Mcguire P, Borgwardt S. Mapping prodromal psychosis: a critical review of neuroimaging studies. Eur Psychiatry. 2012;27(3):181–91. https://doi.org/10.1016/j.eurpsy.2011.06.006.
Fusar-Poli P, Borgwardt S, Bechdolf A, Addington J, Riecher-Rössler A, Schultze-Lutter F, et al. The psychosis high-risk state: a comprehensive state-of-the-art review. JAMA Psychiat. 2015;70(1):107–20. https://doi.org/10.1001/jamapsychiatry.2013.269.The.
Germine L, Robinson EB, Smoller JW, Calkins ME, Moore TM, Hakonarson H, et al. Association between polygenic risk for schizophrenia, neurocognition and social cognition across development. Transl Psychiatry. 2016;6(10):e924–7. https://doi.org/10.1038/tp.2016.147.
Giaroli G, Bass N, Strydom A, Rantell K, McQuillin A. Does rare matter? Copy number variants at 16p11.2 and the risk of psychosis: a systematic review of literature and meta-analysis. Schizophr Res. 2014;159:340–6. https://doi.org/10.1016/j.schres.2014.09.025.
Girgenti MJ, LoTurco JJ, Maher BJ. ZNF804a regulates expression of the schizophrenia-associated genes PRSS16, COMT, PDE4B, and DRD2. PLoS One. 2012;7(2):e32404. https://doi.org/10.1371/journal.pone.0032404.
Glahn DC, Winkler A, Kochunov P, Almasy L, Duggirala R, Carless M, et al. Genetic control over the resting brain. Proc Natl Acad Sci U S A. 2010;107:1223–8. https://doi.org/10.1073/pnas.0909969107.
Gonzalez-Castro TB, Hernandez-Diaz Y, Juarez-Rojop IE, Lopez-Narvaez ML, Tovilla-Zarate CA, Fresan A. The role of a catechol-O-methyltransferase (COMT) Val158Met genetic polymorphism in schizophrenia: A systematic review and updated meta-analysis on 32,816 subjects. Neuromolecular Med. 2016;18:216–23. https://doi.org/10.1007/s12017-016-8392-z.
Greenlaw K, Szefer E, Graham J, Lesperance M, Nathoo FS. A Bayesian group sparse multi-task regression model for imaging genetics arXiv: 1605. 02234v2 [stat. ME]; 2016.
Gurung R, Prata DP. What is the impact of genome-wide supported risk variants for schizophrenia and bipolar disorder on brain structure and function? A systematic review. Psychol Med. 2015;45(12):2461–80. https://doi.org/10.1017/S0033291715000537.
Hagenaars SP, Harris SE, Davies G, et al. Shared genetic aetiology between cognitive functions and physical and mental health in UK biobank (N = 112 151) and 24 GWAS consortia. Mol Psychiatry. 2016;21:1624–32. https://doi.org/10.1038/mp.2015.225.
Hall J, Whalley HC, Job DE, Baig BJ, Mcintosh AM, Evans KL, Thomson PA, Porteous DJ, Cunningham-Owens DG, Johnstone EC, Lawrie SM. A neuregulin 1 variant associated with abnormal cortical function and psychotic symptoms. Nat Neurosci. 2006;9:1477–8. https://doi.org/10.1038/nn1795.
Hall J, Trent S, Thomas KL, O’Donovan MC, Owen MJ. Genetic risk for schizophrenia: convergence on synaptic pathways involved in plasticity. Biol Psychiatry. 2015;77:52–8. https://doi.org/10.1016/j.biopsych.2014.07.011.
Harari JH, Díaz-caneja CM. The association between gene variants and longitudinal structural brain changes in psychosis: a systematic review of longitudinal neuroimaging genetics studies. NPJ Schizophr. 2017;3:40. https://doi.org/10.1038/s41537-017-0036-2.
Hariri AR, Mattay VS, Tessitore A, et al. Serotonin transporter genetic variation and the response of the human amygdala. Science. 2002;297:400–3. https://doi.org/10.1126/science.1071829.
Harrisberger F, Smieskova R, Schmidt A, Lenz C, Walter A, Wittfeld K. Neuroscience and biobehavioral reviews BDNF Val66Met polymorphism and hippocampal volume in neuropsychiatric disorders: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2015;55:107–18. https://doi.org/10.1016/j.neubiorev.2015.04.017.
Harrisberger F, Smieskova R, Vogler C, et al. Impact of polygenic schizophrenia-related risk and hippocampal volumes on the onset of psychosis. Transl Psychiatry. 2016;6(8):e868. https://doi.org/10.1038/tp.2016.143.
Harrison PJ. Recent genetic findings in schizophrenia and their therapeutic relevance. J Psychopharmacol. 2015;29(2):85–96. https://doi.org/10.1177/0269881114553647.
Hashimoto R, Ohi K, Yamamori H, Yasuda Y, Fujimoto M. Imaging genetics and psychiatric disorders. Curr Mol Med. 2015;15(2):168–75.
Hawrylycz M, Lein E, Guillozet-Bongaarts A, Shen E, Ng L, Miller J, et al. An anatomically comprehensive atlas of the adult human brain transcriptome. Nature. 2012;489:391–9. https://doi.org/10.1038/nature11405.
Hibar DP, Stein JL, Renteria ME, Arias-Vasquez A, Desrivières S, Jahanshad N, Toro R, Wittfeld K, Abramovic L, Andersson M, Aribisala BS, Armstrong NJ, Bernard M, Bohlken MM, Boks MP, Bralten J, Brown AA, Mallar Chakravarty M, Chen Q, Ching CRK, Cuellar-Partida G, den Braber A, Giddaluru S, Goldman AL, Grimm O, Guadalupe T, Hass J, Woldehawariat G, Holmes AJ, Hoogman M, Janowitz D, Jia T, Kim S, Klein M, Kraemer B, Lee PH, Olde Loohuis LM, Luciano M, Macare C, Mather KA, Mattheisen M, Milaneschi Y, Nho K, Papmeyer M, Ramasamy A, Risacher SL, Roiz-Santiañez R, Rose EJ, Salami A, Sämann PG, Schmaal L, Schork AJ, Shin J, Strike LT, Teumer A, van Donkelaar MMJ, van Eijk KR, Walters RK, Westlye LT, Whelan CD, Winkler AM, Zwiers MP, Alhusaini S, Athanasiu L, Ehrlich S, Hakobjan MMH, Hartberg CB, Haukvik UK, Heister AJGAM, Hoehn D, Kasperaviciute D, Liewald DCM, Lopez LM, Makkinje RRR, Matarin M, Naber MAM, McKay DR, Needham M, Nugent AC, Pütz B, Royle NA, Shen L, Sprooten E, Trabzuni D, van der Marel SSL, van Hulzen KJE, Walton E, Wolf C, Almasy L, Ames D, Arepalli S, Assareh AA, Bastin ME, Brodaty H, Bulayeva KB, Carless MA, Cichon S, Corvin A, Curran JE, Czisch M, de Zubicaray GI, Dillman A, Duggirala R, Dyer TD, Erk S, Fedko IO, Ferrucci L, Foroud TM, Fox PT, Fukunaga M, Gibbs JR, Göring HHH, Green RC, Guelfi S, Hansell NK, Hartman CA, Hegenscheid K, Heinz A, Hernandez DG, Heslenfeld DJ, Hoekstra PJ, Holsboer F, Homuth G, Hottenga J-J, Ikeda M, Jack CR, Jenkinson M, Johnson R, Kanai R, Keil M, Kent JW, Kochunov P, Kwok JB, Lawrie SM, Liu X, Longo DL, McMahon KL, Meisenzahl E, Melle I, Mohnke S, Montgomery GW, Mostert JC, Mühleisen TW, Nalls MA, Nichols TE, Nilsson LG, Nöthen MM, Ohi K, Olvera RL, Perez-Iglesias R, Pike GB, Potkin SG, Reinvang I, Reppermund S, Rietschel M, Romanczuk-Seiferth N, Rosen GD, Rujescu D, Schnell K, Schofield PR, Smith C, Steen VM, Sussmann JE, Thalamuthu A, Toga AW, Traynor BJ, Troncoso J, Turner JA, Valdés Hernández MC, van’t Ent D, van der Brug M, van der Wee NJA, van Tol M-J, Veltman DJ, Wassink TH, Westman E, Zielke RH, Zonderman AB, Ashbrook DG, Hager R, Lu L, McMahon FJ, Morris DW, Williams RW, Brunner HG, Buckner RL, Buitelaar JK, Cahn W, Calhoun VD, Cavalleri GL, Crespo-Facorro B, Dale AM, Davies GE, Delanty N, Depondt C, Djurovic S, Drevets WC, Espeseth T, Gollub RL, Ho B-C, Hoffmann W, Hosten N, Kahn RS, Le Hellard S, Meyer-Lindenberg A, Müller-Myhsok B, Nauck M, Nyberg L, Pandolfo M, Penninx BWJH, Roffman JL, Sisodiya SM, Smoller JW, van Bokhoven H, van Haren NEM, Völzke H, Walter H, Weiner MW, Wen W, White T, Agartz I, Andreassen OA, Blangero J, Boomsma DI, Brouwer RM, Cannon DM, Cookson MR, de Geus EJC, Deary IJ, Donohoe G, Fernández G, Fisher SE, Francks C, Glahn DC, Grabe HJ, Gruber O, Hardy J, Hashimoto R, Hulshoff Pol HE, Jönsson EG, Kloszewska I, Lovestone S, Mattay VS, Mecocci P, McDonald C, McIntosh AM, Ophoff RA, Paus T, Pausova Z, Ryten M, Sachdev PS, Saykin AJ, Simmons A, Singleton A, Soininen H, Wardlaw JM, Weale ME, Weinberger DR, Adams HHH, Launer LJ, Seiler S, Schmidt R, Chauhan G, Satizabal CL, Becker JT, Yanek L, van der Lee SJ, Ebling M, Fischl B, Longstreth WT, Greve D, Schmidt H, Nyquist P, Vinke LN, van Duijn CM, Xue L, Mazoyer B, Bis JC, Gudnason V, Seshadri S, Ikram MA, Martin NG, Wright MJ, Schumann G, Franke B, Thompson PM, Medland SE. Common genetic variants influence human subcortical brain structures. Nature. 2015;520(7546):224–9.
Hibar DP, Adams HHH, Jahanshad N, Chauhan G, Stein JL, Hofer E, et al. Novel genetic loci associated with hippocampal volume. Nat Commun. 2017;8:13624. https://doi.org/10.1038/ncomms13624.
Hill MJ, Bray NJ. Evidence that schizophrenia risk variation in the ZNF804A gene exerts its effects during fetal brain development. Am J Psychiatry. 2012;169:1301–8. https://doi.org/10.1176/appi.aip.2012.11121845.
Hill MJ, Jeffries AR, Dobson RJ, Price J, Bray NJ. Knockdown of the psychosis susceptibility gene ZNF804A alters expression of genes involved in cell adhesion. Hum Mol Genet. 2012;21(5):1018–24. https://doi.org/10.1093/hmg/ddr532.
Ho BC, Andreasen NC, Ziebell S, Pierson R, Magnotta V. Long-term antipsychotic treatment and brain volumes: a longitudinal study of first-episode schizophrenia. Arch Gen Psychiatry. 2011;68:128–37. https://doi.org/10.1001/archgenpsychiatry.2010.199.
Hong CJ, Liou YJ, Tsai SJ. Effects of BDNF polymorphisms on brain function and behavior in health and disease. Brain Res Bull. 2011;86:287–97. https://doi.org/10.1016/j.brainresbull.2011.08.019.
Hoogman M, Bralten J, Hibar DP, Mennes M, Zwiers MP, Schweren LS, van Hulzen KJ, Medland SE, Shumskaya E, Jahanshad N, et al. Subcortical brain volume differences of participants with ADHD across the lifespan: an ENIGMA collaboration. Lancet Psychiatry. 2017;4:310–9. https://doi.org/10.1016/S2215-0366(17)30049-4.
Horváth S, Janka Z, Mirnics K. Analyzing schizophrenia by DNA microarrays. Biol Psychiatry. 2011;69:157–62. https://doi.org/10.1016/j.biopysch.2010.07.017.
Howes OD, Mccutcheon R. Inflammation and the neural diathesis-stress hypothesis of schizophrenia: a reconceptualization. Transl Psychiatry. 2017;7(2):e1024–11. https://doi.org/10.1038/tp.2016.278.
Howes OD, McCutcheon R, Owen MJ, Murray R. The role of genes, stress and dopamine in the development of schizophrenia. Biol Psychiatry. 2017;81(1):9–20. https://doi.org/10.1016/j.biopsych.2016.07.014.
Hubbard L, Tansey KE, Rai D, et al. Evidence of common genetic overlap between schizophrenia and cognition. Schizophr Bull. 2016;42:832–42. https://doi.org/10.1093/schbul/sbv168.
Ikeda M, Aleksic B, Kinoshita Y, Okochi T, Kawashima K, Kushima I, et al. Genome-wide association study of schizophrenia in a Japanese population. Biol Psychiatry. 2011;69:472–8. https://doi.org/10.1016/j.biopsych.2010.07.010.
Ikuta T, Peters BD, Guha S, John M, Karlsgodt KH, Lencz T, et al. A schizophrenia risk gene, ZNF804A, is associated with brain white matter microstructure. Schizophr Res. 2014;155(1–3):15–20. https://doi.org/10.1016/j.schres.2014.03.001.
Insel TR. Rethinking schizophrenia. Nature. 2010;468:187–93.
Jansen AG, Mous SE, White T, Posthuma D, Polderman TJ. What twin studies tell us about the heritability of brain development, morphology, and function: a review. Neuropsychol Rev. 2015;25:27–46.
Kang HJ, et al. Spatio-temporal transcriptome of the human brain. Nature. 2012;478:483–9.
Kang M, Zhang C, Chun H-W, Ding C, Liu C, Gao J. eQTL epistasis: detecting epistatic effects and inferring hierarchical relationships of genes in biological pathways. Bioinformatics. 2015;31(5):656–64.
Kauppi K, Westlye LT, Tesli M, et al. Polygenic risk for schiz- ophrenia associated with working memory-related prefrontal brain activation in patients with schizophrenia and healthy controls. Schizophr Bull. 2014;41:736–43.
Keri S, Kiss I, Kelemen O. Effects of a neuregulin 1 variant on conversion to schizophrenia and schizophreniform disorder in people at high risk for psychosis. Mol Psychiatry. 2009;14:118–9.
Kuswanto CN, Sum MY, Qiu A, Sitoh Y, Liu J, Sim K. The impact of genome wide supported MicroRNA- 137 ( MIR137 ) risk variants on frontal and striatal White matter integrity, neurocognitive functioning, and negative symptoms in schizophrenia. Am J Med Genet B Neuropsychiatr Genet. 2015;168B(5):317–26. https://doi.org/10.1002/ajmg.b.32314.
Lancaster T, Doherty J, Linden DE, Hall J. Imaging genetics of schizophrenia. In: Bigos KL, Hariri AR, Weinberger DR, editors. Neuroimaging genetics: principles and practices. Oxford, New York: Oxford University Press; 2016a.
Lancaster TM, Ihssen N, Brindley LM, et al. Associations between polygenic risk for schizophrenia and brain function during probabilistic learning in healthy individuals. Hum Brain Mapp. 2016b;37:491–500.
Lancaster TM, Dimitriadis SL, Tansey KE, Perry G, Ihssen N, Jones DK, et al. Structural and functional neuroimaging of polygenic risk for schizophrenia: a recall-by-genotype—based approach. Schizophr Bull. 2018;(April):1–3. https://doi.org/10.1093/schbul/sby037.
Lee S, Abecasis GR, Boehnke M, Lin X. Rare-variant association analysis: study designs and statistical tests. Am J Hum Genet. 2014;95:5–23. https://doi.org/10.1016/j.ajhg.2014.06.009.
Lee PH, Baker JT, Holmes AJ, Jahanshad N, Ge T, Jung J, et al. Partitioning heritability analysis reveals a shared genetic basis of brain anatomy and schizophrenia. 2016;(August):1680–9. https://doi.org/10.1038/mp.2016.164.
Lett TA, Chakavarty MM, Felsky D, Brandl EJ, Tiwari AK, Gonçalves VF, Rajji TK, Daskalakis ZJ, Meltzer HY, Lieberman JA, Lerch JP, Mulsant BH, Kennedy JL, Voineskos AN. The genome-wide supported microRNA-137 variant predicts phenotypic heterogeneity within schizophrenia. Mol Psychiatry. 2013;18(4):443–50.
Li M, Huang L, Wang J, Su B, Luo X-J. No association between schizophrenia susceptibility variants and macroscopic structural brain volume variation in healthy subjects. Am J Med Genet B Neuropsychiatr Genet. 2015;171B(2):160–8.
Lidow MS. Calcium signaling dysfunction in schizophrenia: a unifying approach. Brain Res Brain Res Rev. 2003;43:70–84.
Liu B, Zhang X, Cui Y, Qin W, Tao Y, Li J. Polygenic risk for schizophrenia influences cortical gyrification in 2 independent general populations. Schizophr Bull. 2017;43(3):673–80. https://doi.org/10.1093/schbul/sbw051.
Luykx JJ, Broersen JL, Leeuw MD. Neuroscience and biobehavioral reviews the DRD2 rs1076560 polymorphism and schizophrenia-related intermediate phenotypes: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2017;74:214–24. https://doi.org/10.1016/j.neubiorev.2017.01.006.
Mallas E, Carletti F, Chaddock CA, Kalidindi S, Bramon E, Murray R, Barker GJ (2017) The impact of CACNA1C gene, and its epistasis with ZNF804A, on white matter microstructure in health, schizophrenia and bipolar disorder, vol 1, pp. 479–488. https://doi.org/10.1111/gbb.12355.
Manrique-Garcia E, Zammit S, Dalman C, Hemmingsson T, Andreasson S, Allebeck P. Cannabis, schizophrenia and other non-affective psychoses: 35 years of follow-up of a population-based cohort. Psychol Med. 2012;42(6):1321–8.
Marenco S, Weinberger DR. The neurodevelopmental hypothesis of schizophrenia: following a trail of evidence from cradle to grave. Dev Psychopathol. 2000;12:501–27.
Mathalon DH, Sullivan EV, Lim KO, Pfefferbaum A. Progres- sive brain volume changes and the clinical course of schizophrenia in men: a longitudinal magnetic resonance imaging study. Arch Gen Psychiatry. 2001;58:148–57.
McGrath J, Saha S, Chant D, Welham J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev. 2008;30:67–76.
Meltzer HY, Stahl SM. The dopamine hypothesis of schizophrenia: a review. Schizophrenia bulletin. Bethesda: National Institute of Mental Health; 1976. https://doi.org/10.1093/schbul/2.1.19.
Mendrek A, Mancini-Marïe A. Sex/gender differences in the brain and cognition in schizophrenia. Neurosci Biobehav Rev. 2016;67:57–78. https://doi.org/10.1016/j.neubiorev.2015.10.013.
Meyer-Lindenberg A. Imaging genetics of schizophrenia. Transl Res. 2010:449–56.
Millan MJ, Andrieux A, Bartzokis G, Cadenhead K, Dazzan P. Altering the course of schizophrenia: progress and perspectives. Nat Publ Group. 2016;15(7):485–515. https://doi.org/10.1038/nrd.2016.28.
Moghaddam B, Javitt D. From revolution to evolution: the glutamate hypothesis of schizophrenia and its implication for treatment. Neuropsychopharmacology. 2012;37:4–15.
Mohnke S, Erk S, Schnell K, Schutz C, Romanczuk-Seiferth N, Grimm O, et al. Further evidence for the impact of a genome-wide-supported psychosis risk variant in ZNF804A on the Theory of Mind Network. Neuropsychopharmacology. 2014;39:1196–205.
Mulle JG. The 3q29 deletion confers >40-fold increase in risk for schizophrenia. Mol Psychiatry. 2015;20:1028–9.
Murphy SE, Norbury R, Godlewska BR, Cowen PJ, Mannie ZM, Harmer CJ, et al. The effect of the serotonin transporter polymorphism (5-HTTLPR) on amygdala function: a meta-analysis. Mol Psychiatry. 2013;18:512–20.
Nakazawa K, Zsiros V, Jiang Z, Nakao K, Kolata S, Zhang S, et al. GABAergic interneuron origin of schizophrenia pathophysiology. Neuropharmacology. 2012;62:1574–83.
Neilson E, Bois C, Gibson J, Duff B, Watson A, Roberts N, et al. Effects of environmental risks and polygenic loading for schizophrenia on cortical thickness. Schizophr Res. 2017;184:128–36. https://doi.org/10.1016/j.schres.2016.12.011.
Oertel-knöchel V, Lancaster TM, Knöchel C, Stäblein M, Storchak H, Reinke B, et al. Clinical Schizophrenia risk variants modulate white matter volume across the psychosis spectrum: evidence from two independent cohorts YNICL. Neuroimage. 2015;7:764–70. https://doi.org/10.1016/j.nicl.2015.03.005.
Ohi K, Hashimoto R, Ikeda M, et al. Genetic risk variants of schizophrenia associated with left superior temporal gyrus volume. Cortex. 2014;58:23–6.
Olabi B, et al. Are there progressive brain changes in schizophrenia? A meta-analysis of structural magnetic resonance imaging studies. Biol Psychiatr. 2011;70:88–96.
Ortega MC, Bribian A, Peregrin S, Gil MT, Marin O, de Castro F. Neuregulin-1/ErbB4 signaling controls the migration of oligodendrocyte precursor cells during development. Exp Neurol. 2012;235:610–20.
Owens SF, Picchioni MM, Ettinger U, et al. Prefrontal deviations in function but not volume are putative endophenotypes for schizophrenia. Brain. 2012;135:2231–44.
Papiol S, Mitjans M, Assogna F, et al. Polygenic determinants of white matter volume derived from GWAS lack reproducibility in a replicate sample. Transl Psychiatry. 2014;4:e362.
Papiol S, Popovic D, Keeser D, Hasan A, Degenhardt F, Rossner MJ, et al. Polygenic risk has an impact on the structural plasticity of hippocampal sub fi elds during aerobic exercise combined with cognitive remediation in multi-episode schizophrenia. Nat Publ Group. 2017;7(6):e1159. https://doi.org/10.1038/tp.2017.131.
Patel S, Park MTM, The Alzheimer’s Disease Neuroimaging Initiative, Chakravarty MM, Knight J. Gene prioritization for imaging genetics studies using gene ontology and a stratified false discovery rate approach. Front Neuroinform. 2016;10:14. https://doi.org/10.3389/fninf.2016.00014.
Pearlson GD, Calhoun VD, Liu J. An introductory review of parallel independent component analysis (p-ICA) and a guide to applying p- ICA to genetic data and imaging phenotypes to identify disease-associated biological pathways and systems in common complex disorders. Front Genet. 2015;6:276. https://doi.org/10.3389/fgene.2015.00276.
Pergola G, Di Carlo P, Ambrosio ED, Gelao B, Fazio L, Papalino M, et al. DRD2 co-expression network and a related polygenic index predict imaging, behavioral and clinical phenotypes linked to schizophrenia. Nat Publ Group. 2017;7(1):e1006–8. https://doi.org/10.1038/tp.2016.253.
Petersen RC, Aisen PS, Beckett LA, Donohue MC, Gamst AC, Harvey DJ, Jack CR, Jagust WJ, Shaw LM, Toga AW, Trojanowski JQ, Weiner MW. Alzheimer’s disease neuroimaging initiative (ADNI): clinical characterization. Neurology. 2010;74(3):201–9.
Pettersson-Yeo W, Benetti S, Marquand AF, Dell’acqua F, Williams SC, Allen P, et al. Using genetic, cognitive and multi-modal neuroimaging data to identify ultra-high-risk and first-episode psychosis at the individual level. Psychol Med. 2013;43(12):2547–62. https://doi.org/10.1017/S003329171300024X.
Polderman TJ, Benyamin B, de Leeuw CA, Sullivan PF, van Bochoven A, Visscher PM, et al. Meta-analysis of the heritability of human traits based on fifty years of twin studies. Nat Genet. 2015;47:702–9.
Powell F, LoCastro E, Acosta D, Ahmed M, O’Donoghue S, Forde N, Cannon D, Scanlon C, Rao T, McDonald C, Raj A. Age-related changes in topological degradation of white matter networks and gene expression in chronic schizophrenia. Brain Connect. 2017;7(9):574–89.
Psaty BM, O’Donnell CJ, Gudnason V, et al. Cohorts for heart and aging research in genomic epidemiology (CHARGE) consortium: design of prospective meta- analyses of genome-wide association studies from 5 cohorts. Circ Cardiovasc Genet. 2009;2:73–80.
Raab K, Kirsch P, Mier D. Neuroscience and biobehavioral reviews understanding the impact of 5-HTTLPR, antidepressants, and acute tryptophan depletion on brain activation during facial emotion processing: a review of the imaging literature. Neurosci Biobehav Rev. 2016;71:176–97. https://doi.org/10.1016/j.neubiorev.2016.08.031.
Rasetti R, Weinberger DR. Intermediate phenotypes in psychiatric disorders. Curr Opin Genet Dev. 2011;21:340–8.
Reus LM, Shen X, Gibson J, et al. Association of polygenic risk for major psychiatric illness with subcortical vol- umes and white matter integrity in UK biobank. Sci Rep. 2017;7:42140.
Richards AL, Jones L, Moskvina V, Kirov G, Gejman PV, Levinson DF, et al. Schizophrenia susceptibility alleles are enriched for alleles that affect gene expression in adult human brain. Mol Psychiatry. 2012;17(2):193–201. https://doi.org/10.1038/mp.2011.11.
Richiardi J, Altmann A, Milazzo A-C, Chang C, Mallar Chakravarty M, Banaschewski T, et al. Correlated gene expression supports synchronous activity in brain networks. Science. 2015;348:1241–4. https://doi.org/10.1126/science.1255905.
Romme IAC, De Reus MA, Ophoff RA, Kahn RS, Van Den Heuvel MP. Connectome disconnectivity and cortical gene expression in patients with schizophrenia. Biol Psychiatry. 2016;81(6):495–502. https://doi.org/10.1016/j.biopsych.2016.07.012.
Satterthwaite TD, Wolf DH, Calkins ME, Vandekar SN, Erus G, Ruparel K, et al. Structural brain abnormalities in youth with psychosis spectrum symptoms. JAMA Psychiat. 2016;73(5):515–24. https://doi.org/10.1001/jamapsychiatry.2015.3463.
Schizophrenia Working Group of the Psychiatric Genomics Consortium. Biological insights from 108 schizophrenia- associated genetic loci. Nature. 2014;511:421–7.
Schmaal L, Veltman DJ, van Erp TG, Sämann PG, Frodl T, Jahanshad N, Loehrer E, Tiemeier H, Hofman A, Niessen WJ, Vernooij MW, Ikram MA, Wittfeld K, Grabe HJ, Block A, Hegenscheid K, Völzke H, Hoehn D, Czisch M, Lagopoulos J, Hatton SN, Hickie IB, Goya-Maldonado R, Krämer B, Gruber O, Couvy-Duchesne B, Rentería ME, Strike LT, Mills NT, de Zubicaray GI, McMahon KL, Medland SE, Martin NG, Gillespie NA, Wright MJ, Hall GB, MacQueen GM, Frey EM, Carballedo A, van Velzen LS, van Tol MJ, van der Wee NJ, Veer IM, Walter H, Schnell K, Schramm E, Normann C, Schoepf D, Konrad C, Zurowski B, Nickson T, McIntosh AM, Papmeyer M, Whalley HC, Sussmann JE, Godlewska BR, Cowen PJ, Fischer FH, Rose M, Penninx BW, Thompson PM, Hibar DP. Subcortical brain alterations in major depressive disorder: findings from the ENIGMA major depressive disorder working group. Mol Psychiatry. 2015;21(6):806–12. https://doi.org/10.1038/mp.2015.69.
Schmitt A, Rujescu D, Gawlik M, Hasan A, Hashimoto K, Iceta S. Consensus paper of the WFSBP Task Force on Biological Markers: criteria for biomarkers and endophenotypes of schizophrenia part II: cognition, neuroimaging and genetics. World J Biol Psychiatry. 2016;17(6):406–28.
Schneider M, Debbané M, Bassett AS, Chow EWC, Fung WLA, van den Bree MBM, et al. Psychiatric disorders from childhood to adulthood in 22q11.2 deletion syndrome: results from the international consortium on brain and behavior in 22q11.2 deletion syndrome. Am J Psychiatry. 2014;171:627–39.
Schork AJ, Wang Y, Thompson WK, Dale AM, Andreassen OA. New statistical approaches exploit the polygenic architecture of schizophrenia—implications for the underlying neurobiology. Curr Opin Neurobiol. 2016;50:89–98. https://doi.org/10.1016/j.conb.2015.10.008.New.
Schumann G, Loth E, Banaschewski T, et al. The IMAGEN study: reinforcement-related behavior in normal brain function and psychopathology. Mol Psychiatry. 2010;15:1128–39.
Sebat J, Malhotra D. CNVs: harbinger of a rare variant revolution in psychiatric genetics. Cell. 2013;148:1223–41.
Sebat J, Levy DL, McCarthy SE. Rare structural variants in schizophrenia: one disorder, multiple mutations; one mutation, multiple disorders. Trends Genet. 2009;25:528–35.
Seidman LJ, Giuliano AJ, Meyer EC, Addington J, Cadenhead KS, Cannon TD, McGlashan TH, Perkins DO, Tsuang MT, Walker EF, Woods SW, Bearden CE, Christensen BK, Hawkins K, Heaton R, Keefe RS, Heinssen R, Cornblatt BA, North American Prodrome Longitudinal Study (NAPLS) Group. Neuropsychology of the prodrome to psychosis in the NAPLS consortium: relationship to family history and conversion to psychosis. Arch Gen Psychiatry. 2010;67(6):578–88.
Sekar A, Bialas AR, de Rivera H, Davis A, Hammond TR, Kamitaki N, et al. Schizophrenia risk from complex variation of complement component 4. Nature. 2016;530(7589):177–83. https://doi.org/10.1038/nature16549.
Smeland OB, Wang Y, Frei O, Li W, Hibar DP, Franke B, Bettella F, Witoelar A, Djurovic S, Chen CH, Thompson PM, Dale AM, Andreassen OA. Genetic overlap between schizophrenia and volumes of hippocampus, putamen, and intracranial volume indicates shared molecular genetic mechanisms. Schizophr Bull. 2017;sbx148. https://doi.org/10.1093/schbul/sbx148
Smieskova R, Marmy J, Schmidt A, Bendfeldt K, Walter M, Lang UE. Do subjects at clinical high risk for psychosis differ from those with a genetic high risk?—a systematic review of structural and functional brain abnormalities; 2013. pp. 467–481.
Sprooten E, McIntosh AM, Lawrie SM, et al. An investigation of a genomewide supported psychosis variant in ZNF804A and white matter integrity in the human brain. Magn Reson Imaging. 2012;30(10):1373–80.
Stedehouder J, Kushner SA. Myelination of parvalbumin interneurons: a parsimonious locus of pathophysiological convergence in schizophrenia. Mol Psychiatry. 2017;22(1):4–12. https://doi.org/10.1038/mp.2016.147.
Stein JL, Medland SE, Vasquez AA, et al. Identification of common variants associated with human hippocampal and intracranial volumes. Nat Genet. 2012;44:552–61.
Stingo FC, Guindani M, Vannucci M, Calhoun VD. An integrative Bayesian modeling approach to imaging genetics. J Am Stat Assoc. 2014;108(503):876–91. https://doi.org/10.1080/01621459.2013.804409.
Studerus E, Ramyead A. Prediction of transition to psychosis in patients with a clinical high risk for psychosis: a systematic review of methodology and reporting. 2017. pp. 1163–1178. https://doi.org/10.1017/S0033291716003494.
Sullivan PF, Kendler KS, Neale MC. Schizophrenia as a complex trait: evidence from a meta-analysis of twin studies. Arch Gen Psychiatry. 2003;60:1187–92. https://doi.org/10.1001/archpsyc.60.12.1187.
Sullivan PF, Daly MJ, O’Donovan M. Genetic architectures of psychiatric disorders: the emerging picture and its implications. Nat Rev Genet. 2012;13:537–51.
Sussman D, Leung RC, Chakravarty MM, Lerch JP, Taylor MJ. Developing human brain: age-related changes in cortical, subcortical, and cerebellar anatomy. Brain Behav. 2016;6(4):e00457. https://doi.org/10.1002/brb3.457.
Tao R, Cousijn H, Jaffe AE, Burnet PW, Edwards F, Eastwood SL, et al. Expression of ZNF804A in human brain and alterations in schizophrenia, bipolar disorder, and major depressive disorder: a novel transcript fetally regulated by the psychosis risk variant rs1344706. JAMA Psychiat. 2014;71:1112–20.
Terwisscha van Scheltinga AF, Bakker SC, van Haren NE, et al. Genetic schizophrenia risk variants jointly modulate total brain and white matter volume. Biol Psychiatry. 2013;73(6):525–31.
Thompson PM, Stein JL, Medland SE, Hibar DP, Vasquez AA, Renteria ME, Toro R, Jahanshad N, Schumann G, Franke B, Wright MJ, Martin NG, Agartz I, Alda M, Alhusaini S, Almasy L, Almeida J, Alpert K, Andreasen NC, Andreassen OA, Apostolova LG, Appel K, Armstrong NJ, Aribisala B, Bastin ME, Bauer M, Bearden CE, Bergmann Ø, Binder EB, Blangero J, Bockholt HJ, Bøen E, Bois C, Boomsma DI, Booth T, Bowman IJ, Bralten J, Brouwer RM, Brunner HG, Brohawn DG, Buckner RL, Buitelaar J, Bulayeva K, Bustillo JR, Calhoun VD, Cannon DM, Cantor RM, Carless MA, Caseras X, Cavalleri GL, Mallar Chakravarty M, Chang KD, Ching CRK, Christoforou A, Cichon S, Clark VP, Conrod P, Coppola G, Crespo-Facorro B, Curran JE, Czisch M, Deary IJ, de Geus EJC, den Braber A, Delvecchio G, Depondt C, de Haan L, de Zubicaray GI, Dima D, Dimitrova R, Djurovic S, Dong H, Donohoe G, Duggirala R, Dyer TD, Ehrlich S, Ekman CJ, Elvsåshagen T, Emsell L, Erk S, Espeseth T, Fagerness J, Fears S, Fedko I, Fernández G, Fisher SE, Foroud T, Fox PT, Francks C, Frangou S, Frey EM, Frodl T, Frouin V, Garavan H, Giddaluru S, Glahn DC, Godlewska B, Goldstein RZ, Gollub RL, Grabe HJ, Grimm O, Gruber O, Guadalupe T, Gur RE, Gur RC, Göring HHH, Hagenaars S, Hajek T, Hall GB, Hall J, Hardy J, Hartman CA, Hass J, Hatton SN, Haukvik UK, Hegenscheid K, Heinz A, Hickie IB, Ho B-C, Hoehn D, Hoekstra PJ, Hollinshead M, Holmes AJ, Homuth G, Hoogman M, Hong LE, Hosten N, Hottenga J-J, Hulshoff Pol HE, Hwang KS, Jack CR, Jenkinson M, Johnston C, Jönsson EG, Kahn RS, Kasperaviciute D, Kelly S, Kim S, Kochunov P, Koenders L, Krämer B, Kwok JBJ, Lagopoulos J, Laje G, Landen M, Landman BA, Lauriello J, Lawrie SM, Lee PH, Le Hellard S, Lemaître H, Leonardo CD, Li C-s, Liberg B, Liewald DC, Liu X, Lopez LM, Loth E, Lourdusamy A, Luciano M, Macciardi F, Machielsen MWJ, MacQueen GM, Malt UF, Mandl R, Manoach DS, Martinot J-L, Matarin M, Mather KA, Mattheisen M, Mattingsdal M, Meyer-Lindenberg A, McDonald C, McIntosh AM, McMahon FJ, McMahon KL, Meisenzahl E, Melle I, Milaneschi Y, Mohnke S, Montgomery GW, Morris DW, Moses EK, Mueller BA, Maniega SM, Mühleisen TW, Müller-Myhsok B, Mwangi B, Nauck M, Nho K, Nichols TE, Nilsson L-G, Nugent AC, Nyberg L, Olvera RL, Oosterlaan J, Ophoff RA, Pandolfo M, Papalampropoulou-Tsiridou M, Papmeyer M, Paus T, Pausova Z, Pearlson GD, Penninx BW, Peterson CP, Pfennig A, Phillips M, Pike GB, Poline J-B, Potkin SG, Pütz B, Ramasamy A, Rasmussen J, Rietschel M, Rijpkema M, Risacher SL, Roffman JL, Roiz-Santiañez R, Romanczuk-Seiferth N, Rose EJ, Royle NA, Rujescu D, Ryten M, Sachdev PS, Salami A, Satterthwaite TD, Savitz J, Saykin AJ, Scanlon C, Schmaal L, Schnack HG, Schork AJ, Schulz SC, Schür R, Seidman L, Shen L, Shoemaker JM, Simmons A, Sisodiya SM, Smith C, Smoller JW, Soares JC, Sponheim SR, Sprooten E, Starr JM, Steen VM, Strakowski S, Strike L, Sussmann J, Sämann PG, Teumer A, Toga AW, Tordesillas-Gutierrez D, Trabzuni D, Trost S, Turner J, van den Heuvel M, van der Wee NJ, van Eijk K, van Erp TGM, van Haren NEM, van’t Ent D, van Tol M-J, Valdés Hernández MC, Veltman DJ, Versace A, Völzke H, Walker R, Walter H, Wang L, Wardlaw JM, Weale ME, Weiner MW, Wen W, Westlye LT, Whalley HC, Whelan CD, White T, Winkler AM, Wittfeld K, Woldehawariat G, Wolf C, Zilles D, Zwiers MP, Thalamuthu A, Schofield PR, Freimer NB, Lawrence NS, Drevets W. The ENIGMA Consortium: large-scale collaborative analyses of neuroimaging and genetic data. Brain Imaging Behav. 2014;8(2):153–82.
Thurin K, Rasetti R, Sambataro F, Safrin M, Chen Q, Callicott JH, et al. Effects of ZNF804A on neurophysiologic measures of cognitive control. Mol Psychiatry. 2013;18:852–4.
Toulopoulou T, van Haren N, Zhang X, et al. Reciprocal causation models of cognitive vs volumetric cerebral intermediate phenotypes for schizophrenia in a pan-European twin cohort. Mol Psychiatry. 2015;20:1482.
Trotman HD, Holtzman CW, Ryan AT, Shapiro DI, MacDonald AN, Goulding SM, et al. The development of psychotic disorders in adolescence: a potential role for hormones. Horm Behav. 2013;64(2):411–9. https://doi.org/10.1016/j.yhbeh.2013.02.018.
Van der Auwera S, Wittfeld K, Homuth G, Teumer A, Hegenscheid K, Grabe HJ. No association between polygenic risk for schizophrenia and brain volume in the general population. Biol Psychiatry. 2015;78:e41–2.
Van der Auwera S, Wittfeld K, Shumskaya E, Bralten J, Zwiers MP, Onnink AMH, et al. Predicting brain structure in population-based samples with biologically informed genetic scores for schizophrenia; 2017. pp. 324–32. https://doi.org/10.1002/ajmg.b.32519.
Van Dongen J, Boomsma DI. The evolutionary paradox and the missing heritability of schizophrenia. Am J Med Genet B Neuropsychiatr Genet. 2013;162B:122–36.
Vita A, De Peri L, Deste G, Sacchetti E. Progressive loss of cortical gray matter in schizophrenia: a meta-analysis and meta-regression of longitudinal MRI studies. Transl Psychiatry. 2012;2:e190.
Voineskos AN, Lerch JP, Felsky D, et al. The ZNF804A gene: characterization of a novel neural risk mechanism for the major psychoses. (2011). Neuropsychopharmacology. 2011;36:1871–8.
Voineskos AN, Felsky D, Wheeler AL, Rotenberg DJ, Levesque M, Patel S, et al. Limited evidence for association of genome-wide schizophrenia risk variants on cortical neuroimaging phenotypes. Schizophr Bull. 2015:sbv180. https://doi.org/10.1093/schbul/sbv180.
Walker EF, Trotman HD, Goulding SM, et al. Developmental mechanisms in the prodrome to psychosis. Dev Psychopathol. 2013;25(4 Pt 2):1585–600. https://doi.org/10.1017/S0954579413000783.
Walter H, Schnell K, Erk S, Arnold C, Kirsch P, Esslinger C, et al. Effects of a genome-wide supported psychosis risk variant on neural activation during a theory-of-mind task. Mol Psychiatry. 2011;16:462–70.
Walton E, Turner J, Gollub RL, et al. Cumulative genetic risk and prefrontal activity in patients with schizophrenia. Schizophr Bull. 2013;39:703–11.
Walton E, Geisler D, Lee PH, et al. Prefrontal inefficiency is associated with polygenic risk for schizophrenia. Schizophr Bull. 2014;40:1263–71.
Wang B, Mezlini AM, Demir F, Fiume M, Tu Z, Brudno M, et al. Similarity network fusion for aggregating data types on a genomic scale. Nat Methods. 2014;11:333. https://doi.org/10.1038/nmeth.2810.
Wang C, Jianping S, Bryan G, Tian G, Hibar Derrek P, Greenwood Celia MT, Qiu A, The Alzheimer’s Disease Neuroimaging Initiative. A set-based mixed effect model for gene-environment interaction and its application to neuroimaging phenotypes. Front Neurosci. 2017;11:191. https://doi.org/10.3389/fnins.2017.00191.
Wei Q, Li M, Kang Z, Li L, Diao F, Zhang R, et al. ZNF804A rs1344706 is associated with cortical thickness, surface area, and cortical volume of the Unmedicated first episode schizophrenia and healthy controls. Am J Med Genet B Neuropsychiatr Genet. 2015;168B(4):265–73. https://doi.org/10.1002/ajmg.b.32308.
Weirauch MT. Gene coexpression networks for the analysis of DNA microarray data. Applied statistics for network biology: methods in systems biology; 2011.
Witte AV, Flöel A. Effects of COMT polymorphisms on brain function and behavior in health and disease. Brain Res Bull. 2012;88:418–28.
Wolf DH, Satterthwaite TD, Calkins ME, Ruparel K, Elliott MA, Hopson RD, et al. Functional neuroimaging abnormalities in psychosis spectrum youth. JAMA Psychiat. 2015;72:456–65. https://doi.org/10.1001/jamapsychiatry.2014.3169.
Wood JD, Bonath F, Kumar S, Ross CA, Cunliffe VT. Disrupted-in-schizophrenia 1 and neuregulin 1 are required for the specification of oligodendrocytes and neurones in the zebrafish brain. Hum Mol Genet. 2009;18:391–404.
Wray NR, Gottesman II. Using summary data from the danish national registers to estimate heritabilities for schizophrenia, bipolar disorder, and major depressive disorder. Front Genet. 2012;3:118. https://doi.org/10.3389/fgene.2012.00118.
Yang H, Liu J, Sui J, Pearlson G, Calhoun VD. A hybrid machine learning method for fusing fMRI and genetic data: combining both improves classification of schizophrenia. Front Hum Neurosci. 2010;4:192.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Jacobs, G.R., Voineskos, A.N. (2020). Genetics and Neuroimaging in Schizophrenia. In: Kubicki, M., Shenton, M. (eds) Neuroimaging in Schizophrenia . Springer, Cham. https://doi.org/10.1007/978-3-030-35206-6_16
Download citation
DOI: https://doi.org/10.1007/978-3-030-35206-6_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-35205-9
Online ISBN: 978-3-030-35206-6
eBook Packages: MedicineMedicine (R0)