
Abstract
Despite its small size, the fetal pituitary gland produces a variety of important hormones. Normal development of the human fetal pituitary gland is essential for fetal homeostasis, as well as for the appropriate differentiation and maturation of several organ systems required for extrauterine survival. This chapter reviews the histological features of the adenohypophysis (the anterior lobe of the pituitary gland) and the neurohypophysis (the posterior lobe of the pituitary gland). In addition, some features unique to the fetal and neonatal pituitary gland, such as laminated calcifications within the anterior lobe, are discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Despite its small size, the fetal pituitary gland produces a variety of important hormones. Normal development of the human fetal pituitary gland is essential for fetal homeostasis, as well as for the appropriate differentiation and maturation of several organ systems required for extrauterine survival [1]. This chapter reviews the histological features of the adenohypophysis (the anterior lobe of the pituitary gland) and the neurohypophysis (the posterior lobe of the pituitary gland). In addition, some features unique to the fetal and neonatal pituitary gland, such as laminated calcifications within the anterior lobe, are discussed.
Embryology
The pituitary gland is formed from two different ectodermally derived structures: Rathke’s pouch and a portion of the diencephalon known as the infundibulum. These distinctive embryologic origins correlate with the two distinct histological compartments of the pituitary gland, the adenohypophysis (anterior lobe), derived from Rathke’s pouch, and the neurohypophysis (posterior lobe), derived from the infundibulum [2,3,4].
Rathke’s pouch begins in the third week of gestation as an outgrowth of ectoderm from the stomodeum, the primitive mouth of the embryo. The epithelial outgrowth develops a lumen and forms an epithelium-lined diverticulum. This pouch extends dorsally toward the infundibulum, which is the small ventral extension of the floor of the diencephalon; it will become the neurohypophysis . At approximately 6 weeks gestation, Rathke’s pouch loses its connection with the surface ectoderm of the mouth and becomes an epithelium-lined cyst. The posterior wall of the cyst remains thin and is in close contact with the infundibulum; it will become the pars intermedia. The epithelium of the anterior wall of the cyst proliferates to form the rounded mass of the anterior lobe of the pituitary gland, the pars distalis (Fig. 23.1). A small group of cells from the posterior portion of the anterior lobe grow up the stalk of the infundibulum and are known as the pars tuberalis . The lumen of the original Rathke’s pouch becomes flattened in the anteroposterior direction and becomes a slit-like space between the pars distalis anteriorly and the pars intermedia posteriorly. Its remnants become the microscopic glandular structures of the pars intermedia [2,3,4].

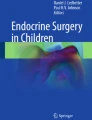
Low-power view of the entire fetal pituitary gland at 17 weeks gestation. The gland, removed with portions of the cartilaginous sella turcica (upper right), is shown here. The slit-like opening of Rathke’s pouch (RP) is visible. The most anterior portion of the anterior lobe or pars distalis (PD) is the rounded mass anterior to Rathke’s pouch. The thin rim of similar-appearing cells of the anterior pituitary on the opposite side of Rathke’s pouch is known as the pars intermedia (PI). The posterior lobe (PL) is adjacent to the PI and has a generally paler staining appearance than the anterior lobe (hematoxylin and eosin (H&E), 2×)
The anterior lobe of the pituitary gland is responsible for elaboration of the pituitary hormones: growth hormone (GH) , adrenal corticotropin hormone (ACTH) , prolactin (PRL) , thyroid-stimulating hormone (TSH) , follicle-stimulating hormone (FSH) , and luteinizing hormone (LH) . Differentiation of the ectodermal cells from Rathke’s pouch into the various hormone-producing cells depends on gradients of growth factors, such as fibroblast growth factor 8, which emanates from the ventral diencephalon, and bone morphogenetic protein 2, which emanates from the ventral pituitary organizing center. These overlapping gradients result in the expression of specific transcription factors that drive differentiation and the production of specific hormones [5,6,7].
The posterior lobe of the pituitary gland forms by the proliferation of neuroglial cells at the distal end of the infundibulum. The infundibulum remains the stalk of the pituitary gland, and nerve fibers from the hypothalamus also grow into the posterior lobe via the infundibular stalk.
Histology
General Overview
Sampling the fetal pituitary gland for histological examination can be difficult because the tissues of the gland are extremely soft and are easily compressed if they are grasped by forceps. After removing the brain, the pituitary gland can be removed intact by excising it along with the bony tissues of the sella turcica . Using this technique, the surrounding cartilaginous and bony tissues of the sella turcica protect the pituitary gland and serve as a “handle” to grasp the gland. The entire gland with the rim of the cartilaginous and bony tissue can be submitted in toto for histologic examination after brief decalcification.
Because of their separate embryologic origins, the anterior and posterior lobes of the pituitary gland have quite distinct histological appearances in the fetus. The anterior lobe of the pituitary gland appears as an ovoid, amphophilic mass of polygonal epithelial cells that are separated by a slit-like cavity from the thin layer of similar-appearing cells, forming the pars intermedia in the posterior aspect of the anterior lobe. Although well demarcated from the anterior lobe, the posterior lobe is in direct contact with the anterior lobe and stands in contrast, with its pale staining and fibrous appearance (Figs. 23.1, 23.2, 23.3, and 23.4). In routine sections of the fetal pituitary gland, the posterior lobe may not be readily identified, because it makes up a smaller proportion of the gland and the gland often has a random orientation. Deeper sections may be needed to assess the posterior pituitary gland.

Higher-power views of the anterior lobe of the pituitary gland at 17 weeks gestation. (a) The anterior lobe is composed of the pars distalis and pars intermedia, separated by residual lumen of Rathke’s pouch. (b) This close-up view is of the cells lining the lumen of Rathke’s pouch. Note the cuboidal to columnar, palisading epithelial cells. ((a) H&E, 4×; (b) H&E, 20×)

Low-power view of the pituitary gland at 26 weeks gestation. Note that the gland is larger, but the overall structure of the anterior and posterior lobes is identical (H&E, 2×)

Closer view of the junction between anterior and posterior pituitary lobes at 26 weeks gestation. Note the residual lumen of Rathke’s pouch and the lining epithelial cells. Glandular structures are formed within the pars intermedia. The posterior lobe (upper left) has a pale, fibrillary appearance (H&E, 4×)
Anterior Pituitary
The anterior lobe of the pituitary gland is composed of epithelial cells arranged in cords and nests with an intervening delicate capillary network. The epithelial cells have round, slightly eccentrically placed nuclei and fairly abundant cytoplasm, which is characterized by an affinity for either acidophilic dye (acidophils), basophilic dye (basophils) , or neither (chromophobes) on H&E staining . The acidophil cells appear to be the most numerous in the fetal pituitary gland and have brightly eosinophilic cytoplasmic granules. As a general rule, acidophil cells are considered to secrete GH and PRL and are located primarily in the rounded lateral projections of the pars distalis . Basophil cells are also commonly present and have dark blue-stained cytoplasmic granules. Basophils that secrete ACTH and TSH are located primarily in the central region of the pars distalis , referred to as the mucoid wedge because the basophil cells are also positive using the periodic acid–Schiff method [8]. Basophil cells that secrete the gonadotropins FSH and LH are scattered throughout the pars distalis . Both acidophils and basophils are generally arranged in clusters throughout the gland (Fig. 23.5). Although chromophobe cells can represent up to 50% of cells in the adult pituitary gland [8], they are not very prominent in the fetal pituitary. They are seen as only small clusters of cells with poorly stained, inconspicuous cytoplasm.

(a, b) Views of the anterior lobe from the pars distalis region at 26 weeks gestation. Cells of the anterior lobe are arranged in small clusters, cords, and nests with intervening capillary network. Acidophil cells with eosinophilic cytoplasm are easy to distinguish from the basophil cells, with their dark, granular cytoplasm. Chromophobe cells are inconspicuous (H&E: a 20×; b 40×)
Immunohistochemical studies in rats indicate that ACTH is the first pituitary hormone, detectable on embryonic day 15, and that the other hormones become detectable in a predictable pattern over the next few days [9]. Immunohistochemical and ultrastructural studies of human fetal pituitary glands [10,11,12] have shown that ACTH-producing cells are seen as early as 6–8 weeks gestation. Features characteristic of somatotrophs, which secrete GH, are seen at 8–9 weeks, and cells producing most other hormones are identifiable by 15–16 weeks gestation. Lactotrophs , PRL-producing cells, are somewhat variable in number in the first and second trimesters but are relatively numerous near term. In general practice, immunohistochemical stains for the pituitary hormones can be performed on the human fetal pituitary gland and will reveal the presence of all the anterior pituitary hormones near term. The staining pattern for each hormone is different, varying in intensity and the number of cells stained, but is similar to the pattern for adult control pituitary glands. The hormones with the most intense and widespread staining in the anterior lobe are ACTH (Fig. 23.6) and GH (Fig. 23.7).

Anterior pituitary gland at 35 weeks gestation. Immunohistochemical stain for ACTH shows numerous anterior pituitary cells with positive staining (ACTH immunohistochemistry, 20×)

Anterior pituitary gland at 35 weeks gestation. Immunohistochemical stain for GH shows numerous anterior pituitary cells with positive staining (GH immunohistochemistry, 20×)
A unique histological feature of the anterior lobe of the fetal and newborn pituitary is the presence of ovoid, calcified concretions (Fig. 23.8). These laminated calcifications have been noted in a majority of fetal pituitaries from mid-gestation to term, but they generally disappear within the first 6 months of life [13, 14]. Although the etiology of these calcifications is uncertain, hypotheses include a relationship to hormonal activity of the fetal pituitary gland or developmental processes associated with cell death [13, 14].

(a, b) Anterior lobe of the pituitary gland at 35 weeks gestation. The overall architecture and cellular components are similar to 26 weeks gestation (as in Fig. 23.5). Acidophil and basophil cells are easily distinguished by their cytoplasmic features. Chromophobe cells are still inconspicuous. Note the ovoid, darkly basophilic concretions present in the anterior lobe. These calcified concretions, which appear partially laminated, are commonly seen in fetal and newborn pituitary glands, until approximately 6 months of age (H&E: a 20×; b 40×)
By adulthood, the lumen of Rathke’s pouch between the pars distalis and pars intermedia is no longer visible, but in the fetal and neonatal pituitary gland, the space may be present and lined by cuboidal to columnar epithelial cells (see Fig. 23.2). Persistence of a so-called Rathke cleft cyst (Fig. 23.9) is identified as an incidental finding in up to one third of autopsy cases [15, 16]. If large enough, the Rathke cleft cyst in adults and children can become symptomatic and require surgical intervention. Embryonic epithelial remnants of the obliterated stalk connecting Rathke’s pouch to the embryonic oral cavity may also persist in the submucosa of the nasopharynx as the “pharyngeal pituitary ” or in the sphenoid bone along the embryonic path of the stalk; these embryonic rests may be functional, may be the origin of ectopic pituitary adenomas, and have been described with central nervous system malformations such as anencephaly, holoprosencephaly, and neural tube defects [17,18,19,20].

Rathke cleft cyst in a 1-year-old infant. Note the large cystic space involving the anterior pituitary gland. The cyst is lined by cuboidal to columnar epithelial cells, which can have cilia (H&E, 1×)
Posterior Pituitary
The main cell type seen in the posterior pituitary is the pituicyte, which is best classified as a subtype of the glial cell. Pituicytes have ovoid to elongate nuclei, and most have fibrillary cytoplasmic processes (Fig. 23.10; see also Figs. 23.1, 23.3, and 23.4). In the adult pituitary gland, the posterior pituitary shows immunoreactivity for glial fibrillary acidic protein, vimentin, and S100 protein, but in fetal life, only very few glial fibrillary acidic protein-positive fibers are seen (Fig. 23.11). The morphologic features of pituicytes can vary, with at least five different types described in the adult pituitary [8]. The second major constituent of the posterior lobe is the nonmyelinated axons of neurosecretory neuronal cell bodies originating in the supraoptic and paraventricular nuclei of the hypothalamus. These axons store the two secretory products of those nuclei, vasopressin or antidiuretic hormone and oxytocin. These axons are easily identifiable in silver-stained sections of adult glands, but they are not as easily identifiable, even with silver stains, in the fetal pituitary. The pituicytes surround the neurosecretory axons, and a major function of the posterior lobe is to release the stored hormones into the circulation. The posterior pituitary also has a rich vascular network.

Posterior lobe of the pituitary gland at 35 weeks gestation. The posterior pituitary occupies most of the field, with a small amount of anterior pituitary on the left for comparison. The posterior pituitary is less cellular, and its pituicytes have ovoid to elongated nuclei and fibrillary cytoplasm (H&E, 20×)

Posterior lobe of the pituitary gland at 35 weeks gestation. Stain for glial fibrillary acidic protein (GFAP) shows only a few positive-staining fibers (GFAP immunohistochemistry, 40×)
Salivary gland rests have been described in a small percentage of normal pituitary glands in children and adults; their presence may explain the occurrence of salivary gland neoplasms within the sella turcica [21]. The rests are typically found either on the surface of the neurohypophysis or within it. They are characterized by a cluster or clusters of small, rounded glandular structures lined by a simple cuboidal to columnar epithelium (Fig. 23.12). The nuclei of the epithelium are usually basally located, and the cytoplasm is granular and strongly PAS-positive [8]. Two possible mechanisms for the formation of these rests are the transfer of salivary glands from the primitive mouth during the formation of Rathke’s pouch or the induction of pituitary epithelium by heterotopic submandibular mesenchyme [21].

Salivary gland rests in the posterior lobe/neurohypophysis of the pituitary gland in a 1-year-old child. This image shows a small cluster of glandular structures lined by a simple columnar epithelium with basally placed nuclei and pale, eosinophilic granular cytoplasm. Note the fibrillary background of the neurohypophysis (H&E, 20×)
References
Ng PC. The fetal and neonatal hypothalamic-pituitary-adrenal axis. Arch Dis Child Fetal Neonatal Ed. 2000;82:F250–4.
Valdes-Dapena MA. Histology of the fetus and newborn. Philadelphia: Saunders; 1979.
Sadler TW, Langman J. Langman’s medical embryology. 11th ed. Philadelphia: Wolters Kluwer Lippincott Williams & Wilkins; 2010.
Schoenwolf GC, Larsen WJ. Larsen’s human embryology. 4th ed. Philadelphia: Elsevier/Churchill Livingstone; 2009.
Dasen JS, O’Connell SM, Flynn SE, Treier M, Gleiberman AS, Szeto DP, et al. Reciprocal interactions of Pit1 and GATA2 mediate signaling gradient-induced determination of pituitary cell types. Cell. 1999;97:587–98.
Nogami H, Hisano S. Functional maturation of growth hormone cells in the anterior pituitary gland of the fetus. Growth Hormon IGF Res. 2008;18:379–88.
Treier M, Gleiberman AS, O'Connell SM, Szeto DP, McMahon JA, McMahon AP, Rosenfeld MG. Multistep signaling requirements for pituitary organogenesis in vivo. Genes Dev. 1998;12:1691–704.
Beatriz M, Lopes S, Pernicone PJ, Scheithauer BW, Horvath E, Kovacs K. Pituitary and sellar region. In: Mills SE, editor. Histology for pathologists. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2012. p. 343–72.
Watanabe YG, Daikoku S. An immunohistochemical study on the cytogenesis of adenohypophysial cells in fetal rats. Dev Biol. 1979;68:557–67.
Asa SL, Kovacs K, Horvath E, Losinski NE, Laszlo FA, Domokos I, Halliday WC. Human fetal adenohypophysis. Electron microscopic and ultrastructural immunocytochemical analysis. Neuroendocrinology. 1988;48:423–31.
Asa SL, Kovacs K, Laszlo FA, Domokos I, Ezrin C. Human fetal adenohypophysis. Histologic and immunocytochemical analysis. Neuroendocrinology. 1986;43:308–16.
Asa SL, Kovacs K, Singer W. Human fetal adenohypophysis: morphologic and functional analysis in vitro. Neuroendocrinology. 1991;53:562–72.
Barson AJ, Symonds J. Calcified pituitary concretions in the newborn. Arch Dis Child. 1977;52:642–5.
Groisman GM, Kerner H, Polak-Charcon S. Calcified concretions in the anterior pituitary gland of the fetus and the newborn: a light and electron microscopic study. Hum Pathol. 1996;27:1139–43.
Naylor MF, Scheithauer BW, Forbes GS, Tomlinson FH, Young WF. Rathke cleft cyst: CT, MR, and pathology of 23 cases. J Comput Assist Tomogr. 1995;19:853–9.
Zada G, Ditty B, McNatt SA, McComb JG, Krieger MD. Surgical treatment of Rathke cleft cysts in children. Neurosurgery. 2009;64:1132–7; author reply 1137–8.
Melchionna RH, Moore RA. The pharyngeal pituitary gland. Am J Pathol. 1938;14:763–72.
Kjaer I, Fischer-Hansen B. Human fetal pituitary gland in holoprosencephaly and anencephaly. J Craniofac Genet Dev Biol. 1995;15:222–9.
Kjaer I, Fischer Hansen B, Reintoft I, Keeling JW. Pituitary gland and axial skeletal malformations in human fetuses with spina bifida. Eur J Pediatr Surg. 1999;9:354–8.
Hori A, Schmidt D, Rickels E. Pharyngeal pituitary: development, malformation, and tumorigenesis. Acta Neuropathol. 1999;98:262–72.
Hampton TA, Scheithauer BW, Rojiani AM, Kovacs K, Horvath E, Vogt P. Salivary gland-like tumors of the sellar region. Am J Surg Pathol. 1997;21:424–34.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ernst, L.M. (2019). Pituitary Gland. In: Ernst, L., Ruchelli, E., Carreon, C., Huff, D. (eds) Color Atlas of Human Fetal and Neonatal Histology. Springer, Cham. https://doi.org/10.1007/978-3-030-11425-1_23
Download citation
DOI: https://doi.org/10.1007/978-3-030-11425-1_23
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-11424-4
Online ISBN: 978-3-030-11425-1
eBook Packages: MedicineMedicine (R0)