
Abstract
Intracranial vessel wall imaging is a rapidly evolving method for identifying and characterizing neurovascular disease and is complementary to conventional angiographic imaging techniques such as catheter angiography, CT angiography, and MR angiography. It can diagnose etiologies underlying intracranial stenosis, identify culprit plaques in the setting of ischemic stroke, and characterize ruptured aneurysm in the setting of subarachnoid hemorrhage or unstable/at-risk aneurysms. In this chapter, we review the current literature and potential future directions.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Three-dimensional vessel wall MRI
- Atherosclerotic disease
- Plaque
- Intracranial vessels
- Black blood MRI
- Vasculitis
Introduction
Conventional angiographic techniques such as CT angiography, MR angiography, and digital subtraction angiography demonstrate luminal stenosis but are unable to characterize the underlying disease within the vessel wall. Depiction of the vessel wall abnormality improves the ability to distinguish vasculopathies with similar angiographic findings and can offer insight into risk and management of the underlying disease. Vessel wall visualization requires suppression of blood flow most commonly using black blood MRI (BBMRI) sequences [1]. Historically, two-dimensional (2-D) T1 or proton density black blood sequences were developed to characterize the vessel wall of carotid arteries driven partly by access to endarterectomy specimens for comparison with imaging [2, 3]. However, application of 2-D sequences for imaging intracranial vessels is challenging given the smaller size and tortuosity of these vessels. 2-D techniques have a non-isotropic resolution that results in overestimation of vessel wall thickness due to the small size of vessels compared to even the most optimized 2-D voxel size [4]. In addition, achieving contiguous 2-D slices orthogonal to the course of intracranial vessels can be very challenging due to the tortuosity of these vessels [5]. Isotropic 3-D vessel wall MRI (VWMRI) overcomes this challenge and enables characterization of the intracranial vessel wall with reduced partial volume averaging [6]. A detailed explanation of the 3-D high isotropic resolution black blood MRI technique and protocols has been previously reported [1, 7].
In this chapter, we review the role of vessel wall MRI for evaluation of vasculopathies including atherosclerotic disease, vasculitis, reversible cerebral vasoconstriction syndrome (RCVS), dissection, and aneurysms. In addition, we review 4D flow MRI, 4D-CTA, and transcranial Doppler ultrasound.
Intracranial Vasa Vasorum
Vasa vasorum consist of networks of arteries, capillaries, and veins supplying oxygen and nutrients to the walls of larger blood vessels. Intracranial vessels are unique in the paucity of vasa vasorum found in their adventitia under normal conditions, thought to be a consequence of the surrounding cerebrospinal fluid environment [8]. Vasa vasorum may develop within intracranial arteries with age, predominantly at the proximal portions [9], and as a consequence of vascular diseases such as atherosclerosis, vasculitis, and aneurysms [8, 10]. Its development has been implicated in promoting inflammatory processes, which can progress to the inner layers [11] leading to the initiation and acceleration of intracranial atherosclerosis [8]. For example, there is a strong association between presence of vasa vasorum and atherosclerotic plaque particularly in thicker intracranial vessels [10]. The relative paucity of intracranial vasa vasorum offers an explanation for the lower frequency of intracranial atherosclerosis compared to coronary and carotid atherosclerosis and higher correlation of extracranial carotid and coronary atherosclerosis compared to intracranial and coronary atherosclerosis [12].
Given the unique features of intracranial vasa vasorum and its implication in intracranial vasculopathies, imaging detection of intracranial vasa vasorum may have an important role in disease diagnosis and prognostication. Intracranial vasa vasorum can be detected by contrast-enhanced MR and CT techniques and is evident by vessel wall enhancement [8, 13].
Intracranial Atherosclerotic Disease
Intracranial atherosclerotic disease (ICAD) is very prevalent and a major cause of ischemic stroke [14]. The estimated prevalence of symptomatic intracranial stenosis varies from 1 in 100,000 for whites to 15 in 100,000 in African Americans in population-based studies [15]. Autopsy studies have noted intracranial atherosclerotic disease to be present in as many as 23% and 80% of people in their 6th and 9th decades of life, respectively [15]. Traditional methods of diagnosing atherosclerosis have been based on measures of luminal narrowing which underestimates plaque burden because of compensatory dilatation (remodeling) to accommodate plaque formation especially early on [6]. In coronary arteries, outward (positive) remodeling can preserve the lumen at a plaque burden as high as 40% of the arterial lumen circumscribed by the internal elastic lamina based on plaque specimen analyses [16]. Negative or inward remodeling results in luminal narrowing and may alter hemodynamics. Although outward remodeling limits the hemodynamic impact of the plaque, it may be associated with increased plaque vulnerability and clinical events as shown in coronary arteries [17, 18].
Imaging Intracranial Atherosclerotic Plaque
Vessel wall magnetic resonance imaging is an effective method for measurement of wall thickness and characterization of pathologic features of the carotid arteries [3] and intracranial vessels [1, 19]. 3D high isotropic resolution black blood MR imaging has made it possible to identify and characterize intracranial atherosclerotic disease [1, 20] and discriminating it from other vasculopathies [7, 21].
A US community-based population study (the Atherosclerosis Risk in Communities (ARIC) study) estimated the prevalence of having at least one intracranial atherosclerotic plaque to be 34.4% using VWMRI [22] which is higher than previous estimates of intracranial stenosis in population-based studies [15]. In the ARIC study, 10.8% of participants had ICAD with no detectable stenosis [22] which helped to explain the difference in prevalence estimates. Cross-sectional reliability estimates of VWMRI measurements of intracranial atherosclerotic plaque based on 102 repeat scans and 20 inter-reader and 29 intra-reader repeat readings have been shown to range from good to excellent for quantitative measurements (e.g., intracranial vessel lumen, wall thickness) and fair to good for qualitative measurements (plaque presence, ordinal stenosis) [20]. The high reliability is likely a reflection of the reproducibility of 3D imaging and the effect of adequate training for image interpretation, which was heavily emphasized in this study [20].
MR Features of Atherosclerotic Plaque and Identifying Culprit Plaque
Imaging features of atherosclerotic plaque on VWMRI are more challenging to detect in intracranial vessels compared to extracranial vessels due to the smaller size of intracranial vessels. This can result in partial volume averaging of plaque components, including lipid core, fibrous cap, calcification, intraplaque hemorrhage, and enhancement, resulting in a heterogeneous signal [19, 23]. Intracranial atherosclerotic plaques are eccentric often with irregular wall thickening and variable degrees of enhancement (Fig. 3.1) [19, 21, 24]. Although individual plaque components may not be readily visible due to resolution constraints, heterogeneous signal and intraplaque hemorrhage may be helpful discriminators from other lesions [19, 23]. If detected, the fibrous cap may present as a T2 hyperintense and enhancing band overlying a T2 hypointense lipid core [21]. This T2 hyperintense band and heterogeneous signal are typically absent in cases of vasculitis and RCVS [21]. Intracranial atherosclerotic plaque enhancement can vary in degree and, consequently, is not useful for discriminating from other vasculopathies. However, a high degree of enhancement might be useful for identifying lesions that are responsible for downstream ischemic infarcts (culprit plaques) likely reflecting inflammation, endothelial permeability, and neovascularity associated with increased macrophage infiltration and neovascularity as seen in postmortem specimens [25,26,27,28,29]. Therefore, plaque enhancement may be used as a marker for plaque instability and stroke risk assessment. In addition, recanalized vessels following treatment for thromboembolic disease demonstrate concentric vessel wall thickening and enhancement which is more robust in patients who underwent both mechanical thrombectomy and medical therapy than medical therapy alone [30].

Features of an atherosclerotic plaque involving the cavernous carotid artery with an enhancing fibrous cap (short arrow), lipid core (dotted arrow), and peripheral calcification (long arrow)
VWMRI has been used to characterize vascular remodeling in extracranial carotid [31, 32] and intracranial arteries [6] and has enabled our ability to detect atherosclerosis with no luminal stenosis [33]. These non-stenotic lesions appear to be the strongest risk factor for white matter hyperintensities in patients without intracranial stenoses [34]. Luminal preservation in cervical internal carotid arteries has been shown to occur at plaque burdens up to 62% measured using MRI techniques [31, 32]. Intracranial arteries can also remodel to a high degree as a result of plaque formation with the posterior circulation having a higher capacity for positive remodeling than the anterior circulation [6]. Prevalence of positive remodeling in atherosclerotic plaques in stroke patients was shown to be 29.9% in the anterior circulation versus 54% in the posterior circulation, with lumen patency being maintained in the posterior circulation with plaque burdens up to approximately 55.3% [6]. This may be attributed to differences in hemodynamics (i.e., slower flow in the posterior circulation) and sparse sympathetic innervation of the vertebrobasilar system [6, 35, 36].
Another potential application of VWMRI is determining the location of atherosclerotic plaque relative to a branch artery. Although atherosclerotic plaques tend to arise from arterial wall opposite a branch artery ostium [5, 37, 38], some plaques arise close to the ostia and are associated with increased risk of infarction [38]. Angioplasty can push the atheromatous material from the treated artery to a branch resulting in acute stroke. Determining location of plaque relative to ostium may be useful in intracranial angioplasty risk assessment [39].
Vasculitis
Vasculitides are rare group of diseases defined by inflammation of the vessel wall [8]. Central nervous system vasculitis (CNSV) can be defined as any inflammatory vasculopathy that results in nonatheromatous intracranial vascular inflammation [40]. Primary CNSV is caused by direct involvement of vessels, while secondary vascular inflammation can result from infections, autoimmune processes, tumors, or other processes [40]. Although exact mechanism of involvement of vasa vasorum in vasculitis is not well established, higher prevalence of extracranial vasculitis suggests a role given higher density of vasa vasorum in extracranial arteries [8].
Conventional angiographic features of vasculitis are nonspecific and include multifocal luminal irregularity and stenosis that may overlap with a variety of intracranial vasculopathies such as atherosclerosis and RCVS. Intracranial VWMRI may help in distinguishing vasculitis from other etiologies of intracranial stenosis. Furthermore, some of small vessel vasculitides cannot be identified on catheter angiography [40]. Luminal narrowing is only detected on cerebral angiography in 25–43% of patients with biopsy-proven primary CNS angiitis [41, 42]. On VWMRI, intracranial vasculitis tends to present with segmental, concentric homogenous enhancement of the vessel wall and/or circumferential, peri-adventitial enhancement following a vessel segment (Fig. 3.2) [40]. Imaging features that are more suggestive of atherosclerosis such as calcification, fibrous cap and lipid core, or focal, non-circumferential wall thickening may help to exclude vasculitis [40]. Vasculitic lesions typically lack T2 hyperintensity, while ICAD lesions often demonstrate T2 hyperintensity or heterogeneous T2 signal [21]. It is important to note that there is overlap between ICAD and vasculitis as ICAD can demonstrate circumferential wall thickening and vasculitis can have eccentric enhancement [23, 43, 44]. Given the similarity and overlap of imaging findings and clinical manifestations between CNS vasculitis and atherosclerosis and the toxicity of immunosuppressive therapy, a biopsy may be needed for definitive diagnosis [40]. Because of the high false negative rate of biopsies for CNSV due to patchy and segmental involvement of vessels by this disease, VWMRI may be useful for guiding biopsies, and this has yielded higher success rates compared to biopsies guided by conventional imaging [40]. VWMRI should be acquired close to the time of biopsy to ensure the target is actively inflamed since vessel wall inflammation may be transient [40].

VWMRI appearance of small vessel vasculitis in a patient with clinical and radiological diagnosis of small vessel vasculitis. Contrast-enhanced VWMRI demonstrates peri-adventitial enhancement of an inflamed segment of a vessel seen in long axis (arrow)
Pitfalls of VWMRI for vasculitis include inability to distinguish between transmural inflammation (e.g., primary CNSV) and perivascular inflammation (e.g., sarcoidosis) [40]. In addition, concentric wall thickening after thrombectomy may mimic vasculitis if patient’s history is not known [30].
Reversible Cerebral Vasoconstriction Syndrome
Vasospasm results from smooth muscle shortening and increased wall redundancy that can result in a fivefold increase in wall thickness corresponding to 60% luminal narrowing [45, 46]. Arterial wall thickening is a feature of vasospasm on vessel wall imaging [7]. RCVS is characterized by noninflammatory reversible multifocal cerebral vasoconstriction associated with recurrent thunderclap headaches that resolve spontaneously within 3 months [47, 48]. It is an underdiagnosed entity and may lead to complications such as posterior reversible encephalopathy, subarachnoid hemorrhage, and ischemic infarcts [48, 49]. Timely distinction of RCVS from its top differential consideration, vasculitis, is essential since treatment strategies are very different. In particular, the appropriate management of vasculitis by steroids carries a significant morbidity [42].
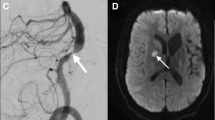
VWMRI can be helpful to distinguish RCVS from CNSV. Both vasoconstriction and vasculitis result in vessel wall thickening and luminal narrowing, but CNSV tends to demonstrate more intense wall enhancement and moderate wall thickening. In contrast, RCVS typically demonstrates little to no enhancement (Fig. 3.3), with only 31–47% of patients showing any enhancement with this disease [43, 44, 47]. However, the sensitivity of using a low degree of enhancement to diagnose RCVS is limited considering strong enhancement was seen in as many as a fourth of cases in one series [47]. The most reliable test for confirming this diagnosis remains follow-up imaging since wall enhancement in RCVS tends to resolve early, within 3 months [44].

VWMRI in a 5-year-old with RCVS. Time-of-flight MR angiography (a) demonstrates focal narrowing of duplicated left posterior cerebral artery. VWMRI shows cross-sectional appearance of normal segment of the vessel (b) compared to narrowed segment (c). No peri-adventitial or vessel wall enhancement in region of focal narrowing of the left posterior cerebral artery is seen (c)
Arterial Dissection
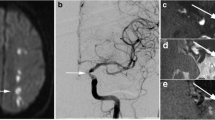
Arterial dissection results from an intimal tear with blood products tracking into the vessel wall. Vasa vasorum are implicated in the pathogenesis of intramural thrombus in arterial dissection [8]. Intracranial vessel wall dissection may result from extension of a dissection from extracranial arteries such as vertebral or carotid arteries or may be an isolated finding [7, 50]. VWMRI features of intracranial arterial dissection include intimal flap (curvilinear T2 hyperintensity) separating the true lumen from the false lumen and eccentric arterial wall thickening with T1 hyperintense intramural hematoma (Fig. 3.4) [7, 50]. A study of dissecting aneurysms demonstrated improved detection of dissections using VWMRI compared to catheter angiography (42% vs 16%, respectively) [50]. Intramural hematoma evolves over time. Deoxyhemoglobin in acute intramural hematoma is iso-intense on T1-weighted images and may be detected using T2∗ or susceptibility-weighted imaging before conversion to methemoglobin which is T1 hyperintense [51]. In a study of dissecting aneurysms, 83% of intramural hematomas were detected on T1-weighted images, and 59% could be seen on T2-weighted images [50]. However, T1 hyperintensity in the wall is not specific to arterial dissection and can also be seen with intraplaque hemorrhage in ICAD lesions [23], so other features such as vascular calcification or a trauma history can be helpful for diagnosis.

Chronic arterial dissection of the horizontal petrous segment of the carotid artery. Non-contrast (a) and contrast-enhanced (b) VWMR images through the short axis of the artery demonstrate enhancement of the vessel wall and flap separating the false lumen (arrow) from the true lumen
Aneurysms
There is ongoing debate regarding the pathophysiology that underlies aneurysm growth and rupture. Vasa vasorum are reported to be present in large (4 mm or larger) saccular aneurysms and fusiform aneurysms and have been implicated in growth and rupture of these lesions [8]. Repetitive intramural hemorrhage from vasa vasorum and reabsorption of blood is believed to induce inflammation and proliferation of microvessels that are prone to re-bleeding. This is postulated to result in enlargement and weakening/rupture of the aneurysm wall [52].
There is a growing body of evidence that supports the use of VWMRI for evaluating aneurysms [53, 54]. Contrast enhancement in the wall of unstable aneurysms has been reported and may be due to a loss of vasa vasorum integrity, intimal angiogenesis, and inflammatory activity [8, 55, 56]. Two recent histological studies of unruptured intracranial aneurysms revealed associations of aneurysm wall enhancement on VWMRI with higher macrophage infiltration, increased cellularity, neovascularization, and a thicker wall of the aneurysm [57, 58].
Retrospective studies have reported thick peripheral enhancement of ruptured aneurysms in the setting of subarachnoid hemorrhage, while unruptured aneurysms do not enhance [56, 59, 60]. It is noteworthy that in these retrospective studies, enhancement may represent inflammatory changes related to the rupture itself [23].
Aneurysm wall enhancement may also be a predictor of progression. In prospective studies of asymptomatic patients, enlarging or morphologically changing aneurysms demonstrate thick peripheral enhancement compared to little to no enhancement in stable asymptomatic aneurysms suggesting a potential role of VWMRI for treatment planning [60, 61]. Circumferential aneurysm wall enhancement >1 mm in thickness is shown to have the highest specificity and negative predictive value for differentiating between stable and unstable aneurysms [61]. In addition, a stronger degree of enhancement was associated with a higher clinical risk for rupture based on PHASES (population, hypertension, age, size, earlier subarachnoid hemorrhage, and size) score [62]. A meta-analysis of five retrospective and prospective studies with 492 subjects showed a significant and independent association of aneurysm wall enhancement with aneurysm rupture [63].
Potential use of VWMRI in detecting the source of hemorrhage in angiogram negative non-perimesencephalic subarachnoid hemorrhage has also been studied with no change in patient management [64]. Further investigation is warranted to understand the mechanism of aneurysm rupture and instability before contrast enhancement can be used as a marker for impending rupture.
4D Flow MRI
New applications of phase-contrast MRI have emerged to noninvasively evaluate blood flow qualitatively (flow visualization and direction) and quantitatively (velocity, pressure, wall shear stress) [65]. Hemodynamic parameters such as flow patterns, location of flow impact on aneurysm wall, size of impact zone, and wall shear stress (WSS) are of particular interest in assessing risk of aneurysm growth and rupture [66]. Low WSS and high oscillatory shear index are thought to initiate inflammatory cell-mediated remodeling in large aneurysms, while high WSS and positive WSS gradients can facilitate mural cell-mediated remodeling in small or secondary bleb aneurysms [66]. Both of these pathways may lead to aneurysm growth and rupture.
4D flow MRI has also been used to measure flow in arteriovenous malformations (AVM), specifically in arterial feeders along with arteries adjacent and contralateral to the AVM for a global hemodynamic evaluation for embolization planning [67, 68]. Velocity-derived flow-tracking cartography can help with functional assessment of the AVM with high reliability and good to excellent agreement with DSA for identification of shunt location and arterial feeders and evaluation of retrograde flow in dural venous sinuses or cortical veins [65]. Virtual MR flow-tracking cartography can classify dural arteriovenous fistulas (AVF) similar to catheter angiography (Cognard classification) providing risk stratification of bleeding based on assessment of venous drainage [69].
4D-CTA
In 4D CT angiography (4D-CTA), images are obtained throughout intravenous administration of contrast bolus using continuous or noncontinuous acquisition [70]. 4D-CTA is shown to be comparable to DSA in detecting and grading of cerebral AVMs [71, 72] and dural AVFs [73, 74]. In the work-up of acute ischemic stroke, 4D-CTA has been shown to be superior to conventional CTA for characterizing the extent and dynamics of collateral flow [75] and intracranial thrombus burden [76]. 4D-CTA has been comparable with DSA in discriminating antegrade flow from retrograde flow across an occluded vessel helping to predict rate of recanalization following intravenous thrombolysis which is correlated with antegrade flow [77]. Characterization of collateral flow also helps with prognostication of clinical outcome after ischemic stroke and rate of complications such as hemorrhagic transformation [70, 78].
Transcranial Doppler Sonography
Transcranial Doppler ultrasound (TCD) is a noninvasive ultrasound technique that can be used at the bedside to detect and localize intracranial arterial narrowing or occlusion. For detecting middle cerebral artery (MCA) occlusion, TCD has greater than a 90% sensitivity and its specificity approximates that of CTA [79]. TCD has lower sensitivity than CTA for detection of basilar or carotid terminus thrombus [79]. In addition to establishing patency, TCD can provide complementary information to CTA such as visualizing real-time embolization, presence of microemboli, and alternating flow signals indicative of steal phenomenon [79]. Furthermore, TCD can detect restenosis or re-occlusion after thrombolysis or thrombectomy [80]. Main drawbacks of its use are lack of adequate sonographic window through the temporal bone and limited availability of experienced technician or clinician [81].
Conclusions
In summary, the current literature supports an important role for intracranial vessel wall imaging in differentiating etiologies of intracranial vessel wall narrowing such as atherosclerosis, vasospasm, vasculitis, and arterial dissection. In addition, it can be useful for identification of non-stenotic lesions that would escape angiographic detection. Potential applications include risk stratification for atherosclerotic plaques and identifying actively inflamed lesions in vasculitis which could be useful for directing targeted biopsies of vessels. Future applications of VWMRI might also include risk stratification of aneurysms for rupture or growth. 4D flow technique is a useful adjunct for assessment of flow dynamics and rupture risk of aneurysms, AVMs, and dural arteriovenous fistulas and may be useful in treatment planning. Further investigations are warranted in larger samples for validation of clinical use of vessel wall MR and 4D MR/CT.
References
Qiao Y, Steinman DA, Qin Q, Etesami M, Schär M, Astor BC, et al. Intracranial arterial wall imaging using three-dimensional high isotropic resolution black blood MRI at 3.0 Tesla. J Magn Reson Imaging. 2011;34:22–30. https://doi.org/10.1002/jmri.22592.
Saba L, Yuan C, Hatsukami TS, Balu N, Qiao Y, DeMarco JK, et al. Carotid artery wall imaging: perspective and guidelines from the ASNR Vessel Wall Imaging Study Group and Expert Consensus Recommendations of the American Society of Neuroradiology. AJNR Am J Neuroradiol. 2018;39:E9–31. https://doi.org/10.3174/ajnr.A5488.
Wasserman BA, Smith WI, Trout HH, Cannon RO, Balaban RS, Arai AE. Carotid artery atherosclerosis: in vivo morphologic characterization with gadolinium-enhanced double-oblique MR imaging initial results. Radiology. 2002;223:566–73. https://doi.org/10.1148/radiol.2232010659.
Antiga L, Wasserman BA, Steinman DA. On the overestimation of early wall thickening at the carotid bulb by black blood MRI, with implications for coronary and vulnerable plaque imaging. Magn Reson Med. 2008;60:1020–8. https://doi.org/10.1002/mrm.21758.
Zhu XJ, Du B, Lou X, Hui FK, Ma L, Zheng BW, et al. Morphologic characteristics of atherosclerotic middle cerebral arteries on 3T high-resolution MRI. AJNR Am J Neuroradiol. 2013;34:1717–22. https://doi.org/10.3174/ajnr.A3573.
Qiao Y, Anwar Z, Intrapiromkul J, Liu L, Zeiler SR, Leigh R, et al. Patterns and implications of intracranial arterial remodeling in stroke patients. Stroke. 2016;47:434–40. https://doi.org/10.1161/STROKEAHA.115.009955.
Mandell DM, Mossa-Basha M, Qiao Y, Hess CP, Hui F, Matouk C, et al. Intracranial vessel wall MRI: principles and expert consensus recommendations of the American Society of Neuroradiology. AJNR Am J Neuroradiol. 2017;38:218–29. https://doi.org/10.3174/ajnr.A4893.
Portanova A, Hakakian N, Mikulis DJ, Virmani R, Abdalla WMA, Wasserman BA. Intracranial vasa vasorum: insights and implications for imaging. Radiology. 2013;267:667–79. https://doi.org/10.1148/radiol.13112310.
Connolly ES, Huang J, Goldman JE, Holtzman RN. Immunohistochemical detection of intracranial vasa vasorum: a human autopsy study. Neurosurgery. 1996;38:789–93.
Takaba M, Endo S, Kurimoto M, Kuwayama N, Nishijima M, Takaku A. Vasa vasorum of the intracranial arteries. Acta Neurochir. 1998;140:411–6.
Maiellaro K, Taylor WR. The role of the adventitia in vascular inflammation. Cardiovasc Res. 2007;75:640–8. https://doi.org/10.1016/j.cardiores.2007.06.023.
Bae H-J, Yoon B-W, Kang D-W, Koo J-S, Lee S-H, Kim K-B, et al. Correlation of coronary and cerebral atherosclerosis: difference between extracranial and intracranial arteries. Cerebrovasc Dis. 2006;21:112–9. https://doi.org/10.1159/000090209.
Qiao Y, Etesami M, Astor BC, Zeiler SR, Trout HH, Wasserman BA. Carotid plaque neovascularization and hemorrhage detected by MR imaging are associated with recent cerebrovascular ischemic events. AJNR Am J Neuroradiol. 2012;33:755–60. https://doi.org/10.3174/ajnr.A2863.
Wong LKS. Global burden of intracranial atherosclerosis. Int J Stroke. 2006;1:158–9. https://doi.org/10.1111/j.1747-4949.2006.00045.x.
Suri MFK, Johnston SC. Epidemiology of intracranial stenosis. J Neuroimaging. 2009;19(S1):11S–6S. https://doi.org/10.1111/j.1552-6569.2009.00415.x.
Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Compensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med. 1987;316:1371–5. https://doi.org/10.1056/NEJM198705283162204.
Varnava AM, Mills PG, Davies MJ. Relationship between coronary artery remodeling and plaque vulnerability. Circulation. 2002;105:939–43.
White AJ, Duffy SJ, Walton AS, Ng JF, Rice GE, Mukherjee S, et al. Matrix metalloproteinase-3 and coronary remodelling: implications for unstable coronary disease. Cardiovasc Res. 2007;75:813–20. https://doi.org/10.1016/j.cardiores.2007.05.003.
Qiao Y, Zeiler SR, Mirbagheri S, Leigh R, Urrutia V, Wityk R, et al. Intracranial plaque enhancement in patients with cerebrovascular events on high-spatial-resolution MR images. Radiology. 2014;271:534–42. https://doi.org/10.1148/radiol.13122812.
Qiao Y, Guallar E, Suri FK, Liu L, Zhang Y, Anwar Z, et al. MR imaging measures of intracranial atherosclerosis in a population-based study. Radiology. 2016;280:860–8. https://doi.org/10.1148/radiol.2016151124.
Mossa-Basha M, Hwang WD, De Havenon A, Hippe D, Balu N, Becker KJ, et al. Multicontrast high-resolution vessel wall magnetic resonance imaging and its value in differentiating intracranial vasculopathic processes. Stroke. 2015;46:1567–73. https://doi.org/10.1161/STROKEAHA.115.009037.
Qiao Y, Suri FK, Zhang Y, Liu L, Gottesman R, Alonso A, et al. Racial differences in prevalence and risk for intracranial atherosclerosis in a US Community-Based Population. JAMA Cardiol. 2017;2:1341–8. https://doi.org/10.1001/jamacardio.2017.4041.
Kontzialis M, Wasserman BA. Intracranial vessel wall imaging: current applications and clinical implications. Neurovasc Imaging. 2016;2:4. https://doi.org/10.1186/s40809-016-0014-5.
Swartz RH, Bhuta SS, Farb RI, Agid R, Willinsky RA, Terbrugge KG, et al. Intracranial arterial wall imaging using high-resolution 3-tesla contrast-enhanced MRI. Neurology. 2009;72:627–34. https://doi.org/10.1212/01.wnl.0000342470.69739.b3.
Chen XY, Wong KS, Lam WWM, Zhao H-L, Ng HK. Middle cerebral artery atherosclerosis: histological comparison between plaques associated with and not associated with infarct in a postmortem study. Cerebrovasc Dis. 2008;25:74–80. https://doi.org/10.1159/000111525.
Mazighi M, Labreuche J, Gongora-Rivera F, Duyckaerts C, Hauw J-J, Amarenco P. Autopsy prevalence of proximal extracranial atherosclerosis in patients with fatal stroke. Stroke. 2009;40:713–8. https://doi.org/10.1161/STROKEAHA.108.514349.
Labadzhyan A, Csiba L, Narula N, Zhou J, Narula J, Fisher M. Histopathologic evaluation of basilar artery atherosclerosis. J Neurol Sci. 2011;307:97–9. https://doi.org/10.1016/j.jns.2011.05.004.
Aoki S, Shirouzu I, Sasaki Y, Okubo T, Hayashi N, Machida T, et al. Enhancement of the intracranial arterial wall at MR imaging: relationship to cerebral atherosclerosis. Radiology. 1995;194:477–81. https://doi.org/10.1148/radiology.194.2.7824729.
Kerwin WS, Oikawa M, Yuan C, Jarvik GP, Hatsukami TS. MR imaging of adventitial vasa vasorum in carotid atherosclerosis. Magn Reson Med. 2008;59:507–14. https://doi.org/10.1002/mrm.21532.
Power S, Matouk C, Casaubon LK, Silver FL, Krings T, Mikulis DJ, et al. Vessel wall magnetic resonance imaging in acute ischemic stroke: effects of embolism and mechanical thrombectomy on the arterial wall. Stroke. 2014;45:2330–4. https://doi.org/10.1161/STROKEAHA.114.005618.
Astor BC, Sharrett AR, Coresh J, Chambless LE, Wasserman BA. Remodeling of carotid arteries detected with MR imaging: atherosclerosis risk in communities carotid MRI study. Radiology. 2010;256:879–86. https://doi.org/10.1148/radiol.10091162.
Babiarz LS, Astor B, Mohamed MA, Wasserman BA. Comparison of gadolinium-enhanced cardiovascular magnetic resonance angiography with high-resolution black blood cardiovascular magnetic resonance for assessing carotid artery stenosis. J Cardiovasc Magn Reson. 2007;9:63–70. https://doi.org/10.1080/10976640600843462.
Lee WJ, Choi HS, Jang J, Sung J, Kim T-W, Koo J, et al. Non-stenotic intracranial arteries have atherosclerotic changes in acute ischemic stroke patients: a 3T MRI study. Neuroradiology. 2015;57:1007–13. https://doi.org/10.1007/s00234-015-1566-9.
Kim TH, Choi JW, Roh HG, Moon W-J, Moon SG, Chun YI, et al. Atherosclerotic arterial wall change of non-stenotic intracranial arteries on high-resolution MRI at 3.0T: correlation with cerebrovascular risk factors and white matter hyperintensity. Clin Neurol Neurosurg. 2014;126:1–6. https://doi.org/10.1016/j.clineuro.2014.08.010.
Beausang-Linder M, Bill A. Cerebral circulation in acute arterial hypertension--protective effects of sympathetic nervous activity. Acta Physiol Scand. 1981;111:193–9. https://doi.org/10.1111/j.1748-1716.1981.tb06724.x.
Chatzizisis YS, Coskun AU, Jonas M, Edelman ER, Feldman CL, Stone PH. Role of endothelial shear stress in the natural history of coronary atherosclerosis and vascular remodeling: molecular, cellular, and vascular behavior. J Am Coll Cardiol. 2007;26(49):2379–93. https://doi.org/10.1016/j.jacc.2007.02.059.
Huang B, Yang W-Q, Liu X-T, Liu H-J, Li P-J, Lu H-K. Basilar artery atherosclerotic plaques distribution in symptomatic patients: a 3.0T high-resolution MRI study. Eur J Radiol. 2013;82:e199–203. https://doi.org/10.1016/j.ejrad.2012.10.031.
Xu W-H, Li M-L, Gao S, Ni J, Zhou L-X, Yao M, et al. Plaque distribution of stenotic middle cerebral artery and its clinical relevance. Stroke. 2011;42:2957–9. https://doi.org/10.1161/STROKEAHA.111.618132.
Jiang W-J, Yu W, Ma N, Du B, Lou X, Rasmussen PA. High resolution MRI guided endovascular intervention of basilar artery disease. J Neurointerv Surg. 2011;3:375–8. https://doi.org/10.1136/jnis.2010.004291.
Zeiler SR, Qiao Y, Pardo CA, Lim M, Wasserman BA. Vessel wall MRI for targeting biopsies of intracranial vasculitis. AJNR Am J Neuroradiol. 2018;39:2034–6. https://doi.org/10.3174/ajnr.A5801.
Hajj-Ali RA, Singhal AB, Benseler S, Molloy E, Calabrese LH. Primary angiitis of the CNS. Lancet Neurol. 2011;10:561–72. https://doi.org/10.1016/S1474-4422(11)70081-3.
Salvarani C, Brown RD, Calamia KT, Christianson TJH, Weigand SD, Miller DV, et al. Primary central nervous system vasculitis: analysis of 101 patients. Ann Neurol. 2007;62:442–51. https://doi.org/10.1002/ana.21226.
Mossa-Basha M, Shibata DK, Hallam DK, De Havenon A, Hippe DS, Becker KJ, et al. Added value of vessel wall MRI for differentiation of non-occlusive intracranial vasculopathies. Stroke. 2017;48:3026–33. https://doi.org/10.1161/STROKEAHA.117.018227.
Obusez EC, Hui F, Hajj-Ali RA, Cerejo R, Calabrese LH, Hammad T, et al. High-resolution MRI vessel wall imaging: spatial and temporal patterns of reversible cerebral vasoconstriction syndrome and central nervous system vasculitis. AJNR Am J Neuroradiol. 2014;35:1527–32. https://doi.org/10.3174/ajnr.A3909.
Findlay JM, Weir BK, Kanamaru K, Espinosa F. Arterial wall changes in cerebral vasospasm. Neurosurgery. 1989;25:736–45. discussion 745-746
Mandell DM, Matouk CC, Farb RI, Krings T, Agid R, terBrugge K, et al. Vessel wall MRI to differentiate between reversible cerebral vasoconstriction syndrome and central nervous system vasculitis: preliminary results. Stroke. 2012;43:860–2. https://doi.org/10.1161/STROKEAHA.111.626184.
Chen C-Y, Chen S-P, Fuh J-L, Lirng J-F, Chang F-C, Wang Y-F, et al. Vascular wall imaging in reversible cerebral vasoconstriction syndrome - a 3-T contrast-enhanced MRI study. J Headache Pain. 2018;19:74. https://doi.org/10.1186/s10194-018-0906-7.
Ducros A, Boukobza M, Porcher R, Sarov M, Valade D, Bousser M-G. The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome. A prospective series of 67 patients. Brain. 2007;130:3091–101. https://doi.org/10.1093/brain/awm256.
Singhal AB, Hajj-Ali RA, Topcuoglu MA, Fok J, Bena J, Yang D, et al. Reversible cerebral vasoconstriction syndromes: analysis of 139 cases. Arch Neurol. 2011;68:1005–12. https://doi.org/10.1001/archneurol.2011.68.
Wang Y, Lou X, Li Y, Sui B, Sun S, Li C, et al. Imaging investigation of intracranial arterial dissecting aneurysms by using 3 T high-resolution MRI and DSA: from the interventional neuroradiologists’ view. Acta Neurochir. 2014;156:515–25. https://doi.org/10.1007/s00701-013-1989-1.
Kim T-W, Choi HS, Koo J, Jung SL, Ahn K-J, Kim B-S, et al. Intramural hematoma detection by susceptibility-weighted imaging in intracranial vertebral artery dissection. Cerebrovasc Dis. 2013;36:292–8. https://doi.org/10.1159/000354811.
Krings T, Piske RL, Lasjaunias PL. Intracranial arterial aneurysm vasculopathies: targeting the outer vessel wall. Neuroradiology. 2005;47:931–7. https://doi.org/10.1007/s00234-005-1438-9.
Park JK, Lee CS, Sim KB, Huh JS, Park JC. Imaging of the walls of saccular cerebral aneurysms with double inversion recovery black-blood sequence. J Magn Reson Imaging. 2009;30:1179–83. https://doi.org/10.1002/jmri.21942.
Kleinloog R, Korkmaz E, Zwanenburg JJM, Kuijf HJ, Visser F, Blankena R, et al. Visualization of the aneurysm wall: a 7.0-tesla magnetic resonance imaging study. Neurosurgery. 2014;75:614–22 . discussion 622. https://doi.org/10.1227/NEU.000000000000055.
Scanarini M, Mingrino S, Giordano R, Baroni A. Histological and ultrastructural study of intracranial saccular aneurysmal wall. Acta Neurochir. 1978;43:171–82.
Nagahata S, Nagahata M, Obara M, Kondo R, Minagawa N, Sato S, et al. Wall enhancement of the intracranial aneurysms revealed by magnetic resonance vessel wall imaging using three-dimensional turbo spin-echo sequence with motion-sensitized driven-equilibrium: a sign of ruptured aneurysm? Clin Neuroradiol. 2016;26:277–83. https://doi.org/10.1007/s00062-014-0353-z.
Shimonaga K, Matsushige T, Ishii D, Sakamoto S, Hosogai M, Kawasumi T, et al. Clinicopathological insights from vessel wall imaging of unruptured intracranial aneurysms. Stroke. 2018;49:2516–9. https://doi.org/10.1161/STROKEAHA.118.021819.
Hudson Joseph S, Mario Z, Daichi N, Kung David K, Pascal J, Samaniego Edgar A, et al. Magnetic resonance vessel wall imaging in human intracranial aneurysms. Stroke. 2019;50:e1. https://doi.org/10.1161/STROKEAHA.118.023701.
Matouk CC, Mandell DM, Günel M, Bulsara KR, Malhotra A, Hebert R, et al. Vessel wall magnetic resonance imaging identifies the site of rupture in patients with multiple intracranial aneurysms: proof of principle. Neurosurgery. 2013;72:492–6 . discussion 496. https://doi.org/10.1227/NEU.0b013e31827d1012.
Edjlali M, Gentric J-C, Régent-Rodriguez C, Trystram D, Hassen WB, Lion S, et al. Does aneurysmal wall enhancement on vessel wall MRI help to distinguish stable from unstable intracranial aneurysms? Stroke. 2014;45:3704–6. https://doi.org/10.1161/STROKEAHA.114.006626.
Edjlali M, Guédon A, Ben Hassen W, Boulouis G, Benzakoun J, Rodriguez-Régent C, et al. Circumferential thick enhancement at vessel wall MRI has high specificity for intracranial aneurysm instability. Radiology. 2018;289:181–7. https://doi.org/10.1148/radiol.2018172879.
Hartman JB, Watase H, Sun J, Hippe DS, Kim L, Levitt M, et al. Intracranial aneurysms at higher clinical risk for rupture demonstrate increased wall enhancement and thinning on multicontrast 3D vessel wall MRI. Br J Radiol. 2019; https://doi.org/10.1259/bjr.20180950.
Wang X, Zhu C, Leng Y, Degnan AJ, Lu J. Intracranial aneurysm wall enhancement associated with aneurysm rupture: a systematic review and meta-analysis. Acad Radiol. 2018; https://doi.org/10.1016/j.acra.2018.05.005.
Coutinho JM, Sacho RH, Schaafsma JD, Agid R, Krings T, Radovanovic I, et al. High-resolution vessel wall magnetic resonance imaging in angiogram-negative non-perimesencephalic subarachnoid hemorRHAGE. Clin Neuroradiol. 2017;27:175–83. https://doi.org/10.1007/s00062-015-0484-x.
Edjlali M, Roca P, Gentric J-C, Trystram D, Rodriguez-Régent C, Nataf F, et al. Advanced technologies applied to physiopathological analysis of central nervous system aneurysms and vascular malformations. Diagn Interv Imaging. 2014;95:1187–93. https://doi.org/10.1016/j.diii.2014.05.003.
Meng H, Tutino VM, Xiang J, Siddiqui A. High WSS or low WSS? Complex interactions of hemodynamics with intracranial aneurysm initiation, growth, and rupture: toward a unifying hypothesis. AJNR Am J Neuroradiol. 2014;35:1254–62. https://doi.org/10.3174/ajnr.A3558.
Ansari SA, Schnell S, Carroll T, Vakil P, Hurley MC, Wu C, et al. Intracranial 4D flow MRI: toward individualized assessment of arteriovenous malformation hemodynamics and treatment-induced changes. AJNR Am J Neuroradiol. 2013;34:1922–8. https://doi.org/10.3174/ajnr.A3537.
Wasserman BA, Lin W, Tarr RW, Haacke EM, Müller E. Cerebral arteriovenous malformations: flow quantitation by means of two-dimensional cardiac-gated phase-contrast MR imaging. Radiology. 1995;194:681–6. https://doi.org/10.1148/radiology.194.3.7862962.
Edjlali M, Roca P, Rabrait C, Trystram D, Rodriguez-Régent C, Johnson KM, et al. MR selective flow-tracking cartography: a postprocessing procedure applied to four-dimensional flow MR imaging for complete characterization of cranial dural arteriovenous fistulas. Radiology. 2014;270:261–8. https://doi.org/10.1148/radiol.13130507.
Kortman HGJ, Smit EJ, Oei MTH, Manniesing R, Prokop M, Meijer FJA. 4D-CTA in neurovascular disease: a review. AJNR Am J Neuroradiol. 2015;36:1026–33. https://doi.org/10.3174/ajnr.A4162.
Wang H, Ye X, Gao X, Zhou S, Lin Z. The diagnosis of arteriovenous malformations by 4D-CTA: a clinical study. J Neuroradiol. 2014;41:117–23. https://doi.org/10.1016/j.neurad.2013.04.004.
Willems PWA, Taeshineetanakul P, Schenk B, Brouwer PA, Terbrugge KG, Krings T. The use of 4D-CTA in the diagnostic work-up of brain arteriovenous malformations. Neuroradiology. 2012;54:123–31. https://doi.org/10.1007/s00234-011-0864-0.
Willems PWA, Brouwer PA, Barfett JJ, terBrugge KG, Krings T. Detection and classification of cranial dural arteriovenous fistulas using 4D-CT angiography: initial experience. AJNR Am J Neuroradiol. 2011;32:49–53. https://doi.org/10.3174/ajnr.A2248.
Fujiwara H, Momoshima S, Akiyama T, Kuribayashi S. Whole-brain CT digital subtraction angiography of cerebral dural arteriovenous fistula using 320-detector row CT. Neuroradiology. 2013;55:837–43. https://doi.org/10.1007/s00234-013-1181-6.
Frölich AMJ, Wolff SL, Psychogios MN, Klotz E, Schramm R, Wasser K, et al. Time-resolved assessment of collateral flow using 4D CT angiography in large-vessel occlusion stroke. Eur Radiol. 2014;24:390–6. https://doi.org/10.1007/s00330-013-3024-6.
Frölich AMJ, Schrader D, Klotz E, Schramm R, Wasser K, Knauth M, et al. 4D CT angiography more closely defines intracranial thrombus burden than single-phase CT angiography. AJNR Am J Neuroradiol. 2013;34:1908–13. https://doi.org/10.3174/ajnr.A3533.
Frölich AMJ, Psychogios MN, Klotz E, Schramm R, Knauth M, Schramm P. Antegrade flow across incomplete vessel occlusions can be distinguished from retrograde collateral flow using 4-dimensional computed tomographic angiography. Stroke. 2012;43:2974–9. https://doi.org/10.1161/STROKEAHA.112.668889.
Tan IYL, Demchuk AM, Hopyan J, Zhang L, Gladstone D, Wong K, et al. CT angiography clot burden score and collateral score: correlation with clinical and radiologic outcomes in acute middle cerebral artery infarct. AJNR Am J Neuroradiol. 2009;30:525–31. https://doi.org/10.3174/ajnr.A1408.
Tsivgoulis G, Sharma VK, Lao AY, Malkoff MD, Alexandrov AV. Validation of transcranial Doppler with computed tomography angiography in acute cerebral ischemia. Stroke. 2007;38:1245–9. https://doi.org/10.1161/01.STR.0000259712.64772.85.
Brunser AM, Mansilla E, Hoppe A, Olavarría V, Sujima E, Lavados PM. The role of TCD in the evaluation of acute stroke. J Neuroimaging. 2016;26:420–5. https://doi.org/10.1111/jon.12334.
Kilburg C, McNally JS, de Havenon A, Taussky P, Kalani MYS, Park MS. Advanced imaging in acute ischemic stroke. Neurosurg Focus. 2017;42:E10. https://doi.org/10.3171/2017.1.FOCUS16503.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Yahyavi-Firouz-Abadi, N., Wasserman, B.A. (2020). Advanced Intracranial Vessel Wall Imaging and Future Directions. In: Yuan, C., Hatsukami, T., Mossa-Basha, M. (eds) Vessel Based Imaging Techniques . Springer, Cham. https://doi.org/10.1007/978-3-030-25249-6_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-25249-6_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-25248-9
Online ISBN: 978-3-030-25249-6
eBook Packages: MedicineMedicine (R0)