
Abstract
Cannabis sativa preparations are among the illicit drugs most commonly used by young people, including pregnant women. The endocannabinoid (eCB) system, which is involved in the regulation of emotional and motivational homeostasis, synaptic plasticity and cognitive functions, also plays a critical role in diverse phases of brain development. Both perinatal and periadolescent periods are critical for brain eCB system development. Thus, interference of endocannabinoid signalling by cannabis exposure may contribute to explain the enduring negative impact of cannabis on neurodevelopmental processes and the resulting psycho-physio-pathological consequences. In the present chapter we describe and discuss published data dealing with the long-term neurobehavioural effects of cannabis exposure during the prenatal and adolescent periods. Human studies have demonstrated that marijuana consumption by pregnant women critically affects the neurobehavioural development of their children. Investigations using animal models provide useful information for a better understanding of the long-lasting deleterious consequences of cannabis exposure during pregnancy and lactation. Increasing use of cannabis among adolescents is a matter of great public concern that has led to a parallel increase in research on appropriate animal models. Chronic administration of cannabinoid agonists during the periadolescent period causes persistent behavioural alterations related to cognitive deficits, increased risk of psychosis, mood disorders and addiction to cannabis and other drugs of abuse. The underlying mechanisms by which cannabis use may lead to these disorders, including genetic vulnerability and the increasing content of the main psychoactive ingredient in cannabis preparations, delta-9-tetrahydrocannabinol (THC), will be discussed. To conclude, prevention and therapeutic strategies based on scientific knowledge will be proposed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
Cannabis contains psychoactive components, mainly ∆9-Tetrahydrocannabinol (THC), which interfere with the brain’s endogenous cannabinoid system (endocannabinoid, eCB, system) through the activation of the cannabinoid type 1 (CB1) and type 2 (CB2) receptors. The eCB system plays a relevant regulatory role in a wide variety of functions; eCB signalling is critically involved not only in processes of synaptic plasticity but also in cognitive functions, motivation, and regulation of emotional homeostasis [1–7]. The eCB system plays a crucial role in diverse phases of brain development [8–11]. Interference of eCB signalling by cannabis exposure during the perinatal and the adolescent periods may contribute to explain the enduring negative impact of cannabis on neurodevelopmental processes and the resulting psycho-physio-pathological consequences [3, 12–19].
The main feature of the recreational use of cannabis is a euphoric effect. This “high” can be accompanied by decreased anxiety and increased sociability. However, acute aversive emotional reactions such as feelings of anxiety, panic and paranoia have also been reported [15, 20]. Dependence on cannabis consumption has been reported and an associated withdrawal syndrome has been described [21–23]. Cannabis withdrawal syndrome includes anxiety and nervousness, craving, decreased appetite and weight loss, restlessness, sleep difficulties, strange dreams, chills, depressed mood, stomach pain, physical discomfort, shakiness, and sweating [21, 24, 25]. The syndrome has a transient course after cessation of cannabis use and is pharmacologically specific. Cannabis withdrawal is reported by up to one-third of regular cannabis users in the general population, and by 50–95 % of heavy users in treatment. The clinical relevance of cannabis withdrawal is demonstrated by the use of cannabis or other substances to relieve its symptoms, by the reports of difficulty in quitting, and by the worsening of treatment outcomes in association with greater withdrawal severity.
Marijuana has been associated with disrupted functioning in a variety of cognitive and performance tasks, and chronic marijuana smoking has been reported to cause persistent memory deficiencies [26, 27]. In addition, pharmacological studies have shown that cannabinoids can induce a full range of transient positive, negative, and cognitive symptoms in healthy individuals that are similar to those seen in schizophrenia. Despite most of the current research has focused on the effects of cannabis on psychosis and schizophrenia, there is also increasing evidence indicating a close relationship between cannabis consumption and an increased risk for depression, anxiety disorders, and drug addiction [13, 15, 28–30].
Cannabis preparations are the illicit drugs most widely used by young people, peaking between 15 and 30 years of age, although a trend has been reported for continued cannabis use in people aged 30–40. Growing evidence from human and animal studies suggests a differential effect of cannabis exposure depending on the age of exposure [31]. In this chapter, we will pay special attention to two periods that appear to be of special vulnerability, i.e. the perinatal and the adolescent period. Substance use by pregnant women poses significant risks to the unborn child. Accumulating evidence from both human and preclinical studies indicates that maternal substance use during pregnancy can affect foetal development, birth weight and infant outcomes. Thus, the prenatal period can be regarded as an important sensitive period of development [16, 32]. Actually, cannabis is the most commonly used illicit substance among pregnant women, and given the lipophilic nature of THC, it is estimated that one-third of THC in the plasma crosses the foetus-placental barrier [33, 34]. Moreover, THC is secreted through the breast milk [35]. Therefore, it is plausible that THC can easily reach the developing foetal brain. In fact, human epidemiological and animal studies have found that prenatal/perinatal cannabis exposure influences brain development and can have long-lasting impacts on cognitive functions and other behavioural aspects, notably reward and emotional responses [12, 16, 36–39].
In this chapter we will consider adolescence as the gradual period of transition from childhood to adulthood, including pubertal maturation. Adolescence represents a developmental period of unique plasticity during which the brain is particularly sensitive to environmental insults such as stress and drugs of abuse. There is evidence indicating that during this sensitive period exposure to drugs may have a greater impact on neurocognition compared to adult exposure [40]. A “window of vulnerability” appears to exist during the adolescent period regarding the onset of certain neuropsychiatric disorders such as schizophrenia and the effects of drugs of abuse [14, 17, 18, 41, 42]. In particular, both human and animal studies indicate that cannabis use during adolescence may produce cognition impairments [26, 27] and depressive symptoms, and may increase the risk to develop psychiatric and substance abuse disorders [3, 18, 39, 43]. We will also discuss a number of factors of vulnerability to the harmful effects of cannabis such as the age of starting to use cannabis, the degree of cannabis exposure and genetic susceptibility, as well as the composition of the cannabis plant consumed.
Developmental Aspects of the Endocannabinoid System
During early phases of neuronal development, eCB signalling is integral for an array of processes including proliferation and differentiation of progenitor cells, neuronal migration, axonal guidance, fasciculation, positioning of cortical interneurons, neurite outgrowth and morphogenesis. At early developmental stages, the eCB system seems to both influence the appearance of key cellular signals and modify the expression of genes that are relevant for neural development [8–12, 44]. Both CB1 receptors and eCB ligands can be detected in the rat [45, 46] and human [47] brain during early developmental periods. Moreover, stimulation of [35S]GTP gamma-S binding by cannabinoid agonists suggests that embryonic CB1 receptors are already functional [48]. During the perinatal period, a common atypical pattern of CB1 receptor expression has been found both in rodents and humans, with high densities of CB1 receptors observed in fibre-enriched areas that are practically devoid of them in the adult brain. This transient pattern of CB1 receptor localization in white matter areas during the prenatal stages suggests a specific role of the eCB system in neural development, which may be important for guidance processes that result in the establishment of cortical-subcortical connections [45–47]. Gaffuri et al. [44] have recently reviewed current knowledge about the effects of CB1 receptor signalling during different phases of brain development, i.e. migration and differentiation of progenitor cells, neurite outgrowth, axonal path finding and synaptogenesis. Authors highlighted the eCB signalling as dependent upon the diacylglycerol lipases (DAGLs), the enzymes responsible for the synthesis of the endocannabinoid 2-arachidonoylglycerol (2-AG). DAGL-dependent eCB signalling regulates axonal growth and guidance during development, and is required for the generation and migration of new neurons in the adult brain. It is now clear that DAGLs and CB1 receptors can modulate growth cone dynamics in vitro, and that they are expressed in advancing growth cones during development likely playing a key role in axonal growth and guidance in vivo. In the same growth cone, 2-AG acts upon CB1 receptors to promote motility [49]. The importance of the eCB system during early developmental periods is further supported by the aberrations that occur following disruption of normal eCB signalling during ontogenetic phases. For example, pharmacological blockade of the CB1 receptor in mid-to-late gestational periods impairs progenitor proliferation in the subventricular zone, disrupts axonal path finding and results in cortical delamination [50]. In turn, in utero exposure to THC hampers appropriate interneuron positioning during corticogenesis and results in increased density of cholecystokinin-positive (CCK + ) interneurons in the hippocampus [51].
Development of the eCB system continues during adolescence. In humans, expression patterns of CB1 receptors have been found to increase dramatically from infancy to young adulthood, in regions such as the frontal cortex, striatum and hippocampus [47]. Rodent studies have provided further time- and region-specific data. Ontogeny of cannabinoid receptors in rat striatum, limbic forebrain and ventral mesencephalon is relatively similar, exhibiting a progressive increase that peaks on postnatal days 30 or 40 and then subsequently decrease to adult values [46]. In animal models, the content of the endocannabinoid N-arachidonoylethanolamine (anandamide, AEA) has been observed to gradually increase during early postnatal stages, reaching its maximum in the adolescent brain [8]. Similarly, in rat brain CB1 receptors exhibit a largely postnatal pattern of development, reaching maximal densities during adolescence which later drop to adult expression levels, as detected in the dorsal striatum [45, 46]. Whereas most data available in the literature refer to expression of protein or mRNA for brain CB1 receptors, it would be extremely interesting to examine the developmental changes of CB1 receptor functional activity throughout these critical developmental periods. In the female rat hypothalamus, AEA levels are seen to peak at the onset of puberty and then decline into adulthood [52]. More recent studies have revealed clear developmental fluctuations throughout adolescence in eCB levels in diverse brain regions involved in reward, motivation, and cognition. The most profound alteration was the continuous increase in prefrontal cortex (PFC) of AEA levels throughout the adolescent period; concentrations were almost three times higher in late than early adolescence [53]. However, 2-AG concentrations were lower in the PFC in the later phases than in the beginning of the adolescent period, a finding paralleled within the nucleus accumbens (NAc). In addition, CB1 receptors were found to vary in the PFC and NAc core during the different phases of adolescence, although the alterations were less marked than for eCB levels. These findings emphasize dynamic alterations in eCB function in mesocorticolimbic regions of the adolescent brain that are relevant to reward and, to a greater extent, to cognition and emotional learning, and underscore the specific association of the eCB system with neurodevelopment, not only for the perinatal period but also during adolescence [53]. Lee et al. [54] have further characterized temporal changes in N-acylethanolamine (NAE) content and fatty acid amide hydrolase (FAAH) activity across the periadolescent period, in PFC, amygdala, hippocampus, and hypothalamus. Four developmental points were analysed, specifically postnatal days (pnd) 25, 35, 45, and 70, representing respectively pre-adolescence, early- to mid-adolescence, late adolescence, and adulthood. The observed age-dependent patterns of NAE content and FAAH activity further demonstrate temporal specificity in the development of the system that could contribute to alterations in stress sensitivity, emotionality, and executive functions which also fluctuate during this developmental period.
Another aspect that deserves further investigation is the possible existence of sex differences in developmental patterns. In the developmental study quoted above Rodriguez de Fonseca et al. [46], found subtle sexual dimorphisms in the rat striatum and ventral mesencephalon but not the limbic forebrain. At pnd 43, subtle differences in the expression of hippocampal CB1 receptors were found, with female rats showing lower cannabinoid CB1 receptor density when compared with males [55]. Moreover, clear sex differences in the expression and functionality of hippocampal CB1 receptors are also evidenced in adult rats. Male rats show higher levels of hippocampal CB1 receptor expression than females [56], which in turn exhibit a pattern of higher CB1 receptor-mediated G protein activation in hippocampus when compared to males [57]. Thus, it seems likely that sexual differences in CB1 receptor expression (at least in certain regions such as the hippocampus) are established beyond pnd 40. Interestingly, however, diverse kinds of stress exert differential effects on hippocampal CB1 receptor expression of male and female rats in both adult [56] and 13-day-old neonate animals [58], suggesting a role for organizational effects of gonadal steroids during the perinatal period. The sexual dimorphism observed in the eCB system may contribute to explain the sex differences observed in cannabinoid-induced behavioural alterations (see Chap. 13).
Despite CB2 receptor was initially claimed as a peripheral cannabinoid receptor, it has been detected in a diversity of brain regions including cerebral cortex, hippocampus, amygdala, hypothalamus, and cerebellum, thus suggesting a role for CB2 receptors in emotional and cognitive function [15]. There is also evidence supporting a role of CB2 receptor in neural development [59, 60]. It would be highly interesting to characterize the developmental pattern of CB2 receptors expression and functionality, as well as to investigate on possible interactions between CB1 and CB2 receptors during brain development.
To sum up, in both the rodent and the human foetal brain, cannabinoid receptors are present from early developmental stages onwards. Moreover, there is evidence that the eCB system has a central signalling role in brain development of rodents. Endocannabinoid signalling modulates fundamental developmental processes such as cell proliferation, neurogenesis, migration and axonal path finding, and undergoes important changes and fluctuations through the perinatal and the adolescent periods. Therefore, it is plausible that exposure to exogenous cannabinoids during brain development and/or adolescence may impact the normal developmental course, and lead to adverse outcomes [12, 16, 31].
Long-term Effects of Chronic Cannabinoid Exposure During the Perinatal Period
Studies on the effects of cannabinoids in humans have demonstrated that the consumption of marijuana by women during pregnancy affects the neurobehavioural development of their children. While human studies on long-term neurobehavioural effects of drugs of abuse usually include a number of confounding factors that do not allow to control for potentially important environmental factors, preclinical studies allow a tight control of environmental variables and provides insights about potential mechanisms through which prenatal cannabinoid exposure may exert its impact on the developing foetus. Perinatal exposure to THC or synthetic cannabinoid agonists has been shown to induce long-term effects on diverse parameters (see Table 11.1).
Cannabis and Cognitive Deficit
In a recent review on longitudinal cohort studies, Wu et al. [12] reported that cannabis consumption during pregnancy has profound but variable effects on the offspring in several areas of cognitive development, and suggested an association between maternal cannabis use and impaired high-order cognitive function in the offspring. Maternal cannabis use during pregnancy has also been associated with growth restriction in mid and late pregnancy, and with lower body weight at birth, while similar associations were not found for paternal cannabis use during the reproductive period, demonstrating a direct biological effect of maternal intrauterine exposure to cannabis on foetal growth.
Executive functions refer to higher-order cognitive functions such as cognitive flexibility, sustained and focused attention, planning and working memory: prenatal marijuana exposure exerts a negative effect on these functions [31]. For instance, several reports by Fried and co-workers indicate that cannabis has a negative effect on self-regulatory abilities, including tasks that require impulse control, and is associated with deficits in sustained attention and visual memory, analysis and integration [61–64]. By using functional magnetic resonance imaging (fMRI), Smith et al. [65] investigated the long-lasting neurophysiological effects of prenatal marijuana exposure on visuospatial working memory in 18–22 years old young adults. The study revealed that prenatal marijuana exposure alters neural functioning during visuospatial working memory processing in young adulthood suggesting that deficits in executive functions induced by prenatal cannabis exposure are long-lasting.
In rodents, prenatal exposure to cannabinoid agonists has been reported to induce notable impairments in cognitive function (see Table 11.1), among which a disruption in memory retention in the passive avoidance task [66], an impairment in the active avoidance task [67], and a long-term impairment in the inhibitory avoidance and in a social discrimination task [68]. Similarly, postnatal administration of cannabinoid compounds induces impairments in working memory and object recognition [69, 70], confirming that the gestational and the perinatal age windows are critical periods for the adverse consequences of cannabis on cognition.
Emotional Long-Term Adverse Effects of Cannabis
Findings from animal studies are often controversial given the diversity of behavioural paradigms employed, the time windows investigated and the drug and dose range employed (see Table 11.1). However, in general, gestational exposure to cannabinoid agonists induces motor activation in rodents [66, 71], or no motor effects [72–74] whereas late postnatal exposure reduces locomotor and exploratory activity [75, 76]. The emotional consequences of perinatal cannabis exposure strictly depend upon the time of cannabinoid exposure. If cannabinoid agonists are administered during either the gestational or the early postnatal period, animals exhibit increased anxiety-related behaviour [74, 77] and inhibited social interaction and play behaviour at adolescence [77], as well as an increased exploratory behaviour in the elevated plus maze [71]. If cannabinoid agonist administration is prolonged until weaning, animals exhibit an increment in exploratory behaviour both in the elevated plus maze [71] and the social interaction test [73]. If cannabinoid agonists are administered during early postnatal life, animals are more anxious and prone to exhibit a depressive-like behaviour, consequences that seem to depend upon the sex of the animals [74, 75].
Early Cannabis Consumption and the Risk of Addiction to Other Drugs of Abuse
Regarding associated risk for drug addiction, studies in rodents have reported that perinatal exposure to THC induced in adult females, but not in adult males, an increase in the amount of morphine consumed in the self-administration paradigm under a fixed-ratio (FR-1) schedule of reinforcement [78]. However, perinatal THC exposure does not affect the reinforcing efficacy of morphine in a progressive ratio (PR) schedule of reinforcement [79]. Taken as a whole, these findings suggest that morphine is particularly preferred by adult females that had been exposed perinatally to THC, but that this vulnerability to morphine may disappear when animals are submitted to a higher requirement to obtain the drug. The possibility that perinatal THC exposure induces sensitization to opiates has also been addressed by evaluating morphine place preference conditioning in the adult offspring. In this case, the results indicated that THC-exposed offspring of both sexes exhibited enhanced sensitivity to the rewarding effects of morphine [71]. Moreover, these changes in motivation for drugs seem to be specific for opioid consumption since no changes were observed when alcohol was self administered [80].
Neurobiological Mechanisms Underlying Perinatal Cannabinoid Exposure
Preclinical studies provide also insights about potential neurobiological mechanisms underlying perinatal cannabinoid exposure. For example, cannabinoid exposure in pregnant rats can affect the expression of key genes (e.g. related to the neural adhesion molecule L1) for foetal neural development, possibly resulting in neurotransmitter and behavioural disturbances [34]. The dopaminergic and the opioid systems appear to be markedly affected by perinatal cannabinoid administration. The effects on dopaminergic transmission have been widely studied [81]. It has been shown that perinatal exposure to THC affects the functionality of dopaminergic autoreceptors, inducing a greater sensitivity to the presynaptic actions of dopamine D2 receptor agonists [72]. With respect to the endogenous opioid system, perinatal treatment with THC induces a decrease in pain sensitivity and an increase in the tolerance to the analgesic effect of morphine in males [82]. Baseline opioid activity may be affected since females perinatally exposed to THC showed a decrease in proenkephalin gene expression in the caudate-putamen in adulthood [83]. This result may be related with the sexual dimorphism observed in morphine self-administration following perinatal THC exposure, i.e. females self-administer a higher amount of the drug [78].
The glutamatergic system has also been studied in both neurons and glial cells. Developmental THC exposure induces a decrease in the expression of glutamate receptors, which could lead to functional alterations through the inhibition of glutamatergic neurotransmission [84]. Prenatal exposure to WIN 55,212–2 (WIN) induces a remarkable memory impairment that is correlated with alterations in both long-term potentiation (LTP) and glutamate release in the hippocampus. The decrease in hippocampal glutamate outflow appears to be the cause of LTP disruption, which in turn might underlie, at least in part, the long-lasting impairment of cognitive functions caused by the gestational exposure to WIN [66]. Similarly, in a more recent study, Ferraro et al. [85] showed that the cognitive deficit induced by gestational exposure to cannabinoids is associated with alterations of cortical and hippocampal glutamate outflow, cortical neuron morphology and hippocampal long-term potentiation. As a whole, these data support the view that altered glutamate transmission might underlie, at least in part, some of the cognitive deficits affecting the offspring of marijuana users. Last but not least, prenatal THC exposure also affects cerebellar astroglial cells. Both glial fibrillary acidic protein (GFAP) and glutamine synthetase are decreased in astroglial cells not only during THC exposure but also at adult ages. Thus, cannabinoids may exert developmental toxicity not only on neurons but also on astroglial cells, which could contribute to foetal brain growth retardation [86]. In this respect, it is important to note that glial cells also express components of the cannabinoid signalling system and that marijuana-derived compounds act at cannabinoid receptors expressed on glial cells, affecting their functions [87].
Long-Term Effects of Chronic Cannabinoid Exposure During Adolescence
Adolescence is a period of intense growth, reshaping and maturation of grey and white matters in the human brain. This period involves neurocognitive, hormonal and psychosocial changes with considerable modifications in cognition, mood, arousal, motivation, sleeping patterns, personality, social interactions, behaviour and affection. In humans, the ages associated with adolescence are commonly considered to be approximately 12 to 20–25 years of age, whereas in rodents adolescence is considered within the time frame of 28 to 42 pnd. During this period, the brain undergoes radical functional alterations that are associated with a high degree of plastic structural remodelling. A key finding from structural MRI studies is that the volume of grey matter, which contains brain cell bodies and synapses, changes between childhood and adulthood. In the prefrontal cortex, grey matter volume increases during childhood, peaks in early adolescence, and then declines in late adolescence and throughout the twenties. The loss of grey matter during adolescence is thought to be due, at least partly, to synaptic pruning—the process by which excessive synapses are eliminated. This process of synaptic pruning that sculpts neuronal circuitry during critical periods of brain development is sensitive to environmental factors, including exposure to drugs of abuse [88]. Different brain regions have different peaks of maturation, and changes include modifications in the volume of grey and white matter [19].
Cannabis and Cognitive Deficit
The maturational processes that occur during adolescence are likely to confer a higher risk for suffering from adverse consequences of cannabinoid exposure [89]. Persistent cannabis use has been associated with important deficits in cognitive functions. One of the most important study to date on this topic examined the impact of regular marijuana use on intelligence quotient (IQ) and neuropsychological functioning in a longitudinal sample of 1,037 individuals followed from birth to age 38 [27]. Neuropsychological testing was conducted at 13 years old, before initiation of cannabis use, and again at age 38, after a pattern of persistent cannabis use had developed. Results indicated that persistent cannabis use is related to a broad neuropsychological decline across domains of functioning. Indeed, the statistically significant decline in cognitive ability was present even after controlling for years of education. The more persistent the cannabis use, the greater the cognitive decline. Remarkably, the association between persistent cannabis use and cognitive decline was significantly greater for early marijuana onset, i.e. people who began using cannabis before 18 years old. Converging lines of evidence suggest that regular use of marijuana starting before 18 years old is associated with poorer attention, increased deficits in visual search, reduced overall or verbal IQ, and executive functioning [40]. Moreover, if cannabis use started before 18 years, the cognitive deficit remained significant when people had stopped using for at least 1 year before testing. In line with these results Pope et al. [90] has reported that early onset cannabis users, i.e. people who began smoking before age 17, exhibit poorer cognitive performance, especially in verbal IQ, than late-onset users, i.e. people who began smoking at age ≥ 17 or later, or control subjects.
Cannabis and Psychiatric Disorders—A Focus on Schizophrenia
There is now evidence demonstrating an association between increased rates of cannabis use and new cases of schizophrenia. Epidemiological studies suggest a high incidence of schizophrenia within marijuana smokers, and long-term users of cannabis exhibit cognitive deficits similar to those seen in schizophrenia. A series of longitudinal studies in the general population have investigated the role of cannabis as a risk factor for schizophrenia. Overall, it has been found that cannabis-use approximately doubles the odds of developing schizophrenia [28]. Importantly, there appears to be a dose-response relationship, so that the more extensive the use of cannabis the higher the risk. For example Zammit et al. [91] reported that heavy cannabis users were six times more likely than non-users to subsequently receive a diagnosis of schizophrenia, while DiForti et al. [92] found a clear relationship between the frequency of cannabis use and development of a psychotic illness. Importantly, cannabis has been considered a risk factor for development or worsening of schizophrenia, and there is evidence indicating that young people at genetic high risk of schizophrenia are particularly vulnerable to mental health problems associated with cannabis use. Cannabis use has been associated with a decrease in age of onset of schizophrenia, frequently related with a poorer outcome. Moreover, cannabis-using patients experience more positive symptoms and frequency of relapse and hospitalization and respond poorly to antipsychotic medication [3, 13–15, 28, 92]. However, the ultimate proof of a causal relationship between cannabis use and psychotic illness later in life would come from studies in which healthy young people were exposed to THC and followed-up until adulthood. Obviously, for practical and ethical reasons, such an approach is impossible.
Among many other important health risks, it is well known that cannabis induces harmful effects on cognitive function. While any animal model cannot represent the full phenotypic spectrum of a psychiatric disorder, such as schizophrenia or depression, specific phenotypic components of disorders can be used to construct adequate animal models that may be useful to investigate disease mechanisms and that may allow testing novel interventions. Such studies can be performed in animals under well-controlled conditions and allow pharmacological manipulation that may contribute to unravel causative links.
The most common protocols involve treating rats or mice with THC or synthetic cannabinoids during adolescence and then during adulthood, i.e., after a relatively long wash out period, analyzing a series of behavioural responses that are considered to reflect psychotic-like symptoms. One of the most used and accepted paradigms is the so called pre-pulse inhibition (PPI) of the startle response, a measure of sensorimotor gating that reflects the ability of an organism to attain information and process it correctly. Loss of normal PPI is widely accepted as an endophenotype of schizophrenia with high translational validity, and it can be assessed in both animals and humans. Another usual paradigm that is frequently used is the social interaction test, since individuals suffering from schizophrenia often exhibit impaired social interaction (in form of social withdrawal), which is considered a negative symptom of the disorder. Measurements of social behaviour in rats are relatively easy, as they show a well-structured stable degree of social behaviour. Several cognitive tests, including the analysis of working memory, are also employed. Cognitive symptoms associated with schizophrenia include deficits in attention and working memory that lead to an inability to organize one’s life and to work effectively [39].
The most relevant results obtained from preclinical studies on long-term effects of adolescent cannabinoid exposure are presented in Table 11.2. Chronic pubertal treatment with the cannabinoid agonist WIN resulted in impaired memory in adulthood as well as in a disrupted PPI of the acoustic startle response [93]. These behavioural alterations resemble schizophrenic like-symptoms since PPI deficit, object recognition memory impairment, and anhedonia are among the endophenotypes of schizophrenia. Importantly, Schneider and Koch [94] also showed that if the chronic treatment with the drug occurs during adulthood, it does not lead to behavioural changes. In another study, a 21-day treatment with the cannabinoid receptor agonist CP in 30-day-old rats resulted in a lasting impairment of working memory [95] and, again, these later behavioural changes are observed in adolescent but not adult treated rats. A more recent study performed in male rats has shown that pubertal, but not adult, chronic WIN administration induced persistent disturbances in object and social recognition memory (indicating impairments in working memory and social memory, respectively) and led to social withdrawal and alterations in social behaviour [93]. Furthermore, acute administration of WIN induces more severe behavioural effects in pubertal than in adult rats [93]. Exposure of male rats to chronic THC causes greater lasting memory deficit and hippocampal alterations in adolescent than adult rats [96]. On the other hand, O’Shea et al. [70] found that chronic exposure to the cannabinoid agonist CP during perinatal, adolescent or early adult-hood induced similar long-term memory impairments in male rats. To explain the different results with respect to their previous study performed in female rats [95], authors claimed that adult males might be more vulnerable than adult females to some detrimental effects of cannabinoids, such as cognitive impairment. In line with this proposal, we have recently shown that, in the novel object recognition test, males are more vulnerable than females to the detrimental effects of chronic adolescent administration of CP [57]. Our results also indicate that in the object location task, only the females showed a significantly impaired performance in response to adolescent (pnd 28–43) cannabinoid exposure, suggesting that diverse aspects of memory function may be differentially affected in each sex [57].
Harte and Dow-Edwards [97] examined the effects of THC administered daily during juvenile or early adolescence (pnd 22–40) or late adolescence (pnd 41–60) on locomotor activity, development of tolerance, and acquisition/retention of spatial avoidance in adulthood. THC causes locomotor depression in both male and female animals treated during early adolescence but only in females treated during late adolescence. Evidence of reverse tolerance to THC is seen in early adolescent treated animals only. In the active place avoidance test, male and female animals administered THC during early adolescence made more errors on the reversal trial requiring flexibility in learning, but in animals treated during late adolescence there are no significant sex or treatment differences. The results of the locomotor activity study suggest that females may be more sensitive to the effects of THC than males, while results of both locomotor activity and active place avoidance studies suggest that early adolescent animals are more vulnerable to these effects than late adolescents/young adults. As a whole, these animal studies indicate that the nature of at least certain long-term residual effects of adolescent cannabinoid exposure may be gender- and task-dependent, and that different time intervals of specific vulnerabilities may exist throughout the periadolescent period. The duration and onset of the treatments are also important factors that may affect outcomes, but it seems clear that chronic adolescent cannabinoid treatments induce deleterious effects on cognitive function that can be observed after a long wash-out period.
Some few data from human studies also suggest the existence of gender differences as regards cannabis-induced residual effects at least in certain aspects of cognitive function in young people [90]. However, there is very scarce information regarding gender differences in residual effects of cannabis in humans, even because the vast majority of human and animal studies typically focus on males and do not recognize the importance of sex [98]. In order to gain further insights into this particular aspect, it is important to highlight the necessity of analyzing the two sexes separately.
All together, the data described above indicate that chronic pubertal cannabinoid treatment in rats results in long-lasting behavioural alterations that reflect certain characteristics of schizophrenia symptomatology, such as deficits in sensorimotor gating, impaired memory, reduced motivation and inappropriate and scarce social behaviour. Acute injections of the typical antipsychotic haloperidol are able to restore sensorimotor gating deficits, while the atypical antipsychotic quetiapine is able to acutely restore deficits in social behaviour induced by developmental cannabinoid exposure, and even exerts some persistent beneficial effects. All these data provide support for using pubertal cannabinoid administration as an animal model for investigating aspects of psychosis and schizophrenia [18].
Emotional Long-Term Adverse Effects of Cannabis
In addition to psychotic-like signs, adolescent cannabis use has been shown to induce other types of psychiatric disorders. Longitudinal research suggests that cannabis use predicts the development of anxiety disorders, depression, suicidal ideation, certain personality disorders, and interpersonal violence. Stronger associations have been found in adolescents relative to adults, and younger age of initiation increases the risk of developing mental health disorders [30, 99]. Preclinical studies specifically focused at analyzing depressive and anxiety responses to cannabinoid exposure agree with human observations (see Table 11.2). For instance, adult rats exposed to CP during the juvenile period (pnd 35–45) show anxiolytic-like responses in adulthood, as measured in the elevated plus-maze and the illuminated open field test, as well as sex-dependent effects regarding locomotion and exploration [100]. However, the effects on anxiety-related responses appear to be dependent on the duration of the pharmacological treatment, and likely the test employed, since a 21-day treatment with CP in 30-day-old rats results in increased anxiety in the social interaction test [95]. Moreover, in this latter study, the behavioural test was performed 23 days after the end of the pharmacological treatment, whereas in our case, the animals were tested approximately 37 days after the end of the treatment [100]. As for other types of emotional response, Rubino et al. [101] demonstrated that chronic administration of THC in adolescent rats induced subtle but lasting alterations in the emotional circuit ending in depressive-like behaviour in adulthood, and that this effect is observed in female but not male rats. These animal findings resemble certain observations in humans showing that frequent cannabis use in teenage girls predicts later depression and anxiety, with daily users carrying the highest risk [102].
Early Cannabis Consumption and the Risk of Addiction to Other Drugs of Abuse
Clinical and epidemiological studies have documented a significant link between repeated early cannabis exposure and an increased risk of other illicit drug use [17]. According to the phenotypic causation—“gateway model”—early initiation of cannabis use might be a risk factor for the consumption of other drugs of abuse [103], though the alternative “correlated liabilities model” proposes that cannabis use and other illicit drug use is influenced by correlated genetic and environmental factors [104]. Ferguson et al. [105] examined the associations between the frequency of cannabis use and the use of other illicit drugs in a 25-year longitudinal study of a birth cohort of 1,265 New Zealand children. They obtained annual assessments of the frequency of cannabis use for the period 14–25 years, together with measures of the use of other illicit drugs from the same time period. Regular or heavy cannabis use was associated with an increased risk of using other illicit drugs, abusing or becoming dependent upon other illicit drugs, and using a wider variety of other illicit drugs [105]. This association was particularly strong during adolescence but declined with increasing age. The findings may support a general causal model but they do not clarify the actual underlying mechanisms and the extent to which these causal mechanisms are direct or indirect. Lynskey et al. [103] have further analysed whether the association between early cannabis use and subsequent progression to use of other drugs and drug abuse/dependence persists after controlling for genetic and shared environmental influences. They found that individuals who used cannabis by age 17 years have odds of other drug use, alcohol dependence, and drug abuse/dependence that were 2.1–5.2 times higher than those of their co-twin, who did not use cannabis before age 17 years. Controlling for known risk factors (early-onset alcohol or tobacco use, parental conflict/separation, childhood sexual abuse, conduct disorder, major depression, and social anxiety) had only negligible effects on these results, and the associations do not differ significantly between monozygotic and dizygotic twins. In view of these data, it seems that associations between early cannabis use and later drug use and abuse/dependence cannot solely be explained by common predisposing genetic or shared environmental factors.
An important limitation of human studies is the difficulty of demonstrating a causal relationship between adolescent cannabis use and the use and/or dependence of other substances. However, animal studies suggest that the association may reflect neurobiological disturbances caused by early cannabis exposure that make individuals more vulnerable to the reinforcing effects of other drugs. In fact, there is evidence suggesting a causal relationship between early cannabis exposure and use or abuse of other addictive substances later in life [17, 36]. Ellgren et al. [106], in a study performed on male rats demonstrated that exposure to THC in adolescent animals produced an increase in heroin self-administration, preproenkephalin mRNA expression and functionality of µ opioid receptors in adulthood. Accordingly, we found that chronic periadolescent exposure to CP altered morphine self-administration and the opioid system in adult rats in a sex-dependent manner. In particular, CP increases the acquisition of morphine self-administration and decreases µ-opioid receptor functionality in the nucleus accumbens shell in males but not female animals [107]. In line with our results, decreased µ-opioid-coupled G-protein activity was found in the nucleus accumbens shell of male rats exposed prenatally to THC, with no changes in the nucleus accumbens core or caudate putamen [108]. Together, these data suggest that cannabinoid exposure in early stages of development and adolescence produces perdurable changes in µ opioid receptor functionality that are specific to the nucleus accumbens shell, which is one of the brain regions most closely related to natural and drug-induced reward. Other authors have reported that a chronic treatment with CP during adolescence resulted in a higher rate of cocaine self-administration during the acquisition phase in adult females, whereas no effect was found in males [109]. Thus, the direction of sex differences regarding long-lasting effects of adolescent cannabinoid exposure on self-administration of other drugs of abuse may depend of the specific nature of the drug. Tomasiewicz et al. [110] have shown that over-expression of the pro-enkephalin gene in the nucleus accumbens shell enhances heroin self-administration and heroin-seeking behaviour in animals naïve to THC, whereas knocking down the pro-enkephalin gene in THC-exposed rats reduces heroin intake. Given the well-known interactions between the endocannabinoid and the opioid system and the involvement of the two systems in the brain reward mechanisms, it is likely that exposure to THC during adolescence induces alterations in the opioid system that likely contribute to the development of opiate abuse in adults [17].
The mesolimbic dopaminergic system, which is related to the mechanisms mediating natural and drug-induced reward and the neuropathology of psychoses, is a relevant possible target that might be affected by cannabinoid exposure during puberty. The effects of repeated cannabinoid administration on meso-accumbens dopaminergic neuronal functions and responses to drugs of abuse have been analysed. Animals were pre-treated during adolescence or adulthood, for 3 days, with WIN or vehicle and allowed a 2-week interval. In WIN administered rats dopaminergic neurons were significantly less responsive to the stimulating action of the cannabinoid, regardless of the age of pre-treatment. However, in the adolescent group, but not in the adults, long-lasting cross-tolerance developed to morphine, cocaine and amphetamine [111]. These results suggest that cannabis exposure at a young age may induce long-term neuronal adaptations in the mesolimbic dopaminergic system and hence affect the responses to drugs of abuse. Hurd and co-workers [17] showed that in their model of adolescent THC exposure, reduced levels of Drd2 mRNA, which encodes dopamine D2 receptor, are observed within the nucleus accumbens of adult animals. In addition to adolescent THC exposure, prenatal THC also leads to dysregulation of the Drd2 gene in adulthood. Since a reduced D2 receptor level has long been a characteristic neurobiological feature of addiction vulnerability, that developmental THC exposure reduces Drd2 mRNA expression in the striatum and affects related behavioural traits supports the hypothesis that developmental cannabis may induce a neurobiological state of addiction vulnerability [17].
Neurobiological Mechanisms Underlying Adolescent Cannabinoid Exposure
Several studies provided interesting data suggesting possible neurobiological mechanisms, including molecular and cellular alterations, which may underlie behavioural alterations and psychiatric disorders induced by adolescent cannabinoid exposure, although much more work is necessary to this respect [39]. CP has been reported to impair not only PPI in rats but also auditory gating and neuronal synchrony in limbic areas such as the hippocampus and entorhinal cortex, as evaluated through theta field potential oscillations [112]. It seems clear that, at least in rats, cannabinoid agonists impair auditory gating function in the limbic circuitry, supporting a connection between cannabis abuse and schizophrenia as evaluated through this animal model. More recently, Raver et al. [113] have shown that chronic adolescent, but not adult, cannabinoid exposure in mice suppresses pharmacologically evoked cortical oscillations, that are integral for cognitive processes and are abnormal in patients with schizophrenia, and impairs working memory performance in adults. These data further support a link between chronic adolescent cannabinoid exposure and alterations in adult cortical network activities that underlie cognitive processes. Mice exposed to WIN during adolescence that exhibit in adulthood deficits in PPI and fear conditioning, also show a reduction of hippocampal metabotropic glutamate receptors type 5 (mGluR5) and increased levels of monoacylglycerol lipase (MAGL) and FAAH, indicative of increases in endocannabinoid uptake and degradation [114]. These data further support the idea that cannabis use during adolescence may be a contributory causal factor in the development of at least certain features of schizophrenia probably in relation to altered endocannabinoid signalling in the hippocampus. Page et al. [115] demonstrated that, in adult rats, repeated administration of WIN induces transient anxiety-like behaviours that correlate with increases in catecholamine synthesizing enzyme expression in the locus coeruleus and in norepinephrine efflux in response to a challenge injection of the same drug. Bambico et al. [116] have recently shown that chronic adolescent, but not adult, exposure to low (0.2 mg/kg) and high (1 mg/kg) doses of WIN leads to depression-like behaviour, while the high dose also induces anxiety-like responses in rats. Electrophysiological recordings revealed that both doses attenuate serotonergic activity, while the high dose also leads to a hyperactivity of noradrenergic neurons only after adolescent exposure. These results suggest that the anxiety-like and depression-like behaviour shown by adult rats exposed to the cannabinoid agonist in the adolescent period might be a result of serotonergic hypoactivity and noradrenergic hyperactivity.
Morphological changes in the hippocampus have been observed following chronic administration of cannabinoids [117, 118]. Two-dimensional gel electrophoresis proteomic analysis conducted on THC-treated hippocampal samples revealed several proteins showing long-lasting alterations in response to THC administration. The greater number of differentially expressed protein spots in adolescent THC-pre-treated rats compared with adult THC-pre-treated rats suggests a greater vulnerability to lasting effects of THC in the former group. Differentially expressed proteins in adolescent THC exposed rats include cytoskeletal and other structural proteins, including transgelin-3 (NP25), α and β tubulin and myelin basic protein [96]. This may be linked to structural changes or remodelling occurring after THC exposure in adolescents and is consistent with observations of cytoarchitectural changes occurring with cannabinoid treatment [117]. As a whole, differentially expressed proteins in the hippocampus of THC pre-exposed adolescents have a variety of functions broadly related to oxidative stress, mitochondrial and metabolic function and regulation of the cytoskeleton and signalling. Reductions in dendrite length and complexity and in the number of dendritic spines in the dentate gyrus of the hippocampus have been also found in these animals [118]. Moreover, recent findings suggest that adolescent cannabinoid exposure may induce long-term alterations in astrocytes [119]. These latter results highlight the potential functional importance of astrocytes and their interaction with the eCB system in relation to long-term consequences of adolescent cannabis exposure.
Most of these studies have been carried out in male animals. When female rats were used, adolescent THC exposure induced a significant reduction in cell proliferation in the dentate gyrus of the hippocampus [120] as well as less synaptic density and/or efficiency throughout the prefrontal cortex [121]. Further studies analyzing both sexes are urgently needed to get a clearer picture of possible differential vulnerabilities in both genders.
MRI studies further suggest that heavy cannabis use may modify brain structure. Just to mention some of them, Yucel et al. [122] showed that heavy cannabis users had bilaterally reduced hippocampal and amygdala volumes with greater effect in the former. Left hemisphere hippocampal volume was inversely associated with cumulative exposure to cannabis and with sub-threshold positive psychotic symptoms. Interestingly, hippocampal abnormalities in schizophrenia are more prominent in the left hemisphere. In another imaging study, long-term use of cannabis during adolescence was associated with gyrification abnormalities in the cortex, suggesting that early cannabis use affected normal neurodevelopment [123]. Arnone et al. [124] used an MRI technique sensitive to the structural integrity of brain tissue that combines with a white matter mapping tractography to investigate structural changes in the corpus callosum. Mean diffusivity, which measures structural integrity, was significantly increased in marijuana users relative to controls in the region of the corpus callosum where white matter passes between the prefrontal lobes. Moreover, there was a trend towards a positive correlation between mean diffusivity and length of use, which suggests the possibility of a cumulative effect of marijuana over time and that a younger age at onset of use may predispose individuals to structural white matter damage.
More recently, Zalesky et al. [125] have found that axonal connectivity is impaired in the right fimbria of the hippocampus (fornix), splenium of the corpus callosum and commissural fibres, suggesting that long-term cannabis use is hazardous to white matter in the developing brain. Adolescent onset marijuana use has also been linked with increased prefrontal cortex white matter diffusivity and increased impulsivity compared to later onset in a sample of well-matched adolescent onset marijuana users [126]. A recent review by Lorenzetti et al. [127] has examined evidence from structural neuroimaging investigations of regular cannabis users. This review supports the notion that regular cannabis use is associated with alterations of brain morphology, specifically medial temporal, frontal and cerebellar brain regions. Greater brain morphological alterations are evident among samples that used higher doses for longer periods. To sum up, structural abnormalities, disturbed brain connectivity and altered brain activation patterns may underlie cognitive impairment, behavioural alterations and vulnerability to certain psychiatric disorders that are observed in long-term heavy cannabis users.
Cannabis Plant Composition
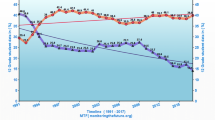
The composition of the cannabis plant (“cannabis brands”) has a critical influence on its possible long-term effects. Until recently, the main types of cannabis available on the “street” were marijuana (grass) and resin (hash), but in recent years a more potent variant termed sinsemilla or skunk has become available in many countries. Marijuana and resin have traditionally contained about 4 % THC, but the concentration of THC in skunk in countries such as England and the Netherlands has increased to about 16 and 20 % respectively, partly due to the use of intensive indoor cultivation methods [28]. The content of THC in confiscated cannabis preparations has substantially increased over the past 20 years. Recent data showed an upward trend in the mean THC content, which increased from 3.4 % in 1993 to 8.8 % in 2008 [128]. Thus, cannabis consumption nowadays implies exposure to very high amounts of THC, especially if sinsemilla (skunk) or synthetic cannabinoids are consumed. The risk associated with use of these stronger forms of cannabis needs to be further and deeply evaluated, since it is plausible that there are greater health risks than thought. The risk of psychosis is much greater among people who are frequent cannabis users, and among those using sinsemilla (skunk) rather than traditional hash [92]. It is not surprising that those who use skunk daily are at the highest risk, and public education about the risks of heavy use of high-potency cannabis is therefore urgently needed.
There is growing public health concern about the increasing use of a new generation of synthetic cannabinoid agonists marketed as natural herbal incense mixtures comprised under the “Spice” name. “Spice” refers to a wide variety of herbal mixtures that produce experiences similar to marijuana and that are marketed as “safe”, legal alternatives to cannabis. Sold under many names, including K2, fake weed, Yucatan Fire, Skunk, Moon Rocks, and others—and labelled “not for human consumption”—these products contain dried, shredded plant material and chemical additives that are responsible for their psychoactive (mind-altering) effects. Spice products do contain dried plant material, but chemical analyses show that their active ingredients are synthetic cannabinoid compounds, e.g. JWH-018, CP-47,497. Spice users report experiences similar to those produced by marijuana—elevated mood, relaxation, and altered perception—and, in some cases, the effects are even stronger than those of marijuana [129]. Some users report psychotic effects like extreme anxiety, paranoia, and hallucinations. Spice can also raise blood pressure, can induce myocardial ischemia, and, in a few cases, it has been associated with heart attacks. Regular users may experience craving and withdrawal symptoms [130].
THC and cannabidiol (CBD), the two main ingredients of the Cannabis sativa plant have distinct symptomatic and behavioural effects. CBD has been demonstrated to have low affinity for both cannabinoid CB1 and CB2 receptors, but it can behave as a CB2 receptor inverse agonist [131]. Recent data suggest that THC and CBD can have opposite effects on regional brain function, which may underlie their different symptomatic and behavioural effects, and the potential ability of CBD to somehow ‘buffer’ the detrimental consequences of THC [132]. Notably, the ratio of CBD and THC seems to have changed in an unfavourable manner in the last years, and this fact may underlay the increased risk for adverse, and long-lasting detrimental consequences of marijuana consumption during adolescence. Nevertheless, more information is urgently needed in order to further clarify the potential therapeutic effect of CBD and the extent to which it is able to diminish the detrimental effects of THC [15]. Future studies are needed regarding the investigation of the long-term effects of chronic CBD administration alone or in combination with THC, and animal models would be a very useful tool for this purpose.
Genetics Factors of Vulnerability
In spite of the fact that cannabis is the most widely used drug in the world, only a relatively small proportion of users develop psychotic illness, suggesting the relevance of individual genetic factors in the susceptibility to the psychotic-inducing potential of cannabis. To date, most research has focused on the catechol-O-methyltransferase (COMT) gene. COMT is a key enzyme involved in the metabolism of dopamine that is highly expressed in the prefrontal cortex. Caspi et al. [133] showed that a functional polymorphism in the COMT gene moderates the influence of adolescent cannabis use on developing adult psychosis. Homozygous carriers of the COMT valine158 allele (Val/Val) are most likely to exhibit psychotic symptoms and to later develop schizophrenia-like disorders if they have used cannabis during adolescence (relative risk: 10.9). Heterozygous individuals with the valine/methionine (Val/Met) genotype who used cannabis during adolescence show an intermediate risk, while those homozygous for the methionine allele (Met/Met) show the lowest risk (relative risk: 1.1). A subsequent study by Henquet et al. [134] showed that carriers of the Val allele (Val/Val) are more sensitive to THC-induced memory and attention impairments compared to carriers of the Met allele (Met/Met), and are most sensitive to THC-induced psychotic experiences only in the presence of prior evidence of psychometric psychosis liability.
Taken together, it seems that the effects of THC on cognition and psychosis are moderated by COMT genotype, although partially conditioned to the presence of pre-existing psychosis liability. Notably, negative results have also been reported in this regard since Zammit et al. [135] did not report differential effects of cannabis use on schizophrenia due to COMT variations.
More recently, Van Winkel et al. [136] have examined the interactions between cannabis use and 152 single-nucleotide polymorphisms in 42 genes in 740 unaffected siblings of 801 patients with psychosis. Authors showed that genetic variation in AKT1 may mediate the effects on psychosis expression associated with cannabis use. AKT1 is a serine/threonine kinase central in many signal-transduction pathways. Cannabinoids are able to activate the AKT1 pathway through the activation of CB1 and CB2 receptors. Polymorphisms in the AKT1 gene may be involved in cannabis induced psychosis through a mechanism of cannabinoid-regulated AKY1/GSK-3 signalling downstream of the dopamine D2 receptor [28]. However, individual responses to cannabis use might be modulated by several genes rather than by a single polymorphism. Future research is needed to gain insights into genetic vulnerability to the harmful effects of cannabis.
Final Remarks
There is still scarce research available to determine whether sustained abstinence from cannabis results in recovery of cognitive functions. Though certain preliminary findings seem to be hopeful, further research is needed to learn whether cannabis-induced impairments in the brain are reversible. It has been proposed that “interventions geared toward lowering alcohol and drug exposure in teens and young adults that have shown evidence of efficacy need to be implemented more aggressively in schools and college campuses to not only reduce symptoms of drug abuse and dependence, but delay the onset of regular use from early teen years to early adult years in order to prevent long-term neuronal damage and ensure optimal brain health and cognitive functioning in youth” [40]. Yet, besides delaying the onset of use, it should be important to also promote abstinence. In addition to the age of onset, other factors such as genetic vulnerability, dosing, personality traits and amount of THC present in the drug are also important factors that may influence the impact of drug use. For example, genetic background might be a crucial factor in terms of vulnerability, but we are still far from having a clear knowledge about the nature of the genes implicated and from predicting and controlling these risk factors. It is also worth noticing that though cannabis use is most prevalent among adolescents and young adults, it is by no means restricted to this age group and increasing recognition is currently given to cannabis users in older age groups, including individuals who initiate cannabis use at a later age [137]. As pointed out by Agrawal and Lynskey [137], while later onsets are rare, their impact may be fairly profound, and attempts to identify correlates of new onsets and of persistence of cannabis use through adulthood seem to be relevant. Not to forget, the importance of sex differences regarding not only the prevalence of cannabis use but also the possible differential effects of the drug on males and females and the different underlying motivation to consume it (see Chap. 13). This approach may result in better prevention and treatment strategies. A fluent interaction between basic researchers, clinicians and epidemiologists together with a clear message to the society about the detrimental effects of cannabis are urgently needed. Giving healthy alternatives to young people, promoting exercise and considering that availability of the drug are all important aspects to establish efficacious treatment and prevention campaigns.
References
Marco EM, Romero-Zerbo SY, Viveros MP, Bermudez-Silva FJ. The role of the endocannabinoid system in eating disorders: pharmacological implications. Behav Pharmacol. 2012;23(5–6):526–36.
Bermudez-Silva FJ, Viveros MP, McPartland JM, Rodriguez de Fonseca F. The endocannabinoid system, eating behavior and energy homeostasis: the end or a new beginning? Pharmacol Biochem Behav. 2010;95(4):375–82.
Marco EM, Viveros MP. The critical role of the endocannabinoid system in emotional homeostasis: avoiding excess and deficiencies. Mini Rev Med Chem. 2009;9(12):1407–15.
Castillo PE, Younts TJ, Chavez AE, Hashimotodani Y. Endocannabinoid signaling and synaptic function. Neuron. 2012;76(1):70–81.
Katona I, Freund TF. Multiple functions of endocannabinoid signaling in the brain. Annu Rev Neurosci. 2012;35:529–58.
Oleson EB, Cheer JF. A brain on cannabinoids: the role of dopamine release in reward seeking. Cold Spring Harb Perspect Med. 2012;2(8).
Gardner EL. Addiction and brain reward and antireward pathways. Adv Psychosom Med. 2011;30:22–60.
Harkany T, Guzman M, Galve-Roperh I, Berghuis P, Devi LA, Mackie K. The emerging functions of endocannabinoid signaling during CNS development. Trends Pharmacol Sci. 2007;28(2):83–92.
Galve-Roperh I, Palazuelos J, Aguado T, Guzman M. The endocannabinoid system and the regulation of neural development: potential implications in psychiatric disorders. Eur Arch Psychiatry Clin Neurosci. 2009;259(7):371–82.
Keimpema E, Alpar A, Howell F, Malenczyk K, Hobbs C, Hurd YL, et al. Diacylglycerol lipase alpha manipulation reveals developmental roles for intercellular endocannabinoid signaling. Sci Rep. 2013;3:2093.
Keimpema E, Mackie K, Harkany T. Molecular model of cannabis sensitivity in developing neuronal circuits. Trends Pharmacol Sci. 2011;32(9):551–61.
Wu CS, Jew CP, Lu HC. Lasting impacts of prenatal cannabis exposure and the role of endogenous cannabinoids in the developing brain. Future Neurol. 2011;6(4):459–80.
Burns JK. Pathways from cannabis to psychosis: a review of the Evidence. Front Psychiatry. 2013;4:128.
Fernandez-Espejo E, Viveros MP, Nunez L, Ellenbroek BA, Rodriguez de Fonseca F. Role of cannabis and endocannabinoids in the genesis of schizophrenia. Psychopharmacology (Berl). 2009;206(4):531–49.
Marco EM, Garcia-Gutierrez MS, Bermudez-Silva FJ, Moreira FA, Guimaraes F, Manzanares J, et al. Endocannabinoid system and psychiatry: in search of a neurobiological basis for detrimental and potential therapeutic effects. Front Behav Neurosci. 2011;5:63.
Huizink AC. Prenatal cannabis exposure and infant outcomes: overview of studies. Prog Neuropsychopharmacol Biol Psychiatry. 2013.
Hurd YL, Michaelides M, Miller ML, Jutras-Aswad D. Trajectory of adolescent cannabis use on addiction vulnerability. Neuropharmacology 2014;76 Pt B:416–24.
Viveros MP, Llorente R, Suarez J, Llorente-Berzal A, Lopez-Gallardo M, de Fonseca FR. The endocannabinoid system in critical neurodevelopmental periods: sex differences and neuropsychiatric implications. J Psychopharmacol. 2012;26(1):164–76.
Viveros MP, Marco EM, Lopez-Gallardo M, Garcia-Segura LM, Wagner EJ. Framework for sex differences in adolescent neurobiology: a focus on cannabinoids. Neurosci Biobehav Rev. 2011;35(8):1740–51.
Crippa JA, Zuardi AW, Martin-Santos R, Bhattacharyya S, Atakan Z, McGuire P, et al. Cannabis and anxiety: a critical review of the evidence. Hum Psychopharmacol. 2009;24(7):515–23.
Budney AJ, Hughes JR. The cannabis withdrawal syndrome. Curr Opin Psychiatry. 2006;19(3):233–8.
Fattore L, Fadda P, Spano MS, Pistis M, Fratta W. Neurobiological mechanisms of cannabinoid addiction. Mol Cell Endocrinol. 2008;286(1–2 Suppl 1):S97–S107.
Hasin DS, O’Brien CP, Auriacombe M, Borges G, Bucholz K, Budney A, et al. DSM-5 criteria for substance use disorders: recommendations and rationale. Am J Psychiatry. 2013;170(8):834–51.
Hesse M, Thylstrup B. Time-course of the DSM-5 cannabis withdrawal symptoms in poly-substance abusers. BMC Psychiatry. 2013;13:258.
Gorelick DA, Levin KH, Copersino ML, Heishman SJ, Liu F, Boggs DL, et al. Diagnostic criteria for cannabis withdrawal syndrome. Drug Alcohol Depend. 2012;123(1–3):141–7.
Solowij N, Pesa N. Cannabis and cognition: short and long-term effects. In: Castle D, Murray R, D’Souza DC, editors. Marijuana and madness. 2nd ed. Cambridge: Cambridge University Press; 2012. p. 91–102.
Meier MH, Caspi A, Ambler A, Harrington H, Houts R, Keefe RS, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci U S A. 2012;109(40):E2657–64.
Casadio P, Fernandes C, Murray RM, Di Forti M. Cannabis use in young people: the risk for schizophrenia. Neurosci Biobehav Rev. 2011;35(8):1779–87.
Hurd YL, Michaelides M, Miller ML, Jutras-Aswad D. Trajectory of adolescent cannabis use on addiction vulnerability. Neuropharmacology. 2014;76PB:416–24.
Copeland J, Rooke S, Swift W. Changes in cannabis use among young people: impact on mental health. Curr Opin Psychiatry. 2013;26(4):325–9.
Trezza V, Campolongo P, Manduca A, Morena M, Palmery M, Vanderschuren LJ, et al. Altering endocannabinoid neurotransmission at critical developmental ages: impact on rodent emotionality and cognitive performance. Front Behav Neurosci. 2012;6:2.
Passey ME, Sanson-Fisher RW, D’Este CA, Stirling JM. Tobacco, alcohol and cannabis use during pregnancy: Clustering of risks. Drug Alcohol Depend. 2013.
Hutchings DE, Martin BR, Gamagaris Z, Miller N, Fico T. Plasma concentrations of delta-9-tetrahydrocannabinol in dams and fetuses following acute or multiple prenatal dosing in rats. Life Sci. 1989;44(11):697–701.
Gomez M, Hernandez M, Johansson B, de Miguel R, Ramos JA, Fernandez-Ruiz J. Prenatal cannabinoid and gene expression for neural adhesion molecule L1 in the fetal rat brain. Brain Res Dev Brain Res. 2003;147(1–2):201–7.
Perez-Reyes M, Wall ME. Presence of delta9-tetrahydrocannabinol in human milk. N Engl J Med. 1982;307(13):819–20.
DiNieri JA, Hurd YL. Rat Models of prenatal and adolescent cannabis exposure. In: Kobeissy FH, editor. Psychiatric disorders: methods and protocols: Springer protocols. USA: Humana Press; 2012. p. 231–42.
Viveros MP, Llorente R, Moreno E, Marco EM. Behavioural and neuroendocrine effects of cannabinoids in critical developmental periods. Behav Pharmacol. 2005 Sep;16(5–6):353–62.
Schneider M. Cannabis use in pregnancy and early life and its consequences: animal models. Eur Arch Psychiatry Clin Neurosci. 2009;259(7):383–93.
Rubino T, Parolaro D. Cannabis abuse in adolescence and the risk of psychosis: a brief review of the preclinical evidence. Prog Neuropsychopharmacol Biol Psychiatry. 2014;52:41–4.
Lisdahl KM, Gilbart ER, Wright NE, Shollenbarger S. Dare to delay? The impacts of adolescent alcohol and marijuana use onset on cognition, brain structure, and function. Front Psychiatry. 2013;4:53.
Adriani W, Laviola G. Windows of vulnerability to psychopathology and therapeutic strategy in the adolescent rodent model. Behav Pharmacol. 2004;15(5–6):341–52.
Schneider M. Adolescence as a vulnerable period to alter rodent behavior. Cell Tissue Res. 2013;354(1):99–106.
Viveros MP, Marco EM, File SE. Endocannabinoid system and stress and anxiety responses. Pharmacol Biochem Behav. 2005;81(2):331–42.
Gaffuri AL, Ladarre D, Lenkei Z. Type-1 cannabinoid receptor signaling in neuronal development. Pharmacology 2012;90(1–2):19–39.
Belue RC, Howlett AC, Westlake TM, Hutchings DE. The ontogeny of cannabinoid receptors in the brain of postnatal and aging rats. Neurotoxicol Teratol. 1995;17(1):25–30.
Rodriguez de Fonseca F Ramos JA Bonnin A Fernandez-Ruiz JJ. Presence of cannabinoid binding sites in the brain from early postnatal ages. Neuroreport. 1993;4(2):135–8.
Mato S, Del Olmo E, Pazos A. Ontogenetic development of cannabinoid receptor expression and signal transduction functionality in the human brain. Eur J Neurosci. 2003;17(9):1747–54.
Berrendero F, Garcia-Gil L, Hernandez ML, Romero J, Cebeira M, de Miguel R, et al. Localization of mRNA expression and activation of signal transduction mechanisms for cannabinoid receptor in rat brain during fetal development. Development. 1998;125(16):3179–88.
Reisenberg M, Singh PK, Williams G, Doherty P. The diacylglycerol lipases: structure, regulation and roles in and beyond endocannabinoid signalling. Philos Trans R Soc Lond B Biol Sci. 2012;367(1607):3264–75.
Mulder J, Aguado T, Keimpema E, Barabas K, Ballester Rosado CJ, Nguyen L, et al. Endocannabinoid signaling controls pyramidal cell specification and long-range axon patterning. Proc Natl Acad Sci U S A. 2008;105(25):8760–5.
Berghuis P, Dobszay MB, Wang X, Spano S, Ledda F, Sousa KM, et al. Endocannabinoids regulate interneuron migration and morphogenesis by transactivating the TrkB receptor. Proc Natl Acad Sci U S A. 2005;102(52):19115–20.
Wenger T, Gerendai I, Fezza F, Gonzalez S, Bisogno T, Fernandez-Ruiz J, et al. The hypothalamic levels of the endocannabinoid, anandamide, peak immediately before the onset of puberty in female rats. Life Sci. 2002;70(12):1407–14.
Ellgren M, Artmann A, Tkalych O, Gupta A, Hansen HS, Hansen SH, et al. Dynamic changes of the endogenous cannabinoid and opioid mesocorticolimbic systems during adolescence: THC effects. Eur Neuropsychopharmacol. 2008;18(11):826–34.
Lee TT, Hill MN, Hillard CJ, Gorzalka BB. Temporal changes in N-acylethanolamine content and metabolism throughout the peri-adolescent period. Synapse. 2013;67(1):4–10.
Marco EM, Adriani W, Canese R, Podo F, Viveros MP, Laviola G. Enhancement of endocannabinoid signalling during adolescence: Modulation of impulsivity and long-term consequences on metabolic brain parameters in early maternally deprived rats. Pharmacol Biochem Behav. 2007;86(2):334–45.
Reich CG, Taylor ME, McCarthy MM. Differential effects of chronic unpredictable stress on hippocampal CB1 receptors in male and female rats. Behav Brain Res. 2009;203(2):264–9.
Mateos B, Borcel E, Loriga R, Luesu W, Bini V, Llorente R, et al. Adolescent exposure to nicotine and/or the cannabinoid agonist CP 55,940 induces gender-dependent long-lasting memory impairments and changes in brain nicotinic and CB(1) cannabinoid receptors. J Psychopharmacol. 2011;25(12):1676–90.
Suarez J, Llorente R, Romero-Zerbo SY, Mateos B, Bermudez-Silva FJ, de Fonseca FR, et al. Early maternal deprivation induces gender-dependent changes on the expression of hippocampal CB(1) and CB(2) cannabinoid receptors of neonatal rats. Hippocampus. 2009;19(7):623–32.
Duff G, Argaw A, Cecyre B, Cherif H, Tea N, Zabouri N, et al. Cannabinoid receptor CB2 modulates axon guidance. PLoS ONE. 2013;8(8):e70849.
Palazuelos J, Ortega Z, Diaz-Alonso J, Guzman M, Galve-Roperh I. CB2 cannabinoid receptors promote neural progenitor cell proliferation via mTORC1 signaling. J Biol Chem. 2012;287(2):1198–209.
Fried PA, Watkinson B. Differential effects on facets of attention in adolescents prenatally exposed to cigarettes and marihuana. Neurotoxicol Teratol. 2001;23(5):421–30.
Fried PA, Watkinson B, Gray R. A follow-up study of attentional behavior in 6-year-old children exposed prenatally to marihuana, cigarettes, and alcohol. Neurotoxicol Teratol. 1992;14(5):299–311.
Fried PA, Watkinson B, Gray R. Differential effects on cognitive functioning in 9–12-year olds prenatally exposed to cigarettes and marihuana. Neurotoxicol Teratol. 1998;20(3):293–306.
Fried PA, Watkinson B, Gray R. Differential effects on cognitive functioning in 13–16-year-olds prenatally exposed to cigarettes and marihuana. Neurotoxicol Teratol. 2003;25(4):427–36.
Smith AM, Fried PA, Hogan MJ, Cameron I. Effects of prenatal marijuana on visuospatial working memory: an fMRI study in young adults. Neurotoxicol Teratol. 2006;28(2):286–95.
Mereu G, Fa M, Ferraro L, Cagiano R, Antonelli T, Tattoli M, et al. Prenatal exposure to a cannabinoid agonist produces memory deficits linked to dysfunction in hippocampal long-term potentiation and glutamate release. Proc Natl Acad Sci U S A. 2003;100(8):4915–20.
Antonelli T, Tomasini MC, Tattoli M, Cassano T, Tanganelli S, Finetti S, et al. Prenatal exposure to the CB1 receptor agonist WIN 55,212–2 causes learning disruption associated with impaired cortical NMDA receptor function and emotional reactivity changes in rat offspring. Cereb Cortex. 2005;15(12):2013–20.
Campolongo P, Trezza V, Cassano T, Gaetani S, Morgese MG, Ubaldi M, et al. Perinatal exposure to delta-9-tetrahydrocannabinol causes enduring cognitive deficits associated with alteration of cortical gene expression and neurotransmission in rats. Addict Biol. 2007;12(3–4):485–95.
O’Shea M, Mallet PE. Impaired learning in adulthood following neonatal delta9-THC exposure. Behav Pharmacol. 2005;16(5–6):455–61.
O’Shea M, McGregor IS, Mallet PE. Repeated cannabinoid exposure during perinatal, adolescent or early adult ages produces similar longlasting deficits in object recognition and reduced social interaction in rats. J Psychopharmacol. 2006;20(5):611–21.
Rubio P, Rodriguez de Fonseca F, Munoz RM, Ariznavarreta C, Martin-Calderon JL, Navarro M. Long-term behavioral effects of perinatal exposure to delta9-tetrahydrocannabinol in rats: possible role of pituitary-adrenal axis. Life Sci. 1995;56(23–24):2169–76.
Moreno M, Trigo JM, Escuredo L, Rodriguez de Fonseca F, Navarro M. Perinatal exposure to delta9-tetrahydrocannabinol increases presynaptic dopamine D2 receptor sensitivity: a behavioral study in rats. Pharmacol Biochem Behav. 2003;75(3):565–75.
Navarro M, de Miguel R, Rodriguez de Fonseca F, Ramos JA, Fernandez-Ruiz JJ. Perinatal cannabinoid exposure modifies the sociosexual approach behavior and the mesolimbic dopaminergic activity of adult male rats. Behav Brain Res. 1996;75(1–2):91–8.
Newsom RJ, Kelly SJ. Perinatal delta-9-tetrahydrocannabinol exposure disrupts social and open field behavior in adult male rats. Neurotoxicol Teratol. 2008;30(3):213–9.
Llorente R, Arranz L, Marco EM, Moreno E, Puerto M, Guaza C, et al. Early maternal deprivation and neonatal single administration with a cannabinoid agonist induce long-term sex-dependent psychoimmunoendocrine effects in adolescent rats. Psychoneuroendocrinology. 2007;32(6):636–50.
Schneider M, Drews E, Koch M. Behavioral effects in adult rats of chronic prepubertal treatment with the cannabinoid receptor agonist WIN 55,212–2. Behav Pharmacol. 2005;16(5–6):447–54.
Trezza V, Campolongo P, Cassano T, Macheda T, Dipasquale P, Carratu MR, et al. Effects of perinatal exposure to delta-9-tetrahydrocannabinol on the emotional reactivity of the offspring: a longitudinal behavioral study in Wistar rats. Psychopharmacology (Berl). 2008;198(4):529–37.
Vela G, Martin S, Garcia-Gil L, Crespo JA, Ruiz-Gayo M, Fernandez-Ruiz JJ, et al. Maternal exposure to delta9-tetrahydrocannabinol facilitates morphine self-administration behavior and changes regional binding to central mu opioid receptors in adult offspring female rats. Brain Res. 1998;807(1–2):101–9.
Gonzalez B, de Miguel R, Martin S, Perez-Rosado A, Romero J, Garcia-Lecumberri C, et al. Effects of perinatal exposure to delta9-tetrahydrocannabinol on operant morphine-reinforced behavior. Pharmacol Biochem Behav. 2003;75(3):577–84.
Economidou D, Mattioli L, Ubaldi M, Lourdusamy A, Soverchia L, Hardiman G, et al. Role of cannabinoidergic mechanisms in ethanol self-administration and ethanol seeking in rat adult offspring following perinatal exposure to Delta9-tetrahydrocannabinol. Toxicol Appl Pharmacol. 2007;223(1):73–85.
Fernandez-Ruiz JJ, Berrendero F, Hernandez ML, Romero J, Ramos JA. Role of endocannabinoids in brain development. Life Sci 1999;65(6–7):725–36.
Vela G, Fuentes JA, Bonnin A, Fernandez-Ruiz J, Ruiz-Gayo M. Perinatal exposure to delta9-tetrahydrocannabinol (delta9-THC) leads to changes in opioid-related behavioral patterns in rats. Brain Res. 1995;680(1–2):142–7.
Corchero J, Garcia-Gil L, Manzanares J, Fernandez-Ruiz JJ, Fuentes JA, Ramos JA. Perinatal delta9-tetrahydrocannabinol exposure reduces proenkephalin gene expression in the caudate-putamen of adult female rats. Life Sci. 1998;63(10):843–50.
Suarez I, Bodega G, Fernandez-Ruiz J, Ramos JA, Rubio M, Fernandez B. Down-regulation of the AMPA glutamate receptor subunits GluR1 and GluR2/3 in the rat cerebellum following pre- and perinatal delta9-tetrahydrocannabinol exposure. Cerebellum. 2004;3(2):66–74.
Ferraro L, Tomasini MC, Beggiato S, Gaetani S, Cassano T, Cuomo V, et al. Short- and long-term consequences of prenatal exposure to the cannabinoid agonist WIN55,212–2 on rat glutamate transmission and cognitive functions. J Neural Transm. 2009;116(8):1017–27.
Suarez I, Bodega G, Fernandez-Ruiz JJ, Ramos JA, Rubio M, Fernandez B. Reduced glial fibrillary acidic protein and glutamine synthetase expression in astrocytes and Bergmann glial cells in the rat cerebellum caused by delta(9)-tetrahydrocannabinol administration during development. Dev Neurosci. 2002;24(4):300–12.
Stella N. Cannabinoid signaling in glial cells. Glia. 2004;48(4):267–77.
Blakemore SJ. Teenage kicks: cannabis and the adolescent brain. Lancet. 2013;381(9870):888–9.
SAMHSA. Results from the 2008 National Survey on Drug Use and Health National Findings: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Office of Applied Studies, North Carolina. 2008.
Pope HG, Jr., Gruber AJ, Hudson JI, Cohane G, Huestis MA, Yurgelun-Todd D. Early-onset cannabis use and cognitive deficits: what is the nature of the association? Drug Alcohol Depend. 2003;69(3):303–10.
Zammit S, Allebeck P, Andreasson S, Lundberg I, Lewis G. Self reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: historical cohort study. BMJ. 2002;325(7374):1199.
Di Forti M, Morgan C, Dazzan P, Pariante C, Mondelli V, Marques TR, et al. High-potency cannabis and the risk of psychosis. Br J Psychiatry. 2009;195(6):488–91.
Schneider M, Schomig E, Leweke FM. Acute and chronic cannabinoid treatment differentially affects recognition memory and social behavior in pubertal and adult rats. Addict Biol. 2008;13(3–4):345–57.
Schneider M, Koch M. Chronic pubertal, but not adult chronic cannabinoid treatment impairs sensorimotor gating, recognition memory, and the performance in a progressive ratio task in adult rats. Neuropsychopharmacology. 2003;28(10):1760–9.
O’Shea M, Singh ME, McGregor IS, Mallet PE. Chronic cannabinoid exposure produces lasting memory impairment and increased anxiety in adolescent but not adult rats. J Psychopharmacol. 2004;18(4):502–8.
Quinn HR, Matsumoto I, Callaghan PD, Long LE, Arnold JC, Gunasekaran N, et al. Adolescent rats find repeated Delta(9)-THC less aversive than adult rats but display greater residual cognitive deficits and changes in hippocampal protein expression following exposure. Neuropsychopharmacology. 2008;33(5):1113–26.
Harte LC, Dow-Edwards D. Sexually dimorphic alterations in locomotion and reversal learning after adolescent tetrahydrocannabinol exposure in the rat. Neurotoxicol Teratol. 2010;32(5):515–24.
Viveros MP, Mendrek A, Paus T, Lopez-Rodriguez AB, Marco EM, Yehuda R, et al. A comparative, developmental, and clinical perspective of neurobehavioral sexual dimorphisms. Front Neurosci. 2012;6:84.
Chadwick B, Miller ML, Hurd YL. Cannabis Use during Adolescent Development: Susceptibility to Psychiatric Illness. Front Psychiatry. 2013;4:129.
Biscaia M, Marin S, Fernandez B, Marco EM, Rubio M, Guaza C, et al. Chronic treatment with CP 55,940 during the peri-adolescent period differentially affects the behavioural responses of male and female rats in adulthood. Psychopharmacology (Berl). 2003;170(3):301–8.
Rubino T, Vigano D, Realini N, Guidali C, Braida D, Capurro V, et al. Chronic delta9-tetrahydrocannabinol during adolescence provokes sex-dependent changes in the emotional profile in adult rats: behavioral and biochemical correlates. Neuropsychopharmacology. 2008;33(11):2760–71.
Patton GC, Coffey C, Carlin JB, Degenhardt L, Lynskey M, Hall W. Cannabis use and mental health in young people: cohort study. BMJ. 2002;325(7374):1195–8.
Lynskey MT, Heath AC, Bucholz KK, Slutske WS, Madden PA, Nelson EC, et al. Escalation of drug use in early-onset cannabis users vs co-twin controls. JAMA. 2003 22–29;289(4):427–33.
Agrawal A, Neale MC, Prescott CA, Kendler KS. Cannabis and other illicit drugs: comorbid use and abuse/dependence in males and females. Behav Genet. 2004;34(3):217–28.
Fergusson DM, Boden JM, Horwood LJ. Cannabis use and other illicit drug use: testing the cannabis gateway hypothesis. Addiction. 2006;101(4):556–69.
Ellgren M, Spano SM, Hurd YL. Adolescent cannabis exposure alters opiate intake and opioid limbic neuronal populations in adult rats. Neuropsychopharmacology. 2007;32(3):607–15.
Biscaia M, Fernandez B, Higuera-Matas A, Miguens M, Viveros MP, Garcia-Lecumberri C, et al. Sex-dependent effects of periadolescent exposure to the cannabinoid agonist CP-55,940 on morphine self-administration behaviour and the endogenous opioid system. Neuropharmacology. 2008;54(5):863–73.
Spano MS, Ellgren M, Wang X, Hurd YL. Prenatal cannabis exposure increases heroin seeking with allostatic changes in limbic enkephalin systems in adulthood. Biol Psychiatry. 2007;61(4):554–63.
Higuera-Matas A, Soto-Montenegro ML, del Olmo N, Miguens M, Torres I, Vaquero JJ, et al. Augmented acquisition of cocaine self-administration and altered brain glucose metabolism in adult female but not male rats exposed to a cannabinoid agonist during adolescence. Neuropsychopharmacology. 2008;33(4):806–13.
Tomasiewicz HC, Jacobs MM, Wilkinson MB, Wilson SP, Nestler EJ, Hurd YL. Proenkephalin mediates the enduring effects of adolescent cannabis exposure associated with adult opiate vulnerability. Biol Psychiatry. 2012;72(10):803–10.
Pistis M, Perra S, Pillolla G, Melis M, Muntoni AL, Gessa GL. Adolescent exposure to cannabinoids induces long-lasting changes in the response to drugs of abuse of rat midbrain dopamine neurons. Biol Psychiatry 2004.;56(2):86–94.
Hajos M, Hoffmann WE, Kocsis B. Activation of cannabinoid-1 receptors disrupts sensory gating and neuronal oscillation: relevance to schizophrenia. Biol Psychiatry. 2008;63(11):1075–83.
Raver SM, Haughwout SP, Keller A. Adolescent cannabinoid exposure permanently suppresses cortical oscillations in adult mice. Neuropsychopharmacology. 2013;38(12):2338–47.
Gleason KA, Birnbaum SG, Shukla A, Ghose S. Susceptibility of the adolescent brain to cannabinoids: long-term hippocampal effects and relevance to schizophrenia. Transl Psychiatry. 2012;2:e199.
Page ME, Oropeza VC, Sparks SE, Qian Y, Menko AS, Van Bockstaele EJ. Repeated cannabinoid administration increases indices of noradrenergic activity in rats. Pharmacol Biochem Behav. 2007;86(1):162–8.
Bambico FR, Nguyen NT, Katz N, Gobbi G. Chronic exposure to cannabinoids during adolescence but not during adulthood impairs emotional behaviour and monoaminergic neurotransmission. Neurobiol Dis. 2010;37(3):641–55.
Tagliaferro P, Javier Ramos A, Onaivi ES, Evrard SG, Lujilde J, Brusco A. Neuronal cytoskeleton and synaptic densities are altered after a chronic treatment with the cannabinoid receptor agonist WIN 55,212–2. Brain Res. 2006;1085(1):163–76.
Rubino T, Realini N, Braida D, Guidi S, Capurro V, Vigano D, et al. Changes in hippocampal morphology and neuroplasticity induced by adolescent THC treatment are associated with cognitive impairment in adulthood. Hippocampus. 2009;19(8):763–72.
Lopez-Gallardo M, Lopez-Rodriguez AB, Llorente-Berzal A, Rotllant D, Mackie K, Armario A, et al. Maternal deprivation and adolescent cannabinoid exposure impact hippocampal astrocytes, CB1 receptors and brain-derived neurotrophic factor in a sexually dimorphic fashion. Neuroscience. 2012;204:90–103.
Realini N, Vigano D, Guidali C, Zamberletti E, Rubino T, Parolaro D. Chronic URB597 treatment at adulthood reverted most depressive-like symptoms induced by adolescent exposure to THC in female rats. Neuropharmacology. 2011;60(2–3):235–43.
Rubino T, Realini N, Braida D, Alberio T, Capurro V, Vigano D, et al. The depressive phenotype induced in adult female rats by adolescent exposure to THC is associated with cognitive impairment and altered neuroplasticity in the prefrontal cortex. Neurotox Res. 2009;15(4):291–302.
Yucel M, Solowij N, Respondek C, Whittle S, Fornito A, Pantelis C, et al. Regional brain abnormalities associated with long-term heavy cannabis use. Arch Gen Psychiatry. 2008;65(6):694–701.
Mata I, Perez-Iglesias R, Roiz-Santianez R, Tordesillas-Gutierrez D, Pazos A, Gutierrez A, et al. Gyrification brain abnormalities associated with adolescence and early-adulthood cannabis use. Brain Res. 2010;1317:297–304.
Arnone D, Barrick TR, Chengappa S, Mackay CE, Clark CA, Abou-Saleh MT. Corpus callosum damage in heavy marijuana use: preliminary evidence from diffusion tensor tractography and tract-based spatial statistics. Neuroimage. 2008;41(3):1067–74.
Zalesky A, Solowij N, Yucel M, Lubman DI, Takagi M, Harding IH, et al. Effect of long-term cannabis use on axonal fibre connectivity. Brain. 2012;135(Pt 7):2245–55.
Gruber SA, Silveri MM, Dahlgren MK, Yurgelun-Todd D. Why so impulsive? White matter alterations are associated with impulsivity in chronic marijuana smokers. Exp Clin Psychopharmacol. 2011;19(3):231–42.
Lorenzetti V, Solowij N, Fornito A, Lubman DI, Yucel M. The Association between Regular Cannabis Exposure and Alterations of Human Brain Morphology: An Updated Review of the Literature. Curr Pharm Des. 2014;20(13):2138–67.
Mehmedic Z, Chandra S, Slade D, Denham H, Foster S, Patel AS, et al. Potency trends of Delta9-THC and other cannabinoids in confiscated cannabis preparations from 1993 to 2008. J Forensic Sci. 2010;55(5):1209–17.
Seely KA, Lapoint J, Moran JH, Fattore L. Spice drugs are more than harmless herbal blends: a review of the pharmacology and toxicology of synthetic cannabinoids. Prog Neuropsychopharmacol Biol Psychiatry. 2012;39(2):234–43.
EMCDDA. Thematic paper- Understanding the ‘Spice’ phenomenon. Luxembourg: Office for Official Publications of the European Communities 2009 Contract No.: ISBN 978–92-9168–411–3, doi:10.2810/27063.
Thomas A, Baillie GL, Phillips AM, Razdan RK, Ross RA, Pertwee RG. Cannabidiol displays unexpectedly high potency as an antagonist of CB1 and CB2 receptor agonists in vitro. Br J Pharmacol. 2007;150(5):613–23.
Bhattacharyya S, Morrison PD, Fusar-Poli P, Martin-Santos R, Borgwardt S, Winton-Brown T, et al. Opposite effects of delta-9-tetrahydrocannabinol and cannabidiol on human brain function and psychopathology. Neuropsychopharmacology. 2010;35(3):764–74.
Caspi A, Moffitt TE, Cannon M, McClay J, Murray R, Harrington H, et al. Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O-methyltransferase gene: longitudinal evidence of a gene X environment interaction. Biol Psychiatry. 2005;57(10):1117–27.
Henquet C, Rosa A, Krabbendam L, Papiol S, Fananas L, Drukker M, et al. An experimental study of catechol-o-methyltransferase Val158Met moderation of delta-9-tetrahydrocannabinol-induced effects on psychosis and cognition. Neuropsychopharmacology. 2006;31(12):2748–57.
Zammit S, Spurlock G, Williams H, Norton N, Williams N, O’Donovan MC, et al. Genotype effects of CHRNA7, CNR1 and COMT in schizophrenia: interactions with tobacco and cannabis use. Br J Psychiatry. 2007;191:402–7.
van Winkel R van Beveren NJ Simons C. AKT1 moderation of cannabis-induced cognitive alterations in psychotic disorder. Neuropsychopharmacology. 2011;36(12):2529–37.
Agrawal A, Lynskey MT. Correlates of later-onset cannabis use in the National Epidemiological Survey on Alcohol and Related Conditions (NESARC). Drug Alcohol Depend. 2009;105(1–2):71–5.
Wegener N, Koch M. Neurobiology and systems physiology of the endocannabinoid system. Pharmacopsychiatry. 2009;42 Suppl 1:S79–86.
Llorente-Berzal A, Fuentes S, Gagliano H, Lopez-Gallardo M, Armario A, Viveros MP, et al. Sex-dependent effects of maternal deprivation and adolescent cannabinoid treatment on adult rat behaviour. Addict Biol. 2011;16(4):624–37.
Llorente-Berzal A, Puighermanal E, Burokas A, Ozaita A, Maldonado R, Marco EM, et al. Sex-dependent psychoneuroendocrine effects of THC and MDMA in an animal model of adolescent drug consumption. PLoS ONE 2013;8(11):e78386.
Higuera-Matas A, Botreau F, Miguens M, Del Olmo N, Borcel E, Perez-Alvarez L, et al. Chronic periadolescent cannabinoid treatment enhances adult hippocampal PSA-NCAM expression in male Wistar rats but only has marginal effects on anxiety, learning and memory. Pharmacol Biochem Behav. 2009;93(4):482–90.
Abush H, Akirav I. Short- and long-term cognitive effects of chronic cannabinoids administration in late-adolescence rats. PLoS ONE. 2012;7(2):e31731.
O’Tuathaigh CM, Clarke G, Walsh J, Desbonnet L, Petit E, O’Leary C, et al. Genetic vs. pharmacological inactivation of COMT influences cannabinoid-induced expression of schizophrenia-related phenotypes. Int J Neuropsychopharmacol. 2012;15(9):1331–42.
Cha YM, Jones KH, Kuhn CM, Wilson WA, Swartzwelder HS. Sex differences in the effects of delta9-tetrahydrocannabinol on spatial learning in adolescent and adult rats. Behav Pharmacol. 2007;18(5–6):563–9.
Renard J, Krebs MO, Jay TM, Le Pen G. Long-term cognitive impairments induced by chronic cannabinoid exposure during adolescence in rats: a strain comparison. Psychopharmacology (Berl). 2013;225(4):781–90.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Viveros, MP., Marco, E. (2015). Age-Dependent Effects of Cannabinoids on Neurophysiological, Emotional, and Motivational States. In: Campolongo, P., Fattore, L. (eds) Cannabinoid Modulation of Emotion, Memory, and Motivation. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-2294-9_11
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2294-9_11
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-2293-2
Online ISBN: 978-1-4939-2294-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)