
Abstract
Interactions between knowledge and health are studied in a three-period overlapping generations model with health persistence. Agents face a non-zero probability of death in adulthood. In addition to working, adults allocate time to child rearing. Growth dynamics depend in important ways on the externalities associated with knowledge and health. Depending on the strength of these externalities, increases in government spending on education or health (financed by a cut in unproductive spending) may have ambiguous effects on growth. Trade-offs between education and health spending can be internalized by solving for the growth-maximizing expenditure allocation. With an endogenous adult survival rate, multiple growth paths may emerge. A reallocation of public spending from education to health may shift the economy from a low-growth equilibrium to a high-growth equilibrium.
I am grateful to Barış Alpaslan and an anonymous reviewer for helpful comments on a preliminary draft. However, I bear sole responsibility for the views expressed here. The technical appendix is available upon request.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


JEL Classification Numbers
1 Introduction
A large strand of the literature on economic growth focuses on human capital, which is often defined to include the knowledge, skills (or more generally abilities), and health that individuals accumulate or achieve in the course of their lives.Footnote 1 A key premise of that literature is that education and good health combine to enhance worker productivity and promote growth. Investments in health, in particular, can influence the pace of economic growth via their effects on a variety of health outcomes and health-related factors, including labor market participation and labor productivity, life expectancy, savings, and fertility decisions (Bloom and Canning, 2009). Conversely, poor health may impede not only physical strength but also mental abilities, incentives to invest in education (which affects an individual’s future earning capacity), and the ability of parents to provide child care. As a result, it may not only be a cause of persistent poverty, but also an outcome of poverty. There is much evidence to support this two-way causality; Lorentzen et al. (2008), for instance, found a bidirectional link between life expectancy and income.
An extensive analytical and empirical literature has also focused on the possible interactions between components of human capital, especially education and health, and how they affect growth. Benos and Zotou (2014) for instance, in a comprehensive meta-regression analysis, found that the growth effect of education is not homogeneous across studies, but varies according to several factors, including differences in the data used to measure education and model specification. More importantly from the perspective of this contribution, they point out that heterogeneity may be due to the fact that education is conditional on health outcomes, and that these effects vary across countries.Footnote 2 Conversely, increasing education levels—above and beyond their effect on income—can also improve health outcomes. This implies that, in general, education, health and growth are all determined simultaneously, as documented empirically by Finlay (2007) in a cross-country study.
At the same time, there is significant evidence suggesting that late life health is the outcome of a cumulative process of exposure to health risks in childhood, especially infectious diseases in the first years of life. By determining health outcomes later in life, health in childhood may therefore play a critical role in the determination of health and socioeconomic status in adulthood (see Case et al., 2005; Smith, 2009). There is therefore health persistence, which represents an important source of dynamics in a growth context. The link between childhood health and health in adulthood can operate in the opposite direction as well. Indeed, there is evidence suggesting that cognitive and physical impairments of children may begin in utero, due to inadequate nutrition and poor health of the mother—illustrated most dramatically through mother-to-child transmission of HIV.Footnote 3 According to estimates reported by Bloom and Canning (2005), for instance, an estimated 30 million infants are born each year in developing countries with impaired growth due to poor nutrition during fetal life. More generally, the health of parents may also affect the health of their children, after they are born, to the extent that it determines (as noted earlier) their own physical and mental ability to provide child care. Footnote 4
This chapter examines the interactions between education and health, as two key components of human capital, and their impact on economic growth, in an overlapping generations (OLG) model.Footnote 5 In the model, education and health outcomes are jointly determined, taking into account the possible externalities alluded to earlier. At the same time, the key difference between these components is that education (or knowledge) can be accumulated without bounds, whereas health status cannot.Footnote 6 In addition, the chapter accounts for the fact that (as also noted earlier) parents’ health affects directly the health of their children (intergenerational transmission), and that health outcomes in childhood may affect health outcomes in adulthood (intragenerational transmission). As a result, health status displays persistence, as in Osang and Sarkar (2008), de la Croix and Licandro (2013), and Agénor (2015) for instance. In addition, in the model the provision of education or health services, while complementary to each other at the microeconomic level, requires the use of public resources. At the macroeconomic level, there is therefore an inherent trade-off between the provision of these two types of services. Understanding the nature of these trade-offs, and the role that externalities may play, is thus critical for public policy.
The remainder of the chapter is organized as follows. Section 8.2 provides a discussion of the interactions between education and health. Section 8.3 presents a 3-period OLG model that captures the key linkages between education and health as well as the persistence in health. In the model both components of human capital, like conventional economic goods, require a variety of inputs to be produced. Section 8.4 solves for the optimal household decision rules and derives the balanced growth path. Section 8.5 studies the impact of public policy on education and health outcomes, as well as economic growth. Section 8.6 endogenizes the adult survival rate and considers the extent to which multiple growth paths may emerge.Footnote 7 The issue of whether an increase in public spending in health or education may allow a country to escape from a low-growth equilibrium is also addressed. The last section of the chapter offers some concluding remarks.
2 Background
As noted earlier, health and education are largely interlinked in their contribution to growth because they both contribute to human capital accumulation. This section provides a more detailed review of the recent evidence on the two-way interactions between health and education.Footnote 8 The causal link from health to education is first discussed whereas the reverse link is taken up next.
2.1 Impact of Health on Education
It is now well recognized that health can have a sizable effect on education and the accumulation of knowledge.Footnote 9 Indeed, good health and nutrition are essential prerequisites for effective learning by children (see Glewwe and Miguel, 2008). In a study based on Ecuadorian data, Paxson and Schady (2007) found that health measures such as height for age and weight for age are positively related to language development (a measure of cognitive ability). Healthier children do better in school and this in turn may promote health-related knowledge (see Behrman, 2009).
Improving the health of individuals also increases the effectiveness of education. In Bangladesh, the Food for Education program, which provided a free monthly ration of food grains to poor families in rural areas if their children attended school, was highly successful in increasing school enrollment (particularly for girls), promoting attendance, and reducing dropout rates (see Ahmed and Arends-Kuenning, 2006). In a study focusing on rural Guatemala, Maluccio et al. (2009) found that improving nutrition during early childhood had a substantial impact on adult educational outcomes. Field et al. (2009), in a study of Tanzania, found that intensive iodine supplementation in utero had a large impact on cognition and human capital—particularly for girls. For their part, Bharadwaj et al. (2013) found that in Chile, children who received extra medical care at birth had not only lower mortality rates but subsequently also higher test scores and grades in school.
Conversely, inadequate nutrition, which often takes the form of deficiencies in micronutrients, reduces the ability to learn and study. Zinc deficiency, in particular, impairs brain and motor functions. Poor nutritional status can therefore adversely affect children’s cognitive development, and this may translate into poor educational attainment, as documented in Behrman (1996, 2009), Miguel (2005), Schultz (2005), and Bundy et al. (2006). Footnote 10 For instance, as documented by Ampaabeng and Tan (2013), differences in intelligence test scores in Ghana can be robustly explained by the differential impact of a famine that occurred in 1983 in different parts of the country. Moreover, the impact was most severe for children under two years of age during the famine. Poor health, in the form of respiratory infections for instance, is also an important underlying factor for low school enrollment, absenteeism, and high dropout rates. Inadequate diets may have adverse effects on mental health as well, and therefore the ability to raise children (Mental Health Foundation, 2006).
The role of early childhood health on schooling outcomes is also well illustrated in studies focusing on the incidence of malaria. Bundy et al. (2006) found that in Tanzania, the use of insecticide-treated bed nets reduced the incidence of malaria and increased attendance rates in schools. Using data on the malaria-eradication campaigns in the United States (circa 1920) and in Brazil, Colombia, and Mexico (circa 1955), Bleakley (2010a) found that, relative to nonmalarious areas, cohorts born after eradication of the disease had higher income as adults than the preceding generation—presumably as a result of higher human capital. Conversely, McCarthy et al. (2000) found that malaria morbidity, viewed as a proxy for the overall incidence of malaria among children, had a negative effect on secondary enrollment ratios. Related results are obtained by Thuilliez (2009), using cross-country regressions.
Similarly, early vaccination appears to have a significant effect on subsequent learning outcomes. In western Kenya, deworming treatment improved primary school participation by 9.3 percent, with an estimated 0.14 additional years of education per pupil treated (see Miguel and Kremer, 2004). In the same vein, Bleakley (2007) found that deworming of children in the American South had an effect on their educational achievements while in school, whereas Bloom et al. (2005) found that children vaccinated against a range of diseases (including measles, polio, and tuberculosis) as infants in the Philippines performed better in language and IQ scores at the age of ten, compared to unvaccinated children—even within similar social groups. Bundy et al. (2006), in their overview of experience on the content and consequences of school health programs (which include for instance treatment for intestinal worm infections), emphasized that these programs can raise productivity in adult life not only through higher levels of cognitive ability but also through their effect on school participation and years of schooling attained.
Another channel through which health can improve education outcomes and spur growth is through higher life expectancy and changes in time allocation within households. Increases in life expectancy tend to raise the incentive to invest in education (in addition to increasing the propensity to save, as discussed later) because the returns to schooling are expected to accrue over longer periods. Thus, at the individual level, to the extent that spending on health lengthens planning horizons, it may also raise the returns (as measured by the discounted present value of wages) of greater resources devoted to education. In a study of Sri Lanka between the period 1946 and 1953, Jayachandran and Lleras-Muney (2009) found that a reduction in maternal mortality risk increases both female life expectancy and female literacy. In a study of Brazil, Soares (2006) also found that higher longevity is associated with improved schooling outcomes. These results are consistent with the view that longer life expectancy encourages investment in education.
The evidence also suggests that intrafamily allocations regarding school and work time of children tend to be adjusted in the face of disease within the family; in turn, these adjustments may influence education outcomes and thus the rate of economic growth. As discussed by Corrigan et al. (2005), for instance, when parents become ill, children may be pulled out of school to care for them, take on other responsibilities in the household, or work to support their siblings. Hamoudi and Birdsall (2004) provided evidence that AIDS reduced schooling rates in sub-Saharan Africa. These results are consistent with the view that the risk that children may be infected by AIDS tends to deter parents from investing in their education, as argued by Bell et al. (2006). Put differently, an environment where there is great uncertainty about child survival may create a precautionary demand for children, with less education being provided to each of them. In turn, the lack of skilled labor may hamper economic growth, as illustrated by Arndt (2006) in his study of AIDS and growth in Mozambique.
Health in childhood may affect health and income in adulthood through education.Footnote 11 Pain, fatigue, and malnutrition—in addition to being a primary cause of child mortality, as documented by Pelletier et al. (2003)—can reduce the ability to concentrate and to learn. Illness can crowd out other activities that might be beneficial to child development. Some health conditions, such as attention-deficit hyperactivity disorder or deafness for instance, can also have a direct, negative impact on cognitive or verbal ability, respectively. Studies have shown indeed that education levels in adulthood are to a large extent already determined during childhood. Measures of child development, such as cognitive and verbal ability, predict fairly well measures of education outcomes in adulthood, such as earnings and employment (see Currie, 2000).Footnote 12 For instance, in a study of German data, Salm and Schunk (2008) found that gaps in child development between socioeconomic groups can be explained by differences in child health—specifically, 18.4 percent of the gap in cognitive ability and 64.8 percent of the gap in verbal ability between children of college educated parents and less educated parents can be attributed to poor initial health conditions.Footnote 13
2.2 Impact of Education on Health
A significant body of research, at both the micro and macro levels, has also shown that better education can improve health outcomes. The positive effect of education on health (just like the effect of health on education) works to a significant extent through productivity and income; but there are other channels as well.
Several studies have found that where mothers are better educated, infant mortality rates are lower.Footnote 14 This is likely because better-educated women tend, on average, to be more aware or to have more knowledge about the health risks that their children face.Footnote 15 For developing countries in general, Smith and Haddad (2000) estimated that improvements in female secondary school enrollment rates are responsible for 43 percent of the 15.5 percentage point reduction in the child underweight rate recorded during the period 1970–1995.Footnote 16 In the cross-section regressions reported by McGuire (2006), average years of female schooling have a statistically significant impact on under-five mortality rates. For sub-Saharan Africa alone, it has been estimated that five additional years of education for women could reduce infant mortality rates by up to 40 percent (see Summers, 1994). For Niger specifically, researchers have found that infant mortality rates are lower by 30 percent when mothers have a primary education level, and by 50 percent when they have completed secondary education. In a study of Uganda, Keats (2018) found that women with more schooling have higher early child health investments and have less chronically malnourished children. In the same vein, Paxson and Schady (2007), in a study of Ecuador, found that the cognitive development of children aged 3–6 years is positively associated with the level of education of their mother. Of course, third factors could be at play as well; more educated women normally earn more (thereby allowing them to spend more on the health of their children) and are more likely to live in urban areas, where access to health facilities, or nutritional supplements, is easier. But in many instances the positive effect of education on health persists even after controlling for income, location and other socio-economic factors. Indeed, Wagstaff and Claeson (2004) found that an increase in female education reduces infant mortality and raises the survival rate for children, even after controlling for income effects.
The diversity of factors through which parental schooling can affect child health outcomes is well illustrated in a study of Pakistan by Aslam and Aslam and Kingdon (2012). They considered several mechanisms through which parental schooling may promote better health outcomes (height and weight) for their children: educated parents’ greater household income, exposure to media, literacy, labor market participation, health knowledge, and the extent of maternal empowerment within the home. They found that while father’s education is positively associated with the immunization decision, mother’s education is more critically associated with longer term health outcomes. Footnote 17
Finally, there is also evidence suggesting that better educated individuals are more able to adopt healthy lifestyles and inspire their children to follow the same type of behavior (see Grossman and Kaestner, 1997; Silles, 2009; Mullahy and Robert, 2010). For instance, Cutler and Lleras-Muney (2008) found that, controlling for several factors, better educated people in the United Kingdom and the United States are less likely to be obese, less likely to smoke, and less likely to be heavy drinkers. The broader evidence that they review also suggests that increasing levels of education lead to different thinking and decision-making patterns. Conversely, a low level of education may also lead to maternal malnutrition, with dire consequences for children: inadequate intakes of nutrients during pregnancy can have irreversible effects on children’s brain development, as noted earlier.
The foregoing discussion suggests that the causality between health and education can go in both directions, and that taking into account these interactions is essential to study their joint effect on economic growth. Some of the evidence reported earlier can indeed be interpreted from the perspective of bidirectional causality. The results of Kohler and Soldo (2004) for instance, who found in a study of Mexico that individuals with low levels of education have higher mortality rates than better-educated individuals, may also be due to the fact that the level of education varies positively with health status. The next section presents a formal analysis of the interactions between education and health and their impact on economic growth.
3 The Model
Consider an OLG economy where a single good is produced and individuals live (at most) for three periods: childhood, adulthood and old age. They accumulate knowledge in the first period, supply labor in the second, and retire in the third. The good can be either consumed in the period it is produced or stored to yield capital at the beginning of the following period. All individuals are endowed with one unit of time in each period of life. Schooling is mandatory; children therefore devote all their time to education and depend on their parents for consumption. In middle age, individuals become parents and allocate their time between child rearing and the labor market. In old age, all time is devoted leisure. The only source of income is therefore wages in the second period of life, which serves to finance consumption in adulthood and old age. Savings can be held only in the form of physical capital. Agents have no other endowments, except for an initial stock of physical capital, K 0 at time t = 0, which is held by an initial generation of retirees.
Reproduction is asexual. In adulthood each individual bears n ≥ 1 children, who are born with the same innate abilities. Keeping children healthy and fostering their education involves a cost, in terms of the parent’s time.Footnote 18 Children mature safely into adulthood. At the end of the second period of life, there is a non-zero probability of dying. For children, education and health status depend on the time parents allocate to rearing their offspring, on the parent’s level of education or health, as well as access to public services. Health status in adulthood depends solely on the individual’s health in childhood. There is therefore state dependence in health outcomes. This specification is consistent with the evidence discussed earlier on intragenerational health persistence.
In addition to individuals, the economy is populated by firms and an infinitely-lived government. Firms produce marketed goods using private capital and effective labor. The government spends on education, health, and some unproductive activities. All government services are provided free of charge. Only the wage income of adults is subject to taxation. The government cannot borrow and therefore must run a balanced budget in each period. Finally, all markets clear and there are no debts or bequests between generations.
3.1 Individuals
At the beginning of their adult life in t, each individual born at t − 1 bears 1 child. Population is thus constant. Raising a child involves a time cost; each parent devotes \(\varepsilon _{t}^{R}\in (0,1)\) units of time to that activity, namely for home schooling and to take care of the child’s health (breast feeding, taking children to medical facilities for vaccines, and so on). Adults also allocate time, in proportion\(\ \varepsilon _{t}^{W}\) , to working. The individual’s time constraint is thus
By implication, although access to “out of home” health and education services per se are free, child rearing involves a cost in terms of foregone wage income and consumption.
Assuming that consumption of children is subsumed in their parent’s consumption, an individual’s expected lifetime utility at the beginning of period t is specified as
where \(c_{t+j}^{t-1}\) denotes consumption in period t + j, with j = 0, 1, ρ > 0 is the discount rate, and p ∈ (0, 1) the probability of survival from adulthood to old age, which is taken as constant for the moment. Children’s education, \(e_{t}^{C}\), and health, \(h_{t}^{C}\), matter to parents. Coefficients η E and η H are both positive and measure the individual’s relative preference for children’s education and health, respectively.Footnote 19
The period-specific budget constraints are
where a t is individual labor productivity, w t the wage rate, s t saving, r t+1 the rental rate of capital, and τ ∈ (0, 1) the tax rate. Equation (8.4) indicates that individuals consume at period t + 1 with probability p.Footnote 20
Combining these two equations yields the consolidated budget constraint
Each individual maximizes (8.2), subject to (8.5), with respect to \(c_{t}^{t-1}\), \(c_{t+1}^{t-1}\) and \(\varepsilon _{t}^{R}\), with \(\varepsilon _{t}^{W}\) solved for residually from (8.1). In a second step, parents allocate rearing time between education and health, in fixed proportions χ ∈ (0, 1) and 1 − χ, respectively. Thus, along the lines suggested by Guryan et al. (2008), time spent with children is an investment in their education and health outcomes.
3.2 Firms
There is a continuum of identical firms, indexed by i ∈ (0, 1). They produce a single nonstorable good, which is used either for consumption or investment. Production requires the use of effective labor and physical capital, which firms rent from the currently old agents.
Assuming a Cobb-Douglas technology, the production function of firm i takes therefore the form
where \(K_{t}^{i}\) denotes the firm-specific stock of physical capital, A t average, economy-wide labor productivity, \(N_{t}^{i}\) the number of adult workers employed by firm i, \(\varepsilon _{t}^{W,i}\) the time allocated by each individual to work at firm i, and β ∈ (0, 1). Thus, production exhibits constant returns to scale in firm-specific inputs, effective labor \(A_{t}\varepsilon _{t}^{W,i}N_{t}^{i}\) and capital \( K_{t}^{i} \). However, there is a population externality; the greater the size of the adult population, \(\bar {N}\), the lower the productivity of each firm’s capital stock. This congestion effect reflects the possibility that if more workers use fixed physical assets (such as roads or electricity) it becomes more difficult for each firm to use them (due to traffic jams, which prevent trucks from moving around to deliver goods, or to frequent power outages, which limit the use of machines and equipment). The magnitude of this congestion effect is measured by the parameter ϕ N ≥ 0.
Markets for both physical capital and labor are competitive. Each firm’s objective is to maximize profits, \(\Pi _{t}^{i}\), with respect to raw labor and capital, taking A t, \(\varepsilon _{t}^{W,i}\) and input prices as given:
Profit maximization yields
which implies that inputs are paid at their marginal product.
Given that all firms are identical, in a symmetric equilibrium \( N_{t}^{i}=N_{t}=\bar {N}\) and \(K_{t}^{i}=K_{t}\), ∀i. Thus, these conditions become
Average productivity is given by
where E t is the average stock of knowledge and h t average adult health status. Thus, both education and health affect individual productivity. For tractability, a simple multiplicative form is used. Footnote 21
Because the number of firms is normalized to 1, aggregate output is given by, using (8.9),
To eliminate the scale effect associated with population requires setting β − ϕ N(1 − β) = 0, or equivalently ϕ N = β∕(1 − β) . Consequently, using (8.1),
where x t = E t∕K t is the knowledge-physical capital ratio (or, for short, the knowledge-capital ratio). Given that, as shown later, both x t and h t, as well as \(\varepsilon _{t}^{R}\), are constant in the steady state, the model is linear in the physical capital stock and exhibits therefore endogenous growth.
3.3 Schooling
The schooling technology depends on several inputs. First, it depends on the time allocated to education in childhood; as noted earlier, children must allocate all of their time to education, and this is normalized to unity. Second, knowledge accumulation is affected by the time allocated by parents to child rearing. As noted earlier, a sequential process is considered: parents determine first the total amount of time allocated to rearing their children, \(\varepsilon _{t}^{R}\), and then subdivide that time into a fraction χ ∈ (0, 1) allocated to home schooling and 1 − χ to health care.
Third, knowledge accumulation depends on government spending on education, \( G_{t}^{E}\), per child. Given that each individual has only one child, the total number of children is simply equal to the adult population, \(\bar {N}\). Fourth, it depends on the level of education of the parent. Because individuals are identical within a generation, parental education is taken to be equal to the average stock of knowledge of the current generation. Finally, to capture the health externality discussed earlier, schooling depends on how healthy the individual is in childhood.
Normalizing the adult population to unity, knowledge acquired in childhood, \( e_{t}^{C}\), is thus given by
where ν 1 ∈ (0, 1) and ν 2, ν 3 > 0. For tractability, constant returns to scale are imposed on the education technology with respect to public spending per child and average parental knowledge. In addition, as in Hazan and Zoabi (2006) for instance, education and health are gross complements in the production of knowledge (\(\partial ^{2}e_{t}^{C}/\partial E_{t}\partial h_{t}^{C}>0\)).
In adulthood, individuals do not engage in additional learning.Footnote 22 Assuming for simplicity no depreciation and full persistence in learning, the knowledge that each individual has in the second period of life, e t+1, is therefore
Substituting (8.11) in (8.12) yields
Thus, because a parent’s education affects his children’s learning ability, there is serial dependence in knowledge. In addition, knowledge in adulthood also depends on health status in childhood.
3.4 Health Status
The health status of a child, \(h_{t}^{C}\), depends on the amount of time allocated by each parent to rearing them, the average parent’s level of education and health, E t and h t, respectively, and government expenditure on health, \(G_{t}^{H}\), per child. This last effect captures for instance the impact of public spending on nutritional programs in schools and vaccination campaigns, which reduce children’s vulnerability to disease and improves their health. Thus, health status in childhood is given by
where all coefficients are positive. The externality associated with parental education is captured by θ 3, whereas the external (intergenerational) effect associated with parental health is captured by θ 4. With θ 4 < 1, parental health exerts a diminishing marginal effect on a child’s health. In addition, the supply of public health services is congested by the stock of physical capital, with a congestion parameter ϕ H > 0.Footnote 23 As before, this congestion effect could represent the effect of an intensive use of a fixed stock of public physical assets (such as roads or electricity) to produce goods, which makes it more difficult to access health facilities. Alternatively, the scaling of \( G_{t}^{H}\) by \(K_{t}^{\phi _{H}}\) can be viewed as capturing the fact that greater economic activity (as proxied by the capital stock) has potentially adverse effects on children’s well-being (as a result of air pollution for instance), which in turn mitigates the benefits of public spending on health. Footnote 24
Equation (8.15) can be rewritten as
To ensure that health status is stationary, the restriction ϕ H = (θ 1 + θ 3)∕θ 1 is also imposed. The above expression therefore becomes
To capture the idea (discussed in the introduction) that cognitive deficits in early life may be impossible to reverse, and that health does not deteriorate over time, the health status of adults is assumed to depend only on their health status in childhood:
Substituting (8.15) in (8.16) yields
In the steady state, the public health spending-capital ratio, time allocated to child rearing, and the knowledge-capital ratio are all constant; health status is thus stationary as well. Knowledge, by contrast, grows without bounds. This is the fundamental difference, alluded to earlier, between education and health as sources of human capital.
3.5 Government
The government taxes only adults at the constant rate τ ∈ (0, 1) and spends a total of \(G_{t}^{E}\) on education, \(G_{t}^{H}\) on health, and \( G_{t}^{U}\) on other (unproductive) items. It cannot issue bonds and must therefore run a balanced budget:
Shares of spending are constant fractions of revenues:
where υ h ∈ (0, 1). Combining (8.18) and (8.19) therefore yields
In sum, the model captures the possible bidirectional externalities associated with health and education, discussed in the previous section, through the parameters ν 3 and θ 3. If ν 3 = 0, health generates no benefit in terms of childhood education, whereas if θ 3 = 0 knowledge has no benefit in terms of health outcomes. Through the parameter θ 4, the model captures also intergenerational persistence in health.
3.6 Market Clearing and Equilibrium
Given the assumption of full depreciation of the stock of physical capital, the asset market-clearing condition requires tomorrow’s capital stock to be equal to today’s aggregate savings:
The following definition may therefore be proposed:
Definition 8.1
A competitive equilibrium for this economy is a sequence of prices \(\{w_{t},r_{t}\}_{t=0}^{\infty }\), income and time allocations \(\{c_{t}^{t-1},c_{t+1}^{t-1},s_{t},\varepsilon _{t}^{R}\}_{t=0}^{\infty }\), physical capital stock \( \{K_{t+1}\}_{t=0}^{\infty }\), knowledge stock \(\{E_{t+1}\}_{t=0}^{ \infty }\), health status of children and adults \( \{h_{t}^{C},h_{t}\}_{t=0}^{\infty }\), a constant tax rate τ and constant spending shares υ E, υ H such that, given the initial stocks K 0, E 0 > 0, and health status h 0, individuals maximize utility, firms maximize profits, markets clear, and the government budget is balanced.
In equilibrium, individual productivity must also be equal to the economy-wide average productivity, so that a t = A t, and similarly for knowledge, so that e t = E t. The following definition characterizes the balanced growth path:
Definition 8.2
A balanced growth equilibrium is a competitive equilibrium in which \(c_{t}^{t-1}\), \(c_{t}^{t-1}\), A t, E t, K t, Y t and w t all grow at the constant endogenous rate 1 + γ, the rate of return on private capital is constant, and health status is constant.
4 Steady-State Growth
The solution of the individual’s maximization problem is provided in the Appendix. It shows that in equilibrium,
where σ is the marginal propensity to save, defined as
From these solutions, it can be shown that an increase in the survival probability, p, raises the savings rate, s, lowers time allocated to child rearing, \(\tilde {\varepsilon }^{R}\), and raises time allocated to market work, \(\tilde {\varepsilon }^{W}\). The first result is fairly standard and consistent with the empirical evidence on longevity.Footnote 25 Through a life-cycle effect, a higher adult survival rate dictates a need for higher savings to finance consumption in old age, and thereby has a positive effect, ceteris paribus, on the incentive to save in adulthood, that is, the savings rate. At the same time, an increase in the survival rate leads, ceteris paribus, to less total time allocated to caring for children, as in Zhang and Zhang (2005), for instance. Thus, parents also increase the level of their savings by allocating more time to market work.
The dynamic system driving the economy is also derived in the Appendix, in terms of two variables: health status in adulthood, h t, and the knowledge-capital ratio, x t = E t∕K t. Specifically, the model can be condensed into a first-order linear difference equation system in \(\hat {h} _{t}=\ln h_{t}\) and \(\hat {x}_{t}=\ln x_{t}\) which (ignoring constant terms) can be written as
where
and
As also shown in the Appendix, the balanced-growth rate of output per worker is given by
where \(\tilde {x}\) and \(\tilde {h}\) are the steady-state values of x t and h t, which are solutions of the system
where
In what follows it will be assumed that θ 4 ∈ (0, 1) is not too large, to ensure that 1 − (βθ 1 + θ 4) > 0.Footnote 26 But to make further progress, alternative cases regarding the externality parameters θ 3 and ν 3 must be considered.
- Case 1.:
-
If there are no externalities of any sort, that is, θ 3 = ν 3 = 0, then ϕ 1 = −(1 − β)ν 1 < 0, so that β − ϕ 1 > 0 and, given that ν 1 ∈ (0, 1), ϕ 2 − β = β(ν 1 − 1) < 0.
- Case 2.:
-
If there is only an education externality for health, that is, ν 3 = 0 and θ 3 > 0, then again ϕ 1 = −(1 − β)ν 1 < 0, β − ϕ 1 > 0, and ϕ 2 − β = β(ν 1 − 1) < 0.
- Case 3.:
-
If there is only a health externality for education , that is, ν 3 > 0 and θ 3 = 0, then \(\phi _{1}=-(1-\beta )(\nu _{1}+\theta _{1}\nu _{3})+\theta _{1}\nu _{3}\beta (\nu _{1}+\theta _{1}\nu _{3})-\nu _{1}\gtrless 0\), \(\beta -\phi _{1}=-\beta \lbrack (\nu _{1}+\theta _{1}\nu _{3})-1]+\nu _{1}\gtrless 0\), and \(\phi _{2}-\beta =\beta \lbrack (\nu _{1}+\theta _{1}\nu _{3})-1]+\theta _{4}\nu _{3}\gtrless 0\).
- Case 4.:
-
If both types of externalities are present, that is, ν 3, θ 3 > 0, then in order to have β − ϕ 1 > 0, it must be that (θ 1 + θ 3)ν 3 < β + (1 − β)(ν 1 + θ 1ν 3), whereas for ϕ 2 − β < 0 it must be that ν 3 < β(1 − ν 1)∕(βθ 1 + θ 4).
In what follows, the focus will be on the two opposite cases 1 and 4, assuming in the latter that the combination of ν 3 and θ 3 is such that both restrictions are satisfied.Footnote 27 To establish the signs of a 11 and a 12, note that in Case 1,
whereas in Case 4, given that again β − ϕ 1 > 0, then − β + ϕ 1 < 0, and thus, \(a_{11}=1-\beta +\phi _{1}\gtrless 0\). And given that ϕ 2 − β < 0 then a 12 < 0.Footnote 28
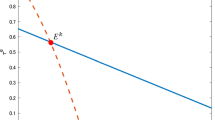
Equations (8.26) and (8.27) define the steady-state relationships between x t and h t. In both Cases 1 and 4, β − ϕ 1 > 0 and ϕ 2 − β < 0. Equation (8.26) defines a convex curve depicted as XX in Fig. 8.1, whose slope is negative and given by (ϕ 2 − β)∕(β − ϕ 1) < 0. Similarly, Eq. (8.27 ) defines a curve depicted as HH, whose slope is positive and given by [1 − (βθ 1 + θ 4)]∕(βθ 1 + θ 3) > 0. Footnote 29 It is immediately clear from the shape of these curves that there is a unique equilibrium, located at point E. The knowledge-physical capital ratio and health status in adulthood are thus both constant in the steady state. As shown in the Appendix, for empirically plausible values of the parameters β, θ 4, ν 1 and θ 1, the equilibrium is stable in Case 1 (where there are no externalities, or, more generally, when these externalities are weak), as well as in Case 4.Footnote 30

Balanced growth equilibrium
Before studying the effects of public policy in this setting, it is worth noting the conflicting effects of time allocated to child rearing, \(\tilde { \varepsilon }^{R}\), on the steady-state solutions (8.26) and (8.27 ), and thus on the steady-state growth rate (8.25). On the one hand, increased time devoted to child rearing improves health and education (both in childhood and adulthood), which raise productivity, but on the other it reduces time allocated to market work. This trade-off becomes even more palpable when considering, as is done later, the case of an endogenous survival rate.
5 Public Policy
Equations (8.22) and (8.23), as well as (8.25)–(8.27) can be used to study the impact of changes in the shares of government spending on time allocation and growth, assuming that these increases are either budget neutral and financed by a cut in unproductive spending (dυ h + dυ U = 0, h = E, H) or instead by a cut in the other component of productive spending (dυ E + dυ H = 0). Footnote 31 In the latter case, there is a trade-off between the two components of expenditure, which can be internalized by solving for the growth-maximizing share of one of them. These issues are considered in turn, with a focus on steady-state effects rather than transitional dynamics.
5.1 Changes in Government Spending
Consider first a budget-neutral increase in public spending in education, financed by a cut in unproductive expenditure (dυ E + dυ U = 0). The results are illustrated in Fig. 8.2. Curve XX shifts to the right, whereas curve HH does not change. The equilibrium moves from point E to point E ′, implying that the outcome is both an improvement in health status and a higher knowledge-physical capital ratio. Consequently, the steady-state growth rate, as can be inferred from (8.25), increases unambiguously. The stronger the externalities associated with education and health, the stronger these effects are. Even though higher output means higher savings and investment, the increase in the stock of knowledge is always larger than the increase in the stock of physical capital. As a result, the knowledge-capital ratio always increases.

Increase in government spending on education
Consider now a budget-neutral increase in health spending, again financed by a cut in unproductive expenditure (dυ H + dυ U = 0). The results are illustrated in Fig. 8.3. Curve XX shifts to the right, whereas curve HH shifts down. However, there are now two cases to consider, depending on the magnitude of the shift in these curves. In both cases, while health status always improves, the net effect on education outcomes is ambiguous.

Increase in government spending on health
Indeed, Scenario A depicts the case where XX shifts strongly, to X ′X ′, relatively to HH. The new equilibrium is at E ′, characterized (as in the case of higher spending on education), by an improvement in both health status and education. However, the figure also illustrates the case where XX shifts relatively little, to X ′′X ′′, so that the new equilibrium is at E ′′. In this scenario, which is likely to occur when the externality of health for education is low, health status improves but (relative) education outcomes deteriorate. Similarly, Scenario B corresponds to the case where HH can either shift a little (to H ′H ′ , so that the new equilibrium is at E ′) or a lot (to H ′′H ′′, so that the new equilibrium is at E ′′). In the first scenario, both education and health outcomes improve, whereas in the second the only benefits are in terms of health status. When the effects on education outcomes are negative, the net effect on growth is ambiguous—even if changes in government spending are financed by cuts in unproductive spending. As shown in the Appendix, outcome E ′′ corresponds to the case where the health externality for education is weak, whereas outcome E ′ corresponds to the case where that externality is sufficiently strong. In addition, outcomes C in Scenario A, and outcomes C and C ′′ in Scenario B, correspond to the case where XX does not change at all, which is what occurs when there is no health externality for education, that is, ν 3 = 0.
Intuitively, the reason why the effect on education outcomes (or, more precisely, the human-physical capital ratio) is ambiguous when health spending is increased is as follows. The direct effect of higher spending on health is an improvement in health status and productivity, which raises output, and therefore government spending across the board. This has a positive effect on both education and health outcomes. However, at the same time the increase in income raises savings and investment, and therefore the stock of physical capital as well. When the health externality for education is weak, the latter effect dominates, so that the human-physical capital ratio falls. By contrast, when the health externality for education is sufficiently strong, the increase in knowledge dominates, and the human-physical capital ratio increases. Thus, whether the net effect on the steady-state growth rate of output is negative or positive cannot be determined a priori. But the stronger the direct effect of health spending on health status, or the stronger the health externality, the more likely it is that an increase in government spending on health will lead to higher growth.
5.2 Growth-Maximizing Policy
Consider now the case where there is a trade-off in spending, that is, dυ E + dυ H = 0. In such conditions, even in the absence of externalities, the government faces a choice regarding how best to allocate its tax revenues. Specifically, suppose that that the government internalizes this trade-off by choosing a spending allocation that maximizes growth, rather than welfare.Footnote 32
From (8.25) to (8.27), the growth-maximizing share of government spending on education is given by setting \(d\ln (1+\gamma )/d\upsilon _{E}=0\) , that is,
As shown in the Appendix, the growth-maximizing share of spending on education is given by
where, in both Cases 1 and 4,
which imply that
Formula (8.30) is quite complicated in general—even without education and health externalities, because the direct effects (as measured by ν 1 and θ 1) matter. To make further progress in assessing the role of externalities, a simple numerical exercise can be performed. Parameter values are set at β = 0.65 (a standard value), θ 4 = 0.6 (to ensure that 1 − (βθ 1 + θ 4) > 0), ν 1 = 0.55 (as in Osang and Sarkar, 2008), θ 1 = 0.55 (for symmetry), and ν 3 = θ 3 = 0 initially. Thus, as implied by (8.30), with no externalities of any sort, \(\upsilon _{E}^{\ast }=0.421\). Using the same values, with ν 3 = 0 and θ 3 = 0.4 yields \( \upsilon _{E}^{\ast }=0.593\), whereas with ν 3 = 0.4 and θ 3 = 0 the result is \(\upsilon _{E}^{\ast }=0.296\). With ν 3 = θ 3 = 0.4 , then \(\upsilon _{E}^{\ast }=0.457\). More generally, Fig. 8.4 illustrates how the optimal share of spending on education changes when ν 3 and θ 3 vary between 0 and 1. What these results indicate is that the stronger the externality of education for health is, the larger the share of spending on education should be (or the lower the share of health spending should be). Conversely, the stronger the health externality for knowledge accumulation, the lower should be the share of spending on education. At the same time, the knowledge externality for health has a particularly strong impact on the growth-maximizing allocation; as θ 3 increases (for any given value of ν 3), the growth-maximizing share of spending on education increases rapidly—much more so than in the reverse scenario where ν 3 increases (for any given value of θ 3). Even when the externalities are equally strong, the effect is not symmetric; it is still optimal to spend a bit more on education. These results are also consistent with the fact that changes in education expenditure have unambiguous effects (as discussed earlier) on the knowledge-capital ratio and the rate of economic growth, in contrast with changes in health expenditure.

Externalities and growth-maximizing share of spending on education
6 Endogenous Survival Rate
In the foregoing analysis the survival rate, p, was assumed exogenous. Suppose now, as in Finlay (2006), Tang and Zhang (2007), Osang and Sarkar (2008), and Agénor (2015) for instance, that life expectancy is endogenous and related directly to health status.Footnote 33 To capture this link, one approach is to relate the survival rate directly to the individual’s own health status. In solving their optimization problem, parents would then internalize the implications of their time allocation decisions. An alternative approach is to assume that the survival probability of any particular individual depends on average health status in the economy—which, in equilibrium, is of course the same for all individuals. Thus, when choosing their consumption and time allocation, agents would continue to take p as given and the solutions derived earlier continue to apply.
Suppose then that the adult survival rate is a piece-wise function defined as
where f ′ > 0 and f ′′ < 0. Thus, if health status is below h L, the likelihood of surviving to old age is p m. In the context of poor countries, this could reflect the fact that at first, improvements in health status do not translate into higher survival rates. As health status improves above that threshold, the relationship between p t and h t is positive and concave over the range (h L, h H). Footnote 34It becomes constant again at p M and p m < p M < 1 for values of health status above h H. Put differently, beyond a certain point, further changes in health status have no effect on the probability to survive—perhaps reflecting the fact that there always remains a risk of accidental death.Footnote 35
The implication of this analysis is as follows. Consider first the case where initially health status is at or below h L, so that p is constant. Suppose that an ambitious increase in spending on health, financed by a cut in unproductive spending, leads to an improvement in health status—despite possibly having ambiguous effects on education outcomes, as discussed earlier—and that this increase is large enough to move the economy into the intermediate range (h L, h H). The survival rate therefore increases, which raises the savings rate and time allocated to market work, thereby promoting growth. However, in this setting rearing time is productive; it benefits both education and health outcomes. A reduction in rearing time may therefore have adverse effects on these variables, despite higher government spending. Moreover, these effects may be magnified if externalities are strong. As a result, the net effect on growth can be ambiguous—even if the increase in public spending on health is offset by a cut in unproductive spending.Footnote 36 Conversely, it is also possible that the net effect on growth is positive; a health subsidy can help move the economy from a low-growth equilibrium to an equilibrium with a higher saving rate, higher life expectancy, and faster growth. If the direct effect on health status is positive, a strong externality of health on education would increase the likelihood of a transition from stagnation to growth. This result is thus consistent with those of Tang and Zhang (2007), albeit in a model where health and education externalities are not accounted for, and Hazan and Zoabi (2006), who emphasize (as is the case here) the importance of a sufficiently high degree of complementarity between health and education in the production of knowledge.Footnote 37 In addition, even if an increase in spending on health is financed by a cut in education expenditure, it is still possible for the net effect on growth to be positive if the health externality for education is strong.
Finally, it is worth noting that, with p constant, the values of ν 2 and θ 2 (which measure the effect of rearing time on education and health outcomes, respectively) do not matter for stability, as shown in the Appendix. However, when p is endogenously related to health status, h, it affects the savings rate and thus time allocated to child rearing, \( \tilde {\varepsilon }^{R}\), which therefore becomes endogenous—and so does time allocated to market work. Consequently, the stability conditions discussed in the Appendix would be more complicated. In addition, this would affect the slopes of XX and HH in Figs. 8.1, 8.2 and 8.3, as well as the impact of changes in government spending on growth, as discussed earlier. Finally, with an endogenous survival rate, the solution of the growth-maximizing problem would also become highly nonlinear, thereby precluding the derivation of an explicit expenditure allocation rule, as in (8.30).
7 Concluding Remarks
Education and health are two important dimensions of human capital. The purpose of this chapter was to review the evidence on the interactions between these two dimensions, present an endogenous growth model that captures their interactions, and study the impact of public policy in that setting. A key feature of the model is that health is distinct from knowledge as a source of human capital because it cannot grow without bounds. In addition, consistent with the evidence, the model accounts for the possibility that causality can go both ways: policies that impact educational attainment may have a large effect on health outcomes, and vice versa. It also accounts for the well-documented facts that parental health effects the health of children at birth, and that health in late life is the outcome of a cumulative process of exposure to health risks in childhood.
The analysis showed that growth dynamics depend in critical ways on the externalities associated with knowledge and health. Depending on the strength of these externalities, an increase in government spending on health (financed by a cut in unproductive spending) may have ambiguous effects on economic growth. It was also shown that trade-offs between education and health spending can be internalized by setting the composition of expenditure so as to maximize the growth rate. All else equal, the stronger the health (education) externality in education (health), the smaller (larger) the share of spending on education should be. With an endogenous adult survival rate, multiple growth paths may emerge. A reallocation of public spending from education to health may shift the economy from a low-growth equilibrium to a high-growth path. However, if the time allocation effect associated with an endogenous increase in the survival probability—a reduction in time allocated to child rearing, due to life-cycle considerations, which on the one hand leads to an increase in time allocated to market work, but on the other may adversely affect education and health outcomes, and thus productivity—it is theoretically possible that an increase in government spending on health may have an adverse effect on growth.
The analysis presented in this chapter can be extended in several directions. First, at the empirical level, it would be useful to conduct a comprehensive cross-country econometric analysis of a simultaneous determination of schooling or education levels, health outcomes and economic growth. This would allow an assessment of the magnitude of the externalities associated with education and health, and provide some of the key parameters needed for a full-blown calibration of the model, in order to study numerically its properties.
Second, the fertility rate could be endogenized, to assess how changes in health outcomes can affect the decision to have children. Based on the results in Agénor (2015), one can infer what is likely to happen in that case: an increase in the survival rate (due to an improvement in health status, itself related to higher spending on health, as discussed earlier), would reduce the fertility rate and total time allocated to child rearing. The effect on unit rearing time, however, is likely to be ambiguous. Intuitively, the reduction in the fertility rate allows parents to allocate more time to each of them to improve their health—even though total time devoted to child rearing falls—in effect, substituting quality to quantity. Because changes in rearing time have persistent effects on health and education, they would also alter in significant ways the dynamics of the economy and whether multiple equilibria may emerge.
Finally, the analysis could be extended by introducing a gender dimension. This would allow, in particular, to study how the level of knowledge of each parent (which may differ due to discrimination, both at home and in the market place, against women) affects education and health outcomes for their children. For instance, Breierova and Duflo (2004), in a study of Indonesia, found that female and male education seem equally important factors in reducing child mortality. However, as noted earlier, Aslam and Kingdon (2012) in a study of Pakistan found that while a father’s education is positively associated with the immunization decision, a mother’s education is more critically associated with longer term health outcomes. Accounting for a gender dimension would help to consider how a broader set of policies can affect education and health outcomes, as well as, ultimately, economic growth.
Notes
- 1.
Two comprehensive composite measures of human capital have been published recently. The first, by the Institute for Health Metrics and Evaluation, covers 195 countries, whereas the second, by the World Bank, covers 157 countries. See https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31941-X/fulltext and http://www.worldbank.org/en/publication/wdr2019.
- 2.
Among available studies, Baldacci et al. (2004), using cross-country regressions, found that health outcomes (as proxied by the under-five child mortality rate) have a statistically significant effect on school enrollment rates.
- 3.
- 4.
See for instance the results of Powdthavee and Vignoles (2008) for Britain.
- 5.
Tang and Zhang (2007) develop an OLG model with education and health but do not account for direct interactions between them. Tamura (2006) and Ricci and Zachariadis (2013) develop OLG models where schooling exerts external effects on health, in the form of a negative effect on adult mortality in the first case and a positive effect on longevity in the second. In the models of Galor and Mayer-Foulkes (2004) and Hazan and Zoabi (2006), health is, in addition to education, an input in the production of human capital. However, none of these contributions fully examines bidirectional effects, and the role of public policy, as is done here. Finally, Agénor (2011) do account for bidirectional effects in a continuous time, infinite-horizon setting, but in their model health is not stationary.
- 6.
- 7.
The assumption that the survival rate is constant initially is for expositional reasons. It helps to clarify the role of externalities and the fundamental trade-off between spending on education and spending on health.
- 8.
- 9.
See Bleakley (2010b) for an overview of the evidence on the impact of health and education.
- 10.
Research at the National institute of Health in the United States has also shown that the children of mothers who did not eat food with ample omega-3 fatty acids had a lower IQ than children who did.
- 11.
- 12.
At the same time, child development may also be related to a child’s socioeconomic background (see Taylor et al., 2004). If so then children from disadvantaged families may fall behind early in life and may be unable to catch up later.
- 13.
See also Oreopoulos et al. (2008), who found in a study for Canada that poor infant health is a strong predictor of future education outcomes.
- 14.
- 15.
As noted by Kohler and Soldo (2004) for instance, it is useful to separate two potential channels that may relate parents’ education to their children’s health and offsprings’ late life health outcomes. The first is the father’s education, which likely operates through economic circumstances (because fathers may be those who were the primary suppliers of economic resources in the family). The second is the mother’s education, which operates through knowledge about health care and health behavior that are essential determinants of children’s health outcomes.
- 16.
- 17.
The gender dimension of the interactions between education and health is further discussed in the concluding remarks.
- 18.
For simplicity, the direct cost of schooling and the cost of keeping children healthy (medicines, and so on) are abstracted from.
- 19.
If parents care equally about the health and education of their child, η E = η H.
- 20.
Alternatively, it could be assumed that the saving left by individuals who do not survive to old age is confiscated by the government, which transfers them in lump-sum fashion to surviving members of the same cohort. The effective rate of return to saving would thus be (1 + r t+1)∕p, which would yield an equation similar to (8.4). See Agénor (2012, Chapter 3) for a simple derivation.
- 21.
A more general specification would be to set \(A_{t}=E_{t}^{\chi }h_{t}^{1-\chi }\), where χ ∈ (0, 1).
- 22.
This assumption is consistent with the evidence for Sub-Saharan Africa for instance, which suggests that only 6.8 percent of youth engage in tertiary education, compared to a world average of 30 percent (United Nations, 2016, p. 46).
- 23.
See Osang and Sarkar (2008) and Agénor (2015). Of course, a similar argument could apply for the production of education services in (8.11). However, unlike health, knowledge does grow without bounds and the specification adopted in that equation is sufficient to ensure constant growth in the steady state.
- 24.
Activity in that case could of course be measured by the level of final output, but given the linear relationship between Y t and K t implied by (8.10) the use of the latter is mainly a matter of convenience.
- 25.
- 26.
Using θ 1 = 0.55, as in Osang and Sarkar (2008, Table 4) for instance, and a standard value of β = 0.65, this condition implies that θ 4 cannot be higher than 0.64.
- 27.
Note that Case 2 is qualitatively very similar to Case 1. An exhaustive analysis of all cases would require a numerical calibration.
- 28.
There are also intermediate cases, where one type of externality is high and the other low, which are ignored for the moment to facilitate the exposition of the graphical analysis.
- 29.
Curve HH can be either concave or convex, depending on whether \([1-(\beta \theta _{1}+\theta _{4})]/(\beta \theta _{1}+\theta _{3})\gtrless 1\). For illustrative purposes, it is shown as concave in Fig. 8.1. The difference between Cases 1 and 4, of course, is that the slopes of the two curves would be different, depending on the values of ν 3 and θ 3. However, this difference is inconsequential for a qualitative analysis.
- 30.
Note that if ϕ 2 = β then a 12 = 0 and system (8.24) is recursive; the dynamics are in terms of \(\hat {x}_{t}\) only. Then stability requires a 11 = 1 − β + ϕ 1 < 1, or ϕ 1 < β. If ν 3 = 0, then this condition becomes β(ν 1 − 1) < 1 which is always satisfied.
- 31.
A variety of other experiments could also be conducted, such as for instance a change in parental time allocated between the health and education needs of their children, that is, a change in χ. These experiments are left to the interested reader.
- 32.
The focus on growth could be because the economy considered is poor and the priority is to raise living standards. More formally, differences between the growth- and welfare-maximizing solutions can lead to relatively small differences in growth rates, and possibly welfare levels. See Misch et al. (2013) for a discussion.
- 33.
Some other contributions which focus on knowledge accumulation, such as Blackburn and Cipriani (2002), Cervellati and Sunde (2005), Castelló-Climent and Doménech (2008), for instance, have assumed that life expectancy is related to education. This can be justified by arguing that, as noted earlier, improved knowledge can lead to changes in lifestyle that may translate into better health outcomes. In the present setting, a more general approach, of course, would be to consider jointly education and health status as determinants of life expectancy. However, this would complicate significantly the analysis and would detract from the main contribution of this chapter.
- 34.
A simple functional form for f could be the exponential function, that is, \(p_{t}=1-1/\exp (h_{t})\).
- 35.
As noted in Agénor (2015), in the model health status can be interpreted as a broad measure of health, such as the body mass index (BMI). From that perspective, the thresholds h L and h H can be thought of as the lower and upper bounds of the BMI Chart, which are commonly used to measure the ranges for underweight (up to h L in the model), healthy weight (between h L and h H), and overweightandobesity (above h H), based on a person’s height. The last threshold is, in practice, further decomposed into separate thresholds for overweight and obesity but this does not matter from the perspective of this discussion.
- 36.
Based on the previous discussion, if the increase in public spending on health is financed by a cut in spending on education, the possibility of an adverse effect on growth would be magnified.
- 37.
Hazan and Zoabi (2006), however, focus on private expenditure on health and education, not public spending.
References
Agénor, Pierre-Richard, “Schooling and Public Capital in a Model of Endogenous Growth,” Economica, 78 (January 2011), 108–32.
——, Public Capital, Growth and Welfare, Princeton University Press (Princeton, New Jersey: 2012).
——, “Public Capital, Health Persistence and Poverty Traps,” Journal of Economics, 115 (June 2015), 103–31.
Agénor, Pierre-Richard, Otaviano Canuto, and Luiz Pereira da Silva, “On Gender and Growth: The Role of Intergenerational Health Externalities and Women’s Occupational Constraints,” Structural Change and Economic Dynamics, 30 (September 2014), 132–47.
Ahmed, Akhter, and Mary Arends-Kuenning, “Do Crowded Classrooms Crowd Out Learning? Evidence from the Food for Education Program in Bangladesh,” World Development, 34 (April 2006), 665–84.
Altindag, Duha, Colin Cannonier, and Naci Mocan, “The Impact of Education on Health Knowledge,” Economics of Education Review, 30 (November 2011), 792–812.
Ampaabeng, Samuel K., and Chih Ming Tan, “The Long-Term Cognitive Consequences of Early Childhood Malnutrition: The Case of Famine in Ghana,” Journal of Health Economics, 32 (December 2013), 1013–27.
Arndt, Channing, “HIV/AIDS, Human Capital, and Economic Growth Prospects for Mozambique,” Journal of Policy Modeling, 28 (July 2006), 477–489.
Aslam, Monazza, and Geeta G. Kingdon, “Parental Education and Child Health—Under- standing the Pathways of Impact in Pakistan,” World Development, 40 (October 2012), 2014–32.
Baldacci, Emanuele, Benedict Clements, Sanjeev Gupta, and Qiang Cui, “Social Spending, Human Capital, and Growth in Developing Countries: Implications for Achieving the MDGs,” Working Paper No. 04/217, International Monetary Fund (November 2004).
Behrman, Jere R., “The Impact of Health and Nutrition on Education,” World Bank Research Observer, 11 (February 1996), 23–37.
——, “Early Life Nutrition and Subsequent Education, Health, Wage, and Intergenerational Effects,” in Health and Growth, ed. by Michael Spence and Maureen Lewis, World Bank (Washington, D.C.: 2009).
Bell, Clive, Shantayanan Devarajan, and Hans Gersbach, “The Long-Run Economic Costs of AIDS: A Model with an Application to South Africa,” World Bank Economic Review, 20 (March 2006), 55–89.
Benos, Nikos, and Stefania Zotou, “Education and Economic Growth: A Meta-Regression Analysis,” World Development, 64 (December 2014), 669–89.
Bharadwaj, Prashant, Katrine V. Løken, and Christopher Neilson, “Early Life Health Interventions and Academic Achievement,” American Economic Review, 103 (August 2013), 1862–91.
Blackburn. Keith, and Giam P. Cipriani, “A Model of Longevity and Growth,” Journal of Economic Dynamics and Control,” 26 (February 2002), 187–204.
Bleakley, Hoyt, “Disease and Development: Evidence from Hookworm Eradication in the American South,” Quarterly Journal of Economics, 122 (February 2007), 73–117.
——, “Malaria Eradication in the Americas: A Retrospective Analysis of Childhood Exposure,” American Economic Journal: Applied Economics, 2 (April 2010a), 1–45.
——, “Health, Human Capital, and Development,” Annual Review of Economics, 2 (September 2010b), 283–310.
Bloom, David E., David Canning, and Mark Weston, “The Value of Vaccination,” World Economics, 6 (July 2005), 1–13.
Bloom, David, and David Canning, “Schooling, Health, and Economic Growth: Reconciling the Micro and Macro Evidence,” unpublished, Harvard School of Public Health (February 2005).
Bloom, David E., and David Canning, “Population Health and Economic Growth,” in Health and Growth, ed. by Michael Spence and Maureen Lewis, World Bank (Washington DC: 2009).
Breierova, Lucia, and Esther Duflo, “The Impact of Education on Fertility and Child Mortality: Do Fathers really Matter less than Mothers?” Working Paper No. 10513, National Bureau of Economic Research (May 2004).
Bundy, Donald, et al., “School-Based Health and Nutrition Programs,” in Disease Control Priorities in Developing Countries, ed. by Dean Jamison et al., 2nd ed., Oxford University Press (New York: 2006).
Case, Anne, Angela Fertig, and Christina Paxson, “The Lasting Impact of Childhood Health and Circumstance,” Journal of Health Economics, 24 (March 2005), 365–89.
Castelló-Climent, Amparo, and Rafael Doménech, “Human Capital Inequality, Life Expectancy and Economic Growth,” Economic Journal, 118 (April 2008), 653–77.
Cervellati, Matteo, and Uwe Sunde, “Human Capital, Life Expectancy, and the Process of Economic Development,” American Economic Review, 95 (December 2005), 1653–72.
Chou, Shin-Yi, Jin-Tan Liu, Michael Grossman, and Ted Joyce, “Parental Education and Child Health: Evidence from a Natural Experiment in Taiwan,” American Economic Journal: Applied Economics, 2 (January 2010), 33–61.
Corrigan, Paul, Gerhard Glomm, and Fabio Mendez, “AIDS Crisis and Growth,” Journal of Development Economics, 77 (June 2005), 107–24.
Currie, Janet “Child Health in Developed Countries,” in Handbook of Health Economics, Vol. 1B, ed. by A. Culyer and J. Newhouse, North Holland (Amsterdam: 2000).
——, “Healthy, Wealthy, and Wise: Socioeconomic Status, Poor Health in Childhood, and Human Capital Development,” Journal of Economic Literature, 47 (March 2009) 87–122.
Cutler, David M., Angus Deaton, and Adriana Lleras-Muney, “The Determinants of Mortality,” Journal of Economic Perspectives, 20 (June 2006), 97–120.
Cutler, David M., and Adriana Lleras-Muney, “Education and Health: Evaluating Theories and Evidence,” in Making Americans Healthier: Social and Economic Policy as Health Policy, ed. by J. House, R. Schoeni, G. Kaplan, and H. Pollack, Russell Sage Foundation (New York: 2008).
de la Croix, David, and Omar Licandro, “The Child is Father of the Man: Implications for the Demographic Transition,” 123 (March 2013), 236–61.
Field, Erica, Omar Robles, and Maximo Torero, “Iodine Deficiency and Schooling Attainment in Tanzania,” American Economic Journal: Applied Economics, 1 (March 2009), 140–69.
Finlay, Jocelyn, “Endogenous Longevity and Economic Growth,” unpublished, Australian National University (February 2006).
——, “The Role of Health in Economic Development,” PGDA Working Paper No. 21, Harvard School of Public Health (March 2007).
Galor, Oded, and David Mayer-Foulkes, “Food for Thought: Basic Needs and Persistent Educational Inequality,” unpublished, Brown University (June 2004).
Gertler, Paul, and Jenifer Zeitlin, “The Returns to Childhood Investments in terms of Health later in Life,” in Health and Health Care in Asia, ed. by Teh-Wei Hu and H- Cheen, Oxford University Press (Oxford: 1996).
——, “Do Childhood Investments in Education and Nutrition Improve Adult Health in Indonesia?,” in The Economics of Health care in Asia-Pacific Countries, ed. by Teh-Wei Hu, E. Elgar (Cheltenham: 2002).
Glewwe, Paul, “Why Does Mother’s Schooling Raise Child Health in Developing Countries? Evidence from Morocco,” Journal of Human Resources, 34 (March 1999), 124–59.
——, “Schools and Skills in Developing Countries: Education Policies and Socioeconomic Outcomes,” Journal of Economic Literature, 40 (June 2002), 436–82.
Glewwe, Paul, and Edward Miguel, “The Impact of Child Health and Nutrition on Education in Less Developed Countries,” in Handbook of Development Economics, Vol. 4, ed. by T. Paul Schultz and John Strauss, North Holland (Amsterdam: 2008).
Grossman, Michael, and R. Kaestner, “Effects of Education on Health,” in The Social Benefits of Education, ed. by Jere R. Berhman and Nevzer Stacey, University of Michigan Press (Ann Arbor: 1997).
Grossman, Michael, “The Relationship between Health and Schooling,” Nordic Journal of Health Economics, 3 (March 2015), 7–17.
Groot, Wim, and Henriette M. van den Brink, “The Effects of Education on Health,” in Human Capital: Advances in Theory and Evidence, ed. by Joop Hartog and Henriette M. van den Brink, Cambridge University Press (Cambridge: 2007).
Guryan, Jonathan, Erik Hurst, and Melissa Kearney, “Parental Education and Parental Time with Children,” Journal of Economic Perspectives, 22 (June 2008), 23–46.
Hamoudi, Amar, and Nancy Birdsall, “HIV/AIDS and the Accumulation and Utilization of Human Capital in Africa,” in The Macroeconomics of HIV/AIDS, ed. by M. Haacker, International Monetary Fund (Washington, D.C.: 2004).
Hazan, Moshe, and Hosny Zoabi, “Does Longevity Cause Growth? A Theoretical Critique,” Journal of Economic Growth, 11 (December 2006), 363–76.
Jayachandran, Seema, and Adriana Lleras-Muney, “ Life Expectancy and Human Capital Investments: Evidence from Maternal Mortality Declines,” Quarterly Journal of Economics, 124 (February 2009), 349–97.
Keats, Anthony, “Women’s Schooling, Fertility, and Child Health Outcomes: Evidence from Uganda’s Free Primary Education Program,” Journal of Development Economics, 135 (November 2018), 142–59.
Kohler, Iliana, and Beth J. Soldo, “Early Life Events and Health Outcomes in Late Life in Developing Countries—Evidence from the Mexican Health and Aging Study,” unpublished, University of Pennsylvania (March 2004).
Lorentzen, Peter, John McMillan, and Romain Wacziarg, “Death and Development,” Journal of Economic Growth , 13 (June 2008), 81–124.
Maluccio, John A., John Hoddinott, Jere R. Behrman, Reynaldo Martorell, Agnes R. Quisumbing, Aryeh D. Stein, “The Impact of Improving Nutrition during Early Childhood on Education among Guatemalan Adults,” Economic Journal, 119 (April 2009), 734–63.
Mayer-Foulkes, David, “Human Development Traps and Economic Growth,” in Health and Economic Growth: Findings and Policy Implications, ed. by Guillem López-Casasnovas, Berta Rivera and Luis Currais, MIT Press (Boston, Mass.: 2005).
McCarthy, Desmond, Holger Wolf, and Yi Wu, “The Growth Costs of Malaria,” Working Paper No. 7541, National Bureau of Economic Research (February 2000).
McGuire, James W., “Basic Health Care Provision and Under-5 Mortality: A Cross-National Study of Developing Countries,” World Development (March 2006), 405–25.
Mental Health Foundation, Feeding Minds—The Impact of Food on Mental Health, London (January 2006).
Miguel, Edward, “Health, Education, and Economic Development,” in Health and Economic Growth: Findings and Policy Implications, ed. by Guillem López-Casasnovas, Berta Rivera, and Luis Currais, MIT Press (Cambridge, Mass.: 2005).
Miguel, Edward, and Michael Kremer, “Worms: Identifying Impacts on Education and Health in the Presence of Treatment Externalities,” Econometrica, 72 (January 2004), 159–217.
Misch, Florian, Norman Gemmell, and Richard Kneller, “Growth and Welfare Maximization in Models of Public Finance and Endogenous Growth,” Journal of Public Economic Theory, 15 (December 2013), 939–67.
Mullahy, John, and Stephanie A. Robert, “No Time to Lose: Time Constraints and Physical Activity in the Production of Health,” Review of Economics of the Household, 8 (December 2010), 409–32.
Oreopoulos, Philip, Mark Stabile, Rand Walld, and Leslie Roos, “Short, Medium, and Long-Term Consequences of Poor Infant Health: An Analysis using Siblings and Twins,” Journal of Human Resources, 43 (March 2008), 88–138.
Osang, Thomas, and Jayanta Sarkar, “Endogenous Mortality, Human Capital and Endogenous Growth.” Journal of Macroeconomics, 30 (December 2008), 1423–45.
Paxson, Christina H., and Norbert Schady, “Cognitive Development among Young Children in Ecuador: The Roles of Wealth, Health and Parenting,” Journal of Human Resources, 42 (March 2007), 49–84.
Pelletier, D. L., E. A. Frongillo, J-P. Habicht, “Epidemiologic Evidence for a Potentiating Effect of Malnutrition on Child Mortality,” American Journal of Public Health, 83 (December 2003), 1130–33.
Powdthavee, Nattavudh, and Anna Vignoles, “Mental Health of Parents and Life Satisfaction of Children: A within-Family Analysis of Intergenerational Transmission of Well-being,” Social Indicators Research, 88 (September 2008), pages 397–422.
Ricci, Francesco, and Marios Zachariadis, “Education Externalities on Longevity,” Economica, 80 (July 2013), 404–40.
Salm, Martin, and Daniel Schunk, “The Role of Childhood Health for the Intergenerational Transmission of Human Capital: Evidence from Administrative Data,” IZA Discussion Paper No. 3646 (August 2008).
Schultz, T. Paul, “Productive Benefits of Health: Evidence from Low-Income Countries,” in Health and Economic Growth: Findings and Policy Implications, ed. by Guillem Ló pez-Casasnovas, Berta Rivera, and Luis Currais, MIT Press (Cambridge, Mass.: 2005).
Silles, Mary A., “The Causal Effect of Education on Health: Evidence from the United Kingdom,” Economics of Education Review, 28 (February 2009), 122–28.
Smith, James P., “The Impact of Childhood Health on Adult Labor Market Outcomes,” Review of Economics and Statistics, 91 (August 2009), 478–89.
Smith, Lisa C., and Lawrence Haddad, “Explaining Child Malnutrition in Developing Countries: A Cross-Country Analysis,” Research Report No. 111, International Food Policy Research Institute (May 2000).
Soares, Rodrigo R., “The Effect of Longevity on Schooling and Fertility: Evidence from the Brazilian Demographic and Health Survey,” Journal of Population Economics, 19 (February 2006), 71–97.
Summers, Lawrence H., Investing in All the People: Educating Women in Developing Countries, World Bank (Washington, D.C.: 1994).
Tamura, Robert, “Human Capital and Economic Development,” Journal of Development Economics, 79 (January 2006), 26–72.
Tang, Kam Ki, and Jie Zhang, “Health, Education, and Life Cycle Savings in the Development Process,” Economic Inquiry, 45 (July 2007), 615–30.
Taylor, Beck A., Eric Dearing, and Kathleen McCartney, “Incomes and Outcomes in Early Childhood,” Journal of Human Resources, 39 (December 2004), 980–1007.
Thuilliez, Josselin, “Malaria and Primary Education: A Cross-country Analysis on Repetition and Completion Rates,” Revue d’économie du développement , 2 (December 2009), 127–57.
United Nations, Accelerating Gender Equality and Women’s Empowerment in Africa, Africa Human Development Report (New York: 2016).
Wagstaff, Adam, and Mariam Claeson, The Millennium Development Goals for Health: Rising to the Challenges, World Bank (Washington DC: 2004).
Zhang, Junsen, and Jie Zhang, “The Effect of Life Expectancy on Fertility, Saving, Schooling and Economic Growth: Theory and Evidence,” Scandinavian Journal of Economics, 107 (March 2005), 45–66.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 The Author(s)
About this chapter

Cite this chapter
Agénor, PR. (2019). Health and Knowledge Externalities: Implications for Growth and Public Policy. In: Bucci, A., Prettner, K., Prskawetz, A. (eds) Human Capital and Economic Growth. Palgrave Macmillan, Cham. https://doi.org/10.1007/978-3-030-21599-6_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-21599-6_8
Published:
Publisher Name: Palgrave Macmillan, Cham
Print ISBN: 978-3-030-21598-9
Online ISBN: 978-3-030-21599-6
eBook Packages: Economics and FinanceEconomics and Finance (R0)