
Abstract
The mesenteric vascular supply is a combination of rich collateral networks and commonly encountered variant anatomy. The effect of normal and variant anatomy has implications on pathology, treatment choices, and planning interventions. The goal of this chapter is to review the standard vascular anatomy with details of the potential collateral systems that may be present. Finally, a review of anatomic variants will assist in understanding the implications of abnormal anatomy on treatment for diseases associated with the mesentery.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Mesenteric artery anatomy
- Mesenteric artery collaterals
- Variant arterial anatomy
- Anatomy of mesenteric artery
- Inferior mesenteric artery
The mesenteric vascular supply is a combination of rich collateral networks and commonly encountered variant anatomy. The effect of normal and variant anatomy has implications on pathology, treatment choices, and planning interventions. The goal of this chapter is to review the standard vascular anatomy with details of the potential collateral systems that may be present. Finally, a review of anatomic variants will assist in understanding the implications of abnormal anatomy on treatment for diseases associated with the mesentery.
Embryology
Understanding the vascular supply of the mesentery and the pathological implications of mesenteric vascular disease is best understood by a solid appreciation for the embryologic development of the mesenteric structures and their blood supply. This helps the clinician understand the pathological consequences of diseases of the mesenteric vasculature.
At three weeks, the early embryo consists of three flat germ layers (endoderm, mesoderm, and ectoderm) that will develop along separate paths to create each necessary organ system and tissue (endoderm will form the aerodigestive tract, and the mesoderm will form the mesenchymal tissue including the vasculature). The primitive gut is derived from the endodermal germ layer as it undergoes tubal formation. The cranial and caudal aspects fold to form the foregut and hindgut, while the intervening segment (midgut) remains open to the yolk sac, creating the yolk stalk (the eventual omphalomesenteric or vitelline duct). These three distinct segments of the primitive gut have important implications for mesenteric vascular supply.
At about the same time, the embryo becomes too large to meet its metabolic needs by simple diffusion alone. The circulatory system begins its iterative development to support embryonic growth and formation. The paired dorsal aortae develop three sets of paired arterial branches: the dorsal intersegmental, the lateral segmental, and the ventral segmental vessels. The paired ventral segmental arteries course over the dorsal and lateral walls of the gut and yolk sac. Ultimately, as the dorsal aorta fuse, so do specific paired ventral vessels, namely, the 10th, 13th, and 21st. They fuse in the midline with gut closure and narrowing of the dorsal mesentery to form the celiac artery, superior mesenteric artery (SMA), and inferior mesenteric artery (IMA), respectively.
These three vessels go on to provide the blood supply for each segment of the developing gut. The foregut will form the lower esophagus to the duodenum and be supplied by the celiac artery. The midgut will form the lower duodenum to the cranial half of the transverse colon and be supplied by the SMA. Finally, the hindgut will form the caudal half of the transverse colon to the superior rectum and be supplied by the IMA [1].
Normal Anatomy
Normal mesenteric vascular anatomy is based on these three separate branches of the aorta [2]. Although not all patients will display normal mesenteric vascular anatomy, as this may have implications for disease treatment.
Celiac Artery
As the aorta passes below the crus of the diaphragm at the 12th thoracic vertebra, it immediately gives of the celiac artery (also referred to as the celiac trunk or celiac axis) a wide ventrally oriented branch that typically trifurcates during its 1.5 cm length. Of note, there may be a paired set of inferior phrenic vessels that come off the aorta more laterally to supply the inferior diaphragm at this location. Branches include [2]:
-
1.
Left gastric artery
-
2.
Splenic artery
-
a.
Dorsal and caudal pancreatic arteries
-
b.
Short gastric arteries
-
c.
Left gastroepiploic artery
-
d.
Posterior gastric artery
-
a.
-
3.
Common hepatic artery
-
a.
Gastroduodenal artery
-
i.
Right gastroepiploic artery
-
ii.
Superior anterior and posterior pancreaticoduodenal arteries
-
i.
-
b.
Right gastric artery
-
c.
Left hepatic artery
-
d.
Right hepatic artery
-
a.
The typical configuration of the celiac artery is to give off a small left gastric artery and then divide into the splenic artery and the common hepatic artery (Fig. 2.1). This anatomy is present in approximately 50 % of the population. The left gastric and the splenic artery travel to the left, while the common hepatic artery turns towards the right and the porta hepatis.

Celiac artery anatomy and superior mesenteric artery collaterals. CA celiac artery, SMA superior mesenteric artery (By permission of Mayo Foundation for Medical Education and Research. All rights reserved)
The left gastric artery may originate from the aorta or anywhere along the celiac artery. It travels superiorly supplying the distal esophagus and then descends along the lesser curvature of the stomach to collateralize with the right gastric artery (Figs. 2.1 and 2.2a). Importantly, the left hepatic artery may be replaced, originating from the left gastric. When present, it is important to preserve this during access to the supraceliac aorta though the lesser sac. Conversely, the left hepatic artery may supply an accessory left gastric artery.

Gastric and bowel collateral networks. (a) Gastric collaterals. Right and left gastric arteries collateralize along the lesser curvature, while the right and left gastroepiploic arteries collateralize along the greater curvature of the stomach. (b) Celiac to superior mesenteric artery (SMA) collaterals include the arch of Bühler and gastroduodenal arcade. SMA to inferior mesenteric artery (IMA) collaterals include the arc of Riolan and the marginal artery of Drummond. Perirectal collaterals form from the IMA, superior rectal artery, and internal iliac artery (By permission of Mayo Foundation for Medical Education and Research. All rights reserved)
The splenic artery originates from the celiac artery 80 % of the time. As the splenic artery traverses to the left, it gives off segmental branches to the pancreas (the dorsal pancreatic and caudal pancreatic arteries). These supply the body and the tail of the pancreas, respectively, collateralizing via the transverse pancreatic artery (Fig. 2.1). Distal branches of the splenic artery include the short gastric arteries, posterior gastric, left gastroepiploic, and the terminal splenic branches. The short gastric arteries number from 1 to 4 and collateralize to the greater curvature of the stomach and the aforementioned left gastric artery. The posterior gastric artery supplies the posterior fundus of the stomach. The left gastroepiploic artery often arises from the distal splenic artery in a common branch with the inferior splenic branch but may be a single branch. It travels along the greater curvature of the stomach giving off omental branches and collateralizing with the right gastroepiploic artery (Figs. 2.1 and 2.2a).
The common hepatic artery is the final branch of the celiac artery. It is of variable length and ends at the gastroduodenal artery branch, after which it continues as the proper hepatic artery to supply the liver and gallbladder. The proper hepatic artery bifurcates into the right and left hepatic arteries (Fig. 2.1). Alternatively, there may be a trifurcation of the common hepatic artery with no proper hepatic artery. The proper hepatic artery or only the right hepatic may arise from the SMA as variants. As mentioned, the left hepatic artery may arise from the left gastric artery. The right gastric artery may arise anywhere along the common or proper hepatic artery to collateralize along the lesser curvature with the left gastric artery (Figs. 2.1 and 2.2a).
The gastroduodenal artery passes inferiorly between the duodenum and the pancreas, giving rise to the right gastroepiploic artery and the superior pancreaticoduodenal artery. This has anterior and posterior divisions that are important collaterals to the superior mesenteric artery (Figs. 2.1 and 2.3).

Celiac artery and superior mesenteric artery collaterals. CHA common hepatic artery, SA splenic artery, RGA right gastric artery, PHA proper hepatic artery, GDA gastroduodenal artery, SMA superior mesenteric artery, SPDA superior pancreaticoduodenal artery, IPDA inferior pancreaticoduodenal artery
Superior Mesenteric Artery (SMA)
The SMA is the second ventral branch of the abdominal aorta. As mentioned above in the discussion of embryology, this artery will supply the distal duodenum, the small intestine, and the large intestine to the mid transverse colon. Given the vitally important structures its supplies and the important collaterals it provides to both the celiac and IMA, there is a very high morbidity associated with SMA occlusions. Anatomically, the SMA origin is about a centimeter distal to the celiac artery and accessible through the lesser sac near the superior border of the pancreas. The SMA comes off at an acute angle in comparison to the celiac artery. In this aortomesenteric angle, the left renal vein and the fourth portion of the duodenum pass. If this angle is too acute, it may lead to either nutcracker syndrome or SMA syndrome. Symptoms include flank pain and hematuria related to renal vein compression for the former and a gastric outlet obstruction syndrome related to the latter.
SMA branches include [2]:
-
1.
Inferior anterior and posterior pancreaticoduodenal arteries
-
2.
Middle colic artery
-
3.
Right colic artery
-
4.
Ileocolic artery
-
5.
Jejunal and ileal branches
The first branches of the SMA include the inferior pancreaticoduodenal artery. This comes off the right side of the SMA and divides in to an anterior posterior branch that collateralize to the celiac artery via the previously mentioned collateral pathway (Figs. 2.1, 2.2, and 2.3). The middle colic artery arises from the proximal SMA after passing below the pancreas. This artery travels to the transverse mesocolon giving a right and left branch. During an infracolic exposure of the SMA, when this artery is identified within the transverse mesocolon, it can be followed down to identify the SMA. Within the mid SMA, the right colic artery originates. It is the last branch off the right side of the SMA. As the right colic artery traverses behind the parietal peritoneum, its supplies a descending and ascending branch. The ascending branch collateralizing with the middle colic artery and supplies the ascending right colon. The descending branch collateralizes to the ileocolic artery, supplying the more proximal right colon (Figs. 2.4 and 2.5).

Superior mesenteric artery and inferior mesenteric artery anatomy and collaterals. SMA superior mesenteric artery, IMA inferior mesenteric artery, IC ileocolic artery, RC right colic artery, MC middle colic artery, LC left colic artery, SA sigmoid arteries, SR superior rectal artery. The marginal artery of Drummond is formed by the arterial network from the ileocolic to the superior rectal. Critical regions of collateralization include Griffith’s point (SMA to IMA) and Sudeck’s point (IMA to internal iliac artery) (By permission of Mayo Foundation for Medical Education and Research. All rights reserved)

Superior mesenteric artery angiographic anatomy. IC ileocolic artery, RC right colic artery, MC middle colic artery, JB jejunal branches
The ileocolic artery is the final major branch of the SMA but may share a common origin with the right colic artery. The ileocolic artery vascularizes the terminal ileum, right colon, cecum, and appendix. There are four identifiable branches. These included the descending branch (to the right colon), cecal branch (an anterior and posterior), ileal branch, and the appendicular artery (to the appendix). Finally, on the left aspect of the SMA arise the multiple jejunal and ileal branches. These fan out, forming several arches to create a collateralized network to the small bowel (Figs. 2.4 and 2.5).
Inferior Mesenteric Artery
The inferior mesenteric artery is responsible for supplying blood flow to the distal third of the transverse colon, descending colon, sigmoid colon, as well as the upper rectum. It originates in an anterior lateral orientation to the left just above the aortic bifurcation, typically between the L2 and L4 vertebral bodies [3]. It travels in a retroperitoneal plane towards the sigmoid colon.
Branches include [2]:
-
1.
Left colic artery
-
2.
Sigmoid arteries
-
3.
Superior rectal artery
The left colic artery is comprised of an ascending and descending branch. The ascending collateralizes to the middle colic artery, distal transverse colon, and splenic flexure (Griffith’s point [4], Fig. 2.4). This collateralization is important, as this area is at high risk for watershed ischemia in the setting of dehydration or mesenteric occlusive disease. The descending left colic artery branch collateralizes to the sigmoid arteries. These are comprised of two or three sigmoid artery branches within the mesocolon. The uppermost sigmoid artery collateralizes to the left colic artery, whereas the lowermost collateralizes to the superior rectal artery. The superior rectal artery descends into the pelvis dividing into right and left branches. The superior rectal artery collateralizes with both the middle rectal (branch of the internal iliac artery) and the inferior rectal artery (branch of the internal pudendal artery, Fig. 2.4).
Collateral Pathways
The mesenteric vasculature is rich with collateral blood supply. It is typically necessary to have disease in multiple vessels for clinical sequelae to develop due to the number of collateral networks. It is often ascribed that in chronic mesenteric ischemia, at least two of the three mesenteric arteries must be severely diseased, one of which being the SMA, for symptoms to be present due to this collateral network. The overall collateral blood supply can be thought of within three distinct patterns. These include collaterals within the same vessel distribution, between mesenteric vessels, and between the mesenteric and the parietal circulation [5].
Within Vessel Collaterals [5]
Celiac Axis
-
1.
Collaterals between the left and right gastric and left and right gastroepiploic vessels to supply the stomach (Figs. 2.1 and 2.2a).
-
2.
The fundus of the stomach possesses collaterals between the left gastric and short gastric arteries (from the splenic artery).
-
3.
Pancreatic anastomotic collaterals between the pancreatic branches of the GDA and splenic origin (Fig. 2.1).
SMA
-
1.
Collaterals between the inferior pancreaticoduodenal and jejunal vessels.
-
2.
Collaterals between first and second jejunal vessels.
-
3.
The collateral cascade between the right, middle, and ileocolic arteries as they formed the marginal artery of Drummond (Figs. 2.2b and 2.4).
IMA
-
1.
Collaterals between the sigmoid, rectosigmoid, and superior rectal arteries and their formation of the latter part of the marginal artery of Drummond (Figs. 2.2b and 2.4).
Between Mesenteric Vessels
Celiac and SMA Collaterals
-
1.
The arch of Bühler – an embryological remnant of an artery that linked the celiac and SMA (Fig. 2.2b) [6].
-
2.
The pancreaticoduodenal arteries link the celiac and SMA via the superior and inferior pancreaticoduodenal arteries, respectively (Figs. 2.1, 2.2, and 2.3).
-
3.
If present, an aberrant middle colic artery originating from the celiac would form collaterals to the SMA.
SMA and IMA Collaterals
The collateral circulation between the SMA and IMA is critically important, especially in the setting of chronic mesenteric ischemia. It is also a source of access for embolization of type II endoleaks after endovascular aneurysm repair. However, the terminology surrounding this collateral network is confusing. This is due to variations in nomenclature over time [7].
-
1.
The marginal artery – the marginal artery (of Drummond) is a potential collateral pathway that connects the superior mesenteric and inferior mesenteric arterial systems. This anastomotic channel originates from the descending branch of the ileocolic artery. It involves the communication of this branch to the right colic artery via the right colic artery’s descending and ascending branches, then the right and left branches of the middle colic artery, the ascending and descending branches of the left colic artery, and the sigmoid branches of the inferior mesenteric artery terminating in the superior rectal artery (Figs. 2.2b and 2.4). When well developed, this can be a rich source of collateral circulation to the colon, particularly in the event of colonic resection. The artery may run close to the bowel wall or in some instances more within the mesentery. Less than 50 % of the time, this collateral pathway may not be complete at the splenic flexure, a location named Griffith’s point (Fig. 2.4). This void of collaterals from the left branch of the middle colic artery to the ascending left colic artery can result in colonic ischemia in the setting of bowel surgery or occlusive disease [4, 7].
-
2.
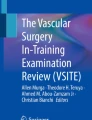
Meandering mesenteric artery (also referred to as the arc of Riolan or meandering mesenteric artery of Moskowitz) [8] – this represents another collateral pathway between the SMA and IMA. It was named after anatomist Jean Riolan. When present, this connects the middle colic artery of the SMA with the left colic branch of the IMA (Fig. 2.2b). In the era of endovascular aneurysm repair, this is an important collateral pathway to permit coil embolization for type II endoleaks (Fig. 2.6).
Fig. 2.6 
Arc of Riolan. Catheter is placed in the middle colic artery through the SMA. The collateral connects to the IMA, in this case resulting in a type II endoleak after endovascular aneurysm repair. AR arc of Riolan, IMA inferior mesenteric artery

Mesenteric and Parietal Arterial Collaterals
-
1.
Collaterals flow may exist between the celiac artery and parietal circulation from the esophageal branches of the inferior phrenic artery to the left gastric and short gastric arteries.
-
2.
Although typically obliterated, the falciform ligament, if recanalized, can be a source of collateral flow between the hepatic arteries and internal thoracic and superior epigastric arteries.
-
3.
The IMA and the internal iliac artery form a perirectal plexus involving collaterals between the superior rectal, middle sacral, and middle and inferior rectal vessels (Sudeck’s point – collateral communication between last sigmoidal branch and the superior rectal, Fig. 2.4) [3, 9].
-
4.
The middle sacral artery can collateralize to the IMA circulation [3].
-
5.
Less common collaterals can develop to permit collateral blood flow (1) to the liver via intercostal posterior abdominal wall arteries, (2) to the renal capsule via the marginal artery, and (3) from lumbar arteries on the posterior abdominal wall to the marginal artery [5].
Variant Anatomy
The anatomy of mesenteric vascular structures is highly variable. It is quite common to encounter patients with variations of either the celiac, SMA, or IMA, although the first two are much more common.
Celiac Artery Variants
The “normal” celiac artery consists of the left gastric, splenic, and common hepatic arteries as described above (Fig. 2.7a). This occurs in 55–89 % in series of anatomic dissections and arteriograms performed over the last 50 years [10–12]. In <10 % of cases, the common hepatic artery originates separate from the aorta, while the left gastric and splenic arteries form a common origin (gastrosplenic trunk, Fig. 2.7b). Less commonly, a hepatosplenic (Fig. 2.7c) or hepatogastric trunk (Fig. 2.7d) is formed, with the remaining branch coming from the aorta. In rare circumstances, the SMA originates from the celiac artery as a common celiacomesenteric axis (Fig. 2.7e) [12]. The left gastric artery is a relatively constant structure. However, it may give rise to an accessory left hepatic artery (1–16 % of cases) or a replaced left hepatic artery 10 % of the time [10, 11, 13].

Celiac artery anatomic variants. (a) Normal celiac artery anatomy with left gastric, common hepatic, and splenic artery, (b) gastrosplenic artery with separate common hepatic artery origin. (c) Hepatosplenic artery with separate left gastric origin. (d) Hepatogastric artery with separate splenic artery origin. (e) Celiacomesenteric axis – combined celiac and superior mesenteric artery origin (By permission of Mayo Foundation for Medical Education and Research. All rights reserved)
The common hepatic artery and the pancreaticoduodenal arcade anatomy can be highly variable. Variations can occur in all vessels and their branches. Detailed descriptions of all possible anatomic variants are beyond the scope of this chapter, and further descriptions are available in other texts [14]. The “typical” common hepatic artery arising from the celiac artery may occur in 80 % of cases. The most common variant is the absence of the common hepatic artery in 12 % of cases, while a common hepatic origin from the SMA occurs in <5 % of cases [12, 15]. If the common hepatic artery is absent, its branches may originate from the aorta, the SMA, or the celiac artery.
The left and right hepatic artery variants can occur with variations of the common hepatic artery or as isolated variants themselves. As mentioned previously, left hepatic arterial variations occur 20 % of the time in isolation and more often in combination with other variants. This is typically a replaced or accessory left hepatic artery from the left gastric artery. When the common hepatic artery is absent, the left hepatic artery may originate from the aorta or the celiac artery. Variations of the right hepatic artery occur in 6–18 % of cases as either a replaced right hepatic from the SMA (most common 6–11 % [10–15] or an accessory right hepatic artery (2–8 %) [10, 11, 13]). The replaced or accessory right hepatic artery may originate from the SMA (common) or the aorta when no common hepatic artery exists. The cystic artery commonly arises from the right hepatic artery in 70 % of cases; however, its relationship to the common hepatic duct is variable, and accessory cystic arteries may occur in 11 % of cases [15]. The “normal” gastroduodenal artery originating from the common hepatic artery occurs 75 % of the time [15]. Variations in its origin are commonly due to common hepatic artery variants. As such, it may arise from an aberrant common hepatic artery (off the SMA), a replaced right hepatic artery, or the left hepatic artery [12]. Finally, the right gastric artery is in its normal position in half of cases. Variations can include originating from the left or right hepatic artery or the GDA [15].
The splenic artery may be part of anomalous permutations of the celiac artery as discussed previously. The splenic artery can originate from the SMA as opposed to the celiac artery. It may also be duplicated with one or both branches originating from the aorta. Additionally, it may give rise to the left gastric, middle colic, or left hepatic artery [12].
SMA Variants
As noted above, the SMA can have a great number of variants related to arteries typically seen from the celiac axis. The SMA may originate from the celiac axis (Fig. 2.7e) or provide any combination of hepatic arteries, or accessory gastric, splenic, or pancreatic vessels. The “normal” SMA anatomy may be present in as many as 68 % of cases (Fig. 2.8a) [12]. The ileocolic artery appears to be the most consistent structure from the SMA. The other vessels have some degree of variability. Although normally a separate branch, the middle colic artery, can share a common trunk with the right colic artery (middle colic-right colic trunk, Fig. 2.8b) in up to 52 % of cases, representing the most common variant. If not involved in aberrant anatomy with the middle colic artery, the right colic artery may be an independent branch of the SMA (38 %) or a branch of the ileocolic artery in 8 % of cases (Fig. 2.8c). There may be an accessory right colic in 8–10 % of cases. Less commonly, the middle and right colic artery are absent (<10 % of the time), or the middle colic may send a large branch to the splenic flexure. In very rare cases, the middle colic artery may be a branch of the celiac artery [9, 12].

Superior mesenteric artery anatomic variants. IC ileocolic artery, RC right colic artery, MC middle colic artery. (a) normal anatomy with separate IC, RC, and MC origins. (b) Combine MC and RC origin and separate IC origin. (c) Common RC and IC origin and separate MC origin (By permission of Mayo Foundation for Medical Education and Research. All rights reserved)
IMA Variants
The IMA has little variation in terms of position and origin. However, the left colic artery may be limited in its ascension to the splenic flexure in 86 % of cases, threatening the collateralization of the marginal artery in this region. In fact, adequate collateralization may only occur in 60 % of cases at the splenic flexure (Griffith’s point) and in 50 % of cases in the upper rectum (Sudeck’s point) (Fig. 2.4). The predominant variations of the IMA circulation involve the division of the sigmoidal arteries in forming the arterial arcades and collateralization to the internal iliac artery branches. Further details are available from Michels detailed description of these variations [9]. Rarely, there can sigmoidal artery origins from the internal iliac artery [12].
References
Carlson BM. Human embryology and developmental biology. 5th ed. Philadelphia: Elsevier/Saunders; 2013.
Uflacker R, Selby JB. Atlas of vascular anatomy : an angiographic approach. 2nd ed. Phila-delphia: Lippincott Williams & Wilkins; 2007. xiv, 905 p.
Kahn P, Abrams HL. Inferior mesenteric arterial patterns; an angiographic study. Radiology. 1964;82:429–42.
Meyers MA. Griffiths' point: critical anastomosis at the splenic flexure. Significance in ischemia of the colon. Am J Roentgenol. 1976;126(1):77–94.
Geroulakos G, Cherry KJ. Diseases of the visceral circulation. London/New York: Arnold, Distributed in the USA by Oxford University Press; 2002. viii, 228 p., 12 p. of plates.
Rosenblum JD, Boyle CM, Schwartz LB. The mesenteric circulation. Anatomy and physiology. Surg Clin North Am. 1997;77(2):289–306.
Fisher Jr DF, Fry WJ. Collateral mesenteric circulation. Surg Gynecol Obstet. 1987;164(5):487–92.
Gourley EJ, Gering SA. The meandering mesenteric artery: a historic review and surgical implications. Dis Colon Rectum. 2005;48(5):996–1000.
Michels NA, Siddharth P, Kornblith PL, Parke WW. The variant blood supply to the descending colon, rectosigmoid and rectum based on 400 dissections. Its importance in regional resections: a review of medical literature. Dis Colon Rectum. 1965;8:251–78.
Covey AM, Brody LA, Maluccio MA, Getrajdman GI, Brown KT. Variant hepatic arterial anatomy revisited: digital subtraction angiography performed in 600 patients. Radiology. 2002;224(2):542–7.
Hiatt JR, Gabbay J, Busuttil RW. Surgical anatomy of the hepatic arteries in 1000 cases. Ann Surg. 1994;220(1):50–2.
Valentine RJ, Wind GG. Anatomic exposures in vascular surgery. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2003. xiii, 577 p.
De Cecco CN, Ferrari R, Rengo M, Paolantonio P, Vecchietti F, Laghi A. Anatomic variations of the hepatic arteries in 250 patients studied with 64-row CT angiography. Eur Radiol. 2009;19(11):2765–70.
Michels NA. The anatomic variations of the arterial pancreaticoduodenal arcades: their import in regional resection involving the gall bladder, bile ducts, liver, pancreas and parts of the small and large intestines. J Int Coll Surg. 1962;37:13–40.
Daseler EH, Anson BJ, et al. The cystic artery and constituents of the hepatic pedicle; a study of 500 specimens. Surg Gynecol Obstet. 1947;85(1):47–63.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
De Martino, R.R. (2015). Normal and Variant Mesenteric Anatomy. In: Oderich, G. (eds) Mesenteric Vascular Disease. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1847-8_2
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1847-8_2
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1846-1
Online ISBN: 978-1-4939-1847-8
eBook Packages: MedicineMedicine (R0)