
Abstract
This chapter describes brain networks related to reward processing. We will first consider the reward regions identified by decades of preclinical and more recently human research and the circuits that connect them. These will include the classical “reward centers” along with various cortical and subcortical structures that contribute to reward learning and reward-based decision-making. The second section explores how these nodes, identified and described primarily in nonhuman mammals, are identified in humans through the use of noninvasive imaging techniques like functional magnetic resonance imaging (fMRI) and positron emission tomography (PET). We next discuss reward processing from a network-level perspective, including the methods by which structural and functional connectivity can be identified in humans with MRI-based tools. The final section will discuss functional connectivity networks that center on reward-related circuitry, as well as networks that serve many behavioral purposes but are affected by reward. Dysregulation of these reward networks circuitry in neuropsychiatric disorders will be explored using addiction as an exemplar.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Cue-reactivity paradigms
- Default mode network
- Delay discounting
- Dependence
- Diffusion tensor imaging (DTI)
- Dorsal anterior cingulate cortex
- Dorsal striatum
- Executive control network
- Functional MRI
- Habit formation
- Incentive salience
- Independent component analysis (ICA)
- Instrumental conditioning
- Mesocorticolimbic (MCL) system
- Monetary incentive delay (MID) task
- Neuropharmacological mapping studies
- Nucleus accumbens
- Orbitofrontal cortex (OFC)
- Pavlovian conditioning
- PET
- Reinforcement learning task
- Resting-state fMRI
- Resting-state functional connectivity
- Salience network
- Seed-based correlation analysis
- Substance use disorders
- Triple network model
- Value-based decision-making
- Ventral striatum
- Ventromedial prefrontal cortex
- Withdrawal syndrome
Brief History
Different Facets of Reward
While at first glance it may seem an intuitive and unitary construct, reward can be considered to have two distinct components: a “liking” component and a “wanting” component. The “liking” component refers to the pleasurable or hedonic experience. This aspect of reward is intuitive but difficult to empirically capture. Indirect measures of hedonic pleasure in animal models can include certain expressions or behaviors (e.g., licking in response to sweet, but not bitter flavors) and, in humans, a verbal report of a conscious experience. The “wanting” aspect of reward refers to its motivational effect or its reinforcing qualities. A stimulus is deemed rewarding if an animal or human behaves in such a way as to maximize the receipt of this stimulus, that is, if it acts as a reinforcer in reinforcement learning (see also glossary). As such, reward, motivation, and learning are closely tied constructs. From the standpoint of everyday experience, these “liking” and “wanting” aspects of reward can be seen as two sides of the same coin. However, the hedonic and motivational aspects may well be mediated by separable neural mechanisms. In practice these are nearly impossible to dissociate: the pleasurable experience of a rewarding stimulus is difficult to measure in the absence of either a behavioral effect or a verbal report. As a result, reward processes are typically studied from the behaviorally observable perspective, focusing on motivation and reinforcement learning. The present chapter reflects this focus on the “wanting” component, and hedonic processing is discussed in more detail in Chap. 46, “Limbic Cortex: The Functional Neuroanatomy of Emotion and Hedonic Processing.”
Rewarding stimuli capture our attention and guide our behavior in potent ways, and the presence of such a mechanism has a clear evolutionary advantage. Natural rewards such as food, water, and sex are crucial to our continued existence as a species. An organism therefore has better chances of survival if it attends to, is motivated to pursue, and learns to perform the behaviors necessary to attain such rewards. It should then come as no surprise that the neural representation of reward spreads far and wide in the brain. That said, while many interacting brain regions, circuits, and networks are ultimately affected by reward representations, a reasonably limited set of subcortical and prefrontal brain areas is considered primarily implicated in reward processing.
A Brief History of Reward-Processing Research
The study of the neurobiology of reward began in 1954 by a serendipitous finding by Olds and Milner. Olds and Milner implanted stimulating electrodes into rats’ forebrain and placed the rats in chambers. Upon stimulation the experimenters noticed that rats kept coming back to the places where they had previously received stimulation. In later versions of the task, rats could press a lever in exchange for self-administered electrical stimulation. They found that when the electrode was placed in certain areas (e.g., the septum, close to the nucleus accumbens and the ventral pallidum) but not others, the rat would vigorously press the lever so as to acquire more brain stimulation. Conversely, when pressing the lever no longer resulted in stimulation of this region, the behavior quickly extinguished. The authors noted that the extraordinary reinforcing properties of this stimulation “possibly exceeded [the control over the behavior] exercised by any other reward previously used in animal experimentation” (Olds and Milner 1954, p. 426). This seminal finding sparked a fruitful line of intracranial stimulation mapping experiments whereby various subcortical (and subsequently, cortical) brain areas in rodents were probed to determine if electrical stimulation supported various operant behaviors (e.g., nose poke, lever presses, runways, etc.). Similar powerful reinforcing effects were observed after stimulation of various sites in the ventral tegmental area (VTA), lateral hypothalamus, nucleus accumbens, and the medial forebrain bundle that interconnects these regions. Together, these areas were thought of as “pleasure centers” or “reward centers.” An important question at the time was whether these effects were driven by norepinephrine or by dopamine neurotransmission. A diverse range of techniques were used to tease apart how these centers and their connecting pathways contributed to the observed reinforcing effects and which neurotransmitter was active within each of these regions. Electrophysiological methods were used to trace the brain regions connected by the medial forebrain bundle, identifying importantly the ventral tegmental area (VTA). Around this time, it was discovered that the VTA houses the majority of dopamine neuron cell bodies that project to the identified reward centers (Falck and Hillarp 1959). The role of dopamine in this process was further confirmed by microdialysis and neuropharmacological mapping studies. Microdialysis can be used to measure extracellular dopamine levels during or following an intervention by placing a small catheter in a region of interest and subsequently measuring the content of the dialyzed extracellular fluid. Neuropharmacological mapping studies , where dopamine antagonist injections into reward centers blocked reinforcing effects of stimulation, further demonstrated the involvement of dopamine in this process. Thus, a combination of electrophysiology and pharmacological methods identified reward centers, the pathways that connect them, and the crucial role of dopamine in reward processing.
In the decades since these early explorations of reward processes, knowledge of the role of dopamine and other contributing neurotransmitters and neuromodulators has been considerably refined. A more nuanced role for dopamine signaling as a reward prediction error and learning signal has emerged (see also Chap. 52, “Networks Associated with Reward”). The dopamine signal should therefore not be considered as synonymous with reward, at least not as indicative of the hedonic experience of reward. Further, with the advent of noninvasive neuroimaging techniques, the study of the neurobiology of reward processing in humans has recently become possible.
Evolving Perspectives: Centers, Circuits, and Networks
Centers, Circuits, and Networks
Initial efforts to understand the brain were geared toward identifying “centers” for various functions: specialized regions that perform a specific function. Neuroscientists would traditionally look for a speech center, a mathematics center, a pleasure center, etc. As understanding of the brain has evolved, however, there is a growing appreciation that brain functions are not governed by a set of isolated, highly specialized centers. Rather, it has become clear that brain activity relevant to any behavior recruits a distributed group of brain regions, which are interconnected. The terms circuit and network both refer to connectivity and are sometimes used interchangeably in the literature, but in this chapter we will consider the two terms separately. A network is made up of many nodes and edges (that connect the nodes), whereas a circuit is a single connection between two nodes. For example, a road in a city that connects building A to building B is a circuit, whereas the entirety of the city’s roads form a network. In the case of reward processing, an anatomical projection from the ventromedial prefrontal cortex to the shell of the nucleus accumbens constitutes a circuit, whereas the broader, distributed group of interconnected brain regions that deal with reward processing makes up a network. Thus, individual brain regions identified to be important for reward (reward centers) make up the nodes of these networks, whereas the edges of the network are comprised of circuits connecting these nodes. Because the term network may be more loosely defined in the extant literature, the definition of “reward network” can include different sets of regions depending on context. A well-accepted perspective today is that brain functions are governed by sets of connected and interacting circuits: networks. Methodological advances, notably the introduction of whole-brain connectivity studies, allow us to identify and analyze such networks in human subjects. Thus, neuroscientists are taking the leap toward putting these reward-related circuits together to consider networks and dynamic alterations between networks.
Outline of This Chapter
This chapter describes brain networks related to reward processing. We will first consider the reward regions identified by decades of preclinical and more recently human research and the circuits that connect them. These will include the classical “reward centers” along with various cortical and subcortical structures that contribute to reward learning and reward-based decision-making. The second section explores how these nodes, identified and described primarily in nonhuman mammals, are identified in humans through the use of noninvasive imaging techniques like functional magnetic resonance imaging (fMRI) and positron emission tomography (PET). We next discuss reward processing from a network-level perspective, including the methods by which structural and functional connectivity can be identified in humans with MRI-based tools. The final section will discuss functional connectivity networks that center on reward-related circuitry, as well as networks that serve many behavioral purposes but are affected by reward. Dysregulation of these reward networks circuitry in neuropsychiatric disorders will be explored using addiction as an exemplar.
An Overview of Reward Centers and Circuitry
The identified reward regions and the circuitry that interconnects them are centered on dopaminergic ascending neuronal pathways. Despite their profound impact on reward, motivation, and motor control, there are only a very small number of dopamine neurons – fewer than 1 % of the brain’s neurons. Their cell bodies are primarily found in the ventral tegmental area (VTA) and the substantia nigra pars compacta (SNc), two areas that lie very closely together in the midbrain or mesencephalon. These midbrain dopamine neurons project primarily to the striatum, amygdala, and hippocampus (mesolimbic pathway) and to the prefrontal cortex (mesocortical pathway) and receive direct and indirect input from a very large number of regions, including the prefrontal cortex, ventral and dorsal striatum, and medial temporal regions (see Fig. 1a, b). Together, these regions form the mesocorticolimbic (MCL) system. The regions and circuits in the MCL system are not closed circuits. Indeed, the connectivity suggests that striatal reward areas integrate a wide variety of cortical and subcortical signals and influence activity in limbic regions, in association cortex, and in motor cortex. In turn, the cortical regions that project to the ventral striatum reward circuitry are also part of different networks that govern emotional processing and cognitive and motor function. Below, we will provide a brief overview of the regions and pathways most commonly associated with reward processing. Because of the emphasis in this chapter on the relevance of reward processing for goal-directed decision-making, we include dorsal striatal and prefrontal association areas in this section. We refer the reader to Haber and Knutson (2010) for an excellent and more detailed review of this circuitry and Chap. 37, “Basal Ganglia: Basic Principles” for more information about motor functions of the basal ganglia.

The mesocorticolimbic (MCL) dopamine system. (a) Overview of key structures and pathways in the MCL system. Red-to-yellow color scheme represents the limbic-to-cognitive gradient in prefrontal cortex (top) and striatum (middle). Amy amygdala, Hipp hippocampus, Hypo hypothalamus, LHb lateral habenula, VP ventral pallidum, PPT pedunculopontine nucleus, STN subthalamic nucleus, s NAcc shell. (b) Schematic representation of reward circuitry situated in the human brain. (c) Ascending spiral-like connectivity through the MCL system. Red-to-yellow colors represent the limbic-to-cognitive gradient in prefrontal cortex, striatum, and midbrain. Fronto-striatal projections and striato-mesencephalic projections are more diffuse than striato-frontal and mesencephalo-striatal projections, such that the limbic loop signals impact upon both limbic and associative structures and that associative loop signals impact upon both associative and motor structures. This ascending spiral connectivity pattern allows for reward signals to influence cognitive and motor behavior (Panels (a) and (c) reprinted, with permission, from Haber and Knutson © (2010) Nature Publishing Group. Panel (b) reprinted, with permission, from Everitt & Robbins © (2005) Macmillan Publishers Ltd.)
The Mesocorticolimbic (MCL) System
Box 1 Value-Related Decision-Making, Pavlovian Conditioning, Instrumental Conditioning, and Habit Formation
Reward learning and reward-related decision-making involve various processes, including classical and instrumental conditioning, and economic decision-making. Here, we illustrate some of these reward processes with an example. Suppose that you have a weekly meeting at a fixed time, always in the same room with the same people. Whenever there is a meeting, there is a plate of cookies on the meeting table. When deciding whether or not to take a cookie, several factors may weigh in. Eating a cookie may be in conflict with another goal (like eating healthier or losing weight); there may be alternatives right now (there is also a bowl of candy on the table) or alternatives later (someone has a birthday and there will be cake later). This value-based decision-making process involves weighing these different choices. When you reach for a cookie and eat it, you have the experience of a pleasant taste (unconditioned response) and texture and you are also motivated to take another cookie. Over many weeks, the consistent pairing of the meeting time, place, people present (conditional stimulus), and the availability of the cookie (unconditioned stimulus) will cause Pavlovian (or classical) conditioning. The time of the meeting or the meeting room (conditioned stimulus) causes you to want cookies and your mouth may begin to water (conditioned response). Instrumental (or operant) conditioning may also occur; you may go to the meeting in order to obtain the cookies. Over time, the act of eating cookies at this meeting may become a habit rather than a goal-directed action. You may find yourself absentmindedly reaching for the cookies, even if you are not hungry or feel like a sweet snack. Even if you’ve just eaten a very large meal and do not feel like eating anything sweet, you may still eat a cookie. This constitutes stimulus–response learning or habit formation : there is no longer a link between any goal and the response.
The Midbrain
The ventral tegmental area (VTA) and the substantia nigra pars compacta (SNc), located in the brainstem mesencephalon (midbrain), house the cell bodies of nearly all the brain’s dopamine neurons. These are adjoining areas, with the VTA just medial and just inferior from the SNc. Major outputs of the VTA/SNc are the striatum and the frontal cortex (via the globus pallidus and thalamus). VTA/SNc projections to the striatum and to the cortex follow a topographical organization. That is, the VTA projects preferentially to the ventral striatum (mesolimbic pathway) and limbic prefrontal regions (mesocortical pathway), whereas the SNc projects preferentially to the dorsal striatum (nigrostriatal pathway) and cognitive and motor frontal areas. Aside from the striatum and frontal cortex, the VTA and SNc also project to the amygdala, hippocampus, the bed nucleus of the stria terminalis, and the periaqueductal gray. The largest input into the VTA/SNc comes from the striatum (through the globus pallidus) and from the brainstem. These latter brainstem projections carry direct sensory information that can likely trigger immediate dopaminergic responses to a salient event or reward.
The Striatum
The striatum consists of the caudate nucleus and the putamen, which are separated by the internal capsule. Within the striatum, there is a functionally very important gradient from ventral to dorsal regions. Although there are no cytoarchitectonic boundaries between the ventral and dorsal striatum, these regions can be functionally separated by several methods, including the projections they receive (Haber and Knutson 2010). Like the midbrain dopamine areas, these projections to the striatum are topologically organized and follow a gradient, such that input into the dorsolateral striatum is primarily from premotor and motor cortex, input into the dorsomedial striatum is from association cortex (dorsolateral prefrontal cortex), and input into the ventral striatum is from limbic prefrontal areas (consisting of orbital and ventromedial prefrontal cortex and dorsal anterior cingulate cortex). A strict conceptualization of the MCL system would include the ventral, but not the dorsal striatum.
The ventral striatum (VS) is the portion of the striatum that lies ventral to the anterior limb of the internal capsule. The major component of the VS is the nucleus accumbens, which receives projections from mesencephalic dopamine centers, the orbitofrontal and ventromedial prefrontal cortex (OFC/vmPFC), and the dorsal anterior cingulate cortex (dACC). Input is also received from medial temporal structures, amygdala and hippocampus, and these latter inputs are specific to the ventral striatum. The nucleus accumbens (NAcc) can be divided into the NAcc shell and the core, which have different structural and functional properties, including different functions in Pavlovian conditioning (Everitt and Robbins 2005). The NAcc shell is proposed to code for the primary reinforcing effects of a reward (the cookie in the example above), but not to the cue that predicts the reward (the context of the meeting). The NAcc shell projects to the various motor structures that may mediate the reflexive and autonomic responses to rewards (like salivating). Conversely, the NAcc core is necessary to acquire Pavlovian conditioning, and after conditioning this region responds best to reward-predicting cues. The NAcc core also works together with the basolateral amygdala to bridge delays in reinforcement; when the connection between these regions is severed, animals cannot retain the association between a stimulus and a delayed reward. The ventral striatum projects directly to the ventral pallidum and to the VTA and medial portions of the SNc. In addition, the NAcc shell projects to the lateral hypothalamus and sparsely to the periaqueductal gray. Both NAcc core and shell project to the bed nucleus of the stria terminalis, part of the extended amygdala.
The dorsal striatum (DS) consists of the dorsal aspects of the caudate and putamen and is primarily implicated in cognitive (associative) and motor functions. Perhaps most relevant to reward processing, the DS is involved in habitual stimulus–response association. After conditioning has taken place, neurons in the DS fire in response to a conditioned stimulus. When stimulus–response behavior is formed, responses to the predictive cues are no longer seen in the ventral but instead in the dorsal striatum. When the dorsal striatum is disconnected from the ventral striatum, this habitual responding is disrupted. More about the functions of the dorsal striatum can be found in Chap. 37, “Basal Ganglia: Basic Principles”.
The Prefrontal Cortex
Many prefrontal cortical areas project to the striatum. The ventromedial and orbital prefrontal cortex and the dorsal anterior cingulate cortex are most directly implicated in reward processing and project to the ventral striatum. Dorsal and dorsolateral prefrontal areas project to the central striatum, and premotor and motor cortical areas project to the dorsal striatum.
The orbitofrontal cortex (OFC) is generally defined as the entire ventral surface of the frontal lobes. The OFC receives input from all sensory modalities and projects to many regions in the MCL system, including the NAcc core, anterior portions of the dorsal striatum, the dACC, as well as the basolateral amygdala and hippocampus. The OFC is the prefrontal brain area most consistently implicated in the representation of value (Wallis 2007). Both primary rewards (pleasant tastes or odors) and secondary or learned rewards (such as money) require OFC processing. A medial-lateral gradient has been proposed whereby lateral portions of the OFC code for value representations relevant to action, and medial portions of the OFC code for value per se. This medial region, along with the subcallosal gyrus immediately superior to the medial orbitofrontal gyrus, makes up the ventromedial prefrontal cortex (vmPFC). In this chapter, we primarily deal with vmPFC/OFC as it relates to value and reward. In humans, vmPFC/OFC lesions are associated with deficits in flexibly updating the reward value of different options. That is, patients with lesions in this area can initially learn to associate a stimulus with a rewarding outcome, but when the choice for this reward is no longer advantageous, the individual is not able to update this information and flexibly adapt their behavior. It has been proposed that vmPFC/OFC integrates multimodal information regarding the reward value of different alternatives, which allows a choice to be made. When reward contingencies change, this value is updated. The OFC/vmPFC receives input from the insula and the VS and is therefore well placed to integrate costs and benefits when people engage in decision-making (Knutson et al. 2005). In human neuroimaging research, the vmPFC/OFC consistently responds to the anticipation and receipt of rewarding stimuli. Other prefrontal regions such as the dorsal ACC and the dorsolateral prefrontal cortex also respond to rewarding stimuli, but less consistently.
The dorsal anterior cingulate cortex (dACC) receives input from areas engaged in affective, cognitive, and motor functions. It is especially active in situations with conflicting alternatives and is thought to be involved in monitoring performance and inhibiting inappropriate responses. As it receives projections from areas that represent value (the OFC/vmPFC and VS), it is well placed to adjudicate between multiple potential options with different value weights.
Other prefrontal regions that contribute to reward-based decision-making but do not directly represent value are dorsal areas of the prefrontal cortex: the dorsolateral prefrontal cortex (DLPFC) and dorsal aspects of the superior frontal gyrus. The DLPFC is especially engaged in working-memory tasks and rule-based decision-making. As such, this region is engaged when multiple alternatives must be kept on line and manipulated during decision-making.
The Amygdala
The amygdala has historically been associated with fear processing, but is now thought to play a role in emotional processing more generally and importantly contributes to reward learning and punishment learning. The amygdala is strongly connected with the NAcc, but also shows some connectivity with other parts of the VS. While it is often considered as a single structure, the amygdala consists of several subnuclei. One functionally relevant distinction is between the basolateral and a corticomedial amygdala. The basolateral amygdala i s densely connected with the NAcc core, the OFC, and the hippocampus. Importantly for reward learning, the basolateral amygdala and the NAcc core play an important role in the acquisition of stimulus–reward associations. However, once these associations are acquired, the amygdala is not necessary for maintaining the association. In fMRI studies, both amygdala and NAcc respond to a reward-predicting cue during the beginning of the learning process, but amygdalar activity decreases over time, whereas NAcc activity increases over time. The NAcc core and basolateral amygdala circuit is thought to bridge delays in reinforcement. Lesions of the basolateral amygdala make it more likely that a smaller, immediate reward will be chosen over a larger delayed reward (impulsive choice). In contrast, the centromedial amygdala , along with the NAcc shell, the bed nucleus of the stria terminalis, and the sublenticular substantia innominata form the extended amygdala, which together share similar cytoarchitectonic properties and are important in reward and fear processing. The extended amygdala is important in negative reinforcement and plays a key role in cue-induced (i.e., conditional stimulus-induced) drug craving.
Other Structures
The globus pallidus is the brain region that receives the majority of the output from the striatum. The ventral pallidum (VP) is the ventral portion of the globus pallidus and receives the main VS output. Connections from the VS to the prefrontal cortex must first go through the VP and the medial dorsal thalamus. In turn, the VP projects back to large portions of the striatum. It also projects to the subthalamic nucleus, the hypothalamus, the VTA, and the lateral habenula.
The medial dorsal (MD) thalamus completes the circuit from VS through the VP to prefrontal cortex (see Fig. 1a). Its connectivity with PFC is bidirectional, so prefrontal areas can also exert top-down control on signals coming from VP and VS. The MD thalamus also supports direct projections back to the VS. The MD thalamus is implicated in reward processing, but its activation profile in fMRI studies is more consistent with general arousal than with reward per se.
The hippocampus projects to the NAcc shell areas that overlap with projections from the amygdala and vmPFC/OFC. The hippocampus is proposed to provide contextual information to other nodes in the reward circuit.
The lateral habenula (LHb) receives information from the VS through the ventral pallidum and supports inhibitory projections to midbrain dopamine neurons. The LHb shows exactly the opposite pattern of activity from the VTA, i.e., experimental activation of the LHb results in decreased firing in the VTA/SNc. Thus, it appears that the LHb codes for a non-reward or punishment signal.
Though not commonly considered part of the reward circuitry, the anterior insula supports strong connectivity with many nodes in the reward circuitry and plays a large role in the neurobiology of drug addiction, particularly drug craving. The anterior insula receives sensory and emotional input from a variety of subcortical structures and is thought to track and compute homeostatic imbalances. The anterior insula is densely connected with dACC and is ideally placed to relay information about homeostatic imbalances to the dACC (Craig 2011).
Parallel and Overlapping Loops: A Ventral-to-Dorsal Cascade
The connectivity in the prefrontal-striatal-mesencephalic system described above is organized in the form of topographically structured parallel and overlapping loops. A consistent limbic-cognitive-motor gradient can be discerned in the prefrontal, striatal, and midbrain structures. In the midbrain, the VTA is primarily implicated in limbic processes, whereas the SNc is more engaged in cognitive and motor processes. Similarly, the striatum is characterized by a gradient whereby reward signaling is subserved by the VS and cognitive and motor signals by the dorsal striatum. Finally, in prefrontal cortex, vmPFC/OFC and dACC are considered limbic prefrontal structures and primarily involved in reward, whereas DLPFC is involved with cognitive processing and premotor and motor cortices with motor function. Parallel limbic, associative, and motor loops can therefore be discerned. Importantly, these loops are not separate: projections overlap and the loops influence each other’s activity following a limbic-to-motor gradient. That is, signals in the limbic loop can modify signals in the cognitive loop, and the latter can bias signaling in the motor loop (see Fig. 1c). Applied to striatal-midbrain-striatal connectivity, projections from the limbic striatum affect a relatively large part of the dopaminergic midbrain neurons, not only the portions that project back to the limbic striatum but also those that project back to the associative striatum. In turn, projections from the associative parts of the striatum project not just to midbrain areas that project back to the associative striatum but also to the midbrain areas that project back to the motor striatum. A similar connectivity structure applies to fronto-striato-frontal connectivity; ventral striatal signals (indirectly) project to limbic prefrontal regions, but these limbic prefrontal regions project to both VS and DS regions. This spiral-like pattern of connectivity has been dubbed a motivation-to-movement interface (Haber and Knutson 2010) and is proposed to be the anatomical substrate by which reward-related information can influence cognitive processes and motor output. This cascade is also heavily implicated in reward-based associative learning and habit formation (Everitt and Robbins 2005).
Capturing Nodes in the Reward Network with Neuroimaging
Whole-Brain Imaging of Reward Processing
The study of brain function in humans requires a different set of tools than that in rodents or nonhuman primates. For obvious ethical reasons, invasive techniques such as intracranial self-stimulation and microdialysis cannot be used in humans. Over the last few decades, whole-brain imaging methods such as PET and functional MRI have propelled human neuroscience research forward. Applied to the investigation of reward processing, these methods have been used to capture the brain’s computations of and response to the anticipation and receipt of rewarding stimuli, to investigate neural activity during reward-related decision-making, and to characterize dysfunctional reward processing.
PET requires injecting participants with a radioactive tracer (see Chap. 98, “Molecular Imaging: Positron Emission Tomography”). The gamma rays emitted by the tracer are detected by the PET scanner and, after processing, provide a 3D image of where the tracer is localized in the brain. What is being measured and the temporal resolution depend on the properties of the particular tracer being used. For example, one of the most commonly used tracers is radioactive water [H2 15O], which enables quantitative measure of cerebral blood flow (CBF). As a brain region becomes more active, it requires more oxygen. In response, the influx of oxygenated blood is increased to meet this demand. This demand-related increase in oxygen can be captured with PET imaging and is thus an indirect marker of neuronal activity. Metabolic demand can also be measured using radioactive oxygen [15O] or with a radioactive version of the common metabolic substrate, glucose. In addition to capturing metabolic demand, different radioactive tracers can be used to image various neurotransmitters. Especially useful in the context of reward processing are tracers that bind to dopamine receptors, the most common example of which is [11C]raclopride, which binds to dopamine D2/D3 receptors in the striatum. Other tracers exist that also bind to dopamine receptors in cortical areas (e.g., fallypride), albeit with a lower signal to noise ratio.
In contrast, fMRI does not require the exogenous administration of a radiotracer, but rather takes advantage of the different magnetic properties of endogenous oxygenated and deoxygenated hemoglobin, the ratio of which changes with neuronal activity-induced metabolic demand and gives rise to the commonly measured blood oxygenation-dependent (BOLD) fMRI signal (see Chap. 99, “Functional Imaging: Magnetic Resonance Imaging”). While the exact neurovascular coupling mechanisms of this signal remain to be fully determined, brain areas where more neuronal activity is taking place require more oxygen, and following processes related to local vasodilation, more oxygenated blood is transported to these brain areas in response to the increased demand. The most common way of using fMRI is task-based fMRI, wherein the amplitude (size) of the BOLD response is compared between a condition where a process of interest is being actively manipulated and one where this process is constant. For example, one might compare BOLD activity at a time when a reward is being received with the BOLD activity in the absence of reward receipt.
It is important to note that both metabolic PET and fMRI are indirect measures of neural activity. Unlike electroencepalography (EEG) neither method records neural electrical activity. However, there is ample evidence that both the PET cerebral blood flow and metabolism signal and the BOLD fMRI signal correlates well with neural activity. For some brain areas, in-depth animal studies using microdialysis and pharmacological studies have been able to link BOLD responses to the activity of a specific neurotransmitter. For example, BOLD responses in the NAcc have been shown to be directly related to dopamine D1 receptor activation (Knutson and Gibbs 2007). Because of the superior spatial resolution (a few cubic millimeters) and temporal resolution (an image can be collected every few seconds) and because no radioactive injections are required, fMRI has largely replaced metabolic PET. However, PET remains uniquely able to investigate specific receptor systems using a wide variety of ligands.
Reward Anticipation and Receipt, and Economic Decision-Making
The responsiveness of MCL structures to rewarding stimuli has been replicated in humans in a variety of tasks that capture the anticipation or receipt of a primary or monetary reward and in decision-making tasks where participants learn to predict rewards or make a choice with the aim of maximizing a reward. This section will cover three fMRI tasks that have been used to study reward anticipation, economic decision-making, and reward learning.
The first and one of the most widely used fMRI reward tasks, the monetary incentive delay (MID) task , captures the anticipation and receipt of a reward. In this task, participants are shown a visual cue, must wait for a variable amount of time, and respond following a second visual stimulus prompt. The cue either indicates that the participant can earn money or avoid a monetary loss by pressing a response button. By analyzing the BOLD response during the delay period, we can identify which brain areas are more active when a reward is anticipated versus when a punishment is anticipated. In a meta-analysis of the MID task (Knutson and Greer 2008), this reward versus punishment contrast shows activation of the VS, dorsal striatum, vmPFC, anterior insula, and thalamus (See Fig. 2a).

fMRI-based studies of reward processing. (a) MID task. BOLD activity in the nucleus accumbens in response to the anticipation of a large versus a small reward (top left) and the anticipation of a reward versus a neutral outcome (top right). The lower panel shows the BOLD signal in the NAcc as a function of monetary outcome (ranging from −$5 to +$5). This demonstrates that the NAcc response increases as a function of increased reward magnitude (positive outcomes), but is not significantly changed as a function of punishment severity (negative outcomes). (b) Delay discounting task. The top panel shows regions in the ventral striatum, vmPFC/OFC, and posterior cingulate cortex that show larger responses to rewards that are immediately available in a delay discounting task. The lower panel shows the BOLD signal for these areas in trials where a reward is available immediately (red), in 2 weeks (green), or in 1 month (blue) (Reprinted with permission from Knutson et al. © (2001) Society for Neuroscience. Panel (b) modified, with permission, from McClure et al. © (2004) AAAS)
Much reward-based processing in everyday life goes beyond simply expecting and receiving a reward. We often need to make choices between options that vary on a number of different parameters that determine their subjective value. These parameters include the size of the reward, how likely it is that the choice will be rewarded (risk), and the amount of time you need to wait to receive the reward. In a delay discounting task, participants make a choice between an immediate monetary reward versus a larger reward that is delayed by a variable amount of time. Rewards lose some of their value as a function of time (e.g., a $2 reward is more rewarding when received today than when received in 1 year’s time), and this phenomenon is called delay discounting . The degree by which people discount rewards as a function of time in this task predicts a large range of real-life outcomes and can be captured with a discounting function. fMRI analysis of this task identifies regions that respond to the immediate reward and regions that respond to choosing to wait for a reward, which also relates to the construct of impulsivity. The immediately available reward is associated with activity in the VS, vmPFC, OFC, hippocampus, and posterior parietal cortex (McClure 2004). Delayed choices are associated with activity in areas related to executive control and response inhibition, including the DLPFC, posterior parietal cortex, and premotor areas.
A different approach to using fMRI to study reward learning is to incorporate a computational model of a hypothesized process in the brain. For example, in a reinforcement learning task, participants learn to associate cues with rewards or punishments. In well-established models of reinforcement learning, the level of surprise, or prediction error, is the driving force behind learning: when there is a discrepancy between the expected outcome and the actual outcome (a prediction error), this expectation is adjusted for the next trial. When the association is learnt completely, there is no longer a prediction error. O’Doherty and colleagues (2003) sought to find which brain areas correspond with a prediction error as modeled by a reinforcement learning equation. They found that activity in VS, OFC, inferior frontal, and cerebellar regions corresponded to the prediction error signal that drives reward learning.
In sum, neuroimaging investigations of tasks that involve reward and reward learning have confirmed preclinical data of the importance of striatal and prefrontal areas in reward processing. Beyond simple reward processing, economic decision-making paradigms allow researchers to capture complex decision-making and reward learning in humans, for example, by applying reinforcement learning models in fMRI analysis.
Disordered Reward Responses in Addiction
Reward processing is altered in many neuropsychiatric disorders such as depression, ADHD, schizophrenia, and addiction. We use drug addiction as an exemplar of dysregulated reward processing. Addiction is a chronic disease that is characterized by compulsive drug use, especially in the face of negative consequences. The terms drug addiction and substance abuse are sometimes used interchangeably, although the official classification by the DSM-V, the diagnostic and statistical manual for mental disorders, is substance use disorder (SUD). In line with the role of compulsivity in drug seeking and subsequent drug use, the DSM-V diagnostic criteria for SUD emphasizes loss of control over intake and continued use in spite of negative consequences, along with drug tolerance and craving.
Not all drug use leads to an SUD, and the vast majority of people who take a drug once or just a few times never become addicted. Unfortunately it is still not possible to predict those individuals who can, for example, socially engage in responsible alcohol consumption versus those who will go on to develop a SUD. Many substances, including caffeine, nicotine, and alcohol, induce tolerance when taken frequently. That is, you need more of the substance to achieve the same drug effect. Generally speaking, tolerance is necessary to develop a SUD, but not all tolerance is indicative of a SUD. Dependence occurs when a person needs to take a substance in order to function normally. When a person is dependent on a substance but is not taking that substance, this results in a withdrawal syndrome , which may include unpleasant physical, emotional, and cognitive symptoms that vary depending on the substance. Physical withdrawal symptoms can include symptoms like nausea, heart palpitation, headache, delirium tremens (DTs), and others. Emotional and cognitive withdrawal symptoms can include lack of concentration, dysphoria, and anhedonia. Physical withdrawal symptoms typically dissipate sooner than the negative emotional state. Withdrawal is often accompanied by conscious craving, i.e., a strong urge to use the substance.
There are various schools of thought and different neurobiological models that describe addiction. These ideas rarely directly contradict one another, but instead different models highlight different aspects or phases of addiction. We briefly mention some contemporary theoretical constructs, but due to space, the reader is referred to several excellent reviews (Everitt and Robbins 2005; Koob and Moal 1997; Koob and Volkow 2010).
Most drugs of abuse directly or indirectly increase levels of dopamine in the MCL system, which elicits a very powerful reinforcement learning process. The presence of the drug itself together with associated stimuli, for example, drug use paraphernalia, becomes strongly associated with the rewarding experience. These stimuli thus acquire incentive salience: they acquire similar motivational properties as the drug and exposure to these cues elicit drug craving (cue-induced craving, which leads to drug seeking and ultimately consumption). Addiction can be characterized as disordered reward learning or reward overlearning. Initial use and intoxication are marked by the engagement of ventral striatal circuits. Over time, with repeated drug use, there is a transition into habitual and compulsive drug taking with the further engagement of dorsal striatal circuitry. The overlearned motivation for the drug overshadows other motivations, and people who suffer from addiction show a decreased attention to nondrug-related rewarding stimuli. This has been described as a shift in the hedonic set point: natural rewards are no longer considered rewarding enough to motivate behavior. There is ample evidence that addicts show much decreased levels of attention to nondrug-related cues (including such natural rewarding stimuli as sexual stimuli) as well as increased attention to drug-related cues. Thus, dopaminergic reward circuits that evolved to cause us to approach natural rewards like food and sexual activity are “hijacked” by drugs of abuse. As a result, addicted individuals are strongly motivated to approach the drug more than natural rewards.
When studying the effects of addiction, a distinction can be made between addiction as a state and as a trait. State effects refer to the effects that occur in the moment, i.e., the acute consequences of the presence (such as intoxication) or absence (such as withdrawal) of the drug. The trait of addiction refers to the long-term consequences of repeated drug use on the brain, regardless of whether drugs are presently in the system or not, e.g., drug dependence level. Whole-brain imaging studies, as well as animal studies, have shown that neural activity in reward-related areas changes as a consequence of acute drug intake (state) and as a consequence of long-term drug use (trait).
Like natural rewards and learned rewards, substances of abuse activate the MCL reward circuitry, and substance use disorders are associated with long-term changes to structure and function of these (and other) brain areas. Drugs of abuse vary widely according to their pharmacological classification and mechanisms of action. The reader is referred to the chapters of the part “Addictive Disorders” for an in-depth description of nicotine, psychostimulant, opioid, alcohol, food, and internet addictions. Despite the heterogeneity in addictive substances, the neural basis of addiction shows remarkable coherence. The same reward-related areas are affected, and SUDs based on different abused drugs share many of the same predisposing vulnerabilities and cognitive consequences.
The effects of an acutely administered drug generally include an increase in striatal dopamine and an increased neuronal response in the MCL dopamine system. PET imaging of dopamine D2/D3 receptors has shown that administration of stimulants, mostly amphetamine or cocaine, increases striatal dopamine concentrations. This increase is positively associated with the subjective “high” (Goldstein & Volkow 2002). In contrast, individuals with a SUD in the absence of acute drug administration show decreased levels of striatal dopamine (see Fig. 3a). Thus, addicted people have lower base levels of striatal dopamine, and this deficit is at least partially remedied with drug intake.

Substance use disorders are associated with changes in the MCL system. (a) PET imaging studies using [11C]raclopride show that striatal dopamine D2/D3 receptor availability is reduced in subjects with substance use disorder for cocaine (top), methamphetamine (middle), and alcohol (bottom). (b) Inhibitory control impairments in cocaine users. During a Go-NoGo task, in which participants are required to press a button in response to a Go stimulus but suppress a response in response to a NoGo stimulus, cocaine users perform worse than control participants at inhibiting these inappropriate responses. When failing to withhold an inappropriate response, cocaine users show reduced neural activity in dACC, a region important for response inhibition and conflict monitoring. This reduced activation is shown in the sagittal cross sections (top left) and bar graph (top right). The bottom panel shows BOLD differences between cocaine users and controls, showing areas that are less active in cocaine users during correct inhibitions (red) and during failed inhibitions (blue) (Panel (a) reprinted, with permission, from Goldstein & Volkow © (2002). Panel (b) modified, with permission, from Kaufman et al. © (2003) Society for Neuroscience)
This drug-induced dopamine increase is also seen when addicted individuals see stimuli that have acquired incentive salience. These stimuli have been repeatedly associated with drug use, such as a shop where cigarettes can be bought or an environment where individuals have often previously used the drug. In cue-reactivity paradigms , drug-associated stimuli (e.g., a hand holding a cigarette) and neutral stimuli (e.g., a hand holding a pen) are presented to the subject. BOLD increases in MCL areas (VS, amygdala, OFC, anterior insula) are observed in addicted groups when looking at drug cues compared to neutral cues (but not in healthy nondrug users). In addicted groups, these increases in neuronal activity and dopamine release are correlated with stimulus-induced drug cravings.
In persons with cocaine addiction, areas like the dACC become hyperactive when drug cues are presented and hypoactive when nondrug-related stimuli are presented. The dACC plays a role in reward prediction and reward learning, but is also engaged in demanding cognitive tasks and in conflict monitoring and resolution. The decreased activity of the dACC as indicated by fMRI is tied to the decreased ability to perform cognitive tasks and to inhibit inappropriate responses (Kaufman et al. 2003). These deficits are most striking when the subject is abstinent and in a state of withdrawal.
In sum, drug cues, the anticipation of drug administration, and the actual administration of drugs of abuse all lead to activity increases in the MCL dopamine system. Repeated drug use leads to plasticity in the MCL system, such that tonic dopamine levels are lower and natural rewards elicit weaker responses than in the absence of addiction. Substance use disorders are associated with widespread dynamic changes throughout the reward network. Individuals with SUDs show increased impulsivity and decreased performance on cognitively demanding tasks and tasks that require inhibitory control. These deficits are accompanied by decreased activation in prefrontal regions such as the dACC.
Brain Networks Associated with Reward
Noninvasive Neuroimaging Techniques Capture Structural and Functional Connectivity
MRI methods can be used to probe structural and functional brain connectivity. Structural connectivity refers to the white matter tracts (bundles of axons) that connect brain regions. In nonhuman animals, invasive methods such as viral tracers can be used to identify brain areas that project to other regions. In humans, diffusion-weighted MRI (i.e., diffusion tensor imaging) can be used to indirectly estimate the localization and the integrity of white matter tracts noninvasively. Functional brain connectivity is a more recent construct that refers to correlated activity between two or more brain regions. Brain areas that are structurally connected and/or brain regions that support the same process show correlated activity. There are different methodologies that measure functional connectivity, but by far the most often used has been resting-state fMRI, whereby the correlation of BOLD signal fluctuations over time is used as an indicator that two or more areas are functionally connected (see Chap. 51, “Intrinsic Brain Activity and Resting State Networks”).
Diffusion tensor imaging (DTI) captures the orientation and integrity of white matter tracts by estimating local water diffusivity. The white matter consists of bundles of fatty, myelinated axons that connect brain regions with one another. Because the myelin sheaths along these fibers are hydrophobic, water can move more freely along the fibers than across them. Therefore, water diffusivity will occur predominantly in one direction – parallel to the white matter tract. Conversely, in the gray matter and in the cerebrospinal fluid, there are no such boundaries to water diffusion, and diffusivity is roughly equal in all directions. DTI is an indirect measure of structural connectivity, because it cannot directly assess the fiber tracts. Instead, diffusion-weighted MR captures how water diffuses in the tissue, and this information can be used to estimate the location and the integrity of fiber tracts.
Resting-state fMRI uses the same kind of BOLD data as task-related fMRI (described above), but the participant is not performing a task during scanning. Rather, resting-state fMRI focuses on spontaneous, intrinsic fluctuations of the BOLD response and is thought to represent spontaneous neuronal communication between regions (see Chap. 51, “Intrinsic Brain Activity and Resting State Networks”). Typically participants are instructed to lie still and think of nothing in particular. That is not to say that the participant is not performing a “task” (they may be mentally making a grocery list, planning the rest of their week, or writing their next novel in the scanner), but rather that there is no specific goal-directed activity required; the aim is to “capture the statistical properties of endogenously generated neural activity.” This neural activity is operationalized through the BOLD timecourse, and the statistical properties most often examined are correlations between these timecourses: measures of resting-state functional connectivity (RSFC). Using RSFC analyses, the brain can be parcellated into district, independent networks of regions that show highly correlated timecourses: resting-state networks. These networks have a number of remarkable properties that make them a powerful tool to probe human brain function, both in health and in disease. The networks are highly consistent within and between individuals, and they correspond well with structural connectivity. Moreover, these networks are consistent with activation patterns found during task-based fMRI. Further, the functional connectivity patterns found at rest are predictive of activation patterns seen when subjects are actually performing a task. Thus, even in the absence of an overt task, brain areas appear to always be in “communication,” and this can be assessed and compared with RSFC. These characteristics make resting-state fMRI a very versatile (because the findings are not limited to one particular task) and very easy to acquire (because there is no task that needs to be performed to a specific level). Its task independence and versatility make for very easily comparable datasets. RSFC has proven a powerful method in identifying meaningful, behaviorally relevant networks. Further, it has enabled researchers to consider large-scale interactions between these networks and how these interactions change in various neuropsychiatric disorders.
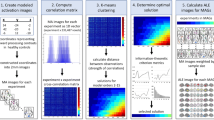
Over the last decade, a variety of data analysis methods for resting-state fMRI has been proposed. The three most common methods are seed-based correlation analysis, independent component analysis, and graph theoretical analysis. In a seed-based correlation analysis , the timecourse from an a priori region of interest (the seed region) is correlated with the timecourse in every other voxel in the brain. For example, placing a seed in the VS identifies a network of regions that are temporally correlated and therefore functionally connected, with this seed (see Fig. 4a). Independent component analysis (ICA) , a blind source separation technique, divides the imaging data into spatial components that show very strong correlations within a given component but that are not correlated with other components (i.e., independent). While the computational mechanisms of seed-based correlation analyses and ICA are very different, the resultant maps and the interpretation of these maps can be quite similar. For example, the executive control network can be identified as an independent component in an ICA or by placing a seed in the dorsolateral prefrontal cortex, a constituent of this network. Both approaches result in a map that includes DLPFC and the ipsilateral posterior parietal cortex. Of the two approaches, ICA is model-free (i.e., data driven) and requires no assumptions, whereas seed-based correlation analyses are best suited to hypothesis-driven studies. A further consideration is that an ICA solution does not always include the specific networks one might be interested in or that it otherwise clumps together several networks into one component. For example, the MCL areas do not typically emerge as a single ICA component even though these regions do show functional connectivity when seeds are placed in the striatum or in the ACC.

Resting-state functional connectivity networks in the MCL system in healthy participants and cocaine users. (a) Resting-state networks from seed-based correlation analysis with seeds (1–6) in multiple nodes of the MCL in cocaine users (red) and control participants (yellow) and areas where such connectivity overlaps between the two populations (orange). (b) Summary of the decreased MCL connectivity in cocaine users compared to control participants. (c) Connectivity between VTA and left striatum is related to years of cocaine use (Figures reprinted, with permission, from © Gu et al. (2010) Elsevier)
A third kind of analysis approaches resting-state fMRI data from a graph theoretical perspective. Graph theory has been used in a myriad of contexts, for example, describing social networks and optimizing routes for mail delivery. By describing networks as graphs, a number of properties can be computed, and these properties have implications for the efficiency of a network, how vulnerable it is to perturbations, and how energy-demanding it is. Applied to the brain, areas (nodes) and their connections (edges; connections can be structural or functional) make up the “graph.” One important node property is its centrality, which is captured by node degree (the number of edges) and node betweenness (the proportion of paths that run through this node). Brain areas with high node centrality are hubs and play an important part in the network structure. Modules are subsets of nodes that densely connected to each other but sparsely to nodes in other modules. An important general property of the entire network or graph is its small world-ness. Complex networks like the human brain adhere to small-world properties; they show high clustering and short path lengths. Small-world structures allow for efficient information transfer on a local (within module) and global scale and are robust to perturbations. Many naturally occurring and man-made networks, such as social networks, electric power grids, and the brain, conform to small-world characteristics. The strength of a graph theoretical approach to network analysis in the human brain is that central concepts from graph theory can be used to capture functionally relevant changes in development and disease. For example, a variety of disorders, such as schizophrenia and heroin dependence, are associated with a breakdown of the brain’s small world structure.
Resting-State Networks in Reward
The use of resting-state functional connectivity to describe human reward networks is relatively recent. The advantage of a network approach to reward processing is that one is no longer limited to the closely defined circuitry described in previous sections of this chapter. We can visualize and identify how reward-related circuitry impacts other networks and functions and how these interactions can go awry in disease.
In this section we discuss how resting-state connectivity networks are used to identify and describe aberrant function in addiction. First, we will discuss functional connectivity with the MCL reward system and how this connectivity is altered in addiction. Then, we will outline a recent triple network model that describes how three large-scale functional resting-state networks interact and how many neuropsychiatric disorders can be described in terms of the breakdown of or altered connections within and between these networks. Network approaches will be discussed with an emphasis on disordered reward processing in addiction.
Resting-State Functional Connectivity with the MCL System
Resting-state functional connectivity investigations of MCL circuitry have emerged in the last few years. Typically, this network is interrogated by placing seeds in one area of the MCL system and comparing connectivity patterns between different groups or conditions of interest. Here, we give some examples of how RSFC using seed-based connectivity analysis can probe MCL network changes in addiction.
Gu et al. (2010) compared resting-state networks between cocaine users and control subjects by placing seeds in six nodes of the MCL system (Fig. 4a). Cocaine users showed reduced connectivity with five of the six seeds: dACC, amygdala, hippocampus, VTA, and MD thalamus (but not with NAcc; see Fig. 4b). More recently, Hu et al. (2015) investigated RSFC networks seeded from different subdivisions of the striatum and compared the resultant maps between cocaine-addicted and control subjects. These differences were then related to measures of impulsivity and compulsive drug use. Results showed that cocaine users have decreased connectivity between striatum and dACC, whereas between striatum and executive control regions such as the DLPFC, there was increased connectivity in users, which correlated with impulsivity. Linking MCL connectivity to the severity of nicotine addiction, Hong et al. (2009) performed a seed-based connectivity analysis in a group of smokers, placing seeds in seven subregions of the cingulate cortex. Connectivity between the dorsal ACC and the VS was significantly negatively related to nicotine addiction severity. This negative relation with addiction severity was independent of whether subjects had nicotine in their system or not, demonstration that the decreased connectivity was related to the trait of addiction and a not a state effect. In a similar vein, Hong et al. (2010) investigated dACC-striatal connectivity in terms of genetic risk for smoking. A risk allele for nicotine addiction was related to decreased connectivity between dACC and striatum and other MCL regions including the extended amygdala. Moreover, smokers had weaker connectivity between these nodes than nonsmokers. Thus, RSFC between dACC and the striatum appears to be related to trait nicotine addiction. Given the dACC’s role in response inhibition and control, this decreased connectivity is consistent with the loss of control reported in these subjects.
These examples show that RSFC with nodes in the MCL system can be used to characterize brain signatures of dysfunctional reward processing in SUD.
Triple Network Model
Harnessing the power of large-scale functional connectivity networks, Menon (2011) proposed a triple network model composed of the executive control network (ECN), the default mode network (DMN), and the salience network (SN; see Fig. 5a). The executive control network , also named central executive network, frontoparietal network, or task-positive network, has its most important nodes in DLPFC and posterior parietal cortex. This network appears to be lateralized, i.e., most studies have identified a distinct left and a right ECN. This network is also dubbed the task-positive network because its composite regions are activated in a wide variety of cognitively demanding tasks, as shown by a large body of task-related fMRI studies. When BOLD activity during any task that requires working memory, the application of rules to solve a problem, or a strong attention to an external stimulus is compared with BOLD activity during rest, these areas virtually always emerge. In contrast, the default mode network or task-negative network has its core nodes in the posterior cingulate cortex and the medial prefrontal cortex, with other nodes in the medial temporal lobe and the bilateral angular gyrus. This network has been called task negative, since these areas are more active during rest periods than while executing a demanding task. There is a negative relationship between the DMN and the ECN, i.e., while one is active the other is less active (Fox et al. 2005). In fact, better performance on cognitively demanding tasks is associated with strongly negative correlations between ECN and DMN. Because the DMN is chiefly defined by what it is not, its actual functions are somewhat elusive, having been referred to as “day dreaming” or “mind wandering.” More specifically, its nodes have been implicated in tasks involving social cognitive processing, value-based decision-making, navigation, and autobiographical memory. Together, the DMN is then thought to engage in self-referential mental processing. Finally, the salience network consists of the bilateral anterior insula and the dorsal anterior cingulate cortex. These brain regions are implicated in detecting, filtering, and aiding in the action of homeostatically relevant emotional, interoceptive, and autonomic information. Other nodes often identified in the salience network are the amygdala and the VTA/SNc. These cortical and subcortical salience nodes are also part of the extended MCL system (see above). The anterior insula and the dorsal ACC are particularly involved in the urge to take drugs and in craving.

Triple network model . (a) Localization of the salience network (SN, yellow), the central executive network (CEN, blue), and the default mode network (DMN, red). (b) Basic interactions in the triple network model. The SN receives and integrates input from sensory and limbic sources and toggles between CEN and DMN based on homeostatic needs. CEN and DMN are inversely related and also relay back to the SN (Figures adapted, with permission, from Menon © (2011) Elsevier)
In the triple network framework, the SN is thought to act as a switch between the externally oriented ECN and the more internally oriented DMN (Fig. 5b). The SN, the nodes of which are part of the MCL system, assigns salience to internal events or external stimuli and biases processing toward the most homeostatically relevant stimuli at the moment. Thus, the SN becomes more engaged with ECN processing when attention should be directed outward and more engaged with DMN processing when attention should be directed inward. For example, when an important task is at hand and environmental stimuli need to be closely attended to, the SN will engage with the ECN and suppress DMN activity. Conversely when a person is hungry, this homeostatic imbalance will be picked up by the SN, which will allow the DMN to become more active and suppress ECN activity. Processing will then be preoccupied with alleviating the deficit state (hunger), and cognitive performance, which is governed by the ECN, will be less effective.
The proper functioning of and interaction between these three networks are necessary for successful goal-directed behavior. This system can break down in many different ways, and such disruption of normal functioning may underlie different neuropsychiatric disorders such as addiction, ADHD, schizophrenia, depression, autism, Alzheimer’s disease, and others. The triple network model provides a framework that can account for both the similarities between disorders (e.g., impaired executive functioning in schizophrenia and depression) and specificities of disorders (e.g., auditory hallucinations in schizophrenia). A less extensive but related between-network framework concerns just ECN and DMN. There, aberrant interactions between these two networks, notably weaker anticorrelations, are linked to poorer functioning.
The triple network model has been applied to a number of different disorders. In the case of addiction, Sutherland and colleagues (2012, 2013) have applied this model to state effects of nicotine addiction. The withdrawal state in smoking is associated with increased irritability, anxiety, and decreased concentration. The SN (especially the insula) tracks the physiological effects of withdrawal and biases processing toward internally oriented DMN processing and away from ECN processing. When the state of withdrawal is lifted by the administration of the abused drug, the SN becomes more engaged with the ECN, biasing resources toward cognitively demanding, goal-oriented tasks. Indeed, when smokers are deprived of nicotine, connectivity between the insula node of the SN and several DMN nodes increases. This increase correlates with more reported symptoms of withdrawal and cravings and with poorer performance on a task that requires executive processing. When nicotine is administered, the SN–DMN coupling becomes normalized, similar to that of a group of nonsmokers (Lerman et al. 2014). Dysfunctional relationship between the ECN and the DMN, which is normally strongly negative, has also been tied to deficits related to withdrawal. Cole et al. (2010) showed increased correlations between the ECN and the DMN in acutely abstinent smokers, with this correlation becoming more negative after nicotine was administered. Janes et al. (2012) also showed increased connectivity between default mode and executive control networks, and this abnormal increased activity correlated with reported difficulty to concentrate. Furthermore, stronger DMN–ECN connectivity was correlated to stronger dorsal striatal responses to smoking cues in a cue-reactivity paradigm. Tying in with the premise of the triple code network, the failure to suppress DMN activity or enhance ECN activity would be predicted to lead to behavioral deficits.
In sum, the triple network model addresses the relationship between three networks defined by RSFC. Such internetwork dynamics are altered in a variety of different neuropsychiatric disorders, including addiction. Importantly, dynamics between networks can be used to identify dysregulated behavior and may be targets for intervention.
Outlook
Arguably there is no single neurological process in the human brain that is not directly or indirectly influenced by reward. We have evolved to maximize our own survival and that of our species, and the (naturally occurring) stimuli that maximize these goals are perceived as rewarding. From this viewpoint, reward should be expected to have far-reaching impacts on most aspects of behavior and the neural processes that underlie behavior.
The study of the neurobiology of reward processes started over 50 years ago with the identification of reward centers in the midbrain and striatum. In the decades since, the MCL circuitry has been described in animals and replicated in humans, and preclinical and clinical models have been used to characterize functional and dysfunctional reward processing. With the advent of noninvasive whole-brain imaging and resting-state fMRI, a large-scale functional network view has become possible. For example, in the triple network model first proposed by Menon, the salience network, which overlaps considerably with the MCL network, detects salient events and toggles flexibly between states of externally oriented processing and internally oriented attention. Thus, processes generated by MCL nodes can have consequences for processing across different networks.
Unsurprisingly, the evolution in perspective from single reward centers to multiple interacting networks has led to a much more nuanced picture of reward processing both in health and in disease. However, moving beyond intracranial self-stimulation and microdialysis studies into the large-scale whole-brain network perspective is not merely an academic endeavor. The multifaceted nature of disordered brain function demands a characterization that is also multifaceted. A network perspective is rooted in the understanding that nearly all major psychiatric problems show a heterogeneous, distributed pattern of abnormalities in structure and function throughout the brain. Thus, in order to tackle disordered reward processing in such disorders as depression, schizophrenia and addiction, an understanding of how not just reward centers but also large-scale networks are affected is necessary.
At present, network approaches to psychiatric disorders are still in their infancy. However, an appreciation for network interactions may be crucial to developing better assessment tools and more effective treatments. For example, as we learn more about reward networks and how they are altered in various brain disorders, signatures of connectivity between these networks could be used as biomarkers. That is, it may be possible to track disease status and recovery progress based on how reward network connectivity is different and what types of node or edge disruptions respond to which treatment. Second, upon understanding these network dynamics and how they change as a function of disease state, these connections themselves can become targets for intervention. Pharmacological interventions can aim to normalize dysfunctional connectivity, or brain stimulation such as deep brain stimulation (DBS), transcranial magnetic stimulation (TMS), and transcranial direct current stimulation (tDCS) may be employed to alter resting-state connectivity, normalize network structure, and hopefully ameliorate disease status or severity.
References
Cole DM, Beckmann CF, Long CJ, Matthews PM, Durcan MJ, Beaver JD (2010) Nicotine replacement in abstinent smokers improves cognitive withdrawal symptoms with modulation of resting brain network dynamics. Neuroimage 52(2):590–599
Craig AD (2011) Significance of the insula for the evolution of human awareness of feelings from the body. Ann N Y Acad Sci 1225(1):72–82
Everitt BJ, Robbins TW (2005) Neural systems of reinforcement for drug addiction: from actions to habits to compulsion. Nat Neurosci 8(11):1481–1489
Falck B, Hillarp NA (1959) On the cellular localization of catechol amines in the brain. Acta Anatomica 38:277–279
Fox MD, Snyder AZ, Vincent JL, Corbetta M, Essen DCV, Raichle ME (2005) The human brain is intrinsically organized into dynamic, anticorrelated functional networks. Proc Natl Acad Sci U S A 102(27):9673–9678
Goldstein RZ, Volkow ND (2002) Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry 159(10):1642–1652
Gu H, Salmeron BJ, Ross TJ, Geng X, Zhan W, Stein EA, Yang Y (2010) Mesocorticolimbic circuits are impaired in chronic cocaine users as demonstrated by resting-state functional connectivity. Neuroimage 53(2):593–601
Haber SN, Knutson B (2010) The reward circuit: linking primate anatomy and human imaging. Neuropsychopharmacology 35(1):4–26
Hong LE, Gu H, Yang Y, Ross TJ, Salmeron BJ, Buchholz B, … Stein EA (2009) Nicotine addiction and nicotine’s actions are associated with separate cingulate cortex functional circuits. Arch Gen Psychiatry 66(4):431–441
Hu Y, Salmeron B, Gu H, Stein EA, Yang Y (2015) IMpaired functional connectivity within and between frontostriatal circuits and its association with compulsive drug use and trait impulsivity in cocaine addiction. JAMA Psychiatry 72(6):584–592
Janes AC, Nickerson LD, Frederick B dB, Kaufman MJ (2012) Prefrontal and limbic resting state brain network functional connectivity differs between nicotine-dependent smokers and non-smoking controls. Drug Alcohol Depend 125(3):252–259
Kaufman JN, Ross TJ, Stein EA, Garavan H (2003) Cingulate hypoactivity in cocaine users during a GO-NOGO task as revealed by event-related functional magnetic resonance imaging. J Neurosci 23(21):7839–7843
Knutson B, Gibbs SEB (2007) Linking nucleus accumbens dopamine and blood oxygenation. Psychopharmacology 191(3):813–822
Knutson B, Greer SM (2008) Anticipatory affect: neural correlates and consequences for choice. Philos Trans R Soc Lond B Biol Sci 363(1511):3771–3786
Knutson B, Adams CM, Fong GW, Hommer D (2001) Anticipation of increasing monetary reward selectively recruits nucleus accumbens. J Neurosci 21(16):RC159
Knutson B, Taylor J, Kaufman M, Peterson R, Glover G (2005) Distributed neural representation of expected value. J Neurosci 25(19):4806–4812
Koob GF, Moal ML (1997) Drug abuse: hedonic homeostatic dysregulation. Science 278(5335):52–58. 8.5335.52
Koob GF, Volkow ND (2010) Neurocircuitry of addiction. Neuropsychopharmacology 35(1):217–238
Lerman C, Gu H, Loughead J, Ruparel K, Yang Y, Stein EA (2014) Large-scale brain network coupling predicts acute nicotine abstinence effects on craving and cognitive function. JAMA Psychiatry 71(5):523–530
McClure SM (2004) Separate neural systems value immediate and delayed monetary rewards. Science 306(5695):503–507
Menon V (2011) Large-scale brain networks and psychopathology: a unifying triple network model. Trends Cogn Sci 15(10):483–506
O’Doherty JP, Dayan P, Friston K, Critchley H, Dolan RJ (2003) Temporal difference models and reward-related learning in the human brain. Neuron 38(2):329–337
Olds J, Milner P (1954) Positive reinforcement produced by electrical stimulation of septal area and other regions of rat brain. J Comp Physiol Psychol 47(6):419
Sutherland MT, McHugh MJ, Pariyadath V, Stein EA (2012) Resting state functional connectivity in addiction: lessons learned and a road ahead. Neuroimage 62(4):2281–2295
Sutherland MT, Carroll AJ, Salmeron BJ, Ross TJ, Hong LE, Stein EA (2013) Down-regulation of amygdala and insula functional circuits by varenicline and nicotine in abstinent cigarette smokers. Biol Psychiatry 74(7):538–546
Volkow ND, Fowler JS, Wang G-J (2002) Role of dopamine in drug reinforcement and addiction in humans: results from imaging studies. Behav Pharmacol 13(5–6):355–366
Wallis JD (2007) Orbitofrontal cortex and its contribution to decision-making. Annu Rev Neurosci 30(1):31–56
Acknowledgments
This work was supported by the NIDA Intramural Research Program. The authors would like to thank Drs. V. Pariyadath, J.R. Fedota and J.L. Gowin for stimulating discussion.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media New York (outside the USA)
About this entry
Cite this entry
Lesage, E., Stein, E.A. (2016). Networks Associated with Reward. In: Pfaff, D., Volkow, N. (eds) Neuroscience in the 21st Century. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-3474-4_134
Download citation
DOI: https://doi.org/10.1007/978-1-4939-3474-4_134
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-3473-7
Online ISBN: 978-1-4939-3474-4
eBook Packages: Biomedical and Life SciencesReference Module Biomedical and Life Sciences