
Abstract
Intrauterine adhesions (IUA) also referred to as Asherman’s syndrome or intrauterine synechiae is a well-defined clinical entity, manifested by anatomic obliteration of the uterine cavity by adhesions. It may be caused by surgical trauma to the basal layer of the endometrium, usually secondary to curettage of the postpartum uterus, elective termination of early pregnancies, and genital tuberculosis, and may culminate in a spectrum of disorders ranging from menstrual disturbances to normal menses, infertility, recurrent pregnancy loss, and, possibly, endometriosis.
Several diagnostic techniques, such as transvaginal sonography (TVS), hysterosalpingography (HSG), saline infusion hysterography (SIS), sonohysterography, saline contrast hysterosonography (SCHS), 3D ultrasound, sonohysterosalpingography, 3D hysterosonography, hydrosonography, and, rarely, magnetic resonance imaging, have been used for screening IUA. MR might give additional information with the use of DW and T2W high-resolution images. The uterine cavity must be evaluated as the place where the embryo is implanted and where pregnancy is developed. Any occupation of the cavity can thwart embryo development. Although MR hysterosalpingography can properly evaluate these abnormalities, standard MR examinations also can be of value. Intrauterine adhesions or synechiae may be secondary to pregnancy, curettages, surgeries, or earlier infections. They might be identified as hypointense linear images that cross the endometrial cavity in T2-weighted images. However, though these techniques are noninvasive and cost-effective with a short learning curve and may accurately assess most intrauterine pathology with a high specificity, they have limited accuracy for the detection of IUA with a high false-positive diagnosis rate and have to fall back on hysteroscopy as the reference standard owing to its higher sensitivity. Combined with history and a high index of suspicion, operative hysteroscopy is the gold standard for the accurate diagnosis, classification, and treatment of IUA.
Adhesiolysis followed by the use of anti-adhesive barriers to prevent reformation and combined with cyclic estrogen therapy to stimulate endometrial growth is the therapy of choice. Auto-cross-linked hyaluronic acid (ACP) gel, obtained by condensation of hyaluronic acid, is a reabsorbable agent that can be applied to the uterine cavity for the prevention of IUAs. Approximately 7 days after the application, ACP is completely reabsorbed. Prevention of IUAs is essential, and application of ACP gel may be considered to reduce the incidence and severity of IUAs. Perivascular stem cells (PVSCs) are recently proposed as the origin of all mesenchymal stem cells, and PVSCs from human umbilical cords (HUCs) are known to be the most effective cells to respond rapidly in intrauterine injuries. PVSCs transplantation gives us a promising option to facilitate restoration processes of impaired endometrium and improve poor pregnancy outcomes in the uterus with intrauterine adhesions based on murine research. Several techniques, such as hysteroscopic adhesiolysis with scissors, electrosurgery or laser, ultrasound-directed hysteroscopic adhesiolysis, fluoroscopically guided hysteroscopic synechiolysis and balloon hysteroplasty, laparoscopic intracorporeal ultrasound-guided hysteroscopic adhesiolysis, pressure lavage under ultrasound guidance (PLUG), and sonohysterographic (SHG) adhesiolysis, have been proposed for the treatment of IUA. Hysteroscopic adhesiolysis is a unanimously recognized safe and effective first choice for restoring menstrual function and fertility even in women with severe adhesions and postmenopausal women with highly favorable pregnancy and live birth rates. Intraoperative ultrasonography, as an adjunct, has a significant role in hysteroscopic adhesiolysis in coordinating images of the endometrial cavity, uterine wall, and the tip of the hysteroscope, directing and ensuring dissection in the proper tissue plane, thus avoiding the possibility of inadvertent uterine perforation, and in examining the endometrial pattern and predicting the surgical and clinical outcome in women with severe Asherman’s syndrome and in extensive, recurrent adhesions. Fluoroscopically guided hysteroscopic synechiolysis and PLUG are minimally invasive and cost-effective alternatives compared to labor-intensive, expensive endoscopic techniques with a high potential for restoration of menses and fertility, and PLUG enables complete lysis in mild to moderate IUA obviating the need for operative hysteroscopy. However, their efficacy must be explored further.
Hence, while ultrasonography may have a limited role in the diagnosis of IUA compared to hysteroscopy, it has a significant role in guiding the surgical management of IUA.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Ever since the first description of intrauterine adhesions (IUAs) by Joseph Asherman in 1948, this intrauterine pathology has been recognized as a significant gynecological complication, diagnosed with increased frequency [1, 2]. Commonly referred to as Asherman’s syndrome and intrauterine synechiae, these lesions cover a spectrum that ranges from minor and insignificant to severe cohesive adhesions that affect menstrual function and fertility [3]. Pathology shows fibrous connective tissue bands with or without glandular tissue, although this may range from filmy to dense [1]. Adhesions may be classified into grades I to IV depending on the consistency and severity. Seven classification systems are described, with no universal acceptance of any one system and no validation of any of them [4].
Incidence
Intrauterine adhesions are the most frequent complications after hysteroscopic surgery in women of reproductive age, the prevalence of IUA after hysteroscopic surgery being correlated with intrauterine pathology (myoma, polyp, or adhesions) [5]. The true incidence of IUA is unknown, with most cases occurring within close temporal proximity to a pregnancy, usually within 4 months and, usually, while the woman is in a hypoestrogenized state [1]. Westendorp et al. [6] reported intrauterine adhesions in 40% of patients at ambulatory hysteroscopy, performed 3 months after secondary removal of placental remnants more than 24 hours after delivery or a repeat curettage for incomplete abortions [6]. Salzani et al. [7] reported IUA on hysteroscopy performed 3–12 months after curettage following abortion in 37.6% of the women, which were mostly mucous and grade I (56.1%) [7]. Khanna and Agrawal [8] reported intrauterine adhesions in 34.8% of the women at hysteroscopy, of whom 68.8% were positive for tubercular bacilli [8]. The number of previous abortions and curettage procedures did not correlate with the presence of IUA [7].
Causes
Intrauterine adhesions or synechiae evolve after trauma to the endometrium from surgical procedures usually secondary to curettage of a recently pregnant uterus in the context of missed abortion or pregnancy-related hemorrhage [1,2,3], following hysteroscopic myomectomy (10%) and transmural myomectomies, especially when combined with uterine ischemia [9]. Previous curettage on a gravid uterus has been reported as the possible cause of Asherman’s syndrome in the majority (64%) of patients [10]. In a prospective, randomized, controlled trial in 82 women, Tam et al. [11] reported that conservative management and medical evacuation for spontaneous abortion are both acceptable alternatives to standard surgical evacuation, which resulted in a prevalence of 7.7% filmy IUA at hysteroscopic diagnosis of IUA, 6 months after initial treatment [11].
Dawood et al. [12] evaluated the predisposing factors and treatment outcomes of different stages of intrauterine adhesions over a 7-year period in 65 patients. They identified stage I intrauterine adhesions in 36.9%, stage II in 46.2%, and stage III in 16.9% of patients, the main reasons for referral being infertility (stage I 75%, stage II 73.3%, stage III 27.3%) and amenorrhea (stage I 25%, stage II 23.3%, stage III 72.7%). The main predisposing factor was dilatation and curettage, with 40 patients reporting IUA related to early pregnancy curettage; 45% had stage I adhesions, 42.5% had stage II, and 12.5% had stage III in contrast with 10 patients who had peripartum curettage, in whom 60% developed stage III adhesions (p = 0.004) [12].
Genital tuberculosis has been reported as an important and common cause of Asherman’s syndrome in India, causing oligomenorrhea or amenorrhea with infertility. Sharma et al. [13] studied 28 women with positive evidence of genital tuberculosis on endometrial biopsy (histopathology or culture) or positive polymerase chain reaction (PCR) on endometrial aspirate or positive findings of tuberculosis on laparoscopy or hysteroscopy who underwent hysteroscopy with or without laparoscopy for suspected Asherman’s syndrome . They reported various grades of adhesions (grade I in 17.8%, grade II in 28.5%, grade III in 28.5%, and grade IV in 17.5%) at hysteroscopy in all women , bilateral (28.5%) or unilateral (21.3%) blocked ostia, or inability to see the ostia (28.5%). Only four women (14.3%) had open ostia. On laparoscopy performed on 18 women, there were varying grades of adhesions in 16 (88.8%) women, with beading (33.3%), tubercles (33.3%), caseation (11.1%), and tubo-ovarian masses (11.1%) [13].
Risk Factors
In women with menstrual disorders, a statistically significant 12-fold increased risk for Asherman’s syndrome grades I–IV was found, previous abortion, as well as infection during surgery being associated with a mildly but nonsignificant increased risk [6]. Myomectomy for multiple, apposing fibroids is reported to have a higher incidence of IUA [9]. Uterine arteries embolization also carries a risk of intracavitary adhesions. Poujade et al. [14] reported a significant risk of uterine synechiae after placement of uterine compression sutures [(Hackethal technique) that transverse the uterine cavity for controlling postpartum hemorrhage (PPH) ], with the development of uterine synechiae on explorative hysteroscopy or HSG in 26.7% of women [14].
Effects
In addition to abnormal menses , infertility and recurrent spontaneous abortion are common complaints of IUA, and the accompanying retrograde menstruation may lead to endometriosis [2, 15]. Adhesions are a significant source of impaired organ functioning , decreased fertility, bowel obstruction, difficult reoperation, and, possibly, pain with consequent financial sequelae [16].
Diagnosis
History and a high index of suspicion contribute significantly to the diagnosis of IUA. Several confirmatory tests , such as hysteroscopy, ultrasound-guided techniques (3D hysterosonography [3D HS], two-dimensional [2D] and three-dimensional [3D] transvaginal ultrasonography [TVS] , hydrosonography, minimal invasive saline contrast hysterosonography [SCHS], saline infusion hysterography [SIS], sonohysterosalpingography ), radiographic techniques (hysterosalpingography [HSG] ), and rarely magnetic resonance imaging, have been used for the diagnosis of IUA. However, hysteroscopy has been documented as the gold standard for the diagnosis and treatment of IUA, and the several comparative studies evaluating these techniques have used hysteroscopy as the reference standard to evaluate the efficiency of a particular technique against the other. Hysteroscopy may be recommended in patients who develop menstrual disorders, either after secondary intervention for placental remnants after delivery or after a repeat curettage [6].
The Role of Ultrasound in the Diagnosis
Several ultrasound techniques , such as transvaginal color Doppler sonography (TCDS) , sonohysterosalpingography (SHSG) , and three-dimensional sonography (3DS) , are capable of providing diagnostic information that, in some cases, is equivalent to the information afforded by established techniques that require exposure to radiation, such as hysterosalpingography (HSG) , or that are more invasive, such as hysteroscopy or diagnostic laparoscopy [17], tissue biopsies, and dilation and curettage (D&C). The role of ultrasonography for the diagnosis of IUA has been studied by several authors with mixed opinions, and all these studies used hysteroscopy as the most reliable reference standard.
El-Mazny et al. [18] reported abnormal hysteroscopic findings, including IUA, in 33.1% of patients with reported normal uterine findings on HSG who were scheduled for assisted reproductive techniques (ART) (in vitro fertilization [IVF]/intracytoplasmic sperm injection [ICSI] investigations) [1].
Transvaginal sonography (TVS) has been reported to be specific (100%), but not sensitive (41.7%) compared with outpatient hysteroscopy, which leads the authors to suggest that outpatient hysteroscopy should be part of the infertility workup before ART even in patients with normal HSG and/or TVS and especially in patients with prior failed ART cycles who reported a significantly higher incidence of abnormal hysteroscopic findings. The procedure was acceptable in almost all patients with no reported complications [18].
Fedele et al. [19] performed transvaginal US before hysteroscopy as part of the routine diagnostic workup in 77 women who had repeated spontaneous abortions. They were able to correctly identify uterine adhesions (minimal in ten instances and moderate in one) with TVS in 90.0% (10/11) of the women in whom this finding was subsequently confirmed at hysteroscopy. The sensitivity, specificity, PPV, and NPV of transvaginal US were 91, 100, 100, and 98.5%, respectively. Hysteroscopic findings were considered the reference . They concluded that TVS , which is a noninvasive and relatively inexpensive procedure, seems to be effective in screening for uterine adhesions in a population at risk [19].
Narayan and Goswamy [20] correlated preoperative TVS (performed on days 7, 14, and 21 in spontaneous ovulatory cycles) with hysteroscopic findings (performed in the subsequent cycle) in 200 patients being investigated for infertility . A total of 182 patients were diagnosed correctly to have an abnormality by TVS giving a false-positive rate of 5.5%. The sensitivity and PPV of TVS in detecting endometrial pathology were 98.9 and 94.3%, respectively, with a PPV of 98.5% for the detection of intrauterine adhesions and a strong correlation between findings from transvaginal sonography and hysteroscopy. The authors concluded that TVS may be used to detect intrauterine pathology and identify patients in whom hysteroscopy and hysteroscopic surgery are indicated [20]. With further advance in ultrasound technology , Knopman and Copperman [21] assessed the value of three-dimensional (3D) ultrasound in the management of patients with suspected Asherman’s syndrome in a case series of 54 infertile patients who presented with suspected Asherman’s syndrome . Intrauterine adhesions (IUAs) were demonstrated on 3D ultrasound and HSG in all cases and confirmed by hysteroscopy. They reported 100% sensitivity with 3D ultrasound for correctly grading the extent of IUAs compared to only 66.7% for HSG. In 61.1% of cases in which HSG results were inconsistent with hysteroscopy, lower uterine segment outflow obstruction was present , and HSG misclassified findings as severe Asherman’s with complete cavity obstruction. With a postoperative conception rate of 90%, the authors concluded that 3D ultrasound provides a more accurate depiction of adhesions and extent of cavity damage than HSG in patients with suspected Asherman’s syndrome, particularly when differentiating severe IUAs from lower uterine segment outflow obstruction. Therefore, grading systems utilizing HSG to classify severity of disease should be revised to include 3D ultrasound findings [21].
Sonohysterography , a simple ultrasound (US) procedure technique, involves placement of a 5-F catheter into the endometrial canal with subsequent instillation of sterile saline solution under US guidance. Saline infusion offers a good contrast, enabling improved visualization and distinction between diffuse and focal abnormalities. Sonohysterography has been shown to be a safe, simple, and cost-effective outpatient method for evaluating the potentially abnormal endometrium using transvaginal ultrasound (US) in an outpatient setting and to plan the next step in case management [22]. Besides the cost-related issues, it has been indicated as a well-tolerated technique with a short learning curve in the diagnosis of abnormal uterine bleeding (premenopausal and postmenopausal), bleeding while using tamoxifen, suspected congenital uterine abnormality, and Asherman’s syndrome [23]. According to Badu-Peprah et al. [24], sonohysterography is an affordable and feasible diagnostic modality in developing nations for evaluating the endometrial cavity that should be used more often where equipment and skill permit [24], thereby obviating the need for laparoscopy and hysteroscopy in the majority of cases [25]. In a very recent study, Kowalczyk et al. [26] reported real-time 3D sonohysterography (SIS 3D) to be a minimally invasive advance to conventional 2D sonohysterography (sensitivity 72% and specificity 96%) that enables a three-dimensional image of the uterine cavity and enables examination of endometrial lesions with a sensitivity and specificity of 83 and 99%, respectively, and a diagnostic precision similar to the results achieved by hysteroscopy [26].
In a prospective study on 65 infertile women 19–43 years of age, Soares et al. [27] compared the diagnostic accuracy of sonohysterography (SHG) in uterine cavity diseases in infertile patients with that of HSG and TVS, using hysteroscopy as the gold standard . Sonohysterography and HSG had a sensitivity of 75% in the detection of intrauterine adhesions and respective PPVs of 42.9 and 50%, while TVS showed a sensitivity and PPV of 0% for this diagnosis. The authors concluded that while sonohysterography was in general the most accurate test with a markedly superior diagnostic accuracy for polypoid lesions and endometrial hyperplasia (EH) , with total agreement with the gold standard, however, in diagnosis of intrauterine adhesions, SHG had limited accuracy, similar to that obtained by HSG, with a high false-positive diagnosis rate [27]. Makris et al. [28] compared 3D hysterosonography (3D HS) and diagnostic hysteroscopy in 242 women with abnormal uterine bleeding. They reported a similar specificity (99.4%) but a higher sensitivity for hysteroscopy compared to 3D HS (98.7% vs. 93.5%, respectively). The PPV and NPV of 3D HS were 98.6 and 97%, respectively, compared to 98.7 and 99.4% for hysteroscopy, respectively. The 2 techniques were in agreement for 8 cases of adhesions and in 165 cases of normal endometrium [28].
de Kroon et al. [23] evaluated the accuracy of minimal invasive saline contrast hysterosonography (SCHS) i n the diagnosis of uterine pathology . They reported that this technique can detect intracavity abnormalities (with a prevalence of 54%) with a sensitivity, specificity, PPV, and NPV of 94, 89, 91, and 92%, respectively, and in combination with endometrial sampling, whenever indicated, it might be able to replace diagnostic hysteroscopy as the gold standard in the evaluation of the uterine cavity in 84% of the diagnostic hysteroscopies as SCHS is two to nine times cheaper than diagnostic hysteroscopy . However, SCHS fails more frequently in postmenopausal women than premenopausal women (12.5% vs. 4.7%; p = 0.03), and the chance of a non-conclusive SCHS is 7.6%, being higher if the uterine volume is greater than 600 cm3 (relative risk, 2.63; 95%-CI, 1.05–6.60) and if two or more myomas are present: (RR, 2.65; 95%-CI, 1.16–6.10) [23].
Yucebilgin et al. [29] reported a sensitivity, specificity, positive, and negative predictive values of 85, 75, 75, and 84%, respectively, for hydrosonography in the detection of structural endometrial cavity lesions where 45 (85%) of 53 women, who were supposed to have normal findings on hydrosonography, were confirmed by hysteroscopy. They, however, suggested that hydrosonography may be a useful tool in the evaluation of intrauterine cavity structural pathologies in infertile patients with the exception of intrauterine adhesions [29].
Alborzi et al. [30] compared the diagnostic accuracy of hysterosalpingography and sonohysterosalpingography in detecting tubal and uterine abnormalities with surgical findings as the gold standard . They reported a sensitivity, specificity , positive predictive value, and negative predictive value of 78.2, 93.1, 82.7, and 91%, respectively, for the detection of total tubal and uterine pathologies compared to 76.3, 81.8, 90.9, and 59.2%, respectively, for HSG. They concluded that sonohysterosalpingography is a safe, easy, and promising procedure and more accurate than hysterosalpingography for detecting intrauterine adhesions and various forms of uterine anomalies [30].
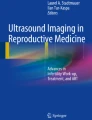
There have been reports of MRI appearances in four cases of Asherman’s syndrome in which the diagnosis was confirmed by hysteroscopy. However, the full range of MRI appearances in Asherman’s syndrome has not been established, and there has been only one case reported in the literature [31]. Figure 11.1 shows intrauterine adhesions using a multiplanar view after sonohysterography.

Saline sonogram showing intrauterine adhesions
Risk Factors for IUA
Mo et al. investigated the risk factors for intrauterine adhesions in patients with artificial abortion and clinical efficacy of hysteroscopic dissection [32]. 1500 patients undergoing artificial abortion between January 2014 and June 2015 were enrolled into this study. The incidence rate for intrauterine adhesions following induced abortion is 17.0%. Univariate analysis showed that preoperative inflammation, multiple pregnancies, and suction evacuation time are the influence risk factors of intrauterine adhesions. Multiple logistic regression demonstrates that multiple pregnancies, high intrauterine negative pressure, and long suction evacuation time are independent risk factors for the development of intrauterine adhesions following induced abortion. Additionally, intrauterine adhesions were observed in 105 mild, 80 moderate, and 70 severe cases. The cure rates for these three categories of intrauterine adhesions by hysteroscopic surgery were 100.0%, 93.8%, and 85.7%, respectively. The authors concluded that multiple pregnancies, high negative pressure suction evacuation, and long suction evacuation time are independent risk factors for the development of intrauterine adhesions following induced abortions [32].
Of 167 women treated for RPOC, 84 (50.3%) had undergone a follow-up hysteroscopic evaluation after the operative hysteroscopy and were included in the study [33]. Intrauterine adhesions were found in 16 cases (19.0%), of which only 3 (3.6%) were severe adhesions. Multivariate analysis showed that the presence of IUA was associated with RPOC after cesarean section (5 of 10 [50.5%] developed IUA, vs. 7 of 49 [14.3%] after vaginal delivery). Intrauterine adhesions were also found in 4 of 23 women (17.4%) undergoing hysteroscopy for RPOC after abortion. Patient age, gravidity, parity, and the interval between the index pregnancy and treatment for RPOC were not associated with postoperative IUA. Hysteroscopic treatment for RPOC had a 3.6% incidence of severe intrauterine adhesions formation in this descriptive series [33]. Women with RPOC occurring after delivery by cesarean section are particularly at risk for development of IUA [33].
Laparotomic myomectomy is often the only realistic solution for symptomatic women with multiple or large myomas who wish to retain their fertility. The aim of a recent study was to document the rate of uterine synechiae and their associated risk factors after laparotomic myomectomy [34]. This prospective observational study took place in a teaching hospital from May 2009 to June 2014. It included all women aged 18–45 years who had laparotomic myomectomies (without diagnostic hysteroscopy at the time of surgery) for myomas and a postoperative diagnostic office hysteroscopy 6–8 weeks later. The study included 98 women with a laparotomic myomectomy and a postoperative hysteroscopic follow-up. Women with a laparotomic myomectomy for a subserosal myoma were excluded. The intrauterine adhesion rate after laparotomic myomectomy was 25.51% (25/98); 44% (11/25) of them were complex intrauterine adhesions. Opening the uterine cavity was a major risk factor for these complex adhesions, with an OR of 6.42 (95% CI 1.27–32.52). Office hysteroscopy could be carried out after surgery in such cases [34].
Management of IUA
Diagnosis and treatment of intrauterine adhesions are integral to the optimization of fertility outcomes [15]. Surgical management of IUA presents a challenge to the hysteroscopic surgeon. Though the appropriate management is controversial [3], and more often than not, guided by the clinician’s choice , skill, and operative setting, hysteroscopic adhesiolysis with antibiotic prophylaxis followed by the use of postoperative adjuvants such as systemic estrogens and intrauterine devices or systems designed to impede the development of adhesions is the treatment of choice with favorable results in terms of pregnancy and live birth rates [3, 15, 35, 36]. Clinicians should maintain a level of suspicion of intrauterine adhesions and should investigate by hysteroscopy if necessary [35]. Non-hysteroscopic techniques are also beginning to be developed, but whether they will replace the current “gold” standard of hysteroscopy remains to be seen [37]. The success of treatment regarding term deliveries and rate of abortions depends on the severity of the adhesions, and pregnancy, when achieved, may be complicated by premature labor, placenta previa, and placenta accreta [36].
Hysteroscopic Surgery
Technological progress in optic fibers and instrumentation has made it possible to video endoscope and determine the fibrous nature of the lesions and its precise localization and control endocavitary surgeries such as hysteroscopic adhesiolysis for uterine synechiae [38]. Though sonohysterography and hysterosalpingography are useful as screening tests of intrauterine adhesions [15], hysteroscopy has been considered the mainstay of diagnosis, classification, and treatment of the intrauterine adhesions, with medical treatments having no role in management [1, 2, 4, 15, 35, 39]. Diagnostic and therapeutic hysteroscopy is a simple, feasible, safe, reproducible, effective, quick, well-tolerated, and low-cost surgical procedure that is highly successful in an outpatient setting, offering a see-and-treat approach in majority of the subjects with intrauterine adhesions [40, 41]. Hysteroscopy has also become accepted as the optimum route of surgery, the aim being to restore the size and shape of the uterine cavity, normal endometrial function, and fertility [15, 16]. Lysis of intrauterine adhesions, for the treatment of infertility and recurrent pregnancy loss, results in improved fecundability and decreased pregnancy loss. Though adhesiolysis for pain relief appears efficacious in certain subsets of women, unfortunately, even when lysed, adhesions have a great propensity to reform [16]. According to Bettocchi et al. [41], there is no consensus on the effectiveness of hysteroscopic surgery in improving the prognosis of subfertile women. However, office hysteroscopy is a powerful tool for the diagnosis and treatment of intrauterine benign pathologies, and in patients with at least two failed cycles of assisted reproductive technology, diagnostic hysteroscopy and, if necessary , operative hysteroscopy are mandatory to improve reproductive outcome [41]. A descriptive study (Canadian Task Force classification II-2) concluded that hysteroscopic adhesiolysis is an effective and safe option even for postmenopausal women with intrauterine lesions adhesions on hysteroscopy or ultrasound. It allows the correct diagnosis to be made, reduces the need for major and unnecessary surgery, and is therapeutic in most patients [42].
Treatment can range from simple cervical dilatation in the case of cervical stenosis, but an intact uterine cavity, to extensive adhesiolysis of dense intrauterine adhesions using scissors, electro- or laser energy, or a combination of blunt and sharp dissection [34, 37]. Various techniques for adhesiolysis and for prevention of scar reformation have been advocated. According to March [2], the use of miniature scissors for adhesiolysis and the placement of a balloon stent inside the uterus immediately after surgery appear to be the most efficacious [2]. Patients with more severe adhesions, in whom the uterine fundus is completely obscured, and those with a greatly narrowed fibrotic cavity present the greatest therapeutic challenge. Several techniques have been described for these difficult cases , but the outcome is far worse than in patients with mild, endometrial-type adhesions [4, 37]. A significantly obliterated cavity may require multiple hysteroscopic adhesiolysis to achieve a satisfactory anatomical and functional result [15, 39], while laparoscopic or ultrasound guidance may aid in the hysteroscopic lysis of dense scar tissue and difficult entry into the cervix [1].
Treatment Outcome
Treatment outcomes are difficult to assess as there is no universally agreed upon classification system [1]. Anatomic, but most of all functional prognosis, is directly correlated to the severity of adhesions, and the number of surgical procedures required to complete treatment [43].
Restoration of menstruation is highly successful (more than 90%), and pregnancy rates around 50–60% with live birth rates around 40–50% can be achieved [35]. The risk of complications for those that achieve pregnancy is significant with a significant risk for placenta accreta and subsequent blood loss, transfusion, and hysterectomy [12]. In perhaps the largest study, involving 6680 hysteroscopies with hysteroscopic adhesiolysis in 75 patients, 94.6% functional restoration and 93.3% anatomic resolution, with pregnancy rates ranging from 28.7% to 53.6%, were achieved. At 2-month follow-up, the uterine cavity was completely regular in 70 cases, while in four cases, a second surgical treatment was necessary [44].
Using a standard technique with a loop electrode and glycine 1.5% as distension medium, Dawood et al. [12] reported an improvement in the rate of amenorrhea from 32.3% before adhesiolysis to 9.2% after the procedure with an overall pregnancy rate of 51.2% and the live birth rate 32.6% among women who wished to conceive. Severe intrauterine adhesions were managed with the assistance of abdominal ultrasound to ensure that the uterine cavity was not breached, and the rates of pregnancy and term pregnancy among this selected group of women were similar regardless of the severity of adhesions [12].
Yu et al. [45] evaluated the outcome of hysteroscopic adhesiolysis with electrode needle or loop under direct vision in 85 women with Asherman’s syndrome who presented with a history of infertility or recurrent pregnancy loss. After hysteroscopic adhesiolysis, the chances of conception among the 18.2% of women who remained amenorrheic were significantly lower than those who continued to have menses (50%). The conception rate in women who had reformation of intrauterine adhesions at second-look hysteroscopy (11.8%) was significantly lower than that of women who had a normal cavity (59.1%), suggesting that the outcome of hysteroscopic adhesiolysis for Asherman’s syndrome is significantly affected by recurrence of intrauterine adhesions [45].
Hysteroscopic adhesiolysis with monopolar or bipolar energy can be performed safely and effectively for severe stage III and IV adhesions with a 97% restoration of menses, 43.8% PR, and 32.8% LBR. The pregnancy rate was significantly higher in patients ≤35 years compared to patients older than 35 years (66.6% vs. 23.5%, respectively; p = 0.01), suggesting that age is the main predictive factor of success: the pregnancies were at risk of abnormal placentation [46]. The impact of age on the outcome of hysteroscopic adhesiolysis is in agreement with a previous study by Capella-Allouc et al. [47] that reported a pregnancy rate of 42.8%, live birth rate of 32.1%, the pregnancy rate being much higher in patients ≤35 years compared to patients older than 35 years (62.5% vs.16.6%, respectively; p = 0.01) following hysteroscopic adhesiolysis in 31 patients with severe Asherman’s syndrome. However, these pregnancies were at risk for hemorrhage with abnormal placentation [47].
Roy et al. [10] reported an overall conception rate of 40.4%, live birth rate of 86.1%, and a miscarriage rate of 11.1% in a mean conception time after surgery of 12.8 months following hysteroscopic adhesiolysis with the monopolar electrode knife in 89 infertile patients with Asherman’s syndrome . The cumulative pregnancy rate showed that 97.2% of patients conceived within 24 months. The conception rate was higher (58%) in mild Asherman’s syndrome compared to 30% conception rate in moderate and 33.3% conception rate in severe cases. There was a significantly higher likelihood of conception (44.3%) in those who continued to have improved menstrual pattern compared to only 10% likelihood of conception in those who continued to have amenorrhea after adhesiolysis. A second-look office hysteroscopy, performed after 2 months, showed reformation of adhesions in 12 patients that needed a repeat adhesiolysis with no conception in these patients. The authors concluded that hysteroscopic adhesiolysis for Asherman’s syndrome is a safe and effective method of choice for restoring menstrual function and fertility [10].
Shokeir et al. [48] attempted to analyze the adhesion grade in multiple hysteroscopic-guided biopsies from IUA following the initial hysteroscopic adhesiolysis at a follow-up diagnostic hysteroscopy , performed early (2–4 weeks) after the initial operation or late, about 12 months (8–16 months). They observed that at follow-up hysteroscopy, 25% of both groups had no significant adhesions. Grade I adhesions (thin, filmy) occurred in 60% of the early hysteroscopy patients and in only 12% of the late group (P < 0.05). Grade II adhesions were present in 10% of the early group and in up to 41% in the late group (P < 0.05), whereas grade III adhesions were present in only 5% of the early hysteroscopy group but in 22% of the late one (P < 0.05). Correlation between hysteroscopic and histologic findings were good in most of cases in both groups. The follow-up to determine the subsequent reproductive outcome revealed similar conception rates in both groups. The authors suggested that the IUA that might be formed immediately following hysteroscopic reproductive surgery is histologically different from those appearing a longer time after the original operation. Routine early follow-up hysteroscopy can influence the prognosis resulting from the original surgery [48].
Having excluded hormonal imbalances, premature ovarian failure, and congenital uterine abnormalities, Yasmin et al. [49] reported thick fibrous adhesions in 45% of patients, flimsy adhesions in 40%, and muscular adhesions in 15% at hysteroscopy, with 65% adhesions in the body of uterus, 25% at the site of internal os, and 1% adhesions in the cervical canal as well as the body of the uterus. Following diagnostic hysteroscopy and resection of adhesions in 20 patients (median age 26 years), presenting with scanty menses and secondary infertility (65%), secondary amenorrhea (20%), or primary infertility alone (15%), they reported a restoration of menses in 95% of the patients and conception in 10% of the patients. Though the patient number was small, the authors suggested that hysteroscopy is not only an effective procedure for diagnosing Asherman’s syndrome but is equally effective for treating it [49].
Hysteroscopic adhesiolysis in women with Asherman’s syndrome and poor reproductive performance (previous spontaneous abortions or a premature delivery) contributes significantly to a successful reproductive outcome. Whereas pregnancy outcome prior to the hysteroscopic adhesiolysis was 18.3% term deliveries, 3.3% premature deliveries, 62.4% first-trimester abortions, and 16.0% late abortions, after hysteroscopic adhesiolysis, the pregnancy outcome was 68.6% term deliveries, 9.3% premature deliveries, 17.4% first-trimester abortions, and 4.7% late abortions. The operative success rate, measured by delivering a healthy newborn, improved from 18.3% preoperatively to 64% postoperatively in women with two previous unsuccessful pregnancies [50], whereas in women with three or more unsuccessful pregnancies, the success rate improved from 18.3% to 75%. Successful outcome of adhesiolysis was observed in 61.9% of mild (stage I) and in 70.6% of moderate-to-severe cases (stages II and III) of intrauterine adhesions [50].
Blunt adhesiolysis with a flexible hysteroscope, following primary treatment of intrauterine adhesions with sharp adhesiolysis, has been suggested as an effective technique for the maintenance of cavity patency with an improvement in menstrual flow in 95% of the patients, relief of dysmenorrhea in 92%, 92% improvement in disease staging over the treatment interval, and a pregnancy rate of 46%. Initially, 50% had severe adhesions, 46% had moderate, and 4% had minimal disease according to the March criteria [51].
Colacurci et al. [52] analyzed the reproductive outcome in 53 women undergoing hysteroscopic lysis of intrauterine adhesions, according to their localization and severity. Hysteroscopic surgery restored an acceptable menstrual cycle in almost all the patients affected by intrauterine isolated adhesions in 52% of women with complex incomplete adhesions and in none of the patients with an entirely obliterated cavity. In isolated, isthmic, central, or marginal synechiae, a pregnancy rate of 73.3% was observed with a pregnancy rate to term, respectively, of 63.3% and of 86.3%, while in case of complex but not complete adhesions, the pregnancy rate was 25% with only two term pregnancies. There were no pregnancies in three cases of complex synechiae. The authors concluded that the basic parameter to define the functional and reproductive prognosis of the hysteroscopic lysis of intrauterine adhesions is not the menstrual profile or the histological characteristic of the lesions but rather their extension [52].
Hysteroscopy and hysteroscopic surgery have been the gold standard of diagnosis and treatment, respectively, for patients with Asherman’s syndrome who presented with amenorrhea or hypomenorrhea , infertility, or recurrent pregnancy loss. However, according to most authors, despite the advances in hysteroscopic surgery, the treatment of moderate-to-severe Asherman’s syndrome still presents a challenge [43, 53]. Furthermore, pregnancy after treatment remains high risk with complications including spontaneous abortion, preterm delivery, intrauterine growth restriction, placenta accreta or previa, or even uterine rupture that necessitate close antenatal surveillance and monitoring for women who conceive after treatment [53]. According to Piketty et al. [43] despite the infrequent but well-known complications during surgery and the less frequent but often severe obstetrical complications , the benefit gained by the recovery of fertility (either spontaneous or not) remains superior to the risks of the surgical management [43].
Role of Ultrasonography in the Treatment
Serial intrauterine device-guided hysteroscopic adhesiolysis of intrauterine synechiae, especially for early intervention, may prevent complications during the treatment of severe intrauterine adhesions and may present a secure and effective alternative for constructive clinical outcomes with spontaneous pregnancy rates of 47.2 and 30% and live birth rates of 28 and 20% in patients who did and did not undergo early intervention of office hysteroscopy, 1 week after insertion of the IUD at hysteroscopic adhesiolysis, respectively [54]. Following echo-controlled hysteroscopic surgical cure of complex and/or recurrent uterine synechiae in 11 patients, Salat-Baroux et al. [38] concluded that intraoperative echography allowed hysteroscopic adhesiolysis of intrauterine adhesions at a controlled and equivalent distance from the uterine walls, enabling better treatment of the uterine cornua since the operator is informed when to limit progression to avoid massive fluid infusion into the abdominal cavity and perforation of the uterus. The intraoperative echographic control was validated in the operating theater radiographically. With this technique normal cavities with bilateral tube permeability were obtained in 72.72% of the patients and normal cycles in 90.9% of the patients [38]. Following hysteroscopic lysis under ultrasound control for significant intrauterine synechiae, Bellingham [55] reported normal menstruation in 61% of the patients and live births in 80% of the patients, of whom 50% had had severe adhesions. They reported that ultrasound control is ideally essential if the adhesions are extensive [55]. However, in both these studies, the number of patients was very small to effectively document the role of ultrasound in the treatment of IUA.
Coccia et al. [56] described a new therapeutic procedure called pressure lavage under ultrasound guidance (PLUG) for selected cases of IUA. This technique is based on sonohysterography to monitor the effects of intrauterine injections of saline solution on the continuous accumulation of saline in the uterine cavity for the mechanical disruption of IUA. In an open clinical investigation with no control group , they reported satisfactory lysis of adhesions and restoration of menses in 71.4% of the patients with mild IUA with a pregnancy rate of 66.63% following the use of the PLUG technique. A second-look hysteroscopy after 1 month showed the persistence of filmy adhesions in two patients with moderate IUA that were removed successfully during hysteroscopy. The authors suggested that PLUG is a safe and ideal in-office procedure that allows complete lysis in mild IUA cases avoiding the need for therapeutic and, possibly, follow-up hysteroscopy and may represent a useful initial step in moderate IUA cases reducing the need for operative hysteroscopy [56]. In a recent study, Taniguchi and Suginami [57] also suggested that sonohysterographic (SHG) lysis for recurrent adhesions following hysteroscopic lysis may be a treatment option for recurrent adhesions in infertile patients, with improved menstrual cycles and restored tubal patency [57].
Tiras et al. [58] demonstrated the value of laparoscopic intracorporeal ultrasound (LIU)-guided hysteroscopic adhesiolysis in a patient with amenorrhea and infertility with total intrauterine synechiae. Adequate intrauterine adhesiolysis was performed by a resectoscope with a wire loop, suggesting that complex intrauterine procedures can be easily performed by the guidance of endoscopic ultrasonography to avoid the possibility of inadvertent uterine perforation [58].
Schlaff and Hurst [59] evaluated the predictive value of preoperative endometrial sonography in the diagnosis and surgical treatment of women with amenorrhea due to severe Asherman’s syndrome , characterized by complete obstruction of the cavity at hysterosalpingogram . They suggested that an endometrial pattern, demonstrating a well-developed endometrial stripe on transvaginal sonography, is highly predictive of a positive surgical and clinical outcome in women with severe Asherman’s syndrome with resumption of normal menses and normalization of the cavity after hysteroscopy in contrast to women with minimal endometrium who had no cavity identified and derived no benefit from surgery [59]. However, this study was limited to just seven patients, and hence, substantial evidence in this direction is lacking.
Radiographic Methods
In a small but significant study, Karande et al. [60] demonstrated that in-office lysis of intrauterine adhesions, under fluoroscopic control, using a specially designed catheter (gynecoradiologic control), can be carried out safely in the majority of patients, using minimally invasive techniques. They could successfully lyse adhesions in 76% (13/17) of the patients (9 mild, 3 moderate, and 1 severe), while in remaining 4 patients (2 moderate and 2 severe), lysis was only partially successful . Nine procedures were performed with the catheter’s balloon tip and four with hysteroscopic scissors. Procedure complications resulting in the abandoning of the procedure included patient discomfort before attempting the use of scissors (n = 1), extravasation of dye into the myometrium making visualization difficult (n = 1), and thick, fibrotic adhesions that were resistant to scissors (n = 2). They opined that the potential cost savings with this technique in comparison with endoscopic procedures, which require utilization of expensive operating room time, are especially relevant in a cost-conscious managed care environment and only failures of in-office procedures would reach the operating room [60]. The fluoroscopic approach to adhesions was further evaluated a decade later by Chason et al. [61] who used hysteroplasty with fluoroscopic cannulation and balloon uterine dilation to treat intrauterine adhesions and cervical stenosis and lower uterine defects in select cases. They concluded that while the treatment of intrauterine adhesions resulted in an improved pregnancy outcome, albeit in a case study, the effect of lower uterine segment-filling defects from cesarean deliveries on pregnancy outcome in assisted reproductive technology cycles warrants further investigation [61]. In a 5-year retrospective, uncontrolled cohort study, Thomson et al. [62] conducted fluoroscopically guided hysteroscopic synechiolysis for Asherman’s syndrome in 30 patients (13% AFS grade I, 43% AFS grade II, and 43% AFS grade III), 60% of whom were amenorrheic. They reported a 96% restoration of regular menses with a 53% pregnancy rate among patients who attempted to conceive and concluded that hysteroscopic synechiolysis, performed by injecting radiographic contrast medium and visualized under image-intensifier control, followed by cyclic high-dose estrogen therapy to stimulate endometrial proliferation , appears to be an effective treatment for Asherman’s syndrome. Repeat procedures were performed monthly until the endometrial cavity was reestablished [62].
Prevention of IUA
One of the most important features of treatment for intrauterine synechiae is the prevention of recurrence [4]. Follow-up studies to assure resolution of the scarring are mandatory before the patient attempts to conceive as is careful monitoring of pregnancies for cervical incompetence, placenta accreta, and intrauterine growth retardation [2]. The best available evidence demonstrates that the newly developed adhesion barriers, such as hyaluronic acid, show promise for preventing new adhesions [4, 15]. Postoperative mechanical distention of the endometrial cavity with the use of intrauterine contraceptive devices and postoperative hormonal treatment with estrogen +/− progestogen to facilitate endometrial regrowth are important in the prevention of recurrence [15, 35].
With regard to primary adhesion formation, a recent study by Rein et al. [63] demonstrated that selective hysteroscopic resection (HR) of residual trophoblastic tissue after first- or second-trimester miscarriage or term delivery significantly reduces the incidence of intrauterine adhesions and increases pregnancy rates compared to ultrasound-guided evacuation with a curette (D&E). They reported mild adhesion in 4.2% of the patients after selective HR compared to an incidence of 30.8% after D&E, of which 17.9% were mild, 7.7% single dense adhesions, and 2.6% with extensive endometrial fibrosis. Conception rates were significantly higher in the HR patients compared to curetted patients (68.8% vs. 59.9%, respectively; p < 0.05) and 78.1% vs. 66.6%, respectively; p < 0.05 in patients younger than 35 years of age with a significantly (p < 0.05) shorter time to conception (11.5 months vs. 14.5 months) [63]. Operative hysteroscopy for selective curettage of residual trophoblastic tissue instead of nonselective conventional curettage may prevent intrauterine adhesions [39].
Mechanical Barriers
The efficiency of barrier agents’ postoperative hysteroscopic adhesiolysis to prevent the recurrence of adhesions has been addressed in a few clinical trials. Barrier agents have been grouped under mechanical agents (intrauterine device-IUCD, Foley catheter), fluid agents (Seprafilm, Hyalobarrier, auto-cross-linked hyaluronic acid [ACP] gel), postoperative systemic treatment (cyclic estrogen-progesterone therapy), and the latest tissue barriers (fresh or dries amnion grafts).
Several comparative studies, evaluating the efficacy of various barrier agents, have been conducted. Orhue et al. [64] compared two adjunctive treatments following intrauterine adhesiolysis—the intrauterine contraceptive device (IUCD) and the Foley catheter. In a 4-year initial period, patients with intrauterine adhesions were treated with the insertion of an IUCD after adhesiolysis . In the next 4 years, a pediatric Foley catheter balloon was used after adhesiolysis instead of the IUCD. They reported a significantly higher restoration of normal menstruation (81.4% vs. 62.7%, p < 0.05), less frequent persistent posttreatment amenorrhea and hypomenorrhea (18.6% vs. 37.3%; P < 0.03), a higher conception rate (33.9% vs. 22.5%), and a significantly lesser need for repeated treatment in the Foley catheter group compared to the IUCD group, respectively. They concluded that the Foley catheter is a safer and more effective adjunctive method of treatment of IUA compared with the IUCD [64].
Fluid Barriers
The application of auto-cross-linked hyaluronic acid (ACP) gel has been reported to significantly reduce the incidence and severity of de novo formation of intrauterine adhesions after hysteroscopic surgery, with a significant decrease in adhesion severity on staging of adhesions [65].
Tissue Barriers
The role of amnion grafts as barrier agents to prevent recurrence of adhesions has currently gained a lot of attention. In a pilot study involving 25 patients with moderate or severe intrauterine adhesions , Amer et al. [66] reported that hysteroscopic adhesiolysis followed by intrauterine application of a fresh amnion graft over an inflated balloon of a Foley catheter for 2 weeks seems to be a promising procedure for decreasing recurrence of adhesions and encouraging endometrial regeneration. They reported failure to achieve normal menstrual flow in 16.7% of the patients with moderate versus 23.1% of the patients with severe adhesions and observed adhesion reformation at follow-up hysteroscopy in 48% of the patients, all with severe adhesions. However, randomized comparative studies are needed to validate its benefits, including reproductive outcome [66].
In a more recent pilot prospective randomized comparative study (Canadian Task Force classification I), Ameret et al. [67] estimated the efficacy of inserting fresh and dried amnion graft after hysteroscopic lysis of severe intrauterine adhesions in decreasing its recurrence and encouraging endometrial regeneration in 45 patients. Hysteroscopic lysis of intrauterine adhesions was followed by insertion of an intrauterine balloon only (group 1) or either fresh amnion graft (group 2) or dried amnion graft (group 3) for 2 weeks. Diagnostic hysteroscopy, performed at 2 to 4 months postoperatively, revealed significant improvement in adhesion grade with the amnion graft versus intrauterine balloon alone (p = 0.003) and significant improvement with fresh compared to dried amnion graft (p = 0.01). Restoration of normal menstruation (46.7% in group 3, 35.7% in group 2, 28.6% in group 1) and the conception rate (80% after amnion graft and 20% without amnion) was higher in patients with the graft compared to the balloon. The overall conception rate was 23.3% with a miscarriage rate of 60%. The authors concluded that hysteroscopic lysis of severe intrauterine adhesions with grafting of either fresh or dried amnion is a promising adjunctive procedure for decreasing recurrence of adhesions and encouraging endometrial regeneration [67].
Peng et al. set up a study to determine the safety and efficacy of amnion grafts in preventing the recurrence of intrauterine adhesions after hysteroscopic adhesiolysis in women with severe intrauterine adhesions [68]. A total of 120 patients underwent intrauterine adhesiolysis for severe intrauterine adhesions: 40 patients in the treatment group and 80 patients in the control group matched for age and adhesion scores. The mean duration of follow-up was 14.6 months. A Foley balloon with/without a fresh amnion graft was introduced into the uterine cavity after hysteroscopic adhesiolysis. In both groups, the balloon was kept in place for 7 days, cyclic hormone treatment was given for 3 months, and second-look and third-look hysteroscopies were performed 1 and 3 months after the operation. Outcome measures included the incidence of the recurrence of intrauterine adhesions, the score of intrauterine adhesions (if present), and the impact of the surgery on the amount of menstrual flow. In the study group, the menstrual score at the end of 3 months was significantly higher, and the intrauterine adhesion score at third-look hysteroscopy was significantly lower compared with those in the control group. The incidences of the recurrence of intrauterine adhesions at third-look hysteroscopy in the treatment and control groups were 30% and 48.7%, respectively (p = 0.05). The adhesion scores at third-look hysteroscopy in the treatment and control groups were 1.3 and 2.1, respectively (p < 0.05). The use of an amnion graft after intrauterine adhesiolysis appears to be beneficial in improving menstruation and reducing the recurrence of adhesion reformation [68].
Prevention Strategies
Prevention strategies, including bipolar resection, barrier gel, or postoperative estradiol, might be useful, but stronger evidence is needed, and there is a need for other randomized controlled trials to fully justify the use of adhesion barriers for clinical use [5, 9]. In view of the current knowledge, Gambadauro et al. [9] recommend a prevention strategy based on a combination of surgical trauma minimization and identification of high-risk cases, with early hysteroscopic diagnosis and lysis possibly representing the best means of secondary prevention and treatment of postoperative intrauterine adhesions [9]. Considering the decreased pregnancy outcome in patient with recurrence of adhesions, further research in Asherman’s syndrome should be directed toward reduction of adhesion reformation with a view to improving outcome [45].
Hooker et al. set up a study to examine whether intrauterine application of auto-cross-linked hyaluronic acid (ACP) gel , after dilatation and curettage (D&C) , reduces the incidence of intrauterine adhesions (IUAs) [69]. A total of 152 women with a miscarriage of <14 weeks with at least one previous D&C for miscarriage or termination of pregnancy were included. Women were randomly assigned to either D&C plus ACP gel (intervention group) or D&C alone (control group). A follow-up diagnostic hysteroscopy was scheduled 8–12 weeks after the D&C procedure. The primary outcome was the number of women with IUAs, and the secondary outcome was the severity of IUAs. Outcomes were available for 149 women: 77 in the intervention group and 72 in the control group. The IUAs were observed in 10 (13.0%) and 22 women (30.6%), respectively (relative risk, 0.43; 95% confidence interval, 0.22–0.83). Mean adhesion score and the amount of moderate-to-severe IUAs were significantly lower in the intervention group according to the American Fertility Society (AFS) and European Society of Gynecological Endoscopy classifications systems of adhesions. The authors concluded that intrauterine application of ACP gel after D&C for miscarriage in women with at least one previous D&C seems to reduce the incidence and severity of IUAs but does not eliminate the process of adhesion formation completely [69].
Risk of Recurrence of IUA After Hysteroscopic Adhesiolysis
Yang et al. investigated the recurrence potential of intrauterine adhesions after hysteroscopic adhesiolysis [70]. This study included 115 women who had intrauterine adhesions completely separated during hysteroscopic surgery. The treated adhesions were classified into four groups according to their location and extent: group 1, central type (i.e., intervening space between the adhesions and both lateral uterine sidewalls) at the middle area of uterine cavity; group 2, central type at uterine cornua; group 3, cervico-isthmic; and group 4, extensive if the adhesions were dense with occlusion of part of the uterine cavity other than cervico-isthmic region. Postoperative outpatient hysteroscopic adhesiolysis was scheduled 10–14 days after the initial hysteroscopic surgery, and procedures were repeated every 10–14 days until no reformed adhesions were detected. Multivariate logistic regression models were built to examine initial adhesion characteristics and other factors associated with adhesion reformation and need for subsequent outpatient adhesiolysis. Categorical data were compared using Fisher’s exact test. The location and extent of adhesions according to the allocated group was the only parameter independently related to the number of postoperative outpatient adhesiolysis procedures (P = 0.0004). Women with group 1 adhesions underwent a lower number of postoperative interventions compared with those with group 2, 3, and 4 adhesions (P = 0.0355, P = 0.0004, and P = 0.0087, respectively). There is an increased likelihood of intrauterine adhesion recurrence when successfully divided adhesions were originally located at the uterine cornua, the cervico-isthmic region or involved a large portion of the uterine cavity [70].
The aim of Xu et al.’s study was to assess the effect of early second-look hysteroscopy after hysteroscopic adhesiolysis for intrauterine adhesions (IUAs) on the pregnancy rate (PR) and live birth rate (LBR) (71). Of 151 women treated for IUAs, the general PR was 71.5%, and LBR was 53.0%. The PR and LBR were higher in the earlier second-look group (compared with second hysteroscopy later than 2 months group) and the group which received less than three times adhesiolysis (p < 0.05). The PR was higher in the amenorrhea group (compared with normal menses group) and recurrent miscarriage group (compared with infertility group) (p < 0.05). Logistic regression showed that the second-look time interval, times of operation to relieve adhesion, and pregnancy history were associated with the PR, while age and the second-look time interval were associated with the LBR. Early second-look hysteroscopic examinations within 2 months may increase the cumulative PR and LBR [71].
Recent Advances
Recently, the endometrium has been identified as a repository for anti-Mullerian hormone (AMH) , with endometrial masses associated with AMH serum levels. Promberger and Ott aimed to compare AMH levels, as well as other parameters for ovarian reserve, in women with endometrial trauma due to Asherman’s syndrome (AS) and matched controls [72]. In a retrospective study, nine women with hysteroscopically confirmed AS were compared to nine matched controls. Follicle-stimulating hormone, luteinizing hormone, and estradiol levels did not differ between women with and without AS, whereas significantly lower AMH levels were found in patients (median 0.50 pg/mL; IQR 0.25–0.75) than in controls (median 1.14 pg/mL; IQR 0.63–1.77; p = 0.026). The results suggest that decreased AMH levels in patients with AS do not necessarily indicate decreased ovarian reserve. The study is limited by the small sample size, and, thus, future research on the role of AMH in endometrial tissue and function are necessary to clarify the importance of these findings [72].
In an effort to treat injured endometrium nonresponsive to conventional treatment for Asherman’s syndrome (IUCD) with cyclical hormonal therapy for 6 months, Nagori et al. [73] demonstrated that placement of endometrial angiogenic stem cells in the endometrial cavity under ultrasound guidance after curettage followed by cyclical hormonal therapy can regenerate injured endometrium. These cells could be isolated from adult autologous stem cells isolated from a patient’s own bone marrow using immunomagnetic isolation [73]. Gargett and Healy [74] also reported regeneration of thin endometrium refractory to estrogen stimulation following intrauterine administration of bone marrow stem/progenitor cells sufficiently to support a pregnancy in a case study. However, whether its local endometrial damage is induced by concurrent curettage that stimulated endogenous endometrial stem/progenitor cells into action, or both, is open to question [74].
Recently, stem cell transplantation has been proposed to promote the recovery process. Gan et al. investigated whether human amniotic mesenchymal stromal cells (hAMSCs) , a valuable resource for transplantation therapy, could improve endometrial regeneration in rodent IUA models [75]. hAMSC transplantation promotes endometrial regeneration after injury in IUA rat models, possibly due to immunomodulatory properties. These cells provide a more easily accessible source of stem cells for future research into the impact of cell transplantation on damaged endometria [75].
There are few effective treatments due to the complex function of endometrium and shortage of native materials. 17β-estradiol (E2) is commonly used as an ancillary treatment in IUA patients, but it is limited by its poor solubility in aqueous solutions and low concentrations at the injured sites. In a recent publication, a mini-endometrial curette was used to injure the rat’s endometrium to form an IUA model [76]. 17β-estradiol was encapsulated into the micelles of heparin-poloxamer, and a thermosensitive hydrogel (E2-HP hydrogel ) was formed. This sustained releasing system was applied to restore the structure and function of the injured uterus. E2-HP hydrogel was constructed, and relevant characteristics including gelation temperature and micromorphology were evaluated. Sustained release of 17β-estradiol from HP hydrogel was performed both in vitro and in vivo. Ultrasonography measurement and pathologic characteristics on the IUA rats were performed to evaluate the therapeutic effect of E2-HP hydrogel. Endoplasmic reticulum (ER) stress-related apoptosis was analyzed to explore the possible mechanisms in IUA recovery. E2-HP hydrogel showed a prolonged release of E2 at the targeting region and more effective endometrium regeneration in IUA rats. Significant improvements in both gland numbers and fibrosis area were observed in the E2-HP hydrogel group [76]. The paper also demonstrated that E2-HP hydrogel in the recovery of IUA was closely related to the suppression of ER stress signals via the activation of downstream signals, PI3K/Akt and ERK1/2. HP hydrogel might be an effective approach to deliver E2 into the injured endometrium. Therapeutic strategies targeting ER stress using E2-HP hydrogel might be a promising solution for the treatment of women with intrauterine adhesions [76].
Conclusion
Intrauterine adhesions are a significant gynecological complication that requires prompt and accurate diagnosis and treatment. Despite its invasiveness, cost issues, and the technical skill required, hysteroscopy is recognized as the gold standard for the diagnosis, classification, and treatment of adhesions with an encouraging restoration of fertility in terms of menstruation, pregnancy rates, and live birth rates in patients with mild, moderate, and severe IUA, including postmenopausal women. Moreover, it offers a see-and-treat approach in majority of the patients where therapy is required, thus obviating the need for a second intervention. Though ultrasonography is gradually gaining acceptance in the diagnosis of IUA, particularly in economically compromised settings, with the purpose of avoiding costly invasive techniques, it has limited accuracy and sensitivity in the diagnosis of IUA compared to hysteroscopy. The addition of 3D ultrasound is reported to have improved accuracy in the diagnosis, but consistent large-scale studies are lacking. However, with regard to treatment, ultrasound may have a significant role in controlling hysteroscopic surgery, especially in patients with complex severe adhesions, to avoid inadvertent uterine perforation. More large-scale randomized trials will be required before ultrasonography can be established as a more functionally effective alternative to hysteroscopy in the diagnosis and treatment of IUA.
References
Berman JM. Intrauterine adhesions. Semin Reprod Med. 2008;26(4):349–55.
March CM. Asherman’s syndrome. Semin Reprod Med. 2011;29(2):83–94.
Fedele L, Bianchi S, Frontino G. Septums and synechiae: approaches to surgical correction. Clin Obstet Gynecol. 2006;49(4):767–88.
Deans R, Abbott J. Review of intrauterine adhesions. J Minim Invasive Gynecol. 2010;17(5):555–69.
Revaux A, Ducarme G, Luton D. Prevention of intrauterine adhesions after hysteroscopic surgery. [Article in French]. Gynecol Obstet Fertil. 2008;36(3):311–7.
Westendorp IC, Ankum WM, Mol BW, Vonk J. Prevalence of Asherman’s syndrome after secondary removal of placental remnants or a repeat curettage for incomplete abortion. Hum Reprod. 1998;13(12):3347–50.
Salzani A, Yela DA, Gabiatti JR, Bedone AJ, Monteiro IM. Prevalence of uterine synechia after abortion evacuation curettage. Sao Paulo Med J. 2007;125(5):261–4.
Khanna A, Agrawal A. Markers of genital tuberculosis in infertility. Singapore Med J. 2011;52(12):864–7.
Gambadauro P, Gudmundsson J, Torrejón R. Intrauterine adhesions following conservative treatment of uterine fibroids. Obstet Gynecol Int. 2012;2012:853269.
Roy KK, Baruah J, Sharma JB, Kumar S, Kachawa G, Singh N. Reproductive outcome following hysteroscopic adhesiolysis in patients with infertility due to Asherman’s syndrome. Arch Gynecol Obstet. 2010;281(2):355–61.
Tam WH, Lau WC, Cheung LP, Yuen PM, Chung TK. Intrauterine adhesions after conservative and surgical management of spontaneous abortion. J Am Assoc Gynecol Laparosc. 2002;9(2):182–5.
Dawood A, Al-Talib A, Tulandi T. Predisposing factors and treatment outcome of different stages of intrauterine adhesions. J Obstet Gynaecol Can. 2010;32(8):767–70.
Sharma JB, Roy KK, Pushparaj M, Gupta N, Jain SK, Malhotra N, Mittal S. Genital tuberculosis: an important cause of Asherman’s syndrome in India. Arch Gynecol Obstet. 2008;277(1):37–41.
Poujade O, Grossetti A, Mougel L, Ceccaldi PF, Ducarme G, Luton D. Risk of synechiae following uterine compression sutures in the management of major postpartum haemorrhage. BJOG. 2011;118(4):433–9.
Kodaman PH, Arici A. Intra-uterine adhesions and fertility outcome: how to optimize success? Curr Opin Obstet Gynecol. 2007;19(3):207–14.
Diamond MP, Freeman ML. Clinical implications of postsurgical adhesions. Hum Reprod Update. 2001;7(6):567–76.
Bonilla-Musoles F, De Velasco LA, Osborn NG, MacHado LE, Flores DP, MacHado FR, Bonilla F Jr. Two-dimensional and three-dimensional ultrasound differential diagnosis of endometrial hyperplasia and endometrial adenocarcinoma. J Gynecol Surg. 2003;19(3):105–20.
El-Mazny A, Abou-Salem N, El-Sherbiny W, Saber W. Outpatient hysteroscopy: a routine investigation before assisted reproductive techniques? Fertil Steril. 2011;95(1):272–6.
Fedele L, Bianchi S, Dorta M, Vignali M. Intrauterine adhesions: detection with transvaginal US. Radiology. 1996;199(3):757–9.
Narayan R, Goswamy RK. Transvaginal sonography of the uterine cavity with hysteroscopic correlation in the investigation of infertility. Ultrasound Obstet Gynecol. 1993;3(2):129–33.
Knopman J, Copperman AB. Value of 3D ultrasound in the management of suspected Asherman’s syndrome. J Reprod Med. 2007;52(11):1016–22.
Jorizzo JH, Riccio GJ, Chen MYM, Carr JJ. Sonohysterography: the next step in the evaluation of the abnormal endometrium. Radiographics. 1999;19:S117–30.
de Kroon CD, Jansen FW, Trimbos JB. Efficiency of saline contrast hysterosonography for evaluating the uterine cavity. [Article in Dutch]. Ned Tijdschr Geneeskd. 2003;147(32):1539–44.
Badu-Peprah A, Odoi AT, Dassah ET, Amo-Wiafe Y. Sonohysterography: time to step up its use in gynaecologic imaging in West Africa. Afr J Reprod Health. 2011;15(3):133–9.
Onah HE, Ezike HA, Mgbor SO. Saline sonohysterosalpingographic findings in infertile Nigerian women. J Obstet Gynaecol. 2006;26(8):788–90.
Kowalczyk D, Guzikowski W, Więcek J, Sioma-Markowska U. Clinical value of real time 3D sonohysterography and 2D sonohysterography in comparison to hysteroscopy with subsequent histopathological examination in perimenopausal women with abnormal uterine bleeding. Neuro Endocrinol Lett. 2012;33(2):212–6.
Soares SR, Barbosa dos Reis MM, Camargos AF. Diagnostic accuracy of sonohysterography, transvaginal sonography, and hysterosalpingography in patients with uterine cavity diseases. Fertil Steril. 2000;73(2):406–11.
Makris N, Skartados N, Kalmantis K, Mantzaris G, Papadimitriou A, Antsaklis A. Evaluation of abnormal uterine bleeding by transvaginal 3-D hysterosonography and diagnostic hysteroscopy. Eur J Gynaecol Oncol. 2007;28(1):39–42.
Yucebilgin MS, Aktan E, Bozkurt K, Kazandi M, Akercan F, Mgoyi L, Terek MC. Comparison of hydrosonography and diagnostic hysteroscopy in the evaluation of infertile patients. Clin Exp Obstet Gynecol. 2004;31(1):56–8.
Alborzi S, Dehbashi S, Khodaee R. Sonohysterosalpingographic screening for infertile patients. Int J Gynaecol Obstet. 2003;82(1):57–62.
Bacelar AC, Wilcock D, Powell M, Worthington BS. The value of MRI in the assessment of traumatic intra-uterine adhesions (Asherman’s syndrome). Clin Radiol. 1995;50(2):80–3.
Mo X, Qin G, Zhou Z, Jiang X. Assessment of risk factors of intrauterine adhesions in patients with induced abortion and the curative effect of hysteroscopic surgery. J Invest Surg. 2017:1–5. https://doi.org/10.1080/08941939.2017.1376130. [Epub ahead of print].
Barel O, Krakov A, Pansky M, Vaknin Z, Halperin R, Smorgick N. Intrauterine adhesions after hysteroscopic treatment for retained products of conception: what are the risk factors? Fertil Steril. 2015;103(3):775–9. https://doi.org/10.1016/j.fertnstert.2014.11.016. Epub 2014 Dec 17.
Capmas P, Pourcelot AG, Fernandez H. Are synechiae a complication of laparotomic myomectomy? Reprod Biomed Online. 2018;36(4):450–4. https://doi.org/10.1016/j.rbmo.2018.01.010. Epub 2018 Feb 2.
Thomson AJ, Abbott JA, Deans R, Kingston A, Vancaillie TG. The management of intrauterine synechiae. Curr Opin Obstet Gynecol. 2009;21(4):335–41.
Schenker JG. Etiology of and therapeutic approach to synechia uteri. Eur J Obstet Gynecol Reprod Biol. 1996;65(1):109–13.
Magos A. Hysteroscopic treatment of Asherman’s syndrome. Reprod Biomed Online. 2002;4(Suppl 3):46–51.
Salat-Baroux J, Pambou O, Guyot B. Hysteroscopic cure under ultrasonic control of complex and/or recurrent uterine synechiae. [Article in French]. Presse Med. 1995;24(17):811–4.
Heinonen PK. Intrauterine adhesions – Asherman’s syndrome. [Article in Finnish]. Duodecim. 2010;126(21):2486–91.
Gulumser C, Narvekar N, Pathak M, Palmer E, Parker S, Saridogan E. See-and-treat outpatient hysteroscopy: an analysis of 1109 examinations. Reprod Biomed Online. 2010;20(3):423–9.
Bettocchi S, Achilarre MT, Ceci O, Luigi S. Fertility-enhancing hysteroscopic surgery. Semin Reprod Med. 2011;29(2):75–82.
Shushan A, Protopapas A, Hart R, Magos AL. Diagnostic and therapeutic advantages of hysteroscopic surgery in management of intrauterine lesions in postmenopausal women. J Am Assoc Gynecol Laparosc. 2001;8(1):87–91.
Piketty M, Lesavre M, Prat-Ellenberg L, Benifla JL. Surgical management of intrauterine adhesions: is benefice bigger than risk? [Article in French]. Gynecol Obstet Fertil. 2010;38(9):547–9.
Pace S, Stentella P, Catania R, Palazzetti PL, Frega A. Endoscopic treatment of intrauterine adhesions. Clin Exp Obstet Gynecol. 2003;30(1):26–8.
Yu D, Li TC, Xia E, Huang X, Liu Y, Peng X. Factors affecting reproductive outcome of hysteroscopic adhesiolysis for Asherman’s syndrome. Fertil Steril. 2008;89(3):715–22.
Fernandez H, Al-Najjar F, Chauveaud-Lambling A, Frydman R, Gervaise A. Fertility after treatment of Asherman’s syndrome stage 3 and 4. J Minim Invasive Gynecol. 2006;13(5):398–402.
Capella-Allouc S, Morsad F, Rongières-Bertrand C, Taylor S, Fernandez H. Hysteroscopic treatment of severe Asherman’s syndrome and subsequent fertility. Hum Reprod. 1999;14(5):1230–3.
Shokeir TA, Fawzy M, Tatongy M. The nature of intrauterine adhesions following reproductive hysteroscopic surgery as determined by early and late follow-up hysteroscopy: clinical implications. Arch Gynecol Obstet. 2008;277(5):423–7.
Yasmin H, Nasir A, Noorani KJ. Hysteroscopic management of Ashermans syndrome. J Pak Med Assoc. 2007;57(11):553–5.
Katz Z, Ben-Arie A, Lurie S, Manor M, Insler V. Reproductive outcome following hysteroscopic adhesiolysis in Asherman’s syndrome. Int J Fertil Menopausal Stud. 1996;41(5):462–5.
Robinson JK, Colimon LM, Isaacson KB. Postoperative adhesiolysis therapy for intrauterine adhesions (Asherman’s syndrome). Fertil Steril. 2008;90(2):409–14.
Colacurci N, Fortunato N, Nasto R, Mele D, Errico G, De Franciscis P, Zarcone R. Reproductive outcome of hysteroscopic lysis of intrauterine adhesions. [Article in Italian]. Minerva Ginecol. 1997;49(7–8):325–7.
Yu D, Wong YM, Cheong Y, Xia E, Li TC. Asherman syndrome – one century later. Fertil Steril. 2008;89(4):759–79.
Pabuccu R, Onalan G, Kaya C, Selam B, Ceyhan T, Ornek T, Kuzudisli E. Efficiency and pregnancy outcome of serial intrauterine device-guided hysteroscopic adhesiolysis of intrauterine synechiae. Fertil Steril. 2008;90(5):1973–7.
Bellingham FR. Intrauterine adhesions: hysteroscopic lysis and adjunctive methods. Aust N Z J Obstet Gynaecol. 1996;36(2):171–4.
Coccia ME, Becattini C, Bracco GL, Pampaloni F, Bargelli G, Scarselli G. Pressure lavage under ultrasound guidance: a new approach for outpatient treatment of intrauterine adhesions. Fertil Steril. 2001;75(3):601–6.
Taniguchi F, Suginami H. Pregnancy and delivery following sonohysterographic lysis to treat recurrence after hysteroscopic lysis of severe intrauterine adhesions: a case report. Clin Exp Obstet Gynecol. 2008;35(3):215–7.
Tiras MB, Oktem M, Noyan V. Laparoscopic intracorporeal ultrasound guidance during hysteroscopic adhesiolysis. Eur J Obstet Gynecol Reprod Biol. 2003;108(1):80–4.
Schlaff WD, Hurst BS. Preoperative sonographic measurement of endometrial pattern predicts outcome of surgical repair in patients with severe Asherman’s syndrome. Fertil Steril. 1995;63(2):410–3.
Karande V, Levrant S, Hoxsey R, Rinehart J, Gleicher N. Lysis of intrauterine adhesions using gynecoradiologic techniques. Fertil Steril. 1997;68(4):658–62.
Chason RJ, Levens ED, Yauger BJ, Payson MD, Cho K, Larsen FW. Balloon fluoroscopy as treatment for intrauterine adhesions: a novel approach. Fertil Steril. 2008;90(5):2005.e15–7.e15.
Thomson AJ, Abbott JA, Kingston A, Lenart M, Vancaillie TG. Fluoroscopically guided synechiolysis for patients with Asherman’s syndrome: menstrual and fertility outcomes. Fertil Steril. 2007;87(2):405–10.
Rein DT, Schmidt T, Hess AP, Volkmer A, Schöndorf T, Breidenbach M. Hysteroscopic management of residual trophoblastic tissue is superior to ultrasound-guided curettage. J Minim Invasive Gynecol. 2011;18(6):774–8.
Orhue AA, Aziken ME, Igbefoh JO. A comparison of two adjunctive treatments for intrauterine adhesions following lysis. Int J Gynaecol Obstet. 2003;82(1):49–56.
Guida M, Acunzo G, Di Spiezio Sardo A, Bifulco G, Piccoli R, Pellicano M, Cerrota G, Cirillo D, Nappi C. Effectiveness of auto-crosslinked hyaluronic acid gel in the prevention of intrauterine adhesions after hysteroscopic surgery: a prospective, randomized, controlled study. Hum Reprod. 2004;19(6):1461–4.
Amer MI, Abd-El-Maeboud KH. Amnion graft following hysteroscopic lysis of intrauterine adhesions. J Obstet Gynaecol Res. 2006;32(6):559–66.
Amer MI, Abd-El-Maeboud KH, Abdelfatah I, Salama FA, Abdallah AS. Human amnion as a temporary biologic barrier after hysteroscopic lysis of severe intrauterine adhesions: pilot study. J Minim Invasive Gynecol. 2010;17(5):605–11.
Peng X, Li T, Zhao Y, Guo Y, Xia E. Safety and efficacy of amnion graft in preventing reformation of intrauterine adhesions. J Minim Invasive Gynecol. 2017;24(7):1204–10. https://doi.org/10.1016/j.jmig.2017.08.005. Epub 2017 Aug 12.
Hooker AB, de Leeuw R, van de Ven PM, Bakkum EA, Thurkow AL, Vogel NEA, et al. Prevalence of intrauterine adhesions after the application of hyaluronic acid gel after dilatation and curettage in women with at least one previous curettage: short-term outcomes of a multicenter, prospective randomized controlled trial. Fertil Steril. 2017;107(5):1223–1231.e3. https://doi.org/10.1016/j.fertnstert.2017.02.113. Epub 2017 Apr 6.
Yang JH, Chen CD, Chen SU, Yang YS, Chen MJ. The influence of the location and extent of intrauterine adhesions on recurrence after hysteroscopic adhesiolysis. BJOG. 2016;123(4):618–23. https://doi.org/10.1111/1471-0528.13353. Epub 2015 Mar 6.
Xu W, Zhang Y, Yang Y, Zhang S, Lin X. Effect of early second-look hysteroscopy on reproductive outcomes after hysteroscopic adhesiolysis in patients with intrauterine adhesion, a retrospective study in China. Int J Surg. 2018;50:49–54. https://doi.org/10.1016/j.ijsu.2017.11.040. Epub 2017 Dec 1.
Promberger R, Ott J. Anti-Mullerian hormone as a parameter for endometrial trauma in Asherman syndrome: a retrospective data analysis. Reprod Biol. 2017;17(2):151–3. https://doi.org/10.1016/j.repbio.2017.03.005. Epub 2017 Apr 8.
Nagori CB, Panchal SY, Patel H. Endometrial regeneration using autologous adult stem cells followed by conception by in vitro fertilization in a patient of severe Asherman’s syndrome. J Hum Reprod Sci. 2011;4(1):43–8.
Gargett CE, Healy DL. Generating receptive endometrium in Asherman’s syndrome. J Hum Reprod Sci. 2011;4(1):49–51.
Gan L, Duan H, Xu Q, Tang YQ, Li JJ, Sun FQ, Wang S. Human amniotic mesenchymal stromal cell transplantation improves endometrial regeneration in rodent models of intrauterine adhesions. Cytotherapy. 2017;19(5):603–16. https://doi.org/10.1016/j.jcyt.2017.02.003. Epub 2017 Mar 9.
Zhang SS, Xia WT, Xu J, Xu HL, Lu CT, Zhao YZ, Wu XQ. Three-dimensional structure micelles of heparin-poloxamer improve the therapeutic effect of 17β-estradiol on endometrial regeneration for intrauterine adhesions in a rat model. Int J Nanomedicine. 2017;12:5643–57. https://doi.org/10.2147/IJN.S137237. eCollection 2017.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Allahbadia, G.N., Gupta, A.A., Maham, A.H. (2019). Intrauterine Adhesions. In: Stadtmauer, L., Tur-Kaspa, I. (eds) Ultrasound Imaging in Reproductive Medicine. Springer, Cham. https://doi.org/10.1007/978-3-030-16699-1_11
Download citation
DOI: https://doi.org/10.1007/978-3-030-16699-1_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-16698-4
Online ISBN: 978-3-030-16699-1
eBook Packages: MedicineMedicine (R0)