
Abstract
Headache and rhinosinusitis are two of the most common conditions seen in clinical practice. Although headache is common in patients with sinus disease, recurrent disabling headache is usually due to migraine or a related disorder. Migraine frequently presents with symptoms such as frontal pressure, congestion, or facial pain which can mimic sinus pathology. Cluster headache and other trigeminal autonomic cephalalgias can cause significant autonomic symptoms, such as tearing, congestion, and rhinorrhea. Cluster headache is more common in tobacco users and in some cases can result from sinus pathology. Stimulation of the sphenopalatine ganglion is an emerging treatment for cluster headache. Contact point headache should be considered in patients with focal headaches and a contact point on the lateral nasal wall. Spinal fluid leak due to nasal disease may produce a low-pressure headache syndrome. Trigeminal neuralgia and other facial pains may be attributed to sinus disease, but proven nasal/sinus causes are unusual. Although most cases of frontal, maxillary, and ethmoid sinusitis are fairly easy to diagnose and not often confused with headache, sphenoid sinusitis is more commonly overlooked as a source of head pain and can present with progressive or thunderclap headache.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Headache disorders are extremely common in clinical practice and frequently cause frontal or sinus pain and pressure. Many patients attribute their symptoms to sinus pathology, which may bring them to the attention of an otolaryngologist and allergist. Primary headache disorders, such as migraine and cluster headache, which commonly produce associated autonomic symptoms, such as tearing, ptosis, rhinorrhea, conjunctival injection, or facial flushing, may cause patients or clinicians to wrongly diagnose “sinus headache” [1].
Clinicians who treat sinus disease should be familiar with common headache disorders, such as migraine and tension-type headache, and trigeminal autonomic cephalalgias, such as cluster headache, that present with frontal pain. Sinusitis, more accurately rhinosinusitis, does not usually cause severe headache and is usually diagnosed on the basis of clinical symptoms and imaging studies. Sphenoid sinusitis, however, may present with intractable headache without typical sinusitis symptoms. The anatomy of the nasal cavity may contribute to headache presentation or location and may cause chronic pain. This chapter focuses on the common headaches that might present with frontal headache, reviews common secondary headaches, and outlines the diagnosis and treatment of headache associated with sinusitis.
Headache Disorders and the Sinus
Headache and rhinosinusitis are both extremely common. In most cases diagnosing either is relatively straightforward. Many patients will not seek medical attention for mild cases of either disorder. Acute rhinosinusitis usually involves nasal airway inflammation and infection of one or more paranasal sinuses. Viral infections are the most common cause of upper airway inflammation and up to 2 % of patients develop bacterial infections [2]. Common symptoms include nasal discharge, tooth pain, anosmia or hyposmia, pain when bending forward, fever, malaise, and facial pain or headache. The sinus areas affected predict the pain’s location, but severe headache is relatively uncommon. In fact, the sinuses are not particularly pain sensitive [3].
Recurrent frontal headache in a patient without signs of sinusitis is more typically caused by a primary headache disorder. Migraine and other headaches commonly produce frontal or facial pain during attacks. Nasal congestion is a common migraine prodrome [4]. Parasympathetic fibers of the sphenopalatine ganglion and their surrounding blood vessels in the pterygopalatine fossa commonly produce autonomic symptoms that may be mistaken for sinus disease in association with headache attacks [5]. These autonomic symptoms, common in migraine and obligatory in cluster headache (CH), include nasal congestion or rhinorrhea, conjunctival injection or lacrimation, and eyelid edema.
Referred Pain and Wolff’s Experiments
The phenomenon of referred pain is well known to health-care providers with examples such as shoulder pain being triggered from gall bladder or cardiac dysfunction. Although the exact mechanisms remain obscure, the concept of axonal reflex initiated through the nasal mucosa and the release of neuropeptides has long been discussed [6] (Fig. 13.1). Harold Wolff, in his classic experiments in the 1940s, defined patterns of referred pain from stimulating the various points in the nasal cavity [7] (Table 13.1). Wolff evaluated the pain distribution and intensity referred from stimulating the nasal and sinus mucosa of human volunteers with a blunt probe, faradic electric current, and epinephrine-soaked cotton pledgets. His study group was composed of five normal subjects, ten subjects who were post-complete excision of a left acoustic neuroma with facial nerve resection, five with CRS, four with acute rhinosinusitis, and one subject with an oroantral fistula. Wolff came to three basic conclusions:

Diagram depicting how an intranasal irritant stimulus (mechanical, thermal, chemical, or inflammatory) can induce referred reflex pain in other areas in the distribution of the trigeminal nervous system, as well as autonomic phenomena. The intranasal stimulus initiates an orthodromic sensory impulse back to the CNS. However, the signal may also get rerouted along other branches of the stimulated nerve (antidromic conduction). These branches innervate pain-sensitive structures such as the dura, eye, and skin of the scalp. The release of substance P (SP) as a result of antidromic conduction at these other peripheral terminals leads to inflammatory events pictured. Since SP-immunoreactive nerves have been found in high concentration around the sphenopalatine ganglion, reflex parasympathetic stimulation may also ensue. The CNS probably modulates incoming impulses through a variety of mechanisms, including the influence of enkephalins (EK) (Reprinted from Clerico [6]. With permission from John Wiley & Sons, Inc.)
-
1.
The mucosa covering the sinus ostia are the most pain-sensitive areas in the sinonasal cavity, followed by the turbinates, and then the septum and mucosa within the sinuses.
-
2.
Stimulation within the sinonasal cavity produced referred pain rather than pain at the site of stimulation.
-
3.
If a headache was not associated with inflammation and engorgement of the turbinates, it was in all probability not referred from nasal and sinus structures [8].
Subsequent studies have suggested that the middle turbinate is more sensitive than the inferior turbinate using a pressure probe and gives credence to the nasal contact point theory as a possible headache source (see below) [9].
The chemosensory innervation of the nasal respiratory epithelium has been more recently investigated, and the information sheds some light on why certain individual patients complain of headache from nasal stimuli and sinus infection while others do not. The nasal mucosa is the first tissue of the body to have contact with potentially toxic agents within the inhaled airstream. Consequently, a number of protective neurovascular mechanisms are associated with the nasal mucosa. The nasal respiratory epithelium is densely innervated by the first and second branches of the trigeminal nerve. This intranasal sensory system provides feedback to protective neuromechanisms about our airborne environment. Thus, humidity, temperature, and irritation of inhaled air are all directly analyzed. Many agents, such as dust, smoke, or irritative gases such as some perfumes, activate trigeminal nerve fibers that innervate the epithelium, triggering local axon reflexes. These have been shown to generate, for example, calcitonin gene-related peptide and substance P liberation and nasopulmonary reflexes such as sneezing and coughing to prevent noxious substances from entering the respiratory system [10]. Innervation of the nasal/sinus epithelium depends on two major trigeminal fiber systems: the unmyelinated C-fibers and the myelinated Ad-fibers [11]. C-fibers stimulation induces a burning pain sensation and Ad-fibers mediate a sharp, stinging sensation [12].
A number of studies have established that intranasal trigeminal fibers act as a detection system for noxious chemicals and trigger a protective respiratory response [13–16].
The nerve endings of trigeminal fibers in the nasal mucosa are not covered by squamous epithelium which provides most chemicals and inflammatory mediators ready access to receptors that innervate the nasal mucosa and increases their sensitivity to painful stimuli [17]. In a study by Meusel et al., the authors found that trigeminal sensitivity of the human nasal mucosa varies in relation to the site of stimulation and to the type of chemical irritants with the posterior region of the nasal cavity, namely, the posterior septum and the lateral side wall of the posterior nasal cavity, being the most sensitive to noxious stimuli [18]. Several authors have shown specific distribution patterns of sensory immune reactivity and sensitivity within the nasal mucosa. For example, Scheibe et al. showed repeatedly that the anterior nasal septum is more sensitive to stimulation by CO2, ethyl acetate, and acetic acid compared with other locations within the nasal cavity [19]. Frasnelli et al. reported that the anterior region is more sensitive to chemical irritation, while the opposite is true for mechanical stimulation [20]. Taken together, these observations indicate that irritants entering the nasal cavity trigger a defense mechanism in the human airway. The posterior region of the nose appears to be specifically responsive to pungent and cooling agents, and the middle turbinate and septal wall to pressure and some noxious stimuli.
In summary, these studies suggest that the chemosensory system within the respiratory mucosa of the nasal cavity is not homogeneous but rather heterogeneous with various specific functions. It is not unreasonable to consider that some patients, through the irritant effect of noxious stimuli (such as perfume, smoke, gases) or a neurovascular response to a milieu of inflammatory mediators, can experience pain and a headache through trigeminal nerve receptor stimulation from inspired air or from a mucosal impaction site.
Primary Headache Disorders
Migraine
Migraine is a very common, highly disabling primary headache disorder. Attacks consist of moderate to severe pain that is often unilateral, with a throbbing or pulsating quality that is aggravated by movement. Associated symptoms, such as nausea or vomiting and autonomic dysfunction, are common and physical activity usually worsens symptoms. During migraine, most sufferers are sensitive to light (photophobia), noise (phonophobia), and odors (osmophobia). Multiple triggers, including stress, foods, weather changes, menstrual changes, or sleep changes, can lead to attacks. About 20 % of patients experience an aura involving neurologic symptoms. Visual auras are the most common [21]. Migraine has a 1-year prevalence of approximately 18 % in women and 8 % in men and is most common between the ages of 25 and 55 [22]. If the headaches occur fewer than 15 days per month, it is classified as episodic migraine; if headache occur 15 or more days per month (of which at least 8 are migraine), it is classified as chronic migraine [1]. Individuals with migraine cannot work the equivalent of 1 day per month on average, although the most disabled patients account for the majority of those on disability [23]. Patients who have a recurrent headache accompanied by nausea, light sensitivity, or any disability overwhelmingly have migraine [24].
The current accepted criteria for migraine without aura are as follows [1]:
Diagnostic criteria:
-
A.
At least five attacks fulfilling criteria B–D
-
B.
Headache attacks lasting 4–72 h (untreated or unsuccessfully treated)
-
C.
Headache has at least two of the following characteristics:
-
1.
Unilateral location
-
2.
Pulsating quality
-
3.
Moderate or severe pain intensity
-
4.
Aggravation by or causing avoidance of routine physical activity (e.g., walking or climbing stairs)
-
1.
-
D.
During headache at least one of the following:
-
1.
Nausea and/or vomiting
-
2.
Photophobia and phonophobia
-
1.
-
E.
Not attributed to another disorder
Migraine is now recognized as a neurologic disorder that is generally inherited. It is estimated that about 70–80 % of migraine sufferers have a relative with migraine [25]. Migraine and severe headaches are often underreported in first-degree relatives in family history interviews, meaning a negative family history may underestimate the true prevalence [26].
Although rhinosinusitis is common, moderate or severe headache is more likely to indicate migraine. Because migraine and other primary headaches often present with frontal, ocular, or facial pain, patients or clinicians may falsely attribute their symptoms to sinus disease. Making an accurate diagnosis reassures the patient, prevents unnecessary diagnostic testing, and allows better treatment with migraine-specific medications [27].
The ICHD-II does not recognize chronic rhinosinusitis as a cause of headache. Many patients or clinicians incorrectly diagnose primary headache disorders as “sinus headache” due to the location of their pain or the parasympathetic symptoms that accompany attacks. Eross and colleagues evaluated 100 consecutive patients with self-diagnosed sinus headache. The actual diagnoses were migraine (52 %), probable migraine (23 %), chronic migraine (11 %), other unclassifiable headaches (9 %), cluster headaches (1 %), and hemicrania continua (1 %). Only 3 % of patients could be accurately diagnosed as headache attributable to rhinosinusitis [28]. Nasal congestion was present in 73 % of patients and postnasal drip in 56 %. Most reported pain is triggered by changes in weather or season, and many noted changes with allergies or altitude, which are also common migraine triggers [29].
Orbital or retro-orbital pain, rhinorrhea, nasal congestion, miosis, lacrimation, and facial sweating are common in both primary headache disorders and rhinosinusitis. The proximity of the parasympathetic nerves to the trigeminal nerves may explain this overlap.
Cluster Headache and Other Trigeminal Autonomic Cephalalgias
Trigeminal autonomic cephalalgias (TAC) are a group of primary headache disorders characterized by unilateral headache and autonomic features. Cluster headache is the most common, with a prevalence of up to 3 per 1,000 persons [30].
The current accepted criteria for cluster headache are as follows [1]:
-
A.
At least five attacks fulfilling criteria B–E
-
B.
Severe or very severe unilateral orbital, supraorbital, and/or temporal pain lasting 15–180 min if untreated
-
C.
Headache is accompanied by at least one of the following:
-
Ipsilateral conjunctival injection and/or lacrimation
-
Ipsilateral nasal congestion and/or rhinorrhea
-
Ipsilateral eyelid edema
-
Ipsilateral forehead and facial sweating
-
Ipsilateral miosis and/or ptosis
-
A sense of restless or agitation
-
-
D.
Attacks occur from one every other day to eight per day
-
E.
Not attributed to another disorder
Unlike migraine, cluster headache is more common in men. Recent case series report the male to female ratio to be between 2.5:1 and 3.5:1. Cluster headache can begin at any age, but most commonly begins in the second to fourth decade of life. The majority of cluster headache sufferers are smokers and may be more likely to consume excessive coffee. About 4 % of patients have a family history of cluster headaches. Cluster headache is 5–18 times more common in first-degree relatives, suggesting a genetic link for the disease [31].
Cluster headache is one of the most painful conditions we see in clinical practice. The pain typically becomes maximally intense within 10 min. Attacks often occur with circadian patterns, often nocturnally starting about 1–2 h after sleep onset. This suggests a correlation with the rapid eye movement sleep stage and may be related to oxygen desaturation and obstructive sleep apnea in some patients [32]. Light and sound sensitivity are unusual, but alcohol is a common trigger for attacks. Common pain descriptors include burning, boring, or screwing. Some patients report a feeling of a “hot poker in the eye.” A minority of patients experience throbbing or pulsating pain [33]. Some patients experience fluctuations of pain during an attack, and a few experience milder head pain between attacks [34]. Cluster headache pain is typically located over the retro-orbital, supraorbital, or temporal area, but may occur in the jaw, cheek, teeth, ear, nose, or neck.
Many patients report seasonal attacks, with cycles of attacks lasting weeks to months, with periods of remission. The majority of cluster headache patients experience cycles of attacks about twice a year to every 2 years, although some patients go many years between cycles. A typical cycle lasts 1–3 months, often with a seasonal pattern, with the cycle always beginning around the same month of the year. Cluster headache attacks tend to be milder at the beginning and near the end of a cycle.
Treatment of acute cluster headaches includes sumatriptan injection and inhaled oxygen. Oxygen may work by blocking the release of inflammatory neuropeptides, including calcitonin gene-related peptide [35]. Given the frequent nature of cluster headaches, preventive treatment is usually indicated, and corticosteroids are often effective for short-term use in CH cycles.
Differentiating between migraine and cluster headache is usually straightforward, but occasionally the disorders overlap [36]. The following table reviews the distinguishing features of these two distinct diseases (Table 13.2).
Paroxysmal hemicrania is a trigeminal autonomic cephalalgia with shorter-lasting (usually 5–30 min), unilateral attacks that occur 5 or more times per day, accompanied by autonomic symptoms. The disorder resolves completely with therapeutic doses of indomethacin. Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) are very short lasting (5 s to 4 min), with orbital or frontal pain. Autonomic symptoms are usually dramatic, and patients may experience dozens or even hundreds of attacks per day. Hemicrania continua is a strictly unilateral, constant headache with milder autonomic features. Technically, hemicrania continua is not a trigeminal autonomic cephalgia, but it does have an absolute response to indomethacin [1].
Multiple case reports of secondary trigeminal autonomic cephalgias exist in the literature, and neuroimaging should be performed if any unusual features are present (Table 13.3).
A recent area of interest is the use of sphenopalatine ganglion blockade or stimulation to treat cluster headaches and other disorders characterized by headache and autonomic symptoms. Blocking the sphenopalatine ganglion after endoscopic surgery appears to improve postoperative analgesia [37]. Intranasal lidocaine has been proposed as a possible treatment of cluster headaches [38]. Stimulating the sphenopalatine ganglion may be effective in both the acute and chronic treatment of migraine and particularly cluster attacks [38–40].
Facial Pain and Trigeminal Neuralgia
Trigeminal neuralgia is a short-lasting, sharp, and distinct pain in the face, usually lasting only seconds. This shock-like pain may be precipitated by touching the affected area or by seemingly trivial stimuli, such as wind or talking. Trigeminal neuralgia is most common in elderly patients (ICHD 2004) and felt to be related to compression of the trigeminal nerve by a vascular loop in most cases [1, 41]. Secondary causes, such as multiple sclerosis and posterior fossa tumors, have been described, but sinus disease does not usually cause TN [42]. Most individuals have pain-free periods between attacks, but others have constant pain, and these patients have a worse prognosis [43]. The attacks are typically located in multiple areas with V2 and combinations such as V2 and V3 being the most common distribution.
Secondary Headaches
Headache Attributed to Sinusitis
Rhinosinusitis is a common illness characterized by nasal discharge (sometimes purulent), nasal congestion, hyposmia or anosmia, facial pain or headache worse with bending forward, fever, malaise, maxillary tooth pain, halitosis, and pain with mastication. Rhinosinusitis is divided into four categories based on the time frame and symptoms of the disease as follows:
-
Acute rhinosinusitis: One day to 4 weeks, usually viral if less than 7 days, often bacterial if >1 week, with complete resolution of symptoms
-
Recurrent rhinosinusitis: Four or more episodes of at least 7 days in a year
-
Subacute rhinosinusitis: Four to 12 weeks
-
Chronic rhinosinusitis: Signs or symptoms last more than 12 weeks
The International Classification of Headache Disorders, 2nd edition defines headache attributed to rhinosinusitis as follows [1]:
-
A.
Frontal headache accompanied by pain in one or more regions of the face, ears, or teeth, fulfilling criteria C and D.
-
B.
Clinical, nasal endoscopic, CT and/or MRI imaging, and/or laboratory evidence of acute or acute-on-chronic rhinosinusitis.
-
C.
Headache and facial pain develop simultaneously with onset or acute exacerbation of rhinosinusitis.
-
D.
Headache and/or facial pain resolves within 7 days after remission or successful treatment of acute or acute-on-chronic rhinosinusitis.
Headache location and severity, however, does not predict the presence of infection [44]. Other symptoms such as maxillary toothache are more predictive of sinusitis but less common. Hyposmia and purulent nasal discharge are strong predictors of sinus infection [45, 46].
The clinical predictors of rhinosinusitis are shown in Table 13.4.
The four major pairs of sinuses and their association with pain are as follows:
-
Maxillary sinuses: The largest sinuses, the maxillary sinuses, are present at birth and located anteriorly within the maxilla. Acute inflammation can cause pain in the cheeks, upper teeth (particularly molar), and jaw (Fig. 13.2).
Fig. 13.2 
Area of pain in acute maxillary sinusitis (Courtesy of David W. Kennedy, MD, FACS, FRCSI)
-
Ethmoid sinuses: Located between the eyes, behind the bridge of the nose, the ethmoid sinuses are present and filled with fluid at birth but become pneumatized in the first year of life. Inflammation tends to cause pain behind the eyes and nose (Fig. 13.3).
Fig. 13.3 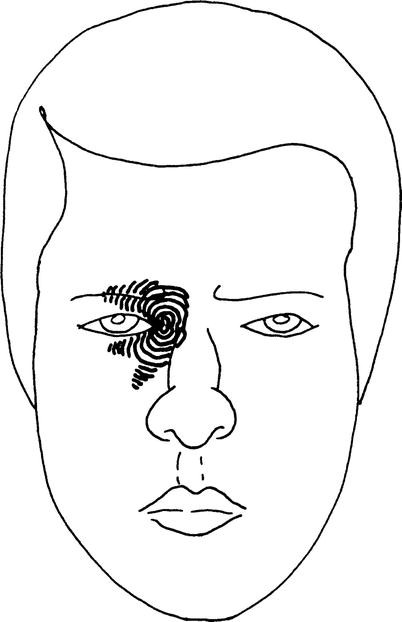
Area of referred pain in acute ethmoid sinusitis (Courtesy of David W. Kennedy, MD, FACS, FRCSI)
-
Frontal sinuses: Located above the eyes, these sinuses variably develop by about 6 years of age and can be unilateral. Inflammation may cause pain in the forehead (Fig. 13.4).
Fig. 13.4 
Areas of referred pain seen in acute frontal sinusitis (Courtesy of David W. Kennedy, MD, FACS, FRCSI)
-
Sphenoid sinuses: Located behind the eyes and nasal structures, the sphenoid sinuses are present at birth, but pneumatization does not begin until around age three. Inflammation may produce earache, deep aching at the vertex, and neck pain (Fig. 13.5). Neurologic symptoms can also be generated from the cavernous sinuses, which are lateral to the sphenoid sinus and contain the third, fourth, fifth, and sixth cranial nerves and the internal carotid arteries. Symptoms of cavernous sinus syndrome include ophthalmoplegia, proptosis, Horner syndrome, and trigeminal sensory loss. Potential causes of neurologic symptoms associated with the sphenoid sinus and cavernous sinus include infection, inflammatory disorders such as Tolosa-Hunt syndrome, vascular problems such as internal carotid artery aneurysm, trauma, and neoplasm.
Fig. 13.5 
Patterns of referred pain in acute sphenoid sinusitis (Courtesy of David W. Kennedy, MD, FACS, FRCSI)




Sphenoid Sinusitis and Its Unique Association with Headache and Other Neurologic Symptoms
Maxillary, frontal, and ethmoid sinusitis are usually associated with nasal discharge and may be diagnosed with direct examination, endoscopy, or CT scanning. Clinicians are usually able to identify most cases of acute, subacute, and chronic sinusitis. However, about 3 % of those with sinusitis have sphenoid sinusitis, which, due to its location, is difficult to diagnose clinically without radiographic or endoscopic confirmation. Symptoms such as postnasal drip or discharge are less common in sphenoid sinusitis and headache becomes more common. In a case series of 30 patients, headache was the most prominent symptom [47]. The headache of sphenoid sinusitis is often severe, with either frontal, retro-orbital, or temporal pain. Pain may radiate to the occipital or trigeminal (V1–V3) regions. Usually sphenoid sinusitis occurs with pansinusitis, but it may occur alone, causing acute or subacute headache. Mucocele and neoplasm are potential noninfectious causes of sphenoid sinus disease and should be considered in the differential diagnosis [48] (Table 13.5).
Sinus infections, especially sphenoid sinusitis, may produce serious complications when the diagnosis is missed or treatment is ineffective, leading to head pain and a variety of neurologic abnormalities depending on the location of the complication. Those serious medical conditions are summarized as follows:
-
1.
Orbital diseases (cellulitis, edema, abscess)
-
2.
Epidural or cerebral abscess
-
3.
Meningitis
-
4.
Superior sagittal sinus thrombosis
-
5.
Cavernous sinus thrombosis, ophthalmoplegia
-
6.
Pituitary insufficiency
-
7.
Mucocele (retention cyst)
Nasal or Contact Point Headache
Physicians for years have pondered on whether or not the existence of chronic headache can be due to nasal contact points on sensitive structures (Fig. 13.6). Septal deformations with a contact point on the lateral nasal wall may produce episodic or transient headache. McAuliffe et al. reported that the nasal turbinates and sinus ostia were more sensitive than the general nasal lining of the septum and sinuses [49]. These abnormalities may be ignored by radiologists and should be considered in cases of headache refractory to standard therapy. ENT evaluation may be useful, and intranasal blockade with an anesthetic such as lidocaine may confirm the diagnosis. If diagnosed correctly, removal of the contact point may improve headaches.

Schematic demonstrating the phenomenon of mucosal contact causing a pain reflex with hyperalgesia. (a) Depicts two mucosa-covered structures with intact sensory supply in close approximation but not contacting each other. (b) Demonstrates that with mucosal contact, such as by the continued pneumatization of a concha bullosa or the continued growth of a septal spur (arrows), sensory stimulation results in the transmission of an electrical signal back to the CNS (arrow heads), as well as the release of neuropeptides (such as SP) at the site of stimulation and the surrounding mucosa (shaded area). This local release of SP excites other free nerve endings and induces inflammatory changes in the mucosa
Given that these radiologic abnormalities are common in patients without headache, it is unclear if contact point headache can occur without a central disorder, such as a genetic predisposition to migraine or headache. Schønsted-Madsen et al. noted that successful surgical intervention that relieved sinus obstruction was most effective in relieving sinusitis-associated headache [50]. A lack of controlled trials makes the relationship between contract points and headache difficult to determine [51] (Figs. 13.7 and 13.8).

Left-sided septal spur (asterisk) impacting the inferior turbinate (IT) as seen with a 0° nasal telescope. Injection of the spur with local anesthesia abolished the patient’s pain, suggesting that the septum, rather than the inferior turbinate, was the cause of pain. MT middle turbinate

Left nasal contact point (arrow) in a patient with chronic migraine (Reprinted from Rozen [51]. With permission from Wolter Kluwers Health)
Low-Pressure Headache
Low-pressure headache is characterized by orthostatic head pain. The most common cause is a leak of cerebrospinal fluid (CSF), usually in the cervical spine. MRI of the brain with gadolinium is usually abnormal and suggests a CNS origin to the head pain. Other common abnormalities seen in this setting include pachymeningeal enhancement, low-lying cerebellar tonsils, subdural fluid collections, engorged pituitary and venous sinuses, and small ventricles [52, 53]. Multiple cases of CSF rhinorrhea due to nasal trauma, pituitary tumor, or iatrogenic complications of sinus surgery have been described, often with headache as a prominent symptom [54]. However, it is unclear if CSF rhinorrhea always causes orthostatic headache when present.
The primary goal of endoscopic surgery to repair CSF leaks is to prevent ascending meningitis [55]. Neuroimaging is indicated whenever CSF leak is suspected. Cisternography with nasal pledgets is useful in confirming the diagnosis. CSF leaks from the skull base producing orthostatic headache are exceedingly rare. Scheivink et al. report no cases of CSF leaks at the skull base in 273 consecutive cases at a large tertiary center [56].
Allergy and Headache
Although sinus congestion and tearing are common in migraine due to parasympathetic activation, headache in this setting is rarely related to sinus disease. In contrast, there appears to be an increased prevalence of migraine in persons with allergic rhinitis or atopy who, in turn, experience a higher frequency of sinus disease [57, 58]. Allergic rhinitis, like migraine, is an extremely common disorder that typically presents in early adulthood. Martin et al. evaluated 536 consecutive patients presenting at an allergy clinic, 174 of whom met criteria for migraine. In this group, the treatment of allergies with immunotherapy was significantly associated with less migraine frequency and disabling discomfort. This study supports some causative or influencing connection between atopic disorders and migraine headaches [59].
Conclusion
Many patients conclude that facial pain, with or without congestion, is a sinus-related event. Scientific evidence points to the exact opposite conclusion. This is particularly true for the head pain sufferer who has no direct evidence of airway inflammation and normal sinus CT imaging where the majority of such patients are found to be experiencing migraine headaches. It is important for the primary care provider to look closely for definitive signs and symptoms of sinus infection before prescribing antibiotics for a patient whose primary complaint is headache. The otolaryngologist must be cautious in associating variations in nasal structural and/or abnormal sinus CT findings of mucosal thickening as a source of an individual patient’s head pain. Though a higher proportion of atopic patients experience migraine headaches as compared to the general population, the allergist must be cautious in identifying atopic triggers as a source of head pain or suggesting that the treatment of atopic disease will resolve a head pain problem. The triggers and sources of a headache problem are potentially as heterogeneous as the neuroreceptor responses of the nasal mucosa.
References
Headache Classification Committee. The international classification of headache disorders, 2nd edition. Cephalalgia. 2004;24 Suppl 1:1–160.
Piccirillo JF. Acute bacterial sinus infections are frequently overdiagnosed. N Engl J Med. 2004;351:902–10.
Wolff HG. Wolff's headache and other head pain. 1st ed. New York: Oxford University Press; 1948.
Kelman L. The premonitory symptoms (prodrome): a tertiary care study of 893 migraineurs. Headache. 2004;44(9):865–72.
Hardebo JE, Elner A. Nerves and vessels in the pterygopalatine fossa and symptoms of cluster headache. Headache. 1987;27(10):528–32.
Clerico DM. Sinus headaches reconsidered: referred cephalgia of rhinologic origin masquerading as refractory primary headaches. Headache. 1995;35:185–92.
Dalessio DJ, Silberstein SD, editors. Wolff’s headache and other head pain. 6th ed. New York: Oxford University Press; 1993. p. 297–305.
Gershwin ME, Incaudo GA, editors. Diseases of the sinuses, a comprehensive textbook of diagnosis and treatment. 1st ed. Ottawa: Humana Press; 1996. p. 409.
Fairley JW, Yardley MPJ, Durham LH. Pressure applied to the middle turbinate causes pain at the lower threshold than the inferior turbinate or nasal septum (Abstract). Abstract book-14th Congress European Rhinologic Society, Rome; 6–10 Oct, 1992. p. 96.
Eccles R, Lancashire B, Tolley NS. Experimental studies on nasal sensation of airflow. Acta Otolaryngol. 1987;103:303–6.
Sekizawa S, Tsubone H, Kuwahara M, Sugano S. Nasal receptors responding to cold and l-menthol airflow in the guinea pig. Respir Physiol. 1996;103:211–9.
Torebjork HE, Hallin RG. Perceptual changes accompanying controlled preferential blocking of A and C fibre responses in intact human skin nerves. Exp Brain Res. 1973;16:321–32.
Doty RL. Intranasal trigeminal detection of chemical vapors by humans. Physiol Behav. 1975;14:855–9.
Doty RL, Brugger WE, Jurs PC, Orndorff MA, Snyder PJ, Lowry LD. Intranasal trigeminal stimulation from odorous volatiles: psychometric responses from anosmic and normal humans. Physiol Behav. 1978;20:175–85.
Silver WL, Moulton DG. Chemosensitivity of rat nasal trigeminal receptors. Physiol Behav. 1982;28:927–31.
Stevens JC, Cain WS. Aging and the perception of nasal irritation. Physiol Behav. 1986;37:323–8.
Handwerker H, Kobal G. Psychophysiology of experimentally induced pain. Physiol Rev. 1993;73:639–71.
Meusel T, Negoias S, Scheibe M, Hummel T. Topographical differences in distribution and responsiveness of trigeminal sensitivity within the human nasal mucosa. Pain. 2010;151(2):516–21.
Scheibe M, van Thriel C, Hummel T. Responses to trigeminal irritants at different locations of the human nasal mucosa. Laryngoscope. 2008;118:152–5.
Frasnelli J, Heilmann S, Hummel T. Responsiveness of human nasal mucosa to trigeminal stimuli depends on the site of stimulation. Neurosci Lett. 2004;362:65–9.
Silberstein SD. Migraine symptoms: results of a survey of self-reported migraineurs. Headache. 1995;35:387–96.
Lipton RB, Bigal M, Diamond M. Migraine prevalence, disease burden and the need for preventive therapy. Neurology. 2007;68:343–9.
VonKorff M, Stewart WF, Simon DS, Lipton RB. Migraine and reduced work performance: a population-based diary study. Neurology. 1998;50:1741–5.
Lipton RB, Kolodner K, Dodick D et al. A self-administered screener for migraine in primary care: the ID migraine validation study. Headache 2003;43 (abstract).
Russell MB. Genetic epidemiology of migraine and cluster headache. Cephalalgia. 1997;17:683–701.
Ottman R, Hong S, Lipton RB. Validity of family history data on severe headache and migraine. Neurology. 1993;43:154–96.
Silberstein SD, Lipton RB. Overview of diagnosis and treatment of migraine. Neurology. 1994;44 suppl 7:6–16.
Eross E, Dodick D, Eross M. The Sinus, Allergy and Migraine Study (SAMS). Headache. 2007;47(2):213–24.
Chabriat H, Danchot J, Michel P, Joire JE, Henry P. Precipitating factors of headache. A prospective study in a national control-matched survey in migraineurs and nonmigraineurs. Headache. 1999;39(5):335–8.
Sjaastad O, Bakketeig LS. Cluster headache prevalence. Vaga study of headache epidemiology. Cephalalgia. 2003;23(7):528–33.
Russell MB. Epidemiology and genetics of cluster headache. Lancet Neurol. 2004;3(5):279–83.
Kudrow L, McGinty DJ, Phillips ER, Stevenson M. Sleep apnea in cluster headache. Cephalalgia. 1984;4:33–8.
Donnet A, Lanteri-Minet M, Guegan-Massardier E, et al. Chronic cluster headache: a French clinical descriptive study. J Neurol Neurosurg Psychiatry. 2007;78(12):1354–8.
Marmura MJ, Silberstein SD. Current understanding and treatment of headache disorders: five new things. Neurology. 2011;76(7 Suppl 2):S31–6.
Goadsby PJ, Edvinsson L. Human in vivo evidence for trigeminovascular activation in cluster headache. Brain. 1994;117:427–34.
Peatfield R. Migrainous features in cluster headache. Curr Pain Headache Rep. 2001;5(1):67–70.
DeMaria Jr S, Govindaraj S, Chinosorvatana N, Kang S, Levine AI. Bilateral sphenopalatine ganglion blockade improves postoperative analgesia after endoscopic sinus surgery. Am J Rhinol Allergy. 2012;26(1):e23–7.
Bakbak B, Gedik S, Koktekir BE, Okka M. Cluster headache with ptosis responsive to intranasal lidocaine application: a case report. J Med Case Rep. 2012;6:64.
Ansarinia M, Rezai A, Tepper SJ, et al. Electrical stimulation of sphenopalatine ganglion for acute treatment of cluster headaches. Headache. 2010;50(7):1164–74.
Oomen KP, van Wijck AJ, Hordijk GJ, de Ru JA. Effects of radiofrequency thermocoagulation of the sphenopalatine ganglion on headache and facial pain: correlation with diagnosis. J Orofac Pain. 2012;26(1):59–64.
Love S, Coakham HB. Trigeminal neuralgia: pathology and pathogenesis. Brain. 2001;124(Pt 12):2347–60.
Zakrzewska JM. Diagnosis and differential diagnosis of trigeminal neuralgia. Clin J Pain. 2002;18(1):14–21.
Szapiro Jr J, Sindou M, Szapiro J. Prognostic factors in microvascular decompression for trigeminal neuralgia. Neurosurgery. 1985;17(6):920–9.
Gupta M, Silberstein SD. Therapeutic options in the management of headache attributed to rhinosinusitis. Expert Opin Pharmacother. 2005;6(5):715–22.
Cady RK, Dodick DW, Levine HL, et al. Sinus headache: a neurology, otolaryngology, allergy, and primary care consensus on diagnosis and treatment. Mayo Clin Proc. 2005;80(7):908–16.
Houser SM, Levine HL. Chronic daily headache: when to suspect sinus disease. Curr Pain Headache Rep. 2008;12(1):45–9.
Lew D, Southwick FS, Montgomery WW, Weber AL, Baker AS. Sphenoid sinusitis: a review of 30 cases. N Engl J Med. 1983;19:1149–54.
Levine HL, Setzen M, Cady RK, et al. An otolaryngology, neurology, allergy, and primary care consensus on diagnosis and treatment of sinus headache. Otolaryngol Head Neck Surg. 2006;134(3):516–23.
McAuliffe GW, Goodell H, Wolff HG. Experimental studies on headache: pain from the nasal and paranasal structures. Res Publ Assoc Res Nerv Ment Dis. 1943;23:185–206.
Schonsted-Madsen U, Stoksted P, Christensen PH, Koch-Henriksen N. Chronic headache related to nasal obstruction. J Laryngol Otol. 1986;100:165–70.
Rozen TD. Intranasal contact point headache: missing the “point” on brain MRI. Neurology. 2009;72(12):1107.
Spelle L, Boulin A, Tainturier C, Visot A, Graveleau P, Pierot L. Neuroimaging features of spontaneous intracranial hypotension. Neuroradiology. 2001;43(8):622–7.
Mokri B, Bahram MD. Spontaneous cerebrospinal fluid leaks: from intracranial hypotension to cerebrospinal fluid hypovolemia–evolution of a concept. Mayo Clin Proc. 1999;74(11):1113–23.
Makin V, Hatipoglu B, Hamrahian AH, et al. Spontaneous cerebrospinal fluid rhinorrhea as the initial presentation of growth hormone-secreting pituitary adenoma. Am J Otolaryngol. 2011;32(5):433–7.
Daele JJ, Goffart Y, Machiels S. Traumatic, iatrogenic, and spontaneous cerebrospinal fluid (CSF) leak: endoscopic repair. B-ENT. 2011;7 Suppl 17:47–60.
Schievink WI, Schwartz MS, Maya MM, Moser FG, Rozen TD. Lack of causal association between spontaneous intracranial hypotension and cranial cerebrospinal fluid leaks. J Neurosurg. 2012;116(4):749–54.
Ku M, Silverman B, Prifti N, Ying W, Persaud Y, Schneider A. Prevalence of migraine headaches in patients with allergic rhinitis. Ann Allergy Asthma Immunol. 2006;97(2):226–30.
Mortimer MJ, Kay J, Gawkrodger DJ, Jaron A, Barker DC. The prevalence of headache and migraine in atopic children: an epidemiological study in general practice. Headache. 1993;33(8):427–31.
Martin VT, Taylor F, Gebhardt B, et al. Allergy and immunotherapy: are they related to migraine headache? Headache. 2011;51(1):8–20.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Marmura, M.J., Silberstein, S.D. (2014). Headache and Sinonasal Disease. In: Chang, C., Incaudo, G., Gershwin, M. (eds) Diseases of the Sinuses. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0265-1_13
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0265-1_13
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-0264-4
Online ISBN: 978-1-4939-0265-1
eBook Packages: MedicineMedicine (R0)