
Abstract
This chapter provides an overview of this section and discusses various strategies to reduce risk and design formulations. It provides a stepwise strategy to reduce risk and outlines the risk involved in incorporating different solid forms of drugs into drug products. It addresses solubility, BCS class, instability, and formulation design.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
The first chapter in this section outlined a strategy to reduce risk in early development of solid oral dosage forms. The second chapter summarized strategies for drug candidate phase optimization in discovery space. This chapter outlines later stage screening and formulation design during the development process. In particular, this chapter outlines a strategy to reduce risk in formulation design by determining solid state properties and then incorporating solid forms with known properties into a formulation that does not change that form.
The first step in assessing and reducing risk is understanding whether a solid material for formulation and development exists in a crystalline or amorphous state or mixtures. Figure 8.1 illustrates the crystalline state as a perfectly ordered solid with molecules (circles) packed in an orderly array. Figure 8.1 illustrates an amorphous material as a disordered material with only short-range order. Crystalline materials give an X-ray diffraction pattern because Bragg planes exist in the material (see Fig. 8.2). Amorphous materials do not give a diffraction pattern (see Fig. 8.2). Of course, there are many interesting cases where a pharmaceutical material shows an intermediate degree of order falling somewhere between the highly ordered crystalline state and the disordered amorphous state. From a thermodynamic point of view, crystalline materials are more stable but the rate of transformation of amorphous materials to crystalline materials can be highly variable (Taylor et al. 2010).

Idealized view of crystalline (left panel) and amorphous (right panel) amorphous material. In this two-dimensional figure the molecule are viewed as circle

X-ray diffraction pattern of two samples, crystalline, and amorphous
Additionally, as outlined in the second chapter in this section, crystals of pharmaceutical materials can exist in different forms. These solid-state modifications of a compound are referred to as crystalline forms. When differences between early batches of a substance are found, the use of the term “form” is particularly helpful since it allows subsequent, more accurate, description of a given variant batch (i.e., polymorph, solvate, habit, or amorphous material). The term pseudopolymorphism is applied frequently to designate solvates. These solid state modifications have different physical properties.
To put these definitions into a practical context, consider two cases (aspirin and paroxetine hydrochloride) in which a compound was crystallized for subsequent formulation and different-shaped crystals resulted in each experiment. Although sometimes dramatically different shapes were obtained upon changing solvents for the various crystallizations, the final interpretations in the two cases are different. For aspirin, X-ray powder diffraction showed that all crystals regardless of shape had the same diffraction pattern. Thus, the different shaped crystals are termed crystal habits. For paroxetine hydrochloride, the different shaped crystals had different X-ray powder diffraction patterns. Subsequent analysis showed that the crystals did not contain solvent. Thus, these different crystals are polymorphs. (Note that hydrates of paroxetine hydrochloride also exist.)
Another important step in reducing risk during formulation is to understand the size and shape of the crystalline form to be formulated. Crystals of a pharmaceutical material from different sources can vary greatly in their size and shape. Typical particles in different samples may resemble, for example, needles, rods, plates, prisms, etc. Such differences in shape are collectively referred to as differences in morphology and particle size. Lack of control of particle size represents a risk to control of critical drug product properties for formulation.
1 Risk in Selecting Amorphous Materials for Incorporation into Drug Product
Selecting amorphous materials for a final formulation has substantial risk but also substantial gain. Amorphous materials have no long range order and are thermodynamically metastable as pointed out in Chap. 2 of this series. An amorphous solid is characterized by a unique glass transition temperature T g, the temperature at which it changes from a glass to a rubber. When T rises above T g, the rigid solid can flow and the corresponding increase in molecular mobility can result in crystallization or increased chemical reactivity of the solid. Several historic papers describe some additional details of amorphous materials. Pikal and coworkers at Eli Lilly showed that amorphous materials can also have reduced chemical stability (Pikal et al. 1977) and Fukuoka showed amorphous materials had a tendency to crystallize (Fukuoka et al. 1991). Nevertheless, in some cases, amorphous forms were historically used as products. An excellent example is novobiocin (Mullins and Macek 1960) which exists in a crystalline and an amorphous form. The crystalline form is poorly absorbed and does not provide therapeutic blood levels; in contrast, the amorphous form is readily absorbed and is therapeutically active. Further studies show that the solubility rate of the amorphous form is 70 times greater than the crystalline form in 0.1 N HCl at 25 °C when particles <10 mm are used. Table 1.7 (Haleblian 1975) presents data for the plasma levels of novobiocin’s amorphous and crystalline forms and for sodium novobiocin, which also gives detectable plasma levels, but is chemically unstable in solution. Amorphous materials are of tremendous interest in current development regimes. More information will be presented on amorphous formulations below.
It is possible to summarize the risks involved in selecting amorphous materials as the final form:
-
1.
Lower purity
-
2.
Less physically and chemically stable
Crystalline hydrate > anhydrous crystal > amorphous
-
3.
More hygroscopic
From this list it is clear that crystalline materials are generally more desirable and impart lower risk unless they are so insoluble that they cannot be used as medicines.
2 Risk in Selecting Solvates and Cocrystals for Incorporation into Drug Product
In some cases selecting a solvate as a final form involves risk. Solvates contain solvents regularly incorporated into the crystal lattice. When the solvent is water the solid form is called a hydrate. Solvates and hydrates can, in some cases, lose solvent at temperatures near room temperature. In such cases there is a substantial risk of solid form changes during storage.
Solvates and hydrates do not have the same composition as unsolvated materials. Solvates and hydrates are sometimes referred to as pseudomorphs or solvatomorphs. Interestingly it is possible for solvates and hydrates to be polymorphic. In such a case one has polymorphic solvates. Kuhnert Brandstatter in her 1971 book showed photomicrographs of 16 solvated forms of estradiol.
Figure 8.3 shows the crystal structure of caffeine monohydrate. The crystal of caffeine is built up by stacking the layers shown in Fig. 8.3 on top of each other. Thus, the hydrate molecules are in tunnels in this solid form.

Projection of the crystal structure of caffeine hydrate on the ab plane
It is important to note that the FDA has defined polymorphs as “different crystalline forms of the same drug substance. This may include solvation or hydration products (also known as pseudopolymorphs) and amorphous forms. Per the current regulatory scheme, different polymorphic forms are considered the same active ingredients.” Thus, for purposes of registration, scientists are directed to define polymorphs more broadly to include amorphous forms, solvates, and hydrates.
Cocrystals, that is, two component crystals, are another solid material of interest. Like solvates, the new crystalline structure imparts different properties including solubility, stability, and mechanical properties to the material. Of special interest are cocrystals with altered solubility of stability. Figure 8.4 shows the crystal structure of a cocrystal of 2-methoxy-4-nitrophenol-4-(dimethylamino)pyridine (2:1) (Huang et al. 1997). The FDA has recently released a draft guidance defining cocrystals as “Solids that are crystalline materials composed of two or more molecules in the same crystal lattice.” Currently, there are no or few cocrystalline materials on the market. Thus, the development of a cocrystalline form may impart some risk.

Crystal structure of a cocrystal (2-methoxy-4-nitrophenol-4-(dimethylamino)pyridine (2:1).). The unit cell parameters are a = 6.880, b = 38.40, c = 8.454 and the space group is Pna21
3 Risk in Selecting Salts for Incorporation into Drug Product
Pharmaceutical salts are substances formed by a reaction of an acid and a base. When a carboxylic acid reacts with an amine a salt is typically formed. However, the degree of proton transfer can vary
depending on the acidity and basicity of the reacting groups.
Figure 8.5 shows the crystal structure of calcium tolfenamate trihydrate. It is clear that the unit cell is composed of regions containing mostly hydrocarbon functional groups and regions containing polar functionalities. This type of crystal packing is typical for salts.

Crystal packing of calcium tolfenamate trihydrate showing hydrogen bonding network. The directions of the unit cell axis are (a) vertical, (c) across, and (b) out of the plane of the paper (F. Atassi Ph.D., Purdue University, 2007)
The selection of salts as the final crystal form does not typically impart additional risk.
4 Using Decision Trees as a Guide for Reducing Risk
In 1995 Byrn, Pfeiffer, Ganey, Poochikian, and Hoiberg from Purdue University and the FDA published a paper using decision trees to describe a strategy to reduce risk by identifying the best solid form early in development (Byrn et al. 1995). In this way it is possible to ensure uniformity of solid form in clinical trials and resolve solid state issues before critical stages of development. The decision trees also suggested appropriate analytical methods for control. This is important since appropriate analytical methods reduce risk by providing reliable information. Four decision trees were presented: polymorphs, hydrates/solvates, desolvated solvates, and amorphous forms. This 1995 paper described a typical postdiscovery screen as follows:
Solvents should include those used in the final crystallization steps and those used during formulation and processing and may also include water, methanol, ethanol, propanol, isopropanol, acetone, acetonitrile, ethyl acetate, hexane and mixtures if appropriate. New crystal forms can often be obtained by cooling hot saturated solutions or partly evaporating clear saturated solutions. The solids produced are analyzed using X-ray diffraction and at least one of the other methods. In these analyses, care must be taken to show that the method of sample preparation (i.e. drying, grinding) has not affected the solid form.
In the late 1990s the International Committee on Harmonization used a similar decision tree approach to describe how final specifications for the solid form in drug substances (API) and drug product should be determined. In this case, risk is reduced by developing appropriate specifications. Several decision trees were presented in the ICH Q6A document including decision trees on particle size and polymorphs. The ICH utilized the broadened definition of polymorphs that includes hydrates, solvates, and amorphous forms. The ICH decision trees on polymorphs are divided into three questions as shown in Figs. 8.6, 8.7, and 8.8.

ICH Q6A question 1 on polymorphs: can different polymorphs be formed?

ICH Q6A question 2 on polymorphs: do the forms have different properties (solubility, stability, melting point)

ICH Q6A question 3 on polymorphs: does products performance testing provide adequate control if polymorph ratio changes (e.g. dissolution)?
These three decision trees outline a strategy that is widely used today during postdiscovery drug development as a means of reducing risk. Most firms conduct a polymorph screen postdiscovery to address question number 1. If new forms have been identified, their properties (solubility, stability, melting point) are determined and an effort is made to understand whether these differences in properties will represent a risk of changing drug product safety, performance, or efficacy. If the different solid forms can affect safety, efficacy, or performance then question 3 in the decision tree (Fig. 8.1) is addressed by determining whether drug product testing can detect changes in ratios of these forms. Additionally, the ratios of forms are monitored during stability studies to make sure changes that affect performance, safety, or efficacy do not occur. Using this strategy it is possible to reduce risk by finding a developable solid form rapidly.
5 Additional Steps to Reduce Risk in Designing a Formulation
Simultaneously with screening for the solid form, a number of questions need to be addressed: (a) What is the “intrinsic stability” of the compound? (b) What is the likely dose? (c) How soluble is the compound/formulation? (d) How well is the compound absorbed? (e) What is its BCS class? (f) What are its solid state properties and stability? (g) How well will the powder flow? (h) Is moisture an issue? and (i) What is the likely design, composition, and manufacturing procedure of the formulation/product?
As has already been discussed the solubility of the compound is a critical quality important for specifications and development. The solubility of a solid substance is the concentration at which the solution phase is in equilibrium with a given solid phase at a stated temperature and pressure. Under these conditions, the solid is neither dissolving nor continuing to crystallize. Note that the definition implies the presence of a specific solid phase. Once determined under the stated conditions, however, we can talk about the “solubility” of a given phase (e.g., a specific polymorph or pseudopolymorph) as a quantity, even in the absence of that solid phase. The Gibbs phase rule specifies that at constant temperature and pressure a two-phase system, such as solid drug and solvent, should achieve a well-defined, invariant concentration given sufficient time (i.e., at equilibrium). Thus, the term, equilibrium solubility, which is also referred to as the thermodynamic solubility. For the two-phase system to be at equilibrium, the chemical potential of both components must be equal to each other. If this is not the case, then depending upon the relative values, the system will experience a thermodynamic driving force toward dissolution or precipitation. Note also that while the rule confirms the ability of a compound to have a particular solubility under defined conditions, it says nothing about what actual value of solubility is eventually attained.
Use of the term “equilibrium” in connection with crystallizing systems requires clarification. When a substance exists in more than one crystal form, that is, when other polymorphs are possible, only the least soluble of these at a given temperature is considered the most physically stable form at that temperature, all others are considered to be metastable forms. In given cases, a solution of a substance may be in apparent equilibrium with one of these metastable phases for a long time, in which case, the system is in metastable equilibrium and is expressing the thermodynamic solubility of that solid form.
The most easily conceptualized driver of solubility is the manner which the compound interacts with the solvent. The more extensively a compound interacts with the solvent molecules at the expense of the solvent interacting with itself, the greater the enthalpic contribution toward having more drug solution at equilibrium. The entropic considerations are more complex. The increase in disorder brought about by spreading a drug molecule from an immobile solid into a fluid is opposed by the loss of disorder experienced by the solvent molecules as they are displaced by the presence of a drug compound. It is the relative contribution of these two mechanisms that determines if dissolution is entropically favored or not. Equally important to the solvent–drug interactions in solution are the drug–drug interactions that must be disrupted in order for a compound to be removed from the solid form in the first place. Because the strength of these interactions in the solid state depends upon the orientation of the compositional atoms with respect to each other, the chemical potential represented by a given solid is determined by the particular polymorph in which it exists. Since, as noted earlier, the relative chemical potential of the solid and solution defines the solubility, the choice of solid form will determine the measured value of this critical parameter.
Figure 8.9 is useful in describing supersaturation phenomena and definitions and their relationship to solubility. Supersaturation is the amount of compound in solution in excess of that present under equilibrium conditions. However, in the same sense that equilibrium solubility has little meaning in the absence of a defined solid form, some supersaturation scenarios require knowing the solid phase present. For example, when the chemical potential represented by Solution 2 is equal to that of Polymorph 2, the amount of dissolved drug can be considered to be the equilibrium solubility. It can also be considered the most stable situation involving the least risk since Polymorph 2 is the lowest energy solid in which the compound can exist at a specified temperature and pressure. Similarly, the amount of drug in Solution 1 can be considered to be the equilibrium solubility of Polymorph 1. It is important to note that this represents a higher order of risk since while Solution 1 is saturated with respect to Polymorph 1, it is supersaturated with respect to Polymorph 2. Were a third solid form of even higher energy to exist, call it Polymorph 3, then the solution at the equilibrium solubility of this form would be supersaturated with respect to both Polymorph 2 and Polymorph 1. In all cases, the possibility of a high energy polymorph converting to one of lower energy represents the source of risk.

Solubility and energy diagram of two forms
There is another scenario deserving of consideration and that is when there is more compound in solution than consistent with the equilibrium solubilities of Polymorphs 1 and 2, yet there is no solid simultaneously present. Setting aside the possibility that the hypothesized Polymorph 3 is present, but only in a state difficult to observe, (i.e., subvisible particles), this level of drug can be considered the kinetic solubility of the compound. Such a solution, which can be prepared by a shift in pH, dilution from water-miscible solvents, or dissolution of a salt, is likely to be highly unstable toward precipitation and represent the highest risk of all. It is important to note that unlike equilibrium solubility, the measured kinetic solubility of a compound may be highly dependent on the manner in which the experiment was conducted (Alsenz and Kansey 2007).
5.1 Experimental Considerations for Measuring Solubility
As noted earlier, the solubility is affected by the solids and solvents employed, and while its theoretical value is completely defined, it is ultimately determined through experiment. Thus, the manner in which the solubility of a compound is evaluated can also have an effect if not on its absolute value then on the practitioner’s ability to understand it. There are several important aspects to consider.
Time: The equilibrium solubility with respect to any solid form can only be determined when sufficient time has been allowed to elapse to ensure saturation. The surrogate for knowing if this has occurred is to make a measurement at multiple time points after combining drug and solvent and then assume that a lack of change in value indicates the attainment of equilibrium.
Separation: Assessing the quantity of drug in solution necessitates separating the solid material, be it undissolved or precipitated, from the supernatant before analysis. Thus, the degree to which the separation is “complete” will affect the experimental value. In many cases filtration, frequently using membranes possessing 0.22 μm diameter pores, is employed. However, the arbitrariness of result so obtained can be addressed by considering the fact that the prevalence of such filters is due primarily to their ability to remove microbes as a means of sterilization. If microbes happened to be of a larger or smaller dimension, then estimates of solubility using this approach would average correspondingly higher or lower since greater or smaller amounts of small drug particles could be mistaken for molecularly dispersed compound. A similar argument can be made with respect to centrifugation since the size cutoff produced will depend on the choice of the force and duration applied.
Sorption: Any surface that contacts the experimental materials, particularly after the aforementioned separation step, is a possible source of compound loss that will inevitably lead to an underestimate of solubility. This is of particular concern for low solubility compounds where the sorption of even nanograms of compound can represent loss of most of the dissolved material. The practical solution to this problem is paying extreme attention to detail—bordering on paranoia—and successfully duplicating results across labs.
Starting Material: Compound can be introduced into the solvent in the form of a solid or as a solution. In the former case, the chemical potential of the solution rises to match that of the solid whereas in the latter case the chemical potential of the solution drops over time. Starting with solution is a perfectly acceptable way of introducing compound to the solvent if the solid form present during separation is unambiguously identified. Indeed, methods that start with dissolved compound, such as potentiometric titrations or light scattering, are those the least subject to artifact (Box et al 2006; Lindfors et al 2006; Ilevbare and Taylor 2013). In all cases sufficient time must be allowed for measured values to reach a steady state.
The most significant practical aspect of the above is that there is an extreme degree of risk associated with any experimental value reported for solubility in the absence of a thorough understanding of the solid phase with which the solution is in equilibrium. All other things being equal, a higher energy solid state will lead to a higher measured value for solubility, whereas lower solubilities are obtained from lower energy solids. However, by its very nature, a higher energy solid is thermodynamically unstable with respect to those at lower energy. The situation is described in Fig. 8.9. Two polymorphs, 1 and 2, are specified to differ from each other by a given amount of energy, ΔE, with the latter being more stable than the former. Under constant experimental conditions, the water solubility of the nonionized drug, ΔS O, will differ by a value corresponding to that same amount of energy, with the higher solubility being associated with the higher energy solid. Should Polymorph 1 be used to generate a saturated solution and the equilibrium solid present convert to Polymorph 2 during the experiment, then the amount of drug in solution will drop. It is important to note, however, that the time scale over which this decrease occurs is not easily predicted (Ozaki et al 2012), but the effect on risk is clear. A formulation prepared from Polymorph 2 has the potential to generate significantly less bioavailability than the same formulation prepared from Polymorph 1. The risk is even greater when transitioning from discovery to development since the amorphous materials (e.g., films, pastes, etc,) frequently used in discovery will likely have ΔE values in substantial excess of the solids employed later in the preclinical space. Any biopharmaceutical assessment of a compound must therefore also try to quantify the extent of these risks. Note also, however, that the utility of amorphous dispersions to enhance bioavailability is based on leveraging this same effect to good purpose, with the difference being that particular formulation emphasis is placed on kinetically stabilizing the enabling solid with respect to conversion to low energy states.
Risk in pharmaceutical development increases as the solubility decreases. In certain cases it is impossible to develop a product if the solubility is too low. Risk in development also increases with an increase in the number of solid forms. It can require substantial effort to develop a formulation if multiple forms exist. In some cases the cost of developing a solid with multiple equilibrating forms can be prohibitive.
The solubility and permeability are combined to determine the BCS class (Table 8.1). BCS class I drugs dissolve easily and are easily transported into the blood stream because they are highly permeable with respect to the membranes in the GI tract. BCS class III and IV drugs have poor permeability and are generally difficult to develop. BCS class II drugs are of the greatest importance for formulation/medicine design because the structure of the solid, the formulation, and many other factors are likely to have a significant effect on bioavailability and ultimately safety, performance, and efficacy. Several important drugs that are widely prescribed are BCS Class 2 including: atorvastatin calcium, celecoxib, efavirenz, irbesartan, lopinavir, medroxyprogesterone acetate, raloxifene hydrochloride, simvastatin, and warfarin sodium. Of the marketed drugs nearly 70 % are in BCS Class I or II with 31 % being in BCS Class II. It has been estimated that as high as 80 % of the drugs under development are BCS Class II. Risk increases as you move from BCS Class I to BCS Class II. Drugs with poor permeability (BCS Classes III and IV) are even harder to develop and have high risk of failure.
Particle size, like polymorphism, is one of the most critical aspects of solid state chemistry and the design of formulations. Failure to control particle size represents one of the greatest risks in development. The incorrect particle size can cause a change in the rate of dissolution and affect safety, efficacy, and performance. The ICH Q6A document on specifications makes it clear that particle size of APIs (drug substances) must be controlled especially if they are poorly soluble.
Likewise, failure to control polymorphism represents one of the greatest risks to development. Screening, as outlined earlier, is an approach often used to reduce this risk by finding the best solid form, and a manufacturing process. Screening can reduce the risk of process failure and lead to a reliable process for manufacturing. During the later stages of development complete screening studies are recommended. In these studies, a wide range of solvents are used including solvents used or of possible use in the manufacturing process, solvents spanning a wide range of polarities, and solvents having various functionalities. Typically, a list of 60 or more solvents is used to select the best solvents for these experiments. Solvents containing water (such as ethyl acetate water) are also used in this screen. In addition, melt-based crystallization on a microscope is recommended. In this regard, the scientists at Innsbruck, Austria have used melt recrystallization as a method for polymorph screening for more than 70 years. In a more recent example, Yu used non-solvent-based melt crystallization methods to discover new forms of ROY (2005). Additionally, grinding is used in an attempt to prepare new forms. Likewise crash cooling out of solvents and crystallization of amorphous materials are also used in an attempt to obtain new forms.
If a supersaturated solution is created it is important to screen for a crystallization inhibitor (Vandecruys et al. 2007). As indicated, screening is typically done for polymorphs including amorphous forms, salts, cocrystals, and nanoparticulate formulations. Unfortunately, all important forms are not found upon screening, and instances of late appearing important forms still occur. Thus, screening can reduce but not eliminate risk.
In addition to screening and selection of the best solid form and optimization/control of API and drug product, additional experiments are also carried out again to reduce risk. These experiments include determination of the partition coefficient (logP). This reflects the hydrophobicity of the drug and can be useful in determining the BCS class. The solubility of all available forms is determined as well as the degree of precipitation of any solid forms. Since solubility can depend on solid form, the solubility is typically determined in aqueous buffers, organic solvents, surfactants, and perhaps cyclodextrins and lipids. The solution and solid state stability of the API is determined under stress conditions including extreme pH, temperature light, and humidity. This provides information on the intrinsic chemical stability of the system and this knowledge is critical in formulation development. The pKa is also determined or calculated. This provides important information on the acidity/basicity of the material.
Once the solid form has been selected based on the above screening experiments, the stability of that form is determined under stress and accelerated conditions. This provides important information on how to handle that particular form and the risk of transformation. The dissolution properties of this form are also monitored. This provides important information on what might happen in the GI tract.
6 Reduction of the Risk of Failure Due to Poor Solubility
For poorly soluble compounds, salt formation and the formation of amorphous forms can reduce the risk of failure. Salt formation was discussed earlier and in the previous chapter. Rapid dissolution rates can be achieved by some salts. In fact, for some pharmaceutical salts, such as sodium phenytoin, a solubility enhancement of about 1,000,000 is achieved. This clearly shows the desirability of finding salt forms and explains why a very large number of drugs are developed as salts. Berge et al. (1977) summarized the approaches to forming salts.
Choosing the appropriate salt … can be a very difficult task, since each salt imparts unique properties to the parent compound.
Salt-forming agents are often chosen empirically. Of the many salts synthesized, the preferred form is selected by pharmaceutical chemists primarily on a practical basis: costs of raw materials, ease of crystallization, and percent yield. Other basic considerations include stability, hydroscopicity and flowability of the resulting bulk drug. Unfortunately, there is no reliable way of predicting the influence of a particular salt series on the behaviour of the parent compound. Furthermore, even after many salts of the same basic agent have been prepared, no efficient screening techniques exist to facilitate selection of the salt most likely to exhibit the desired pharmacokinetic, solubility, and formulation profiles. (Berge at 1.)
The number of salt forms available to a chemist is large … Various salts of the same compound often behave quite differently because of physical, chemical, and thermodynamic properties they impart to the parent compound. For example, a salt’s hydrophobicity and high crystal lattice energy can affect dissolution rate and, hence, bioavailability. (Berge at 2.)
Salt formation is a means of altering the physical, chemical, and biological characteristics of a drug without modifying its chemical structure. Clearly, the salt form can have a dramatic influence on the overall properties of the parent compound. At present, selecting a salt form that exhibits desired combination of properties is a difficult semi-empirical choice. (Berge at 16.)
Berge and the previous chapter lists 80 acids for forming salts with drug compounds that are basic and 21 bases for forming salts with drug compounds that are acidic. In part because hydrochloric acid naturally occurs in the stomach, that acid is by far the most frequently used to make drug salts, accounting for almost half of the salts approved by the FDA. This is despite the fact that due to the “common ion effect,” hydrochloride salts tend to be less soluble in the stomach. Nevertheless, it is a nearly universal practice among chemists tasked with making a salt of a basic drug compound to try to make the hydrochloride salt first. When the hydrochloride salt is unacceptable for one reason or another, there is no universal second choice; the list is very long.
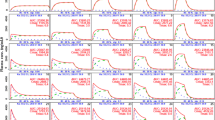
A viable alternative to salt formation, especially in cases where a salt cannot be formed, is to develop an amorphous form/formulation. There are several products containing amorphous forms on the market including Kaletra and sporanox. A recent review reports that amorphous formulations can result in as much as an 82× increase in bioavailability (Newman et al. 2012). Law and coworkers (2003) reported greatly enhanced plasma concentrations of amorphous ritonavir over crystalline material. Ritonavir is one of the components in Kaletra. Figure 8.10 shows the results of studies of a 2:1 HPMC-P:itraconazole dispersion in dogs. Clearly, the amorphous dispersion results in a large increase in bioavailability.

Comparison of the bioavailability of a 2:1 HPMC-P:Itraconazole dispersion in dogs
In order to find the best amorphous form and formulation an amorphous screen is conducted. First a brief study of the solubility of the solid form and polymers is carried out to find a solvent that dissolves both the polymer and drug. Mixtures of methylene chloride and ethanol are particularly attractive but other solvents of interest include acetone, acetonitrile, methanol, isopropanol, THF, ethyl acetate, and pentane. An amorphous dispersion screen is carried out using a 1:1 ratio and 1:2 ratio of the drug and polymer. Pure drug is used as a control. The drug and polymer are mixed in a minimum amount of solvent and the solvent is evaporated as fast as possible using a rotary evaporator with a heated bath on the solvent flask and a good vacuum. Solids are scraped out, dried further in a vacuum oven, ground to a powder, and analyzed by XRPD. The following polymers are typically used: PVP (2 molecular weights), HPMC, HPMC-AS, HPMC-P, crospovidone, polymethacrylates (two), PEG, and pluronic. The dispersions are analyzed by XRPD. Amorphous dispersions are stored at 40 °C/75 % RH for 3 days and reanalyzed by XRPD to verify stability.
Our lab and collaborators have also developed an amorphous screen that can be carried out in the levitated drop apparatus available at Argonne National Laboratory (see Benmore chapter). In this study, the drug-polymer solution is levitated in drops. The evaporating levitated drop/particle is analyzed every 30 s with high energy X-rays at the synchrotron X-ray source. This analysis provides instant feedback on the crystallinity of the evaporated drop/particles. It is also possible to carry out pair distribution function analysis of the diffraction pattern produced during the evaporation. More details are provided in the chapter by Chris Benmore appearing later in this book section.
Shah and coworkers (Hu et al. 2013) have suggested another approach to forming amorphous compounds involving precipitation of amorphous solids from organic solvents. This method is particularly useful for compounds with high melting points, making melt-extrusion difficult, and low solubility in volatile solvents, making spray drying or rotary evaporation difficult. In this method drug and polymer are codissolved in water miscible solvents such as DMA, DMSO, or DMF and added to cold acidic water such as 0.01 N HCl. A variation of this method uses acidic polymers which can form salts or associations with weak bases or hydrogen bonding accepting sites. They suggest using, for example, 3 antisolvent/water ratios, 3 concentrations of drug, and three polymers (see above) for an initial 27 experiments. They suggest working on the 100 mg scale for large scale and they also have suggested a microplate screening method using 96 well plates at the 0.1 mg scale and an X-ray powder diffractometer capable of transmission analysis.
Another alternative to salt formation or amorphous formation is cocrystal formation. Figure 8.11 shows that a cocrystal enhanced the bioavailability of an amide containing API by about 4×.

Enhanced bioavailability of a cocrystal over the parent drug (modified from McNamera et al. 2006)
Amorphous and cocrystalline formulations are classified as supersaturated drug delivery systems as discussed earlier. Crystallization inhibitors are sometimes used to prevent premature crystallization for these formulations. The screening method Brewster and coworkers (Vandecruys et al. 2007) suggested is as follows: The drug is dissolved in DMF typically at 100 mg/mL. In a second vessel was placed 0.01 N HCl and 2.5 % of the crystallization inhibitor candidate (polymer or compound). The DMF solution is added dropwise to a stirred solution of the crystallization inhibitor until a precipitate is just noticed visually. The solution is then filtered and the concentration determined by HPLC. The pH is also measured since it could have an effect on the solubility of some drugs. A control experiment is done without the excipient present in the water. The ability to inhibit precipitation is then determined by the ratio of the concentration of the drug attained in the precipitation experiment to the control. In some cases solubility ratios of >10,000 were attained. Additionally, the stability of the supersaturated solution was assessed. Good crystallization inhibitors are incorporated in the formulation. It is interesting to note that the first steps in this method are quite similar to those used by Shah and coworkers (Hu et al. 2013).
In addition to solubility/dissolution rate, the solid form can influence a number of other properties important for formulation including: milling, blending, tableting, dry filling, suspension formulation, and lyophilization. Transformations to other forms can also occur during these processes.
7 Reducing Risk Due to Instability
Initially, the intrinsic stability is analyzed using functional group analysis and the outline of solid state chemistry provided in Chap. 1 in this section. The solid state stability should be assessed in the phase of choice using forced degradation experiments (usually at 80 °C and 75 °C/40 % RH). Analysis by HPLC provides immediate information on the stability of the solid phase. Photolytic stability should also be investigated. For unstable phases, new solid state structures need to be investigated.
For stable solids, excipient compatibility needs to be done. A few excipients from each class are mixed with the drug in a 1:1 ratio and 5 % moisture is added. The mixture is then stressed at 80 °C for 7 days. HPLC analysis reveals instability and in subsequent formulation the incompatible excipients are excluded.
In addition, it is useful to determine solution stability of the drug in buffers of relevance to the body (pH 1, 6.8 and 7.4). Typically the solution is heated at 50 °C for 3–6 days and analyzed by HPLC. Solution degradation suggests that wet granulation should not be used to prepare the final formulation.
8 Formulation Design to Reduce Risk
The best approach to formulation design is to follow the old adage “Just do something.”
The first choice for reduced risk early formulations is a powder in a capsule formulation. This can be prepared precisely by a modern dosator machine. This formulation requires verifying that the capsule does not cause degradation or physical transformation of the solid form. It has been estimated that over 90 % of the solid materials can be accurately filled into capsules using a dosator. Additionally, a simple dissolution study can verify that there is good release of the drug from this simple formulation.
If an amorphous dispersion is selected for development, it is quite routine to fill this dispersion directly into capsules. We have found that, in some cases, the polymer dispersion and the capsule form a plug during dissolution. In such cases, it is necessary to utilize a disintegrant to break up the dispersion; thus forming a powder + disintegrant in capsule formulation.
In the event that a powder in a capsule does not work, or a larger scale formulation is needed, a wet granulation or direct compression formulation and manufacturing method provides the approach with the lowest risk. Wet granulations are particularly preferred if a thorough analysis of the solid state chemistry indicates there is little possibility of transformation during the formulation process. For these formulations a diluent, binder, disintegrant, and lubricant is typically added. In some cases glidants and flow promoters are also added. For wet granulations, a super disintegrant is sometimes used but it should be remembered that the sodium superdisintegrants can react with ionic bases. Table 8.2 lists common tablet excipients.
Next, the lowest risk approach is to make a trial formulation. A typical small-scale method of manufacture by wet granulation is shown below:
For amorphous dispersions of drug in polymer, wet granulation is not recommended and probably not needed. Instead the polymer–drug dispersion is blended with a superdisintegrant and a lubricant and perhaps a filler such as MCC or lactose and compressed into tablets or filled into capsules. If the drug and/or polymer is ionic it is safest to use a nonionic disintegrant. For early studies the drug–polymer dispersion can be filled directly into capsules using a dosator.
The tablets produced are analyzed for dissolution compared to an equal dose of drug (API) powder. Typically both simulated gastric fluid and simulated intestinal fluid are used. It is easiest to use an in situ probe to determine relative dissolution rate. But HPLC is also recommended especially in cases where aggregation of the drug will cause artifacts in UV analysis.
The tablets are also analyzed by X-ray diffraction and HPLC to make sure the manufacturing process does not cause physical or chemical changes. The API is used as a control. In addition, binary and tertiary mixture of API and excipients are made and analyzed for changes using X-ray diffraction and HPLC. Finally, it is recommended that the tablets be subjected to some degree of forced degradation conditions to rule out physical changes or chemical degradation under stress conditions.
At this point, the risk for development of this formulation is assessed. The tablets produced are stressed at 40 °C/75 % RH for a week and reanalyzed by HPLC and X-ray diffraction. If no changes are detected a full scale early stage forced degradation study is carried out using exposure for a month at stress conditions. The stressed tablets are again tested by X-ray diffraction, HPLC, and dissolution. After these studies another risk assessment is done and the process is repeated until an acceptable formulation and manufacturing method is achieved.
9 Conclusion
In conclusion, this chapter has reviewed strategies to deal with risk in formulation design. Initially, risk of choosing the incorrect form is addressed, subsequently approaches to overcome the barrier to poor solubility including salt formation and the use of amorphous dispersions are outlined. The risk of these various approaches is also briefly addressed. Finally the incorporation of the appropriate solid form or dispersion into a formulation is discussed.
References
Alsenz J, Kansey A (2007) High throughput solubility measurement in drug discovery and development. Adv Drug Deliv Rev 59:546–567
Berge SM et al (1977) Pharmaceutical Salts. J Pharm Sci 66:1–19
Box KJ, Volgyi G et al (2006) Equilibrium versus kinetic measurements of aqueous solubility, and the ability of compounds to supersaturate in solution—a validation study. J Pharm Sci 95(6):1298–1307
Byrn S, Pfeiffer R, Ganey M, Hoiberg C, Poochikian G (1995) Pharmaceutical solids: a strategic approach to regulatory considerations. Pharm Res 12:945–954
Fukuoka E, Makita M, Nakamura Y (1991) Glassy state of pharmaceuticals. V. Relaxation during cooling and heating of glass by differential scanning calorimetry. Chem Pharm Bull 39:2087–2090
Haleblian JK (1975) Characterization of habits and crystalline modifications of solids and their pharmaceutical applications. J Pharm Sci 64:1269–1288
Hu Q, Choi DS, Chokshi H, Shah N et al (2013) Highly efficient miniaturized coprecipitation screening (MiCoS) for amorphous solid dispersion formulation development. Int J Pharm 450:53–62
Huang K-S, Britton D, Etter MC, Byrn SR (1997) A novel class of phenol-pyridine co-crystals for second harmonic generation. J Mater Chem 7(5):713–720
Ilevbare GA, Taylor LS (2013) Liquid−liquid phase separation in highly supersaturated aqueous solutions of poorly water-soluble drugs: implications for solubility enhancing formulations. Cryst Growth Des 13:1497–1509
Kuhnert-Brandstätter M (1971) Thermomicroscopy in the analysis of pharmaceuticals. Pergamon, New York, NY
Law D, Schmitt ED, Kennan I et al (2004) Ritonavir–Peg 8000 amorphous solid dispersions. J Pharm Sci 93(3):563–570
Lindfors L, Forssen S, Skantze P et al (2006) Amorphous drug nanosuspensions. 2. Experimental determination of bulk monomer concentrations. Langmuir 22:911–916
McNamara DP, Childs SL, Giordano J et al (2006) Use of a glutaric acid cocrystal to improve oral bioavailability of a low solubility API. Pharm Res 23:1888–1897
Mullins JD, Macek TJ (1960) Some pharmaceutical properties of novobiocin. J Am Pharm Assoc Sci Ed 49:245–248
Newman A, Knipp G, Zografi G (2012) Assessing performance of amorphous solid dispersions. J Pharm Sci 101:1355–1377
Ozaki S, Minamisono T et al (2012) Supersaturation–nucleation behavior of poorly soluble drugs and its impact on the oral absorption of drugs in thermodynamically high-energy forms. J Pharm Sci 101(1):214–222
Pikal MJ, Lukes AL, Lang JE (1977) Thermal decomposition of amorphous β-lactam antibacterials. J Pharm Sci 66:1312–1316
Taylor LA, Van Eerdenbrugh B, Bard JA (2010) Crystallization tendency of active pharmaceutical ingredients following rapid solvent evaporation—classification and comparison with crystallization tendency from undercooled melts. J Pharm Sci 99:3826–3838
Vandecruys R, Peeters J, Verreck G, Brewster MC (2007) Use of a screening method to determine excipients which optimize the extent and stability of supersaturated drug solutions and application of this system to solid formulation design. Int J Pharm 342:168–175
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 American Association of Pharmaceutical Scientists
About this chapter
Cite this chapter
Byrn, S.R., Haskell, R.J. (2015). Efficient Laboratory Methods to Assess Risk and Design Formulations. In: Templeton, A., Byrn, S., Haskell, R., Prisinzano, T. (eds) Discovering and Developing Molecules with Optimal Drug-Like Properties. AAPS Advances in the Pharmaceutical Sciences Series, vol 15. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1399-2_8
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1399-2_8
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1398-5
Online ISBN: 978-1-4939-1399-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)