
Abstract
Head and neck procedures are often performed in the acute care settings. Historically, anatomical landmarks have guided physicians as they determine accurate location and approach when performing these procedures. Due to anatomical variations, landmark-guided techniques lead to considerable variability in both success and complication rates. In recent years, ultrasound is increasingly being used at the bedside by clinicians. Ultrasound can be extremely useful in identifying relevant anatomy and thus facilitating various head and neck procedures in the acute care settings. Furthermore, because the regions of the face and neck are relatively shallow, high-frequency and high-resolution ultrasound probes can be used to provide significant detail of the anatomy in question. The use of ultrasound guidance for procedures has been demonstrated to decrease complications and improve patient safety and satisfaction. A thorough understanding of the basic principles of ultrasound, sonographic anatomy, and manual dexterity skills is essential in the use of ultrasound for procedural guidance.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Head and neck procedures are routinely performed by healthcare providers in acute care settings. Traditionally, anatomical landmarks are used to determine accurate location and approach when performing these procedures. However, the success and complication rates for landmark-based techniques are quite variable due to anatomical variations. The evaluation of superficial regions of the face and neck is shallow, and as a result, imaging with high-frequency ultrasound probes can provide high-resolution images ideal for the diagnostic workup and procedural guidance. High-resolution ultrasound for evaluation of head and neck soft tissue swelling is far superior to the physical examination and provides a very high sensitivity (96%) and specificity (82%), and cysts as small as 2–3 mm can be identified [1]. More importantly, the use of ultrasound guidance has been demonstrated to improve success rates, minimize inadvertent injury to surrounding tissue, and improve patient experiences.
Advantages of Ultrasound Guidance
The benefit of ultrasound guidance is perhaps most realized when evaluating for and performing needle aspiration of tonsillar and peritonsillar infections. A recent RCT compared anatomical landmark techniques to ultrasound imaging for the diagnosis and drainage of PTAs and found that ultrasound was superior in the following ways: diagnostic accuracy, ultrasound 100% vs. landmark 75%; successful drainage, ultrasound 100% vs. landmark 50%; and consultation of otolaryngology, ultrasound 7% vs. landmark 50% [2]. In small lesions (10–15 mm), landmark guidance in fine needle aspiration leads to 3 times as many failed samples [3]. Ultrasound guidance not only allows the physician to evaluate the relevant anatomy but also allows real-time visualization of the needle as the procedure is performed. A thorough understanding of the basic principles of ultrasound, sonographic anatomy, and manual dexterity skills is essential in the use of ultrasound for procedural guidance.
Head and Neck Cutaneous Abscess Drainage
Anatomy
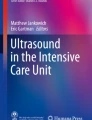
Anatomy of the head and neck includes an extensive supply of nerves and vasculature. When evaluating for an abscess, a keen eye should be used to evaluate for vital anatomical structures before the start of the procedure. For example, in the lateral anterior region of the neck, the carotid artery and internal jugular vein are located below the sternocleidomastoid and should be identified so as not to cause vascular injury during incision and drainage or needle aspiration (Fig. 7.1). Due to the extensive network of neurovascular branches, needle aspiration is the favored technique for a majority of abscesses of the head and neck.

Anatomy of the lateral neck (TC thyroid cartilage, CB carotid bifurcation, CB–Go carotid bifurcation–gonion, CB–ITC carotid bifurcation–isthmus of thyroid cartilage, CCA common carotid artery, ECA external carotid artery, ICA internal carotid artery, STA superior thyroid artery, LA lingual artery). (Reproduced from Topography of carotid bifurcation: considerations for neck examination. Surg Radiol Anat. 2008;30:383–387-p. 384)
Clinicians must also be familiar with sonographic evaluation of the airway. Air-tissue interface can help the operator identify relevant anatomy. In the mouth, air-tissue interface can be identified as a hyperechoic line which follows the curvature of the tongue (Fig. 7.2a) and as a hyperechoic line between the gum line/teeth and the cheek (Fig. 7.2b). In the neck, the interface is used to identify the trachea (Fig. 7.2c).

Mucosa and air interface. (a) Transcervical imaging of the oropharynx demonstrates the tongue and soft palate interface (asterisks). (b) Soft tissue imaging of the face demonstrates the cheek and gingiva interface (asterisks). (c) Airway imaging. The trachea is identified as a result of the mucosa-air interface in a supine patient. In all three images, the hyperechoic line between surfaces is accentuated by trapped air
Physical examination findings of head and neck swelling are not reliable, whereas sonographic evaluation purports a sensitivity >90% and specificity >80% [1]. Clinicians performing cutaneous procedures of the head and neck should use ultrasound to increase success rates and minimize complications.
Indications
The vast majority of etiologies behind swelling and/or discomfort of the head or neck include cellulitis, abscess, cyst, lymphadenopathy, or salivary gland swelling (Fig. 7.3). Patients who are found to have edema or swelling should undergo sonographic evaluation for anechoic fluid collections. As mentioned these patients should generally undergo aspiration or incision and drainage.

(a) Soft tissue swelling of the face with cobblestone appearance consistent with cellulitis. (b) Anechoic fluid collection from periapical dental abscess (asterisk). (c) Lymphadenitis (L) with echogenic hilum (x). (d) Salivary gland inflammation
Contraindications
Head and neck infections (dental infections, facial infections, peritonsillar abscess, etc.) can create direct or indirect airway compression. As a result, the patient’s airway should be assessed prior to starting the procedure. Patients in whom airway obstruction or airway compromise is deemed a risk factor should not undergo bedside drainage, and surgical consultation should be considered.
Equipment/Probe Selection
As with evaluation of most superficial structures, the high-frequency (15–6 MHz) linear array probe should be used. Color Doppler can help evaluate for hyperemia and aid in the identification of surrounding neurovascular structures. Lidocaine with or without epinephrine should be readily available. Chlorhexidine, a sterile probe cover, and #11 blade scalpel or 18 or 20 gauge needle attached to a 10 mL syringe should also be available (Fig. 7.4).

Linear array transducer and other equipment for incision and drainage
Preparation/Preprocedural Evaluation
For cutaneous procedures of the head and neck, the gurney should be at a height comfortable for the physician. The patient’s head should be comfortably turned to the contralateral side, and the neck should be extended to maximize access to the affected area. Topical anesthetic, such as lidocaine-epinephrine-tetracaine gel, can be used over the affected area to minimize discomfort. In certain scenarios, clinicians may choose to provide anxiolysis with benzodiazepines or systemic pain control with a short-acting narcotic. Prior to the procedure, depth of the abscess cavity from the surface of the skin, size of the abscess, and surrounding structures should be evaluated using ultrasound. Color Doppler should be used to identify adjacent vessels which should be avoided during the procedure.
Procedure
The linear array transducer should be used to scan the area in question in both the sagittal and transverse planes; whenever possible, the patient’s contralateral side should be imaged for comparison. An anechoic fluid collection with echoic contents often with posterior acoustic enhancement is concerning for abscess. This should be distinguished from cellulitis, which can have a cobblestone appearance without fluid collections (Figs. 7.5 and 7.6). The physician should gently compress the affected area for squish sign, and color Doppler flow can be used to confirm the lack of vascularity within the cavity (Fig. 7.7). If a fluid collection is located, the boundaries, depth from the skin surface, and estimated size of the cavity should be noted. The relevant adjacent anatomy should be evaluated; and the physician should be mindful of the underlying structures in the neck which include the thyroid, parathyroid, trachea, and vasculature. When draining an abscess of the face, care must be taken to avoid the facial nerve and branches of the trigeminal nerve. When draining abscesses of the neck, care must be taken not to injure the underlying neurovascular structures, and special care must also be taken to remain superficial to the platysma.

(a) Soft tissue swelling with presence of cobblestone appearance consistent with cellulitis. (b) Soft tissue swelling with anechoic fluid collection (asterisk) suggesting abscess

B-mode image of anechoic facial abscess with posterior acoustic enhancement

On color Doppler, no flow noted within the abscess cavity; however, hyperemia is seen surrounding the abscess cavity
Once the abscess and relevant anatomy have been visualized and imaged in at least two planes, the affected area can be anesthetized. The cutaneous area should be cleansed with chlorhexidine. The probe should be covered with a tegaderm, and gel should be placed on top of the probe. Using an 18 or 20 gauge needle attached to a 10 mL syringe, advance the needle tip under ultrasound guidance using an in-plane approach (Fig. 7.8). If necessary, make a small incision using a #11 blade scalpel, and use blunt dissection to break up loculated fluid collections (Fig. 7.9a, b). Extensive abscesses may require irrigation with normal saline to aid in breakdown of loculations. Ultrasound should be used after drainage is complete to verify complete evacuation of the abscess cavity (Fig. 7.10).

Needle aspiration using in-plane approach

Ultrasound-guided incision and drainage. (a) Probe positioning for incision. (b) Probe positioning for drainage

(a) Anechoic abscess cavity (arrows) prior to incision and drainage. (b) Post incision and drainage image confirming abscess evacuation, collapsed abscess cavity (arrows)
Complications
Injury to the surrounding neurovascular structures is a complication associated with head and neck cutaneous procedures. Additionally, lymph nodes may be difficult to distinguish from an abscess. Color Doppler can aid in the identification of vascular structures and lymph nodes. In addition, ultrasound should be used to verify complete evacuation of the abscess cavity. A partially drained abscess may result in the need for further intervention in the future.
Pearls/Pitfalls
-
1.
Injury to surrounding neurovascular structures can be avoided by utilizing color Doppler during the initial evaluation and performing the procedure under ultrasound guidance.
-
2.
Purulent material in the abscess cavity may appear isoechoic. For this reason, any findings should be compared to the contralateral side, color Doppler can be used to demonstrate hyperemic glands or nodes, and compression can help demonstrate abscess content motion.
-
3.
The use of 18 gauge needles is preferred as purulent material may be difficult to aspirate through smaller caliber needles.
-
4.
If purulent material is too viscous to aspirate, a #11 blade scalpel can be used to create a small puncture sufficient to allow for drainage.
-
5.
Use gray-scale imaging and color Doppler imaging to evaluate for necrotic lymph nodes and glands.
-
6.
In-plane approach is recommended while performing needle aspiration.
Integration into Clinical Practice
Physical examination of cutaneous swelling of the head and neck has poor diagnostic utility, whereas ultrasound has a sensitivity >90%. Ultrasound-guided incision and drainage of head and neck abscesses can provide definitive treatment. Furthermore, ultrasound-guided drainage can help prevent the occurrence of common complications, including injury to the surrounding neurovascular structures.
Evidence
High-resolution ultrasound provides a very high sensitivity (96%) and specificity (82%) for identification of purulent collections in evaluation of head and neck swelling [1]. Ultrasound-guided fine needle aspiration has a sensitivity of 89–98% and specificity of 95–98% in the differentiation of neck masses [4]. Yusa et al. described the utility of ultrasound guidance for draining deep face and neck abscesses. In addition, ultrasound guidance has been shown to be helpful in the drainage of submasseteric space abscess and needle aspiration of lateral masticator space [5, 6].
Key Points
-
Ultrasound-guided aspiration of cutaneous swelling of the head and neck will increase success rates, decrease complications, and as a result improve patient care and experience.
-
Hand dexterity and sonographic needle guidance skills are required and can easily be cultivated with practice.
Peritonsillar Abscess Drainage
Anatomy
The throat is divided into three parts: the nasopharynx, oropharynx, and hypopharynx. The nasopharynx includes the nasal cavity and soft palate, the oropharynx includes the posterior mouth down to the superior edge of the epiglottis, and the hypopharynx includes the epiglottis to the cricoid cartilage (Fig. 7.11). Found in the oropharynx, the palatine tonsils are defined anteriorly by the tonsillar pillar and the glosopalatine muscles and posteriorly by the tonsillar pillar and the pharyngopalatine muscle. The palatine tonsil itself is located between the palatoglossal and palatopharyngeal arch. Each tonsil has a number of ingrowths known as tonsillar crypts. During an infection, the peritonsillar space evolves into peritonsillar cellulitis. Peritonsillar abscesses form when the surrounding infection spreads into the tonsillar capsule. In addition to the evaluation of palatine tonsils, clinicians should be familiar with sonographic anatomy of the tongue, soft palate, and carotid artery.

Anatomy of the pharynx and tonsillar tissue
Indications
Patients will often present with any or all of the following: trismus, odynophagia, “hot potato” voice, edema and erythema of the surrounding peritonsillar tissue, cervical lymphadenopathy, limitation of neck movements, torticollis, tonsillitis, tonsillar displacement, and uvula deviation away from the affected side [7, 8]. Intraoral ultrasound can help identify PTA versus peritonsillar cellulitis (PTC) (Fig. 7.12).

Ultrasound imaging of the peritonsillar space is essential to differential tonsillar swelling with abscess. (a) B-mode showing peritonsillar abscess (asterisk). (b) Tonsillar swelling consistent with peritonsillar cellulitis
Contraindications
If there is concern for possible airway obstruction or patient noncompliance during the procedure, an alternative method of drainage, such as intraoperative drainage under general anesthesia, should be considered.
Equipment/Probe Selection
Although the intraoral approach is the most widely utilized technique for ultrasound-guided PTA drainage, the transcervical approach is a great option for patient with significant trismus which can limit placement of the endocavitary transducer into the oropharynx. When conducting the transoral approach, the high-frequency (12–2.5 MHz) curved array endocavitary probe (Figs. 7.13 and 7.14a) is required for optimal oropharynx imaging. When the transcervical approach is conducted, the low-frequency (5–2 MHz) curved array transducer or a (10–5 MHz) linear transducer is used (Fig. 7.15a).

High-frequency endocavitary probe for intraoral approach

Intraoral approach for PTA aspiration. (a) Endocavitary probe and the needle are inserted into the mouth. (b) Identification of a PTA with anechoic fluid collection (asterisk). (c) Measure the size and depth of the abscess cavity. (d) PTA drainage with direct needle visualization (arrows)

Transcervical approach for PTA aspiration. (a) Curved array transducer provides imaging in the submandibular region while the needle is inserted into the mouth. (b) Identification of a PTA with isoechoic fluid collection (asterisk) (T-Tonsil, SP-Soft palate). (c) Measure the size and depth of the abscess cavity. (d) PTA drainage with direct needle visualization (arrows)
Preparation/Preprocedural Evaluation
An airway assessment should be performed prior to starting the procedure, and necessary airway equipment should be readily available at the bedside. The patient should be seated upright, with the bed at a height comfortable for the physician performing the procedure. A topical anesthetic spray should be applied to the affected peritonsillar tissue. Five percent lidocaine ointment or 2% lidocaine jelly can be placed on a tongue depressor and given to the patient in the form of a “popsicle” as a useful anesthetic adjunct. Nebulized 4% lidocaine can provide additional analgesia, and systemic analgesia may be necessary. A 2 in. 18 gauge needle or an 18 gauge spinal needle with the plastic sheath attached to a 10 mL or 20 mL syringe should be available at the bedside. One percent lidocaine without epinephrine should be available in the event the patient requires further analgesia prior to starting the procedure.
PTA should be distinguished from PTC, with PTA appearing as an enlarged tonsil with heterogeneous or cystic appearance and PTC appearing as an enlarged tonsil with a homogenous or striated appearance (Fig. 7.12) [9]. A cobblestone appearance typical of cellulitis may be noted in advanced PTC. Measure the depth of the abscess cavity from the mucosal surface, as this will determine the length of needle required. Measure the length and width of the abscess cavity to determine the overall size of the abscess, and estimate the expected amount of fluid to be drained (Figs. 7.8c and 7.9c). Finally, in short or transverse axis, determine the relationship of the abscess cavity to the carotid artery. The carotid artery will appear as a small, pulsatile, tubular structure, generally 0.5–2.5 cm posterior to the abscess cavity, and use of a color Doppler can help in its identification (Fig. 7.16). Place a small amount of gel over the transducer, and cover the probe with a sheath or condom. Insert the probe into the pharyngeal region, and scan in both the long and short axis.

(a) Intraoral ultrasound image of a left PTA fluid collection. The letter (x) marks the carotid artery. (b) Transcervical ultrasound image of a left PTA fluid collection. The letter (x) marks the carotid artery
Procedure
Intraoral Approach
When performing the intraoral approach to PTA drainage, the endocavitary transducer can be inserted from either the ipsilateral side in line with the mandible or from the contralateral side (Fig. 7.14a). Advance the transducer and image the oropharynx and identify the PTA (Fig. 7.14b). Measure the abscess size and total distance from the carotid artery (Fig. 7.14c). Insert the needle at the middle (in order to align it with the emanating ultrasound beam) of the probe tip, and slowly advance the needle only after the needle tip is visualized on ultrasound. If the needle tip is not identified, the needle should not be advanced further (Figs. 7.14d and 7.17).

(a) Needle tip (arrow) visualized during real-time ultrasound-guided drainage. (b) Needle shaft and tip (arrows) are seen prior to pentretating abscess cavity. (c) Echogenic needle tip (arrow) in the abscess cavity
Transcervical Approach
When performing the transcervical approach to PTA drainage, the curved array transducer can be used transcutaneously on the ipsilateral side in the submandibular space (Fig. 7.15a). As with the intraoral approach, the operator must first evaluate relevant anatomy and identify the PTA (Fig. 7.15b). Be sure to measure the abscess size and total distance from the carotid artery (Fig. 7.15c). Insert the needle in line with the mandible or from the contralateral side, and slowly advance the needle only after the needle tip is visualized on ultrasound. If the needle tip is not identified, the needle should not be advanced further (Fig. 7.15d).
Whether one chooses to perform the intraoral or the transcervical approach, evaluation for the carotid artery using color Doppler is necessary to avoid inadvertent injury. With either approach, a 2 in. 18 gauge needle should be attached to a 10 mL or 20 mL syringe for aspiration. Alternatively, the plastic sheath on an 18 gauge spinal needle can be trimmed to the premeasured depth to prevent injury to the carotid artery. A loculated abscess cavity may require injection with saline to aid in breakdown of loculations and allow for successful needle aspiration. Complete evacuation of the abscess cavity should be confirmed on ultrasound (Fig. 7.18).

Peritonsillar abscess. (a) Prior to drainage, anechoic abscess visualized. (b) Post drainage-collapsed abscess cavity is seen
Complications
Patient cooperation is key for this procedure to be successful; systemic analgesia and topical analgesia used in combination will help maximize patient cooperation. Using ultrasound to distinguish PTA from PTC prior to the procedure will minimize failures. Inadvertent injury to the carotid artery is a theoretical risk associated with PTA needle aspiration and can be minimized by measuring the distance from the abscess cavity to the vessel.
Pearls/Pitfalls
-
1.
Ultrasound evaluation can help minimize the potential for a dry tap and distinguish between PTA and PTC. Heterogeneous/isoechoic abscesses (those with thick purulent material) can also be mistaken for cellulitis. Compression of the peritonsillar space can create movement within the purulent fluid.
-
2.
The hand-eye coordination and dexterity required for this procedure require practice.
-
3.
Determining the distance of the abscess cavity from the carotid artery can help avoid carotid puncture. Color Doppler can help with visualizing the carotid artery.
-
4.
Measuring the abscess cavity can provide a rough estimate of how much fluid is contained in the abscess cavity.
-
5.
Measure the depth of the abscess cavity so you can choose the appropriate length of needle.
-
6.
Aspiration under real-time ultrasound guidance requires skill and practice. If you lose your needle tip on ultrasound, it is best not to advance any further to avoid inadvertent carotid puncture.
-
7.
A loculated abscess may require saline injection to facilitate adequate drainage.
-
8.
PTA drainage requires a cooperative patient and confident physician. Adequate pain management and light sedation are pivotal to success.
-
9.
Encountering an unusually deep PTA may actually represent a retropharyngeal abscess (RTA). RTA can be drained using the same technique if visualization is adequate. Needle length required can increase up to 4 or 5 inches for RTA drainage.
Integration into Clinical Practice
This procedure should take approximately 20 minutes from start to finish. Routine use of intraoral ultrasound for evaluation of peritonsillar swelling can provide an accurate diagnosis with minimal side effects. If PTA is the underlying etiology, intraoral ultrasound can provide real-time evaluation of the relevant anatomy, thereby minimizing risk of harm in this bedside procedure. Patients found to have no abscess on a prescan or having a dry tap of an “at-risk area” can be brought back in 1 or 2 days for a rescan. Some will be noted to have developed a clear abscess in that time, and an aspiration can be performed at that time.
Evidence
Prior studies have demonstrated the superiority of ultrasound-guided needle aspiration over the traditional landmark approach [2, 7, 10]. A recent RCT compared anatomical landmark techniques to ultrasound imaging for the diagnosis and drainage of PTAs and found that ultrasound was superior in the following ways: diagnostic accuracy, ultrasound 100% vs. landmark 75%; successful drainage, ultrasound 100% vs. landmark 50%; and consultation of otolaryngology, ultrasound 7% vs. landmark 50% [2]. Literature for transcervical evaluation of PTA is limited; however, a recent study noted the sensitivity to be 80% and the specificity to be 93% [11].
Key Points
-
Ultrasound-guided PTA needle aspiration requires practice, but real-time use of intraoral ultrasound can aid in visualization of relevant anatomy and minimize potential complications.
-
Needle guidance for PTA drainage increases procedural success and minimizes consultation of otolaryngology colleagues.
-
Transoral approach is diagnostically more accurate than the transcervical approach; however, transcervical approach can be useful for needle guidance in patients with severe trismus.
Suppurative Lymph Node Aspiration
When conducting procedures of the head and neck, it is imperative that clinicians understand the variable appearance of lymph nodes. Lymph nodes tend to be oval and smooth bordered and have an echogenic central hilum (Fig. 7.19). During infections, they may become reactive and will demonstrate increased blood flow in color Doppler mode (Fig. 7.20a, b). When lymph nodes succumb to infections, necrosis can occur. Intranodal necrosis may appear as a cystic area (cystic necrosis) within the lymph node or as a hyperechoic area within the lymph node (coagulation necrosis), but both are pathologic (Figs. 7.20c, 7.21 and 7.22). Lymph nodes round in shape with peripheral flow are considered abnormal (Figs. 7.23 and 7.24). Finally, a suppurative lymphadenitis will present with ultrasound findings similar to an abscess (Fig. 7.20d) [12]. A clinician may need to perform a needle aspiration or needle biopsy of this structure. Topical anesthetic, such as lidocaine-epinephrine-tetracaine gel, can be used over the affected area to minimize discomfort. Chlorhexidine, a tegaderm, and a 21 or 22 gauge needle are attached to a 10 mL syringe. Ultrasound guidance should direct the needle for biopsy or aspiration, and the clinician should advance the needle into the region of interest using in-plane approach. Ultrasound-guided fine needle aspiration has a sensitivity of 89–98% and specificity of 95–98% for successful FNA. The use of ultrasound in FNA has reduced negative FNA rates from 15% to <2% [4].

Normal oval lymph node echogenic central hilum

Lymph node evaluation. (a) Normal lymph node with echogenic central hilum (x). (b) Enlarged reactive lymph node with color Doppler imaging demonstrating increased hilar flow (h-hilum). (c) Round lymph node with anechoic center (asterisk) similar in appearance to a cyst. (d) Necrotic and suppurative lymph node (s) with surrounding fluid collection

Intranodal coagulation necrosis with echogenic debris

Abnormal shape with intranodal cystic necrosis and loss of echogenic hilum

Abnormal shape (round) and loss of normal echotexture

Peripheral flow noted in this necrotic lymph node
References
Mallorie CN, Jones SD, Drage NA, Shepherd J. The reliability of high resolution ultrasound in the identification of pus collections in head and neck swellings. Int J Oral Maxillofac Surg. 2012;41(2):252–5.
Costantino TG, Satz WA, Dehnkamp W, Goett H. Randomized trial comparing intraoral ultrasound to landmark-based needle aspiration in patients with suspected peritonsillar abscess. Acad Emerg Med. 2012;19(6):626–31.
Cesur M, Corapcioglu D, Bulut S, et al. Comparison of palpation-guided fine-needle aspiration biopsy to ultrasound-guided fine-needle aspiration biopsy in the evaluation of thyroid nodules. Thyroid. 2006;16(6):555–61.
Ying M, Bhatia KS, Lee YP, Yuen HY, Ahuja AT. Review of ultrasonography of malignant neck nodes: greyscale, Doppler, contrast enhancement and elastography. Cancer Imaging. 2013;13(4):658–69.
Sivarajasingam V, Sharma V, Crean SJ, Shepherd JP. Ultrasound-guided needle aspiration of lateral masticator space abscess. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88(5):616–9.
Yusa H, Yoshida H, Ueno E, Onizawa K, Yanagawa T. Ultrasound-guided surgical drainage of face and neck abscesses. Int J Oral Maxillofac Surg. 2002;31(3):327–9.
Lyon M, Blaivas M. Intraoral ultrasound in the diagnosis and treatment of suspected peritonsillar abscess in the emergency department. Acad Emerg Med. 2005;12(1):85–8.
Grisaru-Soen G, Komisar O, Aizenstein O, Soudack M, Schwartz D, Paret G. Retropharyngeal and parapharyngeal abscess in children--epidemiology, clinical features and treatment. Int J Pediatr Otorhinolaryngol. 2010;74(9):1016–20.
Buckley AR, Moss EH, Blokmanis A. Diagnosis of peritonsillar abscess: value of intraoral sonography. AJR Am J Roentgenol. 1994;162(4):961–4.
Blaivas M, Theodoro D, Duggal S. Ultrasound-guided drainage of peritonsillar abscess by the emergency physician. Am J Emerg Med. 2003;21(2):155–8.
Araujo Filho BC, Sakae FA, Sennes LU, Imamura R, de Menezes MR. Intraoral and transcutaneous cervical ultrasound in the differential diagnosis of peritonsillar cellulitis and abscesses. Braz J Otorhinolaryngol. 2006;72(3):377–81.
Reshma VJ, Shihab Anwar A, Abdulla Mufeed V, Johnson K. Characterization of cervicofacial lymphnodes – a clinical and ultrasonographic study. J Clin Diagn Res. 2014;8(8):ZC25–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Amini, R., Javedani, P. (2020). Ultrasound-Guided Ear, Nose, and Throat Procedures. In: Adhikari, S., Blaivas, M. (eds) The Ultimate Guide to Point-of-Care Ultrasound-Guided Procedures . Springer, Cham. https://doi.org/10.1007/978-3-030-28267-7_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-28267-7_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-28265-3
Online ISBN: 978-3-030-28267-7
eBook Packages: MedicineMedicine (R0)