
Abstract
It has become clear that susceptibility to hypoxic-ischemic, excitotoxic and oxidative insults is increased at specific stages of postnatal brain maturation, affecting both the acute and lasting injury patterns seen after the insult. For decades, a model of hypoxia-ischemia in postnatal days 7–9 (P7–P9) was the only rodent model relevant to ischemic brain injury in the neonate. This model is more likely to mimic global hypoxic-ischemic encephalopathy rather that focal transient ischemia of a single artery, such as the middle cerebral artery (MCA). To study the mechanisms of arterial pediatric stroke, a transient MCA occlusion model was first developed in juvenile rats. Since focal occlusion of the MCA is more commonly seen in term human babies than children and brain maturation affects the response to cerebral ischemia, we developed a transient MCA occlusion in P7 rats to satisfy the need for age-appropriate stroke models. We produced a series of models of different stroke severity by varying the duration of MCA occlusion and the age of the animals. In this chapter we will describe in detail surgical procedures to induce MCA occlusion, ways to ascertain that the procedure is successful, and discuss factors and limitations that can affect short and longer-term injury outcomes.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The incidence of arterial stroke in newborns—at least 1 in 4000 live term babies [1]—is similar to that in the elderly. The traditional view that neonates have greater resistance to CNS injury than adults has not been confirmed. Rather, it has become clear that at specific early stages of brain maturation susceptibility to hypoxic-ischemic, excitotoxic and oxidative insults may be increased [2,3,4]. The exact reasons for differences in response are yet to be understood but few known major contributing factors include differences in energy metabolism [5, 6], the status of excitatory and inhibitory receptors [2, 7,8,9], oxidative defenses [4, 10, 11], inflammatory responses [12] and a substantially more prominent role of caspase-3-mediated apoptosis in the immature post-hypoxic-ischemic brain than in that of the adult [13,14,15]. These data have been obtained in a model of hypoxia-ischemia (HI), a model that consists of a combined ligation of the common carotid artery of one hemisphere and systemic hypoxia for various periods of time [16]. Due to the presence of a systemic hypoxic exposure, HI model, which was essentially the only available model related to cerebral ischemia in neonatal rodents for many years, mimics hypoxic ischemic encephalopathy (HIE ) more closely than it does focal stroke.
To better understand mechanisms of pediatric arterial stroke , age-appropriate animal stroke models have been developed by modifying the monofilament MCA occlusion model established by Longa et al. in 1989 [17] for studying ischemic brain injury in adult rats. Ashwal et al. [18] first developed a model of transient middle cerebral artery (MCA) occlusion in juvenile, postnatal day 14–18 (P14–P18) spontaneously hypertensive rats. Considering that P14 is the age that corresponds to an age of a toddler and, based on data in adult rats, reperfusion is poorer and infarct is more extensive in spontaneously hypertensive as compared to other rat strains, we developed a monofilament MCA occlusion model in normotensive P7 rat pups [19]. The MCA occlusion model developed by our group produces severe disruption of cerebral blood flow in the region of the occluded MCA and confirmed partial reperfusion upon suture removal, as is evident from contrast-enhanced MRI studies [20]. Developing a model of transient suture occlusion is important because reperfusion is a common situation seen in human neonates with arterial stroke [1, 21]. Another age-appropriate rat stroke model was developed by Renolleau et al. [22] with the use of a combined permanent MCA occlusion and transient occlusion of the common carotid artery in P7 rats. The transient monofilament MCA occlusion model in P7 rat proved useful for short-term stroke studies [19, 20, 23]. This surgical procedure was, however, associated with limited ability of neonates to thrive over longer post-reperfusion periods [24]. To overcome problems in gaining weight by injured pups over time and therefore make the model suitable for long-term studies, we have recently modified the surgical procedure to produce a less invasive surgical procedure [25], a procedure that does not require the use of vessel electocoagulation and use of aneurysm clips.
In this chapter we will describe in detail the modified surgical procedure to induce MCA occlusion, ways to ascertain that the procedure is successful, and discuss factors and limitations that can affect short and longer-term injury outcomes. We will also discuss the effects of different duration of MCA occlusion in P7 rats, including permanent occlusion, on injury and the development of transient MCA occlusion in P10 rats.
Detailed Methods
Animals
All animal research should be approved by institutional Committee of Animal Research. The described experimental procedures were performed in accordance with NIH guidelines for humane handling of animals with prior approval from the Committee of Animal Research at University of California San Francisco. Female Sprague Dawley rats with a 6 day-old litter (10–11 pups per litter) were obtained from Simonson Labs (Gillroy, CA). The mother and her litter were given food and water ad libitum and housed in a temperature/light controlled animal care facility until the pups are 7 days old.
Suture Preparation
Proper suture coating is critical to achieve complete blockage of cerebral blood flow to the MCA and to prevent intracerebral hemorrhage. The coating is accomplished as follows:A 6–0 dermalon monofilament suture (United States Surgical, Norwalk, CT) is cut into 12 mm segments. A 2 mm end of each suture is lightly scratched on all sides with fine, 400 silicone carbide paper, and the tip rounded by heat [19]. To prepare a silicone based polysiloxane impression material (CutterSil, Miles Inc. Dental Products, South Bend, IN), 0.6 ml of the base is mixed for 20–30 s with one drop of the liquid activator on a clean non-porous surface. Under the microscope, the 2 mm scratched end of the suture is dipped in the silicone, lightly wiped against paper to remove excess of silicone and immediately taped upside down. When executed properly, this results in a finely coated, smooth, tapered suture, resembling a baseball bat. The adhesion and hardening process is quick, and the sutures may be used within 10 min of preparation. Each suture is examined under a microscope prior to use and the diameter measured with a micrometer. The ideal dimensions are a distal width of 0.18 ± 0.02 mm. Sutures that do not have a smooth continuous taper or those with a distal tip width of >0.2 mm or <0.14 mm are rejected. The silicone is stripped and the suture is recoated later.
Animal Surgery
-
1.
The P7 pups are anesthetized utilizing 3% isoflurane in a mixture of 70% N2O/30% O2, and then the isoflurane is reduced to 1–1.5%, as needed. Throughout the 15–20 min procedure, the animal temperature is maintained at 38 °C by a heating pad and an overhead lamp.
-
2.
The cervical incision is made directly over the right common carotid (CCA ), external carotid (EC ) and internal carotid (IC ) bifurcation. Beginning at its origin, a 1 mm segment of IC is carefully dissected and tied off with a single strand of silk at its origin [25]. A second silk suture is looped around the IC, just above the pterygopalatine artery (PPA ), and gently pulled laterally to prevent retrograde blood-flow. A small incision is made in the proximal isolated IC vessel segment.
-
3.
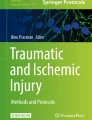
The coated 6–0 occluding suture is inserted and advanced 7.5–9.0 mm, depending on the pup weight. In smaller pups, 12–14 g, the suture is advanced 7.5–8.5 mm; pups over 15 g have the suture filament advanced 8.5–9 mm (see Fig. 1a).
-
4.
The lower knot is gently tightened, securing the suture, and the skin incision is closed with 3 interrupted 7–0 silk sutures.
-
5.
The pups are transferred in a container placed on a heating pad under the lamp until animals are recovered from anesthesia. Hyperthermia must be avoided.
-
6.
The pups are returned to dams after they are fully recovered from anesthesia.
-
7.
For reperfusion, following anesthesia (described in step 1 of Section “Animal Surgery”) the middle skin suture is removed, both knots are removed, and the suture filament together with the coating is gently pulled out and a small piece of surgical with gentle pressure is applied to the arteriotomy. Typically, there is no blood loss during either occlusion or reperfusion.
-
8.
The pups are transferred in a container placed on a heating pad under the lamp until animals are recovered from anesthesia, as described in step 5 of Section “Animal Surgery”.
-
9.
Pups are returned to dams after they are fully recovered from anesthesia.
-
10.
Animal weights are recorded daily. If no weight gain is seen within 2 days after surgical procedure upon the development of surgical techniques, animals are to be gavage-fed with 2% condensed milk until signs of weight gain are evident [24].

(a) A schematic diagram of the suture insertion and advancement to occlude the MCA. CCA common carotid artery, ECA external carotid artery, ICA internal carotid artery. (b) An example of anterior-to-posterior injury distribution pattern on DW-MRI 2 h post-MCA occlusion. DW hyperintensity is observed in brain regions with slowed water diffusion
Non-invasive Delineation of Injury Patterns
Non-invasive injury delineation by MRI is not required but is helpful during the development of the procedure to confirm that the desired injury pattern has been achieved in individual animals. Upon development of the surgical procedure, MRI can also be used as a criterion for excluding uninjured animals in drug-studies.
-
1.
Diffusion-weighted magnetic resonance imaging (DW-MRI) is a non-invasive method which is sensitive to reduced water diffusivity in the tissue following occlusion-induced disruption of CBF. DW-MRI provides information on the presence of injury in minutes; animals need to be anesthetized for imaging. Therefore, the technique can be used for delineation of the spatial pattern of early injury during the occlusion [20, 25]. An example of the anterior-to-posterior injury distribution on DW-MRI 2 h after MCA occlusion is shown in Fig. 1b.
-
2.
Contrast-enhanced MRI can ascertain the completeness of CBF reduction in the MCA vascular territory during the occlusion and restoration of CBF upon retraction of the suture [20]. This method requires intra-jugular injection of the magnetic susceptibility contrast.
Caveats, Limitations and Concerns
-
1.
Inadequate occlusion of the MCA. As described in Section “Suture Preparation”, a combination of factors can affect the successful occlusion of the MCA. The weight of animals can vary substantially even within the same litter thus affecting the length of the suture advancement and the thickness of the suture needed for proper placement of the tip of the suture in proximity to MCA. The use of a shorter than necessary suture will not result in blockage of the MCA. In contrary, the use of a longer than needed suture may produce partial rather than nearly complete disruption of cerebral blood flow through the MCA as the thickest portion of the suture, its coated tip, will be far from the MCA. Unusually high branching of the MCA, which is occasionally seen, can provide sufficient residual blood flow, thus precluding from complete occlusion.
-
2.
Insufficient suture coating. An uncoated suture may perforate the vessel. Thick or uneven coating will make the suture more rigid, making it more difficult to advance or retract. Excessive coating may affect the ability to reperfuse due to vasospasm and affected responsiveness of the vessel. Reuse of the coated suture may affect consistency of results, as the suture will become more rigid and/or the coating may slide off.
-
3.
Excessive anesthesia. Multiple lengthy anesthesia episodes may affect the ability of animals to thrive and therefore the duration of anesthesia should be kept to a necessary minimum, with frequent checking of pinch and other reflexes. Due to the small size of P7 rats, physiological monitoring is limited as MABP monitoring or blood gas analysis are currently not available. The type of anesthetic may affect time necessary for pups to recover form anesthesia. Isoflurane is preferable as animals recover from this agent rapidly. Animals should be put back to their dam for nursing as soon as they are fully awake. If surgery and recovery from anesthesia takes longer then what we described in Section “Detailed Methods”, animals may become dehydrated and saline is to be injected (i.p., 0.1–0.2 ml).
-
4.
Lack/delay in weight gain.
-
(a)
Like with stroke models in adults and HI model in neonates, essentially all animals lose weight over the first 24 h period after the insult. However, weight loss can persist over time, as we described in our previous publications [24, 25], especially following the originally described procedure [19]. The exact reasons for lack of weight gain after MCAO are not known but the coagulation and/or ligation of several arteries, including the external carotid, occipital, superior thyroid, lingual and maxillary arteries may reduce or completely cut off blood flow to the ipsilateral neck muscles, tongue, salivary glands. This will and the face is the likely possibilities. Compared to original procedure, the modified procedure described in this chapter is less invasive due to elimination of bipolar coagulation, electrocautery and use of aneurysm clips from the surgical procedure.
-
(b)
Reduced nursing can occur in case of frequent moving cages from facility to facility. Normal feeding can be reduced due to frequent removal of pups from the cage.
-
(c)
Gavage feeding with milk may be necessary if weight gain of injured pups is diminished [24, 25].
-
(a)
-
5.
The incidence of injury. Intra-litter variations in the incidence may occur.
-
6.
The route of suture insertion. Insertion of suture through the ECA is the common way of occlusion of the MCA, which produces consistent injury acutely. The limitation is that this surgical procedure interferes substantially with animal grow and long-term survival. The surgical procedure described in this chapter that involves suture insertion through the ICA results in an overall similar injury pattern as the later surgical procedure [25].
-
7.
Variable extent of recovery over time. With the use of combined multiple MRI sessions during MCA occlusion, 24 h and 7 days after reperfusion following a 3 h. MCA occlusion we showed that individual pups with nearly identical spatial injury pattern within 24 h may recover to a different extent by 7 days post-MCA occlusion [25], from no to a nearly complete recovery based on histology.
-
8.
The effect of gender. Gender may affect injury evolution and outcome, as has been shown for HI [26, 27].
Advantages and Unknowns
-
1.
Varying the time of MCA occlusion in animals of the same age results in lesions of different size. The use of a 3 h MCA occlusion [24, 25] produced a larger lesion than a 2 h [28]. MCA occlusion in P7 rats. Lack of reperfusion is associated with even larger injury [23].
-
2.
Permanent occlusion of the MCA favors a necrotic type of cell death whereas occlusion-reperfusion induces both apoptosis and necrosis [23]. Following transient MCA occlusion, apoptotic neuronal death is substantial both in the ischemic core and in penumbra [23]; no data on the presence of continuum cell death which has been reported after HI in P7 rats [29] are available.
-
3.
Age of neonatal rats and injury outcome. MCA occlusion in neonatal rats of different ages may require different duration of occlusion to achieve similar injury severity histologically but no systematic comparative studies have been performed. In addition to focal stroke model in P7 rats we have developed a similar model in P10 rats [30]. The latter model produces consistent injury pattern sub-chronically [31] and animals survive for months [32].
Summary and Future Directions
Several focal stroke models in neonatal rats have become available over the last decade, making it possible to study mechanisms of neonatal stroke experimentally. These models are based on occlusion of MCA in P7 [19, 20, 22,23,24,25, 28, 33] and P10 [30,31,32, 34, 35] rats. Reperfusion following monofilament occlusion is induced in some but not all models. The completeness of reperfusion may vary depending on the way MCA occlusion is induced (transient placement of a monofilament to block the MCA compared to transient CCA ligation combined with permanent MCA ligation) and duration of the occlusion (transient compared to permanent). Another important aspect of availability of models in rats of different ages is the ability to determine maturational differences in the response to stroke within the neonatal period (stroke in P7 [19, 22, 25] compared to P10 rats [30, 35]) as well as comparison to stroke effects in juvenile rats (P14–P17 [18]). While much is to be learned about the role of gender and strain on short- and long-term outcomes, availability of several models of focal cerebral ischemia provides ways to advance the field of neonatal stroke.
Other common conditions in human newborns are venous thrombosis and intracerebral hemorrhage. So far, there have been no age-appropriate models developed for those diseases.
References
deVeber G, Roach ES, Riela AR, Wiznitzer M. Stroke in children: recognition, treatment, and future directions. Semin Pediatr Neurol. 2000;7:309–17.
Ikonomidou C, Bosch F, Miksa M, et al. Blockade of NMDA receptors and apoptotic neurodegeneration in the developing brain. Science. 1999;283:70–4.
Olney JW, Wozniak DF, Jevtovic-Todorovic V, Farber NB, Bittigau P, Ikonomidou C. Drug-induced apoptotic neurodegeneration in the developing brain. Brain Pathol. 2002;12:488–98.
Sheldon RA, Jiang X, Francisco C, et al. Manipulation of antioxidant pathways in neonatal murine brain. Pediatr Res. 2004;56:656–62.
Vannucci RC, Vannucci SJ. Glucose metabolism in the developing brain. Semin Perinatol. 2000;24:107–15.
Vannucci SJ, Simpson IA. Developmental switch in brain nutrient transporter expression in the rat. Am J Physiol Endocrinol Metab. 2003;285:E1127–34.
Ikonomidou C, Mosinger JL, Salles KS, Labruyere J, Olney JW. Sensitivity of the developing rat brain to hypobaric/ischemic damage parallels sensitivity to N-methyl-aspartate neurotoxicity. J Neurosci. 1989;9:2809–18.
McDonald JW, Johnston MV. Physiological and pathophysiological roles of excitatory amino acids during central nervous system development. Brain Res Brain Res Rev. 1990;15:41–70.
Bickler PE, Fahlman CS, Ferriero DM. Hypoxia increases calcium flux through cortical neuron glutamate receptors via protein kinase C. J Neurochem. 2004;88:878–84.
Aspberg A, Tottmar O. Development of antioxidant enzymes in rat brain and in reaggregation culture of fetal brain cells. Brain Res Dev Brain Res. 1992;66:55–8.
Fullerton HJ, Ditelberg JS, Chen SF, et al. Copper/zinc superoxide dismutase transgenic brain accumulates hydrogen peroxide after perinatal hypoxia ischemia. Ann Neurol. 1998;44:357–64.
Hedtjarn M, Mallard C, Hagberg H. Inflammatory gene profiling in the developing mouse brain after hypoxia-ischemia. J Cereb Blood Flow Metab. 2004;24:1333–51.
Cheng Y, Deshmukh M, D’Costa A, et al. Caspase inhibitor affords neuroprotection with delayed administration in a rat model of neonatal hypoxic-ischemic brain injury [see comments]. J Clin Invest. 1998;101:1992–9.
Hu BR, Liu CL, Ouyang Y, Blomgren K, Siesjo BK. Involvement of caspase-3 in cell death after hypoxia-ischemia declines during brain maturation. J Cereb Blood Flow Metab. 2000;20:1294–300.
Zhu C, Wang X, Xu F, et al. The influence of age on apoptotic and other mechanisms of cell death after cerebral hypoxia-ischemia. Cell Death Differ. 2005;12:162–76.
Rice JE, Vannucci RC, Brierley JB. The influence of immaturity on hypoxic-ischemic brain damage in the rat. Ann Neurol. 1981;9:131–41.
Longa EZ, Weinstein PR, Carlson S, Cummins R. Reversible middle cerebral artery occlusion without craniectomy in rats. Stroke. 1989;20:84–91.
Ashwal S, Cole DJ, Osborne S, Osborne TN, Pearce WJ. A new model of neonatal stroke: reversible middle cerebral artery occlusion in the rat pup. Pediatr Neurol. 1995;12:191–6.
Derugin N, Ferriero DM, Vexler ZS. Neonatal reversible focal cerebral ischemia: a new model. Neurosci Res. 1998;32:349–53.
Derugin N, Wendland M, Muramatsu K, et al. Evolution of brain injury after transient middle cerebral artery occlusion in neonatal rat. Stroke. 2000;31:1752–61.
Ferriero DM. Neonatal brain injury. N Engl J Med. 2004;351:1985–95.
Renolleau S, Aggoun-Zouaoui D, Ben-Ari Y, Charriaut-Marlangue C. A model of transient unilateral focal ischemia with reperfusion in the P7 neonatal rat: morphological changes indicative of apoptosis. Stroke. 1998;29:1454–60; discussion 1461.
Manabat C, Han BH, Wendland M, et al. Reperfusion differentially induces caspase-3 activation in ischemic core and penumbra after stroke in immature brain. Stroke. 2003;34:207–13.
Fox C, Dingman A, Derugin N, et al. Minocycline confers early but transient protection in the immature brain following focal cerebral ischemia-reperfusion. J Cereb Blood Flow Metab. 2005;25:1138–49.
Derugin N, Dingman A, Wendland M, Fox C, Vexler ZS. Magnetic resonance imaging as a surrogate measure for histological sub-chronic endpoint in a neonatal rat stroke model. Brain Res. 2005;1066:49–56.
Hagberg H, Wilson MA, Matsushita H, et al. PARP-1 gene disruption in mice preferentially protects males from perinatal brain injury. J Neurochem. 2004;90:1068–75.
van den Tweel ER, van Bel F, Kavelaars A, et al. Long-term neuroprotection with 2-iminobiotin, an inhibitor of neuronal and inducible nitric oxide synthase, after cerebral hypoxia-ischemia in neonatal rats. J Cereb Blood Flow Metab. 2005;25:67–74.
Dingman A, Lee SY, Derugin N, Wendland MF, Vexler ZS. Aminoguanidine inhibits caspase-3 and calpain activation without affecting microglial activation following neonatal transient ischemia. J Neurochem. 2006;96:1467–79.
Northington FJ, Graham EM, Martin LJ. Apoptosis in perinatal hypoxic-ischemic brain injury: how important is it and should it be inhibited? Brain Res Brain Res Rev. 2005;50:244–57.
Mu D, Jiang X, Sheldon RA, et al. Regulation of hypoxia-inducible factor 1alpha and induction of vascular endothelial growth factor in a rat neonatal stroke model. Neurobiol Dis. 2003;14:524–34.
Mu D, Chang YS, Vexler ZS, Ferriero DM. Hypoxia-inducible factor 1alpha and erythropoietin upregulation with deferoxamine salvage after neonatal stroke. Exp Neurol. 2005;195(2):407–15.
Chang YS, Mu D, Wendland M, et al. Erythropoietin improves functional and histological outcome in neonatal stroke. Pediatr Res. 2005;58:106–11.
Denker S, Ji S, Lee SY, et al. Macrophages are comprised of resident brain microglia not infiltrating peripheral monocytes acutely after neonatal stroke. J Neurochem. 2007;100:893–904.
Ashwal S, Tone B, Tian HR, Chong S, Obenaus A. Comparison of two neonatal ischemic injury models using magnetic resonance imaging. Pediatr Res. 2007;61:9–14.
Ashwal S, Tone B, Tian HR, Chong S, Obenaus A. Serial magnetic resonance imaging in a rat pup filament stroke model. Exp Neurol. 2006;202:294–301.
Acknowledgements
This study was funded by NIH grants NIH NS44025 to Z.S.V. and NS35902 to D.M.F. and Z.S.V. and AHA GIA grant 0655236Y to Z.S.V. The authors thank Nikita Derugin for critical reading of the manuscript and Joel Faustino for technical assistance.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Vexler, Z.S., Ferriero, D.M. (2019). A Model of Neonatal Focal Cerebral Ischemia-Reperfusion. In: Chen, J., Xu, Z., Xu, X., Zhang, J. (eds) Animal Models of Acute Neurological Injury. Springer Series in Translational Stroke Research. Springer, Cham. https://doi.org/10.1007/978-3-030-16082-1_14
Download citation
DOI: https://doi.org/10.1007/978-3-030-16082-1_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-16080-7
Online ISBN: 978-3-030-16082-1
eBook Packages: MedicineMedicine (R0)