
Abstract
Sarcomas represent an extensive group of divergent malignant diseases, with the only common characteristic of being derived from mesenchymal cells. As such, sarcomas are by definition very heterogeneous, and this heterogeneity does not manifest only upon intertumoral comparison on a bulk tumor level but can be extended to intratumoral level. Whereas part of this intratumoral heterogeneity could be understood in terms of clonal genetic evolution, an essential part includes a hierarchical relationship between sarcoma cells, governed by both genetic and epigenetic influences, signals that sarcoma cells are exposed to, and intrinsic developmental programs derived from sarcoma cells of origin. The notion of this functional hierarchy operating within each tumor implies the existence of sarcoma stem cells, which may originate from mesenchymal stem cells, and indeed, mesenchymal stem cells have been used to establish several crucial experimental sarcoma models and to trace down their respective stem cell populations. Mesenchymal stem cells themselves are heterogeneous, and, moreover, there are alternative possibilities for sarcoma cells of origin, like neural crest-derived stem cells, or mesenchymal committed precursor cells, or – in rhabdomyosarcoma – muscle satellite cells. These various origins result in substantial heterogeneity in possible sarcoma initiation. Genetic and epigenetic changes associated with sarcomagenesis profoundly impact the biology of sarcoma stem cells. For pediatric sarcomas featuring discrete reciprocal translocations and largely stable karyotypes, the translocation-activated oncogenes could be crucial factors that confer stemness, principally by modifying transcriptome and interfering with normal epigenetic regulation; the most extensively studied examples of this process are myxoid/round cell liposarcoma, Ewing sarcoma, and synovial sarcoma. For adult sarcomas, which have typically complex and unstable karyotypes, stemness might be defined more operationally, as a reflection of actual assembly of genetically and epigenetically conditioned stemness factors, with dedifferentiated liposarcoma providing a most thoroughly studied example. Alternatively, stemness can be imposed by tumor microenvironment, as extensively documented in osteosarcoma. In spite of this heterogeneity in both sarcoma initiation and underlying stemness biology, some of the molecular mechanisms of stemness might be remarkably similar in diverse sarcoma types, like abrogation of classical tumor suppressors pRb and p53, activation of Sox-2, or inhibition of canonical Wnt/β-catenin signaling. Moreover, even some stem cell markers initially characterized for their stem cell enrichment capacity in various carcinomas or leukemias seem to function quite similarly in various sarcomas. Understanding the biology of sarcoma stem cells could significantly improve sarcoma patient clinical care, leading to both better patient stratification and, hopefully, development of more effective therapeutic options.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Sarcoma
- Liposarcoma
- Ewing sarcoma
- Chondrosarcoma
- Synovial sarcoma
- Osteosarcoma
- Mesenchymal stem cells
- Sarcoma stem cells
- Sarcoma cells of origin
- Genetic and epigenetic plasticity
- In vitro sarcoma progression models
- Sox-2
- p53
- pRb
- Wnt/β-catenin pathway
- Dickkopf
Sarcomas represent an unusually wide, extensive, and heterogeneous group of tumors, whose sole common denominator is that they originate from mesenchymal cells. They could be divided according to various criteria. The most traditional histopathologic classification divides sarcomas into two large groups according to the type of tissue of primary manifestation, namely bone sarcomas , including osteosarcoma and chondrosarcoma , and soft tissue sarcomas , including liposarcoma , fibrosarcoma , undifferentiated pleomorphic sarcoma, leiomyosarcoma , rhabdomyosarcoma , and a large group of other pediatric sarcomas [1]. Besides, we can classify sarcomas according to genetic criteria, and, again, we can distinguish two large groups: sarcomas with largely normal karyotypes and discrete structural chromosomal changes and sarcomas with complex karyotypes and pronounced karyotypic instability. The first group includes especially pediatric sarcomas, which rely for the most part on reciprocal translocations to activate specific oncogenes (Table 7.1). The adult sarcomas – including osteosarcoma , chondrosarcoma , most liposarcomas , fibrosarcoma , angiosarcoma, leiomyosarcoma, and undifferentiated pleomorphic sarcoma – carry usually very complex karyotypes with numerous structural and numerical alterations [2, 4]. Researchers have only begun to understand the complex mechanisms behind this karyotypic instability. Especially dedifferentiated liposarcoma (one of four major liposarcoma groups [5]) features a constantly changing karyotype involving the so-called neochromosomes – giant, sometimes ring-shaped, chromosomal structures that accumulate most of the amplified oncogene loci originating from different chromosomes and result from multiple complex mechanisms, such as chromothripsis and breakage-fusion-bridge cycles [6].
Mesenchymal Stem Cells
Many of the mesenchymal tissues that can be affected by sarcomas undergo continuous remodeling and renewal much like epithelia, and it comes as little surprise that there is a similar hierarchical cellular organization. Supposedly sitting on the top of this cell hierarchy are mesenchymal stem cells (MSCs), which behave much like other adult stem cells, i.e., they can self-renew and differentiate into the respective downstream cell types. For MSCs, trilineage differentiation potential in vitro is considered a sort of a definition criterion. Upon appropriate stimulation, MSCs can enter osteogenic, adipogenic, and chondrogenic differentiation [7, 8]. The true differentiation potential of MSCs is broader, however. At least in vitro, they are able to enter the neurogenic differentiation pathway as well. Of course, they also differentiate into fibroblasts , the major constituent of lamina propria of most, if not all, epithelial tissues. This fibroblastic differentiation pathway can take a special form – the carcinoma-associated fibroblasts (CAFs) – providing a supportive stroma found in practically all carcinomas. Another differentiated cell type originating from MSCs is endothelium , a differentiation pathway exploited by tumors of various origins as well, yielding tumor vasculature.
MSCs can be isolated and propagated from a lot of tissues in the body, two prototypical sources being bone marrow and white adipose tissue . These cells are, nonetheless, not identical and differ in terms of both their relative differentiation abilities and epigenetic genome regulation [9, 10]. These biological differences extend into different nomenclatures: The bone marrow-derived MSCs (BM-MSCs) have been recently proposed to be called skeletal stem cells [11], while the white adipose tissue MSCs are traditionally called adipose tissue -derived stromal cells (ASCs). A notable exception among mesenchymal tissues as to for their exclusive derivation from MSCs is the skeletal muscle, which carries its own stem cell population, the satellite cells. Remarkably, the satellite stem cell niche also adopts a MSCs-like population, again carrying a special name, the fibroblast-adipocyte precursor (FAP) [12]. To make the things even more complicated, there is a separate adult stem cell population, the neural crest-derived stem cells. These cells have descendant cell types, such as specialized neurons, glial cells, and melanocytes, but they can also differentiate into the full spectrum of mesenchymal cell types [13]. In conclusion, there is a pronounced and rather extensive heterogeneity among stem cell populations of normal mesenchymal tissues.
Molecular Biology of MSC Stemness and Differentiation
As introduced above, MSCs have one of the broadest differentiation capacities among adult stem cells, each of the various differentiation programs dominated by specific signals resulting in the activation of specific transcription factors. Transcription factors crucial for osteogenic differentiation are Runx2 and directly downstream positioned Osterix. Among the signals, bone morphogenetic proteins are prominent, resulting in specific Smad activation; notably, a direct Smad-Runx2 protein-protein interaction has been described. Adipogenic differentiation results from the transcription factor succession C/EBPα–C/EBPβ–PPARγ. As to the chondrogenic differentiation, Sox-9 is regarded as a master transcription factor [14].
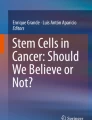
Crucial from the point of view of sarcoma initiation and development, MSC stemness and differentiation seem to be regulated by an intricate network, whose essential players are classical tumor suppressor proteins p53 and pRb on one hand and key stemness regulators SIRT-1 and Sox-2 on the other (Fig. 7.1). First of all, p53 is a general stemness inhibitor, a function not limited to MSCs [15]. Mechanistically, a part of this stemness inhibition relies on direct as well as indirect transcriptional repression of both SIRT-1 (two p53 binding sites in the promoter plus a binding site for the p53 downstream transcription factor HIC-1, as well as p53-inducible miRNA34-mediated silencing) [16, 17] and Sox-2 (mediated mainly by p53-activated miRNA145) [18,19,20]. SIRT-1, a longevity gene, codes for NAD+-dependent protein deacetylase, which, by virtue of this specific posttranslational modification, regulates the activity of numerous cellular proteins. Among them is p53 , with deacetylation resulting in blocking of its nuclear translocation and the significant diminution of transcription activation potency, at least in embryonic stem cells [21]. Sox-2 is another direct SIRT-1 target, but in this case, the effect is exactly opposite: Deacetylation promotes the nuclear localization and transcriptional activation of downstream genes [22]. Besides SIRT-1 and p53-mediated regulation, Sox-2 is transcriptionally repressed in primary fibroblasts by an unusual complex involving cell cycle inhibitor p27 and retinoblastoma family proteins pRb and p130; notably, p53 potentiates this effect [23]. In addition to stemness regulation, p53 is also crucially involved in MSC differentiation. Functional p53 seems to be a necessary prerequisite for successful adipogenic differentiation, in part via mitochondria-generated reactive oxygen species, in part via a direct mutual positive regulation with PPARγ [24]. On the other hand, p53 inhibits both osteogenic (in part by directly repressing the Runx2 gene and inhibiting Osterix activity through a direct protein-protein interaction) [25] and chondrogenic (via the miRNA145-mediated silencing of Sox-9 ) differentiations [18, 19, 26].

Molecular circuitry operating in stemness regulation in MSCs and sarcoma stem cells. See text for detailed explanation
Some of the tumor suppressor activities of p53 and pRb consist in their actions on cellular life span, restricting it and promoting a special type of cell cycle arrest – senescence. Indeed, MSCs – especially of human origin – are not immortal, at least in vitro , and succumb to senescence arrest sometimes after just a few passages; inasmuch these properties lie in the nature of MSCs or result from culture stress (the bone marrow is a frank hypoxic area, whereas MSCs are usually cultured in normal oxygen conditions) is still not entirely clear. Anyway, senescence could be regarded as an antitumor barrier, overcoming of which could be an important step in tumorigenesis. Interestingly, apart from p53 and pRb , there seems to be one more player impacting both MSC differentiation and senescence, namely, the Wnt/β-catenin pathway . The activation of β-catenin has been reported to be part of both osteogenic and chondrogenic differentiations; on the other hand, this pathway also accelerates the senescence of MSCs; MSC immortalization can be promoted by Wnt inhibitor Dickkopf-1 (and by SIRT-1 ) [27, 28].
MSC stemness regulation and sarcomagenesis are associated in various ways. Both SIRT-1 and Sox-2 are poor prognosis factors across various sarcoma types [29, 30]. Diverse sarcomas can be found in increased frequency in affected families suffering from both p53 (Li-Fraumeni syndrome) and pRb (hereditary retinoblastoma) germ line mutation-driven hereditary cancer syndromes [31]. One of the genes carried within the amplified region underlying neochromosome generation in dedifferentiated liposarcoma is MDM2 coding for a direct p53 inhibitor [32]. Our own transcriptomic analysis of two separate progression models of murine soft tissue sarcoma, the JUN fibrosarcoma progression series [33] and the 3T3-L1 – LM3D liposarcoma progression series [34], revealed that Dickopf-2 and Dickkopf-3, as well as additional published inhibitors of canonical Wnt/β-catenin signaling including Adenomatosis polyposis coli down-regulated 1, Fibulin-5, Maternally expressed 3, and Integrator complex subunit 6, are all upregulated during sarcoma progression. Strikingly, this seems to be accompanied by upregulation of the Receptor tyrosine kinase-like orphan receptor 2 (Ror2), suggesting a switch from the canonical Wnt signaling to the noncanonical Wnt5a-Ror2 pathway [34a].
Sarcoma-Initiating Cells and Sarcoma Stem Cells
Keeping in mind the above-outlined development of mesenchymal tissues reflecting an intrinsic cellular hierarchy that starts from mesenchymal stem cells and follows a given differentiation path through progenitors to terminally differentiating cells, it is quite natural to expect that part of this hierarchy would be preserved in sarcomas. Accordingly, we can assume the existence of sarcoma stem cells that both self-renew and differentiate, much like in carcinomas and leukemias. Of course, only some sarcoma types – for example, osteosarcoma , chondrosarcoma , liposarcoma , leiomyosarcoma, or rhabdomyosarcoma – allow to follow a certain differentiation pathway reminiscent of physiological differentiation. Other sarcoma types – diagnosed as undifferentiated pleomorphic sarcoma or simply just spindle cell sarcoma – do not show any easily recognizable differentiation pattern. In fact, the residual differentiation capacity might not be easily discernible even in high-grade tumors of the former sarcoma types. In such cases, the tumorous (pseudo)differentiation can take the form of diversity in functional aspects, like clonogenicity , tumorigenicity , therapeutic resistance, motility, and invasiveness. Various questions about sarcoma stem cells – like those about their abundance, properties, self-renewal, and differentiation ability – should be clearly separated from questions about sarcoma-initiating cells, which are cells that incur the first mutagenic insult ultimately yielding a sarcoma.
In this respect, the various types of mesenchymal stem cells would be apparent candidates [35,36,37]. Several reasons support this conclusion. First, again drawing lessons from various carcinoma and leukemia stem cells, the path from a respective tissue stem cell (mesenchymal for sarcomas) to its derivative cancer stem cell is simpler and more direct than the path assuming cancer initiation in a more differentiated cell, because the various stemness mechanisms are already operating. In addition, the reliance of sarcomas and sarcoma stem cells on Sox-2 and SIRT-1 is a good argument for their derivation from mesenchymal stem cells. We should not forget, however, that MSCs are not a uniform cell type and BM-MSCs clearly differ from ASCs and probably from MSCs isolated from other sources, NCSCs notwithstanding. Another argument is that MSC-specific expression signature has been identified in some sarcomas and it could be especially clearly revealed (together with the restauration of the full multilineage differentiation potential in vitro ) by performing an experimental reversion of sarcoma cells, for example, by an shRNA-mediated knockdown of driver fusion oncogenes in translocation-derived sarcomas. Finally, MSCs are amenable to both spontaneous transformation and purposeful genetic manipulation resulting in sarcomas (see below). This last argument should not be overemphasized, however, because a similar outcome could also be arrived at by the in vitro transformation of normal fibroblasts, that is, differentiated mesenchymal cells [38].
In addition, even though it could be feasible to infer the origin of simpler translocation-dependent sarcomas, this task can be much more complicated in karyotypically complex sarcomas. Indeed, available models suggest alternative possibilities. For example, at least in mouse models, a probable osteosarcoma-initiating cell is an osteogenic progenitor, not MSC [39, 40]. What is more, it could be shown that a human fibrosarcoma cell line could be converted to a liposarcoma by a forced expression of a key liposarcoma oncogene CHOP (DDIT3) [41]. And, of course, rhabdomyosarcomas derive almost certainly from satellite cells [42, 43]. We can thus conclude that there are many potential candidates for the sarcoma cell of origin, including various MSCs and NCSCs and various other mesenchymal cell types.
Modeling Sarcomagenesis in MSCs
Assuming the MSC origin of at least a great part of sarcomas, we can directly use our knowledge of MSC biology – including our ability to differentiate MSCs along a desired path, together with our increasing understanding of underlying biology of diverse sarcomas – to build MSC-based models of sarcoma development. This endeavor can have several forms.
First, we can perform in vitro differentiation of MSCs, identify differentially expressed genes, proteins, or pathways, and relate them to the corresponding sarcoma type. Two studies illustrate well this point. In the first of them, primary human BM-MSCs were subjected to chondrogenic differentiation, and a specific chondrogenesis expression signature was identified. When the gene expression profiles of chondrosarcoma samples of different grades were confronted with the chondrogenesis expression signature, it turned out that all the grade III and grade II metastatic cases clustered together close to the undifferentiated MSCs, whereas grade I and nonmetastatic grade II chondrosarcomas were more similar to late differentiation stages of MSCs approaching mature chondrocytes [44]. This result rather convincingly shows that stemness preservation (or regain) can represent an important contribution to metastatic competence. In addition, the chondrogenesis gene expression signature identified could be of a direct clinical utility, especially for the prognosis of grade II chondrosarcoma patients.
A conceptually similar approach has been applied to liposarcoma . The liposarcoma itself represents a complex diagnosis consisting of at least four distinct tumor types: dedifferentiated, pleomorphic, myxoid/round cell, and well-differentiated [5]. It could be shown that each of them corresponds, at least in terms of their specific gene expression profile, to a different stage of adipogenic differentiated MSC. Again, this result might have an immediate diagnostic value. Dedifferentiated and pleomorphic liposarcomas thus feature the expression of typical MSC markers – like CD44, CD54, and hepatocyte growth factor – while myxoid/round cell and well-differentiated liposarcomas adopt the expression of typical fat markers, namely, adiponectin, leptin, and lipoprotein lipase [45]. This approach made also possible the identification of genes and pathways typical of either path of liposarcomagenesis . Although their clinical utility has yet to be demonstrated, an intriguing candidate pathway compromised in both dedifferentiated and pleomorphic liposarcoma cases is insulin signaling, a very well-defined proadipogenic signaling pathway, which could be amenable to various pharmacological modulations [46]. It should be stressed, nevertheless, that especially dedifferentiated liposarcoma is a very complicated tumor type, for which the cell of origin is largely unclear (it could be a MSC at an early point of adipogenic differentiation or progressing well-differentiated liposarcoma ) and whose genome, as mentioned above, is extremely unstable with unprecedented consequences for gene expression, stemness, and clinical behavior (see below).
If we embrace the idea that most sarcomas may originate from MSCs, a logical next step is to undertake an attempt at deriving sarcoma models by their targeted manipulation. In the last decade, several valuable sarcoma models have been established in this way, revealing several general rules of sarcoma development. First, it turned out that rodent (especially murine) MSCs are distinctly more susceptible to initiate sarcomagenesis than their human counterparts; indeed, murine and rat MSCs are even prone to spontaneous sarcomagenesis upon prolonged in vitro culture, which is practically never observed in human MSCs. We can only speculate about biological reasons for this difference. It is known for quite a long time that mouse adult tissues constitutively express telomerase and the murine cells are thus immortal upon appropriate cell culture conditions, eliminating the senescence barrier (see above). In addition, most – if not all – experiments have been performed on MSCs isolated from various inbred mouse strains, and we can assume a random fixation of various mutant alleles during the inbreeding process. The existing senescence barrier – probably among other mechanisms – makes human MSCs intrinsically resistant to sarcomagenesis, and usually this is the first obstacle to be overcome in order to convert human primary MSCs into desired sarcoma cells. A standard approach is to introduce viral oncogenes that eliminate the p53 - and pRb -mediated senescence arrest (HPV E6 and E7 oncogenes or SV40 large T antigen, respectively), complemented by the stable overexpression of the gene coding for catalytic subunit of telomerase (hTERT) [47, 48]. Even these MSC derivative cell lines (called 3 hit MSCs – E6, E7, and hTERT) were not susceptible to spontaneous sarcomagenesis, and two additional genetic steps turned out to be necessary, namely, c-Myc stabilization by virtue of SV40 small t antigen expression and a permanent mitogenic stimulation by the forced expression of a constitutively active Ha-Ras oncogene [47, 48]; Myc-Ras is a traditional cooperating oncogene pair, defined by its joint ability to transform rat embryonic fibroblasts [49]. The resulting 5 hit MSCs finally yielded undifferentiated pleomorphic sarcomas when injected into a severely immunocompromised mouse [50].
A separate question is which factors promote particular types of sarcomagenesis. This seems to be a very complex issue encompassing several points, such as the source of MSCs (BM-MSCs vs. ASCs), their species origin (mouse or human), and of course the genetic changes either spontaneously accumulated or purposefully introduced. Especially, p53 deficiency (alone or combined with pRb deficiency) can initiate various sarcoma types depending on other factors. In mouse BM-MSCs , spontaneous p53 mutations have been associated with fibrosarcoma development [51], whereas mouse p53−/− ASCs were transformed toward leiomyosarcoma [50], and the combined deficiency of both p16INK4a and p19ARF (two tumor suppressor proteins encoded by a single locus and acting via pRb and p53 pathways, respectively [49]) coupled to c-Myc overexpression in mouse BM-MSCs triggered osteosarcoma development [52]. The knowledge and availability of translocation-activated fusion oncogenes provided additional possibilities of specifically directing sarcomagenesis along a desired pathway. The FUS-CHOP oncoprotein , specific for myxoid/round cell liposarcoma , provided a particularly revealing example. A purposeful expression of FUS-CHOP in mouse ASC of p53−/− background [50], in 4 hit (HPV E6, E7, hTERT, and SV40 small-t) or 5 hit (+ Ha-RasV12) human BM-MSC backgrounds [50], or in HT1080 fibrosarcoma cells [41], respectively, was able to divert the pathway of sarcomagenesis from leiomyosarcoma , undifferentiated pleomorphic sarcoma, or fibrosarcoma to liposarcoma . It seems, therefore, that this type of liposarcomagenesis involves at least two principal causal factors: a general tumorigenic transformation of cells (provided by the recipient cells that are already competent to various types of sarcomagenesis) and a limited, corrupt, and incomplete lipomatous differentiation provided by the FUS-CHOP translocation oncoprotein.
Ewing sarcoma provides another example of a sarcoma that relies on a translocation oncogene imposing its effect on target cells. From a certain point of view, its biology seems to be opposite to myxoid/round cell liposarcoma , with sarcomagenesis resulting from a specific dedifferentiation or reprogramming toward a primitive stem cell phenotype. Indeed, in transgenic mice, a conditional p53 deletion in embryonic limb bud cells led predominantly to osteosarcoma (i.e., a tumor featuring an intrinsic partial differentiation ability) [53], while if combined with EWS-FLI-1 translocation oncogene overexpression, this partial differentiation was lost, leading to Ewing sarcoma-like tumors [54]. Like FUS-CHOP , EWS-FLI-1 alone does not transform human adult BM-MSCs (unlike mouse MSCs), but it is able to impose a gene expression profile reminiscent of Ewing sarcoma [55]. Intriguingly, the degree of matching between these gene expression profiles was even greater if pediatric instead of adult BM-MSCs were used. A further increase was achieved when EWS-FLI-1-transduced pediatric human BM-MSCs were cultured in medium used to raise induced pluripotent stem cells [20], quite clearly classifying Ewing sarcoma as a stem cell- or reprogramming-type malignancy.
On the other hand, it is not yet clear whether MSCs are the cells of origin for Ewing sarcoma . Independent experiments with EWS-FLI-1-transduced NCSCs also showed a strong concordance with the Ewing sarcoma gene expression profile [56], leaving the question of Ewing sarcoma’s cell of origin open. A similar question with a very similar dilemma is also pending for synovial sarcoma [57, 58].
Sarcoma Stem Cell Heterogeneity
From all the discussion above, we can take the existence of sarcoma stem cells as, if not certain, then certainly highly probable. Various approaches have been adopted to identify and isolate sarcoma stem cells (Table 7.2), which are, by and large, identical to those applied in various carcinomas, lymphomas, and leukemias, including a group of “obligate” stem cell markers , like CD44, CD90, and CD133 [80]. Such approaches suffer from an inherent weakness that they are based on an a priori assumption that positive cells equal stem cells, which is not always true. Specific for certain sarcomas could be cell surface markers that define normal mesenchymal stem cells.
Another possibility would be a marker-free approach essentially aimed at identifying chemoresistant cancer and normal stem cells, like side population (SP) sorting directed toward cells with a high expression of ABC efflux membrane transporters, especially ABCB1 and ABCG2, or Aldefluor assay targeting cells specifically overexpressing detoxification enzymes of aldehyde dehydrogenase family, especially ALDH1A1 and ALDH1A3 [81]. Several experimental models in which sarcomagenesis could be followed in a stepwise manner showed that sarcoma development and progression were associated with an increase in the stem cell fraction, expressed as both SP- [79] and Aldefluor-positive cells [65]. This association could be interpreted as sarcomas representing indeed stem cell tumors. Interestingly in this context, the Wnt inhibitor Dickkopf-1 has been reported not only to be crucial to overcoming senescence but also to increase ALDH1A1 expression and thus to promote sarcoma stemness [82]. In addition, specific stem cell targeting could be one mechanism of action of a relatively new antisarcoma chemotherapeutic drug trabectedin [83].
Genetic and Epigenetic Plasticity of Sarcoma Stem Cells
An obvious question is inasmuch stemness of potential sarcoma stem cells is a “heritage” from an initiated normal stem cell (in this case most probably a mesenchymal stem cell) or whether it results directly from the action of sarcoma oncogenes. Two karyotypically simple translocation-dependent sarcomas could be rather instrumental to illustrate the latter possibility.
Synovial sarcoma is initiated by t(X;18)(p11;q11) translocation, resulting in a fusion protein between SS18 (whose gene is located on chromosome 18) and one of the translocation partner proteins SS1, SS2, or, rarely, SS4 (collectively called SSX, encoded by multiple homologous genes located on chromosome X) [84]. It has been reported that synovial sarcoma cells, without any sorting or selection, exhibited a high degree of stemness: Clonogenicity (sarcosphere formation) and tumorigenicity were comparable to those achieved by stem cell marker sorted populations in other tumors [85]. The SS18-SSX chimeric proteins encompass several transcription regulatory and protein-protein interaction domains, but, notably, no DNA-binding domain. The actual notion is that SS18-SSX engages a plethora of protein interaction partners, leading to complex changes in gene expression and finally resulting in accentuated stemness. Well-documented protein-protein interaction takes place between SS18-SSX and epithelial-mesenchymal transition (EMT)-triggering transcription repressors Snail and Slug, which prevents their binding to the E-cadherin gene promoter and results in pseudoepithelial transdifferentiation observed in some synovial sarcomas [85a]. Many SS18-SSX interaction partners involve chromatin modifier proteins, with a complex epigenetic reprogramming as a direct consequence. For example, it has been reported that SS18-SS2 directly interacts with the Polycomb-group complex 1 components Bmi1 and Ring1B, resulting in Bmi1 destabilization and the consequent derepression of a large group of Polycomb-silenced developmental genes. SS18 itself is a component of the mSWI/SNF-BAF chromatin remodeling complex, and its replacement by SS18-SSX fusion oncoproteins leads to complex changes in gene expression, among others to the erasure of the repressive histone mark H3K27me3 at the Sox-2 locus [86, 87].
Strikingly, both of these effects are achieved also by the EWS-FLI-1 fusion oncoprotein underlying Ewing sarcoma , but via different mechanisms. Unlike SS18-SSX, EWS-FLI-1 acts on its own as a direct transcription factor, via the ETS-DNA-binding domain supplied by the FLI-1 translocation partner [88]. According to recent results, EWS-FLI-1 can directly compete with the Polycomb repressor complex 1 (or, more probably, transcription factors mediating its recruitment, like YY-1) for binding to particular loci – notably certain HOX genes, especially posterior HOXD genes – resulting in their derepression [89]. In addition, it likely acts as both direct and indirect activator of Sox-2 . This latter regulatory function is based on its direct transcriptional repression of miRNA145, encoded by a p53 -responsive gene and directly targeting Sox-2 (as well as Oct-4). Intriguingly, EWS-FLI-1 is itself a target of miRNA145-mediated silencing, its repression thus stabilizing EWS-FLI-1 itself as well, a regulatory circuit already described for the relationship between Oct-4 and miRNA145 in embryonic stem cells [20].
Not surprisingly, all the epigenetic regulations crucially depend on the entire regulatory context resulting from signals acting on the cell. In the above-discussed experimental analyses of both synovial sarcoma and Ewing sarcoma , variations in cell culture media played important roles. In vivo, such a regulatory context would probably differ from cell to cell, generating a heterogeneous cell population with variable expressions of stemness traits in each individual sarcoma cell.
What is the situation in karyotypically complex sarcomas? As already mentioned above, dedifferentiated liposarcoma is an example of tumor type with an unusually high degree of genetic and epigenetic instability. This instability manifests at all thinkable levels. Karyotypic instability is mainly represented by neochromosomes , giant or ring chromosomes accumulating amplified segments of various chromosomes. Their origin is not clear, but the consensus is that they are triggered by the originally extrachromosomal amplification of a specific amplicon at 12q. Among the genes amplified are MDM2 (coding for a direct p53 inhibitor, as mentioned above), CDK4, and YEATS2 (coding for an acetylated and crotonylated histone reader). Via repeated breakage-fusion-bridge cycles, the 12q amplicon triggers a progressive genome destabilization, including structural chromosomal aberrations [90]. Notable among them is the translocation between HMGA2 and CPM genes. HMGA2 codes for a nonhistone chromatin protein involved in global gene expression regulation. The translocation removes the 3′-part of the HMGA2 gene, resulting in two principal effects. First, it leads to the production of a shortened protein, and, second, because the removed 3′-part of the gene contains at least three target sequences for the let-7 miRNA, this shortened HMGA2 protein is grossly overexpressed [91]. Intact HMGA2 expressed at a normal level promotes adipogenic differentiation; an overexpressed full-length or shortened protein abolishes it instead, however. In addition, overexpressed HMGA2 has particular gene expression consequences. Among the genes it specifically induces, prominent is the SS1, one of the synovial sarcoma translocation partners (see above), eventually promoting stemness [92]. Copy number alterations in dedifferentiated liposarcoma underlie the overexpression of some additional genes with presumed roles in stemness (c-JUN oncogene, mesenchymal stem cell factor gene TUFT1) or chromatin organization (heterochromatin factor gene CBX1) [90]. There can also be more traditional epigenetic aberrations, like the promoter hypermethylation of the gene encoding the key adipogenic transcription factor C/EBPα or of the miRNA193b gene [93]. One of the miRNA193b targets is the fatty acid synthase – an important cancer metabolic enzyme that (as described for leiomyosarcoma ) at the same time interacts with various histone modification enzymes and modulates their activity [94], producing a sort of feed-forward loop in epigenome destabilization. Last but not the least, some point mutations found in liposarcoma can produce similarly widespread epigenetic consequences to those caused by more extensive changes described above. About 8% of dedifferentiated liposarcoma cases harbor point mutations (mostly missense) in the gene encoding histone deacetylase 1 [93]; striking in this respect is the finding that HDAC inhibitors might specifically target sarcoma stem cells (as described for the osteosarcoma model) [95].
These various mechanisms of dedifferentiated liposarcoma genome instability create an unprecedented level of genetic and epigenetic plasticity and impacts numerous genes implicated in differentiation and stemness regulation. This situation sets a completely new stage for research on cancer stem cell heterogeneity. Traditionally, it has automatically been assumed that a cancer stem cell achieves its stemness either from an initially mutated normal stem cell or as the direct molecular consequence of an initiating mutation. Once established, cancer stemness can be passed to some daughter cells, resulting in a more or less stable cancer stem cell pool, and it can be lost only by differentiation. Isolated populations of cancer stem cells, like side population cells or stem cell marker sorted cells, thus provide quasi-pure stem cells, but for a certain time only – until they are diluted by differentiation. In the context of the huge genetic and epigenetic plasticity, like that found in dedifferentiated liposarcoma , stemness might be understood in a completely different way. Stem cells might correspond simply to cells that at a given moment accumulate a sufficient number of stemness-promoting and differentiation-inhibiting mutations and epigenetic changes; in other words, stemness can be understood as a defined actual functional state rather than a quasi-fixed cell type. Some of such stem cells may differentiate, others can simply lose their stemness-promoting and differentiation-inhibiting genetic and epigenetic changes as a direct consequence of genetic and epigenetic plasticity, and still others, originally non-stem cells, can regain these changes by the same token. Stem and non-stem cells are thus continuously and bidirectionally changing, mixing, and merging.
Microenvironmental Influence on Sarcoma Stem Cells
All the discussion on sarcoma stem cells pursued by now concentrated largely on cell-autonomous mechanisms. We know, however, that tissue homeostasis is regulated by the cross talk between tissue-specific stem cells and their microenvironment, and, in a similar way, signaling from tumor niches may play relevant roles in the regulation of sarcoma stem cells [96,97,98]. Among the different subtypes of sarcoma, the relevance of the interaction between microenvironmental components and cancer (stem) cells has been especially well described in osteosarcoma [99]. Osteosarcoma cells closely interact with local microenvironmental cell types, such as stromal cells (MSCs and cancer-associated fibroblasts), osteoblasts, osteocytes, osteoclasts, or chondrocytes, as well as with immune infiltrates mainly composed of T lymphocytes and macrophages [97, 100]. The interaction between these multiple players results in the production of signaling factors that contribute to either favoring or decrease of stemness properties in osteosarcoma [97]. Thus, signaling mediated by fibroblastic growth factor (FGF)-Sox2 axis [101], transforming growth factor β (TGF-β) [102], the Hippo signaling regulator YAP1 [103], or NOTCH1 [40], among others, was reported to promote stemness in osteosarcoma . On the other hand, signals with proven pro-osteogenic activities, like those dependent on bone morphogenetic proteins (BMP) [104] or WNT factors [101], seem to decrease sarcoma stem cell frequency and to promote osteogenic differentiation. In addition, extracellular matrix components of the tumor microenvironment have also been reported to interact with sarcoma stem cells. This is the case of hyaluronan, which may promote stemness properties in tumor cells through the binding with its receptor, the cancer stem cell marker CD44 ([105] – see Table 7.2). We can assume that details of composition of this complex tumor microenvironment differ in each individual tumor, resulting in a wide spectrum of osteosarcoma stemness modulation.
Notice that within the context of osteosarcoma (and possibly other sarcoma types as well), MSCs can thus be viewed not only as possible cells of origin but also as a stromal supporting type. Indeed, MSCs are the cell type with rather precisely described interactions with osteosarcoma stem cell subpopulations. MSCs may be activated by the acidic conditions generated by osteosarcoma cells and these tumor-conditioned MSCs favor osteosarcoma stemness and chemoresistance via IL6-NF-κB signaling [106]. Moreover, MSCs may increase chemoresistance of osteosarcoma cells through the activation of IL6/STAT3 pathway [107].
Several locations within the bone microenvironment where pro-stemness signaling is particularly active have been proposed as suitable niches for osteosarcoma stem cells [96] (Fig. 7.2): (i) the perivascular niche, which was described as the most likely location for the most immature MSCs and therefore may also constitute a niche for sarcoma stem cells originated by transformed MSCs [108]; (ii) the hypoxic niche, which is an important stemness-promoting environmental condition in bones [109]; and (iii) the endosteal niche, which is a signal-rich environment where tumor cells interfere with the bone remodeling process, establishing a “vicious cycle” that favors osteoclast-mediated osteolysis and the subsequent release of calcium and growth factors (FGF, TGF-β, IGF1, BMP, etc.), which support stem and tumorigenic properties [97]. In any case, these three prototypical osteosarcoma niche types differ in their detailed molecular mechanisms of stem cell support, plausibly resulting in a niche-dependent osteosarcoma stem cell heterogeneity.

Osteosarcoma stem cell niches. Figure shows the most relevant cell types of the bone microenvironment that may interact with osteosarcoma cells. Suggested locations for osteosarcoma stem cells include the perivascular niche, the endosteal niche, and the areas of poor vascularization (hypoxic niche) (adapted from [96]
The detailed knowledge of the microenvironment in maintaining tumor homeostasis has encouraged the development and testing of therapies aimed to counteract pro-tumoral signals, including pro-stemness signals, from the microenvironment [96]. Consequently, several therapeutic strategies have been recently developed to target the role of the tumor-promoting osteoclast activity [110, 111], to reduce the vascularization of tumors [112], and to enhance the immune response against tumors [113, 114].
References
Skubitz KM, D’Adamo DR (2007) Sarcoma. Mayo Clin Proc 82(11):1409–1432
Penzel R, Schirmacher P, Renner M, Mechtersheimer G (2011) Molekularpathologie maligner Weichgewebetumoren. In: Schlag PM, Hartmann JT, Budach V (eds) Weichgewebetumoren: Interdisziplinäres Management. Springer, Berlin Heidelberg, Berlin, Heidelberg, pp 23–35
Oda Y, Yamamoto H, Kohashi K, Yamada Y, Iura K, Ishii T, Maekawa A, Bekki H (2017) Soft tissue sarcomas: from a morphological to a molecular biological approach. Pathol Int 67(9):435–446
Taylor BS, Barretina J, Maki RG, Antonescu CR, Singer S, Ladanyi M (2011a) Advances in sarcoma genomics and new therapeutic targets. Nat Rev Cancer 11(8):541–557
Henze J, Bauer S (2013) Liposarcomas. Hematol Oncol Clin North Am 27(5):939–955
Papenfuss AT, Thomas DM (2015) The life history of neochromosomes revealed. Mol Cell Oncol 2(4):e1000698
Frenette PS, Pinho S, Lucas D, Scheiermann C (2013) Mesenchymal stem cell: keystone of the hematopoietic stem cell niche and a stepping-stone for regenerative medicine. Annu Rev Immunol 31:285–316
Schäfer R, Northoff H (2008) Characteristics of mesenchymal stem cells—new stars in regenerative medicine or unrecognized old fellows in autologous regeneration? Transfus Med Hemotherapy 35(3):154–159
Guneta V, Tan NS, Chan SKJ, Tanavde V, Lim TC, Wong TCM, Choong C (2016) Comparative study of adipose-derived stem cells and bone marrow-derived stem cells in similar microenvironmental conditions. Exp Cell Res 348(2):155–164
Meyer MB, Benkusky NA, Sen B, Rubin J, Pike JW (2016) Epigenetic plasticity drives adipogenic and osteogenic differentiation of marrow-derived mesenchymal stem cells. J Biol Chem 291(34):17,829–17,847
Bianco P, Robey PG (2015) Skeletal stem cells. Development 142(6):1023–1027
Dinulovic I, Furrer R, Handschin C (2017) Plasticity of the muscle stem cell microenvironment. Adv Exp Med Biol 1041:141–169
Shakhova O, Sommer L (2010) Neural crest-derived stem cells. In: The Stem Cell Research Community (ed) StemBook. Harvard Stem Cell Institute, Cambridge, MA
Almalki SG, Agrawal DK (2016) Key transcription factors in the differentiation of mesenchymal stem cells. Differ Res Biol Divers 92(1–2):41–51
Rivlin N, Koifman G, Rotter V (2015) p53 orchestrates between normal differentiation and cancer. Semin Cancer Biol 32:10–17
Chen WY, Wang DH, Yen RC, Luo J, Gu W, Baylin SB (2005) Tumor suppressor HIC1 directly regulates SIRT1 to modulate p53-dependent DNA-damage responses. Cell 123(3):437–448
Yamakuchi M, Lowenstein CJ (2009) miR-34, SIRT1 and p53: the feedback loop. Cell Cycle 8:712–715
Goeman F, Strano S, Blandino G (2017) MicroRNAs as key effectors in the p53 network. Int Rev Cell Mol Biol 333:51–90
Luo Z, Cui R, Tili E, Croce C (2018) Friend or foe: microRNAs in the p53 network. Cancer Lett 419:96–102
Riggi N, Suvà M-L, De Vito C, Provero P, Stehle J-C, Baumer K, Cironi L, Janiszewska M, Petricevic T, Suvà D, Tercier S, Joseph J-M, Guillou L, Stamenkovic I (2010) EWS-FLI-1 modulates miRNA145 and SOX2 expression to initiate mesenchymal stem cell reprogramming toward Ewing sarcoma cancer stem cells. Genes Dev 24(9):916–932
Han M-K, Song E-K, Guo Y, Ou X, Mantel C, Broxmeyer HE (2008) SIRT1 regulates apoptosis and Nanog expression in mouse embryonic stem cells by controlling p53 subcellular localization. Cell Stem Cell 2(3):241–251
Yoon DS, Choi Y, Jang Y, Lee M, Choi WJ, Kim S-H, Lee JW (2014) SIRT1 directly regulates SOX2 to maintain self-renewal and multipotency in bone marrow-derived mesenchymal stem cells. Stem Cells 32(12):3219–3231
Vilas JM, Ferreirós A, Carneiro C, Morey L, Silva-Álvarez SD, Fernandes T, Abad M, Croce LD, García-Caballero T, Serrano M, Rivas C, Vidal A, Collado M (2014) Transcriptional regulation of Sox2 by the retinoblastoma family of pocket proteins. Oncotarget 6(5):2992–3002
Boregowda SV, Krishnappa V, Strivelli J, Haga CL, Booker CN, Phinney DG (2018) Basal p53 expression is indispensable for mesenchymal stem cell integrity. Cell Death Differ 25(4):677–690
Artigas N, Gámez B, Cubillos-Rojas M, Sánchez-de Diego C, Valer JA, Pons G, Rosa JL, Ventura F (2017) p53 inhibits SP7/Osterix activity in the transcriptional program of osteoblast differentiation. Cell Death Differ 24(12):2022–2031
Martinez-Sanchez A, Dudek KA, Murphy CL (2012) Regulation of human chondrocyte function through direct inhibition of cartilage master regulator SOX9 by microRNA-145 (miRNA-145). J Biol Chem 287(2):916–924
Honoki K, Tsujiuchi T (2013) Senescence bypass in mesenchymal stem cells: a potential pathogenesis and implications of pro-senescence therapy in sarcomas. Expert Rev Anticancer Ther 13(8):983–996
Matushansky I, Hernando E, Socci ND, Mills JE, Matos TA, Edgar MA, Singer S, Maki RG, Cordon-Cardo C (2007) Derivation of sarcomas from mesenchymal stem cells via inactivation of the Wnt pathway. J Clin Invest 117(11):3248–3257
Kim JR, Moon YJ, Kwon KS, Bae JS, Wagle S, Yu TK, Kim KM, Park HS, Lee J-H, Moon WS, Lee H, Chung MJ, Jang KY (2013) Expression of SIRT1 and DBC1 is associated with poor prognosis of soft tissue sarcomas. PLoS One 8(9):e74738
Skoda J, Nunukova A, Loja T, Zambo I, Neradil J, Mudry P, Zitterbart K, Hermanova M, Hampl A, Sterba J, Veselska R (2016) Cancer stem cell markers in pediatric sarcomas: Sox2 is associated with tumorigenicity in immunodeficient mice. Tumour Biol 37(7):9535–9548
Plon SE, Malkin D (2010) Childhood cancer and heredity. In: Principles and practice of pediatric oncology, Sixth edition. LWW, Philadelphia, PA, pp 17–37
Kanojia D, Nagata Y, Garg M, Lee DH, Sato A, Yoshida K, Sato Y, Sanada M, Mayakonda A, Bartenhagen C, Klein H-U, Doan NB, Said JW, Mohith S, Gunasekar S, Shiraishi Y, Chiba K, Tanaka H, Miyano S, Myklebost O, Yang H, Dugas M, Meza-Zepeda LA, Silberman AW, Forscher C, Tyner JW, Ogawa S, Koeffler HP (2015) Genomic landscape of liposarcoma. Oncotarget 6(40):42,429–42,444
Hatina J, Hájková L, Peychl J, Rudolf E, Fínek J, Cervinka M, Reischig J (2003) Establishment and characterization of clonal cell lines derived from a fibrosarcoma of the H2-K/V-JUN transgenic mouse. A model of H2-K/V-JUN mediated tumorigenesis. Tumour Biol 24(4):176–184
Mariani O, Brennetot C, Coindre J-M, Gruel N, Ganem C, Delattre O, Stern M-H, Aurias A (2007) JUN oncogene amplification and overexpression block adipocytic differentiation in highly aggressive sarcomas. Cancer Cell 11(4):361–374
Endo M, Nishita M, Fujii M, Minami Y (2015) Insight into the role of Wnt5a-induced signaling in normal and cancer cells. Int Rev Cell Mol Biol 314:117–148
Lye KL, Nordin N, Vidyadaran S, Thilakavathy K (2016) Mesenchymal stem cells: from stem cells to sarcomas. Cell Biol Int 40(6):610–618
Gaebler M, Silvestri A, Haybaeck J, Reichardt P, Lowery CD, Stancato LF, Zybarth G, Regenbrecht CRA (2017) Three-dimensional patient-derived in vitro sarcoma models: Promising tools for improving clinical tumor management. Front Oncol 7:203
Xiao W, Mohseny AB, Hogendoorn PCW, Cleton-Jansen A-M (2013) Mesenchymal stem cell transformation and sarcoma genesis. Clin Sarcoma Res 3(1):10
Hahn WC, Counter CM, Lundberg AS, Beijersbergen RL, Brooks MW, Weinberg RA (1999) Creation of human tumour cells with defined genetic elements. Nature 400(6743):464–468
Rubio R, Gutierrez-Aranda I, Sáez-Castillo AI, Labarga A, Rosu-Myles M, Gonzalez-Garcia S, Toribio ML, Menendez P, Rodriguez R (2013) The differentiation stage of p53-Rb-deficient bone marrow mesenchymal stem cells imposes the phenotype of in vivo sarcoma development. Oncogene 32(41):4970–4980
Tao J, Jiang M-M, Jiang L, Salvo JS, Zeng H-C, Dawson B, Bertin TK, Rao PH, Chen R, Donehower LA, Gannon F, Lee BH (2014) Notch activation as a driver of osteogenic sarcoma. Cancer Cell 26(3):390–401
Engström K, Willén H, Kåbjörn-Gustafsson C, Andersson C, Olsson M, Göransson M, Järnum S, Olofsson A, Warnhammar E, Aman P (2006) The myxoid/round cell liposarcoma fusion oncogene FUS-DDIT3 and the normal DDIT3 induce a liposarcoma phenotype in transfected human fibrosarcoma cells. Am J Pathol 168(5):1642–1653
Morena D, Maestro N, Bersani F, Forni PE, Lingua MF, Foglizzo V, Šćepanović P, Miretti S, Morotti A, Shern JF, Khan J, Ala U, Provero P, Sala V, Crepaldi T, Gasparini P, Casanova M, Ferrari A, Sozzi G, Chiarle R, Ponzetto C, Taulli R (2016) Hepatocyte growth factor-mediated satellite cells niche perturbation promotes development of distinct sarcoma subtypes. Elife 5:pii: e12116
Rubin BP, Nishijo K, Chen H-IH, Yi X, Schuetze DP, Pal R, Prajapati SI, Abraham J, Arenkiel BR, Chen Q-R, Davis S, McCleish AT, Capecchi MR, Michalek JE, Zarzabal LA, Khan J, Yu Z, Parham DM, Barr FG, Meltzer PS, Chen Y, Keller C (2011) Evidence for an unanticipated relationship between undifferentiated pleomorphic sarcoma and embryonal rhabdomyosarcoma. Cancer Cell 19(2):177–191
Boeuf S, Kunz P, Hennig T, Lehner B, Hogendoorn P, Bovée J, Richter W (2008) A chondrogenic gene expression signature in mesenchymal stem cells is a classifier of conventional central chondrosarcoma. J Pathol 216(2):158–166
Matushansky I, Hernando E, Socci ND, Matos T, Mills J, Edgar MA, Schwartz GK, Singer S, Cordon-Cardo C, Maki RG (2008) A developmental model of sarcomagenesis defines a differentiation-based classification for liposarcomas. Am J Pathol 172(4):1069–1080
Borgo C, Milan G, Favaretto F, Stasi F, Fabris R, Salizzato V, Cesaro L, Belligoli A, Sanna M, Foletto M, Prevedello L, Vindigni V, Bardini R, Donella-Deana A, Vettor R (2017) CK2 modulates adipocyte insulin-signaling and is up-regulated in human obesity. Sci Rep 7(1):17,569
Funes JM, Quintero M, Henderson S, Martinez D, Qureshi U, Westwood C, Clements MO, Bourboulia D, Pedley RB, Moncada S, Boshoff C (2007) Transformation of human mesenchymal stem cells increases their dependency on oxidative phosphorylation for energy production. Proc Natl Acad Sci U S A 104(15):6223–6228
Rodriguez R, Rubio R, Menendez P (2012) Modeling sarcomagenesis using multipotent mesenchymal stem cells. Cell Res 22(1):62–77
Schulz W (2005) Molecular biology of human cancers: an advanced student’s textbook. Springer, Netherlands
Rodriguez R, Tornin J, Suarez C, Astudillo A, Rubio R, Yauk C, Williams A, Rosu-Myles M, Funes JM, Boshoff C, Menendez P (2013) Expression of FUS-CHOP fusion protein in immortalized/transformed human mesenchymal stem cells drives mixoid liposarcoma formation. Stem Cells 31(10):2061–2072
Li H, Fan X, Kovi RC, Jo Y, Moquin B, Konz R, Stoicov C, Kurt-Jones E, Grossman SR, Lyle S, Rogers AB, Montrose M, Houghton J (2007) Spontaneous expression of embryonic factors and p53 point mutations in aged mesenchymal stem cells: a model of age-related tumorigenesis in mice. Cancer Res 67(22):10,889–10,898
Shimizu T, Ishikawa T, Sugihara E, Kuninaka S, Miyamoto T, Mabuchi Y, Matsuzaki Y, Tsunoda T, Miya F, Morioka H, Nakayama R, Kobayashi E, Toyama Y, Kawai A, Ichikawa H, Hasegawa T, Okada S, Ito T, Ikeda Y, Suda T, Saya H (2010) c-MYC overexpression with loss of Ink4a/Arf transforms bone marrow stromal cells into osteosarcoma accompanied by loss of adipogenesis. Oncogene 29(42):5687–5699
Lin PP, Pandey MK, Jin F, Raymond AK, Akiyama H, Lozano G (2009) Targeted mutation of p53 and Rb in mesenchymal cells of the limb bud produces sarcomas in mice. Carcinogenesis 30(10):1789–1795
Lin PP, Pandey MK, Jin F, Xiong S, Deavers M, Parant JM, Lozano G (2008) EWS-FLI1 induces developmental abnormalities and accelerates sarcoma formation in a transgenic mouse model. Cancer Res 68(21):8968–8975
Riggi N, Suvà M-L, Suvà D, Cironi L, Provero P, Tercier S, Joseph J-M, Stehle J-C, Baumer K, Kindler V, Stamenkovic I (2008) EWS-FLI-1 expression triggers a Ewing’s sarcoma initiation program in primary human mesenchymal stem cells. Cancer Res 68(7):2176–2185
von Levetzow C, Jiang X, Gwye Y, von Levetzow G, Hung L, Cooper A, Hsu JH-R, Lawlor ER (2011) Modeling initiation of Ewing sarcoma in human neural crest cells. PLoS One 6(4):e19305
Mihály D, Matula Z, Changchien Y-C, Papp G, Tátrai P, Sápi Z (2017) First cloned human immortalized adipose derived mesenchymal stem-cell line with chimeric SS18-SSX1 gene (SS-iASC). Cancer Genet 216-217:52–60
Tamaki S, Fukuta M, Sekiguchi K, Jin Y, Nagata S, Hayakawa K, Hineno S, Okamoto T, Watanabe M, Woltjen K, Ikeya M, Jr TK, Toguchida J (2015) SS18-SSX, the oncogenic fusion protein in synovial sarcoma, is a cellular context-dependent epigenetic modifier. PLoS One 10(11):e0142991
Dela Cruz FS (2013) Cancer stem cells in pediatric sarcomas. Front Oncol 3:168
Skoda J, Veselska R (2018) Cancer stem cells in sarcomas: getting to the stemness core. Biochim Biophys Acta 1862(10):2134–2139
Veselska R, Skoda J, Neradil J (2012) Detection of cancer stem cell markers in sarcomas. Klin Onkol 25(Suppl 2):2S16–2S20
Wu C, Wei Q, Utomo V, Nadesan P, Whetstone H, Kandel R, Wunder JS, Alman BA (2007) Side population cells isolated from mesenchymal neoplasms have tumor initiating potential. Cancer Res 67(17):8216–8222
Zhou Y, Zhou Y, Chen D, Chen D, Qi Y, Qi Y, Liu R, Liu R, Li S, Li S, Zou H, Zou H, Lan J, Lan J, Ju X, Ju X, Jiang J, Jiang J, Liang W, Liang W, Shen Y, Shen Y, Pang L, Pang L, Li F, Li F (2017) Evaluation of expression of cancer stem cell markers and fusion gene in synovial sarcoma: insights into histogenesis and pathogenesis. Oncol Rep 37(6):3351–3360
Lohberger B, Rinner B, Stuendl N, Absenger M, Liegl-Atzwanger B, Walzer SM, Windhager R, Leithner A (2012) Aldehyde dehydrogenase 1, a potential marker for cancer stem cells in human sarcoma. PLoS One 7(8):e43664
Martinez-Cruzado L, Tornin J, Santos L, Rodriguez A, García-Castro J, Morís F, Rodriguez R (2016) Aldh1 expression and activity increase during tumor evolution in sarcoma cancer stem cell populations. Sci Rep 6:27,878
Siclari VA, Qin L (2010) Targeting the osteosarcoma cancer stem cell. J Orthop Surg 5(1):78
Kimura T, Wang L, Tabu K, Tsuda M, Tanino M, Maekawa A, Nishihara H, Hiraga H, Taga T, Oda Y, Tanaka S (2015) Identification and analysis of CXCR4-positive synovial sarcoma-initiating cells. Oncogene 35(30):3932–3943
Adhikari AS, Agarwal N, Wood BM, Porretta C, Ruiz B, Pochampally RR, Iwakuma T (2010) CD117 and Stro-1 identify osteosarcoma tumor-initiating cells associated with metastasis and drug resistance. Cancer Res 70(11):4602–4612
Tirino V, Desiderio V, Paino F, De Rosa A, Papaccio F, Fazioli F, Pirozzi G, Papaccio G (2011) Human primary bone sarcomas contain CD133+ cancer stem cells displaying high tumorigenicity in vivo. FASEB J 25(6):2022–2030
Suvà M-L, Riggi N, Stehle J-C, Baumer K, Tercier S, Joseph J-M, Suvà D, Clément V, Provero P, Cironi L, Osterheld M-C, Guillou L, Stamenkovic I (2009) Identification of cancer stem cells in Ewing’s sarcoma. Cancer Res 69(5):1776–1781
Walter D, Satheesha S, Albrecht P, Bornhauser BC, D’Alessandro V, Oesch SM, Rehrauer H, Leuschner I, Koscielniak E, Gengler C, Moch H, Bernasconi M, Niggli FK, Schäfer BW, CWS Study Group (2011) CD133 positive embryonal rhabdomyosarcoma stem-like cell population is enriched in rhabdospheres. PLoS One 6(5):e19506
Levings PP, McGarry SV, Currie TP, Nickerson DM, McClellan S, Ghivizzani SC, Steindler DA, Gibbs CP (2009) Expression of an exogenous human Oct-4 promoter identifies tumor-initiating cells in osteosarcoma. Cancer Res 69(14):5648–5655
Saini V, Hose CD, Monks A, Nagashima K, Han B, Newton DL, Millione A, Shah J, Hollingshead MG, Hite KM, Burkett MW, Delosh RM, Silvers TE, Scudiero DA, Shoemaker RH (2012) Identification of CBX3 and ABCA5 as putative biomarkers for tumor stem cells in osteosarcoma. PLoS One 7(8):e41401
Yang J, Ren Z, Du X, Hao M, Zhou W (2014) The role of mesenchymal stem/progenitor cells in sarcoma: update and dispute. Stem Cell Investig 1:18
Zhang L, Wang C (2007) Identification of a new class of PAX3-FKHR target promoters: a role of the Pax3 paired box DNA binding domain. Oncogene 26(11):1595–1605
Gibbs CP, Kukekov VG, Reith JD, Tchigrinova O, Suslov ON, Scott EW, Ghivizzani SC, Ignatova TN, Steindler DA (2005) Stem-like cells in bone sarcomas: implications for tumorigenesis. Neoplasia 7(11):967–976
Wei Q, Tang YJ, Voisin V, Sato S, Hirata M, Whetstone H, Han I, Ailles L, Bader GD, Wunder J, Alman BA (2015) Identification of CD146 as a marker enriched for tumor-propagating capacity reveals targetable pathways in primary human sarcoma. Oncotarget 6(37):40,283–40,294
Trucco M, Loeb D (2012) Sarcoma stem cells: do we know what we are looking for? Sarcoma 2012:291705
Wang M-Y, Nestvold J, Rekdal Ø, Kvalheim G, Fodstad Ø (2017) A novel rat fibrosarcoma cell line from transformed bone marrow-derived mesenchymal stem cells with maintained in vitro and in vivo stemness properties. Exp Cell Res 352(2):218–224
Fujiwara T, Kawai A, Yoshida A, Ozaki T, Ochiya T (2013) Cancer stem cells of sarcoma. In: Role of cancer stem cells in cancer biology and therapy. CRC Press, Boca Raton, FL, pp 23–78
Hatina J, Fernandes MI, Hoffmann MJ, Zeimet AG (2013) Cancer stem cells – basic biological properties and experimental approaches. Encyclopedia of Life Sciences. Chichester, John Wiley & Sons. https://doi.org/10.1002/9780470015902.a0021164.pub2
Krause U, Ryan DM, Clough BH, Gregory CA (2014) An unexpected role for a Wnt-inhibitor: Dickkopf-1 triggers a novel cancer survival mechanism through modulation of aldehyde-dehydrogenase-1 activity. Cell Death Dis 5:e1093
Martinez-Cruzado L, Tornin J, Rodriguez A, Santos L, Allonca E, Fernandez-Garcia MT, Astudillo A, Garcia-Pedrero JM, Rodriguez R (2017) Trabectedin and campthotecin synergistically eliminate cancer stem cells in cell-of-origin sarcoma models. Neoplasia 19(6):460–470
Stacchiotti S, Van Tine BA (2017) Synovial sarcoma: current concepts and future perspectives. J Clin Oncol 36(2):180–187
Naka N, Takenaka S, Araki N, Miwa T, Hashimoto N, Yoshioka K, Joyama S, Hamada K-I, Tsukamoto Y, Tomita Y, Ueda T, Yoshikawa H, Itoh K (2010) Synovial sarcoma is a stem cell malignancy. Stem Cells 28(7):1119–1131
Saito T, Nagai M, Ladanyi M (2006) SYT-SSX1 and SYT-SSX2 interfere with repression of E-cadherin by snail and slug: a potential mechanism for aberrant mesenchymal to epithelial transition in human synovial sarcoma. Cancer Res 66(14):6919–6927
Eid JE, Garcia CB (2015) Reprogramming of mesenchymal stem cells by oncogenes. Semin Cancer Biol 32:18–31
Zöllner SK, Rössig C, Toretsky JA (2015) Synovial sarcoma is a gateway to the role of chromatin remodeling in cancer. Cancer Metastasis Rev 34(3):417–428
Jedlicka P (2010) Ewing Sarcoma, an enigmatic malignancy of likely progenitor cell origin, driven by transcription factor oncogenic fusions. Int J Clin Exp Pathol 3(4):338–347
Svoboda LK, Harris A, Bailey NJ, Schwentner R, Tomazou E, von Levetzow C, Magnuson B, Ljungman M, Kovar H, Lawlor ER (2014) Overexpression of HOX genes is prevalent in Ewing sarcoma and is associated with altered epigenetic regulation of developmental transcription programs. Epigenetics 9(12):1613–1625
Beird HC, Wu C-C, Ingram DR, Wang W-L, Alimohamed A, Gumbs C, Little L, Song X, Feig BW, Roland CL, Zhang J, Benjamin RS, Hwu P, Lazar AJ, Futreal PA, Somaiah N (2018) Genomic profiling of dedifferentiated liposarcoma compared to matched well-differentiated liposarcoma reveals higher genomic complexity and a common origin. Cold Spring Harb Mol Case Stud 4(2):pii:a002386
Mayr C, Hemann MT, Bartel DP (2007) Disrupting the pairing between let-7 and Hmga2 enhances oncogenic transformation. Science 315(5818):1576–1579
Henriksen J, Stabell M, Meza-Zepeda LA, Lauvrak SA, Kassem M, Myklebost O (2010) Identification of target genes for wild type and truncated HMGA2 in mesenchymal stem-like cells. BMC Cancer 10:329
Taylor BS, DeCarolis PL, Angeles CV, Brenet F, Schultz N, Antonescu CR, Scandura JM, Sander C, Viale AJ, Socci ND, Singer S (2011b) Frequent alterations and epigenetic silencing of differentiation pathway genes in structurally rearranged liposarcomas. Cancer Discov 1(7):587–597
Guan M, Wu X, Chu P, Chow WA (2017) Fatty acid synthase reprograms the epigenome in uterine leiomyosarcomas. PLoS One 12(6):e0179692
Di Pompo G, Salerno M, Rotili D, Valente S, Zwergel C, Avnet S, Lattanzi G, Baldini N, Mai A (2015) Novel histone deacetylase inhibitors induce growth arrest, apoptosis, and differentiation in sarcoma cancer stem cells. J Med Chem 58(9):4073–4079
Abarrategi A, Tornin J, Martinez-Cruzado L, Hamilton A, Martinez-Campos E, Rodrigo JP, González MV, Baldini N, Garcia-Castro J, Rodriguez R (2016) Osteosarcoma: cells-of-origin, cancer stem cells, and targeted therapies. Stem Cells Int 2016:3631764
Alfranca A, Martinez-Cruzado L, Tornin J, Abarrategi A, Amaral T, de Alava E, Menendez P, Garcia-Castro J, Rodriguez R (2015) Bone microenvironment signals in osteosarcoma development. Cell Mol Life Sci 72(16):3097–3113
Plaks V, Kong N, Werb Z (2015) The cancer stem cell niche: how essential is the niche in regulating stemness of tumor cells? Cell Stem Cell 16(3):225–238
Rubio R, Abarrategi A, Garcia-Castro J, Martinez-Cruzado L, Suarez C, Tornin J, Santos L, Astudillo A, Colmenero I, Mulero F, Rosu-Myles M, Menendez P, Rodriguez R (2014) Bone environment is essential for osteosarcoma development from transformed mesenchymal stem cells. Stem Cells 32(5):1136–1148
Heymann M-F, Lézot F, Heymann D (2017) The contribution of immune infiltrates and the local microenvironment in the pathogenesis of osteosarcoma. Cell Immunol (17):30,189–30,182
Basu-Roy U, Seo E, Ramanathapuram L, Rapp TB, Perry JA, Orkin SH, Mansukhani A, Basilico C (2012) Sox2 maintains self renewal of tumor-initiating cells in osteosarcomas. Oncogene 31(18):2270–2282
Zhang H, Wu H, Zheng J, Yu P, Xu L, Jiang P, Gao J, Wang H, Zhang Y (2013) Transforming growth factor β1 signal is crucial for dedifferentiation of cancer cells to cancer stem cells in osteosarcoma. Stem Cells 31(3):433–446
Basu-Roy U, Bayin NS, Rattanakorn K, Han E, Placantonakis DG, Mansukhani A, Basilico C (2015) Sox2 antagonizes the Hippo pathway to maintain stemness in cancer cells. Nat Commun 6:6411
Wang L, Park P, Zhang H, La Marca F, Claeson A, Valdivia J, Lin C-Y (2011) BMP-2 inhibits the tumorigenicity of cancer stem cells in human osteosarcoma OS99-1 cell line. Cancer Biol Ther 11(5):457–463
Avnet S, Cortini M (2016) Role of pericellular matrix in the regulation of cancer stemness. Stem Cell Rev 12(4):464–475
Avnet S, Di Pompo G, Chano T, Errani C, Ibrahim-Hashim A, Gillies RJ, Donati DM, Baldini N (2017) Cancer-associated mesenchymal stroma fosters the stemness of osteosarcoma cells in response to intratumoral acidosis via NF-κB activation. Int J Cancer 140(6):1331–1345
Tu B, Zhu J, Liu S, Wang L, Fan Q, Hao Y, Fan C, Tang T-T (2016) Mesenchymal stem cells promote osteosarcoma cell survival and drug resistance through activation of STAT3. Oncotarget 7(30):48296–48308
Kuhn NZ, Tuan RS (2010) Regulation of stemness and stem cell niche of mesenchymal stem cells: implications in tumorigenesis and metastasis. J Cell Physiol 222(2):268–277
Zeng W, Wan R, Zheng Y, Singh SR, Wei Y (2011) Hypoxia, stem cells and bone tumor. Cancer Lett 313(2):129–136
Cathomas R, Rothermundt C, Bode B, Fuchs B, von Moos R, Schwitter M (2015) RANK ligand blockade with denosumab in combination with sorafenib in chemorefractory osteosarcoma: a possible step forward? Oncology 88(4):257–260
Moriceau G, Ory B, Gobin B, Verrecchia F, Gouin F, Blanchard F, Redini F, Heymann D (2010) Therapeutic approach of primary bone tumours by bisphosphonates. Curr Pharm Des 16(27):2981–2987
Sampson VB, Gorlick R, Kamara D, Anders Kolb E (2013) A review of targeted therapies evaluated by the pediatric preclinical testing program for osteosarcoma. Front Oncol 3:132
Rainusso N, Brawley VS, Ghazi A, Hicks MJ, Gottschalk S, Rosen JM, Ahmed N (2012) Immunotherapy targeting HER2 with genetically modified T cells eliminates tumor-initiating cells in osteosarcoma. Cancer Gene Ther 19(3):212–217
Tarek N, Lee DA (2014) Natural killer cells for osteosarcoma. Adv Exp Med Biol 804:341–353
Acknowledgments
The original studies cited are supported by the Czech Science Foundation project No. 17-17636S (J.H., M.K., K.H., J.K., J.S., O.S.); by the project CZ.02.1.01/0.0/0.0/16_019/0000787 provided by the European Regional Development Fund and the Ministry of Education, Youth and Sports of the Czech Republic (M.K. and J.K); by Charles University in Prague Specific Student Research Projects No. 260394/2017 and No. 260393/2017 (J.H., M.K., K.H, M.P., J.K.); and by Spanish Plan Nacional de I+D+I 2013-2016: ISCIII (CPII16/00049), CIBERONC (CB16/12/00390), and MINECO/FEDER (SAF2016-75286-R) (R.R.).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Hatina, J. et al. (2019). Sarcoma Stem Cell Heterogeneity. In: Birbrair, A. (eds) Stem Cells Heterogeneity - Novel Concepts. Advances in Experimental Medicine and Biology, vol 1123. Springer, Cham. https://doi.org/10.1007/978-3-030-11096-3_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-11096-3_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-11095-6
Online ISBN: 978-3-030-11096-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)