
Abstract
Beyond the identification of the most appropriate cells and scaffold materials, translation of cardiovascular tissue engineering structures requires optimization of construct biological and mechanical properties in order to permit their long-term functionality in the native hemodynamic environment. Unfortunately, rudimentary tissue growth technologies such as plate or rotisserie culture do not lead to the generation of functional tissues, thereby limiting their usefulness. Dynamic culture systems or bioreactors with true construct mechanical conditioning capabilities thus form an essential part of the research and development pathway in cardiovascular regenerative medicine. This is because engineered tissues cultured under specific bioreactor mechanical environments enhance their biological properties such as functional stem cell differentiation to complex tissue phenotypes and also augment construct structural properties as a result of accelerated tissue formation. In the heart valve tissue engineering arena, based on at least a decade of scientific results, there is now general acceptance that bioreactor usage is a critical preclinical step. In this book chapter, we describe important considerations in bioreactor design as well as focus on the critical scientific findings in the development of de novo valvular tissues, including our own experience in this area. We subsequently detail scaffold and cell sources that have been used in conjunction with these devices and finally conclude by addressing the key challenges that still remain.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
- Tissue Engineering
- Heart valve disease
- Somatic growth
- Extracellular matrix
- Bioreactors
- Flow
- Stretch
- Flexure
- Scaffolds
- Stem cells
1 Introduction
Millions of people worldwide are suffering from valvular heart disease and the rate of incidence is expected to significantly increase in the future [1]. Current techniques for prosthetic valve replacement are reasonable in some cases but have distinct limitations in others. In particular, no robust treatment option is available for the treatment of critical congenital valve diseases in children. An inability of prosthetic valves to accommodate somatic growth and practical size limitations of current commercial valves represent specific technical challenges. The field of tissue engineered heart valves holds promise of filling this unmet need. The living, biological heart valve would function in a similar manner as native tissue with normal hemodynamic performance and minimal degeneration. To achieve this task, current consensus in the scientific community is that a bioreactor will be necessary to help create a tissue engineered valve with ideal function. In this context, the bioreactor is a device that will help to promote engineered tissue properties via the delivery of appropriate biomechanical and biochemical stimuli during tissue culture. There are many variables to consider when designing a bioreactor to condition a tissue engineered heart valve (TEHV). From a biomimetic standpoint, this design needs to consider the hemodynamic environment of the native, healthy heart valve. In addition, the type of scaffold material, the choice of cell source(s), and the duration of culture will affect the de novo tissue properties.
2 Bioreactors
2.1 Design
The basic components of bioreactors as described by Berry et al. to design engineered heart valves are [2]:
-
1.
A driving force or pump for fluid movement
Typical pumps include pneumatically controlled diaphragms, reciprocating pistons, peristaltic pumps, or meshing gears teeth. The pumps are typically controlled by a computer system as it is desirable to have complete control over the fluid movement.
-
2.
A reservoir (for cell culture media)
Culture media should support the growth of the cell type and can contain a variety of different growth factors. Minimizing the overall volume of media with help to reduce costs.
-
3.
A test section containing the heart valve
Location of the test sections can disturb or change the flow patterns. Many groups are using a spiral-bound section to allow for minimal flow disturbances.
-
4.
A fluid capacitance to store and release energy at every pump cycle
As system pressure builds due to forward or reverse fluid flow, a fluid capacitance can help to release this energy.
-
5.
A resistance element
The overall system pressure can be controlled with the resistance element.
-
6.
Allows for Gas exchange
Gas exchange by bubbling of the media or diffusion at the reservoir surface can keep the culture media oxygenated to support cell growth.
2.1.1 Static Designs
A simple example of a static bioreactor is a petri dish or culture flask. These typically include a non-stirred environment or may include packed-bed reactors with porous substrate which allows for culture perfusion [3]. Even though rotisserie culture systems involve rotational movement of tubes containing the engineered tissues, they are still considered static in the context of the negligible mechanical stresses that are imparted onto the developing tissue constructs. Seliktar et al. [4] described an initial static bioreactor that was subsequently modified to permit dynamic mechanical conditioning of tissue engineered constructs composed of cells in a scaffold. The response to this conditioning included increased contraction and mechanical strength as compared to traditional static cultures.
2.1.2 Dynamic Designs
Dynamic bioreactors typically include pulse duplicators and devices for organ tissue culture. This environment allows for the maturation and physical conditioning of engineered tissue. Gandaglia et al. [5] provided a description for a dynamic bioreactor that is similar to the defined components described by Berry et al. [2] above. The dynamic bioreactor for engineered heart valves consist of the following components: (1) a ventricle, driven by a motor (mechanical, pneumatic, or electric) which creates specific pressure and flow patterns, (2) a system to adjust resistance, (3) a chamber to shelter the heart valve, (4) a hydraulic circuit for the different unit joint, (5) probes and sensors for measuring and adjusting flow and pressure, temperature, pH, pO2, pCO2, and metabolite concentration, and (6) hardware and software to control the system.
Berry et al. [2] made a schematic of the typical pulsatile bioreactor designs. Small differences in design can lead to varied environments and therefore major differences in the tissue engineered heart valve properties (Fig. 1).

Schematic diagrams of five contemporary heart valve bioreactor designs. These designs have been reported to deliver physiologic pulsatile flow and pressure while maintaining the proper temperature, gas exchange, and sterility [2]
2.2 Mechanical Environment
The mechanical environment for normal heart valve tissue can be broadly described as a combination of cyclic stretch, forward and oscillating blood-induced shear stresses as well as cyclic flexure. The hemodynamics is time-dependent and is based on heart function over the cardiac cycle as well as the opening and closing events of the valve. Therefore, designing engineered valves that can withstand this environment is challenging. Many investigators have focused on creating specialized bioreactors that divide the environment into components of stretch, flex or flow [2].
2.2.1 Stretch
The commercially available Flexcell system (Flexcell International, Hillsborough, USA) provides an environment for studying cyclic stretch. The Flexcell System is a computerized, pressure-operated instrument that applies a defined controlled, static or variable duration cyclic tension, to cells growing in vitro. This system utilizes regulated vacuum pressure to deform flexible bottomed culture plates. Utilizing the Flexcell system, Carrion et al. [6] demonstrated that bicuspid aortic valve (BAV) leaflets experience increased biomechanical strain as compared to tricuspid aortic valves in response to mechanical stretch. Human aortic valve interstitial cells were exposed to cyclic stretch of 14% at 1 Hz or static condition, the control condition, for 24 h. They demonstrated the molecular pathogenesis involved in the calcification of BAVs especially when exposed to mechanical stretch. Cyclic stretch has been shown to affect cytoskeletal organization as it is sensed by cardiomyocytes. The stretch signal sensing is mediated via focal adhesion kinase and leads to intracellular reorganization and orientation. The oblique orientation of the cell with regard to the direction of stretch may define a directed force vector which could allow the cell to orientate [7]. In one study, human adipose stem cells exposed to mechanical stretch at 12% at 1 Hz frequency for up to 96 h did not differentiate to cardiovascular cell phenotypes [8]. The ability of cells to secrete an array of cytokines, however, remained unchanged by mechanical stretch [8]. In another study, activating transcription factor 3 which is known to have a cardioprotective activity was shown to be activated by mechanical stretch [9].
Ku et al. [10] demonstrated that collagen synthesis by valve interstitial cells as well as mesenchymal stem cells is a function of both the degree and duration of stretch. Depending on the stretching profile that is applied, the properties could be varied to make an appropriate tissue engineered heart valve.
Syedain and Tranquillo [11] considered a controlled cyclic stretch bioreactor as opposed to pulsed flow. This led to improved tensile and compositional properties. They demonstrated that the TEHV could withstand the cyclic pressures of a pulmonary artery in the Ovine model. Another study used aortic valve interstitial cells (VIC) on a porcine aortic valve in a cyclic stretch and pressure bioreactor [12]. The leaflets were stretched at a frequency of 1.167 Hz (equivalent to 70 bpm) at 10% or 15% stretch and a cyclic pressure of either 120/80 or 140/100 mm Hg was applied. The combination of cyclic stretch and pressure was shown to help modulate the VIC phenotype.
2.2.2 Flexure
Dynamic flexure or bending effects on valve leaflets is an important variable to consider when developing TEHVs. Engelmayr et al. [13] developed a bioreactor that considered dynamic flexure. The linear actuator was used to simulate the cardiac cycle at 1 Hz (60 bpm). The scaffolds were displaced 6.35 mm with a flexure angle of 62°. They assessed unidirectional cyclic flexural properties of a nonwoven mesh of polyglycolic acid (PGA) fiber as well as a nonwoven mesh of PGA and poly l-lactic acid (PLLA). Both samples were coated with poly 4-hydroxybutyrate (P4HB). The PGA/PLLA/P4HB scaffolds that were subjected to dynamic flexure were significantly less stiff than the static controls and they developed directional anisotropy. The PGA/P4HB scaffolds showed less stiffness after dynamic flexure but did not develop directional anisotropy. These experiments indicated that dynamic flexure does produce changes in the scaffolds and that this should be considered when developing engineered heart valve tissues.
In another set of experiments, Engelmayr et al. [14] considered cell-seeded scaffolds. Ovine vascular smooth muscle cells (SMC) were seeded on PGA/PLLA scaffolds and subjected to either static conditions or unidirectional cyclic three-point flexure at a frequency of 1 Hz and a central displacement of 6.35 mm. The flexure group showed an increase in stiffness, collagen, and vimentin expression as well as more homogeneous cell distribution as compared to the static group. Similar results were obtained using scaffolds seeded with ovine bone marrow-derived mesenchymal cells (BMSCs) [15].
Mirnajafi et al. [16] designed a device to study controlled cyclic flexural loading on bioprosthetic heart valves. They were able to study layer-specific structural damage induced by cyclic flexural tensile at a frequency of 1 Hz and a central displacement of 6.35 mm and compressive stresses alone. Results indicated that rigidity was reduced after only 10 million cycles.
2.2.3 Flow
Some bioreactors focus on steady fluid flow mechanical conditioning. One system examined the effects of laminar flow (7 days exposure to ~0.066 dyn/cm2, followed by a step change to ~0.13 dyn/cm2 for an additional 7 days) on tissue induced by dialysis roller pump (500 mL/min), and nutrition flow by a perfusion pump (3 mL/h) [17]. Mahler et al. [18] considered a microfluidic bioreactor that applies oscillatory shear stresses. The system was used to study the effects of flow on the transformation of endothelial to mesenchymal cells. For the oscillatory shear experiments, a square wave flow pattern at 1 Hz was used, in which the flow was fully forward at 2, 10, or 20 dyn/cm2 for one-half of the cycle and fully reversed at −2, −10 or −20 dyn/cm2 respectively for the remainder of the cycle. In previous reports, steady shear flows led to differences in morphology and transcriptional profiles [19].
Ramaswamy et al. [20] considered design of a bioreactor that combined all three physiological characteristics of flexure, stretch, and flow in combination or independently. The device consists of four identical chambers and up to three specimens can be placed into each. Specimens can be subjected to changes in curvature, uniaxial tensile strains, and laminar flow. This system provides a useful tool to study the effect of mechanical stimuli on engineered heart valve tissue formation. The flow chamber takes a U-shaped configuration (see Fig. 2). The device is connected to a peristaltic pump and an actuator. There are four chambers each containing three samples. Samples are fixed with a pin at one end and a circular moving post on the other end. In a combination of cyclic flexure and steady flow (flex-flow) experiments for example, the moving post moves linearly using the linear actuator in the axial direction to initiate cyclic flexure. A peristaltic pump is used to create a continuous flow rate (e.g. 850 mL/min).

(a) Schematic diagram of the custom-built U-shaped bioreactor connected to a linear actuator which guides the rods that threads through samples, permitting them to bend and straighten. (b) Inset shows three samples inside the conditioning chamber that can be moved one end (ring) and is fixed on the other (pin). In the current study, the actuator was set to a 1 Hz frequency to permit cyclic flexure while the pump operated at a steady flow rate of 850 mL/min [21]
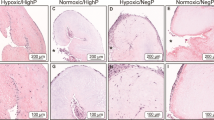
Using this bioreactor under flex-flow conditions to engineer aortic valvular tissues (1 Hz cyclic flexure and shear stress of ~4.73 dyn/cm2 on the “ventricular” side of the specimen), the Ramaswamy group successfully differentiated BMSCs simultaneously in vitro, to both endothelial cells and activated interstitial cells (i.e., alpha-smooth muscle actin positive) which distributed preferentially to the engineered tissue surfaces and interstitium, respectively, similar to native heart valve morphology [21].
In addition to the physiological ranges of flexure, flow, and stretch as well as the intrinsic biochemistry of cell culture media being used, other parameters need to also be considered when conditioning engineered heart valves. Some of these parameters include fluid pressure, temperature, and oxygen diffusion which can all be regulated to promote extracellular matrix (ECM) formation, cellular proliferation and/or cell organization. As one example, pressures in some bioreactors have been typically set to 80–120 mm Hg to simulate systemic circulation or 20–40 mm Hg for the pulmonary circulation [22].
3 Scaffolds
An important factor in the tissue engineering of heart valves is naturally the choice of scaffold material. The type of material utilized in tissue engineering can provide a natural environment which mimics the physiological conditions in the body. The native ECM acts as the backbone for cells to organize and assemble into functioning tissue. An engineered ECM must mimic this environment in order to create and maintain tissues for functional use as an implant. Most cell types utilized in bioreactors are adherent cells and therefore a cell adhesion substrate is critical for success. Cells can be embedded in a complex microenvironment that may include various growth factors and/or cytokines. Scaffolds can be made of synthetic materials or natural materials.
3.1 Synthetic
The most common synthetic materials are polyhydroxyalkanoate (PHA), PGA, poly lactic acid (PLA), and PLLA/PLA blends. One of the major concerns when developing an appropriate scaffold material is the vascularization to support proliferation of cells. Another critical component is to design the appropriate degradation time schedule. The material must allow for cell adhesion and replacement of scaffold material with the development of de novo ECM. If the scaffold degrades too early, the entire construct may fail mechanically.
Shinoka et al. [23] described a PLA scaffold seeded with fibroblasts which formed a tissue-like sheet. The sheet was then seeded with endothelial cells to form a cellular monolayer. The implantation of the seeded scaffold as leaflet replacements was completed in seven animals and all survived the procedure. There was no evidence of stenosis and histology demonstrated appropriate cellular architecture and extracellular matrix. Sodian et al. [24] have used cell-seeded PLA scaffold as well as PHA and P4HB synthetic polymers for heart valve tissue engineering purposes. After comparing PGA, PHA, and P4HB, there was significantly higher cell attachment and collagen content on PGA samples. A variety of different combinations of scaffold material have been reported; however, most have described short-term success in vitro which may not translate into long-term success with in vivo possibility [5, 25,26,27].
3.2 Natural
Natural scaffolds are typically obtained from decellularized animal valves or made from collagen and fibrin-based scaffolds. When obtaining animal valves the processing must be done carefully to preserve the structure of the ECM to allow for cell seeding. Several studies have been described where detergents do not damage the ECM matrix structure and integrity. Some studies have focused on low concentration of detergents for scaffold purification [28, 29] or crosslinking of collagen with nordihydroguaiaretic acid (NDGA) [30]. These valves have several drawbacks which include inflammation, fibrosis, degradation, damage, and possible death of patients. In addition, these designs may be cost prohibitive. Gerdisch et al. [31] have performed studies for mitral valve repair using decellularized ECM from porcine small intestinal submucosa (CorMatrix Cardiovascular Inc., Roswell, GA). A total of 19 patients underwent the surgery and this preliminary study showed promised with good valvular function and no calcification on echocardiographic images.
Another method of natural designs involves collagen and fibrinogen gels to help entrap the seeded cells. By mixing the cells in the gel, the structure contracts and the cells remove water. Unfortunately the final construct remains unpredictable due to large differences in cell density [32, 33]. Moreira et al. [34] discussed the use of a living textile reinforced mitral valve to overcome the limitation of fibrin gel.
Hong et al. [35] fabricated a novel scaffold using an electrospinning technique. Cells were seeded onto decellularized pig valves that had been coated with poly(3-hydroxybutyrate-co-4-hydroxybutyrate). The valves were placed in a pulsatile flow bioreactor and exposed to defined physical signals with a fixed frequency (1 Hz) and pressure conditions (3 L/min and 60/40 mm Hg) over a time period of either 9 or 16 days. As compared to decellularized valves without the coating, the hybrid scaffold showed a significant increase in mechanical strength. Both groups showed similar proliferation of cells and comparable cell mass.
4 Cell Types
After considering the type of scaffold and bioreactor that should be utilized, the cell source(s) to be seeded on the scaffold will need to be chosen. Most groups have focused on using adherent cell types and in many cases stem cells.
4.1 Mesenchymal Stem Cells (MSCs)
Adult stem cells are found in every part of the body and their primary role is to heal and maintain the tissue with which they reside. In addition, they have the ability to differentiate into specialized cell types. Adult stem cells can be harvested from a patient’s own tissue, such as adipose (fat) tissue, bone marrow, teeth, and more. Adult stem cells have a limited potential for growth when placed into culture and do not grow as rapidly as embryonic stem cells.
There is a population of cells known as MSCs which are different from blood cells which may give rise to bone, cartilage, and even fat cells. Caplan [36] first described MSCs in 1990 and the ability of these cells to go down different pathways of differentiation.
Several groups have described the use of MSCs in experiments with bioreactors. MSCs could be used in an autologous (from same patient) or allogeneic (non-matched donor) manner because they usually will not illicit an immune response, i.e., they are considered immunomodulatory [37]. In addition to the immune privileged nature of MSCs, they are a preferable source in that they will respond to mechanical stimuli [38,39,40,41] and allow natural remodeling to heart valve structure [42].
4.2 Fibroblasts/Smooth Muscle Cells/Valvular Interstitial Cells
Fibroblasts are a cell that are responsible for synthesizing the ECM and creating the framework of tissue. Smooth muscle cells (SMCs) or myocytes are responsible for creating muscle tissue in a process called myogenesis. Valvular interstitial cells (VICs) are the cells that make up the interstitial spaces of aortic valves. They exhibit an intermediate phenotype between fibroblasts and SMCs. They are responsible for creating the ECM in the valve and maintaining its mechanical characteristics [43].
Appleton et al. [44] combined vascular SMCs with a mixture of growth factors to create a surrogate cell source for developing a valve graft. They demonstrated that by combining SMCs with transforming growth factor beta-1, epidermal growth factor, and platelet-derived growth factor, they could increase proliferation and expression of ECM constituents found in the aortic valve. There are reports of calcification and other potential drawbacks to cells in the heart valve lineages such as a low rate of matrix remodeling and lack of elastin production. In addition, scaffolds seeded with these cells displayed low mechanical strength with a disarray of fibrous components. Ultimately even if these obstacles are overcome, the reality of being able to incorporate somatic cell sources such as SMCs for heart valve tissue engineering is likely to be impractical due to distinct supply limitations.
4.3 Endothelial Progenitor Cells
Endothelial progenitor cells (EPCs) are a mixture of cells that are responsible for regeneration of the endothelial lining of blood vessels. Because of their ability to create structured ECM, EPCs represent a viable cell source for TEHVs. In addition, EPCs can be used as a cell source for engineered valves because they have characteristics of both interstitial and endothelial tissues. Some researchers have combined EPCs with smooth muscle cells and fibroblasts to help improve the ECM formation [45]. Valves that had been conditioned in a bioreactor demonstrated unobstructed opening and closing. In addition, the tissue presented with collagen types I and II with a homogeneous cell distribution.
4.4 Embryonic/IPS/Amniotic/Cord
Embryonic stem cells (EScs) are the most primitive stem cell. They are derived from the inner cell mass of the blastocyst and are present in the embryo before implantation occurs in the uterus. EScs are capable of dividing rapidly in culture and can be grown indefinitely in an undifferentiated state. They are capable of differentiating into all cells of the adult body. EScs were originally discovered and derived from a mouse in 1981 by Evans and Kaufman [46] and later from a human by Thomson in 1998. Thomson [47] first developed a technique to isolate and grow human embryonic stems cells in culture. The inner cell mass (ICM) of the blastocyst is a pluripotent cell that can become specialized into any cell of the body. Cells from the ICM may maintain the potential to form any cell in the body even after extensive proliferation in culture.
Induced pluripotent stem cells (iPS) are progenitors that have been derived from an adult somatic cell via transcription factor encoding by genes. The adult cell is re-programmed to behave very similar to an ESc. The cells have similar expression of genes and proteins, potency and differentiability. Because iPS cells can be derived from the patient as an autologous product, there is less risk of rejection and no need for immunosuppression. In addition, the production of iPS cells does not require the destruction of an embryo, therefore eliminating some of the ethical debate surrounding embryonic stem cells. These cells are typically derived using transfection techniques to make the non-pluripotent cells express proteins or transcription factors that are typically expressed by pluripotent cells. Takahashi and Yamanaka [48] pioneered these techniques in 2006.
Both EScs and iPS cells represent a novel approach to tissue engineering because of their capacity to differentiate into any cell or tissue. Some groups have explored the use of these types of cells for heart valve tissue formation. As one example, Ghodsizad et al. [49] described the use of embryonic cells seeded in a decellularized valve in a magnetically guided multifunctional bioreactor. Valves were prepared using decellularized porcine pericardium. Half of the samples were prepared using a magnetic field to prevent the loss of cells. This allowed for homogeneous and efficient cell seeding of the decellularized matrix. An absence in cell seeding was observed in the nonmagnetic group. It is important to note that iPS is a new technology and issues relating to repeatability and avoidance of teratomas are likely to delay its applicability for use in translational heart valve tissue engineering investigations. Furthermore, ethical and legal concerns with embryonic cell sources are likely to result in translational studies focused primarily on adult stem cell progenitors for at least the foreseeable future.
Schmidt et al. [50] studied the use of amniotic fluid-derived cells as a potential source for heart valve tissue engineering. They demonstrated that the cells could maintain their characteristics after cryopreservation. In particular, cells expressing CD133 showed characteristics similar to endothelial-like cells and were able to produce ECM elements on a leaflet. Periodontal ligament cells (PDLs) have demonstrated potential in heart valve tissue engineering after flow-based, bioreactor mechanical conditioning [51]. PDLs can differentiate down pathways of endothelial cell and smooth muscle cell phenotypes by applying steady shear stress of 1 dyn/cm2.
5 Preclinical/Clinic Studies
A few studies have been completed where TEHVs were implanted in animals. Many preclinical animal studies were completed with the valve in the pulmonary position [52]. The benefit to testing the valve in the pulmonary position is that the conditions on the right side of the heart are less demanding than those of the systemic circulation. Dohmen et al. [52] described the use of tissue engineered valves in a juvenile sheep model. Decellularized porcine matrices were seeded with vascular endothelial cells. The valves were implanted into the right ventricular outflow tract. The valves exhibited endothelial cells along the inner surface of the valve as well as fibroblast growth on the decellularized matrix. In addition, the calcium contents were very low on the TEHV.
In another study, synthetic scaffolds were seeded with autologous bone marrow cells and implanted into nonhuman primates [53]. Echocardiography showed preserved valve function at 4 weeks post implant. Substantial cellular remodeling and ingrowth on the scaffold was visualized via histology and immunohistochemistry. In addition, there was evidence of new living tissue replacing the biodegradable synthetic matrix. Bert et al. [54] also demonstrated successful implantation of TEHV in young healthy baboons.
Hoerstrup et al. [55] preconditioned leaflet heart valves in pulse duplicators for 14 days prior to implanting in lambs. The valves grown in the bioreactor were under gradually increasing nutrient medium flow and pressure conditions (125 mL/min at 30 mm Hg to 750 mL/min at 55 mm Hg). They were able to function for up to 5 months when they were explanted and resembled normal heart valves in properties and structure. Converse et al. [56] have recently reported on a prototype of a full-scale system that produces pulsatile conditioning using cyclic waveforms. After 72 h of conditioning, full tissue recellularization was not achieved but a subsurface pilot population of cells resulted.
Preconditioning valves prior to implantation has been challenging mostly due to the lack of a disposable system that ensures sterility and can create an appropriate mechanical environment. When moving TEHV therapies to the clinic, it is important to develop a construct that is non-thrombogenic, biocompatible, capable of cell growth, have long-term efficacy, and result in clinical improvement for the patient. Dohmen et al. [57] reported on 63 patients with calcific aortic valve disease who underwent a valve replacement using a TEHV. A biopsy sample of the TEHV indicated the presence of endothelial cells and recellularization.
In 2006, researchers evaluated TEHVs seeded with autologous progenitor cells implanted into pediatric patients [58]. The cells were isolated from peripheral mononuclear cells isolated from human blood. No signs of valve degeneration were observed in either patient. Two clinical trials have been reported using decellularized xenograph heart valves [59]. Several adverse events were reported highlighting the importance of rigorous models prior to human studies. Three of the four children that received the implants died and therefore the fourth valve was removed prophylactically. Two of the three deaths were sudden with severely degenerated valves and the third had rupture after 7 days.
CorMatrix ECM Technology has been used at more than 825 hospitals across the USA and has been implanted in nearly 95,000 cardiac procedures. The FDA issued clearance of an Investigational Device Exemption (IDE) for an Early Feasibility Study of its CorMatrix® ECM® Tricuspid Heart Valve. Gerdisch et al. [31] demonstrated early feasibility on 19 patients for mitral valve repair. The ECM scaffold appeared to resist calcification and infection and may be a satisfactory material for mitral valve surgical situations; however, additional studies are warranted to determine long-term feasibility.
6 Conclusions
Tissue engineered valves provide new hope in the development of cardiac valve replacement. The main considerations when designing a TEHV include the scaffold and cell types as well as mechanical/physiological forces to condition the growing construct. The ability to develop a TEHV to replace damaged valve tissue decreases the risk of complications and improves valve performance. Tissue engineering presents the opportunity to introduce a natural tissue that may have long-term viability and fewer side effects. There are many hurdles still to overcome but TEHVs represent an opportunity to revolutionize the cardiac field. For example, valves which are exposed to dynamic and complex forces must integrate with the native tissue. Hence, designing a TEHV that is capable of integrating with native tissues and functioning in the high throughput of the heart is a challenge. Establishing appropriate in vitro models for optimizing mechanical cues for de novo valvular tissue growth and appropriate in vivo preclinical models can help to advance the field. Major research goals include understanding mechanisms of action, developing biomarkers, assays, and tools, defining appropriate endpoints and establishing reliable animal models. Preliminary work in the clinic is promising but many questions remain unanswered. The major clinical goals include characterizing and designing quality tissue constructs for implant, sterility concerns, addressing rejection complications, and early prediction of clinical outcomes. Thus, there are indeed many variables to be considered and further analyzed in TEHV design and approaches. Nonetheless, TEHVs represent an area in tissue engineering where clinical translation in the foreseeable future is likely, based on the state of the field today. The use of bioreactors as part of this process, in terms of a preconditioning tool, has proven to be essential, thus augmenting the role of the Bioengineer in the overall TEHV treatment strategy.
References
Nkomo VT, Gardin JM, Skelton TN, et al. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–11. https://doi.org/10.1016/S0140-6736(06)69208-8.
Berry JL, Steen JA, Koudy Williams J, Jordan JE, Atala A, Yoo JJ. Bioreactors for development of tissue engineered heart valves. Ann Biomed Eng. 2010;38(11):3272–9. https://doi.org/10.1007/s10439-010-0148-6.
Ohshima N, Yanagi K, Miyoshi H. Packed-bed type reactor to attain high density culture of hepatocytes for use as a bioartificial liver. Artif Organs. 1997;21:1169–76.
Seliktar D, Black RA, Vito RP, Nerem RM. Dynamic mechanical conditioning of collagen-gel blood vessel constructs induces remodeling in vitro. Ann Biomed Eng. 2000;28:351–62.
Gandaglia A, Bagno A, Naso F, Spina M, Gerosa G. Cells, scaffolds and bioreactors for tissue-engineered heart valves: a journey from basic concepts to contemporary developmental innovations. Eur J Cardiothorac Surg. 2011;39(4):523–31.
Carrion K, Dyo J, Patel V, Sasik R, Mohamed SA, Hardiman G, Nigam V. The long non-coding HOTAIR is modulated by cyclic stretch and WNT/ß-CATENIN in human aortic valve cells and is a novel repressor of calcification genes. PLoS One. 2014;9(5):e96577. https://doi.org/10.1371/journal.pone.0096577.
Dhein S, Schreiber A, Steinbach S, Apel D, Salameh A, Schlegel F, Kostelka M, Dohmen PM, Mohr FW. Mechanical control of cell biology. Effects of cyclic mechanical stretch on cardiomyocyte cellular organization. Prog Biophys Mol Biol. 2014;115(2–3):93–102. https://doi.org/10.1016/j.pbiomolbio.2014.06.006.
Girão-Silva T, Bassaneze V, Campos LC, Barauna VG, Dallan LA, Krieger JE, Miyakawa AA. Short-term mechanical stretch fails to differentiate human adipose-derived stem cells into cardiovascular cell phenotypes. Biomed Eng Online. 2014;13:54. https://doi.org/10.1186/1475-925X-13-54.
Koivisto E, Jurado Acosta A, Moilanen AM, Tokola H, Aro J, Pennanen H, Säkkinen H, Kaikkonen L, Ruskoaho H, Rysä J. Characterization of the regulatory mechanisms of activating transcription factor 3 by hypertrophic stimuli in rat cardiomyocytes. PLoS One. 2014;9(8):e105168. https://doi.org/10.1371/journal.pone.0105168.
Ku CH, Johnson PH, Batten P, Sarathchandra P, Chambers RC, Taylor PM, Yacoub MH, Chester AH. Collagen synthesis by mesenchymal stem cells and aortic valve interstitial cells in response to mechanical stretch. Cardiovasc Res. 2006;71(3):548–56.
Syedain ZH, Tranquillo RT. Controlled cyclic stretch bioreactor for tissue-engineered heart valves. Biomaterials. 2009;30(25):4078–84. https://doi.org/10.1016/j.biomaterials.2009.04.027.
Thayer P, Balachandran K, Rathan S, Yap CH, Arjunon S, et al. The effects of combined cyclic stretch and pressure on the aortic valve interstitial cell phenotype. Ann Biomed Eng. 2011;39:1654–67. https://doi.org/10.1007/s10439-011-0273-x.
Engelmayr GC, Hildebrand DK, Sutherland FW, Mayer JE, Sacks MS. A novel bioreactor for the dynamic flexural stimulation of tissue engineered heart valve biomaterials. Biomaterials. 2003;24:2523–32.
Engelmayr GC, Engelmayr GC Jr, Rabkin E, Sutherland FW, Schoen FJ, Mayer JE Jr, Sacks MS. The independent role of cyclic flexure in the early in vitro development of an engineered heart valve tissue. Biomaterials. 2005;26:175–87.
Engelmayr GC Jr, Sales VL, Mayer JE Jr, Sacks MS. Cyclic flexure and laminar flow synergistically accelerate mesenchymal stem cell-mediated engineered tissue formation: implications for engineered heart valve tissues. Biomaterials. 2006;27:6083–95.
Mirnajafi A, Zubiate B, Sacks MS. Effects of cyclic flexural fatigue on porcine bioprosthetic heart valve heterograft biomaterials. J Biomed Mater Res A. 2010;94(1):205–13.
Jockenhoevel S, Zund G, Hoerstrup SP, Schnell A, Turina M. Cardiovascular tissue engineering: a new laminar flow chamber for in vitro improvement of mechanical tissue properties. ASAIO J. 2002;48:8–11.
Mahler GJ, Frendl CM, Cao Q, Butcher JT. Effects of shear stress pattern and magnitude on mesenchymal transformation and invasion of aortic valve endothelial cells. Biotechnol Bioeng. 2014;111(11):2326–37.
Butcher JT, Nerem R. Valvular endothelial cells regulate the phenotype of interstitial cells in co-culture: effects of steady shear stress. Tissue Eng. 2006;12:905–15.
Ramaswamy S, Boronyak SM, Le T, Holmes A, Sotiropoulos F, Sacks MS. A novel bioreactor for mechanobiological studies of engineered heart valve tissue formation under pulmonary arterial physiological flow conditions. J Biomech Eng. 2014;136(12):121009.
Rath S, Salinas M, Villegas AG, Ramaswamy S. Differentiation and distribution of marrow stem cells in flex-flow environments demonstrate support of the valvular phenotype. PLoS One. 2015;10(11):e0141802. https://doi.org/10.1371/journal.pone.0141802.
Xing Y, He Z, Warnock JN, Hilbert SL, Yoganathan AP. Effects of constant static pressure on the biological properties of porcine aortic valve leaflets. Ann Biomed Eng. 2004;32:555–62.
Shinoka T, Breuer CK, Tanel RE, Zund G, Miura T, Ma PX, Langer R, Vacanti JP, Mayer JEJ. Tissue engineering heart valves: valve leaflet replacement study in a lamb model. Ann Thorac Surg. 1995;60:S513.
Sodian R, Hoerstrup SP, Sperling JS, Daebritz S, Martin DP, Moran AM, Kim BS, Schoen FJ, Vacanti JP, Mayer JE Jr. Early in vivo experience with tissue-engineered trileaflet heart valves. Circulation. 2000;102(19 Suppl 3):III22–9.
Filova E, Straka F, Mirejovsky T, et al. Tissue-engineered heart valves. Physiol Res. 2009;58(Suppl 2):S141–58.
Freed LE, Guilak F, Guo XE, et al. Advanced tools for tissue engineering: scaffolds, bioreactors, and signaling. Tissue Eng. 2006;12(12):3285–305.
Ghanbari H, Kidane AG, Burriesci G, et al. The anti-calcification potential of a silsesquioxane nanocomposite polymer under in vitro conditions: potential material for synthetic leaflet heart valve. Acta Biomater. 2010;6(11):4249–60.
Dumont K, Yperman J, Verbeken E, et al. Design of a new pulsatile bioreactor for tissue engineered aortic heart valve formation. Artif Organs. 2002;26(8):710–4.
Eaglstein WH, Falanga V. Tissue engineering and the development of Apligraf, a human skin equivalent. Clin Ther. 1997;19(5):894–905.
Cebotari S, Tudorache I, Jaekel T, et al. Detergent decellularization of heart valves for tissue engineering: toxicological effects of residual detergents on human endothelial cells. Artif Organs. 2010;34(3):206–10.
Gerdisch MW, Shea RJ, Barron MD. Clinical experience with CorMatrix extracellular matrix in the surgical treatment of mitral valve disease. J Thorac Cardiovasc Surg. 2014;148:1370–8.
Flanagan TC, Sachweh JS, Frese J, Schnoring H, Gronloh N, Koch S, Tolba RH, Schmitz-Rode T, Jockenhoevel S. In vivo remodeling and structural characterization of fibrin-based-tissue-engineered heart valves in the adult sheep model. Tissue Eng Part A. 2009;15:2965.
Syedain Z, Lathi M, Johnson SL, Robinson P, Ruth GR, Bianco R, Tranquillo RT. Implantation of a tissue-engineered heart valve from human fibroblasts exhibiting short term function in the sheep pulmonary artery. Cardiovasc Eng Technol. 2011;2:101.
Moreira R, Gesche VN, Hurtado-Aguilar LG, Schmitz-Rode T, Frese J, Jockenhoevel S, Mela P. TexMi: development of tissue-engineered textile-reinforced mitral valve prosthesis. Tissue Eng Part C Methods. 2014;20(9):741–8. https://doi.org/10.1089/ten.tec.2013.0426.
Hong H, Dong N, Shi J, et al. Fabrication of a novel hybrid scaffold for tissue engineered heart valve. J Huazhong Univ Sci Technol Med Sci. 2009;29(5):599–603.
Caplan AI. Mesenchymal stem cells. J Orthopaed Res. 1991;9(5):641–50.
Rubtsov YP, Suzdaltseva YG, Goryunov KV, Kalinina NI, Sysoeva VY, Tkachuk VA. Regulation of immunity via multipotent mesenchymal stromal cells. Acta Nat. 2012;4(1):23–31.
Lu X, Zhai W, Zhou Y, et al. Crosslinking effect of nordihydroguaiaretic acid (NDGA) on decellularized heart valve scaffold for tissue engineering. J Mater Sci Mater Med. 2010;21(2):473–80.
Lutter G, Metzner A, Jahnke T, et al. Percutaneous tissue engineered pulmonary valved stent implantation. Ann Thorac Surg. 2010;89(1):259–63.
Martin DJ, Warren LA, Gunatillake PA, et al. Polydimethylsiloxane/polyether-mixed macrodiol-based polyurethane elastomers: biostability. Biomaterials. 2000;21(10):1021–9.
Martin I, Wendt D, Heberer M. The role of bioreactors in tissue engineering. Trends Biotechnol. 2004;22(2):80–6.
Mathur AB, Collier TO, Kao WJ, et al. In vivo biocompatibility and biostability of modified polyurethanes. J Biomed Mater Res. 1997;36(2):246–57.
Taylor PM, Batten P, Brand NJ, Thomas PS, Yacoub MH. The cardiac valve interstitial cell. Int J Biochem Cell Biol. 2003 Feb;35(2):113–8.
Appleton AJ, Appleton CT, Boughner DR, Rogers KA. Vascular smooth muscle cells as a valvular interstitial cell surrogate in heart valve tissue engineering. Tissue Eng Part A. 2009;15(12):3889–97.
Moreira R, Velz T, Alves N, et al. Tissue-engineered heart valve with a tubular leaflet design for minimally invasive transcatheter implantation. Tissue Eng Part C Methods. 2015;21(6):530–40. https://doi.org/10.1089/ten.tec.2014.0214.
Evans MJ, Kaufman MH. Establishment in culture of pluripotential cells from mouse embryos. Nature. 1981;292:154–6. https://doi.org/10.1038/292154a0.
Thomson JA. Embryonic stem cell lines derived from human blastocysts. Science. 1998;282:1145–7. https://doi.org/10.1126/science.282.5391.1145.
Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006;126:663–76.
Ghodsizad A, Bordel V, Wiedensohler H, Elbanayosy A, Koerner MM, Gonzalez Berjon JM, Barrios R, Farag M, Zeriouh M, Loebe M, Noon GP, Koegler G, Karck M, Ruhparwar A. Magnetically guided recellularization of decellularized stented porcine pericardium-derived aortic valve for TAVI. ASAIO J. 2014;60(5):582–6. https://doi.org/10.1097/MAT.0000000000000110.
Schmidt D, Achermann J, Odermatt B, Genoni M, Zund G, Hoerstrup SP. Cryopreserved amniotic fluid-derived cells: a lifelong autologous fetal stem cell source for heart valve tissue engineering. J Heart Valve Dis. 2008;17(4):446–55.
Martinez C, Rath S, Van Gulden S, Pelaez D, Alfonso A, et al. Periodontal ligament cells cultured under steady-flow environments demonstrate potential for use in heart valve tissue engineering. Tissue Eng A. 2012;19:458–66. https://doi.org/10.1089/ten.TEA.2012.0149.
Dohmen PM, Ozaki S, Nitsch R, Yperman J, Flameng W, Konertz W. A tissue engineered heart valve implanted in a juvenile sheep model. Med Sci Monit. 2003;9:BR137–44.
Weber B, Scherman J, Emmert MY, Gruenenfelder J, Verbeek R, Bracher M, Black M, Kortsmit J, Franz T, Schoenauer R, Baumgartner L, Brokopp C, Agarkova I, Wolint P, Zund G, Falk V, Zilla P, Hoerstrup SP. Injectable living marrow stromal cell-based autologous tissue engineered heart valves: first experiences with a one-step intervention in primates. Eur Heart J. 2011;32:2830.
Bert AA, Drake WB, Quinn RW, Brasky KM, O'Brien JE Jr, Lofland GK, Hopkins RA. Transesophageal echocardiography in healthy young adult male baboons (Papio hamadryas anubis): normal cardiac anatomy and function in subhuman primates compared to humans. Prog Pediatr Cardiol. 2013;35(2):109–20.
Hoerstrup SP, Sodian R, Daebritz S, Wang J, Bacha EA, Martin DP, Moran AM, Guleserian KJ, Sperling JS, Kaushal S, et al. Functional living trileaflet heart valves grown in vitro. Circulation. 2000;102(19 Suppl 3):III44–9.
Converse GL, Buse EE, Neill KR, McFall CR, Lewis HN, VeDepo MC, Quinn RW, Hopkins RA. Design and efficacy of a single-use bioreactor for heart valve tissue engineering. J Biomed Mater Res B Appl Biomater. 2017;105:249–59. https://doi.org/10.1002/jbm.b.33552.
Dohmen PM, Hauptmann S, Terytze A, Konertz WF. In-vivo repopularization of a tissue-engineered heart valve in a human subject. J Heart Valve Dis. 2007;16(4):447–9.
Cebotari S, Lichtenberg A, Tudorache I, Hilfiker A, Mertsching H, Leyh R, Breymann T, Kallenbach K, Maniuc L, Batrinac A, Repin O, Maliga O, Ciubotaru A, Haverich A. Clinical application of tissue engineered human heart valves using autologous progenitor cells. Circulation. 2006;114(1 Suppl):I132–7.
Simon P, Kasimir MT, Seebacher G, et al. Early failure of the tissue engineered porcine heart valve SYNERGRAFT in pediatric patients. Eur J Cardiothorac Surg. 2003;23(6):1002–6; discussion 1006.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Comella, K., Ramaswamy, S. (2018). Novel Bioreactors for Mechanistic Studies of Engineered Heart Valves. In: Sacks, M., Liao, J. (eds) Advances in Heart Valve Biomechanics. Springer, Cham. https://doi.org/10.1007/978-3-030-01993-8_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-01993-8_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-01991-4
Online ISBN: 978-3-030-01993-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)