
Abstract
As of 2015, HIV ranked third globally among the top causes of disability-adjusted life years (DALYs) lost in children and teens aged 10–14 years and tenth among adolescents aged 15–19. Pediatricians and other primary care providers play a crucial role in the detection, treatment, and prevention of HIV. Early diagnosis can reduce secondary HIV transmission and facilitate improved clinical outcomes through early initiation of antiretroviral therapy (ART). Testing should begin with the latest generation of FDA-approved antigen/antibody immunoassays. HIV-infected individuals should receive timely ART following a thorough baseline evaluation, laboratory testing, and social history. A number of evidence-based interventions exist to prevent the transmission of HIV including condom use and preexposure prophylaxis. Providers should be mindful of the many contextual barriers that disproportionately impact HIV-infected individuals, such as housing instability and food insecurity. Individuals with low socioeconomic standing, racial minorities, and sexual minorities are particularly vulnerable.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Human immunodeficiency virus
- HIV
- Sexual and gender minorities
- Adolescents
- Young adults
- Antiretroviral therapy
- ART
- Treatment as prevention
- Preexposure prophylaxis
- PrEP
An 18-year-old-male patient presents to the emergency department with fever, cough, and dyspnea that progressed over the course of 2 weeks. He describes feeling short of breath after attempting routine activities, such as climbing a flight of stairs. On further questioning, he reports receiving an HIV diagnosis at an urgent care clinic 2 years prior. Due to feeling “misunderstood” by his provider, he was lost to follow-up and has never received any treatment for his HIV infection. He denies any sexual activity since his diagnosis. Prior to his diagnosis, he engaged in receptive anal intercourse monogamously with his partner of 2 years, who was the first person he ever had sex with.
On physical examination, he has a temperature of 38.1 C. He is visibly tachypneic, and his pulmonary exam reveals rales and rhonchi on auscultation. Examination of his oropharynx is notable for white, adherent plaques on his palate and buccal mucosa.
A 4th-generation HIV antigen/antibody test is reported as positive. Subsequent laboratory testing results indicate a CD4+ T-cell count of 13 cells/μL and an HIV RNA (viral load) of over one million copies/μL. The plasma level of 1-3-beta-d-glucan – a component of the cell wall of the fungus Pneumocystis jirovecii – is elevated. Chest radiography demonstrates a diffuse, bilateral interstitial pulmonary infiltrate. The patient is diagnosed with AIDS and started on treatment for Pneumocystis pneumonia (PCP).
Questions
-
What are the presenting symptoms of acute and advanced HIV infection?
-
Which laboratory studies should be ordered prior to prescribing antiretroviral medications?
-
What are the major opportunistic infections in patients with advanced AIDS?
-
Why are young black men who have sex with men (YBMSM) at a disproportionately high risk for HIV infection?
Epidemiology
The human immunodeficiency virus (HIV) accounts for a substantial proportion of the global burden of disease among adolescents and young adults aged 10–24. As of 2015, HIV ranked third globally among the top causes of disability-adjusted life years (DALYs) lost in children and teens aged 10–14 years, tenth among adolescents aged 15–19, and seventh among youth aged 20–24 [1]. The prevalence of HIV infection among youth in the United States (US) is also high. As of 2013, there were 6537 HIV-positive adolescents (aged 13–19) and 32,980 HIV-positive young adults (aged 20–24) living in the United States [2]. Adolescents and young adults in the United States represent a uniquely challenging group to provide care for, compared with older HIV-infected adults [3]. Data from 2012 showed that only 66% of HIV-infected youth aged 13–24 were engaged in care within a month of diagnosis, ranking lowest out of any age group in this domain [4]. Adolescents and young adults are also least likely to maintain an undetectable HIV viral load (which is the ultimate goal of therapy with HIV medications), with data from 2012 indicating that only 38.0% of HIV-infected youth had reached this goal [4].
Racial disparities in HIV prevalence and incidence also exist among adolescents and young adults. For example, in 2014, the incidence of HIV was 20 times greater in black adolescents as compared to white adolescents [2]. This discrepancy is even more pronounced with the rate of AIDS diagnoses, which, in the same year, was 41 times greater in the former group [2].
The relative importance of different modes of HIV transmission varies by age group, gender, and sexual behaviors. Among 3766 HIV-positive young adolescent males (aged 13–19) in 2013, 49% were infected through male-male sexual contact, 43% through vertical [perinatal] transmission, and 2% through heterosexual contact. In contrast, among the 26,008 HIV-positive young adult males (aged 20–24), 85% were infected by male-male sexual contact, 7% vertically, and 3% by heterosexual intercourse. A smaller number of females in both age categories were infected: 2770 15–19-year-olds and 6972 20–24-year-olds, respectively. While the majority of female 15–19-year-olds were infected by vertical transmission from their mothers at birth (69%), 63% of female 20–24-year-old young adults were infected by heterosexual contact [2].
Microbiology and Pathophysiology
The HIV Life Cycle
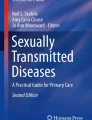
HIV is a retrovirus that impairs the immune system by primarily infecting CD4+ helper T-cells and “hijacking” intracellular DNA [5]. The HIV life cycle can be divided into seven discrete stages (Fig. 17.1). (1) The viral glycoprotein 120 (gp120) binds to the CD4 receptor on activated CD4+ T lymphocytes or other cells that express this ligand, such as resting CD4+ T cells, monocytes, macrophages, and dendritic cells. This induces a conformational change in the virus such that it can bind to a second co-receptor: either the CC-chemokine receptor 5 CCR5, most often, or to the CXC-chemokine receptor 4 (CXCR4) [5,6,7]. (2) Following co-receptor binding, viral gp41 protein becomes exposed on the surface of the virus, which facilitates fusion, whereby the virion and target cell are brought closer together. Fusion allows a “pre-integration complex,” comprised of viral proteins, enzymes, and RNA, to be released into the cytoplasm [5]. (3) The third step is reverse transcription: i n the cytoplasm of the T-helper cell, HIV reverse transcriptase converts single-stranded HIV RNA into double-stranded DNA. (4) The newly synthesized DNA then integrates into the host genome using the viral enzyme integrase [5, 7]. (5) Replication of viral DNA occurs when host enzymes transcribe viral mRNA and translate viral proenzyme. (6) Following glycosylation, phosphorylation, and cleavage of the proenzyme, the newly synthesized HIV proteins and RNA migrate to the T-cell surface in a step called assembly. (7) The final step, budding , involves the release of HIV from host cells, typically at lipid rafts along the cell membrane [5, 7].

The HIV life cycle and associated antiretroviral medication targets. (Reprinted with permission from the National Institutes of Health (NIH [120]))
Acute HIV Infection
HIV transmission occurs at mucosal membranes through infection by a founder virus that replicates via the pathways described above [6, 8]. Acute HIV infection commonly presents with nonspecific clinical manifestations such as fever, headache, and malaise. Physical examination may reveal tachycardia and lymphadenopathy. Patients may also present with diffuse maculopapular skin rash, pharyngitis, myalgias, night sweats, arthralgias, and/or diarrhea [9,10,11].
The symptoms of acute HIV infection correlate closely with viral dynamics. Acute infection is characterized by an initial surge in plasma HIV RNA, and clinical manifestations are most salient at the peak of viremia [10, 12]. However, these symptoms are transient and subside once the host’s innate and adaptive immune responses become activated, which results in a drop in viral load to a newly defined “set point,” typically established within 18–42 days from when viral RNA is first detectable [10]. This set point is an important prognostic indicator, with higher set points being predictive of rapid progression to AIDS [12,13,14,15].
Immune Response and Dysfunction
While CD4+ helper T-cell and CD8+ T-lymphocyte counts maintain homeostasis during initial infection, peak viremia during acute infection corresponds with an immunophenotypical shift associated with a precipitous decrease in CD4+ T cells [10, 16,17,18]. The marked reduction in CD4+ cells and subsequent impairment of the immune system is a hallmark of HIV infection [6]. While there is some reconstitution and recovery of CD4+ cells following this initial decrease during acute infection, in the absence of treatment with antiretroviral therapy (ART), this number continues to decrease over a variable time period [6]. Additionally, while CD8+ T cells may be able to initially reduce viremia, they are incapable of clearing the infection due to viral evasion of host defenses (including development of escape mutants as well as intracellular persistence within viral reservoirs) [19, 20]. These reservoirs develop following latent infection of resting memory T cells including those within lymphoid tissue, the central nervous system (CNS), and the gastrointestinal (GI) tract [21,22,23,24], allowing HIV to persist in a dormant state even once the patient has been started on effective ART.
Other correlates of adaptive immunity include the evolution of humoral immune responses; however, the virus quickly evolves to evade the humoral immune system through escape mutants [25]. The production of IgM and IgG antibodies to HIV serve as useful serological markers for the detection of HIV infection.
Chronic Inflammation and Progression to AIDS
While the gradual depletion of CD4+ cells is more commonly asymptomatic, HIV infection results in a state of chronic inflammation and immune activation, which in turn is associated with depletion of CD4+ cells in the GI tract – an insult which only minimally recovers with effective ART [6, 26]. This GI tract depletion includes loss of T-helper 17 as well as mucosal-associated invariant T cells, both of which play important roles fighting bacterial enteropathogens [27, 28]. The resulting increased gut permeability to bacterial products (e.g., lipopolysaccharides) exacerbates immune activation [29] and is associated with a number of adverse health outcomes, including cardiovascular disease and malignancy [30,31,32,33,34].
The vast majority of untreated patients will eventually progress to acquired immunodeficiency syndrome (AIDS), also referred to as Stage 3 HIV infection by the Centers for Disease Control and Prevention (CDC). AIDS is defined by a CD4 count below 200 cells/μL or a development of an AIDS-defining illness [35, 36]. The immunocompromised state resulting from CD4 depletion below 200 cells/μL predisposes HIV-infected individuals to a host of characteristic opportunistic infections and malignancies [36]. A detailed list of these AIDS-defining illnesses is listed in Table 17.1.
Diagnostic Testing
HIV diagnostic testing has become significantly more accurate and timely over the past two decades. There are now four generations of immunoassays used to detect immune response to HIV, in addition to nucleic acid testing (NAT) that can directly detect viral genetic material [37,38,39]. Each new generation of tests detects HIV earlier in infection compared to the older generation(s). This sequential reactivity of HIV assays has allowed for the designation of four distinct laboratory stages: (1) the eclipse period, (2) acute HIV infection, (3) the seroconversion window, and (4) established HIV infection (Fig. 17.2) [40,41,42,43,44]. Early detection of HIV is critical for both individual and public health outcomes. Early diagnosis can reduce secondary HIV transmission from acutely infected individuals, who have high levels of viremia (making them more likely to transmit the virus) and may not know how to reduce their risk behaviors [45, 46]. Earlier initiation of ART also results in significantly improved clinical outcomes in infected subjects [47].

Sequence of appearance of laboratory markers for HIV-1 infection. (Reprinted with permission from the Centers for Disease Control and Prevention (Branson et al. [39]))
In the eclipse period, there are no assays that can reliably detect HIV infection. Acute HIV infection, characterized by a spike in viral RNA, is detectable by NAT within 10 days of infection [38, 48,49,50,51]. The seroconversion window refers to an interval between initial HIV infection and when an antibody or antibody/antigen combination immunoassay can reliably detect infection. The timing of this window varies slightly by the type of assay [41]. For instance, fourth-generation antigen/antibody immunoassays can detect HIV-1 p24 antigen 4–10 days after HIV-1 RNA becomes detectable by NAT [43]. Third (as well as fourth)-generation immunoassays detect IgM antibodies 10–13 days after the appearance of viral RNA [39, 41,42,43, 52]. Older immunoassays detect IgG during the interval of established infection, 18–38 days following the appearance of viral RNA [39, 41,42,43, 53]. New guidelines by the Centers for Disease Control and Prevention (CDC) and the Association of Public Health Laboratories (APHL) incorporate the use of newer generation antigen/antibody combination immunoassays in combination with NAT [39]. This algorithm (Fig. 17.3) has been shown to be more effective at detecting acute and newly established infections compared to older algorithms using Western blot testing [39]. Individuals with suspected HIV infection should be tested with the latest generation FDA-approved two-step antigen/antibody immunoassays. A positive test could be indicative of established HIV-1 or HIV-2 infection or an acute HIV-1 infection [39]. The second step distinguishes between HIV-1 and HIV-2 through further testing with antibody immunoassays specific to the two different strains [39]. (Note: HIV-2 is a strain of HIV that is highly unusual in the United States – there are some subtle differences in natural history and treatment recommendations that are beyond the scope of this chapter, which is focused on HIV-1 infection). If this step yields indeterminate or negative results, nucleic acid testing can differentiate between acute and established HIV-1 infection or, if negative, indicate false positivity of the initial antigen/antibody immunoassay used at the point of care [39].

Recommended laboratory HIV testing algorithm for serum or plasma specimens. (Reprinted with permission from the Centers for Disease Control and Prevention (Branson et al. [39]))
Treatment
Antiretroviral therapy (ART) has markedly improved in efficacy and tolerability since the implementation of combination therapy in 1996, resulting in substantial declines in HIV and antiretroviral (ARV)-related morbidity and mortality [47, 54]. ART essentially transformed HIV into a chronic condition, so that patients who are able to maintain medication adherence have a life expectancy comparable to that of the general population [55, 56]. Here we discuss treatment guidelines from the Department of Health and Human Services that are informed by expert opinion and scientific evidence [57]. While we summarize some principles of managing HIV-infected patients, it should be noted that HIV management is a complex and nuanced process. Studies have shown that HIV-infected subjects have better clinical outcomes when they receive care from clinicians with expertise and training in HIV medicine (i.e., those who are actively treating at least 20 patients with HIV). Whenever possible, patients should be referred to receive care from providers experienced in HIV/AIDS care [58,59,60,61,62].
Ideally, all HIV-infected individuals should receive ART as soon as baseline laboratory tests have been obtained and an assessment has been made regarding the patient’s barriers and facilitators to medication adherence. Baseline evaluation should include a complete medical history, physical examination, blood draw for laboratory investigations, and counseling about the pathophysiology, clinical course, and treatments of HIV [57]. The two most important lab tests are to assess two important markers: CD4+ T-lymphocyte count and plasma levels of HIV RNA or HIV viral load [15, 57, 63]. The CD4+ T-cell count gives an estimate of the level of immunocompromised (or lack thereof). HIV-uninfected individuals typically have CD4+ values ranging between approximately 450 and 1000 – in patients with HIV, a CD4+ count under 200 cells/μL indicates severe immunocompromised and a need to prescribe prophylaxis against opportunistic infections [64]. The viral load, in contrast, is a marker of how well a patient is responding to ART. The goal of treatment is to achieve an undetectable level of viremia (although it should be noted that the limit of detection varies by assay and can range from <20 to 75 copies of virus/μL) [57]. A viral load of greater than 200 copies/μL is suggestive of virologic failure [65]. This could be due to the development of viral resistance to the ART regimen in use, nonadherence to medications, or both. Both CD4 counts and viral load testing are monitored during clinic appointments, with viral load being the most important marker of continued adherence and medication efficacy [57].
Patients should also undergo baseline drug resistance testing and genetic screening for the HLA B∗5701 allele. Drug resistance testing helps guide which ARVs are active against the patient’s virus and has been shown to improve virological outcomes when incorporated into HIV-management decision-making [57, 66]. In most patients, initiation of ART should be delayed until receiving results of the resistance testing [57, 67]. However, in HIV-infected pregnant women and patients presenting with acute infection, it is recommended to initiate therapy immediately and adjust the regimen later, as necessary [57]. Clinicians can order either genotypic or phenotypic assays to assess for resistance, both of which have been shown to be effective in guiding selection of ARVs [68]. Genotypic assays involve HIV-1 gene sequencing, which allows for detection of mutations that confer resistance [57, 67]. Phenotypic assays, conversely, are culture-based and measure the ability of HIV to grow at different concentrations of ARVs [57, 67]. It should be noted that the absence of detected resistance on the baseline evaluation does not mean that no viral resistance is present. The wild-type (non-mutated) version of the HIV virus is more genetically fit and tends to overgrow other strains in the absence of selective pressure induced by medications. Therefore, those patients whose viral loads are not suppressed within the expected time frame (1–2 months) should have repeat resistance testing done while on ART. Finally, patients should be screened for HLA B∗5701 allele, prior to initiating ART that contains the ARV abacavir, which can cause a life-threatening hypersensitivity reaction in individuals who are HLAB∗5701 positive [69,70,71].
The main goals of therapy are to suppress viremia beneath the level of detection, restore immunologic function, reduce long-term HIV- and ARV-associated morbidity, and prevent onward secondary HIV transmission [57]. This requires selection of an ARV regimen that the virus is susceptible to and that the patient will be able to adhere to. To guide this process, important considerations include drug interactions, side effects, susceptibility and resistance, and “pill burden,” which vary widely across different ARV classes [57]. The current standard is to prescribe ART comprised of three different ARVs from two different classes. ARV classes include nucleos(t)ide reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), protease inhibitors (PIs), integrase strand transfer inhibitors (INSTIs), and fusion inhibitors [57]. A schematic of where these medications intervene in the HIV life cycle is depicted in Fig. 17.1. The most commonly prescribed regimens involve two NRTIs with a medication from a second class [57]. Figure 17.4 lists all currently available medications (at the time of this writing), their major side effects, and special considerations unique to these ARVs. Of note, ARV regimens and recommendations are frequently changing; we recommend consulting the Department of Health and Human Services guidelines (https://aidsinfo.nih.gov/guidelines) for the most up-to-date recommendations.

Classes of antiretroviral medications for the treatment of HIV, including beneficial treatment considerations (green boxes) and major side effects (red boxes)
Early initiation of ART is strongly recommended in pregnant women, in order to reduce the risk of vertical transmission. Most ARVs have not been associated with teratogenic effects beyond those observed in the general population [72], although there are concerns related to a higher rate of preterm delivery and low birth weight infants born to HIV-infected mothers [72, 73]. Current guidelines recommend standard combination ART (i.e., 2 NRTIs with a ritonavir-boosted PI, INSTI, or NNRTI). Previously, efavirenz was not recommended during pregnancy due to concern for increased rates of central nervous system anomalies in the fetus – this warning has largely been discredited, and use of efavirenz is no longer restricted based on sex or pregnancy [74]. Recently, researchers in Botswana noted a higher rate of neural tube defects among children born to women who were taking dolutegravir at the time of conception – this was a small observation of only four infants but represented a significant deviation from the expected rate [75]. Further study is warranted to determine the implications of this observation, and there has been no change in official recommendations at the time of this writing; however, clinicians may want to consider other options besides dolutegravir for young women who are planning on becoming pregnant (or who are of childbearing age but not being prescribed effective contraception). See Fig. 17.4 for ART recommendations during pregnancy.
Prevention
A number of evidence-based behavioral and biomedical interventions exist to prevent the transmission and acquisition of HIV, including educational programs, male and female condoms, male circumcision, pre- and postexposure prophylaxis, and treatment as prevention. Here we discuss the efficacy and effectiveness of some of these interventions in adolescents and young adults, as well as their limitations.
Sexual Education
Comprehensive sexual education is an important component of reducing sexual risk behaviors in adolescents. While there is conflicting evidence, there is general consensus that “risk reduction” programs [i.e., programs that teach safe sexual practices] are more effective at decreasing risky behaviors compared to “risk avoidance” programs [i.e., programs that advocate for delaying initiation of sexual activity] [76].
Risk reduction programs typically target knowledge, perceptions of risk, values about sexuality, self-efficacy to refuse sexual activity, communication with parents and other adults, and self-efficacy to obtain and/or use condoms. They have been shown to decrease the average number of sexual partners, increase the use of condoms, and reduce the incidence of HIV transmission among adolescents [76, 77]. While some studies have shown that abstinence education may result in safer sexual practices, the evidence base is lacking [78].
In practice, the implementation of sexual education curricula varies across the United States. The majority of US schools do not teach all of the content recommended by the CDC [79]. High-risk populations may be particularly disadvantaged by this. For instance, young MSM engaging in risky sexual behaviors have reported that the education they received in school catered exclusively to heterosexual partnerships. This lack of comprehensive sexual education may undermine efforts to reduce in the incidence of HIV infection [80]. Medical providers can therefore play a critically important role in sexual education that is not being provided in schools. Studies have shown that even single-session risk reduction interventions are significantly associated with decreased unprotected sex acts and a decreased risk for STI infection [81].
Male and Female Condoms
The efficacy of male condoms vary depending on the type of sexual activity and are contingent on their consistent use. Among heterosexuals engaging in penetrative vaginal intercourse, consistent use of condoms (defined as use of condoms every time sex is initiated) reduces the risk of HIV transmission by as much as 80% [82]. While the evidence is lacking, condoms appear to be less effective at preventing HIV transmission during anal intercourse. Condom breakage and slippage are reported frequently by young MSM and associated with STI transmission events [83]. A common practice, especially among black MSM, is to use oil-based and other hyperosmolar lubricants in conjunction with condoms. These have been linked to decreased strength of condoms as well as epithelial damage in the rectum, which in turn may increase the risk of HIV transmission and acquisition [83,84,85]. Lastly female condoms have been shown to be just as efficacious and to confer just as much protection from STIs as male condoms among heterosexuals during penetrative vaginal sex [86].
Biomedical and Surgical Interventions
A number of biomedical and surgical interventions have been shown to be effective at reducing the risk of HIV transmission and acquisition. These include male circumcision, which has been shown to reduce the risk of HIV acquisition by 38–66% over a 24-month period among males specifically during heterosexual sex [87]. Circumcision may also be protective among MSM engaging in insertive anal sex; however, data are limited, and the benefits are especially unclear for receptive partners [88].
Preexposure prophylaxis (PrEP) with tenofovir-emtricitabine (TDF-FTC) has been shown to reduce the risk of HIV acquisition in MSM, serodiscordant couples, and among other high-risk populations [89]. At the time of this writing, TDF-FTC (which consists of two active drugs against HIV, not a complete ART regimen) is the only approved regimen for PrEP – it requires patients to take one pill, once daily as a method for preventing HIV acquisition. CDC guidelines are available and recommend consideration of PrEP for HIV-negative MSM (including behaviorally bisexual men) who report any unprotected anal intercourse in the past 6 months (outside of a monogamous relationship with a confirmed HIV-negative partner) or any bacterial STI in the last 6 months. Uptake of PrEP has been much lower for heterosexual men and women, but it should be noted that guidelines also recommend considering PrEP for heterosexual individuals who are sexually active (within the past 6 months) and are diagnosed with bacterial STI within the last 6 months OR report infrequent condom use with partners who are at risk for HIV or known to be HIV-positive [90]. As of May 2018, the US Food and Drug Administration has expanded approval to include high-risk adolescents including those under 18 years of age (provided they weigh at least 35 kg) [91]. Of note, however, the study that led to this approval did demonstrate low rates of adherence to PrEP, suggesting that intensive adherence counseling and monitoring are warranted when prescribing PrEP in this youth population [92]. Prescribing of PrEP requires close follow-up with regular STI and HIV testing, as well as monitoring of renal function (which can be adversely impacted by tenofovir). For more guidance about PrEP, clinicians can refer to the CDC guidelines (available online: https://www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2017.pdf) and/or call the National Clinicians Consultation Center PrEPline at 855-448-7737.
Postexposure prophylaxis (PEP) can also be considered for adolescents and young adults after a high-risk exposure. Non-occupational PEP, or nPEP, encompasses sexual exposures that would be more likely than occupational exposures (i.e., needlestick injuries) in the adolescent population. Following exposure to an individual known or thought to be HIV-infected, persons being considered for nPEP must be tested for HIV – however; dependent on the level of concern for transmission and rapidity of available testing modalities, one does not need to wait for results to start a patient on nPEP [93]. In fact, PEP should be initiated within 72 hours of exposure and discontinued if the potential source of infection is determined to be HIV-negative [93]. nPEP is not recommended when the exposure occurred greater than 72 hours prior to presentation. The CDC currently recommends tenofovir-emtricitabine once daily plus raltegravir twice daily OR dolutegravir once daily or alternatively tenofovir-emtricitabine once daily with ritonavir and darunavir once daily – in contrast to PrEP, these are complete ART regimens that are also recommended for HIV-positive individuals [93]. Receipt of one or more courses of nPEP within a year should lead a clinician to consider prescribing the patient daily PrEP as opposed to multiple 28-day courses of nPEP. Additional information is available in the CDC PEP guidelines (available online: https://www.cdc.gov/hiv/pdf/programresources/cdc-hiv-npep-guidelines.pdf), and consultative assistance is also available from the National Clinicians Consultation Center PEPline at 888-448-4911.
Finally, the single most efficacious form of biomedical HIV prevention is what is referred to as treatment as prevention (TasP). TasP refers to the now well-supported idea that effective ARV treatment associated with viral suppression prevents further viral transmission. A number of large studies have shown that early (as opposed to delayed) initiation of ART with subsequent viral suppression is highly effective at preventing secondary HIV transmission among serodiscordant partners, including heterosexuals as well as MSM [94,95,96]. As an extension of this idea, the risk of perinatal transmission among HIV-infected women giving birth has also been shown to be low – 0.09–0.4% in virologically suppressed mothers who were effectively treated with ART for greater than 4 weeks [97, 98]. The risk of HIV transmission is particularly low for virologically suppressed mothers who initiate care prior to conception [99]. Based on this strong base of scientific evidence, the CDC has endorsed an educational campaign entitled “U=U” or “Undetectable = Untransmittable” to convey to the public the low risk of HIV transmission from individuals who are regularly engaged in care and adherent to their medications. In summary, these data provide support for an encouraging message that clinicians can pass on to their patients with respect to future sexual encounters: although HIV disclosure is still advised and condom use is still recommended to prevent other STIs, patients who maintain an undetectable viral load can feel confident that they are not transmitting HIV to their sexual partners.
Special Considerations
HIV-infected individuals are subject to a number of contextual and socioeconomic factors that warrant consideration by clinicians. Low socioeconomic standing (SES) is significantly associated with higher HIV diagnosis rates in low-income young MSM and across different racial groups [100, 101]. HIV/AIDS also discriminates spatially, such that AIDS prevalence is significantly and independently associated with neighborhood disadvantage, even after controlling for race [102]. HIV-infected persons also have lower survival rates if they live in low-income areas [103]. Other important contextual factors include housing stability and food insecurity. Unstable housing and homelessness among HIV-infected individuals including youth have been linked to riskier sex behaviors such as an increased number of partners and decreased condom use [104,105,106,107]. Similarly, food insecurity among HIV-positive individuals has been linked to a number of risk behaviors, including transactional sex and ARV and medical appointment non-adherence [108,109,110,111]. It is critical for clinicians to adapt treatment plans to meet unique individual needs and to work with patients to address contextual barriers that adversely affect treatment outcomes.
It is also critical for clinicians to understand the role of stigma and how this can affect medical care. Stigma in HIV-infected individuals is a cause for delayed seeking of medical care and ART and medical appointment nonadherence [112,113,114]. Patients have disengaged from care when they felt that their providers were not listening to their concerns or appeared to dislike caring for them [115, 116]. Given that medical adherence is the cornerstone of a successful treatment regimen, it is crucial for clinicians to develop rapport with their patients in a nonjudgmental way.
This brings us to our final point: the relationship between race, sexual orientation, and HIV. Young black MSM have a disproportionately high incidence and prevalence rate of HIV as compared to other demographic and age groups. However, they have also been shown to have less risky behaviors, including a lower number of sex partners and lower instances of unprotected sex compared to young MSM of other races [117]. It is now well established that individual-level factors do not explain the black-white disparity in HIV rates among young MSM. While more investigation is warranted, it is thought that this disparity can be explained at least in part by contextual factors (i.e., the social determinants of health) and engagement of black MSM within a smaller sexual network with a higher background HIV prevalence rate [118, 119].
Case Conclusion
In addition to treatment for Pneumocystis pneumonia, the patient was referred to an outpatient physician specializing in HIV care. His complete blood count, CD4+ T-cell count, HIV viral load, HIV genotype resistance testing, and screening test for HLA0B∗5701 positivity were obtained. Titers were ordered for hepatitis B exposure. He also received a full STI screen including testing for gonorrhea, syphilis, chlamydia, trichomoniasis, and hepatitis A, B, and C.
The majority of the visit was spent discussing the patient’s life circumstances, including an assessment of the patient’s social support, ability to adhere to medications, sexual history, and mental health. The patient reported that he previously disengaged from care after his provider made him feel badly about his sexual behaviors. The patient also admits feeling like he is “not clean” after receiving his diagnosis and explains that as the reason for ceasing sexual activity since his initial diagnosis. He reports that while he is depressed and unemployed, he is currently living with his older sister, who is able to financially support him. The provider explains to the patient that the risk of HIV transmission is negligible in virologically suppressed persons, discusses the complications of HIV and the side effects of treatment, and refers him to a psychiatrist or psychologist and case manager for additional support. The patient is negative for HLA0B∗5701, and titers reveal that he was vaccinated and is now immune to hepatitis B. On a follow-up visit, the HIV provider prescribes a fixed-dose combination pill of ART to be taken once daily and asks him to follow up in 2–4 weeks in order to assess adherence, inquire about any side effects, and re-measure the HIV viral load, looking for a 1–2 log reduction in this value.
References
GBD 2015 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet Lond Engl. 2016;388:1603–58. https://doi.org/10.1016/S0140-6736(16)31460-X.
Centers for Disease Control and Prevention. Diagnoses of HIV infection among adolescents and young adults in the United States and 6 dependent areas, 2010–2014. Atlanta; 2016.
Philbin MM, Tanner AE, DuVal A, Ellen JM, Xu J, Kapogiannis B, Bethel J, Fortenberry JD. HIV testing, care referral, and linkage to care intervals affect time to engagement in Care for Newly Diagnosed HIV-infected adolescents in 15 adolescent medicine clinics in the United States. JAIDS J Acquir Immune Defic Syndr. 2016;72:222–9. https://doi.org/10.1097/QAI.0000000000000958.
Centers for Disease Control and Prevention. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data – United States and 6 dependent areas – 2013. Atlanta; 2015.
Deeks SG, Overbaugh J, Phillips A, Buchbinder S. HIV infection. Nat Rev Dis Primers. 2015;1:15035. https://doi.org/10.1038/nrdp.2015.35.
Maartens G, Celum C, Lewin SR. HIV infection: epidemiology, pathogenesis, treatment, and prevention. Lancet Lond Engl. 2014;384:258–71. https://doi.org/10.1016/S0140-6736(14)60164-1.
Fauci AS, Lane HC. Chapter 189. Human immunodeficiency virus disease: AIDS and related disorders. In: Harrisons Principles Internal Medicine. 18th ed. New York: McGraw-Hill Education; 2012.
Cooper A, García M, Petrovas C, Yamamoto T, Koup RA, Nabel GJ. HIV-1 causes CD4 cell death through DNA-dependent protein kinase during viral integration. Nature. 2013;498:376–9. https://doi.org/10.1038/nature12274.
Robb ML, Ananworanich J. Lessons from acute HIV infection. Curr Opin HIV AIDS. 2016;11:555–60. https://doi.org/10.1097/COH.0000000000000316.
Robb ML, Eller LA, Kibuuka H, Rono K, Maganga L, Nitayaphan S, Kroon E, Sawe FK, Sinei S, Sriplienchan S, Jagodzinski LL, Malia J, Manak M, de Souza MS, Tovanabutra S, Sanders-Buell E, Rolland M, Dorsey-Spitz J, Eller MA, Milazzo M, Li Q, Lewandowski A, Wu H, Swann E, O’Connell RJ, Peel S, Dawson P, Kim JH, Michael NL, RV 217 Study Team. Prospective study of acute HIV-1 infection in adults in East Africa and Thailand. N Engl J Med. 2016;374:2120–30. https://doi.org/10.1056/NEJMoa1508952.
Vanhems P, Routy J-P, Hirschel B, Baratin D, Vora S, Maenza J, Carr A, Trépo C, Touraine J-L, Gillibert R-P, Collier AC, Cooper DA, Vizzard J, Sékaly R-P, Fabry J, Perrin L, Collaborative Group. Clinical features of acute retroviral syndrome differ by route of infection but not by gender and age. J Acquir Immune Defic Syndr 1999. 2002;31:318–21.
Kelley CF, Barbour JD, Hecht FM. The relation between symptoms, viral load, and viral load set point in primary HIV infection. J Acquir Immune Defic Syndr 1999. 2007;45:445–8. https://doi.org/10.1097/QAI.0b013e318074ef6e.
Koup RA, Safrit JT, Cao Y, Andrews CA, McLeod G, Borkowsky W, Farthing C, Ho DD. Temporal association of cellular immune responses with the initial control of viremia in primary human immunodeficiency virus type 1 syndrome. J Virol. 1994;68:4650–5.
Lyles RH, Muñoz A, Yamashita TE, Bazmi H, Detels R, Rinaldo CR, Margolick JB, Phair JP, Mellors JW. Natural history of human immunodeficiency virus type 1 viremia after seroconversion and proximal to AIDS in a large cohort of homosexual men. Multicenter AIDS Cohort Study. J Infect Dis. 2000;181:872–80. https://doi.org/10.1086/315339.
Mellors JW, Muñoz A, Giorgi JV, Margolick JB, Tassoni CJ, Gupta P, Kingsley LA, Todd JA, Saah AJ, Detels R, Phair JP, Rinaldo CR. Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med. 1997;126:946–54.
Walker BD, Flexner C, Paradis TJ, Fuller TC, Hirsch MS, Schooley RT, Moss B. HIV-1 reverse transcriptase is a target for cytotoxic T lymphocytes in infected individuals. Science. 1988;240:64–6.
Borrow P, Lewicki H, Hahn BH, Shaw GM, Oldstone MB. Virus-specific CD8+ cytotoxic T-lymphocyte activity associated with control of viremia in primary human immunodeficiency virus type 1 infection. J Virol. 1994;68:6103–10.
Borrow P, Lewicki H, Wei X, Horwitz MS, Peffer N, Meyers H, Nelson JA, Gairin JE, Hahn BH, Oldstone MB, Shaw GM. Antiviral pressure exerted by HIV-1-specific cytotoxic T lymphocytes (CTLs) during primary infection demonstrated by rapid selection of CTL escape virus. Nat Med. 1997;3:205–11.
Hay CM, Ruhl DJ, Basgoz NO, Wilson CC, Billingsley JM, DePasquale MP, D’Aquila RT, Wolinsky SM, Crawford JM, Montefiori DC, Walker BD. Lack of viral escape and defective in vivo activation of human immunodeficiency virus type 1-specific cytotoxic T lymphocytes in rapidly progressive infection. J Virol. 1999;73:5509–19.
Deng K, Pertea M, Rongvaux A, Wang L, Durand CM, Ghiaur G, Lai J, McHugh HL, Hao H, Zhang H, Margolick JB, Gurer C, Murphy AJ, Valenzuela DM, Yancopoulos GD, Deeks SG, Strowig T, Kumar P, Siliciano JD, Salzberg SL, Flavell RA, Shan L, Siliciano RF. Broad CTL response is required to clear latent HIV-1 due to dominance of escape mutations. Nature. 2015;517:381–5. https://doi.org/10.1038/nature14053.
Buzón MJ, Massanella M, Llibre JM, Esteve A, Dahl V, Puertas MC, Gatell JM, Domingo P, Paredes R, Sharkey M, Palmer S, Stevenson M, Clotet B, Blanco J, Martinez-Picado J. HIV-1 replication and immune dynamics are affected by raltegravir intensification of HAART-suppressed subjects. Nat Med. 2010;16:460–5. https://doi.org/10.1038/nm.2111.
Finzi D, Blankson J, Siliciano JD, Margolick JB, Chadwick K, Pierson T, Smith K, Lisziewicz J, Lori F, Flexner C, Quinn TC, Chaisson RE, Rosenberg E, Walker B, Gange S, Gallant J, Siliciano RF. Latent infection of CD4+ T cells provides a mechanism for lifelong persistence of HIV-1, even in patients on effective combination therapy. Nat Med. 1999;5:512–7. https://doi.org/10.1038/8394.
Chun T-W, Nickle DC, Justement JS, Meyers JH, Roby G, Hallahan CW, Kottilil S, Moir S, Mican JM, Mullins JI, Ward DJ, Kovacs JA, Mannon PJ, Fauci AS. Persistence of HIV in gut-associated lymphoid tissue despite long-term antiretroviral therapy. J Infect Dis. 2008;197:714–20. https://doi.org/10.1086/527324.
Cusini A, Vernazza PL, Yerly S, Decosterd LA, Ledergerber B, Fux CA, Rohrbach J, Widmer N, Hirschel B, Gaudenz R, Cavassini M, Klimkait T, Zenger F, Gutmann C, Opravil M, Günthard HF, Swiss HIV Cohort Study. Higher CNS penetration-effectiveness of long-term combination antiretroviral therapy is associated with better HIV-1 viral suppression in cerebrospinal fluid. J Acquir Immune Defic Syndr 1999. 2013;62:28–35. https://doi.org/10.1097/QAI.0b013e318274e2b0.
Richman DD, Wrin T, Little SJ, Petropoulos CJ. Rapid evolution of the neutralizing antibody response to HIV type 1 infection. Proc Natl Acad Sci U S A. 2003;100:4144–9. https://doi.org/10.1073/pnas.0630530100.
Mehandru S, Poles MA, Tenner-Racz K, Manuelli V, Jean-Pierre P, Lopez P, Shet A, Low A, Mohri H, Boden D, Racz P, Markowitz M. Mechanisms of gastrointestinal CD4+ T-cell depletion during acute and early human immunodeficiency virus type 1 infection. J Virol. 2007;81:599–612. https://doi.org/10.1128/JVI.01739-06.
Prendergast A, Prado JG, Kang Y-H, Chen F, Riddell LA, Luzzi G, Goulder P, Klenerman P. HIV-1 infection is characterized by profound depletion of CD161+ Th17 cells and gradual decline in regulatory T cells. AIDS Lond Engl. 2010;24:491–502. https://doi.org/10.1097/QAD.0b013e3283344895.
Cosgrove C, Ussher JE, Rauch A, Gärtner K, Kurioka A, Hühn MH, Adelmann K, Kang Y-H, Fergusson JR, Simmonds P, Goulder P, Hansen TH, Fox J, Günthard HF, Khanna N, Powrie F, Steel A, Gazzard B, Phillips RE, Frater J, Uhlig H, Klenerman P. Early and nonreversible decrease of CD161++/MAIT cells in HIV infection. Blood. 2013;121:951–61. https://doi.org/10.1182/blood-2012-06-436436.
Mudd JC, Brenchley JM. Gut mucosal barrier dysfunction, microbial dysbiosis, and their role in HIV-1 disease progression. J Infect Dis. 2016;214(Suppl 2):S58–66. https://doi.org/10.1093/infdis/jiw258.
Hsue PY, Scherzer R, Hunt PW, Schnell A, Bolger AF, Kalapus SC, Maka K, Martin JN, Ganz P, Deeks SG. Carotid intima-media thickness progression in HIV-infected adults occurs preferentially at the carotid bifurcation and is predicted by inflammation. J Am Heart Assoc. 2012;1:e000422. https://doi.org/10.1161/JAHA.111.000422.
Kuller LH, Tracy R, Belloso W, De Wit S, Drummond F, Lane HC, Ledergerber B, Lundgren J, Neuhaus J, Nixon D, Paton NI, Neaton JD, INSIGHT SMART Study Group. Inflammatory and coagulation biomarkers and mortality in patients with HIV infection. PLoS Med. 2008;5:e203. https://doi.org/10.1371/journal.pmed.0050203.
Marks MA, Rabkin CS, Engels EA, Busch E, Kopp W, Rager H, Goedert JJ, Chaturvedi AK. Markers of microbial translocation and risk of AIDS-related lymphoma. AIDS Lond Engl. 2013;27:469–74. https://doi.org/10.1097/QAD.0b013e32835c1333.
Ancuta P, Kamat A, Kunstman KJ, Kim E-Y, Autissier P, Wurcel A, Zaman T, Stone D, Mefford M, Morgello S, Singer EJ, Wolinsky SM, Gabuzda D. Microbial translocation is associated with increased monocyte activation and dementia in AIDS patients. PLoS One. 2008;3:e2516. https://doi.org/10.1371/journal.pone.0002516.
Andrade BB, Hullsiek KH, Boulware DR, Rupert A, French MA, Ruxrungtham K, Montes ML, Price H, Barreiro P, Audsley J, Sher A, Lewin SR, Sereti I, INSIGHT Study Group. Biomarkers of inflammation and coagulation are associated with mortality and hepatitis flares in persons coinfected with HIV and hepatitis viruses. J Infect Dis. 2013;207:1379–88. https://doi.org/10.1093/infdis/jit033.
AIDS Case Definition|Definition. In: AIDSinfo. https://aidsinfo.nih.gov/education-materials/glossary/2925/aids-case-definition. Accessed 23 Nov 2016.
Selik RM, Mokotoff ED, Branson B, Owen SM, Whitmore S, Hall I. Revised surveillance case definition for HIV infection – United States, 2014. MMWR Recomm Rep. 2014;63:1–10.
Ly TD, Ebel A, Faucher V, Fihman V, Laperche S. Could the new HIV combined p24 antigen and antibody assays replace p24 antigen specific assays? J Virol Methods. 2007;143:86–94. https://doi.org/10.1016/j.jviromet.2007.02.013.
Pilcher CD, McPherson JT, Leone PA, Smurzynski M, Owen-O’Dowd J, Peace-Brewer AL, Harris J, Hicks CB, Eron JJ, Fiscus SA. Real-time, universal screening for acute HIV infection in a routine HIV counseling and testing population. JAMA. 2002;288:216–21.
Branson BM, Owen SM, Wesolowski LG, Bennett B, Werner BG, Wroblewski KE, Pentella MA. Laboratory testing for the diagnosis of HIV infection: updated recommendations. Atlanta: Centers for Disease Control and Prevention and Association of Public Health Laboratories; 2014.
Busch MP, Satten GA. Time course of viremia and antibody seroconversion following human immunodeficiency virus exposure. Am J Med. 1997;102:117–124–126.
Fiebig EW, Wright DJ, Rawal BD, Garrett PE, Schumacher RT, Peddada L, Heldebrant C, Smith R, Conrad A, Kleinman SH, Busch MP. Dynamics of HIV viremia and antibody seroconversion in plasma donors: implications for diagnosis and staging of primary HIV infection. AIDS Lond Engl. 2003;17:1871–9. https://doi.org/10.1097/01.aids.0000076308.76477.b8.
Owen SM, Yang C, Spira T, Ou CY, Pau CP, Parekh BS, Candal D, Kuehl D, Kennedy MS, Rudolph D, Luo W, Delatorre N, Masciotra S, Kalish ML, Cowart F, Barnett T, Lal R, McDougal JS. Alternative algorithms for human immunodeficiency virus infection diagnosis using tests that are licensed in the United States. J Clin Microbiol. 2008;46:1588–95. https://doi.org/10.1128/JCM.02196-07.
Masciotra S, McDougal JS, Feldman J, Sprinkle P, Wesolowski L, Owen SM. Evaluation of an alternative HIV diagnostic algorithm using specimens from seroconversion panels and persons with established HIV infections. J Clin Virol. 2011;52(Suppl 1):S17–22. https://doi.org/10.1016/j.jcv.2011.09.011.
Masciotra S, Luo W, Youngpairoj AS, Kennedy MS, Wells S, Ambrose K, Sprinkle P, Owen SM. Performance of the Alere Determine™ HIV-1/2 Ag/Ab Combo Rapid Test with specimens from HIV-1 seroconverters from the US and HIV-2 infected individuals from Ivory Coast. J Clin Virol. 2013;58(Suppl 1):e54–8. https://doi.org/10.1016/j.jcv.2013.07.002.
Hollingsworth TD, Anderson RM, Fraser C. HIV-1 transmission, by stage of infection. J Infect Dis. 2008;198:687–93. https://doi.org/10.1086/590501.
Brenner BG, Roger M, Routy J-P, Moisi D, Ntemgwa M, Matte C, Baril J-G, Thomas R, Rouleau D, Bruneau J, Leblanc R, Legault M, Tremblay C, Charest H, Wainberg MA, Quebec Primary HIV Infection Study Group. High rates of forward transmission events after acute/early HIV-1 infection. J Infect Dis. 2007;195:951–9. https://doi.org/10.1086/512088.
Grinsztejn B, Hosseinipour MC, Ribaudo HJ, Swindells S, Eron J, Chen YQ, Wang L, Ou S-S, Anderson M, McCauley M, Gamble T, Kumarasamy N, Hakim JG, Kumwenda J, Pilotto JHS, Godbole SV, Chariyalertsak S, de Melo MG, Mayer KH, Eshleman SH, Piwowar-Manning E, Makhema J, Mills LA, Panchia R, Sanne I, Gallant J, Hoffman I, Taha TE, Nielsen-Saines K, Celentano D, Essex M, Havlir D, Cohen MS. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: results from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect Dis. 2014;14:281–90. https://doi.org/10.1016/S1473-3099(13)70692-3.
Hecht FM, Busch MP, Rawal B, Webb M, Rosenberg E, Swanson M, Chesney M, Anderson J, Levy J, Kahn JO. Use of laboratory tests and clinical symptoms for identification of primary HIV infection. AIDS Lond Engl. 2002;16:1119–29.
Patel P, Mackellar D, Simmons P, Uniyal A, Gallagher K, Bennett B, Sullivan TJ, Kowalski A, Parker MM, LaLota M, Kerndt P, Sullivan PS, Centers for Disease Control and Prevention Acute HIV Infection Study Group. Detecting acute human immunodeficiency virus infection using 3 different screening immunoassays and nucleic acid amplification testing for human immunodeficiency virus RNA, 2006–2008. Arch Intern Med. 2010;170:66–74. https://doi.org/10.1001/archinternmed.2009.445.
Lewis JM, Macpherson P, Adams ER, Ochodo E, Sands A, Taegtmeyer M. Field accuracy of fourth-generation rapid diagnostic tests for acute HIV-1: a systematic review. AIDS Lond Engl. 2015;29:2465–71. https://doi.org/10.1097/QAD.0000000000000855.
Fiebig EW, Heldebrant CM, Smith RIF, Conrad AJ, Delwart EL, Busch MP. Intermittent low-level viremia in very early primary HIV-1 infection. J Acquir Immune Defic Syndr 1999. 2005;39:133–7.
Tomaras GD, Yates NL, Liu P, Qin L, Fouda GG, Chavez LL, Decamp AC, Parks RJ, Ashley VC, Lucas JT, Cohen M, Eron J, Hicks CB, Liao H-X, Self SG, Landucci G, Forthal DN, Weinhold KJ, Keele BF, Hahn BH, Greenberg ML, Morris L, Karim SSA, Blattner WA, Montefiori DC, Shaw GM, Perelson AS, Haynes BF. Initial B-cell responses to transmitted human immunodeficiency virus type 1: virion-binding immunoglobulin M (IgM) and IgG antibodies followed by plasma anti-gp41 antibodies with ineffective control of initial viremia. J Virol. 2008;82:12449–63. https://doi.org/10.1128/JVI.01708-08.
Louie B, Wong E, Klausner JD, Liska S, Hecht F, Dowling T, Obeso M, Phillips SS, Pandori MW. Assessment of rapid tests for detection of human immunodeficiency virus-specific antibodies in recently infected individuals. J Clin Microbiol. 2008;46:1494–7. https://doi.org/10.1128/JCM.01945-07.
Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, Hakim JG, Kumwenda J, Grinsztejn B, Pilotto JHS, Godbole SV, Mehendale S, Chariyalertsak S, Santos BR, Mayer KH, Hoffman IF, Eshleman SH, Piwowar-Manning E, Wang L, Makhema J, Mills LA, de Bruyn G, Sanne I, Eron J, Gallant J, Havlir D, Swindells S, Ribaudo H, Elharrar V, Burns D, Taha TE, Nielsen-Saines K, Celentano D, Essex M, Fleming TR. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365:493–505. https://doi.org/10.1056/NEJMoa1105243.
Johnson LF, Mossong J, Dorrington RE, Schomaker M, Hoffmann CJ, Keiser O, Fox MP, Wood R, Prozesky H, Giddy J, Garone DB, Cornell M, Egger M, Boulle A, International Epidemiologic Databases to Evaluate AIDS Southern Africa Collaboration. Life expectancies of South African adults starting antiretroviral treatment: collaborative analysis of cohort studies. PLoS Med. 2013;10:e1001418. https://doi.org/10.1371/journal.pmed.1001418.
Nakagawa F, May M, Phillips A. Life expectancy living with HIV: recent estimates and future implications. Curr Opin Infect Dis. 2013;26:17–25. https://doi.org/10.1097/QCO.0b013e32835ba6b1.
Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services.
Kitahata MM, Van Rompaey SE, Shields AW. Physician experience in the care of HIV-infected persons is associated with earlier adoption of new antiretroviral therapy. J Acquir Immune Defic Syndr 1999. 2000;24:106–14.
Landon BE, Wilson IB, McInnes K, Landrum MB, Hirschhorn LR, Marsden PV, Cleary PD. Physician specialization and the quality of care for human immunodeficiency virus infection. Arch Intern Med. 2005;165:1133–9. https://doi.org/10.1001/archinte.165.10.1133.
Kitahata MM, Van Rompaey SE, Dillingham PW, Koepsell TD, Deyo RA, Dodge W, Wagner EH. Primary care delivery is associated with greater physician experience and improved survival among persons with AIDS. J Gen Intern Med. 2003;18:95–103.
Delgado J, Heath KV, Yip B, Marion S, Alfonso V, Montaner JSG, O’Shaughnessy MV, Hogg RS. Highly active antiretroviral therapy: physician experience and enhanced adherence to prescription refill. Antivir Ther. 2003;8:471–8.
O’Neill M, Karelas GD, Feller DJ, Knudsen-Strong E, Lajeunesse D, Tsui D, Gordon P, Agins BD. The HIV workforce in New York state: does patient volume correlate with quality? Clin Infect Dis. 2015;61:1871–7. https://doi.org/10.1093/cid/civ719.
Egger M, May M, Chêne G, Phillips AN, Ledergerber B, Dabis F, Costagliola D, D’Arminio Monforte A, de Wolf F, Reiss P, Lundgren JD, Justice AC, Staszewski S, Leport C, Hogg RS, Sabin CA, Gill MJ, Salzberger B, Sterne JAC, ART Cohort Collaboration. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet Lond Engl. 2002;360:119–29.
Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents. Guidelines for the prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America.
Havlir DV, Bassett R, Levitan D, Gilbert P, Tebas P, Collier AC, Hirsch MS, Ignacio C, Condra J, Günthard HF, Richman DD, Wong JK. Prevalence and predictive value of intermittent viremia with combination HIV therapy. JAMA. 2001;286:171–9.
Tural C, Ruiz L, Holtzer C, Schapiro J, Viciana P, González J, Domingo P, Boucher C, Rey-Joly C, Clotet B, Havana Study Group. Clinical utility of HIV-1 genotyping and expert advice: the Havana trial. AIDS Lond Engl. 2002;16:209–18.
Hirsch MS, Günthard HF, Schapiro JM, Brun-Vézinet F, Clotet B, Hammer SM, Johnson VA, Kuritzkes DR, Mellors JW, Pillay D, Yeni PG, Jacobsen DM, Richman DD. Antiretroviral drug resistance testing in adult HIV-1 infection: 2008 recommendations of an international AIDS Society-USA panel. Clin Infect Dis. 2008;47:266–85. https://doi.org/10.1086/589297.
Gianotti N, Mondino V, Rossi MC, Chiesa E, Mezzaroma I, Ladisa N, Guaraldi G, Torti C, Tarquini P, Castelli P, Di Carlo A, Boeri E, Keulen W, Kenna PM, Lazzarin A, Mutations and Salvage (MuSa) Study Group. Comparison of a rule-based algorithm with a phenotype-based algorithm for the interpretation of HIV genotypes in guiding salvage regimens in HIV-infected patients by a randomized clinical trial: the mutations and salvage study. Clin Infect Dis. 2006;42:1470–80. https://doi.org/10.1086/503568.
Phillips EJ, Sullivan JR, Knowles SR, Shear NH. Utility of patch testing in patients with hypersensitivity syndromes associated with abacavir. AIDS Lond Engl. 2002;16:2223–5.
Mallal S, Nolan D, Witt C, Masel G, Martin AM, Moore C, Sayer D, Castley A, Mamotte C, Maxwell D, James I, Christiansen FT. Association between presence of HLA-B∗5701, HLA-DR7, and HLA-DQ3 and hypersensitivity to HIV-1 reverse-transcriptase inhibitor abacavir. Lancet Lond Engl. 2002;359:727–32.
Hetherington S, Hughes AR, Mosteller M, Shortino D, Baker KL, Spreen W, Lai E, Davies K, Handley A, Dow DJ, Fling ME, Stocum M, Bowman C, Thurmond LM, Roses AD. Genetic variations in HLA-B region and hypersensitivity reactions to abacavir. Lancet Lond Engl. 2002;359:1121–2. https://doi.org/10.1016/S0140-6736(02)08158-8.
Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission. Recommendations for use of antiretroviral drugs in pregnant HIV-1-infected women for maternal health and interventions to reduce perinatal HIV transmission in the United States. Department of Health and Human Services; 2016.
Fowler MG, Qin M, Fiscus SA, Currier JS, Flynn PM, Chipato T, McIntyre J, Gnanashanmugam D, Siberry GK, Coletti AS, Taha TE, Klingman KL, Martinson FE, Owor M, Violari A, Moodley D, Theron GB, Bhosale R, Bobat R, Chi BH, Strehlau R, Mlay P, Loftis AJ, Browning R, Fenton T, Purdue L, Basar M, Shapiro DE, Mofenson LM, IMPAACT 1077BF/1077FF PROMISE Study Team. Benefits and risks of antiretroviral therapy for perinatal HIV prevention. N Engl J Med. 2016;375:1726–37. https://doi.org/10.1056/NEJMoa1511691.
Ford N, Mofenson L, Shubber Z, Calmy A, Andrieux-Meyer I, Vitoria M, Shaffer N, Renaud F. Safety of efavirenz in the first trimester of pregnancy: an updated systematic review and meta-analysis. AIDS. 2014;28(Suppl 2):S123–31.
Department of Health and Human Services. 2018. https://aidsinfo.nih.gov/news/2094/statement-on-potential-safety-signal-in-infants-born-to-women-taking-dolutegravir. Accessed 29 June 2018.
Lopez LM, Bernholc A, Chen M, Tolley EE. School-based interventions for improving contraceptive use in adolescents. Cochrane Database Syst Rev. 2016;(6):CD012249. https://doi.org/10.1002/14651858.CD012249.
Kirby D, Coyle K, Alton F, Rolleri L, Robin L. Reducing adolescent sexual risk: a theoretical guide for developing and adapting curriculum-based programs. Scotts Valley: ETR Associates; 2011.
Chin HB, Sipe TA, Elder R, Mercer SL, Chattopadhyay SK, Jacob V, Wethington HR, Kirby D, Elliston DB, Griffith M, Chuke SO, Briss SC, Ericksen I, Galbraith JS, Herbst JH, Johnson RL, Kraft JM, Noar SM, Romero LM, Santelli J. The effectiveness of group-based comprehensive risk-reduction and abstinence education interventions to prevent or reduce the risk of adolescent pregnancy, human immunodeficiency virus, and sexually transmitted infections: two systematic reviews for the Guide to Community Preventive Services. Am J Prev Med. 2012;42:272–94. https://doi.org/10.1016/j.amepre.2011.11.006.
Demissie Z, Brener ND, McManus T, Shanklin SL, Hawkins J, Kann L. School health profiles 2014: characteristics of health programs among secondary schools. Atlanta: Centers for Disease Control and Prevention; 2015.
Camacho-Gonzalez AF, Wallins A, Toledo L, Murray A, Gaul Z, Sutton MY, Gillespie S, Leong T, Graves C, Chakraborty R. Risk factors for HIV transmission and barriers to HIV disclosure: metropolitan Atlanta youth perspectives. AIDS Patient Care STDs. 2015;30:18–24. https://doi.org/10.1089/apc.2015.0163.
Eaton LA, Huedo-Medina TB, Kalichman SC, Pellowski JA, Sagherian MJ, Warren M, Popat AR, Johnson BT. Meta-analysis of single-session behavioral interventions to prevent sexually transmitted infections: implications for bundling prevention packages. Am J Public Health. 2012;102:e34–44. https://doi.org/10.2105/AJPH.2012.300968.
Weller SC, Davis-Beaty K. Condom effectiveness in reducing heterosexual HIV transmission. Cochrane Database Syst Rev. 2002;(1):CD003255.
Mustanski B, Ryan DT, Garofalo R. Associations of sexually transmitted infections with condom problems among young men who have sex with men. Sex Transm Dis. 2014;41:427–32. https://doi.org/10.1097/OLQ.0000000000000150.
Voeller B, Coulson AH, Bernstein GS, Nakamura RM. Mineral oil lubricants cause rapid deterioration of latex condoms. Contraception. 1989;39:95–102.
Rebe KB, De Swardt G, Berman PA, Struthers H, McIntyre JA. Sexual lubricants in South Africa may potentially disrupt mucosal surfaces and increase HIV transmission risk among men who have sex with men. S Afr Med J. 2013;104:49–51.
Minnis AM, Padian NS. Effectiveness of female controlled barrier methods in preventing sexually transmitted infections and HIV: current evidence and future research directions. Sex Transm Infect. 2005;81:193–200. https://doi.org/10.1136/sti.2003.007153.
Siegfried N, Muller M, Deeks JJ, Volmink J. Male circumcision for prevention of heterosexual acquisition of HIV in men. Cochrane Database Syst Rev. 2009;(2):CD003362.
Wiysonge CS, Kongnyuy EJ, Shey M, Muula AS, Navti OB, Akl EA, Lo Y-R. Male circumcision for prevention of homosexual acquisition of HIV in men. Cochrane Database Syst Rev. 2011;(6):CD007496.
Okwundu CI, Uthman OA, Okoromah CA. Antiretroviral pre-exposure prophylaxis (PrEP) for preventing HIV in high-risk individuals. Cochrane Database Syst Rev. 2012;(7):CD007189.
Centers for Disease Control and Prevention. Preexposure Prophylaxis for the Prevention of HIV Infection in the United States – 2017 Update. 2017. https://www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2017.pdf. Accessed 29 June 2018.
Food and Drug Administration. 2018. https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2018/021752Orig1s055ltr.pdf. Accessed 29 June 2018.
Hosek S, Rudy R, Landovitz R, Kapogiannis B, Siberry G, Rutledge B, Liu N, Brothers J, Mulligan K, Zimet G, Lally M, Mayer K, Anderson P, Kiser J, Rooney J, Wilson CM, the Adolescent Trials Network (ATN) for HIV/AIDS Interventions. A HIV-pre-exposure prophylaxis (PrEP) demonstration project and safety study for young MSM. J Acquir Immune Defic Syndr. 2018;74(1):21–9. https://doi.org/10.1097/QAI.0000000000001179.
Centers for Disease Control and Prevention. Updated guidelines for antiretroviral postexposure prophylaxis after sexual, injection drug use, or other nonoccupational exposure to HIV – United States, 2016. Atlanta: Centers for Disease Control and Prevention; 2016.
Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, Hakim JG, Kumwenda J, Grinsztejn B, Pilotto JHS, Godbole SV, Chariyalertsak S, Santos BR, Mayer KH, Hoffman IF, Eshleman SH, Piwowar-Manning E, Cottle L, Zhang XC, Makhema J, Mills LA, Panchia R, Faesen S, Eron J, Gallant J, Havlir D, Swindells S, Elharrar V, Burns D, Taha TE, Nielsen-Saines K, Celentano DD, Essex M, Hudelson SE, Redd AD, Fleming TR, HPTN 052 Study Team. Antiretroviral therapy for the prevention of HIV-1 transmission. N Engl J Med. 2016;375:830–9. https://doi.org/10.1056/NEJMoa1600693.
Anglemyer A, Rutherford GW, Horvath T, Baggaley RC, Egger M, Siegfried N. Antiretroviral therapy for prevention of HIV transmission in HIV-discordant couples. Cochrane Database Syst Rev. 2013;(4):CD009153.
Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, van Lunzen J, Corbelli GM, Estrada V, Geretti AM, Beloukas A, Asboe D, Viciana P, Gutiérrez F, Clotet B, Pradier C, Gerstoft J, Weber R, Westling K, Wandeler G, Prins JM, Rieger A, Stoeckle M, Kümmerle T, Bini T, Ammassari A, Gilson R, Krznaric I, Ristola M, Zangerle R, Handberg P, Antela A, Allan S, Phillips AN, Lundgren J, PARTNER Study Group. Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner is using suppressive antiretroviral therapy. JAMA. 2016;316:171–81. https://doi.org/10.1001/jama.2016.5148.
Townsend CL, Byrne L, Cortina-Borja M, Thorne C, de Ruiter A, Lyall H, Taylor GP, Peckham CS, Tookey PA. Earlier initiation of ART and further decline in mother-to-child HIV transmission rates, 2000–2011. AIDS Lond Engl. 2014;28:1049–57. https://doi.org/10.1097/QAD.0000000000000212.
Forbes JC, Alimenti AM, Singer J, Brophy JC, Bitnun A, Samson LM, Money DM, Lee TCK, Lapointe ND, Read SE, Canadian Pediatric AIDS Research Group (CPARG). A national review of vertical HIV transmission. AIDS Lond Engl. 2012;26:757–63. https://doi.org/10.1097/QAD.0b013e328350995c.
Mandelbrot L, Tubiana R, Le Chenadec J, Dollfus C, Faye A, Pannier E, Matheron S, Khuong M-A, Garrait V, Reliquet V, Devidas A, Berrebi A, Allisy C, Elleau C, Arvieux C, Rouzioux C, Warszawski J, Blanche S, ANRS-EPF Study Group. No perinatal HIV-1 transmission from women with effective antiretroviral therapy starting before conception. Clin Infect Dis. 2015;61:1715–25. https://doi.org/10.1093/cid/civ578.
Gayles TA, Kuhns LM, Kwon S, Mustanski B, Garofalo R. Socioeconomic disconnection as a risk factor for increased HIV infection in young men who have sex with men. LGBT Health. 2016;3:219–24. https://doi.org/10.1089/lgbt.2015.0102.
An Q, Prejean J, McDavid Harrison K, Fang X. Association between community socioeconomic position and HIV diagnosis rate among adults and adolescents in the United States, 2005 to 2009. Am J Public Health. 2013;103:120–6. https://doi.org/10.2105/AJPH.2012.300853.
Arnold M, Hsu L, Pipkin S, McFarland W, Rutherford GW. Race, place and AIDS: the role of socioeconomic context on racial disparities in treatment and survival in San Francisco. Soc Sci Med 1982. 2009;69:121–8. https://doi.org/10.1016/j.socscimed.2009.04.019.
McDavid Harrison K, Ling Q, Song R, Hall HI. County-level socioeconomic status and survival after HIV diagnosis, United States. Ann Epidemiol. 2008;18:919–27. https://doi.org/10.1016/j.annepidem.2008.09.003.
Wolitski RJ, Kidder DP, Pals SL, Royal S, Aidala A, Stall R, Holtgrave DR, Harre D, Courtenay-Quirk C, Housing and Health Study Team. Randomized trial of the effects of housing assistance on the health and risk behaviors of homeless and unstably housed people living with HIV. AIDS Behav. 2010;14:493–503. https://doi.org/10.1007/s10461-009-9643-x.
Schwarcz SK, Hsu LC, Vittinghoff E, Vu A, Bamberger JD, Katz MH. Impact of housing on the survival of persons with AIDS. BMC Public Health. 2009;9:220. https://doi.org/10.1186/1471-2458-9-220.
Marshall BDL, Kerr T, Shoveller JA, Patterson TL, Buxton JA, Wood E. Homelessness and unstable housing associated with an increased risk of HIV and STI transmission among street-involved youth. Health Place. 2009;15:753–60. https://doi.org/10.1016/j.healthplace.2008.12.005.
Kidder DP, Wolitski RJ, Pals SL, Campsmith ML. Housing status and HIV risk behaviors among homeless and housed persons with HIV. J Acquir Immune Defic Syndr 1999. 2008;49:451–5.
Whittle HJ, Palar K, Napoles T, Hufstedler LL, Ching I, Hecht FM, Frongillo EA, Weiser SD. Experiences with food insecurity and risky sex among low-income people living with HIV/AIDS in a resource-rich setting. J Int AIDS Soc. 2015;18:20293.
Whittle HJ, Palar K, Seligman HK, Napoles T, Frongillo EA, Weiser SD. How food insecurity contributes to poor HIV health outcomes: qualitative evidence from the San Francisco Bay Area. Soc Sci Med 1982. 2016;170:228–36. https://doi.org/10.1016/j.socscimed.2016.09.040.
Palar K, Laraia B, Tsai AC, Johnson MO, Weiser SD. Food insecurity is associated with HIV, sexually transmitted infections and drug use among men in the United States. AIDS Lond Engl. 2016;30:1457–65. https://doi.org/10.1097/QAD.0000000000001095.
Singer AW, Weiser SD, McCoy SI. Does food insecurity undermine adherence to antiretroviral therapy? A systematic review. AIDS Behav. 2015;19:1510–26. https://doi.org/10.1007/s10461-014-0873-1.
Hussen SA, Harper GW, Bauermeister JA, Hightow-Weidman LB. Psychosocial influences on engagement in care among HIV-positive young black gay/bisexual and other men who have sex with men. AIDS Patient Care STDs. 2015;29:77–85. https://doi.org/10.1089/apc.2014.0117.
Bauman LJ, Braunstein S, Calderon Y, Chhabra R, Cutler B, Leider J, Rivera A, Sclafane J, Tsoi B, Watnick D. Barriers and facilitators of linkage to HIV primary care in New York City. J Acquir Immune Defic Syndr 1999. 2013;64:S20–6. https://doi.org/10.1097/QAI.0b013e3182a99c19.
Turan B, Smith W, Cohen MH, Wilson TE, Adimora AA, Merenstein D, Adedimeji A, Wentz EL, Foster AG, Metsch L, Tien PC, Weiser SD, Turan JM. Mechanisms for the negative effects of internalized HIV-related stigma on antiretroviral therapy adherence in women: the mediating roles of social isolation and depression. J Acquir Immune Defic Syndr 1999. 2016;72:198–205. https://doi.org/10.1097/QAI.0000000000000948.
Magnus M, Herwehe J, Murtaza-Rossini M, Reine P, Cuffie D, Gruber D, Kaiser M. Linking and retaining HIV patients in care: the importance of provider attitudes and behaviors. AIDS Patient Care STDs. 2013;27:297–303. https://doi.org/10.1089/apc.2012.0423.
Kinsler JJ, Wong MD, Sayles JN, Davis C, Cunningham WE. The effect of perceived stigma from a health care provider on access to care among a low-income HIV-positive population. AIDS Patient Care STDs. 2007;21:584–92. https://doi.org/10.1089/apc.2006.0202.
Sullivan PS, Peterson J, Rosenberg ES, Kelley CF, Cooper H, Vaughan A, Salazar LF, Frew P, Wingood G, Diclemente R, del Rio C, Mulligan M, Sanchez TH. Understanding racial HIV/STI disparities in black and white men who have sex with men: a multilevel approach. PLoS One. 2014;9:e90514. https://doi.org/10.1371/journal.pone.0090514.
Hernández-Romieu AC, Sullivan PS, Rothenberg R, Grey J, Luisi N, Kelley CF, Rosenberg ES. Heterogeneity of HIV prevalence among the sexual networks of black and white men who have sex with men in Atlanta: illuminating a mechanism for increased HIV risk for young black men who have sex with men. Sex Transm Dis. 2015;42:505–12. https://doi.org/10.1097/OLQ.0000000000000332.
Sullivan PS, Rosenberg ES, Sanchez TH, Kelley C, Luisi N, Cooper H, Diclemente R, Frew P, Salazar LF, del Rio C, Mulligan MJ, Peterson J. Explaining racial disparities in HIV incidence in a prospective cohort of black and white men who have sex with men in Atlanta, GA: a prospective observational cohort study. Ann Epidemiol. 2015;25:445–54. https://doi.org/10.1016/j.annepidem.2015.03.006.
NIH. The HIV life cycle. AIDSInfo. https://aidsinfo.nih.gov/understanding-hiv-aids/factsheets/19/73/the-hiv-life-cycle. Accessed 8/16/2019.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ranadive, N., Hussen, S.A., Chakraborty, R. (2020). Human Immunodeficiency Virus. In: Hussen, S. (eds) Sexually Transmitted Infections in Adolescence and Young Adulthood. Springer, Cham. https://doi.org/10.1007/978-3-030-20491-4_17
Download citation
DOI: https://doi.org/10.1007/978-3-030-20491-4_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-20490-7
Online ISBN: 978-3-030-20491-4
eBook Packages: MedicineMedicine (R0)