
Abstract
Technosphere® is an innovative technology developed by MannKind Corporation for drug delivery through the pulmonary route. Mainly composed of an inert excipient, fumaryl diketopiperazine, the microparticles rapidly dissolve in the lung lining fluid, permitting a rapid drug release and providing a fast onset of action. Additionally, the excipient is also rapidly cleared from the lung and excreted in urine, thus contributing for the safety profile of the system. Several drugs are currently being tested using this technology, with insulin and glucagon-like peptide 1 being in clinical trials. In this chapter, the characteristics and abilities of Technosphere® will be fully presented, the capacity to act as inhalable drug carrier examined and the safety profile analyzed. Additionally, interesting studies regarding the patients and physicians perceptions will be described. As a whole, it is intended to provide a comprehensive view of Technosphere® properties and achievements, identifying possible limitations still to overcome.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Biopharmaceuticals
- Fumaryl diketopiperazine
- Glucagon-like peptide 1
- Insulin
- Pulmonary delivery
- Technosphere®
1 Introduction
The lung has been explored for a long time for biopharmaceutical administration, one of the oldest reports dating back to 1924 and referring to inhaled insulin [1]. The advantages of this route for systemic drug delivery are well known, including the large alveolar surface available for absorption, the very thin diffusion path to the bloodstream, the extensive vascularization, the relatively low metabolic activity and the possibility to avoid hepatic first-pass effect [2–4]. However, several limitations have to be considered as well, mainly related with the sinuous architecture of the lung tree that impairs particle flowing, the reduced amount of liquid for drug dissolution and diffusion, and specific defense mechanisms like the mucociliary clearance [3, 5]. A more detailed description of these considerations can be found in Chap. 7, which is fully dedicated to pulmonary delivery of biopharmaceuticals.
Notwithstanding its promising characteristics, systemic pulmonary delivery of drugs is not an established approach. This is due not only to the difficulty in designing adequate drug carriers that overcome the referred limitations, reaching the alveoli successfully and in sufficient amount, but also to the safety concerns raised by the alveolar deposition of drugs, particularly when chronic administration is considered.
In summary, designing adequate carriers for systemic pulmonary delivery demands addressing key considerations related with aerodynamic properties, the ability to provide complete drug release in reduced amount of liquid and, above all, the safety of the drug carrier. In the following sections, the details on how Technosphere® technology met these requirements will be described.
2 The Technosphere® System
Developing inhalable dry powders demands meeting several requirements, not only regarding the difficulties posed by the lung defense mechanisms and airway structure, but also addressing issues related with drug release and stability . An ideal particle engineering technology should permit working on a wide size range to accommodate several therapies which, in turn, also requires an application to different molecules, such as small drugs and large biopharmaceuticals. Additionally, drug pharmacokinetics should be adequate, the involved excipients eliminated and, finally, the technology should be scalable and cost effective.
The Technosphere® technology is a registered trademark of MannKind Corporation and was developed to meet all these requirements. It comprises microparticles mainly composed of fumaryl diketopiperazine (FDKP) , an excipient that is also property of that company, while residual amounts of Tween 80®are further included [6–9]. FDKP is a derivative of diketopiperazines, a group of small cyclic dipeptides commonly found in natural products [10]. They are advantageous in comparison with linear peptides , namely regarding the stability to proteolysis, conformational rigidity, and the promotion of interactions with biological targets by hydrogen bonding mediated by donor and acceptor groups [11]. The latter characteristic is of major importance, because hydrogen bonds are the driving force for the preparation of Technosphere® particles. In fact, FDKP (bis-3,6(4-fumarylaminobutyl)-2,5-diketopiperazine) is a fumaramide derivative of diketopiperazine (Fig. 22.1) that self-assembles into larger constructs by means of intermolecular hydrogen bonding, as described for diketopiperazine-based molecules [12–13]. It was actually identified as the derivative providing the optimal properties for the self-assembly into microspheres , justifying its selection [14]. The self-assembly occurs at acidic pH (< 5.2) [7, 15] in a process that is thought to be mediated either by the carboxylic acid or the amide groups [14]. A deep analysis of the molecular events governing the self-assembly of FDKP is available in [14].

Chemical structure of fumaryl diketopiperazine
Depending on the method used to process FDKP for obtaining the microparticles , the final carriers can be either crystalline or amorphous. The morphological differences between the two types of microparticles are intense (Fig. 22.2). In a publication authored by MannKind scientists, a curious morphological description of the crystalline microparticles was provided, referring that “the particle can be envisioned as a three-dimensional sphere constructed from a deck of playing cards. Each card represents a FDKP nanocrystal and the sphere constructed from the cards represents a Technosphere particle” [16]. The preparation of these crystalline microparticles occurs in solution and involves the formation of FDKP nanocrystals in a controlled, pH-dependent crystallization, followed by the self-assembly of the nanocrystals into microparticles [6, 16]. The incorporation of the drugs occurs by mixing with the excipient solution during the precipitation process, resulting in the adsorption to the nanocrystal surface [6, 17]. Amorphous particles are, in turn, obtained by spray-drying . A salt of FDKP is mixed with the drug and the resultant microparticles are a homogeneous composite of both components [16].

Technosphere® crystalline particle (left) and amorphous particle (right). Average particle size is about 2 µm in diameter. (Images gently provided by MannKind Corporation)
In both cases the particles are monodisperse and exhibit high porosity, thus resulting in low density and suitable aerodynamic properties for deep lung deposition [16]. This aspect appears as a real advantage of Technosphere® , as most standard inhalable dry powder formulations consist of saccharides blended with micronized drug powders, frequently resulting in final heterodisperse particles [18]. The aerodynamic diameter of microparticles ranges between 2 and 2.5 µm [6, 19], more than 90 % being in the respirable size range (0.5–5.8 µm) [6–7].
The Technosphere® engineering technology has been reported as highly versatile, permitting the production of small particles for deep lung inhalation or larger particles for deposition in the upper airways [20]. An optimization of the process parameters is reported as sufficient to endow the microparticles with a preselected size [16]. Therefore, upon formation of either type of microparticles (crystalline or amorphous), no further processing is necessary for size modulation. A final process of freeze-drying is applied to crystalline particles to endow the dry powders with the most suitable properties for inhalation via a small inhaler device [15, 21].
Bearing in mind that this technology was developed to provide systemic lung delivery, aerodynamic suitability provides the guarantee that most of the emitted dose will reach the alveolar zone. However, a problem remains to be solved regarding the release of the drug. As referred before, the amount of lung lining fluid is very small and ensuring drug release and dissolution might be a challenge. Technosphere® has been described to meet this challenge in a very positive manner. In fact, FDKP is highly soluble at pH values above 6 [7, 16]. Therefore, as the pH of alveolar lung lining fluid is approximately 7 [22–23], Technosphere® particles dissolve rapidly upon reaching the alveolar zone, releasing the drug in a complete manner [17]. A complete scheme on Technosphere® drug carrier is available in Fig. 22.3.

Technosphere® drug carrier: mechanism of particle formation and behavior upon administration. (Microparticle image gently provided by MannKind Corporation)
The dissolution profile of inhaled Technosphere® drugs is reported to be very fast, so that their pharmacokinetic profile closely resembles that of intravenous (IV) injection [16, 24], depending on the proper capacity of the drug to dissolve in the lung environment. Absorption begins almost immediately after inhalation and circulating drug concentrations peak within minutes of administration [7]. In vitro studies performed in Calu-3 cells (bronchial cell line) [19] and in vivo in rats [6] revealed that FDKP does not act as permeation enhancer, the rapid drug absorption being attributed to both FDKP and drug dissolution profile.
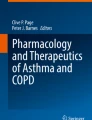
This characteristic of FDKP also contributes for a rapid elimination. FDKP has a plasmatic half-life of 190 min in diabetic patients with normal renal function [6], being cleared from the lung lining fluid with a half-life of approximately 1 h [7]. Similar results were reported in other studies, with FDKP t max determined 10–15 min after dosing [18, 25], as depicted in Fig. 22.4. Altogether, these results describe a very important feature of FDKP, largely contributing for its safety.

Serum insulin and fumaryl diketopiperazine concentrations vs. time (mean ± SE; n = 12). (Reprinted from [7] with kind permission from Springer Science+Business Media)
Although developing inhalation dry powders is known as a challenging task, MannKind appears to have addressed most of the key considerations to be successful with the use of FDKP to produce Technosphere® microparticles . In summary, Technosphere® is a drug carrier technology with simple assembly, suitable aerodynamic properties for deep lung inhalation , permitting a rapid release and, thus, absorption of the carried drugs.
3 Different Drugs for the Same Carrier
Technosphere® is a versatile technology, permitting the association of molecules with distinct properties, namely concerning their molecular size. Small molecules such as felbamate (238 Da) [26] or biopharmaceutical drugs, such as insulin [7], glucagon-like peptide 1 [18], or parathyroid hormone [27] (molecular weight 4–6 kDa), were successfully associated to the microparticles. Felbamate-loaded Technosphere® microparticles [26] were only reported for IV administration and, therefore, will not be further analyzed.
Insulin was the first biopharmaceutical drug to be approached in the context of inhalation and is the most studied. Technosphere® insulin is currently in Phase III clinical trials and Sect. 4 provides a complete overview of the formulation. Technosphere® glucagon-like peptide 1 (GLP-1) is also in Phase I clinical trials for the treatment of diabetes [6], with several reports providing the related data. Parathyroid hormone, oxyntomodulin , peptide YY , atropine, monoclonal antibodies, and bacterial antigens are other molecules that have been formulated in Technosphere® microparticles . However, while data on the former can be found in the literature [27], the others have been mentioned to be tested nonclinically [6] or are only mentioned in a patent [28], no data being available.
Parathyroid hormone (PTH) is a regulator of calcium homeostasis, with a function in maintaining serum calcium levels [29]. When calcium concentration decreases, PTH is secreted and calcium is mobilized from skeletal stores [30]. This makes PTH an unlikely agent for treating osteoporosis, but its intermittent administration has demonstrated to induce bone formation more than bone reabsorption, at least in the first 12 months of therapy [31]. PTH-mediated bone rebuilding in osteoporosis needs rapid absorption and elimination, as prolonged exposure can induce bone loss. Therefore, the pulmonary administration of PTH using Technosphere® is an appealing alternative to the current subcutaneous (SC) injection, as it theoretically meets that important requirement. A study on ten healthy subjects demonstrated a faster and higher increase in PTH (1–34) concentrations resulting from pulmonary as compared with SC administration. The inhalation of 1,600 IU of Technosphere®/PTH (1–34) elicited much lower t max compared to SC injection of 400 IU PTH (1–34) (10 min vs. 29 min), with 48 % relative bioavailability of pulmonary PTH (1–34) for 6 h. Cmax was also much higher upon pulmonary administration (309 pM vs. 102 pM) [27]. This is the only published study on the formulation, perhaps the peak-like pharmacokinetic profile of Technosphere®/PTH (1–34) revealed to have different effects on bone metabolism as compared with the parenteral administration.
GLP-1 is the second molecule integrating a Technosphere®-based formulation undergoing Phase I clinical trials. Secreted at the gastrointestinal tract, it stimulates insulin secretion by pancreatic β-cells after meals and is further involved in the regulation of glucagon release and gastrointestinal motility [32–33]. Very importantly, studies performed in rodents evidenced the ability of GLP-1 to stimulate β-cell growth and replication [34]. Altogether, these effects suggest a broad role of GLP-1 as mediator of postprandial glucose homeostasis and as a potential enhancer of β-cell functioning, with important therapeutic potential in type 2 diabetes. Its utility is somewhat hindered by both a very short circulating half-life (≈ 2 min) and the need for injection [35]. The adequate GLP-1 therapy has been described as one in which the drug is administered at mealtime with exposure limited to the postprandial period [18], thus mimicking its physiological pattern, reaching peak levels soon after a meal and rapidly rising insulin concentration [36]. Inhaled Technosphere® GLP-1 might comply with this requirement. A preliminary study in rats, administered a single inhaled dose, revealed a 5–10 min t max, 10–15 min t 1/2 and reduced food intake [18]. A single Phase I clinical trial is available, enrolling 26 healthy normal subjects and 20 type 2 diabetic subjects. Inhaled GLP-1 produced peak plasmatic concentrations within 5 min in both groups, leading to insulin peak at 10–15 min. GLP-1 returned to baseline within 30 min. Interestingly, subjects in the fasting state, whether healthy or diabetic, registered a decrease of insulin levels to baseline at 30–40 min, whereas diabetic subjects who had eaten a meal showed meal-stimulated insulin levels for several hours. Low bioavailability was estimated (0.5–1.6 %) due to both a low fraction of drug entering the lungs, as the inhaler was not specifically adapted to the formulation, and to the activity of dipeptidyl peptidase-4 present in the lungs and lung vasculature [36]. Generally, it was concluded that the inhalation of GLP-1 Technosphere® in type 2 diabetes patients produced a rapid and transient secretion of insulin that mimics the first-phase response of healthy subjects, restraining typical early glucose postprandial excursions.
As previously mentioned, GLP-1 also has a function on the regulation of gastrointestinal motility. A synthetic GLP-1 analog (ROSE-010) modified to protect against dipeptidyl peptidase-4 proteolytic action [37], evidenced the ability to relax intestinal smooth muscle and relieve pain associated with irritable bowel syndrome in preclinical and clinical assays [38]. A study of ROSE-010 Technosphere® inhaled by a rat model of the disease showed comparable reduction of intestinal motility as IV/SC injections. The effect was found similar to that of normal endogenous GLP-1 [37], evidencing the potential of ROSE-010 Technosphere® to be used as an alternative treatment of irritable bowel syndrome patients.
4 Technosphere® Insulin: An Effective Case-Study
Insulin therapy is a broad commercial hit as type 1 diabetes mellitus patients are totally dependent on the protein and, in parallel, the increasing prevalence of type 2 diabetes mellitus and the fact that people are being diagnosed at an early age, indicates that many of these patients will also develop severe insulin deficiency owing to pancreatic β-cell loss over time. Technosphere® insulin is, therefore, the most advanced of the Technosphere® drugs, not only because of the relevant market, but also because it is expected to attain good patient acceptance, eliminating/decreasing the need for regular uncomfortable injections.
Technosphere® insulin is a dry powder formulation of recombinant human insulin, predominantly composed of insulin and FDKP (1:9, w/w) under the form of crystalline microparticles [7], which is proposed for type 1 and type 2 diabetes treatment under the commercial name of Afrezza®. Available studies were mostly performed in type 2 diabetes patients, as the first Phase III clinical trial on type 1 diabetes patients has finished very recently (May 2013) [39]. The main characteristic of the formulation is perhaps to provide short insulin t max (10–15 min, Fig. 22.4) [21, 24–25, 40–41], closely resembling the normal physiological profile of prandial insulin [42]. Moreover, it provides about 60 % of its glucose lowering effect within 3 h post administration [25]. This pharmacokinetic profile, which is also exhibited in patients with chronic obstructive pulmonary disease [43], is consistent with 2-compartment disposition, as reported for IV/SC administration [44], suggested an application as ultra-rapid-acting prandial insulin, addressing the synchronization between the postprandial action of prandial insulin and the postprandial glucose, thus reducing the incidence of hyperglycemia and hypoglycemia [21]. This allows patients to inhale a dose 5–10 min before a meal, instead of injecting insulin 20–30 min ahead. In comparison, Technosphere® insulin has better pharmacokinetic profile than other inhaled insulin formulations, which provide 50–65 min t max [42, 45–49], while SC insulin has worst performance (t max ≈ 120–140 min) [25, 40, 42], leading to less than 30 % of the total hypoglycemic effect occurring in the first 3 h [25]. This endows the SC formulation with several drawbacks. Particularly, as peak levels usually appear after the meal is already digested, there is a high risk of hypoglycemia, frequently demanding the intake of a preventive snack, apart from very strict treatment regimens [25, 50]. Nevertheless, inhaled insulin is probably less efficient than SC insulin, involving insulin loss within the inhaler and mouth during inhalation [42]. In this context, several studies have reported the relative bioavailability of inhaled insulin to be around 20–30 % [24, 41, 51]. Furthermore, it could also be assumed that pulmonary absorption is more regular than SC, as many parameters affecting the latter are not to be considered in the lung , such as the variable amount of fat, the injection site containing or not connective tissue, and the depth. However, comparing the administration of Technosphere® insulin and SC, regular human insulin in 13 type 2 diabetes patients, revealed a lower (but not statistically significant) intra-subject variability in Technosphere® insulin pharmacokinetic parameters during the first 3 h and significantly higher between subject variability. No significant differences were observed at pharmacodynamic parameters [25].
The first Phase I clinical study with Technosphere® insulin involved 5 nonsmoking healthy volunteers and compared the administration of 100 IU inhaled regular human insulin with that of 5 IU given by IV route and 10 IU by SC route, using euglycemic glucose clamp procedure. It was demonstrated for the first time that this inhaled insulin formulation elicited a very rapid rise of insulin levels (t max at 13 min as compared with 120 min for SC), similar to that observed upon IV administration. The corresponding maximal metabolic effect on glucose occurred more than 2 h earlier with inhaled insulin, with a return to baseline within 3 h. Importantly, the insulin area under-the-curve (AUC) for this period was more than twice as high as those for IV and SC injection [24]. This first study used a commercially available inhaler, but it was soon identified that an improved performance would require a specifically designed device. MannKind then developed a specific inhaler for the Technosphere® technology (MedTone®) , which provides a mean emitted dose of 65 % [7], being used in subsequent studies. The ability to improve glycemic control at mealtime was demonstrated in a meal-challenge study involving 16 nonsmoking type 2 diabetes subjects (administered 48 IU Technosphere® insulin or 14 IU SC regular human insulin), where blood glucose AUC0−240 of inhaled insulin was ≈ 52 % that of SC insulin. Total serum insulin exposure was almost identical in both treatments [40]. Importantly, it was verified that, when selecting an optimized dose of inhaled insulin, patients could ingest meals with variable carbohydrate content or skip meals without severe hypoglycemia. This is the main result of a study evaluating eight type 2 diabetes patients taking Technosphere® insulin (dose of 15 UI or 30 UI, optimized for each subject) with a meal of different carbohydrate content (0, 50, 200 %). Postprandial glucose excursions were determined to be minimal for 0 and 50 % carbohydrate content meals. The meal adjusted to 200 % registered moderate increase of glucose, in any case below American Diabetes Association targets. Additionally, a general decrease of HbA1c around 1.6 % was observed [52].
A first study opposing Technosphere® insulin to placebo Technosphere® demonstrated that the active formulation strongly decreased glycated hemoglobin (HbA1c) , reduced postprandial glucose excursions by 56 % as compared with baseline and maximal postprandial glucose levels by 43 % as compared with placebo. This study enrolled 126 insulin-naïve type 2 diabetes patients suboptimally controlled with oral agents for a total of 12 weeks [53]. It was further demonstrated that the metabolic activity induced by Technosphere® insulin is dose-dependent. Using the euglycemic glucose clamp technique, 11 healthy subjects received three different doses (25, 50, and 100 IU) on three different days. The doses resulted in insulin peaks at 42, 50, and 58 min, respectively, which occurred 2 h earlier than upon SC injection (10 IU). Over the first 3 h, the relative bioavailability was 36, 35, and 32 %, respectively [41]. Comparable results were reported in a similar study [54]. A more prolonged study (11 weeks) tested the dose-response of four Technosphere® insulin doses (14, 28, 42, and 56 IU) on 227 type 2 diabetes patients with inadequate glycemic control. Inhaled insulin was administered daily before each of three meals, in combination with insulin glargine. Technosphere® insulin demonstrated to induce statistically significant dose-dependent reduction of HbA1c, whether versus baseline or placebo (Technosphere® powder alone). Inhaled insulin generally decreased the postprandial maximum glucose concentration (except for the lowest dose) and reduced significantly the postprandial glucose AUC for the two higher doses [55].
Considering the fact that most patients will require the administration of Technosphere® insulin along with other insulin formulations, testing combined effects is important. A one-year study involving 485 type 2 diabetes patients established a group administering prandial inhaled insulin plus SC insulin glargine at bedtime, and another group consisting twice daily SC premixed biaspart insulin. Changes in HbA1c were similar in both groups, but patients from the group of Technosphere® insulin registered a significantly lower weight gain and fewer mild-to-moderate and severe hypoglycemic events [51].
Although the pharmacological efficacy of Technosphere® insulin has been demonstrated, many scientists and physicians are still skeptic about its use. This is mainly due to the issue of insulin accumulation in lung tissue , and the continuous inhalation of a powder, which might compromise common lung functions. Several clinical studies addressed these concerns, evaluating the clearance of the formulation and testing distinct parameters of pulmonary function. The administration of 99mTc-radiolabelled particles to five healthy volunteers revealed that 60 % of the emitted dose reaches the lung (remainder is swallowed), distributing homogeneously to both lung sides. A bronchoalveolar lavage (BAL) study demonstrated that inhaled insulin is rapidly cleared from the lung, with undetectable concentrations after 12 h. Clearance half-life was determined to be ≈ 1 h [7].
All studies on pulmonary function reported acceptable results, with only minimal changes observed upon treatment with inhaled insulin, which were not statistically different from those observed in other test groups. The most usual adverse effect was cough, in which intensity decreases with treatment continuation [7, 24, 55]. One particular study tested the effects on specific parameters of pulmonary function (forced expiratory volume for 1 s, forced vital capacity , total lung capacity and lung diffusion capacity for carbon monoxide) over 2 years. Results from 910 subjects indicated that the evolution of pulmonary function was similar for patients (either with type 1 or type 2 diabetes) using prandial inhaled insulin or usual care (oral antidiabetics or SC insulin). The lung function actually declined in both groups through the study period, showing a tendency for lung function decline associated with diabetes, in which underlying mechanism remains unclear [56].
One important aspect of using inhaler devices is being trained on their use and having the necessary physiological ability to use with maximum benefit. As referred above, after using a commercially available inhaler in the first tests, MannKind developed its proper inhaler MedTone® to be used with the Technosphere® technology. It was demonstrated to work properly in a study with 56 type 1 and type 2 diabetes subjects who have shown to provide the necessary inspiratory effort for Technosphere® insulin inhalation [57]. However, MannKind has developed a second-generation inhaler for Affreza®, called DreamBoat® (Fig. 22.5), which is smaller and uses a lower dose compared with MedTone® [58].

Dreamboat® dry powder inhaler. (Images gently provided by MannKind Corporation)
In summary, it was evidenced by the described assays that Technosphere® insulin generally provides a better glycemic control than other formulations, resulting in lower weight gain and less hypoglycemic events. Therefore, it is taking the forefront for commercialization.
5 Technosphere® Insulin from the Patient Perspective
Improving quality of life is the ultimate goal of any therapeutic regimen. Therefore, perceiving patient reactions to medication is essential, as the patient must be truly committed to enable therapeutic success. After the failure of Exubera® it became very important to address these concerns cautiously, as several reports indicated the inability of the patients to use the inhaler or their discomfort in handling a cumbersome device [59–60]. Some works evaluate type 2 diabetes patients’ perceptions of inhaled insulin therapy effect on health-related quality of life and treatment satisfaction, using a measure of health-related quality of life (SF-36) and the Inhaled Insulin Treatment Questionnaire [61], which were filled before and after treatment. The latter measure assesses diabetes worries, perceptions of insulin therapy, and inhaler performance. One study compared insulin-naïve subjects (119) receiving inhaled Technosphere® insulin or placebo Technosphere® formulation, revealing that perceptions of insulin therapy were significantly more positive after using Technosphere® insulin. Participants on this arm reported no negative impacts on quality of life or worries about diabetes, attitude improvement toward insulin therapy, and satisfaction associated with the inhaler device. The only negative aspect regarding the inhaler was related with the difficulty in evaluating cartridge emptiness [62]. Another study compared patients (618) taking Technosphere® insulin in combination with basal insulin glargine with those taking premixed biphasic rapid-acting insulin 70/30. The decrease in HbA1c was similar in both groups but, with similar overall glucose levels among groups, patients in the Technosphere®/glargine arm had significantly lower weight gain. The same was observed for the incidence of hypoglycemia. Diabetes worries declined significantly in the group taking Technosphere® insulin and glargine, whose participants also reported no negative impacts on quality of life, while perceptions of insulin therapy, treatment satisfaction, and treatment preference improved in both arms of the study [63]. The same authors also addressed the perceptions of both diabetic patients and physicians regarding the use of inhaled insulin. An internet survey, in which 1,094 American patients participated, suggested they evaluate diabetes medications primarily in terms of the ability to control postprandial hyperglycemia and reduce discomfort and inconvenience [64]. The same methodology was used to register the opinion of 602 physicians who treat diabetic adults. Physicians who self-identified as medical innovators or who reported high levels of involvement with patients, tended to rate the inhaled insulin higher. In contrast, those who self-identified as diabetes experts or who avoided using insulin, tended to attribute a lower rate. Interestingly, family physicians were most likely and endocrinologists least likely to say they would recommend inhaled insulin for a variety of patient profiles [60]. The conditions for a patient appealing therapeutic are apparently guaranteed.
6 Safety Concerns of Technosphere®
The withdrawal of Exubera® (Pfizer) and the possibility that it may have been associated with safety reasons, namely lung cancer , has hampered the development and licensing of protein-containing formulations intended for inhalation. Exubera® was only available for a short period (August 2006 to October 2007) and was withdrawn because of cost and bulky device [58]. Nevertheless, this formulation was reported to cause cough, dyspnea, increased sputum, and epistaxis [65]. Although patient satisfaction was higher with inhaled insulin compared with SC injections, regular lung function tests are needed because long-term safety has not been established [66]. The safety reasons that may have been involved pertain mainly to the chronic exposure of the alveolar epithelium and underlying connective tissue to biologically active insulin [67]. Insulin acts as a weak growth factor by binding to the IGF-1 receptor, which raises serious safety concerns [1]. The association of inhaled insulin with small, consistent reductions in lung function has been shown [68], while it was also reported that inhaled insulin rapidly aggregates at the lung air-tissue interface, forming amyloid structures causing a significant reduction in pulmonary air flow [69]. In addition, the role of the lung as immunological organ and the consequences of a chronic deposition of inhaled proteins in the lung epithelium are not fully understood. Therefore, we tend to agree when Bailey and Barnett [67] state “proceed with caution”.
The Technosphere® system has been proposed for inhaled insulin and was submitted to the FDA in 2009 as a New Drug Application, under the trade name Afrezza® . It has shown an acceptable safety profile in the clinical development, overcoming some drawbacks that contributed to the demise of Exubera® [51, 53, 56]. From a technological perspective, the FDKP self-assembly process for microsphere assembly has the advantage of avoiding the use of organic solvents while using mild formulation conditions compatible with protein stability . As aforementioned, after administration the particles dissolve rapidly in the alveolar pH-neutral environment and readily liberate insulin for systemic absorption [70–72]. FDKP is not metabolized, being excreted in urine as ammonium salts within hours of administration [6–7].
The in vivo fate of pulmonary delivered particulate systems depends on their composition and physicochemical characteristics. The uptake by lung macrophages and translocation across respiratory epithelia, either to the systemic circulation or lymphatic circulation, depend on particle size, charge, and hydrophobicity [73–74]. Moreover, inhaled micro- and nanoparticles may influence drug absorption by controlling the release and retaining the drug within the lungs [3, 74–75]. The rapid dissolution of FDKP microspheres is most probably the key for the success of Technosphere® , including its safety. After particle dissolution and protein release, the in vivo fate of the latter depend on its physicochemical properties rather than formulation parameters. The same applies to protein toxicity within the lung compartment. However, as a novel excipient, FDKP microspheres will have to comply with harsh regulatory demands, including full details of manufacture, characterization and controls with cross references to supporting safety, including data concerning toxicology according to the dosage form and the route of administration of the medicinal product. The information should provide the same level of detail as that provided for a drug substance [76–78]. The literature concerning the efficacy and safety assessment of FDKP microspheres is scarce and mostly based on studies performed by MannKind, some of which were already analyzed in this chapter [6–7, 19, 70]. In vitro studies carried out using the Calu-3 human cell line demonstrate it is not cytotoxic [19] and the absence of a pharmacological effect of FDKP was further demonstrated both in vitro and in vivo [6]. A pharmacokinetic study performed on healthy nonsmoking subjects receiving IV FDKP revealed the elimination of more than 90 % of the excipient in 8 h. It was predominantly cleared unchanged by the kidney with negligible oral bioavailability . In another study, diabetic subjects with mild-to-moderate nephropathy were exposed to FDKP only 18–25 % of the time determined for diabetic subjects with normal renal function, which is consistent with the predominant renal clearance of FDKP. As insulin and FDKP cleared from the lungs with a half-life of ≈ 1 h by systemic absorption , authors concluded that the potential for accumulation on chronic administration is minimal because there is an overnight washout period [6]. Nonetheless, only limited data are available on long-term effects of inhaled proteins/excipients of Technosphere® system. This is particularly relevant for chronic diseases and treatments such as diabetes, where any inhalation delivery system must demonstrate long-term pulmonary and systemic safety before it can be approved.
7 Conclusions and Future Perspectives
Counting on many years of testing, Technosphere® appears as one of the most promising formulations designed for the pulmonary delivery of biopharmaceuticals. Technosphere® insulin is taking the forefront of the approach and will soon receive a final decision from FDA. If positive, it might initiate a new meaning for lung drug delivery. Being mostly composed of an excipient highly soluble in the lung fluid, FDKP, Technosphere® usually permits a strong metabolic effect shortly after administration. The rapid lung clearance of FDKP and its renal elimination in nonmetabolized form strongly contribute for its safety profile. The question remaining to be answered is clearly related with the long-term safety of the formulations, which can only be clarified upon the performance of long-term assays, preferably before marketing authorization.
Declaration of Interest
This chapter was written by the authors with no involvement of MannKind Corporation. The authors report no financial disclosures as related to products discussed in this article.
References
Siekmeier R, Scheuch G. Inhaled insulin—does it become reality? J Physiol Pharmacol. 2008;59(Supp 6):81–113.
Pilcer G, Amighi K. Formulation strategy and use of excipients in pulmonary drug delivery. Int J Pharm. 2010;392(1–2):1–19.
Grenha A, Al-Qadi S, Seijo B, Remuñán-López C. The C potential of chitosan for pulmonary drug delivery. J Drug Deliv Sci Technol. 2010;20(1):33–43.
Almeida AJ, Souto E. Solid lipid nanoparticles as a drug delivery system for peptides and proteins. Adv Drug Deliv Rev. 2007;59(6):478–90.
Ungaro F, d’Angelo I, Miro A, La Rotonda MI, Quaglia F. Engineered PLGA nano- and micro-carriers for pulmonary delivery: challenges and promises. J Pharm Pharmacol. 2012;64(9):1217–35.
Potocka E, Cassidy J, Haworth P, Heuman D, van Marle S, Baughman JR. Pharmacokinetic characterization of the novel pulmonary delivery excipient fumaryl diketopiperazine. J Diabetes Sci Technol. 2010;4(5):1164–73.
Cassidy J, Amin N, Marino M, Gotfried M, Meyer T, Sommerer K, Baughman R. Insulin lung deposition and clearance following Technosphere® insulin inhalation powder administration. Pharm Res. 2011;28(9):2157–64.
Feldstein R, Glass J, Steiner S, Self assembling diketopiperazine drug delivery system. United States Patent 5352461 A, 1994.
Steiner S, Feldstein R, Lian H, Rhodes C, Shen G, Microparticles for lung delivery comprising diketopiperazine. United States Patent 6071497 A, 2000.
Cornacchia C, Cacciatore I, Baldassarre L, Mollica A, Feliciani F, Pinnen F. 2,5-Diketopiperazines as neuroprotective agents. Mini Rev Med Chem. 2012;12:2–12.
Martins MB, Carvalho I. Diketopiperazines: biological activity and synthesis. Tetrahedron. 2007;63(40):9923–32.
Bergeron RJ, Phanstiel O, Yao GW, Milstein S, Weimar WR. Macromolecular self-assembly of diketopiperazine tetrapeptides. J Am Chem Soc. 1994;116(19):8479–84.
Luo T-JM, Palmore GTR. Influence of structure on the kinetics of assembly of cyclic dipeptides into supramolecular tapes. J Phys Org Chem. 2000;13(12):870–9.
Kaur N, Zhou B, Breitbeil F, Hardy K, Kraft KS, Trantcheva I, Phanstiel O IV. A delineation of diketopiperazine self-assembly processes: Understanding the molecular events involved in Nϵ-(fumaroyl)diketopiperazine of l-Lys (FDKP) interactions. Mol Pharm. 2008;5(2):294–315.
Neumiller J, Campbell R. Technosphere insulin: an inhaled prandial insulin product. Biodrugs. 2010;24(3);165–72.
Leone-Bay A, Baughman R, Smutney C, Kocinsky J. Innovation in drug delivery by inhalation. OnDrugDelivery Magazine. 2010;4–8. Available at www.ondrugdelivery.com.
Neumiller J, Campbell R, Wood L. A review of inhaled Technosphere insulin. Ann Pharmacother. 2010;44:1231–9.
Leone-Bay A, Grant M, Greene S, Stowell G, Daniels S, Smithson A, Villanueva S, Cope S, Carrera K, Reyes S, Richardson P. Evaluation of novel particles as an inhalation system for GLP-1. Diabetes Obes Metab. 2009;11(11):1050–9.
Angelo R, Rousseau K, Grant M, Leone-Bay A, Richardson P. Technosphere® insulin: defining the role of technosphere particles at the cellular level. J Diabetes Sci Technol. 2009;3(3):545–54.
Leone-Bay A, Smutney C, Kocinsky J. Pulmonary drug delivery—simplified. OnDrugDelivery Magazine. 2011;18–21. Available at www.ondrugdelivery.com.
Boss AH, Petrucci R, Lorber D. Coverage of prandial insulin requirements by means of an ultra-rapid acting inhaled insulin. J Diabetes Sci Technol. 2012;6(4):773–9.
Walters DV. Lung lining liquid—the hidden depths. Neonatology. 2002;81(Suppl. 1):2–5.
Kyle H, Ward J, Widdicombe J. Control of pH of airway surface liquid of the ferret trachea in vitro. J Appl Physiol. 1990;68:135–40.
Steiner S, Pfützner A, Wilson B, Harzer O, Heinemann L, Rave K. Technosphere™/insulin—proof of concept study with a new insulin formulation for pulmonary delivery. Exp Clin Endocrinol Diabetes. 2002;110(1):17–21.
Rave K, Heise T, Heinemann L, Boss A. Inhaled Technosphere® insulin in comparison to subcutaneous regular human insulin: time action profile and variability in subjects with type 2 diabetes. J Diabetes Sci Technol. 2008;2(2):205–12.
Lian H, Steiner SS, Sofia RD, Woodhead JH, Wolf HH, White HS, Shen GS, Rhodes CA, McCabe RT. A self-complementary, self-assembling microsphere system: application for intravenous delivery of the antiepileptic and neuroprotectant compound felbamate. J Pharm Sci. 2000;89(7):867–75.
Pfützner A, Flacke F, Pohl R, Linkie D, Engelbach M, Woods R, Forst T, Beyer J, Steiner S. Pilot study with Technosphere/PTH(1–34)—a new approach for effective pulmonary delivery of parathyroid hormone (1–34). Horm Metab Res. 2003;35:319–23
Steiner S, Gelber C, Feldstein R, Pohl R, Compositions for treatment or prevention of bioterrorism, United States Patent 20040018152 A1, 2006.
Hoyer H, Perera G, Bernkop-Schnürch A. Noninvasive delivery systems for peptides and proteins in osteoporosis therapy: a retroperspective. Drug Dev Ind Pharm. 2010;36(1):31–44.
Toulis K, Anastasilakis A, Polyzos S, Makras P. Targeting the osteoblast: approved and experimental anabolic agents for the treatment of osteoporosis. Hormones. 2011;10(3):174–95.
Lim V, Clarke BL. New therapeutic targets for osteoporosis: beyond denosumab. Maturitas. 2012;73(3):269–72.
Ahrén B, Holst JJ, Mari A. Characterization of GLP-1 effects on β-cell function after meal ingestion in humans. Diabetes Care. 2003;26(10):2860–4.
Yusta B, Baggio LL, Estall JL, Koehler JA, Holland DP, Li H, Pipeleers D, Ling Z, Drucker DJ. GLP-1 receptor activation improves β cell function and survival following induction of endoplasmic reticulum stress. Cell Metab. 2006;4:391–406.
D’Alessio DA, Vahl TP. Glucagon-like peptide 1: evolution of an incretin into a treatment for diabetes. Am J Physiol Endocrinol Metab. 2004;286(6):E882–90.
Vilsbøll T, Agersø H, Krarup T, Holst JJ. Similar elimination rates of glucagon-like peptide-1 in obese type 2 diabetic patients and healthy subjects. J Clin Endocrinol Metab. 2003;88(1):220–4.
Marino M, Costello D, Baughman R, Boss A, Cassidy J, Damico C, van Marle S, van Vliet A, Richardson P. Pharmacokinetics and pharmacodynamics of inhaled GLP-1 (MKC253): proof-of-concept studies in healthy normal volunteers and in patients with type 2 diabetes. Clin Pharmacol Ther. 2010;88(2):243–50.
Hellström PM, Smithson A, Stowell G, Greene S, Kenny E, Damico C, Leone-Bay A, Baughman R, Grant M, Richardson P. Receptor-mediated inhibition of small bowel migrating complex by GLP-1 analog ROSE-010 delivered via pulmonary and systemic routes in the conscious rat. Regul Pept. 2012;179(1–3):71–6.
Hellström PM, Hein J, Bytzer P, Björnssön E, Kristensen J, Schambye H. Clinical trial: the glucagon-like peptide-1 analogue ROSE-010 for management of acute pain in patients with irritable bowel syndrome: a randomized, placebo-controlled, double-blind study. Aliment Pharmacol Ther. 2009;29(2):198–206.
MannKind. 2013-06-20;http://www.mannkindcorp.com/.
Rave K, Heise T, Pfützner A, Boss AH. Coverage of postprandial blood glucose excursions with inhaled Technosphere insulin in comparison to subcutaneously injected regular human insulin in subjects with type 2 diabetes. Diabetes Care. 2007;30(9):2307–8.
Rave K, Potocka E, Boss AH, Marino M, Costello D, Chen R. Pharmacokinetics and linear exposure of AFRESA™ compared with the subcutaneous injection of regular human insulin. Diabetes Obes Metab. 2009;11(7):715–20.
Mandal T. Inhaled insulin for diabetes mellitus. Am J Health Syst Pharm. 2005;62:1359–64.
Potocka E, Amin N, Cassidy J, Schwartz S, Gray M, Richardson P, Baughman R. Insulin pharmacokinetics following dosing with Technosphere insulin in subjects with chronic obstructive pulmonary disease. Curr Med Res Opin. 2010;26(10):2347–53.
Potocka E, Baughman RA, Derendorf H. Population pharmacokinetic model of human insulin following different routes of administration. J Clin Pharmacol. 2011;51(7):1015–24.
Heise T, Brugger A, Cook C, Eckers U, Hutchcraft A, Nosek L, Rave K, Troeger J, Valaitis P, White S, Heinemann L. PROMAXX® inhaled insulin: safe and efficacious administration with a commercially available dry powder inhaler. Diabetes Obes Metab. 2009;11(5):455–9.
Perera AD, Kapitza C, Nosek L, Fishman RS, Shapiro DA, Heise T, Heinemann L. Absorption and metabolic effect of inhaled insulin: intrapatient variability after inhalation via the Aerodose insulin inhaler in patients with type 2 diabetes. Diabetes Care. 2002;25(12):2276–81.
Kim D, Mudaliar S, Chinnapongse S, Chu N, Boies SM, Davis T, Perera AD, Fishman RS, Shapiro DA, Henry R. Dose-response relationships of inhaled insulin delivered via the Aerodose insulin inhaler and subcutaneously injected insulin in patients with type 2 diabetes. Diabetes Care. 2003;26(10):2842–7.
Rave K, Bott S, Heinemann L, Sha S, Becker RHA, Willavize SA, Heise T. Time-action profile of inhaled insulin in comparison with subcutaneously injected insulin lispro and regular human insulin. Diabetes Care. 2005;28(5):1077–82.
Heinemann L. New ways of insulin delivery. Int J Clin Pract. 2010;64(Suppl 166):29–40.
Pfützner A, Mann A, Steiner SS. Technosphere™/insulin—a new approach for effective delivery of human insulin via the pulmonary route. Diabetes Technol Ther. 2002;4(5):589–94.
Rosenstock J, Lorber DL, Gnudi L, Howard CP, Bilheimer DW, Chang PC, Petrucci RE, Boss AH, Richardson PC. Prandial inhaled insulin plus basal insulin glargine versus twice daily biaspart insulin for type 2 diabetes: a multicentre randomised trial. Lancet. 2010;375(9733):2244–53.
Zisser H, Jovanovic L, Markova K, Petrucci R, Boss A, Richardson P, Mann A. Technosphere insulin effectively controls postprandial glycemia in patients with type 2 diabetes mellitus. Diabetes Technol Ther. 2012;14(11):997–1001.
Rosenstock J, Bergenstal R, DeFronzo RA, Hirsch IB, Klonoff D, Boss AH, Kramer D, Petrucci R, Yu W, Levy B. Efficacy and safety of Technosphere inhaled insulin compared with Technosphere powder placebo in insulin-naive type 2 diabetes suboptimally controlled with oral agents. Diabetes Care. 2008;31(11):2177–82.
Pfützner A, Forst T. Pulmonary insulin delivery by means of the Technosphere™ drug carrier mechanism. Expert Opin Drug Deliv. 2005;2(6):1097–106.
Tack C, Christov V, de Galan B, Derwahl K-M, Klausmann G, Pelikánová T, Perušičová J, Boss A, Amin N, Kramer D, Petrucci R, Yu W. Randomized forced titration to different doses of Technosphere® insulin demonstrates reduction in postprandial glucose excursions and hemoglobin A1c in patients with type 2 diabetes. J Diabetes Sci Technol. 2008;2(1):47–57.
Raskin P, Heller S, Honka M, Chang PC, Boss AH, Richardson PC, Amin N. Pulmonary function over 2 years in diabetic patients treated with prandial inhaled Technosphere insulin or usual antidiabetes treatment: a randomized trial. Diabetes Obes Metab. 2012;4(2):163–73.
Smutney C, Friedman E, Polidoro J, Amin N. Inspiratory efforts achieved in use of the Technosphere® insulin inhalation system. J Diabetes Sci Technol. 2009;3(5):1175–82.
Kling J. Dreamboat sinks prospects for fast approval of inhaled insulin. Nat Biotech. 2011;29(3):175–6.
Heinemann L. The failure of Exubera: are we beating a dead horse? J Diabetes Sci Technol. 2008;2(3):518–29.
Rubin R, Peyrot M. Factors associated with physician perceptions of and willingness to recommend inhaled insulin. Curr Med Res Opin. 2011;27(2):285–94.
Rubin R, Peyrot M. Psychometric properties of an instrument for assessing the experience of patients treated with inhaled insulin: the Inhaled Insulin Treatment Questionnaire (IITQ). Health Qual Life Outcomes. 2010;8(1):32.
Peyrot M, Rubin R. Effect of Technosphere inhaled insulin on quality of life and treatment satisfaction. Diabetes Technol Ther. 2010;12(1):49–55.
Peyrot M, Rubin R. Patient-reported outcomes in adults with type 2 diabetes using mealtime inhaled Technosphere insulin and basal insulin versus premixed insulin. Diabetes Technol Ther. 2011;13(12):1201–6.
Peyrot M, Rubin R. Perceived medication benefits and their association with interest in using insulin type 2 diabetes: a model of patients’ cognitive framework. Patient Prefer Adherence. 2011;5:255–65.
Setter SM, Levien TL, Iltz JL, Odegard PS, Neumiller JJ, Baker DE, Campbell RK. Inhaled dry powder insulin for the treatment of diabetes mellitus. Clin Ther. 2007;29(5):795–813.
Brunton S. Insulin delivery systems: reducing barriers to insulin therapy and advancing diabetes mellitus treatment. Am Med. 2008;121(Suppl 6):35–41.
Bailey CJ, Barnett AH. Inhaled insulin: new formulation, new trial. Lancet. 2010;375(9733):2199–201.
Hegewald M, Crapo R, Jensen R. Pulmonary function changes related to acute and chronic administration of inhaled insulin. Diabetes Technol Ther. 2007;9(Suppl 1):S. 93–101.
Lasagna-Reeves CA, Clos AL, Midoro-Hiriuti T, Goldblum RM, Jackson GR, Kayed R. Inhaled insulin forms toxic pulmonary amyloid aggregates. Endocrinology. 2010;151(10):4717–24.
Richardson P, Boss A. Technosphere insulin technology. Diabetes Technol Ther. 2007;9(Suppl 1):65–72.
Sarala N, Bengalorkas G, Bhuvana K. Technosphere: new drug delivery system for inhaled insulin. Pract Diabetes. 2012;29:23–4.
Depreter F, Pilcer G, Amighi K. Inhaled proteins: challenges and perspectives. Int J Pharm. 2013;447(1–2):251–80.
Videira M, Botelho MF, Santos AC, Gouveia LF, Pedroso de Lima JJ, Almeida AJ. Lymphatic uptake of pulmonary delivered radiolabelled solid lipid nanoparticles. J Drug Target. 2002;10:607–13.
Al-Qadi S, Grenha A, Carrión-Recio D, Seijo B, Remuñán-López C. Microencapsulated chitosan nanoparticles for pulmonary protein delivery: in vivo evaluation of insulin-loaded formulations. J Control Release. 2012;157:383–90.
Poyner EA, Alpar HO, Almeida AJ, Gamble MD, Brown MRW. A comparative study on the pulmonary delivery of tobramycin encapsulated into liposomes and PLA microspheres following intravenous and endotracheal delivery. J Control Release. 1995;(31):41–8.
International Conference on Harmonisation, Guideline ICH S7A, Safety pharmacology studies for human pharmaceuticals, 2000.
European Medicines Agency, EMEA/CHMP/QWP/396951/2006, Guideline on excipients in the dossier for application for marketing authorisation of a medicinal product; 2006
Food and Drug Administration, Guidance for industry: nonclinical studies for the safety evaluation of pharmaceutical excipients; 2005.
Acknowledgments
The authors acknowledge the Portuguese government (Fundação para a Ciência e Tecnologia) and FEDER: research project PTDC/SAU-FCF/100291/2008, PTDC/DTP-FTO/0094/2012 and strategic projects PEst-OE/SAU/UI4013/2011 and PEst-OE/EQB/LA0023/2013.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Almeida, A., Grenha, A. (2014). Technosphere®: An Inhalation System for Pulmonary Delivery of Biopharmaceuticals. In: das Neves, J., Sarmento, B. (eds) Mucosal Delivery of Biopharmaceuticals. Springer, Boston, MA. https://doi.org/10.1007/978-1-4614-9524-6_22
Download citation
DOI: https://doi.org/10.1007/978-1-4614-9524-6_22
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4614-9523-9
Online ISBN: 978-1-4614-9524-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)