
Abstract
Surgery is the traditional treatment for thyroid nodules that keep growing over time and are associated with local symptoms. Yet, the direct and indirect expenses due to thyroidectomy and its long-term consequences, the risk of temporary or permanent complications, and the potential adverse influence on the quality of life are important concerns. Due to these considerations, a few image-guided minimally invasive procedures have been proposed for an office-based treatment of nodules that even if benign thyroid nodules are symptomatic or cause cosmetic concern. Among these techniques, US-guided laser thermal ablation (LA) is the most thoroughly assessed and is currently an easy accessible procedure in several thyroid specialized centers in Europe and Asia.
In solid nonfunctioning thyroid nodules, a laser ablation session results in a volume shrinkage that usually ranges from 60% to 80%, followed by the improvement of pressure symptoms. LA is effective for the management of small-size hyperfunctioning nodules that are associated with incomplete suppression of the surrounding thyroid tissue. So this treatment is not followed by irradiation or loss of thyroid function and is especially appealing in young patients. On the other hand, repeated LA treatments are needed to normalize thyroid function in large-size hyperfunctioning lesions. Thus, for these nodules, LA is indicated only as a combined treatment with radioiodine in order to attain a more rapid volume decrease. Notably, these treatments do not require general anesthesia and do not result in any damage to the skin and cervical structures.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Minimally invasive procedures
- Percutaneous image-guided therapy
- Thermal therapy
- Laser ablation
- Thyroid nodules
7.1 Introduction
The clinical management of thyroid lesions has been performed for many years by means of physical examination, thyroid radioisotope scan, and surgery. During the last decades, however, the advent of thyroid ultrasonography (US) and fine-needle aspiration biopsy (FNAB) has radically changed the diagnostic approach to thyroid nodular disease. The widespread application of US is now resulting in the detection of solid and cystic thyroid nodules in a large part of the adult population, with a frequency that rises with adult and old age and with female sex and that, in several series, approximate 50% [1,2,3,4,5,6,7,8]. The cytological assessment with US-guided fine-needle aspiration biopsy (US-FNAB) has sharply reduced the need for diagnostic surgery and only a minority of the recently diagnosed lesions undergo thyroidectomy. Most cytologically benign thyroid nodules are asymptomatic, their volume remain nearly unchanging over the years, and go to long-term follow-up without any intervention [9]. Even if the majority of thyroid lesions do not need therapy, a few of them (about 10%) progressively increase in size and cause local signs or pressure symptoms. Due to the discomfort or the anxiety, a large part of these last lesions are finally dealt with thyroidectomy [10, 11]. Surgery is a well-established treatment and is currently at low risk of major complications. However, the costs of thyroid surgery, the esthetic damage due to the cervical scar (that may be prevented only by rather complicated and expensive trans-axillary or trans-oral surgical approaches [12,13,14,15]), the risk of major or minor complications, and the frequent need of life-long substitution therapy should be evaluated when this clinical problem is approached [16, 17]. On the basis of these considerations, various image-guided office-based, minimally invasive procedures have been proposed with the aim of producing a clinically significant debulking of thyroid lesions and a nonsurgical management of benign symptomatic nodules [18].
In 1990, US-guided percutaneous ethanol injection was the first proposed technique for the shrinkage of autonomously functioning thyroid nodules [19]. Due to the side effects of the treatment and its technical limits, percutaneous ethanol injection is presently used only for the treatment of cystic or predominantly fluid lesions that relapse after a prior aspiration [20]. So, since 2000, US-guided minimally invasive techniques based on thermal ablation by means of energy sources (such as laser, radiofrequency, microwave, and high-intensity focused ultrasound) were investigated and are now increasingly employed in clinical practice. Among these thermal procedures, laser ablation is the most thoroughly assessed and less invasive technique and currently represents a safe and effective tool for the management of benign and selected malignant thyroid lesions.
7.2 Basic Principles of Laser Treatment
The model for the interstitial laser coagulation of body tissues was first proposed by Bown in 1983 and was subsequently validated in several experimental models [21,22,23,24]. Laser light is coherent and monochromatic, is precisely focused on the selected target, and permits the delivery of a considerable amount of energy at a distance through an optical fiber with a silica-based core. The optical fibers are flexible, with a diameter ranging from 300 to 600 μm, and transmit laser light to the tip of the fiber optic [25,26,27]. When laser light interacts with biological tissues, scattering and absorption occur, and the delivered photons induce rapid heating and thermal injury [23, 25, 28, 29].
Different laser sources and wavelengths are available and various types of fibers, tips, and applicators may be employed. Nd:YAG lasers, operating at 1064 nm, seem most suited for procedures in deep-seated organs because of their superior penetration and absorption properties in perfused soft tissues. Currently, the majority of laser procedures use either Nd:YAG or diode lasers (λ = 800–980 nm) operating in the range of 2–40 W [25].
Thermal ablation destroys the tissues by increasing their temperature so as to induce irreversible cellular damage. A temperature set at about 40 °C generally does not adversely influence cellular homeostasis while a temperature level of 45 °C results in a greater susceptibility of the cells to the injury induced by physical and chemical agents [24, 30]. An irreversible cellular damage occurs only when cells are maintained at a temperature value of 46 °C for 1 h, and the damage appears with ever-increasing quickness as the temperature level further rises [31, 32]. At a temperature level between 60 and 100 °C, a rapid coagulation of the proteins takes place with irreversible injury of enzymes, nucleic acids, and proteins, followed by cellular death over the course of a few days [22,23,24, 30, 33,34,35,36]. Critical temperature at the margin of the coagulative zone has been shown to range from 30 to 77 °C for normal tissue and from 41 to 64 °C for neoplastic tissues [37,38,39], with relevant variation of the thermal dose required to induce cell death different tissues [37]. On the other hand, a temperature value greater than 105 °C is followed by tissue carbonization and vaporization, changes that obstacle a total ablation due to the insulating effect on energy diffusion of thermal energy [32, 40,41,42,43]. On the basis of these effects, laser treatment results in a zone of coagulative necrosis with well-defined margins, a well-predictable size, and the destruction of all the cells in the ablated area.
7.3 Technique and Devices
Laser sources are variable but the most used is a 820 nm diode or a 1064 nm neodymium-yttrium-aluminium garnet (Nd:YAG) laser [25, 44,45,46]. Applicators of different gauge [44,45,46,47,48] may be used for the insertion in the target lesion and are preferentially represented by flexible 21G (<1 mm in diameter) spinal needles [47]. The commonly employed laser equipment is a 1064 nm continuous wave Nd:YAG source, operated with an output power that ranges from 3 to 5 W, and a flat-tipped quartz optical fiber with a 300-μm diameter. Laser ablation may be performed either under US guidance (with the use of a dedicated device) or assistance (with a free-hand technique) by means of a last-generation US system equipped with a high-frequency linear transducer (7.5–15 MHz).
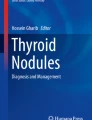
The treatment is usually performed on the patient in supine position with hyperextended neck. An accurate local anesthesia with xylocaine is performed on the skin entry site, along the planned needle tract, and on the thyroid capsule. In the case of anxiety, a mild sedation may be given with diazepam intramuscularly or by mouth. Under US monitoring, the spinal needle is inserted into the target thyroid lesion, in most cases along its longest axis. Treatments are generally performed with a fixed-power protocol (usually with a 3 W output) while the illumination time changes according to the planned ablation volume. Usually, the illumination time ranges from a minimum of 400 s to a maximum of 600 s with a total energy delivery of 1200–1800 J per optical fiber. The use as applicators of thin and minimally traumatic spinal needles allows a precise and safe positioning of one or more needles depending on the volume, shape, and location of the nodule. When multiple applicators are employed, they should be separated by a space of at least 0.8 cm and placed next to each other on the same plane to better allow the simultaneous real time control of two optical fibers. The fiber tip should be positioned at a minimum safety distance of 5–10 mm from the critical structures of the neck. In case of lesions close to the carotid vessels or the trachea wall, as for cancer recurrences in the thyroid bed, a preliminary hydro-dissection with saline solution may be performed to separate the target from the vital structure. From one to three illuminations may be performed during the same session retracting the needle with a “pullback” technique [47]. At US monitoring, the area under ablation is visualized as an echogenic zone that gradually enlarges during the illumination, and the treatment is concluded when the area of hyper-echogenicity due to tissue evaporation is stationary in size [44, 45, 49,50,51,52,53]. A reliable evaluation of the real size of the ablated area is achieved a few hours after treatment with the intravenous injection of a second-generation ultrasound contrast medium or, less precisely, with the use of color- or power-doppler. Notably, the zone of coagulative necrosis attains its maximum size about 72 h after the ablation [54], because the cellular injury and the occlusion of the vessels that supply the tissue fully develop during the days following the treatment. Figure 7.1a–f shows a representative case of a predominantly solid cold nodule before treatment (a, b), during the ablation maneuver (c, d), and 12 months after treatment (e, f).

(a, b) Representative case of solid nodule treated with laser ablation (LA). (a) US axial scan and (b) longitudinal scan—showing the nodule with a fluid component ≥20% of the volume at baseline before the treatment. (c, d) LA performed with two fibers and only one pull-back. The US longitudinal scan (c) shows two thin 21G introducers spaced 1 cm apart from each other in the deepest part of the target nodule during the first illumination. In (d) US imaging shows the second illumination of the nodule. The laser fibers positioned along the long axis of the nodule are retracted about 1 cm for a second illumination to cover the entire volume of the nodule. This technique is also known as “pull-back technique,” which has the advantage of reducing the number of direct nodule punctures, the invasiveness of the procedure, and the discomfort for the patients. During the procedure, it develops gas (visible both in c and d) for temperatures above 100 °C with consequent boiling of the aqueous component of the nodule. (e, f) The two US scans in e (axial) and in f (longitudinal) show the volumetric reduction 12 months after treatment equal to 68% compared to the volume at baseline
7.4 Thyroid Lesions Suitable for Laser Ablation
Thyroid nodules are suitable for laser ablation in the presence of the following criteria: (a) single thyroid nodule or multinodular goiter with an evidently dominant lesion; (b)hypo- or iso-functioning appearance at radioisotope thyroid scan; (c) progressive growth associated with either local compression symptoms or esthetic concern; and (d) consistently benign cytological reports at two FNAs. As the risk of overlooking a thyroid malignancy should be carefully prevented, the presence of suspicious US findings is a partial contraindication to laser ablation even in the case of benign cytological findings.
Thyroid nodules with solid, spongiform, or nearly completely solid structure are successfully ablated while pseudocystic lesions should be drained of the fluid component immediately before laser illumination [53]. Notably, laser ablation is an effective treatment also for pseudocystic nodules that repeatedly relapse after percutaneous ethanol injection.
Before treatment, withdrawal of antiplatelet therapy for at least 72 h is suggested, unless the patient is at high risk of cardiovascular events, while the anticoagulant treatment with NAO drugs may be stopped 24 h before laser ablation. Prothrombin time, partial thromboplastin time, and complete blood cell count should be assessed before the procedure. A preliminary direct laryngoscopy should be routinely performed [47]. Finally, the patient should be informed that a regular US follow-up is appropriate even after a successful minimally invasive treatment and the disappearance of local symptoms.
7.5 Clinical Results in Hypofunctioning Thyroid Nodules
Several preliminary experimental tests were performed in the 1990s, first in laboratory on liver tissue and thereafter in vivo on animal models [55,56,57] and ex vivo on freshly resected thyroid glands [58]. The initial feasibility study in humans on the use of image-guided percutaneous thermal ablation for the treatment of thyroid nodules was published in 2000 [58]. The histological examination confirmed the geometrical shape of tissue damage and its relationship with the delivered energy that was previously observed in experimental models [58]. Subsequent cytological and histological studies on 15 cold thyroid nodules that were sampled or resected 12 months after ablation treatment consistently demonstrated a well-defined area of coagulative necrosis with signs of inflammatory reaction in the ablated areas [59]. No evidence of malignant change was observed in thyroid lesions resected 24 months after laser treatment [60].
During the last years, several case reports [49, 61] and non-randomized [44,45,46,47, 62,63,64] and randomized studies [48, 50, 65, 66] have been performed on the treatment of thyroid lesions with US-guided laser ablation. All these data consistently confirmed the clinical value, good tolerability, and substantial safety of laser thermal ablation for thyroid nodular disease. The reported volume decrease at 12 months ranged from 43% to 84% [65, 67] (Table 7.1). Volume reduction was persistent, as follow-up studies demonstrated that the mean nodule volume decrease remained at 48% and 51% versus baseline size at the 3-[64] and 5-year [52] controls. In 2014, an Italian multicenter prospective randomized trial, performed with a single ablation session and fixed treatment parameters, showed a nodule volume decrease between 49% and 60% 3 years after laser treatment [66]. Accordingly, only a minority (9%) of the treated nodules demonstrated a partial regrowth at 3 years after treatment [64]. These findings were further confirmed by an externally monitored multicenter retrospective study on a series of 1531 patients [70] that demonstrated an up to nearly 80% decrease of thyroid nodules volume after one or more treatments in large size lesions. Notably, in these controlled studies, the vast majority of patients treated with laser ablation reported in a visual-analogue questionnaire the disappearance or the relevant amelioration of their local compression symptoms or esthetic damage and defined the procedure as fairly well tolerated [50, 52, 65, 66].
7.6 Clinical Results in Hyperfunctioning Thyroid Nodules
Several studies on laser treatment of small series of hyperfunctioning thyroid nodules reported the control of thyroid hyperfunction and the disappearance of the previously hyperfunctioning area at post-ablation thyroid scintigraphy [49, 62, 75]. However, at least two other trials showed that laser ablation did not constantly result in normalization of serum TSH levels and that repeated laser treatments were required to achieve satisfactory results [47, 61, 76]. These findings were confirmed by a prospective randomized study on 30 hyperfunctioning nodules associated with hyperthyroidism and suppression of normal thyroid tissue. Treatments were performed either with a single thermal ablation session or with a therapeutic radioiodine dose. Follow-up demonstrated that laser treatment and 131I therapy resulted in a similar nodule size decrease but also that thermal ablation was less effective in the control of hyperthyroidism because induced serum TSH normalization in only about 50% of patients [77]. As a whole, the available evidence demonstrates the clinical efficacy of thermal ablation for the treatment of small size, solitary, and mildly hyperfunctioning nodules [63, 76, 78]. Since functionally satisfactory results are attained only when about 80% of the volume of the hyperfunctioning nodule is ablated [79], clinical results are unsatisfactory in toxic nodular goiter or large size toxic nodules, and in these cases the normalization of thyroid function usually necessitates repeated treatment sessions the favorable results are [61] (Table 7.2). Laser ablation, however, may be of use in selected cases of large toxic nodules for a combined treatment with radioiodine. A prospective trial [80] randomized 15 cases of large hyperfunctioning nodules treated with laser ablation followed by 131I with a similar number of matched patients treated with radioiodine only. The combined treatment resulted in a faster decrease of nodule volume and in a more rapid control of hyperthyroidism and pressure symptoms than the therapy with radioiodine only.
7.7 Clinical Results in Cystic Thyroid Lesions
Few data are available on the use of thermal ablation for cystic thyroid lesions. A prospective study randomly assigned 44 prevalently cystic thyroid nodules to simple drainage or to fluid aspiration without delay followed by laser treatment [53]. A greater than 50% volume decrease and the improvement of pressure symptoms was demonstrated in 15 of 22 (68%) of patients in the thermal ablation group and only in 4 of 22 (18%) cases in the aspiration alone group at the 6-month control. Moreover, thermal ablation induced a relevant shrinkage of the solid part of the predominantly cystic lesion (from 1.8 to 1.0 mL), while in the aspiration only group, the solid part was substantially unchanged (Table 7.3). The procedure was well tolerated, no complications were observed and thyroid function was unchanged.
Percutaneous ethanol injection is the first-line nonsurgical treatment for thyroid cysts and predominantly cystic nodules because of its low expense, safety, and rapidity [81]. So, thermal ablation is selectively appropriate for the treatment of cystic lesions (mostly due to persistent bleeding) that relapse after percutaneous ethanol injection and for mixed nodules with a relevant fluid component both to prevent fluid refilling and to achieve a satisfactory shrinkage of the solid portion of the nodule.
7.8 Complications and Side Effects of Laser Treatment
The technique of image-guided laser treatment is rather simple and is usually well tolerated. A modest cervical pain, some neck swelling, and, rarely, a low fever are described by the patients after the ablation, may persist 24–48 h, and are effectively controlled by the administration of analgesics by mouth.
Minor complications are uncommon and include a more protracted neck and local inflammation pain that persist more than 48 h [47, 68]. Cervical bleeding and skin burn are definitely uncommon events [70, 82]. Relevant neck oedema sometimes associated with cystic change and rupture of the treated lesion have been occasionally reported [64]. Transitory hyperthyroidism or late hypothyroidism is unusual [64].
Major complications are rare and are due to an incorrect or overzealous technique of treatment. No relevant changes besides a modest fibrosis were reported in the cervical tissues surrounding the treated nodule in patients who eventually underwent surgery because of the coexistence of cytologically suspicious areas [59, 60].
An adequate training is anyway necessary before starting the laser procedure. Up to now, the single most relevant complication was a case of injury of the trachea that necessitated surgical repair, induced by the incorrect insertion of the laser fiber by an untrained operator [83]. Indeed, in a series of 122 procedures performed by physicians in the initial part of their learning curve, laryngeal nerve injury was observed in 1.6% of patients [64]. Conversely, a trial performed in four centers with specific expertise in minimally invasive procedures showed a definitely low risk of complications [66]. A spontaneously resolving case of vocal cord paresis was observed (<1%) and the use of analgesics for more than 24 h was required in a minority (5%) of patients [66].
A very low incidence (0.5%) of side effects and complications was confirmed in the large multicenter retrospective Italian study that collected over 1500 thyroid lesions treated by operators with specific expertise in the field [70]. More generally, a recent analysis in order to evaluate the incidence of complications of the entire population treated with LA in the various centers has documented an incidence of major complications of 0.7% and 1.4% of the minor complications [84] (Table 7.1).
As a general rule, the presence of severe pain during the laser procedure is a useful warning symptom that may prevent the risk of periprocedural complications. So, if the patient complains of an increasing pain, laser firing should be discontinued, the position of the fibers should be controlled, and the procedure should be performed after a careful repositioning of the fiber tip within the target nodule [47, 67, 69, 70, 76].
7.9 Conclusions for Clinical Practice
The occurrence of thyroid nodular disease in the general population is definitely high and the number of benign lesions that are growing or become symptomatic is accordingly increasing. In these cases, a timely and appropriate use of thermal ablation is followed by the modification of the natural history of growing benign nodules. So, the nonsurgical treatment of nodules that are cause of concern avoids the unfavorable influence of thyroidectomy on the quality of life (due to the esthetic damage and the long-term substitution therapy), decreases the direct and indirect costs of treatment, and allows a more appropriate use of surgical facilities.
Various image-guided thermal techniques, with different modalities of action, are now accessible. US-guided laser ablation is the most thoroughly assessed and less invasive of these techniques and may be safely used by operators with expertise in the field of thyroid US and US-guided FNA. However, a specific training and an initial tutorship are appropriate for decreasing the potential risk of complications. A second cytologic assessment of the benign nature of the lesion that is increasing in size is recommended before the ablation treatment to further decrease the risk of overlooking a well-differentiated thyroid cancer.
US-guided laser ablation is recommended for the treatment of solid, or predominantly solid, non-functioning thyroid nodules that with time keep growing and become symptomatic or cause cosmetic concern. Laser ablation results in a clinically significant volume decrease and the recovery from pressure symptoms in the vast majority of cases. Volume reduction, as a rule, persists over many years and the procedure can be safely repeated in case of a late, and usually partial, regrowth. Notably, the risk of esthetic cervical injury or thyroid function changes is nearly absent and the risk of periprocedural complications is very low.
Laser ablation may be used for the treatment of small-size hyperfunctioning thyroid nodules that are associated with subclinical hyperthyroidism and do not induce a complete suppression of the surrounding thyroid tissue. In these autonomously functioning nodules, especially in young patients, normalization of serum TSH is achieved without irradiation and no risk of late hypothyroidism.
On the other hand, in large-size hyperfunctioning nodules, laser ablation is generally not cost-effective, due to the need of repeated treatments, in comparison with 131I treatment. So, it should be reserved to patients who cannot access surgical or radioiodine treatments or may be used for a preliminary debulking of huge toxic lesions before 131I therapy.
Finally, laser ablation may be of use for the conclusive treatment of mostly cystic thyroid lesions that repeatedly relapse after percutaneous drainage and ethanol injection. Before thermal ablation, efficacy, complications, and tolerability of laser treatment should be fully explained, discussed with the patient, and weighted against the results and side-effects of traditional management options.
References
Mortensen JD, Woolner LB, Bennett WA. Gross and microscopic findings in clinically normal thyroid glands. J Clin Endocrinol Metab. 1955;15(10):1270–80.
Carroll BA. Asymptomatic thyroid nodules: incidental sonographic detection. AJR Am J Roentgenol. 1982;138(3):499–501.
Harach HR, Franssila KO, Wasenius VM. Occult papillary carcinoma of the thyroid. A “normal” finding in Finland. A systematic autopsy study. Cancer. 1985;56(3):531–8.
Tan GH, Gharib H. Thyroid incidentalomas: management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann Intern Med. 1997;126(3):226–31.
Wiest PW, Hartshorne MF, Inskip PD, Crooks LA, Vela BS, Telepak RJ, et al. Thyroid palpation versus high-resolution thyroid ultrasonography in the detection of nodules. J Ultrasound Med. 1998;17(8):487–96.
Brander AE, Viikinkoski VP, Nickels JI, Kivisaari LM. Importance of thyroid abnormalities detected at US screening: a 5-year follow-up. Radiology. 2000;215(3):801–6.
Frates MC, Benson CB, Charboneau JW, Cibas ES, Clark OH, Coleman BG, et al. Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statement. Radiology. 2005;237(3):794–800.
Gharib H, Papini E. Thyroid nodules: clinical importance, assessment, and treatment. Endocrinol Metab Clin N Am. 2007;36(3):707–35, vi.
Durante C, Costante G, Lucisano G, Bruno R, Meringolo D, Paciaroni A, et al. The natural history of benign thyroid nodules. JAMA. 2015;313(9):926–35.
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–214.
Gharib H, Papini E, Paschke R, Duick DS, Valcavi R, Hegedus L, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules: executive summary of recommendations. J Endocrinol Investig. 2010;33(5 Suppl):51–6.
Piccoli M, Mullineris B, Santi D, Gozzo D. Advances in robotic transaxillary thyroidectomy in Europe. Curr Surg Rep. 2017;5(8):17.
Aidan P, Arora A, Lorincz B, Tolley N, Garas G. Robotic thyroid surgery: current perspectives and future considerations. ORL J Otorhinolaryngol Relat Spec. 2018;80(3–4):186–94.
Shan L, Liu J. A systemic review of transoral thyroidectomy. Surg Laparosc Endosc Percutan Tech. 2018;28(3):135–8.
Materazzi G, Fregoli L, Papini P, Bakkar S, Vasquez MC, Miccoli P. Robot-assisted transaxillary thyroidectomy (RATT): a series appraisal of more than 250 cases from Europe. World J Surg. 2018;42(4):1018–23.
Bergenfelz A, Jansson S, Kristoffersson A, Martensson H, Reihner E, Wallin G, et al. Complications to thyroid surgery: results as reported in a database from a multicenter audit comprising 3,660 patients. Langenbeck’s Arch Surg. 2008;393(5):667–73.
Watt T, Hegedus L, Groenvold M, Bjorner JB, Rasmussen AK, Bonnema SJ, et al. Validity and reliability of the novel thyroid-specific quality of life questionnaire, ThyPRO. Eur J Endocrinol. 2010;162(1):161–7.
Gharib H, Hegedus L, Pacella CM, Baek JH, Papini E. Clinical review:nonsurgical, image-guided, minimally invasive therapy for thyroid nodules. J Clin Endocrinol Metab. 2013;98(10):3949–57.
Bennedbaek FN, Karstrup S, Hegedus L. Percutaneous ethanol injection therapy in the treatment of thyroid and parathyroid diseases. Eur J Endocrinol. 1997;136(3):240–50.
Paschke R, Hegedus L, Alexander E, Valcavi R, Papini E, Gharib H. Thyroid nodule guidelines: agreement, disagreement and need for future research. Nat Rev Endocrinol. 2011;7(6):354–61.
Bown SG. Phototherapy in tumors. World J Surg. 1983;7(6):700–9.
Matthewson K, Coleridge-Smith P, O’Sullivan JP, Northfield TC, Bown SG. Biological effects of intrahepatic neodymium:yttrium-aluminum-garnet laser photocoagulation in rats. Gastroenterology. 1987;93(3):550–7.
Thomsen S. Pathologic analysis of photothermal and photomechanical effects of laser-tissue interactions. Photochem Photobiol. 1991;53(6):825–35.
Muller G, Roggan A. Laser-induced interstitial thermotherapy. Bellingham, WA: SPIE-The International Society for Optical Engineering; 1995.
Stafford RJ, Fuentes D, Elliott AA, Weinberg JS, Ahrar K. Laser-induced thermal therapy for tumor ablation. Crit Rev Biomed Eng. 2010;38(1):79–100.
Ahrar K, Gowda A, Javadi S, Borne A, Fox M, McNichols R, et al. Preclinical assessment of a 980-nm diode laser ablation system in a large animal tumor model. J Vasc Interv Radiol. 2010;21(4):555–61.
Ahmed M, Brace CL, Lee FT Jr, Goldberg SN. Principles of and advances in percutaneous ablation. Radiology. 2011;258(2):351–69.
Trembley H, Ryan T, Strohbehn J. Interstitial hyperthermia: physics, biology, and clinical aspects. Hyperthermia and oncology. Utrecht: VSP; 1992. p. 11–98.
Jacques SL. Laser-tissue interactions. Photochemical, photothermal, and photomechanical. Surg Clin North Am. 1992;72(3):531–58.
Heisterkamp J, van Hillegersberg R, Ijzermans JN. Critical temperature and heating time for coagulation damage: implications for interstitial laser coagulation (ILC) of tumors. Lasers Surg Med. 1999;25(3):257–62.
Larson TR, Bostwick DG, Corica A. Temperature-correlated histopathologic changes following microwave thermoablation of obstructive tissue in patients with benign prostatic hyperplasia. Urology. 1996;47(4):463–9.
Goldberg SN, Gazelle GS, Halpern EF, Rittman WJ, Mueller PR, Rosenthal DI. Radiofrequency tissue ablation: importance of local temperature along the electrode tip exposure in determining lesion shape and size. Acad Radiol. 1996;3(3):212–8.
Zervas NT, Kuwayama A. Pathological characteristics of experimental thermal lesions. Comparison of induction heating and radiofrequency electrocoagulation. J Neurosurg. 1972;37(4):418–22.
Goldberg SN, Gazelle GS, Compton CC, Mueller PR, Tanabe KK. Treatment of intrahepatic malignancy with radiofrequency ablation: radiologic-pathologic correlation. Cancer. 2000;88(11):2452–63.
Nikfarjam M, Muralidharan V, Christophi C. Mechanisms of focal heat destruction of liver tumors. J Surg Res. 2005;127(2):208–23.
Nikfarjam M, Malcontenti-Wilson C, Christophi C. Focal hyperthermia produces progressive tumor necrosis independent of the initial thermal effects. J Gastrointest Surg. 2005;9(3):410–7.
Mertyna P, Hines-Peralta A, Liu ZJ, Halpern E, Goldberg W, Goldberg SN. Radiofrequency ablation: variability in heat sensitivity in tumors and tissues. J Vasc Interv Radiol. 2007;18(5):647–54.
Mertyna P, Dewhirst MW, Halpern E, Goldberg W, Goldberg SN. Radiofrequency ablation: the effect of distance and baseline temperature on thermal dose required for coagulation. Int J Hyperthermia. 2008;24(7):550–9.
Mertyna P, Goldberg W, Yang W, Goldberg SN. Thermal ablation a comparison of thermal dose required for radiofrequency-, microwave-, and laser-induced coagulation in an ex vivo bovine liver model. Acad Radiol. 2009;16(12):1539–48.
Dachman A, Smith M, Burris J, VanDeMerwe W. Interstitial laser ablation in experimental models and in clinical use. Semin Interv Radiol. 1993;10:101–12.
McGahan JP, Browning PD, Brock JM, Tesluk H. Hepatic ablation using radiofrequency electrocautery. Investig Radiol. 1990;25(3):267–70.
Nolsoe CP, Torp-Pedersen S, Burcharth F, Horn T, Pedersen S, Christensen NE, et al. Interstitial hyperthermia of colorectal liver metastases with a US-guided Nd-YAG laser with a diffuser tip: a pilot clinical study. Radiology. 1993;187(2):333–7.
McGahan JP, Dodd GDI. Radiofrequency ablation of the liver: current status. AJR Am J Roentgenol. 2001;176:3–16.
Dossing H, Bennedbaek FN, Karstrup S, Hegedus L. Benign solitary solid cold thyroid nodules: US-guided interstitial laser photocoagulation—initial experience. Radiology. 2002;225(1):53–7.
Cakir B, Topaloglu O, Gul K, Agac T, Aydin C, Dirikoc A, et al. Effects of percutaneous laser ablation treatment in benign solitary thyroid nodules on nodule volume, thyroglobulin and anti-thyroglobulin levels, and cytopathology of nodule in 1 yr follow-up. J Endocrinol Investig. 2006;29(10):876–84.
Amabile G, Rotondi M, Pirali B, Dionisio R, Agozzino L, Lanza M, et al. Interstitial laser photocoagulation for benign thyroid nodules: time to treat large nodules. Lasers Surg Med. 2011;43(8):797–803.
Pacella CM, Bizzarri G, Spiezia S, Bianchini A, Guglielmi R, Crescenzi A, et al. Thyroid tissue: US-guided percutaneous laser thermal ablation. Radiology. 2004;232(1):272–80.
Gambelunghe G, Fatone C, Ranchelli A, Fanelli C, Lucidi P, Cavaliere A, et al. A randomized controlled trial to evaluate the efficacy of ultrasound-guided laser photocoagulation for treatment of benign thyroid nodules. J Endocrinol Investig. 2006;29(9):RC23–6.
Dossing H, Bennedbaek FN, Hegedus L. Ultrasound-guided interstitial laser photocoagulation of an autonomous thyroid nodule: the introduction of a novel alternative. Thyroid. 2003;13(9):885–8.
Dossing H, Bennedbaek FN, Hegedus L. Effect of ultrasound-guided interstitial laser photocoagulation on benign solitary solid cold thyroid nodules—a randomised study. Eur J Endocrinol. 2005;152(3):341–5.
Dossing H, Bennedbaek FN, Hegedus L. Effect of ultrasound-guided interstitial laser photocoagulation on benign solitary solid cold thyroid nodules: one versus three treatments. Thyroid. 2006;16(8):763–8.
Dossing H, Bennedbaek FN, Hegedus L. Long-term outcome following interstitial laser photocoagulation of benign cold thyroid nodules. Eur J Endocrinol. 2011;165(1):123–8.
Dossing H, Bennedbaek FN, Hegedus L. Interstitial laser photocoagulation (ILP) of benign cystic thyroid nodules—a prospective randomized trial. J Clin Endocrinol Metab. 2013;98(7):E1213–7.
Nikfarjam M, Muralidharan V, Malcontenti-Wilson C, Christophi C. Progressive microvascular injury in liver and colorectal liver metastases following laser induced focal hyperthermia therapy. Lasers Surg Med. 2005;37(1):64–73.
Pacella CM, Rossi Z, Bizzarri G, Papini E, Marinozzi V, Paliotta D, et al. Ultrasound-guided percutaneous laser ablation of liver tissue in a rabbit model. Eur Radiol. 1993;3:26–32.
PacellaCM, PapiniE, FabbriniR, BizzarriG, AnelliV, RinaldiG, et al.Ultrasound-guided percutaneous interstitial laser ablation of thyroid nodules. In: Feasibility study: E.C.R.’95—European Congress Radiology, Vienna, 5–10 Mar 1995.
PacellaCM, PapiniE, BizzarriG, AnelliV, CrescenziA, PacellaS.Ultrasound-guided (US) percutaneous interstitial laser photo-coagulation of thyroid tissue. Feasibility study (abstract). In: RSNA, editor. 84th Scientific assembly and annual meeting, Chicago, IL, 29Nov–4 Dec 1998.
Pacella CM, Bizzarri G, Guglielmi R, Anelli V, Bianchini A, Crescenzi A, et al. Thyroid tissue: US-guided percutaneous interstitial laser ablation—a feasibility study. Radiology. 2000;217(3):673–7.
Piana S, Riganti F, Froio E, Andrioli M, Pacella CM, Valcavi R. Pathological findings of thyroid nodules after percutaneous laser ablation: a series of 22 cases with cyto-histological correlation. Endocr Pathol. 2012;23(2):94–100.
Cakir B, Ugras NS, Gul K, Ersoy R, Korukluoglu B. Initial report of the results of percutaneous laser ablation of benign cold thyroid nodules: evaluation of histopathological changes after 2 years. Endocr Pathol. 2009;20(3):170–6.
Rotondi M, Amabile G, Leporati P, Di Filippo B, Chiovato L. Repeated laser thermal ablation of a large functioning thyroid nodule restores euthyroidism and ameliorates constrictive symptoms. J Clin Endocrinol Metab. 2009;94(2):382–3.
Spiezia S, Vitale G, Di Somma C, Pio Assanti A, Ciccarelli A, Lombardi G, et al. Ultrasound-guided laser thermal ablation in the treatment of autonomous hyperfunctioning thyroid nodules and compressive nontoxic nodular goiter. Thyroid. 2003;13(10):941–7.
Valcavi R, Bertani A, Pesenti M, Al Jandali Rifa’Y LR, Frasoldati A, Formisano D, et al. Laser and radiofrequency ablation procedures. In: Baskin HJ, Duick DS, Levine RA, editors. Thyroid ultrasound and ultrasound guided FNA biopsy. 2nd ed. New York: Springer; 2008. p. 191–218.
Valcavi R, Riganti F, Bertani A, Formisano D, Pacella CM. Percutaneous laser ablation of cold benign thyroid nodules: a 3-year follow-up study in 122 patients. Thyroid. 2010;20(11):1253–61.
Papini E, Guglielmi R, Bizzarri G, Graziano F, Bianchini A, Brufani C, et al. Treatment of benign cold thyroid nodules: a randomized clinical trial of percutaneous laser ablation versus levothyroxine therapy or follow-up. Thyroid. 2007;17(3):229–35.
Papini E, Rago T, Gambelunghe G, Valcavi R, Bizzarri G, Vitti P, et al. Long-term efficacy of ultrasound-guided laser ablation for benign solid thyroid nodules. Results of a three-year multicenter prospective randomized trial. J Clin Endocrinol Metab. 2014;99(10):3653–9.
Achille G, Zizzi S, Di Stasio E, Grammatica A, Grammatica L. Ultrasound-guided percutaneous laser ablation in treating symptomatic solid benign thyroid nodules: our experience in 45 patients. Head Neck. 2016;38:677–82.
Papini E, Guglielmi R, Bizzarri G, Pacella CM. Ultrasound-guided laser thermal ablation for treatment of benign thyroid nodules. Endocr Pract. 2004;10(3):276–83.
Gambelunghe G, Bini V, Monacelli M, Avenia N, D’Ajello M, Colella R, et al. The administration of anesthetic in the thyroid pericapsular region increases the possibility of side effects during percutaneous laser photocoagulation of thyroid nodules. Lasers Surg Med. 2013;45(1):34–7.
Pacella CM, Mauri G, Achille G, Barbaro D, Bizzarri G, De Feo P, et al. Outcomes and risk factors for complications of laser ablation for thyroid nodules. A multicenter study on 1531 patients. J Clin Endocrinol Metab. 2015;100(10):3903–10.
Negro R, Salem TM, Greco G. Laser ablation is more effective for spongiform than solid thyroid nodules. A 4-year retrospective follow-up study. Int J Hyperthrmia. 2016;32:822–8. https://doi.org/10.1080/02656736.2016.1212279.
Mauri G, Cova L, Monaco CG, Sconfienza LM, Benedini S, Ambrogi F, Milani V, Baroli A, Ierace T, Corbetta S, Solbiati L. Benign thyroid nodules treatment using percutaneous laser ablation (PLA) and radiofrequency ablation (RFA). Int J Hyperthermia. 2017;33:295–9. https://doi.org/10.1080/02656736.2016.1244707.
Pacella CM, Mauri G, Cesareo R, Paqualini V, De Feo P, Gambelunghe G, Raggiunti B, Tina D, Cianni R, Deandrea M, Limone P, Misischi I, Mormile A, Giusti M, Oddo S, Achille G, Di Stasio E, Papini E. A comparison of laser with radiofrequency ablation for the treatment of benign thyroid nodules: a propensity score matching analysis. Int J Hyperthermia. 2017;33:911–9. https://doi.org/10.1080/02656736.2017.1332395.
Oddo S, Felix E, Mussap M, Giusti M. Quality of life in patients treated with percutaneous laser ablation for non-functioning benign thyroid nodules: a prospective single-center study. Korean J Radiol. 2018;19(1):175–84.
Cakir B, Gul K, Ugras S, Ersoy R, Topaloglu O, Agac T, et al. Percutaneous laser ablation of an autonomous thyroid nodule: effects on nodule size and histopathology of the nodule 2 years after the procedure. Thyroid. 2008;18(7):803–5.
Barbaro D, Orsini P, Lapi P, Pasquini C, Tuco A, Righini A, et al. Percutaneous laser ablation in the treatment of toxic and pretoxic nodular goiter. Endocr Pract. 2007;13(1):30–6.
Dossing H, Bennedbaek FN, Bonnema SJ, Grupe P, Hegedus L. Randomized prospective study comparing a single radioiodine dose and a single laser therapy session in autonomously functioning thyroid nodules. Eur J Endocrinol. 2007;157(1):95–100.
Gambelunghe G, Stefanetti E, Colella R, Monacelli M, Avenia N, De Feo P. A single session of laser ablation for toxic thyroid nodules: three-year follow-up results. Int J Hyperthermia. 2018;34:1–5.
Pacella CM, Mauri G. Is there a role for minimally invasive thermal ablations in the treatment of autonomously functioning thyroid nodules? Int J Hyperthermia. 2018;34:1–3.
Chianelli M, Bizzarri G, Todino V, Misischi I, Bianchini A, Graziano F, et al. Laser ablation and 131-Iodine: a 24-month pilot study of combined treatment for large toxic nodular goitre. J Clin Endocrinol Metab. 2014;99:E1283–6.
Guglielmi R, Pacella CM, Bianchini A, Bizzarri G, Rinaldi R, Graziano FM, et al. Percutaneous ethanol injection treatment in benign thyroid lesions: role and efficacy. Thyroid. 2004;14(2):125–31.
Cakir B, Gul K, Ersoy R, Topaloglu O, Korukluoglu B. Subcapsular hematoma complication during percutaneous laser ablation to a hypoactive benign solitary thyroid nodule. Thyroid. 2008;18(8):917–8.
Di Rienzo G, Surrente C, Lopez C, Quercia R. Tracheal laceration after laser ablation of nodular goitre. Interact Cardiovasc Thorac Surg. 2010;14(1):115–6.
Pacella CM. Image-guided thermal ablation of benign thyroid nodules. J Ultrasound. 2017;20(4):347–9.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Papini, E., Guglielmi, R., Persichetti, A., Pacella, C.M. (2020). Benign Thyroid Nodule Laser Ablation. In: Pacella, C., Jiang, T., Mauri, G. (eds) Image-guided Laser Ablation. Springer, Cham. https://doi.org/10.1007/978-3-030-21748-8_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-21748-8_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-21747-1
Online ISBN: 978-3-030-21748-8
eBook Packages: MedicineMedicine (R0)