
Abstract
Individuals with clinical or subclinical symptoms of depression are not only characterized by alterations with respect to cognitive or emotional processes but also regarding a broad range of processes that are related to the self-regulation of behavior. The first part of this chapter outlines classic and recent models and findings that converge on the conclusion that clinical and subclinical depression is related to altered self-regulation functioning. Such dysfunctions include perfectionistic goal-setting, impairments in the spontaneous initiation of actions and task strategies, reduced approach behavior, reduced responsiveness to rewarding or punishing consequences, maladaptive responsiveness to negative feedback, altered goal or task disengagement, ruminative self-focus, as well as affect regulation difficulties. The second part of this chapter focuses on one specific psychophysiological aspect of impaired self-regulation in depression: maladaptive adjustment of effort mobilization in terms of increased or blunted cardiovascular reactivity during performance of cognitive tasks. Specifically, we report findings from a series of recent studies demonstrating that subclinically depressed individuals show increased cardiovascular reactivity for easy tasks and for tasks without performance standards. In contrast, they show reduced cardiovascular reactivity for challenging tasks and in anticipation of rewarding or punishing consequences. These results suggest that the self-regulation difficulties observed in depression are not necessarily the expression of a general motivational deficit. They rather point to a maladaptive adjustment of effort mobilization. To end with, we exemplarily outline three treatment approaches that act on depressed individuals’ impaired self-regulation functioning as presented throughout the chapter.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Major depression is an affective disorder that is characterized in particular by persistent negative affect and anhedonia, i.e., a loss of interest or pleasure (Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association 2000). It is considered one of the most burdensome mental disabilities in modern societies, with increasing prevalence rates and severe consequences not only for the individual but also for the societies’ economy (e.g., Kessler and Wang 2009). Not surprisingly, a wealth of research efforts from various perspectives have been undertaken to understand the features and mechanisms of this serious disorder. Particularly well documented are cognitive impairments (e.g., reduced cognitive control) and negative cognitive biases (e.g., Gotlib and Joormann 2010). Moreover, research has been interested in depressed individuals’ emotion processing and emotional reactivity (e.g., Rottenberg 2007). However, motivational deficits are also a common feature of the clinical appearance of depression. In this respect, it may be difficult to disentangle depressed individuals’ other types of impairments (e.g., cognitive deficits) from underlying motivational deficits (Scheurich et al. 2008).
Given the important role of motivational deficits in depression and their potential impact on other features of depression, the aim of the present chapter is threefold: First, we present a review of the depression literature from a motivational point of view. Second, from a psychophysiological perspective, we turn to one important aspect of motivation, namely, the intensity of behavior and present hypotheses and empirical evidence for impaired adjustment of effort mobilization of subclinically depressed individuals. Finally, we outline some examples of treatment approaches that act on depressed individuals’ impaired motivational functioning as presented throughout this chapter.
2 Self-Regulation Functioning in Depression
The literature review in the first part of this chapter is guided by the objective of taking the whole motivation process into account. Specifically, we propose an analysis of depressed individuals’ self-regulation functioning starting with the setting of standards and goals, the initiation of behavior, the direction of behavior, and the related aspect of responsiveness to hedonic consequences. We then turn to the role of feedback, the persistence of behavior, and related aspects of disengagement, ruminative self-focus, and affect regulation. We aim at presenting a comprehensive review of the current literature of self-regulation functioning in depression by exemplarily referring to empirical evidence for each of the aspects reviewed. However, this chapter cannot claim to be exhaustive given space concerns and the selective focus on several important aspects of motivation. The choice of these aspects is based on the four dimensions of motivated behavior (i.e., the initiation, direction, intensity, and persistence of behavior; see Geen 1995) and on a self-regulation perspective. A self-regulation perspective is particularly useful because it comprises the whole process of goal-directed behavior, including goal setting, action initiation and maintenance, attention control, and affect regulation (see Carver and Scheier 1998; Klenk et al. 2011).
We are limiting our motivational analysis to theory and research on major depressive disorder and subclinical depression. In brief, major depression is a recurrent disorder characterized by a depressed mood or a loss of interest or pleasure for at least 2 weeks. Moreover, at least four of the following symptoms must be present in a depressive episode: weight change, insomnia or hypersomnia, psychomotor agitation or retardation, loss of energy, feelings of worthlessness, difficulties concentrating or indecisiveness, and suicidal ideation (American Psychiatric Association 2000). Subclinical depression—which is also referred to as dysphoria—is characterized by symptoms that do not meet the threshold for a diagnosis of a depressive episode. However, dysphoric individuals often present similar, albeit minor, impairments and are at an elevated risk for developing major depression (Fergusson et al. 2005; Judd et al. 2002). Theories of depression mainly refer to major depression. However, empirical evidence often comes from both clinical and subclinical samples. Throughout this chapter, we consider studies from both kinds of samples.
2.1 Standards and Goal Setting
The self-regulation process typically starts with goal setting. Prominent theories of depression argue that depressed individuals tend to set goals or standards that exceed the expected or obtained outcomes (see Ahrens 1987, for a review). However, in the past decades, no clear empirical consensus has been reached concerning this assumption. On the one hand, it is well established that clinical and subclinical depression is related to maladaptive forms of perfectionism (e.g., Wheeler et al. 2011). On the other hand, only some goal-setting studies have confirmed that dysphoric individuals set higher standards but found no differences in the expectancy to reach their goals (e.g., Golin and Terrell 1977). Other studies have revealed lower self-efficacy expectancies in subclinical depression but found no differences in goal setting (e.g., Qian et al. 2002). However, when simultaneously considering standard-setting and self-efficacy expectancies, results converge on the fact that clinically and subclinically depressed individuals show a negative discrepancy between standards and expectancies, i.e., they set higher minimal standards for themselves than they reach or expect to reach (e.g., Ahrens 1987; Tillema et al. 2001).
Related to lower outcome expectancies are findings indicating that depressed individuals report approach goals as less likely to happen and avoidance goals as more likely to happen and that they perceive less control over goal outcomes (e.g., Dickson et al. 2011). However, depressed individuals do not consistently report a higher number of avoidance goals (e.g., Dickson et al. 2011). Taken together, theories of depression and empirical research suggest that the self-regulation process of clinically and subclinically depressed individuals might be impaired by maladaptive goal- and standard-setting and by lower expectancies of (positive) outcomes.
2.2 Initiation of Behavior
Following goal setting, one of the critical moments in the self-regulation process is the initiation of actions. The failure to act on one’s intentions has been identified as a common problem (see Gollwitzer and Sheeran 2006). In the particular case of depression, the cognitive-initiative account by Hertel and colleagues (e.g., Hertel 2000) suggests that memory impairments of depressed individuals are due to a lack of spontaneously developed initiative and to difficulties in the initiation of strategies. This assumption converges with the view of initiation as being an approach-related action associated with left frontal activity, both of which have been found to be reduced in depression (Nitschke et al. 2004). Moreover, it also converges with the view that the initiation of strategies (e.g., in a task that requires switching) is related to impaired frontal lobe executive functioning in depression (Lafont et al. 1998). According to the cognitive–initiative account, attention-focusing instructions and highly structured tasks might help overcoming these cognitive impairments (Austin et al. 2001; Hertel 2000). In sum, theory and empirical findings suggest that action initiation and strategy initiation are impaired in clinical and subclinical depression and a crucial aspect to act on.
2.3 Direction of Behavior
As foreshadowed above, the direction of behavior in terms of approach or avoidance is an important aspect of self-regulation . Several theories postulate that depressed and dysphoric individuals are characterized by deficits in approach-related positive affect. Specifically, behavioral theories suggest that depressed individuals learn from their experiences that their actions are not followed by positive reinforcement. As a consequence, the behavior leading to positive consequences is given up in favor of avoidance, withdrawal, and passivity. Such avoidance tendencies in turn produce, sustain, or worsen depressive symptoms (Beck et al. 1979; Jacobson et al. 2001).
Depue and Iacono (1989) argue that depression is characterized by a deficient activity of the behavioral facilitation system—a basic system that mobilizes behavior and that provides a motivational contribution to the process of active engagement in the environment. In a similar vein, a number of studies based on reinforcement sensitivity theory (Gray 1982) demonstrate that depressed and dysphoric individuals report lower levels of the behavioral activation system (BAS) and higher levels of the behavioral inhibition system (BIS; see Bijttebier et al. 2009, for a review). Finally, it is well documented that clinically and subclinically depressed individuals show reduced electrocortical activity in left prefrontal regions that are associated with approach behavior (see Thibodeau et al. 2006, for a review).
Related to the direction of behavior is an intriguing analysis of empirical evidence for low serotonergic function in depression by Carver et al. (2008, 2009). Based on two-mode models of self-regulation, the authors conclude that depressive inaction is characterized by the interaction of low serotonergic function—which is linked to deficient effortful control—and reduced incentive sensitivity. According to this perspective, reduced approach tendencies in depression cannot be overcome because of deficits in a higher-order reflective control system (see also Chap. 2 in this volume).
Taken together, several important theories as well as empirical evidence suggest that clinical and subclinical depression is characterized in particular by reduced approach behavior and deficits to overcome this tendency. What is more, a hypoactive BAS, resting electrocortical frontal asymmetry, and low serotonergic function can be considered as trait-like vulnerability markers of depression.
2.4 Responsiveness to Reward and Punishment
A related aspect of behavioral approach and avoidance tendencies is the responsiveness to hedonic consequences like reward or punishment. In the past two decades, a number of behavioral and neuroscientific studies have been conducted on clinical and subclinical depression. Several behavioral studies demonstrated that dysphoric and depressed individuals are less sensitive to monetary rewards in terms of a less liberal response bias compared to nondepressed individuals (e.g., Henriques and Davidson 2000). However, they did not consistently find this effect in a monetary punishment condition. More recently, some studies revealed that compared to nondepressed individuals, clinically and subclinically depressed participants show a lower response bias toward the more frequently reinforced stimulus (e.g., Liu et al. 2011; Pizzagalli et al. 2009). Moreover, several behavioral studies showed a reward-based decision making deficit in depressed individuals (e.g., Kunisato et al. 2012).
Numerous studies using brain-imaging techniques have investigated depressed individuals’ sensitivity to reward and some of them also to punishment. These studies generally revealed dysfunctions of cortical and subcortical components involved in the neural reward circuit not only in depressed individuals (see Eshel and Roiser 2010; Nestler and Carlezon 2006, for reviews) but also in recovered patients (McCabe et al. 2009) and in daughters of depressed mothers (Gotlib et al. 2010). Furthermore, depression has been linked to a reduced frontal electroencephalogram asymmetry during anticipation of reward (Shankman et al. 2007) and to a blunted feedback-related negativity to monetary gains and losses (e.g., Foti et al. 2011).
Recently, several authors (e.g., Berridge 2003) suggested to divide reward processing into different components: wanting or the anticipatory phase, which is defined as the motivation to obtain rewards, and liking or the consummatory phase, which is defined as the hedonic response to rewards. During anticipation, most of the behavioral and neuroscientific studies revealed that depressed and dysphoric individuals show reduced motivation to obtain rewards (e.g., Chentsova-Dutton and Hanley 2010; Treadway et al. 2012; but see also Dichter et al. 2012). The consummatory phase has been studied less. Most of these studies showed decreased responsiveness to rewards in depression (e.g., Forbes et al. 2009; but see also Smoski et al. 2011).
In sum, numerous studies have investigated reward processing using behavioral and neuroscientific measures. They consistently show a hyposensitivity to rewards in clinical and subclinical depression. In contrast, fewer studies have investigated punishment sensitivity, and the results are less consistent, showing sometimes hypo- and sometimes hypersensitivity in depression.
2.5 Feedback Reactivity
As a particular case of reward and punishment sensitivity and an important aspect of self-regulation , reactivity to positive and negative feedback has also been subject of numerous studies. Concerning negative feedback in particular, several studies have shown that once depressed individuals have made a mistake, they commit more subsequent mistakes (e.g., Elliott et al. 1997; Steffens et al. 2001). This abnormal effect of negative feedback on subsequent performance in depression has also been demonstrated using brain-imaging techniques (e.g., Elliott et al. 1998). In their review, Eshel and Roiser (2010) suggest two alternative interpretations for this well-documented effect, which receive both some empirical support from research with event-related potentials :
Using the error- or feedback-related negativities as measures of the electrophysiological reactivity to errors or negative feedback, some studies demonstrated larger feedback-related negativities in depressed and remitted depressed individuals (e.g., Santesso et al. 2008). These results suggest that depressed individuals are hypersensitive to negative feedback, in the sense that negative feedback leads to failure-related thoughts that, in turn, interfere with subsequent performance. On the other hand, there is also evidence for depressed individuals’ reduced feedback-related negativity in error trials following error trials (e.g., Ruchsow et al. 2004). These findings point to difficulties evaluating negative feedback and using it to improve future performance and suggest thus a hyposensitivity to negative feedback in depression .
Similarly, studies comparing reactivity to both negative and positive feedback diverge on the question whether depression is characterized by increased sensitivity to negative compared to positive feedback or whether depression is characterized by a global reduction in sensitivity to reinforcement (see Chase et al. 2010). Evidence for a negative bias comes, for instance, from a study showing that elderly depressed individuals make worse mistakes after negative but not positive feedback (von Gunten et al. 2011; but see also Chase et al. 2010). However, other studies have demonstrated a blunted behavioral and neural response to both negative and positive feedback in depressed individuals (e.g., Steele et al. 2007).
In sum, the literature converges on the conclusion that self-regulation in clinical and subclinical depression might be impaired by an altered response to negative feedback. However, it is still unclear if this impairment should be interpreted as a hypo- or a hypersensitivity to punishment , and if negative feedback has a more important impact on depressed individuals than positive feedback .
2.6 Persistence and Disengagement
In order to effectively regulate one’s behavior, it is sometimes important to persist, even in the face of obstacles, whereas in other circumstances disengagement from an unattainable goal is warranted. In the case of depression, both facilitated and impaired disengagement have been postulated and observed. On the one hand, classic theories of depression posit that depressive symptoms are associated with facilitated disengagement from unattainable goals and thus with the conservation of resources (see Wrosch and Miller 2009). Similarly, evolutionary psychologists have postulated that facilitated goal disengagement in a depressed mood serves an adaptive function to preserve resources and to avoid danger or loss (e.g., Nesse 2000). On the other hand, depression has been associated with the inability or unwillingness to abandon unattainable goals or values (e.g., Carver and Scheier 1998; Pyszczynski and Greenberg 1987).
Concerning the persistence on a specific ongoing task, there is evidence that dysphoric participants persist less long on frustrating or insoluble laboratory tasks than nondysphoric participants (Ellis et al. 2010). This earlier task disengagement—and related poorer performance outcomes—of dysphoric individuals has been shown to be independent of the kind of stop rule provided: In a study by Brinkmann and Gendolla (2014), dysphoric participants persisted less long on an item generation task, independent of whether they were instructed to stop when they “felt it was a good time to stop” or whether they were instructed to stop when they “no longer enjoyed the task”—a finding that diverges from induced negative mood (see Martin et al. 1993). With respect to the consequences of task persistence, it has been shown that dysphoric individuals’ facilitated disengagement from obsolete plans can have positive consequences, for instance, when relearning new rules (Van den Elzen and MacLeod 2006). Similarly, research by Wrosch and colleagues has demonstrated that the capacity to disengage from unattainable goals is related to subsequent decreases in depressive symptoms and increases in well-being (e.g., Dunne et al. 2011; Wrosch and Miller 2009).
The empirical evidence discussed thus far suggests that clinical and subclinical depression is associated with decreased task persistence and facilitated goal disengagement, at least with respect to concrete actions. Even though this comes with undesirable decreases in task performance, these results accord with the assumption that depression might sometimes serve an adaptive function.
2.7 Rumination and Self-Focus
In the preceding section, we have discussed evidence suggesting lower task persistence and facilitated behavioral disengagement in depression. However, from a cognitive point of view, it is well established that depression is related to impaired attentional disengagement and rumination . In this section, this maladaptive case of disengagement is discussed.
Ruminative responses have been defined as “behaviors and thoughts that focus one’s attention on one’s depressive symptoms and on the implications of these symptoms” (Nolen-Hoeksema 1991, p. 569). Such recurrent negative thoughts play an important role in the onset and maintenance of depression. Studies conducted in the framework of response style theory (Nolen-Hoeksema 1991) consistently demonstrate that the experimental induction of rumination increases negative mood in dysphoric individuals, whereas a distraction induction reduces negative mood in dysphoric individuals (see Nolen-Hoeksema et al. 2008, for a review).
From a self-regulation perspective, Pyszczynski and Greenberg (1987) have postulated that following a negative life event or failure, depressed individuals are unable to disengage from an unattainable goal but instead engage in a depressive self-focusing cycle, which intensifies their negative affect. Similar to the work by Nolen-Hoeksema and colleagues, their studies show that distraction from perseverating on negative self-content and self-discrepancies may deactivate negative self-schemas and alleviate negative biases (Pyszczynski et al. 1989).
Rumination has also been linked to deficient cognitive control and to attentional disengagement. The impaired disengagement hypothesis by Koster et al. (2011) states that depressed individuals have difficulties switching their attention away from negative self-referent material and show prolonged processing of negative stimuli (e.g., Sanchez et al. 2013). Even though empirical evidence is not unequivocal (van Deurzen et al. 2011), depressed individuals’ impaired disengagement from the elaborative processing of negative material is thought to play an important role in the perseverance of negative mood states (Joormann and Siemer 2011). In sum, theory and research presented in this section point to the fact that subclinically and clinically depressed individuals are inclined to rumination and show impaired attentional disengagement from negative material.
2.8 Affect Regulation
Sustained negative affect is the core feature of depression. Moreover, the inability to effectively regulate one’s negative affect is a well-established problem of depressed individuals. Joormann and colleagues (e.g., Joormann and Siemer 2011) suggest that cognitive biases in attention, interpretation, and memory and deficits in cognitive control (i.e., difficulties in inhibiting the elaborative processing of negative material) may be responsible for depressed individuals’ difficulties in effectively using emotion regulation strategies. A number of recent studies document that clinically, subclinically, and remitted depressed individuals indeed report using more frequently maladaptive emotion regulation strategies like rumination and using less frequently adaptive strategies like reappraisal (see Aldao et al. 2010, for a review).
Another common strategy for regulating one’s negative affect is the recall of positive memories. Several studies suggest that clinically, subclinically, and remitted depressed individuals have difficulties using such mood-incongruent recall of positive memories to effectively regulate their negative affect (e.g., Joormann et al. 2007; Josephson et al. 1996). Finally, there is evidence that not only the regulation of negative affect but also the upregulation or amplification of positive affect is impaired in clinical and subclinical depression (Werner-Seidler et al. 2013). Taken together, individuals experiencing clinical or subclinical symptoms of depression have difficulties with respect to the effective self-regulation of their affect. Moreover, maladaptive affect regulation seems to be a trait-like vulnerability that persists after remission and that predicts the future course.
2.9 Summary
In this first part of the chapter, we have outlined self-regulation functioning in clinical and subclinical depression, passing the steps of goal-directed behavior from the setting of a goal or standard, the initiation, the direction, and the persistence of an action to goal disengagement and related aspects of rumination and affect regulation. Throughout the sections, we have pointed out in which ways depressed individuals’ functioning differs from normal functioning. To start with, depressed individuals set higher standards for themselves than they expect to reach and they have difficulties in the spontaneous initiation of actions and task strategies. Moreover, depression is characterized by reduced approach behavior, by reduced responsiveness to an action’s hedonic consequences, and by a maladaptive responsiveness to negative feedback. Finally, depressed individuals show facilitated goal or task disengagement but impaired attentional disengagement from negative material. This latter case is related to depressed individuals’ propensity to ruminative self-focus and difficulties in effective affect regulation.
In the second part of this chapter, we have a closer look at one aspect of the self-regulation of behavior that has not been discussed thus far, namely, the intensity of behavior. The intensity of behavior, i.e., the vigor and engagement with which individuals pursue their goals is an important aspect of self-regulation that has largely been neglected in the depression literature thus far. From a psychophysiological point of view, we present hypotheses and evidence for the impaired adjustment of effort mobilization in subclinically depressed individuals. Finally, we exemplarily propose some treatment approaches that act on some of the aspects of impaired self-regulation functioning presented throughout this chapter.
3 Intensity of Behavior and Effort Mobilization in Dysphoria
As foreshadowed above, the intensity aspect of behavior refers to the vigor and engagement with which individuals pursue their goals. Conceptualizing the intensity of behavior as the momentary mobilization of effort at a point in time in the process of goal pursuit (see also Gendolla and Wright 2009), we have conducted a series of studies and tested several factors that are expected to moderate the effort mobilization of dysphoric individuals. In the following sections, we briefly present the theoretical background of these studies and the operationalization of effort mobilization by individuals’ cardiovascular response. Then, we describe evidence for the moderating impact of task difficulty and task context on effort mobilization. Finally, we report evidence for dysphoric individuals’ reduced effort mobilization for rewarding and punishing consequences.
3.1 Intensity of Motivation and Cardiovascular Response
Based on a resource conservation principle, the motivational intensity theory (Brehm and Self 1989) states that individuals mobilize effort proportionally to task difficulty as long as success is possible and justified: The more difficult a task is, the more effort people invest. When the task is perceived as impossible or when the perceived task difficulty exceeds the importance of success, people should withhold effort. This relationship holds for the case that task difficulty is clear and fixed. In contrast, when task difficulty is fixed but unknown (i.e., unclear task difficulty) or when the task has no fixed difficulty standard (i.e., unfixed task difficulty), effort mobilization should proportionally rise with success importance: The more important a task and its outcomes are, the more effort people invest.
In his integrative model, Wright (1996) proposed that effort mobilization can be operationalized by assessing individuals’ cardiovascular response during goal pursuit. According to this analysis, two noninvasive cardiovascular parameters should be particularly well suited for operationalizing effort mobilization because these parameters are influenced by the contractility of the heart muscle and thus by the impact of the sympathetic nervous system on the heart: pre-ejection period (PEP; in milliseconds) and systolic blood pressure (SBP; in millimeter mercury). The PEP is the time interval from the onset of left ventricular excitation until the opening of the aortic valve. It is considered as a direct measure of the force of myocardial contraction and thus as a reliable index of sympathetic activation. SBP is the maximum pressure against the blood vessels following the ejection of the blood. It is mainly influenced by the force of myocardial contraction and may thus be an indicator of sympathetic activation. Diastolic blood pressure (DBP; in millimeter mercury) is the minimum blood pressure between two heartbeats. It is less influenced by myocardial contractility and thus not considered as a reliable indicator of effort mobilization. Finally, heart rate (HR; in beats per minute) is jointly determined by the sympathetic and parasympathetic nervous systems and may under some circumstances reflect sympathetic activation (see Brownley et al. 2000). Over two decades of research within Wright’s integrative model has corroborated that cardiovascular reactivity follows the predictions of motivational intensity theory as described above (e.g., Gendolla et al. 2012a, b; Wright and Kirby 2001; Wright and Stewart 2012).
3.2 Impact of Task Difficulty and Task Context
Considering that clinical and subclinical depression is characterized by persistent negative affect, we have applied the principles of motivational intensity theory (Brehm and Self 1989) and the reasoning of the mood–behavior model (Gendolla 2000) to systematically investigate depressed individuals’ effort mobilization. According to the mood–behavior model, moods can have an informational impact on evaluations that, in turn, determine behavior. In the context of goal pursuit, we hypothesized that depressed mood should lead to a mood-congruent appraisal of task demand, i.e., to higher perceived task difficulty. For the five quasi-experimental studies reported below, we recruited extreme groups of undergraduate students with low scores (“nondysphoric”) versus high scores (“dysphoric”) on self-report depression scales. According to the dimensional perspective of psychopathology, we considered dysphoric participants to have subclinical symptoms of depression that differ quantitatively but not qualitatively from clinical depression. The dependent variable of the studies reported in the remainder of this chapter was participants’ cardiovascular reactivity, i.e., the change in cardiovascular activity from a rest to a task period. As outlined above, we focused on PEP reactivity and—whenever this parameter was unavailable—on SBP reactivity.
The first two studies (Brinkmann and Gendolla 2007) tested the predictions for tasks with unfixed difficulty, i.e., without fixed performance standard. In the first study, participants were presented with a list of letter series and were asked to correctly memorize within 5 min as many series as possible. Results corroborated that dysphoric participants showed higher SBP reactivity at the beginning of the performance period than nondysphoric participants. This finding was replicated in a second study using a concentration task. During the whole performance period, dysphoric participants showed stronger SBP reactivity than nondysphoric participants. These results suggest that tasks that ask to “do one’s best” can elicit high effort mobilization in dysphoric individuals.
Then, we investigated the joint impact of dysphoria and a clear difficulty standard on participants’ cardiovascular reactivity (Brinkmann and Gendolla 2008). Participants performed either an easy or a difficult version of a concentration task (Study 1) or a memory task (Study 2). In both studies, results revealed the expected crossover interaction pattern: In the easy condition, dysphoric participants showed stronger SBP reactivity than nondysphoric participants. In the difficult condition, however, nondysphoric participants showed stronger SBP reactivity (see Fig. 22.1). Moreover, task demand appraisals assessed before task performance indicated that dysphoric participants perceived the memory task in Study 2 as more difficult than did nondysphoric participants. Together, these findings corroborate the hypothesis that depressed mood leads to higher perceived task difficulty, which, in turn, leads to higher effort mobilization for easy tasks but to disengagement for difficult but still possible tasks because of too high subjective demand.

Cell means and standard errors of systolic blood pressure reactivity during performance of an easy versus difficult memory task in Study 2 by Brinkmann and Gendolla (2008). Does depression interfere with effort mobilization? Effects of dysphoria and task difficulty on cardiovascular response. (Copyright: American Psychological Association. Reprinted with permission)
In order to experimentally show the hypothesized role of an informational mood impact on task demand appraisals, we conducted another study that made use of a discounting manipulation, which aimed at drawing people’s attention to possible mood influences (Brinkmann et al. 2012). We presented dysphoric and nondysphoric participants with a memory task without fixed performance standard. Half of the participants received an additional cue suggesting that their current mood might have an impact while they were working on the task. Results corroborated earlier findings when no cue was provided: Dysphoric individuals had higher SBP reactivity than nondysphoric individuals. In contrast, when participants received the cue about possible mood influences, the SBP reactivity pattern was reversed. This means that mood had lost its informational value for task demand appraisals, which resulted in lower perceived task demand and thus lower SBP reactivity in dysphoric participants. These findings suggest that, when a cue was provided, dysphoric participants managed to reduce the impact of depressed mood on their task demand appraisals and on subsequent effort mobilization .
In summary, the findings of these five studies show that depression is not necessarily characterized by a general motivational deficit and disengagement of effort mobilization . Rather, when task difficulty is unfixed or easy, dysphoric individuals mobilize even more effort than nondysphorics. The results of these studies also qualify previous research that does not unequivocally find either enhanced or attenuated cardiovascular reactivity in depression and dysphoria (e.g., Carroll et al. 2007) and underline the importance of considering task difficulty and task context.
3.3 Impact of Success Importance
Success importance is another important concept of motivational intensity theory (Brehm and Self 1989). Among other variables, success importance is determined by rewards and punishments. It follows that such hedonic consequences have a direct impact on effort mobilization when task difficulty is unclear or unfixed: The more positive or negative the consequences are, the more effort mobilization is expected (see also Wright 1996). As outlined above, behavioral and neuroscientific studies have demonstrated depressed and dysphoric individuals’ reduced responsiveness to reward and, less consistently, to punishment. In the following, we report five quasi-experimental studies that investigated dysphoric individuals’ effort mobilization for obtaining rewards or avoiding punishments during tasks with either unclear or unfixed task difficulty.
In the first two studies, dysphoric and nondysphoric participants worked on mental tasks and could earn a monetary reward or avoid a monetary loss depending on their performance outcome (Brinkmann et al. 2009). Study 1 demonstrated that nondysphoric individuals showed high SBP reactivity when expecting to lose money, whereas dysphoric participants showed low SBP reactivity. Study 2 revealed that nondysphoric individuals showed higher SBP and PEP reactivity in the reward condition than in the neutral condition. In contrast, dysphoric participants showed a blunted cardiovascular response across all conditions. These findings thus suggest a general insensitivity to both monetary reward and punishment in dysphoria.
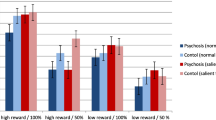
A following study by Franzen and Brinkmann (2014) aimed at investigating reward and punishment responsiveness in dysphoria on both cardiovascular and behavioral levels. Working on a recognition memory task, one third of the participants earned small amounts of money for correct responses, one third lost small amounts of money for incorrect responses, and one third neither earned nor lost money. As expected, reactivity of PEP was higher in both incentive conditions compared to the neutral condition for nondysphoric participants, while it was blunted across all three conditions for dysphoric participants (see Fig. 22.2). On the behavioral level, results revealed that nondysphorics performed better following a monetary loss than did dysphorics. This study thus confirms that dysphorics have a motivational deficit during both reward and punishment anticipation and that they show an altered behavioral response to punishment.

Cell means and standard errors of pre-ejection period reactivity during performance of a recognition memory task in anticipation of monetary rewards or punishments in the study by Franzen and Brinkmann (2014)
In order to investigate the linear increase of effort mobilization with increasing reward value as suggested by motivational intensity theory (Brehm and Self 1989), another study by Brinkmann and Franzen (2013) manipulated monetary reward at three levels. Participants worked on a memory task with unclear performance standard, expecting no reward, a small monetary reward, or a high monetary reward for successful overall task performance. As expected, nondysphorics gradually mobilized more effort in terms of PEP reactivity dependent on reward value, whereas dysphorics did not mobilize more effort during reward anticipation compared to the condition without reward. This study suggests that dysphoric individuals’ insensitivity to monetary reward generalizes across varying reward levels.
Finally, a study by Brinkmann et al. (in press) took into account the fact that not only monetary gains or losses determine the importance of success: Social consequences are also important motivators and at the same time susceptible to impaired effectiveness in depression (Forbes and Dahl 2012). Dysphoric and nondysphoric participants worked on a 5-min memory task. Half of them received the vague instruction that “in case they performed well,” they would have the possibility to enter their name in the study’s public “best list.” As expected, nondysphoric participants’ SBP reactivity was higher when they anticipated getting this kind of social approval for good performance. In contrast, dysphoric individuals had low SBP reactivity regardless of the presence or absence of the social reward. These findings expand prior evidence for reward insensitivity in depression to social rewards.
Our studies on reward and punishment responsiveness in subclinical depression confirm that dysphoric individuals’ effort mobilization is blunted regardless of the kind or amount of incentives at stake. Our motivational analysis thus suggests that the self-regulation of effort mobilization is indeed impaired in subclinical depression and converges with the findings of impaired self-reported, behavioral, and neural reward responsiveness in depression reported above.
3.4 Summary
Taken together, our program of research leads us to conclude that there is no general motivational deficit in subclinical—and presumably also clinical—depression. Rather, one can observe a maladaptive adjustment of effort mobilization: Dysphoric individuals do not seem to take into account information about task difficulty and success importance in an adaptive way. It is of note that recent cardiovascular findings suggest that the effects reported above might be mood-state dependent and thus reflect motivational deficits rather than stable biomarkers of depression (Salomon et al. 2013). Our findings have important implications for the treatment of depression. First, being aware of the impact of negative affect on task demand appraisals, it is important to avoid the impression of tasks being too difficult but rather start with easy or “do your best” tasks (see below). Second, in order to raise the level of maximum effort that a person is willing to invest (see Brehm and Self 1989), treatments have to act on alleviating anhedonic symptoms (see below).
4 Conclusions and Implications
Throughout this chapter, we have reviewed evidence for impaired self-regulation functioning in clinical and subclinical depression. Understanding impaired self-regulation is important as this knowledge is the basis for proposing specific treatments that allow depressed individuals to develop a more adaptive self-regulation of their behavior. Fortunately, there exist a number of treatment approaches that are targeted on specific aspects of depression. To conclude this chapter, we exemplarily focus on reward sensitivity and goal setting and present three specific therapies that are suited for alleviating these impairments in depression.
First, behavioral activation is an appropriate treatment to cope with insensitivity to reward or with depressed individuals’ tendency to set too high goals. This structured approach has emerged in the 1950s (Bennett-Levy et al. 2004) and has been proven effective for clinical depression (e.g., Cuijpers et al. 2007; Hopko et al. 2003). Behavioral activation aims at helping depressed individuals to reengage in pleasant activities, which will increase reinforcement from the environment, and in turn elicit the experience of pleasure. What is more, behavioral activation proposes to start with the identification of small and doable goals. Then, depressed individuals ought to gradually identify and achieve higher goals. In sum, behavioral activation techniques should increase reward sensitivity, avoid the setting of unachievable goals, and counteract the vicious cycle of ruminative self-focus (Dimidjian et al. 2008).
Second, mindfulness-based cognitive therapy (MBCT; Segal et al. 2013) could also be proposed to remitted depressed patients to increase reward sensitivity. This program is specifically designed to prevent depressive relapse. During each session, formal (e.g., sitting meditation, body scan) and informal (e.g., walking, yoga, cultivating mindfulness in daily life) meditation practices are suggested in combination with features of cognitive therapy for depression (e.g., identify the warning signs of depression). Concerning positive affect in particular, one exercise invites participants to think about a recently experienced pleasant event and to analyze it while being aware of related thoughts, feelings , and bodily sensations. Another exercise focuses on identifying nourishing activities during a typical day and on making a list of pleasurable activities that can be programmed when one feels bad. A number of studies have demonstrated the efficacy of MBCT not only for the reduction of depressive symptoms (e.g., Ma and Teasdale 2004) but also for increasing positive emotions and reward experience (Geschwind et al. 2011).
Finally, positive psychotherapy aims at increasing positive emotions, engagement, and meaning and should allow depressed individuals to rediscover pleasure (Seligman et al. 2006). Specifically, the module “savoring” invites participants to take the time to consciously enjoy something that one usually hurries through in daily life (e.g., eating a meal, taking a shower). Then, participants describe what they did, how they did it in a different way than usually, and how they felt compared to how they usually feel. Another module invites participants each evening to write down three good things that happened during the day and to explain why they think these events happened.
To conclude, clinical and subclinical depression is characterized by dysfunctional self-regulation of behavior. Fortunately, a number of specific treatments exist, among which we have exemplarily outlined three. A detailed knowledge of dysfunctional self-regulation in depression is crucial for the development of further treatment approaches and for individually tailoring them to the specific symptoms of the individual patient.
References
Ahrens, A. H. (1987). Theories of depression: The role of goals and the self-evaluation process. Cognitive Therapy and Research, 11, 665–680. doi:10.1007/BF01176004.
Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30, 217–237. doi:10.1016/j.cpr.2009.11.004.
American Psychiatric Association. (2000). DSM-IV-TR: Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
Austin, M. P., Mitchell, P., & Goodwin, G. M. (2001). Cognitive deficits in depression: Possible implications for functional neuropathology. British Journal of Psychiatry, 178, 200–206. doi:10.1192/bjp.178.3.200.
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression. New York: Guilford.
Bennett-Levy, J., Butler, G., Fennell, M., Hackman, A., Mueller, M., & Westbrook, D. (2004). Oxford guide to behavioural experiments in cognitive therapy. New York: Oxford University Press.
Berridge, K. C. (2003). Pleasures of the brain. Brain and Cognition, 52, 106–128. doi:10.1016/s0278-2626(03)00014-9.
Bijttebier, P., Beck, I., Claes, L., & Vandereycken, W. (2009). Gray’s Reinforcement Sensitivity Theory as a framework for research on personality-psychopathology associations. Clinical Psychology Review, 29, 421–430. doi:10.1016/j.cpr.2009.04.002.
Brehm, J. W., & Self, E. A. (1989). The intensity of motivation. Annual Review of Psychology, 40, 109–131. doi:10.1146/annurev.ps.40.020189.000545.
Brinkmann, K., & Gendolla, G. H. E. (2007). Dysphoria and mobilization of mental effort: Effects on cardiovascular reactivity. Motivation and Emotion, 31, 71–82. doi:10.1007/s11031-007-9054-0.
Brinkmann, K., & Gendolla, G. H. E. (2008). Does depression interfere with effort mobilization? Effects of dysphoria and task difficulty on cardiovascular response. Journal of Personality and Social Psychology, 94, 146–157. doi:10.1037/0022-3514.94.1.146.
Brinkmann, K., & Gendolla, G. H. E. (2014). When should I stop? Impaired task persistence in dysphoric individuals. Manuscript submitted for publication.
Brinkmann, K., Grept, J., & Gendolla, G. H. E. (2012). Dysphorics can control depressive mood’s informational impact on effort mobilization. Motivation and Emotion, 36, 232–241. doi:10.1007/s11031-011-9236-7.
Brinkmann, K., & Franzen, J. (2013). Not everyone’s heart contracts to reward: Insensitivity to varying levels of reward in dysphoria. Biological Psychology, 94, 263–271. doi:10.1016/j.biopsycho.2013.07.003.
Brinkmann, K., Franzen, J., Rossier, C., & Gendolla, G. H. E. (in press). I don’t care about others’ approval: Insensitivity to social rewards in dysphoria. Motivation and Emotion.
Brinkmann, K., Schüpbach, L., Ancel Joye, I., & Gendolla, G. H. E. (2009). Anhedonia and effort mobilization in dysphoria: Reduced cardiovascular response to reward and punishment. International Journal of Psychophysiology, 74, 250–258. doi:10.1016/j. ijpsycho.2009.09.009.
Brownley, K. A., Hurwitz, B. E., & Schneiderman, N. (2000). Cardiovascular psychophysiology. In J. T. Cacioppo, L. G. Tassinary, & G. G. Berntson (Eds.), Handbook of psychophysiology (pp. 224–264). New York: Cambridge University Press.
Carroll, D., Phillips, A. C., Hunt, K., & Der, G. (2007). Symptoms of depression and cardiovascular reactions to acute psychological stress: Evidence from a population study. Biological Psychology, 75, 68–74. doi:10.1016/j.biopsycho.2006.12.002.
Carver, C. S., & Scheier, M. F. (1998). On the self-regulation of behavior. New York: Cambridge University Press.
Carver, C. S., Johnson, S. L., & Joormann, J. (2008). Serotonergic function, two-mode models of self-regulation, and vulnerability to depression: What depression has in common with impulsive aggression. Psychological Bulletin, 134, 912–943. doi:10.1037/a0013740.
Carver, C. S., Johnson, S. L., & Joormann, J. (2009). Two-mode models of self-regulation as a tool for conceptualizing effects of the serotonin system in normal behavior and diverse disorders. Current Directions in Psychological Science, 18, 195–199. doi:10.1111/j.1467-8721.2009.01635.x.
Chase, H. W., Frank, M. J., Michael, A., Bullmore, E. T., Sahakian, B. J., & Robbins, T. W. (2010). Approach and avoidance learning in patients with major depression and healthy controls: Relation to anhedonia. Psychological Medicine, 40, 433–440. doi:10.1017/S0033291709990468.
Chentsova-Dutton, Y., & Hanley, K. (2010). The effects of anhedonia and depression on hedonic responses. Psychiatry Research, 179, 176–180. doi:10.1016/j.psychres.2009.06.013.
Cuijpers, P., van Straten, A., & Warmerdam, L. (2007). Behavioral activation treatments of depression: A meta-analysis. Clinical Psychology Review, 27, 318–326. doi:10.1016/j.cpr.2006.11.001.
Depue, R. A., & Iacono, W. G. (1989). Neurobehavioral aspects of affective disorders. Annual Review of Psychology, 40, 457–492. doi:10.1146/annurev.ps.40.020189.002325.
Dichter, G. S., Kozink, R. V., McClernon, F. J., & Smoski, M. J. (2012). Remitted major depression is characterized by reward network hyperactivation during reward anticipation and hypoactivation during reward outcomes. Journal of Affective Disorders, 136, 1126–1134. doi:10.1016/j.jad.2011.09.048.
Dickson, J. M., Moberly, N. J., & Kinderman, P. (2011). Depressed people are not less motivated by personal goals but are more pessimistic about attaining them. Journal of Abnormal Psychology, 120, 975–980. doi:10.1037/a0023665.
Dimidjian, S., Martell, C. R., Addis, M. E., & Herman-Dunn, R. (2008). Behavioral activation for depression. In D. H. Barlow (Ed.), Clinical handbook of psychological disorders: A step-by-step treatment manual (4th ed.; pp. 328–364). New York: Guilford.
Dunne, E., Wrosch, C., & Miller, G. E. (2011). Goal disengagement, functional disability, and depressive symptoms in old age. Health Psychology, 30, 763–770. doi:10.1037/a0024019.
Elliott, R., Sahakian, B. J., Herrod, J. J., Robbins, T. W., & Paykel, E. S. (1997). Abnormal response to negative feedback in unipolar depression: Evidence for a diagnosis specific impairment. Journal of Neurology, Neurosurgery, and Psychiatry, 63, 74–82. doi:10.1136/jnnp.63.1.74.
Elliott, R., Sahakian, B. J., Michael, A., Paykel, E. S., & Dolan, R. J. (1998). Abnormal neural response to feedback on planning and guessing tasks in patients with unipolar depression. Psychological Medicine, 28, 559–571. doi:10.1017/S0033291798006709.
Ellis, A. J., Fischer, K. M., & Beevers, C. G. (2010). Is dysphoria about being red and blue? Potentiation of anger and reduced distress tolerance among dysphoric individuals. Cognition and Emotion, 24, 596–608. doi:10.1080/13803390902851176.
Eshel, N., & Roiser, J. P. (2010). Reward and punishment processing in depression. Biological Psychiatry, 68, 118–124. doi:10.1016/j.biopsych.2010.01.027.
Fergusson, D. M., Horwood, L. J., Ridder, E. M., & Beautrais, A. L. (2005). Subthreshold depression in adolescence and mental health outcomes in adulthood. Archives of General Psychiatry, 62, 66–72. doi:10.1001/archpsyc.62.1.66.
Forbes, E. E., & Dahl, R. E. (2012). Research review: Altered reward function in adolescent depression: What, when and how? Journal of Child Psychology and Psychiatry, 53, 3–15. doi:10.1111/j.1469-7610.2011.02477.x.
Forbes, E. E., Hariri, A. R., Martin, S. L., Silk, J. S., Moyles, D. L., Fisher, P. M., et al. (2009). Altered striatal activation predicting real-world positive affect in adolescent major depressive disorder. American Journal of Psychiatry, 166, 64–73. doi:10.1176/appi.ajp.2008.07081336.
Foti, D., Kotov, R., Klein, D. N., & Hajcak, G. (2011). Abnormal neural sensitivity to monetary gains versus losses among adolescents at risk for depression. Journal of Abnormal Child Psychology, 39, 913–924. doi:10.1007/s10802-011-9503-9.
Franzen, J., & Brinkmann, K. (2014). Blunted cardiovascular reactivity in dysphoria during reward and punishment anticipation. Manuscript submitted for publication.
Geen, R. G. (1995). Human motivation: A social psychological approach. Pacific Grove: Brooks/Cole.
Gendolla, G. H. E. (2000). On the impact of mood on behavior: An integrative theory and a review. Review of General Psychology, 4, 378–408. doi:10.1037/1089-2680.4.4.378.
Gendolla, G. H. E., Brinkmann, K., & Silvestrini, N. (2012a). Gloomy and lazy? On the impact of mood and depressive symptoms on effort-related cardiovascular response. In R. A. Wright & G. H. E. Gendolla (Eds.), How motivation affects cardiovascular response: Mechanisms and applications (pp. 139–155). Washington, DC: American Psychological Association.
Gendolla, G. H. E., & Wright, R. A. (2009). Effort. In D. Sander & K. R. Scherer (Eds.), Oxford companion to the affective sciences (pp. 134–135). New York: Oxford University Press.
Gendolla, G. H. E., Wright, R. A., & Richter, M. (2012b). Effort intensity: Some insights from the cardiovascular system. In R. M. Ryan (Ed.), The Oxford handbook of human motivation (pp. 420–438). New York: Oxford University Press.
Geschwind, N., Peeters, F., Drukker, M., van Os, J., & Wichers, M. (2011). Mindfulness training increases momentary positive emotions and reward experience in adults vulnerable to depression: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 79, 618–628. doi:10.1037/a0024595.
Golin, S., & Terrell, F. (1977). Motivational and associative aspects of mild depression in skill and chance tasks. Journal of Abnormal Psychology, 86, 389–401. doi:10.1037/0021-843X.86.4.389.
Gollwitzer, P. M., & Sheeran, P. (2006). Implementation intentions and goal achievement: A meta-analysis of effects and processes. In M. P. Zanna (Ed.), Advances in experimental social psychology (Vol. 38, pp. 69–119). San Diego: Elsevier Academic.
Gotlib, I. H., Hamilton, J. P., Cooney, R. E., Singh, M. K., Henry, M. L., & Joormann, J. (2010). Neural processing of reward and loss in girls at risk for major depression. Archives of General Psychiatry, 67, 380–387. doi:10.1001/archgenpsychiatry.2010.13.
Gotlib, I. H., & Joormann, J. (2010). Cognition and depression: Current status and future directions. Annual Review of Clinical Psychology, 6, 285–312. doi:10.1146/annurev.clinpsy.121208.131305.
Gray, J. A. (1982). The neuropsychology of anxiety: An enquiry into the functions of the septo-hippocampal system. Oxford: Oxford University Press.
Henriques, J. B., & Davidson, R. J. (2000). Decreased responsiveness to reward in depression. Cognition and Emotion, 14, 711–724. doi:10.1080/02699930050117684.
Hertel, P. T. (2000). The cognitive-initiative account of depression-related impairments in memory. In D. L. Medin (Ed.), The psychology of learning and motivation: Advances in research and theory (Vol. 39, pp. 47–71). San Diego: Academic.
Hopko, D. R., Lejuez, C. W., LePage, J. P., Hopko, S. D., & McNeil, D. W. (2003). A brief behavioral activation treatment for depression: A randomized pilot trial within an inpatient psychiatric hospital. Behavior Modification, 27, 458–469. doi:10.1177/0145445503255489.
Jacobson, N. S., Martell, C. R., & Dimidjian, S. (2001). Behavioral activation treatment for depression: Returning to contextual roots. Clinical Psychology: Science and Practice, 8, 255–270. doi:10.1093/clipsy/8.3.255.
Joormann, J., & Siemer, M. (2011). Affective processing and emotion regulation in dysphoria and depression: Cognitive biases and deficits in cognitive control. Social and Personality Psychology Compass, 5, 13–28. doi:10.1111/j.1751-9004.2010.00335.x.
Joormann, J., Siemer, M., & Gotlib, I. H. (2007). Mood regulation in depression: Differential effects of distraction and recall of happy memories on sad mood. Journal of Abnormal Psychology, 116, 484–490. doi:10.1037/0021-843x.116.3.484.
Josephson, B. R., Singer, J. A., & Salovey, P. (1996). Mood regulation and memory: Repairing sad moods with happy memories. Cognition and Emotion, 10, 437–444. doi:10.1080/026999396380222.
Judd, L. L., Schettler, P. J., & Akiskal, H. S. (2002). The prevalence, clinical relevance, and public health significance of subthreshold depressions. Psychiatric Clinics of North America, 25, 685–698. doi:10.1016/s0193-953×(02)00026-6.
Kessler, R. C., & Wang, P. S. (2009). Epidemiology of depression. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (2nd ed.) (pp. 5–22). New York: Guilford.
Klenk, M. M., Strauman, T. J., & Higgins, E. T. (2011). Regulatory focus and anxiety: A self-regulatory model of GAD-depression comorbidity. Personality and Individual Differences, 50, 935–943. doi:10.1016/j.paid.2010.12.003.
Koster, E. H. W., De Lissnyder, E., Derakshan, N., & De Raedt, R. (2011). Understanding depressive rumination from a cognitive science perspective: The impaired disengagement hypothesis. Clinical Psychology Review, 31, 138–145. doi:10.1016/j.cpr.2010.08.005.
Kunisato, Y., Okamoto, Y., Ueda, K., Onoda, K., Okada, G., Yoshimura, S., et al. (2012). Effects of depression on reward-based decision making and variability of action in probabilistic learning. Journal of Behavior Therapy and Experimental Psychiatry, 43, 1088–1094. doi:10.1016/j.jbtep.2012.05.007.
Lafont, V., Medecin, I., Robert, P. H., Beaulieu, F. E., Kazes, M., Danion, J. M., et al. (1998). Initiation and supervisory process in schizophrenia and depression. Schizophrenia Research, 34, 49–57. doi:10.1016/S0920-9964(98)00084-X.
Liu, W., Chan, R. C. K., Wang, L.-z., Huang, J., Cheung, E. F. C., Gong, Q.-y., et al. (2011). Deficits in sustaining reward responses in subsyndromal and syndromal major depression. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 35, 1045–1052. doi:10.1016/j.pnpbp.2011.02.018.
Ma, S. H., & Teasdale, J. D. (2004). Mindfulness-based cognitive therapy for depression: Replication and exploration of differential relapse prevention effects. Journal of Consulting and Clinical Psychology, 72, 31–40. doi:10.1037/0022 − 006x.72.1.31.
Martin, L. L., Ward, D. W., Achee, J. W., & Wyer, R. S. (1993). Mood as input: People have to interpret the motivational implications of their moods. Journal of Personality and Social Psychology, 64, 317–326. doi:10.1037/0022-3514.64.3.317.
McCabe, C., Cowen, P. J., & Harmer, C. J. (2009). Neural representation of reward in recovered depressed patients. Psychopharmacology, 205, 667–677. doi:10.1007/s00213-009-1573-9.
Nesse, R. M. (2000). Is depression an adaptation? Archives of General Psychiatry, 57, 14–20. doi:10.1001/archpsyc.57.1.14.
Nestler, E. J., & Carlezon, W. A. (2006). The mesolimbic dopamine reward circuit in depression. Biological Psychiatry, 59, 1151–1159. doi:10.1016/j.biopsych.2005.09.018.
Nitschke, J. B., Heller, W., Etienne, M. A., & Miller, G. A. (2004). Prefrontal cortex activity differentiates processes affecting memory in depression. Biological Psychology, 67, 125–143. doi:10.1016/j.biopsycho.2004.03.004.
Nolen-Hoeksema, S. (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100, 569–582. doi:10.1037/0021-843x.100.4.569.
Nolen-Hoeksema, S., Wisco, B. E., & Lyubomirsky, S. (2008). Rethinking rumination. Perspectives on Psychological Science, 3, 400–424. doi:10.1111/j.1745-6924.2008.00088.x.
Pizzagalli, D. A., Iosifescu, D., Hallett, L. A., Ratner, K. G., & Fava, M. (2009). Reduced hedonic capacity in major depressive disorder: Evidence from a probabilistic reward task. Journal of Psychiatric Research, 43, 76–87. doi:10.1016/j.jpsychires.2008.03.001.
Pyszczynski, T., & Greenberg, J. (1987). Self-regulatory perseveration and the depressive self-focusing style: A self-awareness theory of reactive depression. Psychological Bulletin, 102, 122–138. doi:10.1037/0033-2909.102.1.122.
Pyszczynski, T., Hamilton, J. C., Herring, F. H., & Greenberg, J. (1989). Depression, self-focused attention, and the negative memory bias. Journal of Personality and Social Psychology, 57, 351–357. doi:10.1037/0022-3514.57.2.351.
Qian, M., Wang, A., & Chen, Z. (2002). A comparison of classmate and self-evaluation of dysphoric and nondysphoric Chinese students. Cognition and Emotion, 16, 565–576. doi:10.1080/02699930143000329.
Rottenberg, J. (2007). Major depressive disorder: Emerging evidence for emotion context insensitivity. In J. Rottenberg & S. L. Johnson (Eds.), Emotion and psychopathology: Bridging affective and clinical science (pp. 151–165). Washington, DC: American Psychological Association.
Ruchsow, M., Herrnberger, B., Wiesend, C., Grön, G., Spitzer, M., & Kiefer, M. (2004). The effect of erroneous responses on response monitoring in patients with major depressive disorder: A study with event-related potentials. Psychophysiology, 41, 833–840. doi:10.1111/j.1469-8986.2004.00237.x.
Salomon, K., Bylsma, L. M., White, K. E., Panaite, V., & Rottenberg, J. (2013). Is blunted cardiovascular reactivity in depression mood-state dependent? A comparison of major depressive disorder remitted depression and healthy controls. International Journal of Psychophysiology, 90, 50–57. doi:10.1016/j.ijpsycho.2013.05.018.
Sanchez, A., Vazquez, C., Marker, C., LeMoult, J., & Joormann, J. (2013). Attentional disengagement predicts stress recovery in depression: An eye-tracking study. Journal of Abnormal Psychology, 122, 303–313. doi:10.1037/a0031529.
Santesso, D. L., Steele, J. D., Bogdan, R., Holmes, A. J., Deveney, C. M., Meites, T. M., et al. (2008). Enhanced negative feedback responses in remitted depression. Neuroreport, 19, 1045–1048. doi:10.1097/WNR.0b013e3283036e73.
Scheurich, A., Fellgiebel, A., Schermuly, I., Bauer, S., Wölfges, R., & Müller, M. J. (2008). Experimental evidence for a motivational origin of cognitive impairment in major depression. Psychological Medicine, 38, 237–246. doi:10.1017/S0033291707002206.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2013). Mindfulness-based cognitive therapy for depression (2nd ed.). New York: Guilford.
Seligman, M. E. P., Rashid, T., & Parks, A. C. (2006). Positive psychotherapy. American Psychologist, 61, 774–788. doi:10.1037/0003-066x.61.8.774.
Shankman, S. A., Klein, D. N., Tenke, C. E., & Bruder, G. E. (2007). Reward sensitivity in depression: A biobehavioral study. Journal of Abnormal Psychology, 116, 95–104. doi:10.1037/0021-843X.116.1.95.
Smoski, M. J., Rittenberg, A., & Dichter, G. S. (2011). Major depressive disorder is characterized by greater reward network activation to monetary than pleasant image rewards. Psychiatry Research: Neuroimaging, 194, 263–270. doi:10.1016/j.pscychresns.2011.06.012.
Steele, J. D., Kumar, P., & Ebmeier, K. P. (2007). Blunted response to feedback information in depressive illness. Brain: A Journal of Neurology, 130, 2367–2374. doi:10.1093/brain/awm150.
Steffens, D. C., Wagner, H. R., Levy, R. M., Horn, K. A., & Krishnan, K. R. R. (2001). Performance feedback deficit in geriatric depression. Biological Psychiatry, 50, 358–363. doi:10.1016/s0006-3223(01)01165-9.
Thibodeau, R., Jorgensen, R. S., & Kim, S. (2006). Depression, anxiety, and resting frontal EEG asymmetry: A meta-analytic review. Journal of Abnormal Psychology, 115, 715–729. doi:10.1037/0021-843X.115.4.715.
Tillema, J. L., Cervone, D., & Scott, W. D. (2001). Negative mood, perceived self-efficacy, and personal standards in dysphoria: The effects of contextual cues on self-defeating patterns of cognition. Cognitive Therapy and Research, 25, 535–549. doi:10.1023/A:1005511730618.
Treadway, M. T., Bossaller, N. A., Shelton, R. C., & Zald, D. H. (2012). Effort-based decision-making in major depressive disorder: A translational model of motivational anhedonia. Journal of Abnormal Psychology, 121, 553–558. doi:10.1037/a0028813.
Van den Elzen, J., & MacLeod, C. (2006). Facilitated cognitive disengagement in depression. Behavior Therapy, 37, 304–313. doi:10.1016/j.beth.2006.02.005.
van Deurzen, P. A. M., Roelofs, J., Slaats-Willemse, D. I. E., Rinck, M., Buitelaar, J. K., & Speckens, A. E. M. (2011). Facilitated attentional disengagement from negative information in relation to self-reported depressive symptoms of Dutch female undergraduate students. Psychological Reports, 108, 252–262. doi:10.2466/02.09.22.pr0.108.1.252-262.
von Gunten, A., Herrmann, F. R., Elliott, R., & Duc, R. (2011). Abnormal sensitivity to negative feedback in late-life depression. Psychiatry and Clinical Neurosciences, 65, 333–340. doi:10.1111/j.1440-1819.2011.02215.x.
Werner-Seidler, A., Banks, R., Dunn, B. D., & Moulds, M. L. (2013). An investigation of the relationship between positive affect regulation and depression. Behaviour Research and Therapy, 51, 46–56. doi:10.1016/j.brat.2012.11.001.
Wheeler, H. A., Blankstein, K. R., Antony, M. M., McCabe, R. E., & Bieling, P. J. (2011). Perfectionism in anxiety and depression: Comparisons across disorders, relations with symptom severity, and role of comorbidity. International Journal of Cognitive Therapy, 4, 66–91. doi:10.1521/ijct.2011.4.1.66.
Wright, R. A. (1996). Brehm’s theory of motivation as a model of effort and cardiovascular response. In P. M. Gollwitzer & J. A. Bargh (Eds.), The psychology of action: Linking cognition and motivation to behavior (pp. 424–453). New York: Guilford.
Wright, R. A., & Kirby, L. D. (2001). Effort determination of cardiovascular response: An integrative analysis with applications in social psychology. In M. P. Zanna (Ed.), Advances in experimental social psychology (Vol. 33, pp. 255–307). New York: Academic.
Wright, R. A., & Stewart, C. C. (2012). Multifaceted effects of fatigue on effort and associated cardiovascular responses. In R. A. Wright & G. H. E. Gendolla (Eds.), How motivation affects cardiovascular response: Mechanisms and applications (pp. 199–218). Washington, DC: American Psychological Association.
Wrosch, C., & Miller, G. E. (2009). Depressive symptoms can be useful: Self-regulatory and emotional benefits of dysphoric mood in adolescence. Journal of Personality and Social Psychology, 96, 1181–1190. doi:10.1037/a0015172.
Acknowledgments
The preparation of this chapter was supported by a research grant from the Swiss National Science Foundation (SNF 100014-134557) awarded to the first author. We are grateful to Michael Richter for helpful comments on an early draft of this chapter.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Brinkmann, K., Franzen, J. (2015). Depression and Self-Regulation: A Motivational Analysis and Insights from Effort-Related Cardiovascular Reactivity. In: Gendolla, G., Tops, M., Koole, S. (eds) Handbook of Biobehavioral Approaches to Self-Regulation. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1236-0_22
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1236-0_22
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1235-3
Online ISBN: 978-1-4939-1236-0
eBook Packages: Behavioral ScienceBehavioral Science and Psychology (R0)