
Abstract
Ageing of the population will result in significant social changes in the years to come. A way to cope with social impacts produced by growing seniority is to design and provide services for elderly people to improve their quality of life by means of ICT solutions, both fixed and mobile (wearable and not), pervasive and with low invasiveness according to Ambient Intelligence (AmI) paradigms. The Active Ageing At Home project strived to realize a Personal Guidance System to guide people’s behavior and habits for their benefit, their well-being and to stimulate preventive actions. The goal is to allow individuals to have an active role in managing their own health and in maintaining good health conditions by showing them their “virtual model”, which reflects their specific characteristics in terms of personal profile, risk factors, tastes and personal preferences, eating habits, level of physical activity, sleep/wake rhythm and as such improves their self-awareness in the direction of healthy and wellbeing-favorable behaviors.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


1 Introduction
The constant increase of life expectancy and the consequent aging phenomenon in the next 20 years will inevitably produce deep social changes that lead to the need of innovative services for elderly people, focused to maintain independence, autonomy and, in general, improve their wellbeing. The Active Ageing At Home project (AA@H) meant to realize an innovative and integrated system to help improve the quality of life of the elderly, fostering their autonomy to live in their homes, and to provide and manage for themselves in order to keep good health.
The project was developed in the context of Ambient Assisted Living (AAL) that promotes the use of innovative technologies to allow older people to keep living in their own houses, rather than hospices or nursing homes. For this purpose, AAL specifically designs intervention on homes to adapt them to different situations (health or disease), enhancing older people’s autonomy, easing daily activities and guaranteeing safety conditions.
Care of the elderly and promotion of technology in gerontology environments requires a deep knowledge of older people’s need and expectations. AA@H realizes personalized services built upon a comprehensive ICT platform, which can guide people to carry out a healthy life style and to maintain their level of autonomy in different dimensions (security, mobility, memory, and sociality). The goal is to allow individuals to have an active role in managing their own health and in maintaining good health conditions.
The technologies proposed in AA@H are largely based on heterogeneous, distributed and connected smart-sensors, smart-actuators and smart-devices integrated into a scalable technological platform, which is context-aware and enables services to assist and monitor users in their own life environment. The platform is meant as an extension of other domotic solutions inside the home environment and is integrable with open platforms in AAL realm, such as the ones promoted by the UniversAAL project, and by the coordinated European Union EIP-AHA (European Innovation Partnership on Active and Healthy Ageing) action.
ICT solutions with a high technological impact were developed with the concept in mind to extend the time in which elderly people can live independently in their homes. AA@H promoted the porting of Ambient Intelligence (AmI) technologies to the new sector of the “Silver economy”, helping make the involved technologies pervasive to seniors by means of the identification and the removal of the technology barriers that typically prevent them to benefit from ICT tools [1]. The AmI ICT platform designed for AA@H infers knowledge by integrating automatic tools for reasoning, knowledge discovery, ontologies acting also as a decisions support system in the contexts of monitoring, security, assistance and inclusion. The ICT platform upon which AA@H builds its services, is based on a cloud infrastructure in order to organize the collected data in a remote system assuring reliability, scalability, security, performance and independence from the device or application used to access to the data. Special attention is devoted to managing privacy and sensitive information.
The proposed solutions are not aimed at substituting the capabilities and experience of the caregivers, but on the contrary, they provide technological support that allows reducing the cognitive load and stressing on the people, leading to a reduction of the general cost of the assistance and an increase of the quality of service. The collected data are processed by means of modules that are capable to extract key information required by different stakeholders (relatives, caregivers, service providers) identifying automatically critical situations and allowing an efficient monitoring of the well-being level of the user. The solutions and services were also designed using a user centered methodology allowing to realize innovative products according to the specificity and habits of the users [2]:
-
a.
solutions aiming at increasing the sense of safety and self-reliance at home: intrusion detection systems, monitoring and indoor localization using active and passive radiofrequency vision systems;
-
b.
multi-sensing solutions for the prevention/detection of critical or potentially interesting events related both to the person (falls, unconsciousness, difficulty in walking, …) and the environment (flooding, presence of gas and smoke, temperature, …);
-
c.
multi-sensing solutions for primary and secondary prevention of cognitive and affective deterioration by means of the analysis of behavioral patterns targeted to “Activities of Daily Living” (ADL), levels of sedentary, social life, habits. The proposed technologies contribute to keep the elderly autonomous and confident but also prevent degradation of mental, physical and cognitive conditions, detecting potential risk situations at their early stages [3];
-
d.
systems for the evaluation of correct eating behaviors in case pathologies are present and the maintenance of a balanced diet is required;
-
e.
solutions of Personal Fitness for the execution of regular physical exercises with gesture recognition and adaptation to the user’s profile;
-
f.
solutions enabling the socialization using ad hoc social networks developed specifically for the interests and possibilities of elderly people. Such network provide edutainment service as for example: reading books, newspaper or magazines related to the interests of the user; joining discussion groups on specific arguments; sharing images and stories; keeping in contact with family and friends; participate to and organize events by inviting also other people; play online games alone or within a group;
-
g.
solutions of Interaction Design specifically realized for elderly people designed with a user-centered perspective which enhances familiarity, pleasantness and positive impact on everyday life.
The main outcome of AA@H was the development of a Personal Guidance System to orient people’s behavior and habits towards their benefit and their well-being. To this extent, AA@H delivers a Virtual Model system of the individual. The Virtual Model (VM) analyzes behavioral data and detects patterns through fixed and wearable intelligent microsystems, employed and interconnected among them, and through inference logic. The VM also allows the evolution of the monitoring model, from a static profile to individual specificity, taking the overall individual’s wellbeing into account, including psychological and relational aspects, not only physical. Through interaction with users, the system fosters their awareness and participation in managing their own well-being, stimulating change in unhealthy habits in favor of a better life style that can help keep them healthier and prevent or minimize risks of disease. In this way individuals play an active role in managing their own health and in maintaining good health conditions.
2 Virtual Model
The VM is the main contribution and the qualifying element of AA@H. It reflects important characteristics that are specific of each person (e.g. personal profile, risk factors, heart functionality assessment, harmful behaviors, tastes and personal preferences, eating habits, level of physical activity, sleep/wake rhythm, etc.) and can provide personalized indications by interacting with the individuals to make them more conscious of unhealthy behaviors. An intelligent environment was devised to:
-
a.
monitor indicators for health status, physical and intellectual well-being of the individual;
-
b.
act as personal guidance, evaluate the individual’s evolution in time and promote correct life styles and behaviors;
-
c.
prevent and detect critical situations or risk (e.g. smoke in the room or fall), avoiding false alarms but promptly intervening in case of need;
-
d.
promote adequate physical activity;
-
e.
promote active socialization and participation in community life.
eResult delivered its OMNIACARE platform in the AA@H Project, mainly to build the software part of the VM. OMNIACARE is a software product endowed with very broad characteristics of configurability, scalability and robustness. The Virtual Model module is realized extending the PHRS (Personal Health Record System) functionalities in OMNIACARE with behavioral analysis functions. The model is built to be self-adaptive and self-calibrating to adapt to variations in time. The system also analyzes a huge quantity of structured and non-structured data to infer high-level information as posture, behavioral patterns and their interaction with the VM itself.
Given the complexity of the problem, a structured approach is adopted to build the Virtual Model, through a hierarchy of properly coordinated software modules. Among these, a part of activities specifically concerns the development of virtual sensors, based on the techniques of analysis of the raw data of the lowest level, and addressed to the recognition of behavioral changes. These data, mainly coming from the environment in which the person lives, are more difficult to fit directly into a virtual individual model, and must first be processed by a module based on inference techniques, fusion and analysis of large amounts of heterogeneous data, which provides summary information, plus more expressive indexes, consistent with the individual model. The identified areas, for which the collected information is computed and made available for the creation of the VM, are:
-
1.
Food
-
2.
Water
-
3.
Weight
-
4.
Stress
-
5.
Mobility
-
6.
Socialization
-
7.
Sleep/wake cycle
-
8.
Posture
-
9.
Heart and breath parameters.
The VM allows the definition of the user’s standard, i.e. profiles the user in such a way that ranges are defined in each area within which he/she must be maintained in order to preserve a conservative situation (e.g., keep the current weight). The user, based on the default profile, is then stimulated to improve his vital and wellness figures by setting objectives. The information made available by the data management module, allows to define encouragements, which are shown as notifications (e.g.: “You only walked only 1 km today, you should move a little more”). To this purpose, an objective definition module is provided. This module is intended as an extension of the incentive functionality, since it provides different targets compared to the previously mentioned standard. The module allows the definition of consistent objectives with possible pathologies in the user, or with other particular conditions. The configuration of the objectives can take place by a tutor or physician.
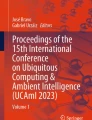
The architecture of the VM is made of a main DB which also hosts the application layer of OMNIACARE, and of different elements all around it. The end user works with a mobile device (smartphone or tablet) from where to use the AA@H applications. In addition, the mobile device in some cases acts as a gateway for associated sensors (e.g. the Pulse), or at least as an input system for certain parameters (food, water, etc.). All of this information is sent to the central server through a layer of services (RESTful web services) and feeds the main DB (Fig. 1).

Virtual model architecture
A middleware software layer is realized which creates a common interface for all data sources, and thereby allows:
-
data collection
-
data encoding/synthesis
-
data provision.
In this way, it is possible to show the measured data in a comprehensive manner and make it available to the physician or caregiver. Similarly, information (or a subset) is accessible to the user, on the OMNIACARE web platform or by an application for mobile devices. Two separate software modules, the Data Aggregator and Statistical Analysis, take care to make the information accessible from the OMNIACARE platform.
The task of the Data Aggregator module is to create an aggregation of data on which to perform the research, collection and synthesis of data in the form of synthetic information, in order to achieve the specific business intelligence solution that shows the user summary information and significant state. The Data Aggregator works on a large number of samples, numerical or otherwise, from heterogeneous sources (applications, services, sensors), and its task is to produce the valuation indexes in the defined areas (sleep/wake, food, water, etc.), which are numeric. Exploiting the numerical representation of the parameters, it is possible to dynamically add other indicators within the system. The Data Aggregator works on the central database, from where it draws the raw data on which to apply the algorithms defined therein. Then it inserts into specific tables the results of calculations that represent the summary information. The identified procedures for the execution of the process are:
-
1.
Data aggregation operations are triggered by appropriate insertions of measurements, or blocks of received data. (Observer–Observable logic);
-
2.
Operations are automatically executed with predetermined frequency: data is processed periodically, generating the corresponding synthetic data.
Depending on the collected information, one of the two modalities or both can be applied.
The task of the Statistical Analysis module is to analyze aggregate data acquired from the outside and correlate it with the user profile, i.e. it works on aggregated data generated by the Data Aggregation module to perform a statistical analysis, comparing the available information generated by the Data Aggregator module with profile information of the user. The Statistical Analysis module provides all information to be displayed directly in the OMNIACARE web platform user interface (UI). It is invoked whenever it is necessary to refresh the UI, or when the client system (for example, a smartphone) needs to receive summary information representing the user’s status. A caching mechanism is used to reduce the number of computations of the Statistical Analysis module, triggering them only in the cases where it is necessary to refresh the UI; in particular when the inner algorithms cannot be quickly executed.
Figure 2 that illustrates the Virtual Model control flow is shown.

Virtual model control flow
The dashed arrow between the Sensors block and the Data Aggregator block shows the ability to pass data directly to the Data Aggregator module, performing a sort of pre-processing of the information, in the cases when this operation is feasible a priori. This is possible whenever the specific aggregation operation is independent from other data and thus computation can be made starting from the single sample received, or from the block of samples received. If the collected data need to be correlated with other information, sensor data will be stored in the database first. All information gathered, both in terms of raw data and aggregate data, are processed by an additional module (“Critical Condition Detection”) that takes care of detecting a series of pre-configured critical conditions. Starting from the aggregated data, the information is processed in a subsequent step by the Statistical Analysis module, which relates the aggregated information with the information that constitutes the user’s profile. The results thus obtained are shown in appropriate interfaces for an easy display of the user’s progress. As can be seen from the diagram, the social media information are handled by a separate Social Data Analysis module, that pre-filters the information acquired by the social section, then provides them to the Statistic Analysis module to be processed by the algorithms defined therein.
In order to support the incentive functionality, substantially it is necessary to evaluate the deviations between the information synthesized by the Statistical Analysis module, and the numerical information relating to the levels defined in the user profile. This mechanism is integrated in the Statistical Analysis module. Notifications depend on the standards defined for the patient. If a threshold is exceeded, a notification is generated and forwarded to the user (client app). Some limitations exists, to make sure that notifications are not repeated or too frequent, thus disturbing the user. It is possible to configure the type of notification for each parameter observed. One-time notifications are available, meaning they will be sent only once to the client. Also, recurring notifications are implemented, dependent from the user reaction (e.g. “every 2 h, until the user responds”, where the answer is also generally indicative of a behavior of the user). This model also determines the priority level. For example, the exceeding of a threshold of a vital parameter is considered as a high priority. At the same time, tolerances are defined for the various types of synthetic observed parameters, expressed in percentage terms. The notification algorithm considers these percentages, avoiding trigger notifications in case there is not a significant deviation with respect to the defined standard.
As concerns the user interface, the visual representation is configurable. For each synthetic parameter it is possible to specify the appropriate indicator from a set of possible widgets available. Among such widgets are:
-
1.
Progress bar/gauge: a horizontal or semi-circular bar that shows the parameter progress in percentage;
-
2.
Pie chart: data is distributed in slices, proportional to the percentage;
-
3.
Histogram: vertical rectangles relating to a specific parameter progress;
-
4.
Semaphore: three light indicator for multiple states evaluation (Fig. 3).
Fig. 3 
Virtual model dashboard widget example

Widgets combined together give form to configurable dashboards, adapted to the user or caregivers’ needs, which constitute the visual output of the VM.
3 An Example of Virtual Model Usage
In the AA@H project context, the two partners eResult and STMicroelectronics worked alongside to develop important parts of the overall system.
One of the contributions to the project by STMicroelectronics was directed to health parameter monitoring in the individual. The effort was to detect a comprehensive set of information in a non-intrusive way that could result acceptable to the senior. For this purpose, a wearable device was employed. The vital parameter detection device used was MR&D’s Pulse Sensor, based on STMicroelectronics BodyGateway’s technology™ chipset, CE certified. It is a wearable, battery operated device intended for use as a part of a multiparameter analysis system. It uses a sensorized component adhesive (plaster), placed on the body of the assisted person. It can record symptomatic and asymptomatic events and is suitable for ambulatory monitoring of non-lethal cardiac arrhythmias. The Pulse Sensor is under the form of a plastic container, round-shaped, measuring 59 mm × 50 mm × 16 mm, with four electrodes on the back, three indicator LEDs and an operation button on the front.
The device permits to record heart rate, respiratory rate and, through an accelerometer, the level of activity of the person, providing the management system of continuous or periodic messages of information to/from the server according to specific settings defined by the medical staff. The raw data acquired and recorded by the Pulse sensor are combined with a number of embedded algorithms, allowing to obtain more information and more reliable, respect to the single signal. The algorithms can also be adapted to the single patient, adjusting the relevant parameters. When the physiological data exceed the limits set in the system, a notification is sent out, and the recipient receives the raw signals for that specific event.
Several types of records are gathered from the device:
-
5-min lasting ECG curve once every hour;
-
5 min lasting R–R Interval measurement once every hour;
-
breath frequency during the day;
-
heart rate during the day;
-
activity level during the day.
Data is collected from the device and sent to eResult’s OMNIACARE cloud for computing and displaying in the VM dashboard. OMNIACARE computes data from the Pulse using a norming algorithm and shows ECG curves in standard mm-chart diagrams and all of the other non-ECG parameters as punctual graphs or trend diagrams (Fig. 4).

VM heart parameter plotting widget
OMNIACARE offers a comprehensive list of comparative charts, including ECG curves on equivalent grid graph paper, where the x axis is scaled on 1 mm = 40 ms (25 mm/s). The VM dashboard is accessible via any Internet connection, using the most common browsers (Internet Explorer, Mozilla Firefox, Google Chrome, Opera). The physician, with appropriate credentials and permissions, can access information about his patients anywhere and prepare comparative analyses, based on the curves of recorded parameters. This allows the evaluation of chronic disease evolution, with particular regard to the patient’s response to drug therapy, in order to adapt the type and dosage of medication to the situation of the individual patient, based on objective factors and thus improving the quality of care.
The Pulse Sensor proves extremely reliable in the vital parameters detection. Results of the experimentation demonstrates that the device, coupled with OMNIACARE and VM, permits not only to monitor the normal parameters (ECG, respiratory rate or activity level) but also to assess the daily behavior of the neurovegetative cardiovascular pattern related to activity level and respiratory rate [4, 5].
The overall system permits to monitor not only the normal parameters (ECG, respiratory rate or activity level) but also to have a daily behavior assessment of the neurovegetative cardiovascular pattern related to activity level and respiratory rate. The Heart widget implemented on the VM can help the physician and the caregiver in the control of particular patients. In fact, data are processed online to determine several physiological indexes (Heart Rate/HR and Heart Rate Variability/HRV, Respiration Rate, Activity Level and Body Posture). From the VM it is possible for medical staff to measure the ECG parameters, especially the impulse formation and conduction, very important in patients under therapy with particular drugs. As an example the pictures below, drawn from the system, show a patient who represent various neurovegetative behaviors in daily routine, plotting the activity level, the HR and the behavior of the principal indexes of HRV, expression of the sympathetic and parasympathetic activity during a day, analyzed by means of linear and non linear analysis in different patients (Fig. 5).

Graphs of a patient with pseudo normal neurovegetative assessment
The device’s wireless connection and the VM reachability from any Internet browser allow various device application and several monitoring arrangements ranging from real-time monitoring to long-term recording of biological signals. Implementation of this virtual model capability may facilitate both accessibility and availability of personalized monitor and therapy. Further studies would validate it in the clinical and healthcare environment.
4 Discussion
Among the other objectives, the AA@H project proposal meant to demonstrate the considerable potential of smart sensor nodes networks in devices based on low power and low cost, which allows performance and new features such as intelligent vision or the sensing of human physiological parameters, compared to current systems made of bulky and high cost sensors. This project, therefore, acted as a forerunner of a possible market offer for monitoring devices and systems, and for systems endowed with algorithms specially developed for the extraction of the information of interest from the data supplied by the sensors.
STMicroelectronics made a platform with advanced features and that provides ability to aggregate complex functions. The dedicated hardware and firmware by STMicroelectronics and the software components designed and realized by eResult, allowed the possibility to implement the functionality required by the application scenarios defined for the project.
The project developed new knowledge about architectures of sensor networks and the development of sensing hardware/software capabilities. The network architecture used in AA@H hides the heterogeneity of the underlying technologies of communication and is robust enough to optimally manage a large number of connected devices even in case of failure of individual nodes.
From a system perspective, it is expected that the technological trend will result in the development of new devices in the field of assistive technologies and further advancements in the next years, such as:
-
the availability of Internet in each device (Internet of Things), that will allow the integration of system for the internal and external support to the person (at home and outside);
-
the concept of web services and web of the objects, that will guarantee the integration of systems and service with an added value, creating new opportunities for a higher number of support services;
-
the realization of technologies and RFID devices, that will evolve into a Wireless Sensor Network;
-
the development of nanotechnologies and sensors systems, that will allow their integration in common materials, as well as the opportunity of wearing them;
-
the increase in networking capacity, that will favor the development of new services devoted to video and multimedia communication within the home and outside;
-
a particular attention for context–aware data, services and application. Assistive technologies in the future will privilege the user’s perception of the presence, location, devices, date, time;
-
the growing potential of robotics, that will favor the development of advanced systems, able to move automatically for giving cures and assistance;
-
the improvement in automated analysis of the user health and cognitive state;
-
the establishment of new methods for the integration of system devoted to entertainment and communication, that will develop new contexts for improving the relationships among older people.
Those advancements will require proper integration and communication, for which the AA@H project paved the way for the participating partners to keep working with, and gain a competitive advantage.
5 Conclusions
From a software integration perspective, the developed Virtual Model by which elderly can keep the pace with a wellness and behavioral improvement program set by coaches and physicians helps to raise the age until which the elderly person can live independently in their own homes. This helps reduce the rise in social costs due to rise in the average age of the population.
On such basis, it can be affirmed that the AA@H project promoted a gradual and acceptable approach to the technologies for the older people, in order to win over their natural mistrust and indifference in face of something new, complex and potentially invasive such as new devices. The elderly were in fact directly involved in identifying appropriate mechanisms of interaction with simple and intuitive IT tools, in the perspective of maintaining autonomy and enrichment of their lives.
From a market perspective, the current situation in home automation is gradually coming to social optimum conditions: the expectations of potential customers is rising, because knowledge of the possibilities offered by this type of technology is high and the use of technical aids to overcome the disability is common and accepted practice. On the supply side, the market now offers solutions that properly meet requests with requirements. With such premises, and for consequences arising from the extension of life span, it is believed that the elderly sector will account for more and more importance in the overall market for home automation. Indeed, it will be one of the most solid pillars, because linked to basic and unavoidable needs of the person and not to the general economy.
The project activities and experience can therefore seen as a collective effort on one side to produce tools and advancements in technologies for the environments of life, on the other to allow the development of new expertise and market possibilities.
References
Davis, F. D. (1989). Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly, 13(3), 319–340.
Graziola, I., Pianesi, F., Zancanaro, M., & Goren-Bar, D. (2015). Dimensions of adaptivity in mobile systems: Personality and people’s attitudes. In Proceedings of the 10th International Conference on Intelligent User Interfaces (IUI ‘05).
Pistoia, M., & Casacci, P. (2015). The active ageing at home project: Building a comprehensive ICT system to improve well-being of ageing people. In Proceedings of 6th ForITAAL.
Raimondi, G., Casacci, P., Sancesario G., Scordamaglia, B., Melchiorri, G., & Pistoia, M. (2016). Telemedicine for dementia-affected patients: The AAL-ACCESS project experience. In Ambient Assisted Living Proceedings of 7th ForITAAL.
Casacci, P., & Pistoia, M. (2016). Remote circadian rhythm monitoring in alzheimer-affected people: A telehealth experience. In Proceedings of ISOCS-MINAB-ICT.
Acknowledgements
The authors gratefully acknowledge the financial support from the Italian Ministry of University and Research (MIUR) in the project “Active Ageing at Home” (CTN01_00128_297061, Area TAV—Tecnologie per gli Ambienti di Vita). This work draws from previous papers, on courtesy from Marco Pistoia, Paolo Casacci, Gianfranco Raimondi, Giuseppe Sancesario, Beatrice Scordamaglia and Gaia Melchiorri, whom the authors thank.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this paper

Cite this paper
Pistoia, M., Parata, C., Giugni, P., Urlini, G., Loi, S., Borrelli, G. (2019). Virtual Modeling of the Elderly to Improve Health and Wellbeing Status: Experiences in the Active Ageing at Home Project. In: Casiddu, N., Porfirione, C., Monteriù, A., Cavallo, F. (eds) Ambient Assisted Living. ForItAAL 2017. Lecture Notes in Electrical Engineering, vol 540. Springer, Cham. https://doi.org/10.1007/978-3-030-04672-9_5
Download citation
DOI: https://doi.org/10.1007/978-3-030-04672-9_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-04671-2
Online ISBN: 978-3-030-04672-9
eBook Packages: EngineeringEngineering (R0)