
Abstract
Pulmonary arterial hypertension (PAH) is a rare disease of the pulmonary vasculature characterized by progressive vascular obliteration, right heart failure, and ultimately death. Basic science has focused for the past several decades on identification of underlying molecular causes of this disease, and multiple potential derangements have been identified and some have led to development of drugs to treat PAH. Unfortunately, however, there is no cure for PAH and research continues to identify common mechanisms of development of pulmonary vascular disease and to develop new, more effective therapies. This chapter highlights much of our understanding of the basic pathobiology underlying PAH including genetic underpinnings, vasoactive substances, alterations in cell proliferation and apoptosis, inflammation, thrombosis, and endocrine factors.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Pulmonary arterial hypertension
- Pathogenesis
- Etiology
- Vasoconstriction
- Thrombosis
- Proliferation
- Plexiform lesion
- Nitric oxide
- BMPR2
Genetic Background
No single mechanism has been shown to be sufficient to cause PAH in man. Rather, a combination of factors likely contributes to disease development and risk. While most PAH develops sporadically, registry data show that ≥6 % of subjects with PAH have a first-degree relative with the disease (familial or heritable PAH, HPAH) and these subjects are clinically indistinguishable from those without a family history (sporadic or idiopathic PAH) [1]. Females are disproportionately affected at a 3:1 ratio [2, 3]. An autosomal dominant inheritance pattern with reduced penetrance (10–20 %) was demonstrated prior to discovery of a genetic locus. Early registry data also suggested genetic anticipation, but later reanalysis with more families and longer follow-up intervals suggest that genetic anticipation is not a feature of familial PAH [4]. Early study of HPAH carried hopes of elucidating the underlying genetic and pathobiologic basis of the disease [5, 6].
Through genetic linkage analysis, the locus for inheritance of HPAH was found to be on the long arm of chromosome 2 [7, 8], and later narrowed to a segment of 2q33 [9, 10]. In 2000, using information from the Human Genome Project, candidate genes in this chromosomal region were sequenced in multiple kindreds of HPAH by two independent groups. Heterogeneous mutations in the gene for bone morphogenic protein receptor type II (BMPR2) were discovered including frameshift, missense, and nonsense mutations which span the BMPR2 gene and resultant TGF-β family protein [11–13]. Given that patients with familial and sporadic PAH are clinically indistinguishable [5, 6], genotyping was undertaken in patients with sporadic disease. Fifty patients with sporadic PAH (defined as having no family history suggestive of PAH) were genotyped. BMPR2 mutations were found in 13 of 50 patients including 11 different mutations [14]. With parental genetic analysis, some mutations were de novo while others were demonstrated in a parent despite exclusion of family history of clinical disease by detailed pedigrees. We now know that BMPR2 mutations are present in up to 80 % of subjects with familial PAH and 15 % of those with sporadic PAH [1, 15–17].
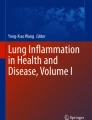
BMPR2 is a member of the TGF-β receptor superfamily which is split into type I and type II receptors; BMPR2 is a type II receptor. All type II receptors are constitutively active serine/threonine kinases. BMPR2 is distinguished from other type II receptors by a long cytoplasmic tail following the kinase domain. There are more than a dozen extracellular ligands which typically have high affinity for the type I receptor and lower affinity for BMPR2. In the presence of extracellular ligand, the type I receptor dimerizes and recruits a type II receptor, forming a functional heterotetrameric receptor complex. The type I receptor is phosphorylated by the constitutively active kinase domain of BMPR2 (or other type II receptor). This signaling family exhibits tissue specificity likely mediated by the specific extracellular ligand and the other receptor proteins present within the heterotetramer as well as multiple known BMP receptor inhibitors (e.g., Noggin, Chordin, Smurf 1). The canonical pathway of downstream signaling involves phosphorylation of Smad1, -5, and -8 by the activated type I receptor. These Smads activate Smad4, a transcription factor. While this is the most ubiquitous description of BMP signaling in the literature, other pathways have been reported and, thus, BMP signaling is much more complex than the canonical pathway alone. BMP signaling also involves mitogen-activated protein kinases (p38MAPK, p42/44MAPK also known as Erk1/2) which activate other nuclear transcription factors, and LIMK which regulates actin polymerization and therefore the cytoskeleton, Tetex-type I, NF-κB, and Src among others [18–21] (Fig. 3.1).

Signaling pathways downstream of BMPR2
Interestingly, it is clear that not all persons with BMPR2 mutation develop PAH and within the same family there is variation in age of onset and disease severity. This variability suggests a “second hit,” perhaps an environmental exposure or additional genetic factor modulating risk of disease development [22]. Recent work has suggested that alterations in expression of the estrogen-metabolizing enzyme CYP1B1 favoring 16-hydroxyestrone over 2-methoxyestradiol may underlie development of PAH in many patients with BMPR2 mutation [23]. Alternative splicing of the normal BMPR2 allele in heterozygous mutation carriers may affect pulmonary vascular disease development [24].
Although BMPR2 mutation is found in many cases of HPAH and some sporadic PAH, we now know that BMPR2 expression is depressed in many forms of PAH including IPAH not associated with mutation [25]. Despite over a decade of research on BMPR2, the exact mechanism through which altered BMPR2 signaling results in the clinical phenotype of pulmonary vascular disease is unknown. Recent work has highlighted the potentially important role that cytoskeletal abnormalities as a function of rac1 defects and metabolic derangements regulated by BMPR2 signaling may play in PAH development [26]. Work continues to explore these and other hypotheses in the development of pulmonary vascular disease related to BMPR2 mutation and signaling depression. Downstream effects of BMPR2 signaling will follow later in this section.
Hereditary hemorrhagic telangiectasia (HHT) is another heritable vascular disorder linked to the TGF-β signaling pathway. Prior to discovery of BMPR2-associated PAH, mutations in two TGF-β signaling proteins (ALK-1 and endoglin) were demonstrated as the genetic basis of HHT [27–29]. Unlike its more common phenotype, a minority of subjects with HHT have PAH that is clinically indistinguishable and pathologically similar to those with IPAH [30, 31]. Mutations of endoglin or ALK-1 have been identified in those families affected by HHT and PAH [29, 31, 32]. PAH in children is often secondary to congenital heart disease, but when this is excluded, they may be more likely to carry an identifiable genetic mutation in BMPR2, endoglin, or ALK-1, reconfirming that different mutations in the TGF-β signaling pathway are often indistinguishable from one another and are frequently found in patients with idiopathic disease [33] (Table 3.1).
Most recently, whole-exome sequencing was used in a family with multiple PAH-affected members in whom no identifiable mutation had been found. All affected family members, and some unaffected members, carried a mutation in the gene encoding caveolin-1 (cav-1), a protein important in formation of caveolae which are cell surface invaginations that modulate cell surface protein endocytosis and recycling. An additional sporadic case of IPAH secondary to cav-1 mutation was also discovered [34]. This study suggests that mutations in cav-1 are a rare cause of PAH and is the first mutation known that does not involve TGF-β signaling directly. Caveolin-1 is known to be important in vascular biology and physiology because it is a crucial negative regulator of eNOS activity [35, 36]. Recent studies using cav-1 and eNOS knockout mice suggest that the lack of cav-1 results in excessive eNOS activity associated with generation of ROS and inactivation of PKG (the major downstream target of NO-generated cGMP) by nitrosylation [37]. Cav-1 knockout mice develop cardiovascular disease including spontaneous PAH and RV failure when exposed to chronic hypoxia [38–40].
Vasoactive Substances and Imbalance
The hallmarks of pulmonary hypertension are elevated pulmonary arterial pressure (PAP) and vascular resistance (PVR). Patients with what is now categorized as IPAH were described early on in biopsy and autopsy series as those with normal lung parenchyma and pathologic findings limited to the small muscular arteries [41]. A logical area of investigation was the balance of vasoactive substances.
Vascular smooth muscle (SMCs) and endothelial cells (ECs) participate in regulation of blood flow in both the systemic and pulmonary vascular bed. The regulation of pulmonary circulation is unique to that of the systemic circulation especially in regard to hypoxic pulmonary vasoconstriction (see Chap. 4). While hypoxic pulmonary vasoconstriction is effective and necessary to maintain homeostasis in health and disease, chronic lung diseases featuring hypoxemia are a common cause of PH (WHO Group 3). While there is still debate as to the mechanism of hypoxic pulmonary vasoconstriction, research in this area has led to a better understanding of pulmonary physiology and a wealth of knowledge that has been adapted to the study of pulmonary vascular disease broadly.
It has long been known that histologic specimens from patients with PAH show normal lung parenchyma but intimal and medial thickening of the vascular wall and intraluminal findings of cellular proliferation and often thrombotic material [41–43]. In addition to pathologic findings limited to pulmonary vessels, an early observation was an acute response to administration of pulmonary vasodilators leading to the theory that the underlying pathobiologic mechanism was a “vasoconstrictive factor” [44–46].
Nitric Oxide
In the 1950s Paul Wood developed a classification scheme for PH not dissimilar to our current WHO classification. He was interested in vasoconstriction as a possible cause of elevated PAP and PVR. In a subject with mitral stenosis and PH, he administered acetylcholine, a known vasodilator. He noted that PAP and PVR fell and systemic pressure increased, presumably from increased cardiac output. This was shown to be reproducible in patients with PAH and PH secondary to mitral stenosis or COPD, but not in Eisenmenger’s syndrome [46]. Through elegant experiments in several labs over the ensuing three decades, acetylcholine’s effect was demonstrated to be via an endothelial dependent mechanism with the effector compound being nitric oxide (NO) from ECs and the target being the vascular SMC [47, 48]. Subsequently it was shown that strips of excised but still endothelialized PA from patients with Eisenmenger’s syndrome and chronic lung disease with secondary PH had blunted vasodilatory responses to acetylcholine, but preserved response to nitroprusside (an NO donor) [49, 50]. Endothelial dysfunction was proposed as the mechanism.
Nitric oxide is a short-lived powerful vasodilator produced from metabolism of L-arginine by the enzyme nitric oxide synthase (NOS). In the lung, endothelial NOS (eNOS) is the predominant isoform. Nitric oxide exerts its effect by increasing cyclic guanosine monophosphate (cGMP) within PASMCs which causes relaxation by activating cGMP-dependent protein kinase (PKG) that then acts on a variety of downstream targets to decrease intracellular calcium concentration. Inhaled NO reduces PAP and PVR in some subjects with PH [51]. Lung specimens from subjects with PAH show reduced or absent eNOS expression. Also, eNOS and endothelin-1 (a vasoconstrictor discussed below) have inverse staining patterns in the endothelium of PAH subjects compared with controls [52]. Subjects with PAH also have higher levels of ADMA (an eNOS inhibitor) and reduced expression of DDAH2 (an enzyme which metabolizes ADMA) in lung specimens compared to controls [53]. Taken together, these findings suggest that endothelial derived NO is reduced in PAH. Whether reduced NO availability is a cause or effect of pulmonary vascular disease is uncertain, but it has led to development of pharmacologic agents designed to increase pulmonary vascular cGMP levels. A family of phosphodiesterases (PDE) degrade cGMP and cAMP. PDE5 is the predominant isoform in pulmonary vascular smooth muscle and PDE5-specific inhibitors such as sildenafil and tadalafil have been shown to reduce PAP in animal models of pulmonary hypertension and in humans with PAH [54–56]. L-arginine has been used with limited success in the treatment of PAH and has been shown to reduce PAP and PVR in some subjects [57, 58]. Recently, soluble guanylate cyclase stimulators that act synergistically with NO to increase cGMP synthesis have also been approved for the treatment of PAH (see Chap. 15 for more discussion on cGMP modifiers for the treatment of PAH).
Prostacyclin
Prostacyclin is also produced by ECs and relaxes pulmonary and systemic smooth muscle [56]. Rubin administered prostacyclin to subjects with PAH and reported favorable acute hemodynamic changes [59] and later a favorable randomized trial of continuous IV prostacyclin therapy [60]. Despite the efficacious effects of prostacyclin (see Chap. 13), it was not known at that time whether abnormalities of prostacyclin synthesis contributed to the pathophysiology of PAH. Further studies found that thromboxane, that is derived from the same synthetic pathway as prostacyclin, but is a known procoagulant and vasoconstrictor, is increased in subjects with PH, whereas prostacyclin metabolites are decreased. The ratio of thromboxane:prostacyclin is increased in subjects with PH of any cause relative to controls [61]. This suggests increased platelet activation and lends further support to the presence of endothelial dysfunction in subjects with PH.
Endothelin-1
Endothelins (ET-1, ET-2, and ET-3) are another potent mediator of pulmonary vasoconstriction and are also SMC mitogens. Endothelin receptors ETA and ETB are both present in the pulmonary vasculature, although their relative expression varies depending on vessel size [62]. The action of ET-1 on ETA receptor on PASMCs causes vasoconstriction and mitogenesis. The ETB receptor has a less clear role in vascular tone, but plays an important role in clearance of ET-1. ETA receptor blockade in experimental conditions reliably attenuates endothelin-induced vascular SMC mitogenesis [62–66] and improves symptoms, exercise tolerance, and hemodynamic parameters in patients [67–71].
In vivo, plasma levels of ET-1 are higher in subjects with PAH or secondary PH compared to controls and are higher in the arterial than venous circulation [72, 73] suggesting increased production or reduced clearance within the pulmonary bed. Compared to controls, PAH subjects have increased ET-1 gene and protein expression in lung tissue which is concentrated in areas of vascular remodeling, especially plexiform lesions [74, 75]. Endothelin effects clearly contribute to pulmonary vascular disease but whether ET-1 overexpression initiates or only propagates pulmonary vascular disease is unknown. Likely, initial endothelial injury results in maladaptive ET-1 release which promotes mitogenesis of vascular SMCs and fibroblasts in patients already prone to uncontrolled cellular proliferation (i.e., those with BMPR2 mutation) or in those in whom endothelial injury is constantly present (i.e., congenital cardiac shunt). Regardless of mechanism, inhibition of the endothelin system has offered another attractive therapeutic target in the treatment of pulmonary hypertension (see Chap. 14).
Serotonin
The “serotonin hypothesis” of PAH was borne out of the observation that certain serotonergic medications are associated with PAH development [76–79]. Serotonin or 5-hydroxytryptamine (5-HT) causes intense vasoconstriction of systemic and pulmonary vessels and also acts as a mitogen for vascular SMCs [80, 81]. Within the circulation 5-HT exists almost exclusively within platelets for release “on demand,” and plasma levels are normally very low. After release from activated platelets, 5-HT is transported into cells including ECs and SMCs via the 5-HT transporter (SERT or 5-HTT) and metabolized by monoamine oxidase. 5-HT1B is the receptor most important for pulmonary vasoconstriction [82, 83].
Experimental disruptions of the 5-HT system have yielded some understanding of its role in human PAH but have not resulted in any therapeutic breakthroughs. Some studies have shown subjects with PAH to have higher concentrations of 5-HT in plasma and within platelets compared to controls which persist after lung transplantation [84]. Polymorphisms of the 5-HTT (the “LL” variant) are likely not associated with PAH in the largest and most recent studies [85–87]. PASMCs from subjects with PAH have higher expression of 5-HTT and are more susceptible to 5-HT-mediated mitogenesis which is reduced by 5-HTT inhibition [85]. Experimental overexpression of 5-HTT causes worsened PH phenotype in animals [88], and 5-HTT knockout mice are protected from pulmonary vascular disease [89]. There are various medications which target the 5-HTT with varying affinities, these being the selective serotonin reuptake inhibitors (SSRIs) commonly employed in the treatment of depression and anxiety. Proliferation of vascular SMCs in response to 5-HT in vitro is inhibited by SSRIs [85, 90]. SSRIs protect against PH in the chronic hypoxia mouse model [91]. In terms of receptors, it is known that the 5-HT1B receptor is involved in pulmonary vasoconstriction and sumatriptan, an FDA-approved medication for treatment of migraine and 5-HT1B/D receptor agonist, causes acute rise in PA pressure [83, 92]. Knockout of the 5-HT2B receptor and knockout or antagonism of the 5-HT1B receptor protect rodents from PH [93, 94]. Further study of the serotonin system and its role in pulmonary vascular disease is ongoing.
Solute Channels
Potassium channels regulate resting membrane potential and voltage-gated Ca2+ influx. Calcium is essential for both vascular SMC contraction and proliferation and higher cytosolic Ca2+ concentration leads to both. Subjects with IPAH have reduced PASMC expression and activity of voltage-gated KV channels [95, 96] which promotes membrane depolarization and Ca2+ influx. Resting and stimulated cytosolic Ca2+ concentrations are known to be higher in PASMCs from subjects with IPAH than controls [95, 97] and this is likely due to both the KV channel defect and upregulation of several Ca2+ channels and regulators [97–100].
Multiple circulating and autocrine vasoactive substances, some having mitogenic potential, are altered in subjects with PAH. The nitric oxide, endothelin, and prostacyclin systems have met realization of clinically useful pharmacologic targets. Further study of other vasoactive mediators may lead to additional treatment options which are sorely needed. There is substantial interaction of vasoconstriction and cellular proliferation which is discussed in the next section.
Cellular Proliferation and Vascular Remodeling
In addition to vasoconstriction, cellular proliferation is one of the major underlying commonalities of PAH pathogenesis. Pulmonary vascular remodeling and proliferation are manifested in all components of the vessel wall: media thickening with vascular smooth muscle cell (SMC) hypertrophy and proliferation, intimal thickening and fibrosis, and intraluminal obstruction of proliferative endothelial cells (ECs) and plexiform lesions. Regulation of the growth and differentiation of ECs and vascular SMCs has been studied extensively in health and disease. Multiple mediators are known, some affecting both ECs and SMCs. Several of these with a focus on their specific role in pulmonary vascular disease will be reviewed herein. Some small molecules, such as 5-HT and ET-1, with prominent pulmonary vasoconstriction properties which have already been discussed also modulate growth and differentiation.
Vascular Endothelial Growth Factor
Vascular remodeling with cellular proliferation is most apparent at plexiform lesions. These histologic lesions are unique to PAH (WHO Group 1). They are composed of proliferating and apoptosis-resistant ECs and other cellular components which have been debated to be myofibroblasts, SMCs, or undifferentiated mesenchymal cells [98]. Within plexiform lesions expression of vascular endothelial growth factor (VEGF), its receptor (VEGFR), HIF-1α, and other remodeling genes are increased [101–103]. VEGF is also increased in plasma samples from subjects with IPAH compared to controls [104]. While VEGF and VEGFR are required for normal angiogenesis, they are also an exploited pathway of malignant-transformed cells. Given increased expression of VEGF and VEGFR within plexiform lesions a cancer paradigm of PAH developed, suggesting that excessive angiogenesis due to a molecular defect within a clone of cells leads to the clinically manifest disease. Preclinical research on VEGF signaling and PH has given conflicting data and has not yet arrived at a therapeutic modality. Experimental overexpression of VEGF is protective in some PH models [105, 106]. Consistent with this, VEGFR inhibition via receptor blockade (with SU5416) in the chronic hypoxia model results in worsened PH and increased EC proliferation [107]. A different VEGF signaling inhibitor, the multikinase inhibitor sorafenib, reduces progression of established PH in monocrotaline-treated rats [108] and prevents PH development in rats exposed to chronic hypoxia and SU5416 [109]. Taken together, this indicates that VEGF signaling is important in vascular maintenance and interrupting the pathway can worsen pulmonary vascular disease phenotype. However, some downstream effects of VEGF signaling may ultimately be maladaptive. The complex relationship of VEGF signaling in pulmonary vascular disease animal models and varying results of treatment approaches has recently been reviewed [110]. Further study is needed in this intriguing area before clinical application can be developed for treatment of PAH.
Mitogens
Several mitogens have been evaluated in PAH including platelet-derived growth factor (PDGF), basic fibroblast growth factor (bFGF), and epidermal growth factor (EGF). While the precise function of PDGF in vivo is still somewhat of a question, it is known as a potent vascular SMC mitogen in vitro which also causes SMC and fibroblast migration. It has been implicated in the pathogenesis of multiple vascular and fibroproliferative diseases [111]. PDGF and its receptor (PDGFR) are increased in vessels of lung specimens from subjects with PAH [112, 113]. bFGF is another mitogen for ECs and vascular SMCs and has been found to be increased in patient samples [114] and overexpressed in patient-derived PA ECs. Interference of bFGF signaling via siRNA for bFGF reduces PASMC proliferation in vivo and in vitro [115]. EGF and TGF-α both activate EGFR and cause growth and vascular remodeling, a pathway exploited in some tumors and targeted pharmacologically. Overexpression of TGF-α leads to pulmonary vascular disease in mice through EGFR signaling [116], and EGFR is overexpressed in the monocrotaline PH model. Inhibition of this pathway is effective in vitro [117] and prevents development of monocrotaline-induced PH in rats, but is ineffective in a chronic hypoxia model [118]. In addition, EGFR expression is no different in clinical specimens of PAH patients versus controls [118]. EGF inhibition therefore has limited therapeutic promise.
Tyrosine Kinases
Many of the above substrates and receptors signal through tyrosine-kinase mechanisms. Multiple tyrosine-kinase inhibitors exist. One of the earliest, imatinib (Gleevec), has been studied in basic and clinical studies of PAH. Imatinib blocks PDGF-mediated PASMC proliferation. However, it does not mitigate the effects of many other known growth factors (VEGF, EGF, bFGF). In monocrotaline-treated or chronic hypoxic rats, imatinib improves pulmonary vascular disease via reduced downstream signaling of PDGF [113]. There are several clinical case reports of beneficial effect of treatment with imatinib (Gleevec) [119–121]. A small phase II study in PAH demonstrated a decline in PVR with imatinib compared to placebo [122]. A subsequent phase III study in PAH patients already on combination PAH therapy demonstrated improvement in 6-min walk distance and in PVR, but there was a greater incidence of hospitalization in the imatinib group and increased risk of cerebral hemorrhage in imatinib-treated patients who also were receiving warfarin therapy [123]. Other multi-targeted tyrosine kinase inhibitors have been considered in PAH, but predicting their clinical effects and avoiding off-target effects remain of concern. The importance of such considerations is exemplified by the finding that dasatinib can cause pulmonary hypertension and pleural effusions in patients being treated for malignancy [124]. These issues are discussed further in Chap. 17.
TGF-β Signaling
As discussed previously, mutations in the gene encoding BMPR2 are the genetic basis of disease in most cases of familial and many cases of sporadic PAH [1, 11, 12]. The TGF-β family of receptors including BMPR2 is highly evolutionarily conserved. BMPR2 is required for embryogenesis and alteration of signals downstream of BMPR2 result in defects in angiogenesis [125]. BMP signaling has been studied extensively since the discovery of a link between BMPR2 mutation and PAH. The major downstream pathways of BMPR2 include (1) Smad1/5/8 which signals through the common Smad2 transcription factor, (2) p38MAPK and Erk1/2, (3) Src, and (4) LIMK, among others. Smad 1/5/8 signaling is facilitated by cGMP activation of PKG. Activated PKGI binds to and phosphorylates BMPR2. In response to ligand binding, PKG1 detaches from BMPR2 and associates with activated Smads and then translocates to the nucleus where it regulates transcription as a nuclear cofactor for Smads [126]. Recent studies demonstrate that Smad signaling is impaired in mice with reduced PKG expression and activation of PKG by cGMP improves Smad signaling in a rat model of PAH [127].
The cellular effects of BMP stimulation and its disruption are dependent on cell type. It is helpful to review the effects of normal and abnormal BMP signaling in SMCs and ECs separately.
In proximal PASMCs, BMP inhibits proliferation, and promotes apoptosis and SMC phenotype differentiation [128–130]. Peripheral PASMCs may have a different response to BMP stimulation, responding with proliferation [130]. BMP’s effect on control of proliferation is mediated through Smad signaling [128, 130]. Subjects with IPAH have less Smad1 activation than controls and unchanged p38MAPK/Erk activation, resulting in an unopposed proliferative stimulus [128, 130].
In contrast to the predominant effect on PASMCs, BMPR2 activation in endothelial cells promotes survival, proliferation, and migration [131, 132]. This effect is also mediated through Smad signaling. BMPR2 gene silencing results in EC apoptosis and makes the endothelium susceptible to damage. In vivo, this loss of endothelial integrity may allow PASMCs to be exposed to serum growth factors and proliferate in the absence of BMPR2-mediated growth regulation. In addition, increased endothelial apoptosis may select for apoptosis-resistant clones which have been demonstrated in plexiform lesions of PAH subjects [98].
Notch Signaling
The Notch family of receptors are single transmembrane proteins which bind to ligands on the surface of adjacent cells. Upon this stimulus, the intracellular portion of Notch is cleaved and translocates to the nucleus where it acts as a transcription factor. Notch ligands are primarily expressed on ECs and the receptors allow cell-cell communication affecting vascular development [133]. There are four known Notch receptors (Notch1–4). Notch3 is expressed only in arterial vascular SMCs and is crucial for development of normal arterial morphology, as evidenced by the study of Notch3-null mice which lack a normal arterial muscular layer [134, 135]. Notch3 overexpression results in vascular SMC proliferation that continues post-confluence in vitro [136]. Li et al. [137] have studied the association of Notch3 and PAH in both humans and animal models, finding increased expression at an mRNA and protein level as well as increased HES-5, a downstream effector. Inhibition of this pathway is protective in the chronic hypoxic PH model. Notch is also known to interact with other pertinent signaling pathways including Smad1, HIF-1α, and VEGF [133, 138].
The components of the vessel wall are under constant stress and appropriate regulation of proliferation, migration, and apoptosis are required to maintain homeostasis in health and under insults of disease. Cellular regulation of these processes is complex and varies not only by cell type, but also by tissue bed. VEGF, VEGFR, BMPR2, and Notch are required for formation of normal vessels during development. When injury to the vascular wall occurs, autocrine and paracrine signals such as VEGF, ET-1, PDGF, EGF, 5-HT, and BMP (and likely many others) respond to direct cellular response. Dysregulation of these adaptive signals in PAH subjects leads to abnormal PASMC and EC proliferation. The number of PAH therapies that target these pathways is minimal. A greater molecular understanding of the intricate balance of this proproliferative/antiproliferative balance has been attained in the last two decades, but research is ongoing and translation to clinical care is still needed.
Inflammation and Infection
Within WHO Group 1, there is a subset of patients with associated inflammatory, immune, or infectious conditions known to result in pulmonary vascular disease [139]. The most common of these are the connective diseases (CTD) and infectious diseases HIV and schistosomiasis. The study of pulmonary vascular disease associated with these diseases has uncovered links with inflammation and immunity. At the same time, study of patients with IPAH and HPAH has also revealed elements of dysregulated inflammation. Thus, there appears to be a strong influence of the immune system on pulmonary vascular disease onset and progression.
Pulmonary hypertension is a frequent manifestation of multiple autoimmune conditions [139] with systemic sclerosis being the most common. Up to 12–40 % of patients with systemic sclerosis will develop PAH and this complication portends a poor prognosis [140, 141]. Systemic sclerosis and other CTDs are characterized by circulating autoantibodies, and clinical evaluation for these conditions is indicated in a patient with newly diagnosed PAH. Study of patients with IPAH has also revealed the presence of autoantibodies, primarily anti-Ku, which in one study was found in 23 % of presumed IPAH patients. Raynaud’s phenomenon, a common feature of systemic sclerosis, was frequently seen (39 %) in the same study [142].
Inflammation is a prominent feature of the pathology of pulmonary vascular disease. Pathologic review of several cohorts has demonstrated B- and T-lymphocytes (CD8+ and CD4+), macrophages, mast cells, and dendritic cells concentrated near areas of vascular remodeling [143–145]. Subjects with IPAH have increased circulating regulatory T-cells compared with subjects with CTEPH or normal controls but lower numbers of them in lung specimens [144–146]. There may also be alterations in natural killer (NK) cell population and function [147]. Any of these changes in circulating immune cell populations may result in altered cytokine response and inadequate control of immune activation manifested in the pulmonary vascular bed. In fact, multiple cytokines are known to be increased in PAH [148–150]. IL-6 levels are increased, correlate with clinical outcome, and do so better than hemodynamics or 6-min walk distance in some studies [149, 150]. Injection of IL-6 [151] or IL-6 overexpression [152] in mice results in PH, and knockout of IL-6 is protective against chronic hypoxic PH [153]. CX3CL1 (also known as fractalkine) and its soluble receptor (CX3CR1) are increased in the plasma and pulmonary endothelium of subjects with IPAH. CX3CL1 and CCL2 expression are elevated in plasma and in pulmonary ECs of PAH patients compared to controls. These chemokines increase leukocyte adhesion to ECs, further propagating perivascular inflammation. Increased cytokine production may be a central component of PAH but its temporal relation to disease development is uncertain.
Some infectious diseases are causally related to PAH development. In the USA, HIV is the most common, whereas schistosomiasis may be the most common cause of PAH worldwide. Up to 1 in 200 AIDS patients will develop PAH, meaning that HIV patients have up to a 600-fold higher incidence of PAH than the general population; [154, 155]. These patients have plexiform lesions indistinguishable from those seen in IPAH. However, the HIV virus has not itself been identified in pulmonary vessels [156, 157]. Indirect effects of HIV infection, either mediated by immune dysregulation or viral proteins, are proposed as mechanisms of pulmonary vascular disease. Several pertinent HIV proteins have been implicated, the most studied being the protein Nef. The predominant animal model of HIV, simian immunodeficiency virus (SIV)-infected macaques, has a low penetrance of pulmonary vascular disease. When infected with a chimeric HIV-SIV virus containing HIV Nef, they develop plexiform lesions containing Nef [158]. Nef, which has a soluble form, can enter non-HIV-infected cells via the chemokine receptor, CXCR4. In addition to lymphocytes, CXCR4 is present on ECs and may allow entry of Nef without direct infection of ECs by HIV virus [159]. Indeed, Nef has been demonstrated in pulmonary ECs of HIV-associated PAH subjects [150]. Nef increases IL-6 expression and multiple proproliferative signals including p38MAPK [155] which could promote PH development. More recently, study of the HIV envelope protein (Env) using SHIV-env in macaques also showed increased pulmonary vascular lesions in those animals compared to SIV-infected animals [160]. Exogenous Env protein has been shown to induce endothelial cell ET-1 expression. It is uncertain if this or another mechanism may underlie its role in HIV-associated PAH development. HIV proteins gp120 and Tat affect pulmonary ECs in vitro and could play a role, but data is preliminary [161, 162].
HHV-8 is a gamma-herpesvirus associated with Kaposi’s sarcoma which is a proliferative vascular lesion seen in patients with HIV infection. HHV-8 encodes a protein similar to IL-6 which induces VEGF expression explaining its disease manifestation. One group reported HHV-8 detected in lung specimens of 10 of 16 patients with IPAH and none of a matched secondary PAH cohort [163]. Since this study, multiple groups have failed to identify HHV-8 infection in various PAH cohorts [164–168]. As it stands, HHV-8 is felt to be unlikely to cause pulmonary vascular disease on its own.
Schistosomiasis is rare in the USA, but probably the most common cause of PAH worldwide. In chronic infections, endemic Schistosoma blood flukes reside in the mesenteric venous system and shed eggs and antigens causing an intense granulomatous reaction. This results in periportal fibrosis and portal hypertension, a syndrome known as hepatosplenic schistosomiasis [169, 170]. Hepatosplenic schistosomiasis precedes pulmonary vascular disease development, but the stepwise progression is uncertain. Regardless of cause, the histology is similar to that of other forms of PAH [171]. Mechanistic studies of PAH secondary to schistosomiasis are limited. One study of lung specimens from subjects with schistosomiasis and PAH failed to demonstrate the presence of egg antigens in pulmonary vessels, but it is uncertain whether antihelmenthic treatments may have eliminated their parasite burden [169, 171, 172]. Intense inflammation in this disorder may result in early pulmonary vascular changes and with continued immune activation, progression to an irreversible vasculopathy of the pulmonary bed. IL-13 has recently been implicated as a mediator of pulmonary vascular disease in schistosomiasis-associated PAH [173]. Schistosomiasis-associated PH is further discussed in Chap. 7.
Thrombosis and Hypercoagulability
Thrombosis has been a proposed central mediator or pulmonary vascular disease for decades. Pulmonary vascular thrombosis and thrombotic arteriopathy are common pathologic findings of PAH, found in 30–56 % of specimens [43, 174–176]. While incomplete evaluation for CTEPH in some studies may reduce the true incidence of thrombotic lesions, it is clear that many subjects with IPAH have some degree of pulmonary vascular thrombosis. Similar thrombotic lesions have been demonstrated in patients with congenital heart disease complicated by PAH, portopulmonary hypertension, and aminorex use [177]. These lesions are described as eccentric with post-thrombotic intimal fibrosis and recanalization. These changes are felt to be the same whether the cause was embolus or in situ thrombus formation [42, 178]. Much debate exists as to whether these real pathologic findings are an epiphenomenon of pulmonary vascular disease or rather a true contributor to disease development and/or progression.
In addition to circulating coagulation factors, the endothelium and its interaction with platelets are integral components of both prothrombotic and antithrombotic pathways [177]. While characterized inherited hypercoagulable states are no more common in patients with PAH or CTEPH than the general population [179], multiple studies demonstrate abnormalities in the prothrombotic and antithrombotic systems. In general, the pro/antithrombotic balance is tipped in favor of coagulation. Circulating von Willebrand factor (vWF) is increased in all forms of PAH [180], but its function may be reduced due to alterations of vWF multimer distribution [177, 180–182]. High shear stress in the pulmonary vasculature may contribute to depletion of high-molecular-weight multimers of vWF in PAH, akin to what occurs in the setting of left ventricular assist devices. vWF abnormalities due to endothelial dysfunction may promote platelet dysfunction and release of multiple mediators. For example, patients with IPAH have higher urinary thromboxane metabolites [61] and plasma 5-HT [83, 84]. Markers of thrombin action and fibrin formation (d-dimers, fibrinopeptide A, fibrin degradation products) are also elevated, but so are the anticoagulant/fibrinolytic factors such as thrombomodulin, tissue factor pathway inhibitor, and PAI-1, a fibrinolytic inhibitor [180, 183, 184].
Control of hemostasis is a complex, highly regulated system. The endothelium is a central component of this system and must balance both constant free-flowing blood and the possibility of endothelial disruption. Multiple lines of evidence suggest that pulmonary vascular disease, especially IPAH or HPAH, demonstrate multiple abnormalities of these systems which may lead to a procoagulant phenotype. Circumstantial evidence that anticoagulation may be beneficial in patients with PAH [185, 186] suggests that a procoagulant phenotype may at least play a role in continued or worsening pulmonary vascular disease.
Endocrine Factors
Rising rates of obesity and metabolic disease in the developed world coupled with recent registry data showing high rates of obesity in PAH [187] has brought intense interest into how endocrine factors may affect the pulmonary vasculature. The first observations were of high incidence of insulin resistance and glucose intolerance in subjects with PAH [188, 189], but other data has recently suggested that dyslipidemia may also play a role [190]. Animal models of PAH have been used to help define if these endocrine factors may play a role in disease promotion. Animal models of obesity, such as adiponectin-deficient mice and ApoE knockout mice, spontaneously develop PH [191, 192]. Moreover, pulmonary vascular disease is reversed by peroxisome proliferator activator receptor gamma (PPARγ) activation with rosiglitazone. BMPR2 signaling has been shown to be a key downregulator of PPARγ-mediated transcription and likely plays a role in promotion of insulin resistance in PAH [193]. Recently, we have demonstrated that in a model of HPAH using transgenic overexpression of mutant BMPR2, insulin resistance is present and worsened insulin resistance through a high-fat diet results in increased pulmonary vascular disease [194]. How insulin signaling is modified by BMPR2 mutation is currently under investigation, and it is presently unknown if reversing insulin resistance in humans with PAH may be a therapeutic option for this disease.
Other endocrine factors, such as estrogen signaling, are also implicated in PAH. The impressive female predominance in PAH has led to the hypothesis that estrogen may promote PAH development [2, 3, 195]. While there is extensive data in chronic hypoxic and monocrotaline models that estrogen and its metabolite 2-methoxyestradiol attenuate PH [196–200], these findings have not been replicated in human specimens or transgenic models of PAH. Indeed, there is growing evidence that estrogen may worsen pulmonary vascular disease in certain animal models that may more closely recapitulate human disease [80, 201–203]. At the same time, recent studies suggest that in patients with PAH, female sex is associated with better right ventricular ejection fraction, cardiac index, and pulmonary hemodynamics than male sex [204–206] and that estrogen and its metabolites may improve right ventricular function in healthy patients and those with cardiovascular diseases [207]. These findings may explain the better overall survival in women than in men with PAH [208]. Further study is needed to reconcile the potentially beneficial effects of estrogens in some animal models with detrimental effects in others and the female predominance of PAH in human disease.
Conclusion
In summary, there are many signaling cascades, exposures, and molecules implicated in PAH development and promotion. While advances have been made in developing successful drug therapy for this disease, none has resulted in a cure. Unfortunately, we do not understand the critical initiating event in PAH, nor how to interrupt it. Another unknown is whether human pulmonary vascular disease is reversible once established. These fundamental questions will need to be answered before curative or disease-altering therapy is available to patients with this devastating disease.
Abbreviations
- 5-HT:
-
5-Hydroxytryptamine or serotonin
- 5-HTT:
-
5-Hydroxytryptamine (serotonin) transporter
- ADMA:
-
Asymmetric dimethylarginine
- ALK:
-
Activin receptor-like kinase
- AVM:
-
Arteriovenous malformation
- bFGF:
-
Basic fibroblast growth factor
- BMP:
-
Bone morphogenic protein
- BMPR2:
-
Bone morphogenic protein receptor type 2
- Cav-1:
-
Caveolin-1
- cGMP:
-
Cyclic guanosine monophosphate
- COPD:
-
Chronic obstructive pulmonary disease
- CTD:
-
Connective tissue disease
- CTEPH:
-
Chronic thromboembolic pulmonary hypertension
- DDAH:
-
Dimethylarginine dimethyaminohydrolase
- EC:
-
Endothelial cell
- EGF:
-
Epidermal growth factor
- EGFR:
-
Epidermal growth factor receptor
- ENG:
-
Endoglin
- ET:
-
Endothelin
- GDF:
-
Growth/differentiation factor
- HHT:
-
Hereditary hemorrhagic telangiectasia
- HHV-8:
-
Human herpesvirus 8
- HIF:
-
Hypoxia-inducible factor
- HIV:
-
Human immunodeficiency virus
- HPAH:
-
Heritable pulmonary arterial hypertension
- IPAH:
-
Idiopathic pulmonary arterial hypertension
- IV:
-
Intravenous
- KV :
-
Voltage-gated potassium channel
- NO:
-
Nitric oxide
- NOS:
-
Nitric oxide synthase
- PA:
-
Pulmonary artery
- PAH:
-
Pulmonary arterial hypertension
- PAP:
-
Pulmonary arterial pressure
- PASMC:
-
Pulmonary artery smooth muscle cell
- PDE5:
-
Phosphodiesterase type 5
- PDGF:
-
Platelet-derived growth factor
- PH:
-
Pulmonary hypertension
- PPARγ:
-
Peroxisome proliferator-activator receptor gamma
- PVR:
-
Pulmonary vascular resistance
- RV:
-
Right ventricle
- siRNA:
-
Small interfering RNA
- SIV:
-
Simian immunodeficiency virus
- SMC:
-
Smooth muscle cell
- SSRI:
-
Selective serotonin reuptake inhibitors
- TFG-α:
-
Transforming growth factor α
- TGF-β:
-
Transforming growth factor β
- VEGF:
-
Vascular endothelial growth factor
- VEGFR:
-
Vascular endothelial growth factor receptor
- vSMC:
-
Vascular smooth muscle cell
- vWF:
-
von Willebrand factor
- WHO:
-
World Health Organization
References
Fessel JP, Loyd JE, Austin ED. The genetics of pulmonary arterial hypertension in the post-BMPR2 era. Pulm Circ. 2011;1(3):305–19. PubMed PMID: 22140620, Pubmed Central PMCID: PMC3224422.
Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173(9):1023–30. PubMed PMID: 16456139.
Badesch DB, Raskob GE, Elliott CG, Krichman AM, Farber HW, Frost AE, et al. Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest. 2010;137(2):376–87. PubMed PMID: 19837821.
Larkin EK, Newman JH, Austin ED, Hemnes AR, Wheeler L, Robbins IM, et al. Longitudinal analysis casts doubt on the presence of genetic anticipation in heritable pulmonary arterial hypertension. Am J Respir Crit Care Med. 2012;186:892. PubMed PMID: 22923661.
Rich S, Dantzker DR, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med. 1987;107(2):216–23. PubMed PMID: 3605900.
Loyd JE, Primm RK, Newman JH. Familial primary pulmonary hypertension: clinical patterns. Am Rev Respir Dis. 1984;129(1):194–7. PubMed PMID: 6703480.
Morse JH, Jones AC, Barst RJ, Hodge SE, Wilhelmsen KC, Nygaard TG. Mapping of familial primary pulmonary hypertension locus (PPH1) to chromosome 2q31-q32. Circulation. 1997;95(12):2603–6. PubMed PMID: 9193425.
Nichols WC, Koller DL, Slovis B, Foroud T, Terry VH, Arnold ND, et al. Localization of the gene for familial primary pulmonary hypertension to chromosome 2q31-32. Nat Genet. 1997;15(3):277–80. PubMed PMID: 9054941.
Machado RD, Pauciulo MW, Fretwell N, Veal C, Thomson JR, Vilarino Guell C, et al. A physical and transcript map based upon refinement of the critical interval for PPH1, a gene for familial primary pulmonary hypertension. The International PPH Consortium. Genomics. 2000;68(2):220–8. PubMed PMID: 10964520.
Deng Z, Haghighi F, Helleby L, Vanterpool K, Horn EM, Barst RJ, et al. Fine mapping of PPH1, a gene for familial primary pulmonary hypertension, to a 3-cM region on chromosome 2q33. Am J Respir Crit Care Med. 2000;161(3 Pt 1):1055–9. PubMed PMID: 10712363.
Lane KB, Machado RD, Pauciulo MW, Thomson JR, Phillips 3rd JA, Loyd JE, et al. Heterozygous germline mutations in BMPR2, encoding a TGF-beta receptor, cause familial primary pulmonary hypertension. Nat Genet. 2000;26(1):81–4. PubMed PMID: 10973254.
Deng Z, Morse JH, Slager SL, Cuervo N, Moore KJ, Venetos G, et al. Familial primary pulmonary hypertension (gene PPH1) is caused by mutations in the bone morphogenetic protein receptor-II gene. Am J Hum Genet. 2000;67(3):737–44. PubMed PMID: 10903931, Pubmed Central PMCID: PMC1287532.
Newman JH, Wheeler L, Lane KB, Loyd E, Gaddipati R, Phillips 3rd JA, et al. Mutation in the gene for bone morphogenetic protein receptor II as a cause of primary pulmonary hypertension in a large kindred. N Engl J Med. 2001;345(5):319–24. PubMed PMID: 11484688.
Thomson JR, Machado RD, Pauciulo MW, Morgan NV, Humbert M, Elliott GC, et al. Sporadic primary pulmonary hypertension is associated with germline mutations of the gene encoding BMPR-II, a receptor member of the TGF-beta family. J Med Genet. 2000;37(10):741–5. PubMed PMID: 11015450, Pubmed Central PMCID: PMC1757155.
Machado RD, Aldred MA, James V, Harrison RE, Patel B, Schwalbe EC, et al. Mutations of the TGF-beta type II receptor BMPR2 in pulmonary arterial hypertension. Hum Mutat. 2006;27(2):121–32. PubMed PMID: 16429395.
Aldred MA, Vijayakrishnan J, James V, Soubrier F, Gomez-Sanchez MA, Martensson G, et al. BMPR2 gene rearrangements account for a significant proportion of mutations in familial and idiopathic pulmonary arterial hypertension. Hum Mutat. 2006;27(2):212–3. PubMed PMID: 16429403.
Cogan JD, Pauciulo MW, Batchman AP, Prince MA, Robbins IM, Hedges LK, et al. High frequency of BMPR2 exonic deletions/duplications in familial pulmonary arterial hypertension. Am J Respir Crit Care Med. 2006;174(5):590–8. PubMed PMID: 16728714, Pubmed Central PMCID: 2648061.
Zeng S, Chen J, Shen H. Controlling of bone morphogenetic protein signaling. Cell Signal. 2010;22(6):888–93. PubMed PMID: 20060893.
Machado RD, Eickelberg O, Elliott CG, Geraci MW, Hanaoka M, Loyd JE, et al. Genetics and genomics of pulmonary arterial hypertension. J Am Coll Cardiol. 2009;54(1 Suppl):S32–42. PubMed PMID: 19555857.
West J. Cross talk between Smad, MAPK, and actin in the etiology of pulmonary arterial hypertension. Adv Exp Med Biol. 2010;661:265–78. PubMed PMID: 20204735.
Morrell NW. Role of bone morphogenetic protein receptors in the development of pulmonary arterial hypertension. Adv Exp Med Biol. 2010;661:251–64. PubMed PMID: 20204735.
Machado RD, Pauciulo MW, Thomson JR, Lane KB, Morgan NV, Wheeler L, et al. BMPR2 haploinsufficiency as the inherited molecular mechanism for primary pulmonary hypertension. Am J Hum Genet. 2001;68(1):92–102. PubMed PMID: 11115378, Pubmed Central PMCID: PMC1234937.
Austin ED, Cogan JD, West JD, Hedges LK, Hamid R, Dawson EP, et al. Alterations in oestrogen metabolism: implications for higher penetrance of familial pulmonary arterial hypertension in females. Eur Respir J. 2009;34(5):1093–9. PubMed PMID: 19357154.
Cogan J, Austin E, Hedges L, Womack B, West J, Loyd J, et al. Role of BMPR2 alternative splicing in HPAH penetrance. Circulation. 2012;126:1907. PubMed PMID: 22923426.
Atkinson C, Stewart S, Upton PD, Machado R, Thomson JR, Trembath RC, et al. Primary pulmonary hypertension is associated with reduced pulmonary vascular expression of type II bone morphogenetic protein receptor. Circulation. 2002;105(14):1672–8. PubMed PMID: 11940546.
Johnson JA, Hemnes AR, Perrien DS, Schuster M, Robinson LJ, Gladson S, et al. Cytoskeletal defects in Bmpr2-associated pulmonary arterial hypertension. Am J Physiol Lung Cell Mol Physiol. 2012;302(5):L474–84. PubMed PMID: 22180660, Pubmed Central PMCID: PMC3311512.
Johnson DW, Berg JN, Baldwin MA, Gallione CJ, Marondel I, Yoon SJ, et al. Mutations in the activin receptor-like kinase 1 gene in hereditary haemorrhagic telangiectasia type 2. Nat Genet. 1996;13(2):189–95. PubMed PMID: 8640225.
McAllister KA, Grogg KM, Johnson DW, Gallione CJ, Baldwin MA, Jackson CE, et al. Endoglin, a TGF-beta binding protein of endothelial cells, is the gene for hereditary haemorrhagic telangiectasia type 1. Nat Genet. 1994;8(4):345–51. PubMed PMID: 7894484.
Harrison RE, Flanagan JA, Sankelo M, Abdalla SA, Rowell J, Machado RD, et al. Molecular and functional analysis identifies ALK-1 as the predominant cause of pulmonary hypertension related to hereditary haemorrhagic telangiectasia. J Med Genet. 2003;40(12):865–71. PubMed PMID: 14684682, Pubmed Central PMCID: PMC1735342.
Trell E, Johansson BW, Linell F, Ripa J. Familial pulmonary hypertension and multiple abnormalities of large systemic arteries in Osler’s disease. Am J Med. 1972;53(1):50–63. PubMed PMID: 5037289.
Trembath RC, Thomson JR, Machado RD, Morgan NV, Atkinson C, Winship I, et al. Clinical and molecular genetic features of pulmonary hypertension in patients with hereditary hemorrhagic telangiectasia. N Engl J Med. 2001;345(5):325–34. PubMed PMID: 11484689.
Chaouat A, Coulet F, Favre C, Simonneau G, Weitzenblum E, Soubrier F, et al. Endoglin germline mutation in a patient with hereditary haemorrhagic telangiectasia and dexfenfluramine associated pulmonary arterial hypertension. Thorax. 2004;59(5):446–8. PubMed PMID: 15115879, Pubmed Central PMCID: PMC1746994.
Harrison RE, Berger R, Haworth SG, Tulloh R, Mache CJ, Morrell NW, et al. Transforming growth factor-beta receptor mutations and pulmonary arterial hypertension in childhood. Circulation. 2005;111(4):435–41. PubMed PMID: 15687131.
Austin ED, Ma L, LeDuc C, Berman Rosenzweig E, Borczuk A, Phillips 3rd JA, et al. Whole exome sequencing to identify a novel gene (caveolin-1) associated with human pulmonary arterial hypertension. Circ Cardiovasc Genet. 2012;5(3):336–43. PubMed PMID: 22474227, Pubmed Central PMCID: PMC3380156.
Bucci M, et al. In vivo delivery of the caveolin-1 scaffolding domain inhibits nitric oxide synthesis and reduces inflammation. Nat Med. 2000;6:1362–7.
Michel JB, Feron O, Sacks D, Michel T. Reciprocal regulation of endothelial nitric oxide synthase by Ca2+-calmodulin and caveolin. J Biol Chem. 1997;272:15583–6.
Zhao YY, Zhao YD, Mirza MK, Huang JH, Potula HH, Vogel SM, Brovkovych V, Yuan JX, Wharton J, Malik AB. Persistent eNOS activation secondary to caveolin-1 deficiency induces pulmonary hypertension in mice and humans through PKG nitration. J Clin Invest. 2009;119(7):2009–18.
Cruz JA, Bauer EM, Rodriguez AI, Gangopadhyay A, Zeineh NS, Wang Y, et al. Chronic hypoxia induces right heart failure in caveolin-1-/- mice. Am J Physiol Heart Circ Physiol. 2012;302(12):H2518–27. PubMed PMID: 22505641, Pubmed Central PMCID: PMC3378264.
Wertz JW, Bauer PM. Caveolin-1 regulates BMPRII localization and signaling in vascular smooth muscle cells. Biochem Biophys Res Commun. 2008;375(4):557–61. PubMed PMID: 18725205.
Zhao YY, Liu Y, Stan RV, Fan L, Gu Y, Dalton N, et al. Defects in caveolin-1 cause dilated cardiomyopathy and pulmonary hypertension in knockout mice. Proc Natl Acad Sci U S A. 2002;99(17):11375–80. PubMed PMID: 12177436, Pubmed Central PMCID: PMC123264.
Newman JH, Ross JC. Primary pulmonary hypertension: a look at the future. J Am Coll Cardiol. 1989;14(3):551–5. PubMed PMID: 2671094.
Heath D, Edwards JE. The pathology of hypertensive pulmonary vascular disease; a description of six grades of structural changes in the pulmonary arteries with special reference to congenital cardiac septal defects. Circulation. 1958;18(4 Part 1):533–47. PubMed PMID: 13573570.
Pietra GG, Edwards WD, Kay JM, Rich S, Kernis J, Schloo B, et al. Histopathology of primary pulmonary hypertension. A qualitative and quantitative study of pulmonary blood vessels from 58 patients in the National Heart, Lung, and Blood Institute, Primary Pulmonary Hypertension Registry. Circulation. 1989;80(5):1198–206. PubMed PMID: 2805258.
Harris P. Influence of acetylcholine on the pulmonary arterial pressure. Br Heart J. 1957;19(2):272–8. PubMed PMID: 13413015, Pubmed Central PMCID: 479625.
Wood P, Besterman EM, Towers MK, McIlroy MB. The effect of acetylcholine on pulmonary vascular resistance and left atrial pressure in mitral stenosis. Br Heart J. 1957;19(2):279–86. PubMed PMID: 13413016, Pubmed Central PMCID: 479626.
Wood P. Pulmonary hypertension with special reference to the vasoconstrictive factor. Br Heart J. 1958;20(4):557–70. PubMed PMID: 13584643, Pubmed Central PMCID: 491807.
Palmer RM, Ferrige AG, Moncada S. Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nature. 1987;327(6122):524–6. PubMed PMID: 3495737.
Furchgott RF, Zawadzki JV. The obligatory role of endothelial cells in the relaxation of arterial smooth muscle by acetylcholine. Nature. 1980;288(5789):373–6. PubMed PMID: 6253831.
Dinh-Xuan AT, Higenbottam TW, Clelland CA, Pepke-Zaba J, Cremona G, Butt AY, et al. Impairment of endothelium-dependent pulmonary-artery relaxation in chronic obstructive lung disease. N Engl J Med. 1991;324(22):1539–47. PubMed PMID: 2027358.
Dinh Xuan AT, Higenbottam TW, Clelland C, Pepke-Zaba J, Cremona G, Wallwork J. Impairment of pulmonary endothelium-dependent relaxation in patients with Eisenmenger’s syndrome. Br J Pharmacol. 1990;99(1):9–10. PubMed PMID: 2331577, Pubmed Central PMCID: 1917494.
Pepke-Zaba J, Higenbottam TW, Dinh-Xuan AT, Stone D, Wallwork J. Inhaled nitric oxide as a cause of selective pulmonary vasodilatation in pulmonary hypertension. Lancet. 1991;338(8776):1173–4. PubMed PMID: 1682593.
Giaid A, Saleh D. Reduced expression of endothelial nitric oxide synthase in the lungs of patients with pulmonary hypertension. N Engl J Med. 1995;333(4):214–21. PubMed PMID: 7540722.
Pullamsetti S, Kiss L, Ghofrani HA, Voswinckel R, Haredza P, Klepetko W, et al. Increased levels and reduced catabolism of asymmetric and symmetric dimethylarginines in pulmonary hypertension. FASEB J. 2005;19(9):1175–7. PubMed PMID: 15827267.
Weimann J, Ullrich R, Hromi J, Fujino Y, Clark MW, Bloch KD, et al. Sildenafil is a pulmonary vasodilator in awake lambs with acute pulmonary hypertension. Anesthesiology. 2000;92(6):1702–12. PubMed PMID: 10839922.
Prasad S, Wilkinson J, Gatzoulis MA. Sildenafil in primary pulmonary hypertension. N Engl J Med. 2000;343(18):1342. PubMed PMID: 11183578.
Wilkens H, Guth A, Konig J, Forestier N, Cremers B, Hennen B, et al. Effect of inhaled iloprost plus oral sildenafil in patients with primary pulmonary hypertension. Circulation. 2001;104(11):1218–22. PubMed PMID: 11551870.
Nagaya N, Uematsu M, Oya H, Sato N, Sakamaki F, Kyotani S, et al. Short-term oral administration of L-arginine improves hemodynamics and exercise capacity in patients with precapillary pulmonary hypertension. Am J Respir Crit Care Med. 2001;163(4):887–91. PubMed PMID: 11282761.
Mehta S, Stewart DJ, Langleben D, Levy RD. Short-term pulmonary vasodilation with L-arginine in pulmonary hypertension. Circulation. 1995;92(6):1539–45. PubMed PMID: 7664438.
Rubin LJ, Groves BM, Reeves JT, Frosolono M, Handel F, Cato AE. Prostacyclin-induced acute pulmonary vasodilation in primary pulmonary hypertension. Circulation. 1982;66(2):334–8. PubMed PMID: 7046988.
Rubin LJ, Mendoza J, Hood M, McGoon M, Barst R, Williams WB, et al. Treatment of primary pulmonary hypertension with continuous intravenous prostacyclin (epoprostenol). Results of a randomized trial. Ann Intern Med. 1990;112(7):485–91. PubMed PMID: 2107780.
Christman BW, McPherson CD, Newman JH, King GA, Bernard GR, Groves BM, et al. An imbalance between the excretion of thromboxane and prostacyclin metabolites in pulmonary hypertension. N Engl J Med. 1992;327(2):70–5. PubMed PMID: 1603138.
Davie N, Haleen SJ, Upton PD, Polak JM, Yacoub MH, Morrell NW, et al. ET(A) and ET(B) receptors modulate the proliferation of human pulmonary artery smooth muscle cells. Am J Respir Crit Care Med. 2002;165(3):398–405. PubMed PMID: 11818328.
Yanagisawa M, Kurihara H, Kimura S, Tomobe Y, Kobayashi M, Mitsui Y, et al. A novel potent vasoconstrictor peptide produced by vascular endothelial cells. Nature. 1988;332(6163):411–5. PubMed PMID: 2451132.
Ryan US, Glassberg MK, Nolop KB. Endothelin-1 from pulmonary artery and microvessels acts on vascular and airway smooth muscle. J Cardiovasc Pharmacol. 1989;13 Suppl 5:S57–62. discussion S74, PubMed PMID: 2473329.
Lippton HL, Hauth TA, Summer WR, Hyman AL. Endothelin produces pulmonary vasoconstriction and systemic vasodilation. J Appl Physiol. 1989;66(2):1008–12. PubMed PMID: 2565328.
Zamora MA, Dempsey EC, Walchak SJ, Stelzner TJ. BQ123, an ETA receptor antagonist, inhibits endothelin-1-mediated proliferation of human pulmonary artery smooth muscle cells. Am J Respir Cell Mol Biol. 1993;9(4):429–33. PubMed PMID: 8398181.
Sitbon O, Badesch DB, Channick RN, Frost A, Robbins IM, Simonneau G, et al. Effects of the dual endothelin receptor antagonist bosentan in patients with pulmonary arterial hypertension: a 1-year follow-up study. Chest. 2003;124(1):247–54. PubMed PMID: 12853530.
McLaughlin VV, Sitbon O, Badesch DB, Barst RJ, Black C, Galie N, et al. Survival with first-line bosentan in patients with primary pulmonary hypertension. Eur Respir J. 2005;25(2):244–9. PubMed PMID: 15684287.
Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, Keogh A, et al. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med. 2002;346(12):896–903. PubMed PMID: 11907289.
Channick RN, Simonneau G, Sitbon O, Robbins IM, Frost A, Tapson VF, et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet. 2001;358(9288):1119–23. PubMed PMID: 11597664.
Liu C, Chen J. Endothelin receptor antagonists for pulmonary arterial hypertension. Cochrane Database Syst Rev. 2006;(3):CD004434. PubMed PMID: 16856046
Cacoub P, Dorent R, Maistre G, Nataf P, Carayon A, Piette C, et al. Endothelin-1 in primary pulmonary hypertension and the Eisenmenger syndrome. Am J Cardiol. 1993;71(5):448–50. PubMed PMID: 8430638.
Stewart DJ, Levy RD, Cernacek P, Langleben D. Increased plasma endothelin-1 in pulmonary hypertension: marker or mediator of disease? Ann Intern Med. 1991;114(6):464–9. PubMed PMID: 1994793.
Cacoub P, Dorent R, Nataf P, Carayon A. Endothelin-1 in pulmonary hypertension. N Engl J Med. 1993;329(26):1967–8. PubMed PMID: 8247067.
Giaid A, Yanagisawa M, Langleben D, Michel RP, Levy R, Shennib H, et al. Expression of endothelin-1 in the lungs of patients with pulmonary hypertension. N Engl J Med. 1993;328(24):1732–9. PubMed PMID: 8497283.
Abenhaim L, Moride Y, Brenot F, Rich S, Benichou J, Kurz X, et al. Appetite-suppressant drugs and the risk of primary pulmonary hypertension. International Primary Pulmonary Hypertension Study Group. N Engl J Med. 1996;335(9):609–16. PubMed PMID: 8692238.
Douglas JG, Munro JF, Kitchin AH, Muir AL, Proudfoot AT. Pulmonary hypertension and fenfluramine. Br Med J (Clin Res Ed). 1981;283(6296):881–3. PubMed PMID: 6793158, Pubmed Central PMCID: PMC1507127.
Kay JM, Smith P, Heath D. Aminorex and the pulmonary circulation. Thorax. 1971;26(3):262–70. PubMed PMID: 5089490, Pubmed Central PMCID: PMC1019080.
Fishman AP. Aminorex to fen/phen: an epidemic foretold. Circulation. 1999;99(1):156–61. PubMed PMID: 9884392.
McGoon MD, Vanhoutte PM. Aggregating platelets contract isolated canine pulmonary arteries by releasing 5-hydroxytryptamine. J Clin Invest. 1984;74(3):828–33. PubMed PMID: 6470141, Pubmed Central PMCID: PMC425237.
Nemecek GM, Coughlin SR, Handley DA, Moskowitz MA. Stimulation of aortic smooth muscle cell mitogenesis by serotonin. Proc Natl Acad Sci U S A. 1986;83(3):674–8. PubMed PMID: 3456163, Pubmed Central PMCID: PMC322926.
Eddahibi S, Adnot S. Anorexigen-induced pulmonary hypertension and the serotonin (5-HT) hypothesis: lessons for the future in pathogenesis. Respir Res. 2002;3:9. PubMed PMID: 11806844, Pubmed Central PMCID: PMC64820.
Maclean MR, Dempsie Y. The serotonin hypothesis of pulmonary hypertension revisited. Adv Exp Med Biol. 2010;661:309–22. PubMed PMID: 20204739.
Herve P, Launay JM, Scrobohaci ML, Brenot F, Simonneau G, Petitpretz P, et al. Increased plasma serotonin in primary pulmonary hypertension. Am J Med. 1995;99(3):249–54. PubMed PMID: 7653484.
Eddahibi S, Humbert M, Fadel E, Raffestin B, Darmon M, Capron F, et al. Serotonin transporter overexpression is responsible for pulmonary artery smooth muscle hyperplasia in primary pulmonary hypertension. J Clin Invest. 2001;108(8):1141–50. PubMed PMID: 11602621, Pubmed Central PMCID: 209526.
Willers ED, Newman JH, Loyd JE, Robbins IM, Wheeler LA, Prince MA, et al. Serotonin transporter polymorphisms in familial and idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med. 2006;173(7):798–802. PubMed PMID: 16339917, Pubmed Central PMCID: 2662954.
Machado RD, Koehler R, Glissmeyer E, Veal C, Suntharalingam J, Kim M, et al. Genetic association of the serotonin transporter in pulmonary arterial hypertension. Am J Respir Crit Care Med. 2006;173(7):793–7. PubMed PMID: 16399993.
MacLean MR, Deuchar GA, Hicks MN, Morecroft I, Shen S, Sheward J, et al. Overexpression of the 5-hydroxytryptamine transporter gene: effect on pulmonary hemodynamics and hypoxia-induced pulmonary hypertension. Circulation. 2004;109(17):2150–5. PubMed PMID: 15078799.
Eddahibi S, Hanoun N, Lanfumey L, Lesch KP, Raffestin B, Hamon M, et al. Attenuated hypoxic pulmonary hypertension in mice lacking the 5-hydroxytryptamine transporter gene. J Clin Invest. 2000;105(11):1555–62. PubMed PMID: 10841514, Pubmed Central PMCID: PMC300850.
Marcos E, Fadel E, Sanchez O, Humbert M, Dartevelle P, Simonneau G, et al. Serotonin-induced smooth muscle hyperplasia in various forms of human pulmonary hypertension. Circ Res. 2004;94(9):1263–70. PubMed PMID: 15059929.
Marcos E, Adnot S, Pham MH, Nosjean A, Raffestin B, Hamon M, et al. Serotonin transporter inhibitors protect against hypoxic pulmonary hypertension. Am J Respir Crit Care Med. 2003;168(4):487–93. PubMed PMID: 12773327.
MacIntyre PD, Bhargava B, Hogg KJ, Gemmill JD, Hillis WS. Effect of subcutaneous sumatriptan, a selective 5HT1 agonist, on the systemic, pulmonary, and coronary circulation. Circulation. 1993;87(2):401–5. PubMed PMID: 8381056.
Launay JM, Herve P, Peoc’h K, Tournois C, Callebert J, Nebigil CG, et al. Function of the serotonin 5-hydroxytryptamine 2B receptor in pulmonary hypertension. Nat Med. 2002;8(10):1129–35. PubMed PMID: 12244304.
Keegan A, Morecroft I, Smillie D, Hicks MN, MacLean MR. Contribution of the 5-HT(1B) receptor to hypoxia-induced pulmonary hypertension: converging evidence using 5-HT(1B)-receptor knockout mice and the 5-HT(1B/1D)-receptor antagonist GR127935. Circ Res. 2001;89(12):1231–9. PubMed PMID: 11739290.
Yuan JX, Aldinger AM, Juhaszova M, Wang J, Conte Jr JV, Gaine SP, et al. Dysfunctional voltage-gated K+ channels in pulmonary artery smooth muscle cells of patients with primary pulmonary hypertension. Circulation. 1998;98(14):1400–6. PubMed PMID: 9760294.
Yuan XJ, Wang J, Juhaszova M, Gaine SP, Rubin LJ. Attenuated K+ channel gene transcription in primary pulmonary hypertension. Lancet. 1998;351(9104):726–7. PubMed PMID: 9504523.
Yu Y, Fantozzi I, Remillard CV, Landsberg JW, Kunichika N, Platoshyn O, et al. Enhanced expression of transient receptor potential channels in idiopathic pulmonary arterial hypertension. Proc Natl Acad Sci U S A. 2004;101(38):13861–6. PubMed PMID: 15358862, Pubmed Central PMCID: PMC518765.
Song MY, Makino A, Yuan JX. STIM2 contributes to enhanced store-operated Ca entry in pulmonary artery smooth muscle cells from patients with idiopathic pulmonary arterial hypertension. Pulm Circ. 2011;1(1):84–94. PubMed PMID: 21709766, Pubmed Central PMCID: PMC3121304.
Golovina VA, Platoshyn O, Bailey CL, Wang J, Limsuwan A, Sweeney M, et al. Upregulated TRP and enhanced capacitative Ca(2+) entry in human pulmonary artery myocytes during proliferation. Am J Physiol Heart Circ Physiol. 2001;280(2):H746–55. PubMed PMID: 11158974.
Kuhr FK, Smith KA, Song MY, Levitan I, Yuan JX. New mechanisms of pulmonary arterial hypertension: role of Ca(2)(+) signaling. Am J Physiol Heart Circ Physiol. 2012;302(8):H1546–62. PubMed PMID: 22245772, Pubmed Central PMCID: PMC3330808.
Jonigk D, Golpon H, Bockmeyer CL, Maegel L, Hoeper MM, Gottlieb J, et al. Plexiform lesions in pulmonary arterial hypertension composition, architecture, and microenvironment. Am J Pathol. 2011;179(1):167–79. PubMed PMID: 21703400, Pubmed Central PMCID: 3123793.
Geiger R, Berger RM, Hess J, Bogers AJ, Sharma HS, Mooi WJ. Enhanced expression of vascular endothelial growth factor in pulmonary plexogenic arteriopathy due to congenital heart disease. J Pathol. 2000;191(2):202–7. PubMed PMID: 10861582.
Tuder RM, Chacon M, Alger L, Wang J, Taraseviciene-Stewart L, Kasahara Y, et al. Expression of angiogenesis-related molecules in plexiform lesions in severe pulmonary hypertension: evidence for a process of disordered angiogenesis. J Pathol. 2001;195(3):367–74. PubMed PMID: 11673836.
Kumpers P, Nickel N, Lukasz A, Golpon H, Westerkamp V, Olsson KM, et al. Circulating angiopoietins in idiopathic pulmonary arterial hypertension. Eur Heart J. 2010;31(18):2291–300. PubMed PMID: 20601390.
Partovian C, Adnot S, Raffestin B, Louzier V, Levame M, Mavier IM, et al. Adenovirus-mediated lung vascular endothelial growth factor overexpression protects against hypoxic pulmonary hypertension in rats. Am J Respir Cell Mol Biol. 2000;23(6):762–71. PubMed PMID: 11104729.
Campbell AI, Zhao Y, Sandhu R, Stewart DJ. Cell-based gene transfer of vascular endothelial growth factor attenuates monocrotaline-induced pulmonary hypertension. Circulation. 2001;104(18):2242–8. PubMed PMID: 11684638.
Taraseviciene-Stewart L, Kasahara Y, Alger L, Hirth P, Mc Mahon G, Waltenberger J, et al. Inhibition of the VEGF receptor 2 combined with chronic hypoxia causes cell death-dependent pulmonary endothelial cell proliferation and severe pulmonary hypertension. FASEB J. 2001;15(2):427–38. PubMed PMID: 11156958.
Klein M, Schermuly RT, Ellinghaus P, Milting H, Riedl B, Nikolova S, et al. Combined tyrosine and serine/threonine kinase inhibition by sorafenib prevents progression of experimental pulmonary hypertension and myocardial remodeling. Circulation. 2008;118(20):2081–90. PubMed PMID: 18955668.
Moreno-Vinasco L, Gomberg-Maitland M, Maitland ML, Desai AA, Singleton PA, Sammani S, et al. Genomic assessment of a multikinase inhibitor, sorafenib, in a rodent model of pulmonary hypertension. Physiol Genomics. 2008;33(2):278–91. PubMed PMID: 18303084.
Voelkel NF, Gomez-Arroyo J. The role of vascular endothelial growth factor in pulmonary arterial hypertension: the angiogenesis paradox. Am J Respir Cell Mol Biol. 2014;51:474.
Grimminger F, Schermuly RT. PDGF receptor and its antagonists: role in treatment of PAH. Adv Exp Med Biol. 2010;661:435–46. PubMed PMID: 20204747.
Perros F, Montani D, Dorfmuller P, Durand-Gasselin I, Tcherakian C, Le Pavec J, et al. Platelet-derived growth factor expression and function in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med. 2008;178(1):81–8. PubMed PMID: 18420966.
Schermuly RT, Dony E, Ghofrani HA, Pullamsetti S, Savai R, Roth M, et al. Reversal of experimental pulmonary hypertension by PDGF inhibition. J Clin Invest. 2005;115(10):2811–21. PubMed PMID: 16200212, Pubmed Central PMCID: PMC1236676.
Benisty JI, McLaughlin VV, Landzberg MJ, Rich JD, Newburger JW, Rich S, et al. Elevated basic fibroblast growth factor levels in patients with pulmonary arterial hypertension. Chest. 2004;126(4):1255–61. PubMed PMID: 15486390.
Izikki M, Guignabert C, Fadel E, Humbert M, Tu L, Zadigue P, et al. Endothelial-derived FGF2 contributes to the progression of pulmonary hypertension in humans and rodents. J Clin Invest. 2009;119(3):512–23. PubMed PMID: 19197140, Pubmed Central PMCID: PMC2648677.
Le Cras TD, Hardie WD, Fagan K, Whitsett JA, Korfhagen TR. Disrupted pulmonary vascular development and pulmonary hypertension in transgenic mice overexpressing transforming growth factor-alpha. Am J Physiol Lung Cell Mol Physiol. 2003;285(5):L1046–54. PubMed PMID: 12896876.
Merklinger SL, Jones PL, Martinez EC, Rabinovitch M. Epidermal growth factor receptor blockade mediates smooth muscle cell apoptosis and improves survival in rats with pulmonary hypertension. Circulation. 2005;112(3):423–31. PubMed PMID: 16027270.
Dahal BK, Cornitescu T, Tretyn A, Pullamsetti SS, Kosanovic D, Dumitrascu R, et al. Role of epidermal growth factor inhibition in experimental pulmonary hypertension. Am J Respir Crit Care Med. 2010;181(2):158–67. PubMed PMID: 19850946.
Souza R, Sitbon O, Parent F, Simonneau G, Humbert M. Long term imatinib treatment in pulmonary arterial hypertension. Thorax. 2006;61(8):736. PubMed PMID: 16877696, Pubmed Central PMCID: PMC2104679.
Patterson KC, Weissmann A, Ahmadi T, Farber HW. Imatinib mesylate in the treatment of refractory idiopathic pulmonary arterial hypertension. Ann Intern Med. 2006;145(2):152–3. PubMed PMID: 16847299.
Ghofrani HA, Seeger W, Grimminger F. Imatinib for the treatment of pulmonary arterial hypertension. N Engl J Med. 2005;353(13):1412–3. PubMed PMID: 16192491.
Ghofrani HA, Morrell NW, Hoeper MM, Olschewski H, Peacock AJ, Barst RJ, et al. Imatinib in pulmonary arterial hypertension patients with inadequate response to established therapy. Am J Respir Crit Care Med. 2010;182(9):1171–7. PubMed PMID: 20581169, Pubmed Central PMCID: PMC3001259.
Hoeper MM, Barst RJ, Bourge RC, Feldman J, Frost AE, Galié N, Gómez-Sánchez MA, Grimminger F, Grünig E, Hassoun PM, Morrell NW, Peacock AJ, Satoh T, Simonneau G, Tapson VF, Torres F, Lawrence D, Quinn DA, Ghofrani HA. Imatinib mesylate as add-on therapy for pulmonary arterial hypertension: results of the randomized IMPRES study. Circulation. 2013;127(10):1128–38.
Montani D, Bergot E, Günther S, Savale L, Bergeron A, Bourdin A, Bouvaist H, Canuet M, Pison C, Macro M, Poubeau P, Girerd B, Natali D, Guignabert C, Perros F, O’Callaghan DS, Jaïs X, Tubert-Bitter P, Zalcman G, Sitbon O, Simonneau G, Humbert M. Pulmonary arterial hypertension in patients treated by dasatinib. Circulation. 2012;125(17):2128–37.
Humbert M, Morrell NW, Archer SL, Stenmark KR, MacLean MR, Lang IM, et al. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43(12 Suppl S):13S–24. PubMed PMID: 15194174.
Schwappacher R, Weiske J, Heining E, Ezerski V, Marom B, Henis YI, Huber O, Knaus P. Novel crosstalk to BMP signalling: cGMP-dependent kinase I modulates BMP receptor and Smad activity. EMBO J. 2009;28(11):1537–50.
Schwappacher R, Kilic A, Kojonazarov B, Lang M, Diep T, Zhuang S, Gawlowski T, Schermuly RT, Pfeifer A, Boss GR, Pilz RB. A molecular mechanism for therapeutic effects of cGMP-elevating agents in pulmonary arterial hypertension. J Biol Chem. 2013;288(23):16557–66.
Morrell NW, Yang X, Upton PD, Jourdan KB, Morgan N, Sheares KK, et al. Altered growth responses of pulmonary artery smooth muscle cells from patients with primary pulmonary hypertension to transforming growth factor-beta(1) and bone morphogenetic proteins. Circulation. 2001;104(7):790–5. PubMed PMID: 11502704.
Hautmann MB, Madsen CS, Owens GK. A transforming growth factor beta (TGFbeta) control element drives TGFbeta-induced stimulation of smooth muscle alpha-actin gene expression in concert with two CArG elements. J Biol Chem. 1997;272(16):10948–56. PubMed PMID: 9099754.
Yang X, Long L, Southwood M, Rudarakanchana N, Upton PD, Jeffery TK, et al. Dysfunctional Smad signaling contributes to abnormal smooth muscle cell proliferation in familial pulmonary arterial hypertension. Circ Res. 2005;96(10):1053–63. PubMed PMID: 15845886.
Valdimarsdottir G, Goumans MJ, Rosendahl A, Brugman M, Itoh S, Lebrin F, et al. Stimulation of Id1 expression by bone morphogenetic protein is sufficient and necessary for bone morphogenetic protein-induced activation of endothelial cells. Circulation. 2002;106(17):2263–70. PubMed PMID: 12390958.
Teichert-Kuliszewska K, Kutryk MJ, Kuliszewski MA, Karoubi G, Courtman DW, Zucco L, et al. Bone morphogenetic protein receptor-2 signaling promotes pulmonary arterial endothelial cell survival: implications for loss-of-function mutations in the pathogenesis of pulmonary hypertension. Circ Res. 2006;98(2):209–17. PubMed PMID: 16357305.
Thistlethwaite PA, Li X, Zhang X. Notch signaling in pulmonary hypertension. Adv Exp Med Biol. 2010;661:279–98. PubMed PMID: 20204737.
Domenga V, Fardoux P, Lacombe P, Monet M, Maciazek J, Krebs LT, et al. Notch3 is required for arterial identity and maturation of vascular smooth muscle cells. Genes Dev. 2004;18(22):2730–5. PubMed PMID: 15545631, Pubmed Central PMCID: PMC528893.
Villa N, Walker L, Lindsell CE, Gasson J, Iruela-Arispe ML, Weinmaster G. Vascular expression of Notch pathway receptors and ligands is restricted to arterial vessels. Mech Dev. 2001;108(1–2):161–4. PubMed PMID: 11578869.
Campos AH, Wang W, Pollman MJ, Gibbons GH. Determinants of Notch-3 receptor expression and signaling in vascular smooth muscle cells: implications in cell-cycle regulation. Circ Res. 2002;91(11):999–1006. PubMed PMID: 12456485.
Li X, Zhang X, Leathers R, Makino A, Huang C, Parsa P, et al. Notch3 signaling promotes the development of pulmonary arterial hypertension. Nat Med. 2009;15(11):1289–97. PubMed PMID: 19855400, Pubmed Central PMCID: PMC2780347.
Benedito R, Rocha SF, Woeste M, Zamykal M, Radtke F, Casanovas O, et al. Notch-dependent VEGFR3 upregulation allows angiogenesis without VEGF-VEGFR2 signalling. Nature. 2012;484(7392):110–4. PubMed PMID: 22426001.
Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54(1 Suppl):S43–54. PubMed PMID: 19555858.
Mukerjee D, St George D, Coleiro B, Knight C, Denton CP, Davar J, et al. Prevalence and outcome in systemic sclerosis associated pulmonary arterial hypertension: application of a registry approach. Ann Rheum Dis. 2003;62(11):1088–93. PubMed PMID: 14583573, Pubmed Central PMCID: PMC1754353.
de Azevedo AB, Sampaio-Barros PD, Torres RM, Moreira C. Prevalence of pulmonary hypertension in systemic sclerosis. Clin Exp Rheumatol. 2005;23(4):447–54. PubMed PMID: 16095111.
Isern RA, Yaneva M, Weiner E, Parke A, Rothfield N, Dantzker D, et al. Autoantibodies in patients with primary pulmonary hypertension: association with anti-Ku. Am J Med. 1992;93(3):307–12. PubMed PMID: 1524083.
Tuder RM, Groves B, Badesch DB, Voelkel NF. Exuberant endothelial cell growth and elements of inflammation are present in plexiform lesions of pulmonary hypertension. Am J Pathol. 1994;144(2):275–85. PubMed PMID: 7508683, Pubmed Central PMCID: PMC1887146.
Savai R, Pullamsetti SS, Kolbe J, Bieniek E, Voswinckel R, Fink L, et al. Immune/inflammatory cell involvement in the pathology of idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med. 2012;186:897. PubMed PMID: 22955318.
Austin ED, Rock MT, Mosse CA, Vnencak-Jones CL, Yoder SM, Robbins IM, et al. T lymphocyte subset abnormalities in the blood and lung in pulmonary arterial hypertension. Respir Med. 2010;104(3):454–62. PubMed PMID: 19880300, Pubmed Central PMCID: PMC2826574.
Ulrich S, Nicolls MR, Taraseviciene L, Speich R, Voelkel N. Increased regulatory and decreased CD8+ cytotoxic T cells in the blood of patients with idiopathic pulmonary arterial hypertension. Respiration. 2008;75(3):272–80. PubMed PMID: 18025812, Pubmed Central PMCID: PMC3030245.
Ormiston ML, Chang C, Long LL, Soon E, Jones D, Machado R, et al. Impaired natural killer cell phenotype and function in idiopathic and heritable pulmonary arterial hypertension. Circulation. 2012;126(9):1099–109. PubMed PMID: 22832786.
Humbert M, Monti G, Brenot F, Sitbon O, Portier A, Grangeot-Keros L, et al. Increased interleukin-1 and interleukin-6 serum concentrations in severe primary pulmonary hypertension. Am J Respir Crit Care Med. 1995;151(5):1628–31. PubMed PMID: 7735624.
Soon E, Holmes AM, Treacy CM, Doughty NJ, Southgate L, Machado RD, et al. Elevated levels of inflammatory cytokines predict survival in idiopathic and familial pulmonary arterial hypertension. Circulation. 2010;122(9):920–7. PubMed PMID: 20713898.
Montani D, Humbert M, Souza R. Letter by Montani et al. regarding article, “Elevated levels of inflammatory cytokines predict survival in idiopathic and familial pulmonary arterial hypertension”. Circulation. 2011;123(21):e614. author reply e5. PubMed PMID: 21632514.
Golembeski SM, West J, Tada Y, Fagan KA. Interleukin-6 causes mild pulmonary hypertension and augments hypoxia-induced pulmonary hypertension in mice. Chest. 2005;128(6 Suppl):572S–3. PubMed PMID: 16373831.
Steiner MK, Syrkina OL, Kolliputi N, Mark EJ, Hales CA, Waxman AB. Interleukin-6 overexpression induces pulmonary hypertension. Circ Res. 2009;104(2):236–44. 28p following 44. PubMed PMID: 19074475.
Savale L, Tu L, Rideau D, Izziki M, Maitre B, Adnot S, et al. Impact of interleukin-6 on hypoxia-induced pulmonary hypertension and lung inflammation in mice. Respir Res. 2009;10:6. PubMed PMID: 19173740, Pubmed Central PMCID: PMC2644669.
Speich R, Jenni R, Opravil M, Pfab M, Russi EW. Primary pulmonary hypertension in HIV infection. Chest. 1991;100(5):1268–71. PubMed PMID: 1935280.
Cool CD, Voelkel NF, Bull T. Viral infection and pulmonary hypertension: is there an association? Expert Rev Respir Med. 2011;5(2):207–16. PubMed PMID: 21510731.
Humbert M, Monti G, Fartoukh M, Magnan A, Brenot F, Rain B, et al. Platelet-derived growth factor expression in primary pulmonary hypertension: comparison of HIV seropositive and HIV seronegative patients. Eur Respir J. 1998;11(3):554–9. PubMed PMID: 9596101.
Mette SA, Palevsky HI, Pietra GG, Williams TM, Bruder E, Prestipino AJ, et al. Primary pulmonary hypertension in association with human immunodeficiency virus infection. A possible viral etiology for some forms of hypertensive pulmonary arteriopathy. Am Rev Respir Dis. 1992;145(5):1196–200. PubMed PMID: 1586065.
Marecki JC, Cool CD, Parr JE, Beckey VE, Luciw PA, Tarantal AF, et al. HIV-1 Nef is associated with complex pulmonary vascular lesions in SHIV-nef-infected macaques. Am J Respir Crit Care Med. 2006;174(4):437–45. PubMed PMID: 16728715, Pubmed Central PMCID: PMC2648120.
James CO, Huang MB, Khan M, Garcia-Barrio M, Powell MD, Bond VC. Extracellular Nef protein targets CD4+ T cells for apoptosis by interacting with CXCR4 surface receptors. J Virol. 2004;78(6):3099–109. PubMed PMID: 14990729, Pubmed Central PMCID: PMC353732.
George MP, Brower A, Kling H, Shipley T, Kristoff J, Reinhart TA, et al. Pulmonary vascular lesions are common in SIV- and SHIV-env-infected macaques. AIDS Res Hum Retroviruses. 2011;27(2):103–11. PubMed PMID: 20961277, Pubmed Central PMCID: PMC3043941.
Hofman FM, Wright AD, Dohadwala MM, Wong-Staal F, Walker SM. Exogenous tat protein activates human endothelial cells. Blood. 1993;82(9):2774–80. PubMed PMID: 7693046.
Kanmogne GD, Primeaux C, Grammas P. Induction of apoptosis and endothelin-1 secretion in primary human lung endothelial cells by HIV-1 gp120 proteins. Biochem Biophys Res Commun. 2005;333(4):1107–15. PubMed PMID: 15979050.
Cool CD, Rai PR, Yeager ME, Hernandez-Saavedra D, Serls AE, Bull TM, et al. Expression of human herpesvirus 8 in primary pulmonary hypertension. N Engl J Med. 2003;349(12):1113–22. PubMed PMID: 13679525.
Laney AS, De Marco T, Peters JS, Malloy M, Teehankee C, Moore PS, et al. Kaposi sarcoma-associated herpesvirus and primary and secondary pulmonary hypertension. Chest. 2005;127(3):762–7. PubMed PMID: 15764755.
Henke-Gendo C, Mengel M, Hoeper MM, Alkharsah K, Schulz TF. Absence of Kaposi’s sarcoma-associated herpesvirus in patients with pulmonary arterial hypertension. Am J Respir Crit Care Med. 2005;172(12):1581–5. PubMed PMID: 16192453.
Bresser P, Cornelissen MI, van der Bij W, van Noesel CJ, Timens W. Idiopathic pulmonary arterial hypertension in Dutch Caucasian patients is not associated with human herpes virus-8 infection. Respir Med. 2007;101(4):854–6. PubMed PMID: 17011770.
Bendayan D, Sarid R, Cohen A, Shitrit D, Shechtman I, Kramer MR. Absence of human herpesvirus 8 DNA sequences in lung biopsies from Israeli patients with pulmonary arterial hypertension. Respiration. 2008;75(2):155–7. PubMed PMID: 17124380.
Valmary S, Dorfmuller P, Montani D, Humbert M, Brousset P, Degano B. Human gamma-herpesviruses Epstein-Barr virus and human herpesvirus-8 are not detected in the lungs of patients with severe pulmonary arterial hypertension. Chest. 2011;139(6):1310–6. PubMed PMID: 21051388.
Bica I, Hamer DH, Stadecker MJ. Hepatic schistosomiasis. Infect Dis Clin North Am. 2000;14(3):583–604. viii, PubMed PMID: 10987111.
Kolosionek E, Graham BB, Tuder RM, Butrous G. Pulmonary vascular disease associated with parasitic infection–the role of schistosomiasis. Clin Microbiol Infect. 2011;17(1):15–24. PubMed PMID: 20636425.
Graham BB, Chabon J, Bandeira A, Espinheira L, Butrous G, Tuder RM. Significant intrapulmonary Schistosoma egg antigens are not present in schistosomiasis-associated pulmonary hypertension. Pulm Circ. 2011;1(4):456–61. PubMed PMID: 22530100, Pubmed Central PMCID: PMC3329075.
Richter J. The impact of chemotherapy on morbidity due to schistosomiasis. Acta Trop. 2003;86(2–3):161–83. PubMed PMID: 12745135.
Graham BB, Mentink-Kane MM, El-Haddad H, Purnell S, Zhang L, Zaiman A, et al. Schistosomiasis-induced experimental pulmonary hypertension: role of interleukin-13 signaling. Am J Pathol. 2010;177(3):1549–61. PubMed PMID: 20671265, Pubmed Central PMCID: PMC2928984.
Wagenvoort CA. Lung biopsy specimens in the evaluation of pulmonary vascular disease. Chest. 1980;77(5):614–25. PubMed PMID: 7363679.
Bjornsson J, Edwards WD. Primary pulmonary hypertension: a histopathologic study of 80 cases. Mayo Clin Proc. 1985;60(1):16–25. PubMed PMID: 3965821.
Wagenvoort CA, Wagenvoort N. Primary pulmonary hypertension. Circulation. 1970;42(6):1163–84.
Johnson SR, Granton JT, Mehta S. Thrombotic arteriopathy and anticoagulation in pulmonary hypertension. Chest. 2006;130(2):545–52. PubMed PMID: 16899857.
Wagenvoort CA. Morphological substrate for the reversibility and irreversibility of pulmonary hypertension. Eur Heart J. 1988;9(Suppl J):7–12. PubMed PMID: 3053185.
Wolf M, Boyer-Neumann C, Parent F, Eschwege V, Jaillet H, Meyer D, et al. Thrombotic risk factors in pulmonary hypertension. Eur Respir J. 2000;15(2):395–9. PubMed PMID: 10706510.
Hoeper MM, Sosada M, Fabel H. Plasma coagulation profiles in patients with severe primary pulmonary hypertension. Eur Respir J. 1998;12(6):1446–9. PubMed PMID: 9877507.
Veyradier A, Nishikubo T, Humbert M, Wolf M, Sitbon O, Simonneau G, et al. Improvement of von Willebrand factor proteolysis after prostacyclin infusion in severe pulmonary arterial hypertension. Circulation. 2000;102(20):2460–2. PubMed PMID: 11076816.
Lopes AA, Maeda NY. Circulating von Willebrand factor antigen as a predictor of short-term prognosis in pulmonary hypertension. Chest. 1998;114(5):1276–82. PubMed PMID: 9824001.
Eisenberg PR, Lucore C, Kaufman L, Sobel BE, Jaffe AS, Rich S. Fibrinopeptide A levels indicative of pulmonary vascular thrombosis in patients with primary pulmonary hypertension. Circulation. 1990;82(3):841–7. PubMed PMID: 2394005.
Tournier A, Wahl D, Chaouat A, Max JP, Regnault V, Lecompte T, et al. Calibrated automated thrombography demonstrates hypercoagulability in patients with idiopathic pulmonary arterial hypertension. Thromb Res. 2010;126(6):e418–22. PubMed PMID: 20888030.
Fuster V, Steele PM, Edwards WD, Gersh BJ, McGoon MD, Frye RL. Primary pulmonary hypertension: natural history and the importance of thrombosis. Circulation. 1984;70(4):580–7. PubMed PMID: 6148159.
Kawut SM, Horn EM, Berekashvili KK, Garofano RP, Goldsmith RL, Widlitz AC, et al. New predictors of outcome in idiopathic pulmonary arterial hypertension. Am J Cardiol. 2005;95(2):199–203. PubMed PMID: 15642552.
Burger CD, Foreman AJ, Miller DP, Safford RE, McGoon MD, Badesch DB. Comparison of body habitus in patients with pulmonary arterial hypertension enrolled in the Registry to Evaluate Early and Long-term PAH Disease Management with normative values from the National Health and Nutrition Examination Survey. Mayo Clin Proc. 2011;86(2):105–12. PubMed PMID: 21282484, Pubmed Central PMCID: PMC3031434.
Zamanian RT, Hansmann G, Snook S, Lilienfeld D, Rappaport KM, Reaven GM, et al. Insulin resistance in pulmonary arterial hypertension. Eur Respir J. 2009;33(2):318–24. PubMed PMID: 19047320, Pubmed Central PMCID: PMC2785883.
Pugh ME, Robbins IM, Rice TW, West J, Newman JH, Hemnes AR. Unrecognized glucose intolerance is common in pulmonary arterial hypertension. J Heart Lung Transplant. 2011;30(8):904–11. PubMed PMID: 21493097, Pubmed Central PMCID: PMC3129440.
Heresi GA, Aytekin M, Newman J, DiDonato J, Dweik RA. Plasma levels of high-density lipoprotein cholesterol and outcomes in pulmonary arterial hypertension. Am J Respir Crit Care Med. 2010;182(5):661–8. PubMed PMID: 20448092, Pubmed Central PMCID: PMC2937236.
Hansmann G, Wagner RA, Schellong S, Perez VA, Urashima T, Wang L, et al. Pulmonary arterial hypertension is linked to insulin resistance and reversed by peroxisome proliferator-activated receptor-gamma activation. Circulation. 2007;115(10):1275–84. PubMed PMID: 17339547.
Summer R, Fiack CA, Ikeda Y, Sato K, Dwyer D, Ouchi N, et al. Adiponectin deficiency: a model of pulmonary hypertension associated with pulmonary vascular disease. Am J Physiol Lung Cell Mol Physiol. 2009;297(3):L432–8. PubMed PMID: 19561137, Pubmed Central PMCID: PMC2739777.
Hansmann G, de Jesus Perez VA, Alastalo TP, Alvira CM, Guignabert C, Bekker JM, et al. An antiproliferative BMP-2/PPARgamma/apoE axis in human and murine SMCs and its role in pulmonary hypertension. J Clin Invest. 2008;118(5):1846–57. PubMed PMID: 18382765, Pubmed Central PMCID: PMC2276393.
West J, Niswender KD, Johnson JA, Pugh ME, Gleaves L, Fessel JP, et al. A potential role for Insulin resistance in experimental pulmonary hypertension. Eur Respir J. 2013;41:861. PubMed PMID: 22936709.
Pugh ME, Hemnes AR. Development of pulmonary arterial hypertension in women: interplay of sex hormones and pulmonary vascular disease. Womens Health (Lond Engl). 2010;6(2):285–96. PubMed PMID: 20187732, Pubmed Central PMCID: PMC2853883.
Tofovic SP, Zhang X, Jackson EK, Dacic S, Petrusevska G. 2-Methoxyestradiol mediates the protective effects of estradiol in monocrotaline-induced pulmonary hypertension. Vascul Pharmacol. 2006;45(6):358–67. PubMed PMID: 16872912.
Tofovic SP, Zhang X, Jackson EK, Zhu H, Petrusevska G. 2-methoxyestradiol attenuates bleomycin-induced pulmonary hypertension and fibrosis in estrogen-deficient rats. Vascul Pharmacol. 2009;51(2–3):190–7. PubMed PMID: 19540933, Pubmed Central PMCID: PMC2760300.
Lahm T, Patel KM, Crisostomo PR, Markel TA, Wang M, Herring C, et al. Endogenous estrogen attenuates pulmonary artery vasoreactivity and acute hypoxic pulmonary vasoconstriction: the effects of sex and menstrual cycle. Am J Physiol Endocrinol Metab. 2007;293(3):E865–71. PubMed PMID: 17595218.
Lahm T, Crisostomo PR, Markel TA, Wang M, Weil BR, Novotny NM, et al. The effects of estrogen on pulmonary artery vasoreactivity and hypoxic pulmonary vasoconstriction: potential new clinical implications for an old hormone. Crit Care Med. 2008;36(7):2174–83. PubMed PMID: 18552699.
Lahm T, Crisostomo PR, Markel TA, Wang M, Wang Y, Tan J, et al. Selective estrogen receptor-alpha and estrogen receptor-beta agonists rapidly decrease pulmonary artery vasoconstriction by a nitric oxide-dependent mechanism. Am J Physiol Regul Integr Comp Physiol. 2008;295(5):R1486–93. PubMed PMID: 18832085, Pubmed Central PMCID: PMC2584849.
White K, Loughlin L, Maqbool Z, Nilsen M, McClure J, Dempsie Y, et al. Serotonin transporter, sex, and hypoxia: microarray analysis in the pulmonary arteries of mice identifies genes with relevance to human PAH. Physiol Genomics. 2011;43(8):417–37. PubMed PMID: 21303932, Pubmed Central PMCID: PMC3092337.
Dempsie Y, Nilsen M, White K, Mair KM, Loughlin L, Ambartsumian N, et al. Development of pulmonary arterial hypertension in mice over-expressing S100A4/Mts1 is specific to females. Respir Res. 2011;12:159. PubMed PMID: 22185646, Pubmed Central PMCID: PMC3276452.
West J, Harral J, Lane K, Deng Y, Ickes B, Crona D, et al. Mice expressing BMPR2R899X transgene in smooth muscle develop pulmonary vascular lesions. Am J Physiol Lung Cell Mol Physiol. 2008;295(5):L744–55. PubMed PMID: 18723761, Pubmed Central PMCID: PMC2584890.
Kawut SM, Al-Naamani N, Agerstrand C, et al. Determinants of right ventricular ejection fraction in pulmonary arterial hypertension. Chest. 2009;135:752–9.
Shapiro S, Traiger GL, Turner M, et al. Sex differences in the diagnosis, treatment, and outcome of patients with pulmonary arterial hypertension enrolled in the Registry To Evaluate Early And Long-Term Pulmonary Arterial Hypertension Disease Management. Chest. 2012;141:363–73.
Ventetuolo CE, Praestgaard A, Palevsky HI, Klinger JR, Halpern SD, Kawut SM. Sex and haemodynamics in pulmonary arterial hypertension. Eur Respir J. 2014;43(2):523–30.
Ventetuolo CE, Ouyang P, Bluemke DA, Tandri H, Barr RG, Bagiella E, Cappola AR, Bristow MR, Johnson C, Kronmal RA, Kizer JR, Lima JA, Kawut SM. Sex hormones are associated with right ventricular structure and function: the MESA-right ventricle study. Am J Respir Crit Care Med. 2011;183(5):659–67.
Humbert M, Sitbon O, Chaouat A, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122:156–63.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Trammell, A.W., Hemnes, A.R. (2015). Pathogenesis of Pulmonary Arterial Hypertension. In: Klinger, J., Frantz, R. (eds) Diagnosis and Management of Pulmonary Hypertension. Respiratory Medicine, vol 12. Humana Press, New York, NY. https://doi.org/10.1007/978-1-4939-2636-7_3
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2636-7_3
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-4939-2635-0
Online ISBN: 978-1-4939-2636-7
eBook Packages: MedicineMedicine (R0)