
Abstract
Human embryonic hypothalamo-pituitary development is a complex process controlled by a spatio-temporal genetic cascade of transcription factors and signalling molecules within the hypothalamus and Rathke’s pouch, the primordium of the anterior pituitary (AP). The anterior and intermediate lobes of the pituitary derive from the oral ectoderm and the posterior lobe from the overlying neural ectoderm. The tightly regulated processes of cell proliferation and differentiation give rise to five different specialized AP cell types that secrete six hormones. Disordered embryogenesis can give rise to congenital hypopituitarism (CH), characterized by deficiencies in one or more of these six hormones in isolation or as combined pituitary hormone deficiency, with a wide variation in severity. CH may present early in the neonatal period or later in childhood, with midline and craniofacial structural abnormalities often accompanying the phenotype, giving rise to a range of highly variable disorders that will be discussed in this chapter.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Hypothalamo-Pituitary Development
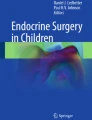
The mature pituitary gland is a central regulator responsible for controlling growth, metabolism, reproduction and development and homeostasis through the regulation and function of other endocrine glands in the body [1]. The pituitary gland is situated within the sella turcica recess of the sphenoid bone at the base of the brain and consists of three lobes derived from two adjacent ectodermal layers: the anterior and intermediate lobes from the oral ectoderm and the posterior lobe from the neural ectoderm [2, 3]. Hypothalamo-pituitary (HP) development is dependent on the communication between the oral ectoderm and the overlying neural ectoderm. This occurs through a complex spatio-temporal genetic cascade of transcription factors and signalling molecules that may be either intrinsic or extrinsic to the developing Rathke’s pouch, the primordium of the anterior pituitary (AP) [4]. A series of tightly regulated steps that result in cell proliferation and differentiation give rise to the five different specialized AP cell types that secrete six hormones: somatotrophs [growth hormone (GH)], thyrotrophs [thyroid-stimulating hormone (TSH)], gonadotrophs [luteinizing hormone (LH) and follicle-stimulating hormone (FSH)], lactotrophs [prolactin (PRL)] and the corticotrophs [adrenocorticotropic hormone (ACTH)] [5] (Fig. 1.1).

A flowchart illustrating human embryonic hypothalamo-pituitary development. A complex spatio-temporal genetic cascade of transcription factors and signalling molecules, intrinsic or extrinsic, to the developing Rathke’s pouch. A series of tightly regulated steps result in cell proliferation and differentiation to give rise to the five different specialized anterior pituitary cell types that secrete six hormones. Specific peptides derived from the hypothalamus regulate the synthesis of these hormones by binding to their respective receptors on each anterior pituitary cell type
The synthesis of each one of the six anterior pituitary hormones is regulated by specific hypothalamic peptides. Many of these ligands travel via the hypophyseal portal system from the hypothalamus into the bloodstream, a transport system that allows rapid communication and migration of hormones to the anterior pituitary. The ligands bind to their respective receptors on each specific anterior pituitary cell type, giving rise to the six hormones that have targets elsewhere in the body, and play distinct roles in endocrine regulation (Fig. 1.1).
Human Conditions Arising from Disordered Hypothalamo-Pituitary Development
Congenital hypopituitarism (CH) is characterized by deficiencies in one or more of these six hormones, with GH being the most frequently occurring hormone deficiency and often seen in isolation [4]. It is a syndrome with a wide variation in severity and may present early in the neonatal period or later in childhood. Midline and craniofacial structural abnormalities are often associated with CH, giving rise to a range of highly variable disorders, ranging from fatality to holoprosencephaly (HPE) , septo-optic dysplasia (SOD) and Kallmann syndrome (KS) , characterized by hypogonadotropic hypogonadism (HH) with anosmia [6]. Thus, disordered embryogenesis can cause variable phenotypes involving a range of craniofacial midline defects, associated with HP disorders. All causative genes for congenital hypopituitarism and related disorders and their inheritance patterns are listed in Table 1.1 and are discussed throughout this chapter.
Isolated Growth Hormone Deficiency
Growth hormone-releasing hormone (GHRH) is released from the hypothalamus and binds to its receptor (GHRHR) on somatotroph cells. This results in the synthesis and release of GH, in the presence of the transcription factor POU1F1 [7]. GH then binds to its receptors on target tissues, primarily the liver, leading to the release of insulin-like growth factor 1 (IGF1) and its binding protein, IGFBP3. The most common isolated deficiency is congenital isolated GH deficiency (IGHD) that has an incidence between 1/4000 and 1/10,000 live births. The majority of cases are sporadic, with a small percentage (3–30%) of familial cases, the aetiology being unknown in most patients [8, 9]. Short stature, ranging from moderate to severe, is the essential phenotypic feature in IGHD and is associated with a poor growth velocity with delayed skeletal maturation. Children with GHD are usually treated with recombinant human GH (rhGH ) and generally respond well [9]. A number of genetic forms of GHD have been described. Autosomal recessive IGHD type IA patients present with severe growth failure in the first 6 months of life with undetectable GH concentrations. These patients frequently develop anti-GH antibodies after receiving exogenous GH, which prevent the growth response anticipated after rhGH therapy [10]. Heterogeneous homozygous GH1 deletions, most frequently measuring 6.7 kb in length, were first described and remain the most common GH1 gene alteration in patients with IGHD type IA [11], with other severe loss-of-function GH1 mutations described subsequently (Table 1.1).
Type IB GHD is associated with recessive mutations in GH1 and GHRHR, the latter also known as Sindh dwarfism [12]. Missense, frameshift, nonsense or splice site mutations may occur in GH1 in patients from consanguineous pedigrees and specific ethnic backgrounds, for example, IVS4 + 1G → T, p.G120 V and p.C182X, respectively [5, 13, 14]. Type IB GHD due to GHRHR mutations is not a classical IGHD phenotype, in that these patients have minimal facial hypoplasia and no microphallus but do manifest anterior pituitary hypoplasia (APH) on magnetic resonance imaging (MRI) [15]. Patients that harbour GHRHR mutations are usually from consanguineous pedigrees from Brazil or the Indian subcontinent [16]. The vast majority of GHRHR mutations are associated with complete loss of function, for example, p.W273S and p.A176V [8, 17], and usually affect cAMP production, such as the p.K329E substitution that fails to show any cAMP response following GHRH treatment in in vitro studies [18]. The first, and still the most common, GHRHR mutation is p.E72X resulting in a truncated protein devoid of both the transmembrane and intracellular domains (Wajnrajch et al. 1996). A recent study described a novel partial loss-of-function homozygous GHRHR mutation , p.P79L, which gives rise to an unusually mild form of IGHD in two unrelated families. The patients were compound homozygous, with a second homozygous variant in GHRHR, p.R4Q, which was not associated with functional impairment [19].
Heterozygous mutations in the GH1 gene commonly affect splicing resulting in exon skipping, leading to the most common autosomal dominant form of GHD, known as type II GHD [20] (Table 1.1). The shorter 17.5 kDa GH isoform, resulting from the skipping of exon 3, has been reported to exert a dominant negative effect on GH secretion, with expression levels directly related to severity of the disorder [21, 22]. Heterozygous GH1 missense mutations , such as p.E32A, p.R178H and p.R183H, have also been described in GHD type II. These patients have variable height deficit and severity, occasionally with a height within the normal range, and may develop additional pituitary hormone deficiencies over time, including ACTH, TSH and gonadotrophin deficiencies [8]. To date, no mutations in GHRH have been described in association with IGHD.
In addition to GH1 and GHRHR, mutations have recently been reported in RNPC3 in patients with GHD. The RNA-binding region (RNA recognition motifs [RRM]) containing 3 on chromosome 1 encodes a 65 K protein component of the U12-type spliceosome. It contains two bipartite nuclear targeting sequences important for nuclear targeting for proteins, especially those functioning in the cell nucleus itself, and its two RRM motifs suggest that it may contact one of the small nuclear RNAs of the minor spliceosome [23]. Biallelic mutations in RNPC3 have been described in three sisters with severe IGHD and pituitary hypoplasia, where anomalies were identified in U11/U12 di-snRNP formation and the splicing of multiple U12-type introns in these patient cells [24]. Through RNA sequencing the authors identified a list of 21 genes with significantly decreased U12/U2 ratios in patient cells, as well as aberrant processing events including exon skipping and activation of cryptic U2-type splice sites [24]. A subset of the 21 genes were found to encode proteins with relevant functions in pituitary development, such as SPCS2 and SPCS3 that encode subunits of the signal peptidase complex, implicated in post-translational processing of preprohormones such as preproghrelin to proghrelin [24, 25], thus themselves becoming candidates for GHD. However, the exact mechanism underlying the GH deficiency remains to be established.
No murine model for Rnpc3 loss of function exists; however studies using a zebrafish mutant model with an induced lethal point mutation in rnpc3 have provided a useful and specific model of aberrant U12-type splicing in vivo. Results showed that the formation of aberrant U11- and U12-containing snRNAs sufficiently impaired the efficiency of U12-type splicing to cause arrested development in the intestine, liver and pancreas. Analysis of the zebrafish transcriptome revealed that efficient mRNA processing is a critical process for the growth and proliferation of cells during vertebrate development [26]. Additionally, mutations have occasionally been described in IGHD patients in genes encoding early (HESX1, SOX2, SOX3 and OTX2) or late (PROP1 and POU1F1) transcription factors implicated in murine and human pituitary development [9, 27, 28].
Other Isolated Hormone Deficiencies and Abnormalities
Congenital functional failure of a single lineage has been reported for all pituitary cell types, giving rise to isolated hormone deficiencies other than IGHD, such as isolated TSH deficiency (TSHD) , isolated hypogonadotropic hypogonadism [IHH; LH and FSH deficiency] that may be part of KS, isolated ACTH deficiency (IAD) and, very rarely, isolated PRL deficiency (PRLD) [29]. Interestingly, an increased prolactin is more likely to occur in children with congenital hypopituitarism , particularly those with midline defects, as opposed to a decrease. Although rare, isolated PRLD also known as hypoprolactinaemia clinically manifests only in women as puerperal alactogenesis , namely, the failure of milk production during breastfeeding [30]. One such familial case involved a mother and daughter that had eight pregnancies cumulatively, all followed by puerperal alactogenesis resulting from isolated PRLD [31]. The aetiology of isolated PRLD is as yet unknown, and candidate genes often screened are those found to be mutated in patients with PRLD as part of combined pituitary hormone deficiency (CPHD) and that are known to be involved in the lineage differentiation of lactotrophs, such as POU1F1, PROP1, LHX3, LHX4, HESX1 and OTX2 [32] (Table 1.1).
In TSHD, inadequate thyroid hormone biosynthesis occurs due to defective stimulation of the thyroid gland by TSH, therefore causing central, or secondary, hypothyroidism in the affected patients. In some rare cases, mutations in genes regulating TSH biosynthesis and secretion, namely, TSHB, TRHR and more recently IGSF1, have been described in patients with isolated TSHD [33, 34]. In addition, a homozygous frameshift mutation in PROP1 in a pedigree has been reported to be associated with isolated central hypothyroidism presenting at a young age [35], indicating that this well-known CPHD causative gene should also be considered in the diagnosis of TSHD.
Mutations in TSHB, encoding the TSHβ subunit, have previously been identified in hypothyroid patients, with TSH concentrations that are highly variable, and not always detectable [36, 37]. The most frequently occurring TSHB mutation, c.373delT (C105Vfs114X) [37], causing secondary hypothyroidism is known as a mutational ‘hotspot’ in TSHB and has been identified in homozygous form in several populations worldwide [38]. It has also been identified in compound heterozygosity with p.Q49X [39], a 5.4kb TSHB deletion (c.1-4389_417*195delinsCTCA) and a missense p.M1P variant [40], amongst others. Screening using both T4 and TSH is a highly sensitive method for detecting congenital hypothyroidism in neonates and helps prevent mental retardation, which could be a consequence of delayed diagnosis [41].
Rare recessive biallelic inactivating mutations in TRHR , namely, p.S115-T117del and p.A118T, have been reported in three affected individuals from two unrelated pedigrees with central congenital hypothyroidism (CCH) , with absent TSH and prolactin responses to exogenous TRH [42, 43]. More recently, the p.P81R missense mutation described in isolated CCH highlights the importance of the second transmembrane helix in mediating TRH receptor activation via hormone binding, making it the first deleterious missense TRHR defect that gives rise to CCH [44]. In addition, a recently identified novel homozygous mutation, p.I131T, that decreases TRH affinity was identified in an overweight patient with CCH and normal stature [33].
More recently, IGSF1 mutations have been associated with an X-linked form of central hypothyroidism associated with macroorchidism; mutations include missense, nonsense, frameshift and submicroscopic gene deletions incorporating IGSF1 [34, 45]. Igsf1 is expressed in murine pituitary thyrotroph, lactotroph and somatotroph cells [34] and in Leydig and germ cells in murine/human testes, with very low levels in Sertoli cells [46]. Furthermore, the latter study implies that IGSF1 stimulates transcription of TRHR by negative modulation of the TGFβ1-Smad signalling pathway, thereby enhancing TSH synthesis and biopotency. In contrast, IGSF1 is suggested to downregulate the activin-Smad pathway, leading to reduced expression of FSHB secreted by gonadotropes. The authors describe a large hemizygous 207.873 Kb deletion on Chr. Xq26.2 associated with hypothyroidism with reduced TSH biopotency, increased secretion of FSH in neonatal minipuberty and macroorchidism from 3 years of age [46]. Macroorchidism does not appear to be a phenotypic feature in all patients with IGSF1 mutations [47], and interestingly, heterozygous female carriers of these IGSF1 mutations may sometimes manifest mild hypothyroidism [48]. Igsf1-deficient male mice (Igsf1_ex1male) show diminished pituitary and serum TSH concentrations, pituitary TRH receptor expression and triiodothyronine concentrations and increased body mass [34]. Recent studies have shown that Igsf1-deficient male mice with a loss-of-function mutation in the C-terminal domain exhibit reduced expression of the TSH subunit genes as well as TSH and TRH proteins. Addition of exogenous TRH resulted in TSH release, albeit to a significantly lesser extent than wild-type littermates [49].
The X-linked transducin β-like protein 1 (TBL1X) gene is a component of the thyroid hormone receptor-corepressor complex, mutations in which have been previously associated with sensorineural hearing loss [50]. In a recent study, six mutations in unrelated pedigrees with congenital isolated central hypothyroidism have been identified [51]. Like IGSF1, TBL1X is associated with an X-linked form of TSHD.
Isolated ACTH deficiency (IAD ) is a very rare and heterogeneous condition making diagnosis very difficult due to the varied clinical presentation. It may be lethal due to the hypocortisolism and has also been associated with neonatal hypoglycaemia, convulsions, hypercalcaemia [52] and/or cholestasis that can be associated with a 20% mortality rate if unrecognized [53, 54]. IAD patients have also presented with an empty sella and severe hyponatraemia [55]. TBX19 , formally known as TPIT, plays a critical role in the terminal differentiation of the pituitary pre-pro-opiomelanocortin (POMC) lineages, namely, corticotrophs and melanotrophs . Mutations in TBX19 have been associated with early-onset IAD [56] and have been found in up to 2/3 of neonatal cases, with complete or severe loss of function as exemplified by studies of DNA binding and/or transactivation [57]. These TBX19 mutations are most often substitutions in the DNA-binding Tbox domain, thereby resulting in impaired DNA binding or protein-protein interaction. However, premature stop codons, aberrant splicing and chromosomal deletions have also been reported in this gene [58]. A recent study described compound heterozygosity in TBX19, with a novel frameshift p.Arg222Lysfs*4 mutation and the previously described p.R286X mutation, respectively, in a patient with IAD combined with recurrent respiratory tract infections. The authors concluded that adrenal insufficiency should be considered in patients with unexplained recurrent infections to prevent a delay in diagnosis [59].
The serial cleavage of POMC by prohormone convertases (PCs) generates ACTH in corticotrophs (PC1) and melanocyte-stimulating hormone (αMSH) in melanotrophs (PC2) that bind to the melanocortin receptors (MC2-R, MC1-R and MC4-R, respectively) [60,61,62]. POMC mutations have been reported in association with IAD. MC1-R function is known to contribute towards hair and skin pigmentation in both mice and humans [63]. ACTH is the only known ligand for MC2-R located in the adrenals [64]. Antagonistic studies on MC4-R signalling have revealed its involvement in the regulation of food intake and in the aetiology of severe obesity in mice [65], which occurs in the absence of the MC4-R ligand α-MSH. Therefore patients with POMC mutations usually have the distinct phenotypic hallmarks of early-onset obesity and red hair, in addition to adrenal insufficiency with hypocortisolism and hypoglycaemia. The first POMC mutations described were the compound heterozygous p.G7013 T/p.C7133Δ and the homozygous p.C3804A identified, respectively, in such patients [66]. Compound heterozygosity has also been described in PCSK1, encoding PC1, in a female patient with ACTH and gonadotrophin deficiency, with severe obesity and glucose dysregulation [67]. PC1 has since been described as being essential for the normal absorptive function of the human small intestine, with compound heterozygosity identified in a second patient with malabsorptive severe refractory neonatal diarrhoea as the predominant phenotype. This patient, similar to the first, also had obesity, hypoadrenalism, reactive hypoglycaemia and elevated circulating levels of specific prohormones [68]. PC1-null mice confirm defective POMC and proinsulin processing seen in PC1-deficient humans; however, mice are growth retarded rather than obese [69]. Subsequent PCSK1 mutations have since been identified in patients, such as the nonsense p.Arg80* loss-of-function mutation, which produces a truncated protein with only 2 exons out of 14, and that co-segregated with obesity in a three-generation family [70]. Furthermore, recent studies have generated PCSK1 (PC1)-deficient human embryonic stem cell (hESC) lines, differentiated into hypothalamic neurons, to investigate POMC processing. Results showed that unprocessed POMC increased and processed POMC-derived peptides in PCSK1 knockout hESC-derived neurons decreased in cells, which phenotypically copies the POMC processing reported in PC1-null mice and PC1-deficient patients [71]. PC1/3-deficient patients often manifest hypothyroidism and hypocortisolism. However some patients may also present with an elevated TSH and ACTH, respectively [72]. In rare cases, GHD and diabetes insipidus may also occur in these patients, thus broadening disease manifestation in PCSK1 insufficient patients [73].
Septo-Optic Dysplasia
SOD , also known as de Morsier syndrome , occurs in 1/10,000 live births with equal prevalence in males and females. It is a heterogeneous disorder with a variable phenotype, loosely defined by any combination of the triad of optic nerve hypoplasia (ONH), midline neuroradiological abnormalities (such as agenesis of the corpus callosum and absence of the septum pellucidum) and pituitary hypoplasia with consequent endocrine deficits [74, 75]. Approximately 40% of SOD patients may actually present with normal endocrinology. Intriguingly, SOD is associated with a younger maternal age, when compared with mothers of children with isolated defects of the HP axis [76]. The reason for this maternal age effect is unknown but has been suggested to be associated with increased maternal drug and alcohol abuse [77, 78]. Approximately 75–80% of patients exhibit ONH, which may be unilateral or, more commonly , bilateral (88% as compared with 12% unilateral cases), and may be the first presenting feature with later onset of endocrine dysfunction [79]. In rare cases, the eye abnormality may be more severe, resulting in microphthalmia or anophthalmia [80], where one or both of the eyes are abnormally small or completely absent, respectively. The association of midline abnormalities with hypopituitarism has long been established, suggesting a common developmental origin of the hypothalamus and pituitary and the midline structures within the brain [81]. Mutations in the gene encoding the transcriptional repressor HESX1 were the first to be associated with the pathogenesis of rare cases of SOD [82, 83]. Significant insights into the pathogenesis of the disorder were provided by the original studies, whereby murine transgenesis resulted in murine phenotypes highly reminiscent of SOD. Thereafter, human mutations have been cloned into mouse models and studied in depth, such as the first HESX1 mutation (p.R160C) identified [84]. More recently, SOX2, SOX3 and OTX2 have been shown to be mutated in rarer forms of SOD, with severe bilateral eye defects including microphthalmia or anophthalmia in patients with SOX2 and OTX2 mutations, and abnormalities of the hypothalamus, pituitary and the infundibulum as well as the corpus callosum in patients with SOX3 mutations [85] (Table 1.1). Recently, mutations in genes implicated in KS have also been linked with SOD; for example, two heterozygous KAL1 mutations were identified in three females from two unrelated families with SOD [86]. Prior to this, three patients with SOD were reported to have heterozygous mutations in FGFR1 that altered receptor signalling, with one predicted to affect splicing [87]. The same report also identified a heterozygous loss-of-function mutation, p.R268C, in PROKR2. This variant had previously been implicated in normosmic HH and KS. The heterozygous missense FGF8 mutation, p.Q216E, has also been described in an SOD patient with microcephaly and neurological defects. Interestingly, FGF8 has also been implicated in a patient with semilobar HPE, diabetes insipidus and TSH and ACTH insufficiency [6], making this KS gene a new candidate for both SOD and HPE. More recently, a defined role for TCF7L1 in the aetiology of SOD has been described. Conditional deletion of murine Tcf7L1 results in forebrain defects and partially penetrant dwarfism [88]. Heterozygous missense TCF7L1 variants were then subsequently identified in two unrelated SOD patients [88].
SOD can be associated with a wide range of phenotypic variability, highlighting the complexity of the disorder and suggesting the impact of both genetic and environmental factors involved in the aetiology of the disease [89]. Other associated features include developmental delay, seizures, visual impairment, sleep disturbance, precocious puberty, obesity, anosmia, sensorineural hearing loss and cardiac anomalies [77]. The majority of cases remain aetiologically unexplained. The following section describes the role of the genes linked with this disorder and other CH syndromes to date.
HESX1
The transcription factor HESX1 is a member of the paired-like class of homeodomain proteins which acts as a transcriptional repressor essential for pituitary organogenesis [83]. Binding partners of human HESX1 such as transducing-like enhancer of split 1 (TLE1) (ortholog of Groucho in Drosophila), the nuclear corepressor (N-COR) and DNA methyltransferase 1 (DNMT1) can all form complexes to enable it to exert its repressive activity [90, 91]. Hesx1 is one of the earliest markers of murine pituitary development, expressed initially during gastrulation in the region fated to form the forebrain and ventral diencephalon, and is then restricted to Rathke’s pouch by embryonic day (E) 9.0 [92]. Hesx1 continues to be expressed in the developing AP until E12, when it then disappears in a spatio-temporal sequence that corresponds to progressive pituitary cell differentiation [4]. Hesx1 transcripts have totally disappeared from the entire ventral portion by E13, giving rise to the anterior lobe of the pituitary [93]. A homozygous null mutation in mice results in a phenotype that resembles SOD, with 5% of Hesx1 null mice exhibiting a severe phenotype with no AP [90]. This is consistent with an insertion mutation in exon 3 in the ‘Alu’ element of HESX1 which was identified in a patient with a retinal coloboma associated with aplasia of the AP. The reported patient had undetectable concentrations of all AP hormones [94]. Patients with HESX1 mutations have variably penetrant phenotypes ranging from isolated GHD, evolving hypopituitarism in the absence of midline and eye defects, through to SOD and pituitary aplasia [95]. Hesx1 null mice show great phenotypic variability with features that include a reduction in forebrain tissue, craniofacial dysplasia with a short nose and absence of developing optic vesicles. These mice also have a significantly decreased head size, absence of telencephalic vesicles, absence of olfactory placodes, hypothalamic and infundibular abnormalities, and aberrant morphogenesis of Rathke’s pouch [83]. Rathke’s pouch formation was variably affected, and abnormal bifurcations were apparent, resulting in multiple pituitary glands in a proportion of the mice [82, 83, 96]. Although of variable severity, both neonatal and adult homozygous mutant mice manifested phenotypes that presented with eye defects such as microphthalmia and anophthalmia , with abnormalities of the septum pellucidum and corpus callosum, closely resembling SOD in humans.
SOX2 and SOX3
SOX2 and SOX3 are members of the SOXB1 subfamily of ‘SRY-related HMG box’ transcription factors. They have an N-terminal domain of unknown function, a DNA- binding high mobility group (HMG) box domain and a longer C-terminal domain involved in transcriptional activation [97]. Members of the SOXB1 subfamily are expressed throughout the CNS and are amongst the earliest neural markers that play a role in neuronal determination [98]. Murine Sox3 is shown to be involved in neurogenesis through its expression in actively dividing undifferentiated neural progenitor cells, and this expression is maintained throughout development [99]. Expression of Sox3 is also seen in the ventral diencephalon, infundibulum and presumptive hypothalamus, a similar expression pattern to that of Wnt5a expression [100]. Sox3-deficient mice exhibit expanded BMP and FGF signalling domains as well as abnormalities in Rathke’s pouch [101], suggesting a possible mechanism underlying the hypopituitary phenotype in these mutants [102]. The mutant mice exhibited variable complex phenotypes including craniofacial abnormalities, midline CNS defects and a reduction in size and fertility [101]. Mutations in SOX3 are usually associated with infundibular hypoplasia and an ectopic or undescended PP and have been shown to result in aggresome formation and impaired transactivation [103]. Duplications within the Xq24-q27.3 region [104], incorporating SOX3, have long been associated with X-linked hypopituitarism and mental retardation. SOX3 was the only gene that was found to be expressed in the murine infundibulum out of three annotated in the smallest duplication (690Kb) to date. Submicroscopic SOX3-spanning duplications at position Xq27.1 have since been described in patients with variable hypopituitary phenotypes including CPHD , absence or hypoplasia of the infundibulum and an abnormality of the corpus callosum [85]. Polyalanine expansions of SOX3 were initially associated with X-linked mental retardation and IGHD in a French pedigree that harboured an in-frame duplication of 33 bp encoding for 11 alanines in the SOX3 gene [105]. A further SOX3 polyalanine expansion was later associated with loss of function in a transcriptional assay in an X-linked pedigree with hypopituitarism [85]. Additionally, a 2.31-Mb deletion on Xq27, again incorporating SOX3, was identified in a patient with haemophilia B due to the loss of factor IX and CH due to loss of SOX3, with the unusual phenotype of a persistent craniopharyngeal canal on MRI [106], a phenotype that was replicated in Sox3 null mice. Furthermore, an 18 bp deletion in the polyalanine tract of SOX3 (p.A243_A248del6) was identified in a CH patient, resulting in an increase in transcriptional activation [107]. These data highlight the critical gene dosage of SOX3 in normal development of the diencephalon and infundibulum and consequently the AP.
SOX2 is expressed in neural progenitor populations throughout the developing and adult CNS and is necessary to maintain their progenitor identity [108]. After gastrulation, murine Sox2 expression is restricted to the presumptive anterior neuroectoderm and, by E9.5, is expressed throughout the CNS, brain, sensory placodes, branchial arches, gut endoderm, oesophagus and trachea. Homozygous null Sox2 mice fail to survive and die shortly after implantation [109], whereas heterozygous mice manifest hypoplasia and abnormal morphology of the AP, with subsequent reduction in GH, LH, ACTH and TSH concentrations [110]. Other studies have shown that retinal progenitor cells with conditionally ablated Sox2 lose competence to both proliferate and terminally differentiate. Additionally, Sox2 hypomorphic/null mice, with a 40% reduction of Sox2 expression compared to wild-type (WT) mice, present with variable microphthalmia as a result of aberrant neural progenitor differentiation. Furthermore, this study suggests that Sox2/SOX2 activity functions in a dose-dependent manner in retinal progenitor cell differentiation [111]. The first description of SOX2 mutations in humans was in a cohort of individuals with severe eye phenotypes. De novo mutations were associated with bilateral anophthalmia , or severe microphthalmia, with accompanying developmental delay, learning difficulties, oesophageal atresia and genital abnormalities in males [112]. SOX2 expression in humans is observed throughout the human brain, including the developing hypothalamus as well as Rathke’s pouch and the eye [80]. Following on from these studies, SOX2 mutations have also been associated with AP hypoplasia and hypogonadotropic hypogonadism (HH) [110] and are usually associated with loss of function. These de novo mutations result in a loss of DNA binding, nuclear localization or transcriptional activation, suggesting that the phenotypes arise as a result of haploinsufficiency of SOX2 during development. Conditional deletion of Sox2 mutant mice in the hypothalamus and pituitary is associated with impaired gonadotrophin secretion as well as TSH and GH deficiencies. This suggests a critical role for Sox2 in the hypothalamus and/or the developing pituitary, particularly with respect to GnRH neuron specification [113]. In addition, SOX2 haploinsufficiency has been implicated in the generation of slow-progressing pituitary tumours in patients [114]. Furthermore, a very recent study [115] has implicated a role for SOX2 in melanotrope cell fate acquisition, independent of its early role in promoting progenitor proliferation. This study showed that SOX2 is maintained at low levels in melanotropes [115] where its expression is likely regulated by P27 [116]. Murine cells expressing Sox2 and E-cadherin are found throughout the RP in embryos but persist scattered throughout the adult gland, predominantly within a narrow zone lining the pituitary cleft. These postnatal Sox2+ cells also express Sox9 and S100 [117]. Interestingly, both embryonic and adult Sox2+ pituitary progenitor/stem cells have shown the ability to differentiate into all hormone-producing lineages, contributing to organ homeostasis during postnatal life. Furthermore, the targeted expression of oncogenic β-catenin in Sox2+ cells gives rise to pituitary tumours [118]. Therefore Sox2+ pituitary stem/progenitor cells not only seem to be involved in long-term physiological maintenance of the adult pituitary, but they also appear accountable for driving tumorigenesis in vivo.
OTX2
OTX2 (orthodenticle homeobox 2) is a transcription factor that is required for the formation of anterior structures and maintenance of the forebrain and has been implicated in 2–3% of anophthalmia-/microphthalmia-related syndromes in humans [82]. In mice, the expression of Otx2 is localized to developing neural and sensory structures of the brain such as the cerebellum, the eye, nose and ear and is required at multiple steps in brain development and neuronal differentiation [119]. Mice homozygous for mutations die from severe brain abnormalities after exhibiting malformations in both the forebrain and the eye due to impaired gastrulation. Heterozygous mice can display a range of phenotypes from normal to severe forms of eye/brain abnormalities such as anophthalmia and HPE [120]. During retinal development, Otx2 regulates retinal pigment epithelium specification and photoreceptor and bipolar cell differentiation and maturation, with expression being maintained in these three cell types throughout life [121]. Otx2 transcripts and protein are normally detectable at E10.5 in both the ventral diencephalon and Rathke’s pouch. By E12.5 Otx2 transcripts are undetectable in Rathke’s pouch but persist in the ventral diencephalon until E14.5, and by E16.5, no Otx2 transcripts are detected in either structure [122]. A previous study showed that Otx2 expression persisted in Rathke’s pouch until E16.5 in Prop1-mutant mice, 4 days after the peak of Prop1 expression and 2 days after any pituitary defects become apparent [122]. This study suggests that Prop1 regulates expression of other factors that suppress Otx2, implying a role for Otx2 in murine pituitary development. Another study reported an HH phenotype in GnRH-neuron-Otx2 knockout mice [123]. These murine data are consistent with human OTX2 phenotypes, which are highly variable and include IGHD, hypopituitarism and HH, usually, but not invariably, associated with severe ocular malformations [124]. Furthermore, OTX2 regulates expression of transcription factors HESX1 and POU1F1, thereby influencing anterior pituitary development. In vitro functional analysis showed that mutant Otx2 abolished activation of the HESX1 promoter and was hypomorphic on the POU1F1 promoter [125]. Despite this knowledge, the precise role of OTX2 in hypothalamo-pituitary development still remains unclear [3]. In addition, in vivo otocephaly gene suppression studies show that OTX2 loss-of-function mutations modify otocephaly and/or dysgnathia phenotypes in humans when in the presence of a second known otocephaly gene mutation. This suggests that mutant OTX2 contributes to the severity of craniofacial defects, such as those affecting the lower jaw [126].
GLI2
The GLI family zinc finger 2 (GLI2) transcription factor is a component of the SHH signalling pathway, known to be implicated in HPE and other midline neurodevelopmental anomalies [127, 128]. Unlike mutated SHH, described to specifically cause HPE, mutated GLI2 is also associated with CH in the absence of midline brain defects [129]. These patients have variable phenotypes ranging from IGHD to complex CPHD, in combination with variable polydactyly, cleft lip/palate, diabetes insipidus, dysmorphic features and an ectopic posterior pituitary on MRI [130,131,132]. Truncated GLI2 is often reported in such cases, for example, p.L788fsX794, p.L694fsX722 and p.E380X, respectively [130], with complete loss of the C-terminal activator domain. In addition, haploinsufficient missense mutations such as p.E518K [129] and p.R516P [133], for example, have been implicated in the aetiology of CH in these patients. Incomplete or variable penetrance may also be apparent for GLI2 mutations, where a heterozygous mutation with functional consequences in the child is present in the unaffected parent or a parent with a mild form of the disease, respectively [129].
Pituitary Stalk Interruption Syndrome
Pituitary stalk interruption syndrome (PSIS) is characterized by a thin or discontinuous pituitary stalk, pituitary gland insufficiency and APH and/or an EPP on MRI. Interestingly, a novel missense mutation in CDON, another member of the SHH signalling pathway that causes HPE, has been reported in a patient with PSIS, with neonatal hypoglycaemia and cholestasis associated with GH, TSH, and ACTH deficiencies, without HPE [134]. This again demonstrates how mutated members of this crucial pathway may elicit other hypopituitary-related phenotypes, aside from their more established association with HPE. GPR161, encoding the orphan G protein-coupled receptor 161, a transmembrane protein, has also been implicated in PSIS. Whole exome sequencing revealed a homozygous missense mutation, p.L19Q, in a consanguineous family with two affected siblings with PSIS [135]. Despite the lack of functional analysis, prediction models and the hypothesis that GPR161 interacts with GLI2, GLI3 and the SHH pathway suggest a possible involvement of this gene in the aetiology of patients with PSIS [135]. ROBO1 is a receptor involved in Slit/Robo signalling that essentially controls embryonic axon guidance and branching in the nervous system during development [136]. ROBO1 is another gene that has recently been implicated in PSIS; a novel heterozygous frameshift, a nonsense and a missense mutation (p.A977Qfs*40, p.Y1114* and p.C240S, respectively) were identified in five affected patients. Ocular anomalies including hypermetropia with strabismus and ptosis were present in four out of five patients with PSIS (two familial and one sporadic case) [137]. Known CH causative genes including LHX4, OTX2, HESX1, SOX3, and PROKR2 have also been described to be mutated in rare cases of PSIS [28, 138, 139].
ARNT2
ARNT2 (aryl hydrocarbon receptor nuclear translocator 2) is a member of the basic helix-loop-helix-Per-Arnt-Sim (bHLH-PAS) superfamily of transcription factors. This protein forms heterodimers with sensor proteins from the same family that then bind regulatory DNA sequences. Arnt2(-/-) null murine embryos die perinatally and exhibit impaired hypothalamic development [140]. Recent studies showed expression of ARNT2 within the CNS, including the hypothalamus, as well as the renal tract during human embryonic development. A homozygous frameshift ARNT2 mutation has been described in several individuals born to a highly consanguineous pedigree with congenital hypopituitarism. These patients exhibit GH, TSH and ACTH deficiencies associated with diabetes insipidus, progressive neurological abnormalities with microcephaly, renal tract abnormalities and post-retinal visual pathway dysfunction, indicating the essential role of ARNT2 in HP development and postnatal brain growth [141]. The disorder appears to be lethal, with several individuals dying in the first few years of life.
PNPLA6
Mutations in the PNPLA6 gene, , encoding neuropathy target esterase (NTE), are known to be associated with a spectrum of rare neurodegenerative conditions, including spastic paraplegia type 39 (SPG39), Gordon–Holmes syndrome (GHS) and Boucher–Neuhäuser syndrome (BNHS) [142, 143]. This gene has recently been implicated in two distinct neurodegenerative disorders: Oliver–McFarlane and Laurence–Moon syndromes . The phenotypes are characterized by chorioretinopathy, spinocerebellar ataxia, spastic paraplegia, learning difficulties, and trichomegaly. These disorders include pituitary dysfunction with a small anterior pituitary on MRI, including variable GHD and HH. In humans, embryonic expression studies show PNPLA6 transcript expression in the developing eye, pituitary and brain. Significant reduction of NTE enzymatic activity was observed in fibroblast cells derived from Oliver–McFarlane syndrome patients. Additionally, full rescue of the pnpla6 morphant zebrafish was achieved using wild-type PNPLA6 mRNA, compared to only partial rescue with mutant PNPLA6 mRNAs [144]. These data signify that defective recessive PNPLA6 alleles can give rise to rare distinct phenotypes with variable neurodegenerative manifestations (Table 1.1).
KCNQ1
The paternally imprinted gene KCNQ1 encodes the alpha subunit of the voltage-gated ion channel Kv7.1, previously implicated in cardiac arrhythmia syndromes amongst other heart defects [145]. It is expressed in mouse and human somatotroph and gonadotroph cells in the postnatal pituitary, in hypothalamic GHRH neurons during murine development and in the human hypothalamus [146]. Mutations in KCNQ1 (p.R116L and p.P369L) have recently been described in patients with GHD, maternally inherited gingival fibromatosis and accompanying mild craniofacial dysmorphic features [146] (Table 1.1). Phenotypic variability is apparent in patients harbouring mutations, even between monozygotic twins where one had more severe growth failure during childhood than the other. This study demonstrates how ion channels are clinically relevant regulators of pituitary function in humans , which supports previous data implicating voltage-gated potassium channel currents in pituitary cells [147,148,149].
IFT172
The IFT172 gene encodes a subunit of the intraflagellar transport (IFT) subcomplex IFT-B, necessary for ciliary assembly and maintenance. Mutations in IFT172 have previously been associated with skeletal ciliopathies, with or without polydactyly, that in turn are often associated with retinal, cerebellar or hepatorenal malformations [150,151,152]. Interestingly, a patient with early growth retardation, APH and an EPP on their MRI harboured compound heterozygous mutations in IFT172, p.C1727R and a novel splice site mutation in intron 4 and c.337–2A >C, identified through WES. This patient manifested retinopathy associated with metaphyseal dysplasia and hypertension with renal failure, indicative of a ciliopathy [153]. This was the first report of an IFT172 mutation present in a patient who presented with GHD in early childhood, signifying the role of ciliary function in pituitary development and the bridge between early-onset growth failure and ciliopathies (Table 1.1).
Furthermore, Alström syndrome , a rare autosomal recessive disease characterized by multiorgan dysfunction and associated with GHD, is caused by a mutation in ALMS1, encoding a protein that localizes to the centrosomes and basal bodies of ciliated cells [154].
References
Davis SW, Castinetti F, Carvalho LR, Ellsworth BS, Potok MA, Lyons RH, et al. Molecular mechanisms of pituitary organogenesis: in search of novel regulatory genes. Mol Cell Endocrinol. 2010;323(1):4–19.
Cohen LE. Genetic disorders of the pituitary. Curr Opin Endocrinol Diabetes Obes. 2012;19(1):33–9.
Bancalari RE, Gregory LC, McCabe MJ, Dattani MT. Pituitary gland development: an update. Endocr Dev. 2012;23:1–15.
Kelberman D, Rizzoti K, Lovell-Badge R, Robinson IC, Dattani MT. Genetic regulation of pituitary gland development in human and mouse. Endocr Rev. 2009;30(7):790–829.
Alatzoglou KS, Dattani MT. Genetic forms of hypopituitarism and their manifestation in the neonatal period. Early Hum Dev. 2009;85(11):705–12.
McCabe MJ, Gaston-Massuet C, Tziaferi V, Gregory LC, Alatzoglou KS, Signore M, et al. Novel FGF8 mutations associated with recessive holoprosencephaly, craniofacial defects, and hypothalamo-pituitary dysfunction. J Clin Endocrinol Metab. 2011;96(10):E1709–18.
Iguchi G, Okimura Y, Takahashi T, Mizuno I, Fumoto M, Takahashi Y, et al. Cloning and characterization of the 5′-flanking region of the human growth hormone-releasing hormone receptor gene. J Biol Chem. 1999;274(17):12108–14.
Alatzoglou KS, Kular D, Dattani MT. Autosomal dominant growth hormone deficiency (Type II). Pediatr Endocrinol Rev. 2015;12(4):347–55.
Alatzoglou KS, Webb EA, Le Tissier P, Dattani MT. Isolated growth hormone deficiency (GHD) in childhood and adolescence: recent advances. Endocr Rev. 2014;35(3):376–432.
Cogan JD, Phillips JA 3rd. GH1 gene deletions and IGHD type 1A. Pediatr Endocrinol Rev. 2006;3(Suppl 3):480–8.
Wagner JK, Eble A, Hindmarsh PC, Mullis PE. Prevalence of human GH-1 gene alterations in patients with isolated growth hormone deficiency. Pediatr Res. 1998;43(1):105–10.
Baumann G, Maheshwari H. The dwarfs of Sindh: severe growth hormone (GH) deficiency caused by a mutation in the GH-releasing hormone receptor gene. Acta Paediatr Suppl. 1997;423:33–8.
Leiberman E, Pesler D, Parvari R, Elbedour K, Abdul-Latif H, Brown MR, et al. Short stature in carriers of recessive mutation causing familial isolated growth hormone deficiency. Am J Med Genet. 2000;90(3):188–92.
Phillips JA 3rd, Cogan JD. Genetic basis of endocrine disease. 6. Molecular basis of familial human growth hormone deficiency. J Clin Endocrinol Metab. 1994;78(1):11–6.
Shohreh R, Sherafat-Kazemzadeh R, Jee YH, Blitz A, Salvatori R. A novel frame shift mutation in the GHRH receptor gene in familial isolated GH deficiency: early occurrence of anterior pituitary hypoplasia. J Clin Endocrinol Metab. 2011;96(10):2982–6.
Baumann G. Mutations in the growth hormone releasing hormone receptor: a new form of dwarfism in humans. Growth Hormon IGF Res. 1999;9 Suppl B:24–9; discussion 9-30.
Carakushansky M, Whatmore AJ, Clayton PE, Shalet SM, Gleeson HK, Price DA, et al. A new missense mutation in the growth hormone-releasing hormone receptor gene in familial isolated GH deficiency. Eur J Endocrinol. 2003;148(1):25–30.
Salvatori R, Fan X, Mullis PE, Haile A, Levine MA. Decreased expression of the GHRH receptor gene due to a mutation in a Pit-1 binding site. Mol Endocrinol. 2002;16(3):450–8.
Gregory LC, Alatzoglou KS, McCabe MJ, Hindmarsh PC, Saldanha JW, Romano N, et al. Partial loss of function of the GHRH receptor leads to mild growth hormone deficiency. J Clin Endocrinol Metab. 2016;101(10):3608–15.
Lee MS, Wajnrajch MP, Kim SS, Plotnick LP, Wang J, Gertner JM, et al. Autosomal dominant growth hormone (GH) deficiency type II: the Del32-71-GH deletion mutant suppresses secretion of wild-type GH. Endocrinology. 2000;141(3):883–90.
McGuinness L, Magoulas C, Sesay AK, Mathers K, Carmignac D, Manneville JB, et al. Autosomal dominant growth hormone deficiency disrupts secretory vesicles in vitro and in vivo in transgenic mice. Endocrinology. 2003;144(2):720–31.
Ryther RC, McGuinness LM, Phillips JA 3rd, Moseley CT, Magoulas CB, Robinson IC, et al. Disruption of exon definition produces a dominant-negative growth hormone isoform that causes somatotroph death and IGHD II. Hum Genet. 2003;113(2):140–8.
Zhao E, Li J, Xie Y, Jin W, Zhang Z, Chen J, et al. Cloning and identification of a novel human RNPC3 gene that encodes a protein with two RRM domains and is expressed in the cell nucleus. Biochem Genet. 2003;41(9–10):315–23.
Argente J, Flores R, Gutierrez-Arumi A, Verma B, Martos-Moreno GA, Cusco I, et al. Defective minor spliceosome mRNA processing results in isolated familial growth hormone deficiency. EMBO Mol Med. 2014;6(3):299–306.
Yin X, Li Y, Xu G, An W, Zhang W. Ghrelin fluctuation, what determines its production? Acta Biochim Biophys Sin. 2009;41(3):188–97.
Markmiller S, Cloonan N, Lardelli RM, Doggett K, Keightley MC, Boglev Y, et al. Minor class splicing shapes the zebrafish transcriptome during development. Proc Natl Acad Sci U S A. 2014;111(8):3062–7.
Ashkenazi-Hoffnung L, Lebenthal Y, Wyatt AW, Ragge NK, Dateki S, Fukami M, et al. A novel loss-of-function mutation in OTX2 in a patient with anophthalmia and isolated growth hormone deficiency. Hum Genet. 2010;127(6):721–9.
Thomas PQ, Dattani MT, Brickman JM, McNay D, Warne G, Zacharin M, et al. Heterozygous HESX1 mutations associated with isolated congenital pituitary hypoplasia and septo-optic dysplasia. Hum Mol Genet. 2001;10(1):39–45.
Douchi T, Nakae M, Yamamoto S, Iwamoto I, Oki T, Nagata Y. A woman with isolated prolactin deficiency. Acta Obstet Gynecol Scand. 2001;80(4):368–70.
Kauppila A. Isolated prolactin deficiency. Curr Ther Endocrinol Metab. 1997;6:31–3.
Zargar AH, Masoodi SR, Laway BA, Shah NA, Salahudin M. Familial puerperal alactogenesis: possibility of a genetically transmitted isolated prolactin deficiency. Br J Obstet Gynaecol. 1997;104(5):629–31.
Iwama S, Welt CK, Romero CJ, Radovick S, Caturegli P. Isolated prolactin deficiency associated with serum autoantibodies against prolactin-secreting cells. J Clin Endocrinol Metab. 2013;98(10):3920–5.
Garcia M, Fernandez A, Moreno JC. Central hypothyroidism in children. Endocr Dev. 2014;26:79–107.
Sun Y, Bak B, Schoenmakers N, van Trotsenburg AS, Oostdijk W, Voshol P, et al. Loss-of-function mutations in IGSF1 cause an X-linked syndrome of central hypothyroidism and testicular enlargement. Nat Genet. 2012;44(12):1375–81.
Wassner AJ, Cohen LE, Hechter E, Dauber A. Isolated central hypothyroidism in young siblings as a manifestation of PROP1 deficiency: clinical impact of whole exome sequencing. Horm Res Paediatr. 2013;79(6):379–86.
Hayashizaki Y, Hiraoka Y, Endo Y, Miyai K, Matsubara K. Thyroid-stimulating hormone (TSH) deficiency caused by a single base substitution in the CAGYC region of the beta-subunit. EMBO J. 1989;8(8):2291–6.
Medeiros-Neto G, Herodotou DT, Rajan S, Kommareddi S, de Lacerda L, Sandrini R, et al. A circulating, biologically inactive thyrotropin caused by a mutation in the beta subunit gene. J Clin Invest. 1996;97(5):1250–6.
McDermott MT, Haugen BR, Black JN, Wood WM, Gordon DF, Ridgway EC. Congenital isolated central hypothyroidism caused by a “hot spot” mutation in the thyrotropin-beta gene. Thyroid. 2002;12(12):1141–6.
Karges B, LeHeup B, Schoenle E, Castro-Correia C, Fontoura M, Pfaffle R, et al. Compound heterozygous and homozygous mutations of the TSHbeta gene as a cause of congenital central hypothyroidism in Europe. Horm Res. 2004;62(3):149–55.
Nicholas AK, Jaleel S, Lyons G, Schoenmakers E, Dattani MT, Crowne E, et al. Molecular spectrum of TSHbeta subunit gene defects in central hypothyroidism in the UK and Ireland. Clin Endocrinol (Oxf). 2017;86(3):410–8.
Buyukgebiz A. Newborn screening for congenital hypothyroidism. J Clin Res Pediatr Endocrinol. 2013;5(Suppl 1):8–12.
Collu R, Tang J, Castagne J, Lagace G, Masson N, Huot C, et al. A novel mechanism for isolated central hypothyroidism: inactivating mutations in the thyrotropin-releasing hormone receptor gene. J Clin Endocrinol Metab. 1997;82(5):1561–5.
Bonomi M, Busnelli M, Beck-Peccoz P, Costanzo D, Antonica F, Dolci C, et al. A family with complete resistance to thyrotropin-releasing hormone. N Engl J Med. 2009;360(7):731–4.
Koulouri O, Nicholas AK, Schoenmakers E, Mokrosinski J, Lane F, Cole T, et al. A novel thyrotropin-releasing hormone receptor missense mutation (P81R) in central congenital hypothyroidism. J Clin Endocrinol Metab. 2016;101(3):847–51.
Tenenbaum-Rakover Y, Turgeon MO, London S, Hermanns P, Pohlenz J, Bernard DJ, et al. Familial central hypothyroidism caused by a novel IGSF1 gene mutation. Thyroid. 2016;26(12):1693–700.
Garcia M, Barrio R, Garcia-Lavandeira M, Garcia-Rendueles AR, Escudero A, Diaz-Rodriguez E, et al. The syndrome of central hypothyroidism and macroorchidism: IGSF1 controls TRHR and FSHB expression by differential modulation of pituitary TGFbeta and Activin pathways. Sci Rep. 2017;7:42937.
Hughes JN, Aubert M, Heatlie J, Gardner A, Gecz J, Morgan T, et al. Identification of an IGSF1-specific deletion in a five-generation pedigree with X-linked Central Hypothyroidism without macroorchidism. Clin Endocrinol. 2016;85(4):609–15.
Joustra SD, Schoenmakers N, Persani L, Campi I, Bonomi M, Radetti G, et al. The IGSF1 deficiency syndrome: characteristics of male and female patients. J Clin Endocrinol Metab. 2013;98(12):4942–52.
Turgeon MO, Silander TL, Doycheva D, Liao XH, Rigden M, Ongaro L, et al. TRH action is impaired in pituitaries of male IGSF1-deficient mice. Endocrinology. 2017;158(4):815–30.
Bassi MT, Ramesar RS, Caciotti B, Winship IM, De Grandi A, Riboni M, et al. X-linked late-onset sensorineural deafness caused by a deletion involving OA1 and a novel gene containing WD-40 repeats. Am J Hum Genet. 1999;64(6):1604–16.
Heinen CA, Losekoot M, Sun Y, Watson PJ, Fairall L, Joustra SD, et al. Mutations in TBL1X are associated with central hypothyroidism. J Clin Endocrinol Metab. 2016;101(12):4564–73.
Ahn SW, Kim TY, Lee S, Jeong JY, Shim H, Han YM, et al. Adrenal insufficiency presenting as hypercalcemia and acute kidney injury. Int Med Case Rep J. 2016;9:223–6.
Alsaleem M, Saadeh L, Misra A, Madani S. Neonatal isolated ACTH deficiency (IAD): a potentially life-threatening but treatable cause of neonatal cholestasis. BMJ Case Rep. 2016;2016. pii: bcr2016215032. https://doi.org/10.1136/bcr-2016-215032.
Bigos ST, Carnes TD. Isolated ACTH deficiency presenting as severe hypercalcemia. Am J Med Sci. 1982;284(1):24–30.
Doroftei NA, de Rudder C, de Visscher N, Hanon F. Isolated ACTH deficiency in a patient with empty sella as revealed by severe hyponatremia. Acta Clin Belg. 2016;71(6):451–4.
Metherell LA, Savage MO, Dattani M, Walker J, Clayton PE, Farooqi IS, et al. TPIT mutations are associated with early-onset, but not late-onset isolated ACTH deficiency. Eur J Endocrinol. 2004;151(4):463–5.
Lamolet B, Pulichino AM, Lamonerie T, Gauthier Y, Brue T, Enjalbert A, et al. A pituitary cell-restricted T box factor, Tpit, activates POMC transcription in cooperation with Pitx homeoproteins. Cell. 2001;104(6):849–59.
Couture C, Saveanu A, Barlier A, Carel JC, Fassnacht M, Fluck CE, et al. Phenotypic homogeneity and genotypic variability in a large series of congenital isolated ACTH-deficiency patients with TPIT gene mutations. J Clin Endocrinol Metab. 2012;97(3):E486–95.
Akcan N, Serakinci N, Turkgenc B, Bundak R, Bahceciler N, Temel SG. A novel TBX19 gene mutation in a case of congenital isolated adrenocorticotropic hormone deficiency presenting with recurrent respiratory tract infections. Front Endocrinol. 2017;8:64.
Seidah NG, Chretien M. Proprotein and prohormone convertases: a family of subtilases generating diverse bioactive polypeptides. Brain Res. 1999;848(1–2):45–62.
Slominski A, Wortsman J, Luger T, Paus R, Solomon S. Corticotropin releasing hormone and proopiomelanocortin involvement in the cutaneous response to stress. Physiol Rev. 2000;80(3):979–1020.
Rousseau K, Kauser S, Pritchard LE, Warhurst A, Oliver RL, Slominski A, et al. Proopiomelanocortin (POMC), the ACTH/melanocortin precursor, is secreted by human epidermal keratinocytes and melanocytes and stimulates melanogenesis. FASEB J. 2007;21(8):1844–56.
Valverde P, Healy E, Jackson I, Rees JL, Thody AJ. Variants of the melanocyte-stimulating hormone receptor gene are associated with red hair and fair skin in humans. Nat Genet. 1995;11(3):328–30.
Gorrigan RJ, Guasti L, King P, Clark AJ, Chan LF. Localisation of the melanocortin-2-receptor and its accessory proteins in the developing and adult adrenal gland. J Mol Endocrinol. 2011;46(3):227–32.
Lu D, Willard D, Patel IR, Kadwell S, Overton L, Kost T, et al. Agouti protein is an antagonist of the melanocyte-stimulating-hormone receptor. Nature. 1994;371(6500):799–802.
Krude H, Biebermann H, Luck W, Horn R, Brabant G, Gruters A. Severe early-onset obesity, adrenal insufficiency and red hair pigmentation caused by POMC mutations in humans. Nat Genet. 1998;19(2):155–7.
Jackson RS, Creemers JW, Ohagi S, Raffin-Sanson ML, Sanders L, Montague CT, et al. Obesity and impaired prohormone processing associated with mutations in the human prohormone convertase 1 gene. Nat Genet. 1997;16(3):303–6.
Jackson RS, Creemers JW, Farooqi IS, Raffin-Sanson ML, Varro A, Dockray GJ, et al. Small-intestinal dysfunction accompanies the complex endocrinopathy of human proprotein convertase 1 deficiency. J Clin Invest. 2003;112(10):1550–60.
Zhu X, Zhou A, Dey A, Norrbom C, Carroll R, Zhang C, et al. Disruption of PC1/3 expression in mice causes dwarfism and multiple neuroendocrine peptide processing defects. Proc Natl Acad Sci U S A. 2002;99(16):10293–8.
Philippe J, Stijnen P, Meyre D, De Graeve F, Thuillier D, Delplanque J, et al. A nonsense loss-of-function mutation in PCSK1 contributes to dominantly inherited human obesity. Int J Obes (2005). 2015;39(2):295–302.
Wang L, Sui L, Panigrahi SK, Meece K, Xin Y, Kim J, et al. PC1/3 deficiency impacts pro-opiomelanocortin processing in human embryonic stem cell-derived hypothalamic neurons. Stem Cell Rep. 2017;8(2):264–77.
Stijnen P, Ramos-Molina B, O’Rahilly S, Creemers JW. PCSK1 mutations and human endocrinopathies: from obesity to gastrointestinal disorders. Endocr Rev. 2016;37(4):347–71.
Martin MG, Lindberg I, Solorzano-Vargas RS, Wang J, Avitzur Y, Bandsma R, et al. Congenital proprotein convertase 1/3 deficiency causes malabsorptive diarrhea and other endocrinopathies in a pediatric cohort. Gastroenterology. 2013;145(1):138–48.
De Morsier G. Studies on malformation of cranio-encephalic sutures. III. Agenesis of the septum lucidum with malformation of the optic tract. Schweizer Archiv fur Neurologie und Psychiatrie Archives suisses de neurologie et de psychiatrie Archivio svizzero di neurologia e psichiatria. 1956;77(1–2):267–92.
Brodsky MC, Glasier CM. Optic nerve hypoplasia. Clinical significance of associated central nervous system abnormalities on magnetic resonance imaging. Arch Ophthalmol (Chicago, Ill: 1960). 1993;111(1):66–74.
McNay DE, Turton JP, Kelberman D, Woods KS, Brauner R, Papadimitriou A, et al. HESX1 mutations are an uncommon cause of septooptic dysplasia and hypopituitarism. J Clin Endocrinol Metab. 2007;92(2):691–7.
Webb EA, Dattani MT. Septo-optic dysplasia. Eur J Hum Genet. 2010;18(4):393–7.
Lippe B, Kaplan SA, LaFranchi S. Septo-optic dysplasia and maternal age. Lancet (London, England). 1979;2(8133):92–3.
Kelberman D, Dattani MT. Genetics of septo-optic dysplasia. Pituitary. 2007;10(4):393–407.
Kelberman D, Dattani MT. Septo-optic dysplasia - novel insights into the aetiology. Horm Res. 2008;69(5):257–65.
Mehta A, Hindmarsh PC, Mehta H, Turton JP, Russell-Eggitt I, Taylor D, et al. Congenital hypopituitarism: clinical, molecular and neuroradiological correlates. Clin Endocrinol (Oxf). 2009;71(3):376–82.
McCabe MJ, Alatzoglou KS, Dattani MT. Septo-optic dysplasia and other midline defects: the role of transcription factors: HESX1 and beyond. Best Pract Res Clin Endocrinol Metab. 2011;25(1):115–24.
Dattani MT, Martinez-Barbera JP, Thomas PQ, Brickman JM, Gupta R, Martensson IL, et al. Mutations in the homeobox gene HESX1/Hesx1 associated with septo-optic dysplasia in human and mouse. Nat Genet. 1998;19(2):125–33.
Sajedi E, Gaston-Massuet C, Signore M, Andoniadou CL, Kelberman D, Castro S, et al. Analysis of mouse models carrying the I26T and R160C substitutions in the transcriptional repressor HESX1 as models for septo-optic dysplasia and hypopituitarism. Dis Model Mech. 2008;1(4–5):241–54.
Woods KS, Cundall M, Turton J, Rizotti K, Mehta A, Palmer R, et al. Over- and underdosage of SOX3 is associated with infundibular hypoplasia and hypopituitarism. Am J Hum Genet. 2005;76(5):833–49.
McCabe MJ, Hu Y, Gregory LC, Gaston-Massuet C, Alatzoglou KS, Saldanha JW, et al. Novel application of luciferase assay for the in vitro functional assessment of KAL1 variants in three females with septo-optic dysplasia (SOD). Mol Cell Endocrinol. 2015;417:63–72.
Raivio T, Avbelj M, McCabe MJ, Romero CJ, Dwyer AA, Tommiska J, et al. Genetic overlap in Kallmann syndrome, combined pituitary hormone deficiency, and septo-optic dysplasia. J Clin Endocrinol Metab. 2012;97(4):E694–9.
Gaston-Massuet C, McCabe MJ, Scagliotti V, Young RM, Carreno G, Gregory LC, et al. Transcription factor 7-like 1 is involved in hypothalamo-pituitary axis development in mice and humans. Proc Natl Acad Sci U S A. 2016;113(5):E548–57.
Polizzi A, Pavone P, Iannetti P, Manfre L, Ruggieri M. Septo-optic dysplasia complex: a heterogeneous malformation syndrome. Pediatr Neurol. 2006;34(1):66–71.
Dasen JS, Martinez Barbera JP, Herman TS, Connell SO, Olson L, Ju B, et al. Temporal regulation of a paired-like homeodomain repressor/TLE corepressor complex and a related activator is required for pituitary organogenesis. Genes Dev. 2001;15(23):3193–207.
Sajedi E, Gaston-Massuet C, Andoniadou CL, Signore M, Hurd PJ, Dattani M, et al. DNMT1 interacts with the developmental transcriptional repressor HESX1. Biochim Biophys Acta. 2008;1783(1):131–43.
Thomas P, Beddington R. Anterior primitive endoderm may be responsible for patterning the anterior neural plate in the mouse embryo. Curr Biol. 1996;6(11):1487–96.
Hermesz E, Mackem S, Mahon KA. Rpx: a novel anterior-restricted homeobox gene progressively activated in the prechordal plate, anterior neural plate and Rathke’s pouch of the mouse embryo. Development. 1996;122(1):41–52.
Sobrier ML, Netchine I, Heinrichs C, Thibaud N, Vie-Luton MP, Van Vliet G, et al. Alu-element insertion in the homeodomain of HESX1 and aplasia of the anterior pituitary. Hum Mutat. 2005;25(5):503.
Kelberman D, Dattani MT. Hypothalamic and pituitary development: novel insights into the aetiology. Eur J Endocrinol. 2007;157(Suppl 1):S3–14.
Newbern K, Natrajan N, Kim HG, Chorich LP, Halvorson LM, Cameron RS, et al. Identification of HESX1 mutations in Kallmann syndrome. Fertil Steril. 2013;99(7):1831–7.
Stevanovic M, Lovell-Badge R, Collignon J, Goodfellow PN. SOX3 is an X-linked gene related to SRY. Hum Mol Genet. 1993;2(12):2013–8.
Hutton SR. Sox gene expression. In: Lemke G, editor. Developmental biology, vol. 2009: Elseveir. p. 165.
Bylund M, Andersson E, Novitch BG, Muhr J. Vertebrate neurogenesis is counteracted by Sox1-3 activity. Nat Neurosci. 2003;6(11):1162–8.
Solomon NM, Ross SA, Morgan T, Belsky JL, Hol FA, Karnes PS, et al. Array comparative genomic hybridisation analysis of boys with X linked hypopituitarism identifies a 3.9 Mb duplicated critical region at Xq27 containing SOX3. J Med Genet. 2004;41(9):669–78.
Rizzoti K, Brunelli S, Carmignac D, Thomas PQ, Robinson IC, Lovell-Badge R. SOX3 is required during the formation of the hypothalamo-pituitary axis. Nat Genet. 2004;36(3):247–55.
Potok MA, Cha KB, Hunt A, Brinkmeier ML, Leitges M, Kispert A, et al. WNT signaling affects gene expression in the ventral diencephalon and pituitary gland growth. Dev Dyn. 2008;237(4):1006–20.
Wong J, Farlie P, Holbert S, Lockhart P, Thomas PQ. Polyalanine expansion mutations in the X-linked hypopituitarism gene SOX3 result in aggresome formation and impaired transactivation. Front Biosci: J Virtual Libr. 2007;12:2085–95.
Hamel BC, Smits AP, Otten BJ, van den Helm B, Ropers HH, Mariman EC. Familial X-linked mental retardation and isolated growth hormone deficiency: clinical and molecular findings. Am J Med Genet. 1996;64(1):35–41.
Laumonnier F, Ronce N, Hamel BC, Thomas P, Lespinasse J, Raynaud M, et al. Transcription factor SOX3 is involved in X-linked mental retardation with growth hormone deficiency. Am J Hum Genet. 2002;71(6):1450–5.
Alatzoglou KS, Azriyanti A, Rogers N, Ryan F, Curry N, Noakes C, et al. SOX3 deletion in mouse and human is associated with persistence of the craniopharyngeal canal. J Clin Endocrinol Metab. 2014;99(12):E2702–8.
Alatzoglou KS, Kelberman D, Cowell CT, Palmer R, Arnhold IJ, Melo ME, et al. Increased transactivation associated with SOX3 polyalanine tract deletion in a patient with hypopituitarism. J Clin Endocrinol Metab. 2011;96(4):E685–90.
Hutton SR, Pevny LH. SOX2 expression levels distinguish between neural progenitor populations of the developing dorsal telencephalon. Dev Biol. 2011;352(1):40–7.
Avilion AA, Nicolis SK, Pevny LH, Perez L, Vivian N, Lovell-Badge R. Multipotent cell lineages in early mouse development depend on SOX2 function. Genes Dev. 2003;17(1):126–40.
Kelberman D, Rizzoti K, Avilion A, Bitner-Glindzicz M, Cianfarani S, Collins J, et al. Mutations within Sox2/SOX2 are associated with abnormalities in the hypothalamo-pituitary-gonadal axis in mice and humans. J Clin Invest. 2006;116(9):2442–55.
Taranova OV, Magness ST, Fagan BM, Wu Y, Surzenko N, Hutton SR, et al. SOX2 is a dose-dependent regulator of retinal neural progenitor competence. Genes Dev. 2006;20(9):1187–202.
Williamson KA, Hever AM, Rainger J, Rogers RC, Magee A, Fiedler Z, et al. Mutations in SOX2 cause anophthalmia-esophageal-genital (AEG) syndrome. Hum Mol Genet. 2006;15(9):1413–22.
Jayakody SA, Andoniadou CL, Gaston-Massuet C, Signore M, Cariboni A, Bouloux PM, et al. SOX2 regulates the hypothalamic-pituitary axis at multiple levels. J Clin Invest. 2012;122(10):3635–46.
Alatzoglou KS, Andoniadou CL, Kelberman D, Buchanan CR, Crolla J, Arriazu MC, et al. SOX2 haploinsufficiency is associated with slow progressing hypothalamo-pituitary tumours. Hum Mutat. 2011;32(12):1376–80.
Goldsmith S, Lovell-Badge R, Rizzoti K. SOX2 is sequentially required for progenitor proliferation and lineage specification in the developing pituitary. Development. 2016;143(13):2376–88.
Li H, Collado M, Villasante A, Matheu A, Lynch CJ, Canamero M, et al. p27(Kip1) directly represses Sox2 during embryonic stem cell differentiation. Cell Stem Cell. 2012;11(6):845–52.
Fauquier T, Rizzoti K, Dattani M, Lovell-Badge R, Robinson IC. SOX2-expressing progenitor cells generate all of the major cell types in the adult mouse pituitary gland. Proc Natl Acad Sci U S A. 2008;105(8):2907–12.
Andoniadou CL, Matsushima D, Mousavy Gharavy SN, Signore M, Mackintosh AI, Schaeffer M, et al. Sox2(+) stem/progenitor cells in the adult mouse pituitary support organ homeostasis and have tumor-inducing potential. Cell Stem Cell. 2013;13(4):433–45.
Frantz GD, Weimann JM, Levin ME, McConnell SK. Otx1 and Otx2 define layers and regions in developing cerebral cortex and cerebellum. J Neurosci. 1994;14(10):5725–40.
Ang SL, Jin O, Rhinn M, Daigle N, Stevenson L, Rossant J. A targeted mouse Otx2 mutation leads to severe defects in gastrulation and formation of axial mesoderm and to deletion of rostral brain. Development. 1996;122(1):243–52.
Housset M, Samuel A, Ettaiche M, Bemelmans A, Beby F, Billon N, et al. Loss of Otx2 in the adult retina disrupts retinal pigment epithelium function, causing photoreceptor degeneration. J Neurosci. 2013;33(24):9890–904.
Mortensen AH, MacDonald JW, Ghosh D, Camper SA. Candidate genes for panhypopituitarism identified by gene expression profiling. Physiol Genomics. 2011;43(19):1105–16.
Diaczok D, DiVall S, Matsuo I, Wondisford FE, Wolfe AM, Radovick S. Deletion of Otx2 in GnRH neurons results in a mouse model of hypogonadotropic hypogonadism. Mol Endocrinol (Baltimore, Md). 2011;25(5):833–46.
Gorbenko Del Blanco D, Romero CJ, Diaczok D, de Graaff LC, Radovick S, Hokken-Koelega AC. A novel OTX2 mutation in a patient with combined pituitary hormone deficiency, pituitary malformation, and an underdeveloped left optic nerve. Eur J Endocrinol. 2012;167(3):441–52.
Tajima T, Ohtake A, Hoshino M, Amemiya S, Sasaki N, Ishizu K, et al. OTX2 loss of function mutation causes anophthalmia and combined pituitary hormone deficiency with a small anterior and ectopic posterior pituitary. J Clin Endocrinol Metab. 2009;94(1):314–9.
Chassaing N, Sorrentino S, Davis EE, Martin-Coignard D, Iacovelli A, Paznekas W, et al. OTX2 mutations contribute to the otocephaly-dysgnathia complex. J Med Genet. 2012;49(6):373–9.
Roessler E, Du YZ, Mullor JL, Casas E, Allen WP, Gillessen-Kaesbach G, et al. Loss-of-function mutations in the human GLI2 gene are associated with pituitary anomalies and holoprosencephaly-like features. Proc Natl Acad Sci U S A. 2003;100(23):13424–9.
Roessler E, Ermilov AN, Grange DK, Wang A, Grachtchouk M, Dlugosz AA, et al. A previously unidentified amino-terminal domain regulates transcriptional activity of wild-type and disease-associated human GLI2. Hum Mol Genet. 2005;14(15):2181–8.
Gregory LC, Gaston-Massuet C, Andoniadou CL, Carreno G, Webb EA, Kelberman D, et al. The role of the sonic hedgehog signalling pathway in patients with midline defects and congenital hypopituitarism. Clin Endocrinol (Oxf). 2015;82(5):728–38.
Franca MM, Jorge AA, Carvalho LR, Costalonga EF, Vasques GA, Leite CC, et al. Novel heterozygous nonsense GLI2 mutations in patients with hypopituitarism and ectopic posterior pituitary lobe without holoprosencephaly. J Clin Endocrinol Metab. 2010;95(11):E384–91.
Franca MM, Jorge AA, Carvalho LR, Costalonga EF, Otto AP, Correa FA, et al. Relatively high frequency of non-synonymous GLI2 variants in patients with congenital hypopituitarism without holoprosencephaly. Clin Endocrinol (Oxf). 2013;78(4):551–7.
Bear KA, Solomon BD, Antonini S, Arnhold IJ, Franca MM, Gerkes EH, et al. Pathogenic mutations in GLI2 cause a specific phenotype that is distinct from holoprosencephaly. J Med Genet. 2014;51(6):413–8.
Flemming GM, Klammt J, Ambler G, Bao Y, Blum WF, Cowell C, et al. Functional characterization of a heterozygous GLI2 missense mutation in patients with multiple pituitary hormone deficiency. J Clin Endocrinol Metab. 2013;98(3):E567–75.
Bashamboo A, Bignon-Topalovic J, Rouba H, McElreavey K, Brauner R. A nonsense mutation in the hedgehog receptor CDON associated with pituitary stalk interruption syndrome. J Clin Endocrinol Metab. 2016;101(1):12–5.
Karaca E, Buyukkaya R, Pehlivan D, Charng WL, Yaykasli KO, Bayram Y, et al. Whole-exome sequencing identifies homozygous GPR161 mutation in a family with pituitary stalk interruption syndrome. J Clin Endocrinol Metab. 2015;100(1):E140–7.
Blockus H, Chedotal A. The multifaceted roles of Slits and Robos in cortical circuits: from proliferation to axon guidance and neurological diseases. Curr Opin Neurobiol. 2014;27:82–8.
Bashamboo A, Bignon-Topalovic J, Moussi N, McElreavey K, Brauner R. Mutations in the human ROBO1 gene in pituitary stalk interruption syndrome. J Clin Endocrinol Metab. 2017;102(7):2401–6.
Diaczok D, Romero C, Zunich J, Marshall I, Radovick S. A novel dominant negative mutation of OTX2 associated with combined pituitary hormone deficiency. J Clin Endocrinol Metab. 2008;93(11):4351–9.
Reynaud R, Jayakody SA, Monnier C, Saveanu A, Bouligand J, Guedj AM, et al. PROKR2 variants in multiple hypopituitarism with pituitary stalk interruption. J Clin Endocrinol Metab. 2012;97(6):E1068–73.
Keith B, Adelman DM, Simon MC. Targeted mutation of the murine arylhydrocarbon receptor nuclear translocator 2 (Arnt2) gene reveals partial redundancy with Arnt. Proc Natl Acad Sci U S A. 2001;98(12):6692–7.
Webb EA, AlMutair A, Kelberman D, Bacchelli C, Chanudet E, Lescai F, et al. ARNT2 mutation causes hypopituitarism, post-natal microcephaly, visual and renal anomalies. Brain: J Neurol. 2013;136(Pt 10):3096–105.
Rainier S, Bui M, Mark E, Thomas D, Tokarz D, Ming L, et al. Neuropathy target esterase gene mutations cause motor neuron disease. Am J Hum Genet. 2008;82(3):780–5.
Topaloglu AK, Lomniczi A, Kretzschmar D, Dissen GA, Kotan LD, McArdle CA, et al. Loss-of-function mutations in PNPLA6 encoding neuropathy target esterase underlie pubertal failure and neurological deficits in Gordon Holmes syndrome. J Clin Endocrinol Metab. 2014;99(10):E2067–75.
Hufnagel RB, Arno G, Hein ND, Hersheson J, Prasad M, Anderson Y, et al. Neuropathy target esterase impairments cause Oliver-McFarlane and Laurence-Moon syndromes. J Med Genet. 2015;52(2):85–94.
Wang Q, Curran ME, Splawski I, Burn TC, Millholland JM, VanRaay TJ, et al. Positional cloning of a novel potassium channel gene: KVLQT1 mutations cause cardiac arrhythmias. Nat Genet. 1996;12(1):17–23.
Tommiska J, Kansakoski J, Skibsbye L, Vaaralahti K, Liu X, Lodge EJ, et al. Two missense mutations in KCNQ1 cause pituitary hormone deficiency and maternally inherited gingival fibromatosis. Nat Commun. 2017;8(1):1289.
Stojilkovic SS, Tabak J, Bertram R. Ion channels and signaling in the pituitary gland. Endocr Rev. 2010;31(6):845–915.
Stojilkovic SS, Bjelobaba I, Zemkova H. Ion channels of pituitary gonadotrophs and their roles in signaling and secretion. Front Endocrinol. 2017;8:126.
Xu R, Roh SG, Loneragan K, Pullar M, Chen C. Human GHRH reduces voltage-gated K+ currents via a non-cAMP-dependent but PKC-mediated pathway in human GH adenoma cells. J Physiol. 1999;520(Pt 3):697–707.
Beales PL, Bland E, Tobin JL, Bacchelli C, Tuysuz B, Hill J, et al. IFT80, which encodes a conserved intraflagellar transport protein, is mutated in Jeune asphyxiating thoracic dystrophy. Nat Genet. 2007;39(6):727–9.
Bredrup C, Saunier S, Oud MM, Fiskerstrand T, Hoischen A, Brackman D, et al. Ciliopathies with skeletal anomalies and renal insufficiency due to mutations in the IFT-A gene WDR19. Am J Hum Genet. 2011;89(5):634–43.
Waters AM, Beales PL. Ciliopathies: an expanding disease spectrum. Pediatr Nephrol (Berlin, Germany). 2011;26(7):1039–56.
Lucas-Herald AK, Kinning E, Iida A, Wang Z, Miyake N, Ikegawa S, et al. A case of functional growth hormone deficiency and early growth retardation in a child with IFT172 mutations. J Clin Endocrinol Metab. 2015;100(4):1221–4.
Romano S, Maffei P, Bettini V, Milan G, Favaretto F, Gardiman M, et al. Alstrom syndrome is associated with short stature and reduced GH reserve. Clin Endocrinol (Oxf). 2013;79(4):529–36.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Gregory, L.C., Dattani, M.T. (2019). Embryologic and Genetic Disorders of the Pituitary Gland. In: Kohn, B. (eds) Pituitary Disorders of Childhood. Contemporary Endocrinology. Humana Press, Cham. https://doi.org/10.1007/978-3-030-11339-1_1
Download citation
DOI: https://doi.org/10.1007/978-3-030-11339-1_1
Published:
Publisher Name: Humana Press, Cham
Print ISBN: 978-3-030-11338-4
Online ISBN: 978-3-030-11339-1
eBook Packages: MedicineMedicine (R0)