
Abstract
Recently, digital techniques have revolutionized the production of partial removable dental prostheses (PRDPs). This chapter reviews current systems for PRDP production, how they are done in clinical practice, its advantages and limitations, and current literature regarding their clinical performance. Currently, several digital techniques are available in the market for PRDP production including subtractive and additive techniques. Subtractive milling technique is mainly effective for nonmetal PRDP. Digital techniques expand the range of materials that can be utilized for PRDP production, including new polymers (PEEK), and facilitate previously difficult procedure such as casting titanium PRDP, which can be produced digitally more easily. This review shows that available evidence suggests that these techniques have promising clinical results. Laser-sintering resulted in higher patient satisfaction compared to conventional technique. However, long-term clinical trials are recommended to explore the long-term effects of these techniques. Moreover, this review showed the lack of evidence on the clinical performance of nonmetal partial removable dental prostheses.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Partial removable dental prosthesis
- Laser-sintering
- 3D printing
- Nonmetal PRDP
- CAD-CAM
- Stereolithography
- Casting
Although digital partial removable dental prostheses (PRDPs) have entered clinical practice only recently, they have revolutionized PRDPs production and disrupted the market. The aim of this chapter is to describe the advances in digital PRDPs, including the clinical procedures, how are they done, and their clinical performance.
1 Introduction
Despite the success of preventive dentistry in reducing the prevalence of edentulism, partial edentulism remains a public health issue worldwide especially among elderly people. Prevalence of partial edentulism ranges from 30% to 60% among Europeans over the age of 65, and given the increased life expectancy and the aging trend in developed countries, the prevalence of partial edentulism is expected to keep growing [1]. In Germany as well as Japan, it has been estimated that the number of partially dentate people will increase, and in the UK, 96% of adults are expected to be at least partially dentate by 2028 [1, 2].
PRDPs are noninvasive simple treatments that improve the quality of life of partially edentulous patients [3, 4]. Despite the great success of dental implant treatments lately, several factors contribute to the continuous need for PRDPs such as lower socioeconomic status, access to care, and compromised general health. It has been reported that 13–29% of European adults wear PRDPs [5], and in the USA it is projected that PRDP treatments will consume a minimum of 270 million hours of dentists’ work per year by 2020 [6, 7].
2 History
Since their conception in the early 1930s, PRDPs have been traditionally made of cast alloys using the traditional lost-wax technique. This involves lengthy steps including manual construction of a wax pattern for the designed prostheses frameworks, investing the pattern to form a model, melting the wax to prepare the space, and then pouring the molten metal to the prepared space in the mold. This lengthy process consumes large amount of materials and is highly prone to human errors [8].
The evolution of computer-aided design and digital milling manufacturing marked a huge milestone in the fabrication of dental restorations. This technology reduces the time, cost, and human errors associated with the rehabilitation of fixed dental prostheses. However, milling manufacturing of partial removable dental prostheses is difficult to accomplish due to the spatial restriction of the complex structure of PRDP frameworks with its clasps, rests, and connectors and proven uneconomical due to the high hardness of PRDP alloys which quickly wears the milling tools. Therefore, lost-wax casting remains the standard technique for metal-based partial removable dental prostheses [9, 10], although milling wax or resin PRDP patterns are available in the market but did not gain widespread popularity.
Stereolithography have been recently used to print the resin or wax sacrificial patterns of the PRDP frameworks [11]. This processing produces frameworks with acceptable fit and reduces some of the costs and human errors associated with the manual wax-ups [12]. However, the printed resin pattern still has to be cast conventionally to get the final PRDP framework [11, 13]. In 2006, laser-sintering was introduced to produce PRDP frameworks digitally in order to eliminate the investing and casting steps [14]. Due to the lack of specialized software, selective laser-sintering originally required the use of physical sculptor to virtually build the framework [15]. The physical sculptor is a haptic device that allows the users to touch and manipulate objects in the 3D virtual environment. It helps technicians to utilize hand movements very close to the hand movements they use for conventional framework wax-up, but it increases the time, cost, and complexity of the procedures [15].
To overcome these limitations, different software solutions were tested to virtually design PRDPs without the need for a sculptor. However, these programs were not specifically developed for PRDP design and required lengthy procedures to determine the path of insertion, eliminate undesirable undercuts, and draw the framework components [16]. Specialized software for designing PRDP framework was not introduced until 2010 [17]. Surface roughness and long post-processing steps are limitations of laser-sintering technology. Recently, simultaneous technology of repeated laser-sintering with high-speed high-precision milling was introduced to fabricate PRDP with higher precision and smoother surfaces [18]. This technology integrates both laser deposition and high-speed milling on the same platform. The fabrication starts with ten layers of laser deposition followed by high-speed milling to smoothen the surface and provide extra detail precision [19]. This technique proves effective for titanium PRDP, which overcomes the casting challenges of titanium [20]. Moreover, laser-sintering followed by metal annealing was also used for titanium PRDP fabrication which increases the ductility and improves resistance to crack [21].
Digital technology has also ameliorated the fabrication of metal-free PRDPs. Metal-free acrylic PRDPs were introduced early as an interim alternative to metal-based PRDP. Around 1950, nylon-based ployamide PRDP (Valplast) was introduced in the USA and gained popularity since then. Later, with the development of denture base fabrication techniques, other thermoplastic resins (polyamide, polyester, polycarbonate, and polypropylene) were utilized to produce nonmetal PRDPs [22]. These prostheses have several advantages over metal-based PRDPs, including improved esthetics, suitability for patients allergic to metal, lightness, flexibility, and cheaper price compared to metal-based PRDPs [22]. Conventional fabrication techniques include compression molding, injection molding, and fluid resin technique. With the introduction of CAD/CAM milling in dentistry, most of these prostheses are easily produced by milling, and more recently 3D printing has been introduced to fabricate nylon-based polyamide flexible prostheses [23, 24]. Upon the success of digital production for PRDP, new materials are now introduced to the market, such as polyether ether ketone (PEEK), which is currently produced by CAD/CAM direct milling [25].
2.1 Digital PRDP in Today’s Market
Nowadays, digital production of PRDPs is widely spread. The current procedures involve first digitization of the case with either intraoral or extraoral laboratory 3D scanners (acquisition stage) and subsequent design of the PRDP frameworks using specialized software with or without the aid of a physical sculptor (manipulation stage) [26]. Most of the available designing systems do not require physical sculptors, although the Geomatic® Touch™ X (3D systems, South Carolina, USA) still requires it. The available digital systems for producing the digital PRDPs are either direct metal production systems including laser-sintering systems or indirect production including the stereolithography systems; the special variation of it is the digital light processing (DLP) and milling (Table 5.1). For metal-free PRDP digital production, direct milling of thermoplastic resin is the most common method; however, a new 3D filament printing system is available for Valplast (Afrona, New York, USA). Table 5.2 shows current materials used for fabrication of digital nonmetal PRDPs.
3 Step-by-Step Procedures of Digital PRDP Fabrication
Following a thorough examination and a careful treatment planning, the clinical steps of PRDP can be started. The digital workflow consists of three steps: acquisition, manipulation, and fabrication [26].
Acquisition
-
1.
Primary impressions are made using alginate impression, which are then poured to have the diagnostic cast. On the diagnostic cast, the case is studied carefully, and the PRDP design is planned. Necessary abutment teeth preparations are planned at this stage.
-
2.
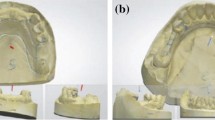
Abutment teeth are prepared as planned. Here, one of two options is possible; either the patient arches are scanned intraorally using an intraoral scanner, which eliminates the need for physical impression, or the final impressions are made in rubber base materials, and then either scanned directly or poured into stone master casts that are subsequently scanned using an extraoral digital scanner. The scanner produces a stereolithographic file (STL) of the master cast that is imported in the designing software (Fig. 5.1). Intraoral scanning involves multiple scans for both arches, taking around 3–17 min depending on the case. These scans are stitched by the software to provide the full-mouth image [27].
Manipulation
-
3.
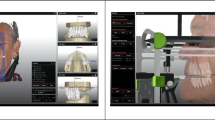
Using a specialized software, the PRDPs are designed digitally through a series of digital steps that mirror the traditional laboratory procedures. First, the path of insertion is determined automatically using a digital survey tool; the software automatically rotates the cast three dimensionally and calculates the parallelism and the depth of undercuts in all dimensions to reach to the best tilt for the path of insertion (Fig. 5.2), and survey line is then automatically made. This step saves a lot of time compared to the conventional manual step. This is followed by blockout of undesirable undercuts (Fig. 5.3). After that, the retentive areas for the retentive clasp tips are determined.
-
4.
Relief areas are marked by laying thin layers of virtual wax on relief areas such as rugae. Next, the meshwork patterns are added (Fig. 5.4), and the major connectors and rests are drawn as built (Fig. 5.5). The clasp arms and the clasp systems (width and thickness) are drawn three dimensionally (Fig. 5.6), and the thickness of the framework is adjusted and smoothed (Fig. 5.7). Finally, the finish lines are drawn using the curve tool which utilizes default or customized profiles (Fig. 5.8), and the designed framework is finished (Fig. 5.9).
-
5.
Sprue is designed for indirect fabrication systems (3D printing and milling) to be used in the casting process. For additive technology systems (laser-sintering and 3D printing), supports are added to the structure before submitting the finished design (Fig. 5.10). Appropriate supports of adequate strength are required to stabilize the PRDP framework layers upon their production as they are laid down in very thin layers. Also, during manufacturing it prevents movement and dissipates heat away from the finished part of framework during manufacturing [14]. The designing process takes approximately 30 min per framework (Fig. 5.11) [17].
Fabrication
-
6.
Once the design file is complete, it is sent to the production machine. At this point, the frameworks are produced with either direct or indirect production systems.
Direct Metal Production
For direct metal production systems including laser-sintering and laser melting, metal powder is laser-sintered to produce PRDP frameworks. One laser-sintering machine takes up to 12 h to fabricate 12 PRDPs in one cycle. After that, the printed PRDP is retrieved (Fig. 5.12) and subjected to post-processing. Most of the uncured metal powder is reused for future frameworks which reduces waste and improves efficiency. PRDP is heat-treated following manufacturer instructions and is then separated from the supporting base. Fit of the framework is checked on the cast and adjusted as necessary (Fig. 5.13).
Indirect Metal Production
For indirect metal production systems including stereolithography, direct light processing, and milling, a resin or wax framework pattern is printed or milled (Fig. 5.14). In the case of 3D printing, several post-curing steps are required including removing any wet resin remnants by immersing the pattern in a solvent, followed by final curing in UV oven to fully harden and get its structural integrity [28]. Resin pattern can also be tried in the patient’s mouth if needed. The pattern is then cast conventionally using the lost-wax technique.
-
7.
The framework is finished and polished in several steps. First, the framework is finished by finishing burs; then the frameworks are finished under rotating barrels of ceramics, followed by barrels of corns. Finally, frameworks are electropolished in electropolishing machines.
-
8.
PRDP framework is checked for fit and occlusion in the patient mouth (Fig. 5.15). Maxillomandibular relationship is recorded at this stage, and teeth shade and form are selected in a similar manner used for conventional PRDP.
-
9.
The framework is returned to the lab for teeth setting, final wax-up, and acrylization.
-
10.
PRDP is tried in the patient mouth and adjusted for fit, retention, and occlusion. Then framework is polished and delivered to the patients.

Virtual casts (STL files) of a PRDP case scanned by extraoral 3D scanner; (a) maxillary arch and (b) mandibular arch

Virtual determination of the path of insertion of a PRDP using 3Shape CAD points software; (a) maxillary arch and (b) mandibular arch

Virtual blockout of undesirable undercuts of a PRDP case using 3Shape CAD points software; (a) maxillary arch and (b) mandibular arch

Virtual building of the meshwork in the edentulous area of a PRDP case using 3Shape CAD points software; (a) maxillary arch and (b) mandibular arch

Virtual building of the major connectors and rests for a PRDP case using 3Shape CAD points software; (a) maxillary arch and (b) mandibular arch

Virtual building of the clasp arms of a PRDP case using 3Shape CAD points software; (a) maxillary arch and (b) mandibular arch

Virtual adjusting of the thickness of the framework of a PRDP using 3Shape CAD points software; (a) maxillary arch and (b) mandibular arch

Virtual drawing of the finish line of a PRDP case using 3Shape CAD points software; (a) maxillary arch and (b) mandibular arch

Finalized virtual design of a PRDP case using 3Shape CAD points software; (a) maxillary arch and (b) mandibular arch

Illustration of the supports required for successful laser-sintering of a partial removable dental prosthesis: (a) maxillary arch, (b) mandibular arch, and (c) PRDP frameworks in the building platform

Illustration showing the arrangement of PRDP frameworks in the building platform

A photograph showing the PRDP frameworks in the building platform processed by laser-sintering technology

Laser-sintered partial removable dental prosthesis framework fitted on the cast

3D printing for fabrication of partial removable dental prosthesis: (a) 3D-printed resin patterns of partial removable dental prostheses, (b) resin pattern of partial removable dental prosthesis framework with wax sprue ready for casting, and (c) metal frameworks of partial removable dental prosthesis cast from 3D-printed resin patterns

Laser-sintered partial removable dental prosthesis in the patient mouth of a patient: (a) occlusal view, (b) frontal view
4 Clinical Evidence on Digital PRDP
Digital PRDPs are new products and therefore have not been studied thoroughly yet. Most of the studies in this field have been focused on testing the feasibility of the technique, and they have shown that digital direct or indirect metal fabrication can produce accurately fitting PRDPs [12, 16, 29,30,31].
Extraoral scanning of the master cast has been reported effective in several studies and resulted in well-fitting RPDP frameworks [12, 32]. On the other hand, intraoral scanning is effective for capturing in Kennedy class III cases [27, 33, 34], but not Kennedy class I and II as the scanning does not capture the physiologic extensions of the movable mucosa [27].
Regarding clinical performance, only few studies have been published. A clinical trial has shown the superiority of digitally produced PRDPs by laser-sintering over the traditional PRDPs in terms of patient satisfaction [35]. It also showed that most of the patients had preferred the laser-sintered PRDPs over the conventional prostheses after using both [35]. Another study showed that although digital PRDPs (produced by laser-sintering) showed statistically significantly larger gap between occlusal rests and corresponding rest seats compared to the traditional casting PRDP, it is considered clinically acceptable [36]. Similarly, digital PRDPs produced by 3D printing followed by casting showed variable fitting discrepancy but were considered clinically acceptable [37].
Laboratory studies showed that laser-sintered cobalt-chromium alloys are about eight times more accurate than casting and have better mechanical properties, higher yield strength and fatigue resistance compared to cast Co-Cr alloys [38]. Moreover, Aker clasps produced by simultaneous repeated laser-sintering and high-speed milling showed higher fitting accuracy and retention forces compared to conventional cast clasps [39]. However, when the fit of laser-sintered PRDP frameworks was compared with lost-wax technique, milled and 3D-printed frameworks, laser-sintered frameworks demonstrated significantly larger gaps than all other techniques. Technical parameters might need to be adjusted to get better fitting results [40]. Several factors can affect the final product in laser-sintering, including heat treatment, amount of relief designed, and position and angulation of the support structure [18]. Moreover, with this new technology, time is required to get to the top of the learning curve and optimize the product [41].
Currently, there is insufficient evidence regarding the metal-free PRDP although they are widely used in the market [22]. Laboratory studies showed that flexible PRDPs have lower color stability and higher risk to fracture compared to polymethyl methacrylate (PMMA) acrylic PRDPs [42]. The newly introduced PEEK high-performance polymer showed good fitting accuracy and adequate clasp retention in vitro; however, it was inferior to metal clasp retention [40, 43]. It could be an alternative to metal PRDP in cases of patients with taste sensitivity or metal allergy; however, more clinical studies are needed before this treatment can be recommended [25].
5 Advantages and Limitations of Digital PRDPs
Digital production of PRDP has several potential advantages. Indirect fabrication techniques benefit from the digital designing step which saves time compared with manual surveying and framework wax-up. Also, direct metal fabrication systems increase productivity and shorten the work flow while reducing manufacturing costs as several steps are omitted (cast duplication, manual wax-up, investing and casting) and reduce maintenance cost for expensive investing and casting machines.
Digital production can be environmentally friendly considering the potential reduction in environmental impact due to reduced waste of alloy, wax, and investment materials (this applies to direct metal production systems) and the recycling potential of uncured metal powder left after laser-sintering.
Moreover, virtual designs can be saved for later use which enable dentists to provide patients with extra prosthesis or replacement prosthesis with the same or modified design without the need to restart the entire process. This also permits sharing designs between technicians and clinicians via internet/e-mail, which improves communication.
Digital production opens the door for endless opportunities to enhance both the work flow and the quality of provided treatment; PRDP with optimized designs can be provided for individual patient to provide required mechanical properties needed in the different oral environment of each case [44, 45]; moreover digital PRDP can be performed for cases requiring altered cast technique and with added simplicity and shorter step [46]. Digital production may open the door for different materials to be used for PRDPs like polymer-based materials, which can overcome some of the limitations of current metal-based PRDP [47].
Utilizing intraoral scanning can provide greater success with gagger patients, patients with special needs, or anxious patients. It involves multiple section scanning so it is easier to control moisture section by section than to control moisture for the whole arch at one time. It uses multiple scans that are stitched together automatically at real time, so any defect or deficiency in the impression can be identified and corrected at the same visit [34].
5.1 Limitations
Digital fabrication of partial removable dental prostheses has some limitations. First, this technology only allows fabrication of the metal framework, but it does not allow for digitalized tooth setup; currently tooth setup needs to be done manually. Another limitation is the high initial cost of the machine. This technology requires time and expertise to learn the technique. Digital PRDPs currently require special supports to hold the prostheses during the 3D-printing process. This adds extra steps for planning the supports and removing them after fabrication. Another limitation is the staircase effect, which may appear due to the layering nature of the 3D-printing process. It can be significantly reduced by reducing the layer thickness which could increase the production time [26]. Moreover, currently this technique cannot be used for all patients, since some special designs cannot be produced easily because of the limitations of the available software and manufacturing procedures [35].
6 Potentials and Future Directions
Currently, digital technologies were used to produce PRDP frameworks; then the denture base is produced conventionally by manual waxing followed by acrylization [35, 37]. The future direction would be toward digitizing this step too. PRDP frameworks could be scanned after being clinically fitted and adjusted in the patient mouth; teeth and denture base can be designed digitally and then produced digitally. This will open the door for a wider range of materials to be utilized but might also create newer challenges regarding the bonding between the framework and denture base or denture base and denture teeth produced from different materials.
Moreover, current digital technologies can produce structures in the nanoscale, and therefore frameworks with thinner sections, and different dimensions than conventionally produced frameworks [26]. This can challenge current designing principles which were mainly set to result in successful casting and acrylization of PRDP. Meshwork design criteria, tissue stops, thickness of major connectors, minor connectors, length of clasp arms, and depth of undercut are all designed to produce successful PRDP. However, currently, these requirements may not be needed to produce accurately fitting digital PRDP. Instead, these different technologies would come up with different requirements that need to be discovered and respected.
Additionally, customized PRDP can be produced with enhanced mechanical properties tailored for individual cases utilizing finite element-based computational design optimization algorithm integrated automatically with the digital designing and the additive manufacturing, which is called bi-directional evolutionary structural optimization (BDES) techniques. BDES refers to adjustment of a structure by progressively adding materials in areas need it most (like underloaded areas in a denture base) and concurrently removing materials from other areas in excess (like pressure areas). A study showed the success of this technique in providing a denture base with optimal pressure on the supporting tissue as evaluated by finite element analysis [45]. This technique shows the potential of digital technology to overcome several clinical problems including multiple post-insertion adjustment visits and long-term residual ridge resorption. Utilizing computational shape optimization automatically with the digital workflow might change the future of PRDP.
7 Conclusions
Digital production of partial removable dental prostheses has revolutionized the fabrication process of both metal and nonmetal partial dental prostheses, and it is gaining increasing popularity in clinical practice. Metal partial removable dental prostheses are fabricated digitally using either direct or indirect production techniques. Direct production replaces the casting step and therefore significantly reduces cost and time, while indirect production involves producing resin patterns digitally, which subsequently are cast using traditional methods.
Digital production has several advantages: it saves time and materials while increasing productivity and reducing human errors, and current scientific evidence regarding the clinical performance of these prostheses, although limited, is very promising. Nevertheless, the digital technologies currently available fall short of finishing the whole partial removable dental prostheses, as tooth setup and acrylization are still done manually using traditional methods.
References
Müller F, Naharro M, Carlsson GE. What are the prevalence and incidence of tooth loss in the adult and elderly population in Europe? Clin Oral Implants Res. 2007;18(s3):2–14.
Carlsson GE. Changes in the prosthodontic literature 1966 to 2042. J Can Dent Assoc. 2005;71(5):328.
Van Waas M, Meeuwissen J, Meuwissen R, Kayser A, Kalk W, Van ‘t Hof M. Relationship between wearing a removable partial denture and satisfaction in the elderly. Community Dent Oral Epidemiol. 1994;22(5 Pt 1):315–8.
John MT, Slade GD, Szentpétery A, Setz JM. Oral health-related quality of life in patients treated with fixed, removable, and complete dentures 1 month and 6 to 12 months after treatment. Int J Prosthodont. 2004;17(5):503–11.
Zitzmann NU, Hagmann E, Weiger R. What is the prevalence of various types of prosthetic dental restorations in Europe? Clin Oral Implants Res. 2007;18(Suppl 3):20–33.
Douglass CW, Watson AJ. Future needs for fixed and removable partial dentures in the United States. J Prosthet Dent. 2002;87(1):9–14.
Hummel SK, Wilson MA, Marker VA, Nunn ME. Quality of removable partial dentures worn by the adult U.S. population. J Prosthet Dent. 2002;88(1):37–43.
Rudd RW, Rudd KD. A review of 243 errors possible during the fabrication of a removable partial denture: part I. J Prosthet Dent. 2001;86(3):251–61.
Koutsoukis T, Zinelis S, Eliades G, Al-Wazzan K, Rifaiy MA, Al Jabbari YS. Selective laser melting technique of co-cr dental alloys: a review of structure and properties and comparative analysis with other available techniques. J Prosthodont. 2015;24(4):303–12.
Sun J, Zhang FQ. The application of rapid prototyping in prosthodontics. J Prosthodont. 2012;21(8):641–4.
Williams R, Bibb R, Rafik T. A technique for fabricating patterns for removable partial denture frameworks using digitized casts and electronic surveying. J Prosthet Dent. 2004;91(1):85–8.
Bibb RJ, Eggbeer D, Williams R, Woodward A. Trial fitting of a removable partial denture framework made using computer-aided design and rapid prototyping techniques. Proc Inst Mech Eng H J Eng Med. 2006;220(7):793–7.
Williams R, Eggbeer D, Bibb R. CAD/CAM in the fabrication of removable partial denture frameworks: a virtual method of surveying 3-dimensionally scanned dental casts. Quintessence J Dent Technol. 2004;2(3):268–76.
Williams R, Bibb R, Eggbeer D, Collis J. Use of CAD/CAM technology to fabricate a removable partial denture framework. J Prosthet Dent. 2006;96(2):96–9.
Eggbeer D, Bibb R, Williams R. The computer-aided design and rapid prototyping fabrication of removable partial denture frameworks. Proc Inst Mech Eng H J Eng Med. 2005;219(3):195–202.
Wu J, Wang X, Zhao X, Zhang C, Gao B. A study on the fabrication method of removable partial denture framework by computer-aided design and rapid prototyping. Rapid Prototyp J. 2012;18(4):318–23.
Han J, Wang Y, Lü P. A preliminary report of designing removable partial denture frameworks using a specifically developed software package. Int J Prosthodont. 2010;23(4):370–5.
Nakata T, Shimpo H, Ohkubo C. Clasp fabrication using one-process molding by repeated laser sintering and high-speed milling. J Prosthodont Res. 2017;61(3):276–82.
Frank L, Kevin S, Mary K, Joseph N, Hsin-Nan C, Robert L. Applications of a hybrid manufacturing process for fabrication of metallic structures. Rapid Prototyp J. 2007;13(4):236–44.
Ohkubo C, Sato Y, Nishiyama Y, Suzuki Y. Titanium removable denture based on a one-metal rehabilitation concept. Dent Mater J. 2017;36(5):517–23.
Wu J, Li Y, Zhang Y. Use of intraoral scanning and 3-dimensional printing in the fabrication of a removable partial denture for a patient with limited mouth opening. J Am Dent Assoc. 2017;148(5):338–41.
Fueki K, Ohkubo C, Yatabe M, Arakawa I, Arita M, Ino S, et al. Clinical application of removable partial dentures using thermoplastic resin-part I: definition and indication of non-metal clasp dentures. J Prosthodont Res. 2014;58(1):3–10.
Takahashi Y, Hamanaka I, Isshi K. CAD/CAM-fabricated nonmetal clasp denture: in vitro pilot study. Int J Prosthodont. 2017;30(3):277–9.
Hamanaka I, Isshi K, Takahashi Y. Fabrication of a nonmetal clasp denture supported by an intraoral scanner and CAD-CAM. J Prosthet Dent. 2017;120(1):9–12.
Zoidis P, Papathanasiou I, Polyzois G. The use of a modified poly-ether-ether-ketone (PEEK) as an alternative framework material for removable dental prostheses. A clinical report. J Prosthodont. 2016;25(7):580–4.
Barazanchi A, Li KC, Al-Amleh B, Lyons K, Waddell JN. Additive technology: update on current materials and applications in dentistry. J Prosthodont. 2017;26(2):156–63.
Kattadiyil MT, Mursic Z, AlRumaih H, Goodacre CJ. Intraoral scanning of hard and soft tissues for partial removable dental prosthesis fabrication. J Prosthet Dent. 2014;112(3):444–8.
Alifui-Segbaya F, Williams RJ, George R. Additive manufacturing: a novel method for fabricating cobalt-chromium removable partial denture frameworks. Eur J Prosthodont Restor Dent. 2017;25(2):73–8.
Bibb R, Eggbeer D, Williams R. Rapid manufacture of removable partial denture frameworks. Rapid Prototyp J. 2006;12(2):95–9.
Williams R, Bibb R, Eggbeer D, Woodward A. A patient-fitted, CAD/CAM produced sacrificial pattern for a removable partial denture. Quintessence J Dent Technol. 2006;4:200–4.
Choi W, Woo Y-H, Kim H-S, Paek J. Comparison of internal adaptation of removable partial denture metal frameworks made by lost wax technique and printing technique of pattern using CAD. J Korean Acad Prosthodont. 2018;56(1):17–24.
Lang LA, Tulunoglu I. A critically appraised topic review of computer-aided design/computer-aided machining of removable partial denture frameworks. Dent Clin N Am. 2014;58(1):247–55.
Gan N, Ruan Y, Sun J, Xiong Y, Jiao T. Comparison of adaptation between the major connectors fabricated from intraoral digital impressions and extraoral digital impressions. Sci Rep. 2018;8(1):529.
Gan N, Xiong Y, Jiao T. Accuracy of intraoral digital impressions for whole upper jaws, including full dentitions and palatal soft tissues. PLoS One. 2016;11(7):e0158800.
Almufleh B, Emami E, Alageel O, de Melo F, Seng F, Caron E, et al. Patient satisfaction with laser-sintered removable partial dentures: a crossover pilot clinical trial. J Prosthet Dent. 2017;119:560–7.e1.
Ye H, Ning J, Li M, Niu L, Yang J, Sun Y, et al. Preliminary clinical application of removable partial denture frameworks fabricated using computer-aided design and rapid prototyping techniques. Int J Prosthodont. 2017;30(4):348–53.
Lee JW, Park JM, Park EJ, Heo SJ, Koak JY, Kim SK. Accuracy of a digital removable partial denture fabricated by casting a rapid prototyped pattern: a clinical study. J Prosthet Dent. 2017;118(4):468–74.
Alageel O, Abdallah MN, Alsheghri A, Song J, Caron E, Tamimi F. Removable partial denture alloys processed by laser-sintering technique. J Biomed Mater Res B Appl Biomater. 2018;106(3):1174–85.
Torii M, Nakata T, Takahashi K, Kawamura N, Shimpo H, Ohkubo C. Fitness and retentive force of cobalt-chromium alloy clasps fabricated with repeated laser sintering and milling. J Prosthodont Res. 2018;62(3):342–6.
Arnold C, Hey J, Schweyen R, Setz JM. Accuracy of CAD-CAM-fabricated removable partial dentures. J Prosthet Dent. 2017;119(4):586–92.
Abduo J, Lyons K, Bennamoun M. Trends in computer-aided manufacturing in prosthodontics: a review of the available streams. Int J Dent. 2014;2014:15.
Fueki K, Ohkubo C, Yatabe M, Arakawa I, Arita M, Ino S, et al. Clinical application of removable partial dentures using thermoplastic resin. Part II: material properties and clinical features of non-metal clasp dentures. J Prosthodont Res. 2014;58(2):71–84.
Tannous F, Steiner M, Shahin R, Kern M. Retentive forces and fatigue resistance of thermoplastic resin clasps. Dent Mater. 2012;28(3):273–8.
Kibi M, Ono T, Dong J, Mitta K, Gonda T, Maeda Y. Development of an RPD CAD system with finite element stress analysis. J Oral Rehabil. 2009;36(6):442–50.
Chen J, Ahmad R, Suenaga H, Li W, Sasaki K, Swain M, et al. Shape optimization for additive manufacturing of removable partial dentures—a new paradigm for prosthetic CAD/CAM. PLoS One. 2015;10(7):e0132552.
Lee JH, Lee CH. A stereolithographic resin pattern for evaluating the framework, altered cast partial removable dental prosthesis impression, and maxillomandibular relationship record in a single appointment. J Prosthet Dent. 2015;114(5):625–6.
Campbell SD, Cooper L, Craddock H, Hyde TP, Nattress B, Pavitt SH, et al. Removable partial dentures: the clinical need for innovation. J Prosthet Dent. 2017;118(3):273–80.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Almufleh, B., Tamimi, F., Caron, E., Alageel, O. (2019). 3D-Printed Removable Partial Dentures. In: Tamimi, F., Hirayama, H. (eds) Digital Restorative Dentistry . Springer, Cham. https://doi.org/10.1007/978-3-030-15974-0_5
Download citation
DOI: https://doi.org/10.1007/978-3-030-15974-0_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-15973-3
Online ISBN: 978-3-030-15974-0
eBook Packages: MedicineMedicine (R0)