
Abstract
Benign serous and mucinous tumors of the ovary are mostly cystic and are derived from the epithelium and stroma of the surface, often without evidence of hormonal activity or clinical manifestations, and are often discovered incidentally during the course of routine gynecological or abdominal scans performed for other reasons. They can occur at any age, and if there are clinical manifestations, they are usually due to size. They can be large and although less frequent can cause twisting, bleeding, or rupturing of the cyst. This is manifested by acute pain. Excellent definition provided by transvaginal ultrasound with color Doppler can allow a diagnosis of these types of cysts. Based on macroscopic descriptions provided by pathologists and the correlation of both the morphological sonographic findings as well as those derived from the vascularization of the cyst studied, the diagnosis can be made. The contribution of three-dimensional sonography allows diagnosis of these types of cysts based primarily on the fact that it allows for more of an anatomical view of the structure to be studied, both from a morphologic and a vascular point of view.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Mature ovaries measure from 2 to 4.5 cm in length by 0.5 to 1.5 cm in width. They can weigh between 5 and 10 g and are connected to the rest of the pelvis via the mesovarium.
Broadly, the ovary is composed of two main areas: cortical and medullary.
The cortical, or peripheral, area accounts for about one-quarter of the ovarian volume. In the stroma there are ovarian follicles in various stages of development. This cortical area is, essentially, the functional region of the ovary, where two types of phenomena play out: the hormonal secretion of progesterone and estrogen and ovulation.
The surface of the ovary is almost always coated by simple cuboidal epithelia, the only epithelial element of the gland.
The spinal cord is the central area, rich in blood and lymphatic vessels, immersed in low-density stroma, ensuring vascularization of the cortical layer. There aren’t any follicles in the medullary zone.
The ovarian hilum is the zone where blood vessels penetrate into the gland. At the hilum level, the pelvic peritoneum replaces the inconsistent cuboidal epithelia of the ovarian lining.
Thus, the ovary contains several cell types:
-
Epithelial tissue: cubic epithelial lining
-
Connective tissue: ovarian stroma
-
Germ cells: intrafollicular oocytes
-
Follicular cells: cells of the theca and granulosa
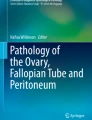
The broad spectrum of histologic features associated with ovarian tumors reflects the diversity of cell types present in normal gonads (Fig. 1).

Graphic representation of the ovary, which reflects the wide variety of cell types that compose it
Neoplastic ovarian cysts are not the most frequent cause of increase in the size of the ovary. The presence of these lesions is usually indicated by menstrual irregularities (due to an imbalance between estrogen and progesterone) and by abdominal pain.
As opposed to benign tumors, neoplasms, in general, are asymptomatic until they acquire enough size to cause mechanical symptoms.
Nonneoplastic cysts are subdivided, at the hormonal level, into functional, when corresponding to an abnormal development of an ovarian follicle, and non-functional, also called organic cysts, that correspond to a proliferative syndrome of the ovarian parenchyma.
Epidemiology and Classification of Benign Ovarian Tumors
Benign ovarian lesions make up around 80 % of the tumors that affect the ovary, 10–15 % are primary malignant tumors of the ovary, and around 5 % are metastatic tumors.
Benign ovarian cysts, both serous and mucinous, can occur at any age.
Alcazar et al. [3], in a series of 1,980 patients, found that the serous cyst is more prevalent in menopausal women, while the mucinous cyst does not present a significant difference in prevalence between premenopausal and postmenopausal patients. In our experience, Pascual et al. [52], among a population of 13,177 postmenopausal patients, we observed the presence of benign ovarian lesions in 1.7 % of patients. Of these lesions, 51 % were simple and/or serous cysts and 1.8 % were mucinous cysts.
Over the course of 25 years, Grapsa et al. [28] observed 86 tumors in adolescent patients between 11 and 19 years of age, 26.7 % of which were epithelial tumors. Twenty-one of them were benign (14 serous cysts and 7 mucinous cysts); two others were borderline. They concluded that the most common cysts among tumors of epithelial origin were benign serous.
Of the three basic components that are involved in the morphogenic development of the gonad: coelomic epithelium, germ cells, and mesenchyme, the first is highly important because it is found in the majority tumors that originate in the ovary. In fact, 70–75 % of all ovarian tumors are of epithelial origin. Of these it is estimated that around 30 % are serous, of which 60 % are benign, and 20–25 % are mucinous, of which 80 % are benign [10, 62].
Tumors derived from the coelomic epithelium, which retain their Müllerian differentiation potential, belong to the group of common epithelial tumors. If the potential retained by the coelomic structures is tubal, serous tumors will form; if they retain the ability to develop in the uterine direction, endometrioid or mucinous neoplasms will be developed.
The need to methodically sort ovarian tumors led them to establish their classification based primarily on histogenesis.
The current World Health Organization (WHO) classification [63] consists of the following varieties of benign tumors of epithelial origin (Table 1).
Clinical Findings
The majority of benign ovarian tumors are cystic derivatives of the epithelium and surface stroma. They are predominantly serous, mucinous, or mixed and are typically asymptomatic.
When these tumors are present but asymptomatic, the diagnosis is usually obtained through explorations stemming from another disease [56] or from a routine gynecological examination either by physical examination or ultrasonography (US).
Clinical manifestations are linked to the size of the cyst; the symptoms are often vague with generalized pelvic discomfort due to pressure on adjacent structures. They may present with abdominal pain of varying intensity and when the growth of the cyst is slow may be accompanied by a sensation of abdominal heaviness.
Larger tumors may be accompanied by an increase in abdominal girth. The extra pressure affects neighboring structures, such as the intestine and ureters, causing bowel and kidney obstructions. When the pressure of the tumor affects vascular structures, complications, such as varicose veins, hemorrhoids, and edema of the lower extremities, can occur due to inferior vena cava compression.
Nonspecific symptoms such as nausea and vomiting, fever, or vagal symptoms may also occur.
Benign ovarian cysts, like serous and mucinous cysts, may occur due to complications such as ovarian torsion, intracystic or intraperitoneal hemorrhage, or a ruptured cyst.
The twisting of the ovary is the most frequent of the aforementioned complications and can occur when there is a significant increase in volume caused by the cyst. Varras et al. [74], in a study of 92 patients with ovarian lesions that were examined for torsion, conclude that 89 % of torsion cases are associated with a benign ovarian tumor. Acute pain is the main symptom, although it may spontaneously recede when the torsion self-corrects. Houry and Abbott [38] also found the same association with ovarian torsion at an 89 % rate in a group of 87 patients and concluded that the diagnosis of ovarian torsion is often missed and ovarian salvage is rare. Characteristics of pain are variable and objective findings are uncommon in ovarian torsion. Prompt diagnosis and treatment through laparoscopy allows for conservative management [12]. Structural changes depend on the evolutionary stage of the process. When only return circulation is affected, marked congestion, edema, and extravasation of blood are observed. In more advanced stages, hemorrhagic necrosis occurs and urgent surgical treatment is needed.
Intracystic hemorrhage results from breakage of some of the vessel wall, without altering it. Intraperitoneal hemorrhage may be seen depending on the size of the affected blood vessel. Hemorrhage presents with intense abdominal pain and the patient can exhibit signs of shock. The condition may spontaneously disappear. Hemorrhagic ovarian cysts are also found in asymptomatic patients.
The rupturing of an ovarian cyst is not a frequent complication. The symptoms depend primarily on the type of tumor and its contents. In the case of a serous cyst, it may even be asymptomatic. The liquid content is drained out through the abdominal cavity, but compared to other ovarian cysts the fluid from the serous cyst is not normally irritating. The rupture of a mucinous cyst may be more serious, since the cells that drain into the abdominal cavity can become implanted in the peritoneum and cause pseudomyxoma peritonei [45], which is complicated to treat. Baratti et al. [7] and Terence et al. [64] obtained acceptable results with radical surgical treatment and intraperitoneal chemotherapy.
Benign ovarian cysts may be discovered in the course of a pregnancy, given that an ultrasound examination is part of routine prenatal care. All guidelines developed include assessment of the ovaries and the adnexa as a required component of a first-trimester examination and are considered clinically appropriate and technically feasible in standard second- and third-trimester examination.
The demonstration of an incidental ovarian or adnexal lesion may provide a morphological evaluation baseline to guide subsequent diagnostic and management strategies. In addition, this information may prove valuable if an acute clinical situation were to develop later on in the pregnancy.
Frequently, the sonographic features of common adnexal lesions such as simple cysts, hemorrhagic cysts, mucinous cysts (Fig. 2), endometriomas, mature cystic teratomas, and ovarian conditions specific to pregnancy, such as ovarian hyperstimulation and large luteinized follicular cysts [47] may permit classification. This allows patients to be classified into conservative management protocols versus those that require further diagnostic and management decisions [26].

Transvaginal US showing a pregnant uterus with a histologic benign mucinous cyst (yellow arrows) in the right adnexal. The image is from a 35-year-old patient with a history of contralateral tumor adnexectomy and ipsilateral cystectomy due to borderline mucinous ovarian tumors. Laparoscopy was performed at 13 weeks gestation due to the rapid growth of the cyst and history. Later, the patient was scheduled for a cesarean due to placenta previa, and a healthy female fetus was born
The goal of US evaluation is to identify those patients in whom conservative management is appropriate versus those who require more immediate intervention such as surgery. The risks of surgical intervention need to be balanced against the potential risks of nonintervention. These may include torsion, rupture, hemorrhage, or the rare spread of a malignant cancer. Atypical features or persistent large lesions should initiate a multidisciplinary team approach to optimize diagnostic and management strategy. Acute symptoms may precipitate emergency intervention at any point in the pregnancy.
Histologic Features
Many pelvic masses have a macroscopic appearance very similar to the image that can be obtained using transvaginal ultrasound in expert hands. Knowing the morphology and characteristics of ovarian tumors is of great help. Sutton et al. [62] reviews the anatomy, embryology, and physiology of the ovary and the different diagnostic modalities, concluding that it is essential to understand the microscopic image in order to make a good differential diagnosis of ovarian masses using US. Lil Valentin [68] confirms that the similarity of the ultrasonographic pattern and the microscopic findings is often very useful for the diagnosis. However, it may also result in false positives, for example, an adenofibroma, which is benign and contains papillary projections.
According to Grases [29], serous tumors are characterized by having an epithelial lining similar to that of the tubal mucosa or the ovarian surface epithelium, with a tendency to form buds and, less frequently, to coat the glandular spaces that are surrounded by fibrous stroma.
Four varieties are distinguished macroscopically, which serves as the basis for their classification. In the cystadenoma, the cavity is unilocular and the wall tends to be thin. When there are numerous buds that stand out in plain view, the term papillary cystadenoma is used. When the papillary proliferation is predominantly present on the outer surface, it qualifies as papilloma or papillomatosis of the surface. For those cases in which the epithelial lesion is part of a solid tumor with abundant fibrous stroma (cellular, edematous, or hyalinized), it is identified as serous adenofibroma, and if there is a combination of solid and cystic lesions, the term cystadenofibroma is used.
In mucinous tumors, the lining epithelium is cylindrical. When cells are mucous secreting and similar to those of the epithelium of the endocervical mucosa or the gastric pyloric mucosa, they are classified as endocervical mucinous cystadenoma. When the epithelium resembles the intestinal mucosa, it is classified as an intestinal mucinous cystadenoma.
Macroscopically, the majority of these tumors is multilocular and can occasionally achieve enormous volume. The external surface is smooth and upon cutting multiple cells of variable size and configuration can be seen, with a smooth, bright, and wavy inner lining (Fig. 3). They are filled with fairly thick mucinous material. Occasionally, there are only a few lobes and rarely a single cavity (Fig. 4).

Gross appearance of a mucinous cystadenoma with multiple septa delimitating cystic spaces filled with mucin

Gross appearance of a mucinous cystadenoma with a focal thickening of the wall lining showing a whitish tissue
Serous tumors, less frequently solid tumors, can be found with a predominance of the fibrous stroma and with a sparse mucinous epithelial component. This is the case with mucinous adenofibromas. When the solid component alternates with cysts lined by mucinous epithelium without atypia, the term mucinous cystadenofibroma is used (Fig. 5).

Gross appearance of a benign mucinous cystadenofibroma with solid areas and mucin filled cystic spaces
The mucinous cystadenoma can coexist with mature cystic teratoma or with other types of ovarian cysts, including those that are malignant.
Occasionally, various types of mural nodules are found in the walls of mucinous ovarian tumors. They include anaplastic carcinoma, carcinosarcoma and sarcoma-like nodules, mixed nodules, and leiomyomas [5].
Diagnostics
The possibility of obtaining an initial diagnosis of a suspected ovarian tumor is based on correct history, general clinical, and, in particular, gynecological examination. The physical examination provides information related to the increase in the size of the ovaries, their mobility, consistency, surface roughness, and whether it is unilateral or bilateral.
A finding of unilaterality, cystic consistency, mobility, and a regular surface point to a benign nature of the tumor. However, it is essential to confirm the suspected ovarian pathology, with US being the technique of choice before considering other more complex, and often unnecessary, technological approaches. Guerriero et al. [31], in a prospective study of 161 premenopausal patients, 83 of which had persistent adnexal mass, concluded, by comparing the results of transvaginal ultrasound and computed tomography (CT), that in premenopausal women, transvaginal ultrasonography remains a cost-effective method in the diagnosis of most cystic ovarian lesions.
Imaging Techniques
The ultrasound for the study of gynecological organs must be transvaginal and whenever possible, with color or power Doppler. Abdominal US with a full bladder is indicated in virgin patients and for completing ultrasound study carried out by transvaginal US in adnexal masses of considerable size.
The majority of tumors affecting the ovaries are benign, and despite the fact that ultrasound is considered the most effective method to predict the histological type, even today, in the absence of clinical symptoms, unnecessary interventions are still recommended instead of minimally invasive procedures or conservative management. An important objective is, therefore, recognizing the different subtypes of benign cysts to make an adequate therapeutic and clinical decision.
Significant advances in technology over the last decade, and improvements in knowledge and training, have allowed experienced ultrasound examiners to correctly classify the majority of growths and in some cases suggest the specific diagnosis through a subjective assessment of sonographic findings in grayscale and color Doppler [68].
Subjective sonographic characterization of benign ovarian cysts based on pattern recognition has been shown to be accurate [67], as well as reproducible [34].
Three-dimensional ultrasound (3D-US) is a technological advance that produces 3D images that give a more realistic reconstruction of anatomical structures in three dimensions. 3D-US enables a more detailed analysis of internal cyst walls, borders, and vascularization, while improving the diagnostic accuracy of US in the evaluation of adnexal masses. The Ultrasound Consensus Conference Statement of the Society of Radiologists [44] concludes that there are many areas for future research that will further our ability to appropriately diagnose and follow adnexal cysts. One of the recommendations is to refine the clinical importance of 3D-US and Doppler findings.
Regarding the management of ovarian and other adnexal cysts imaged sonographically in asymptomatic women, the recommendations of the Society of Radiologists in Ultrasound [44] are:
-
For reproductive age and postmenopausal women with simple adnexal cysts larger than 7 cm, further imaging with magnetic resonance (MR) or surgical evaluation should be considered because the cysts may be difficult to assess completely with US.
-
Multiple thin septations or solid nodules without detectable flow at Doppler US are features that we would specifically consider as indeterminate. These findings are suggestive of neoplasms, most often benign. Irregularities or tiny areas of focal thickening of the cyst wall may be difficult to distinguish from a small solid component and thus cannot determine malignancy. Cysts with either of these indeterminate features merit more attention than the previously described cysts with typical benign sonographic findings. In a woman of reproductive age, this entails a short-interval follow-up (6–12 weeks) with US or, occasionally, further examination with MR imaging. MR imaging may be particularly helpful to confirm the absence of MR contrast enhancement in sonographically solid-appearing areas that do not have demonstrable flow at Doppler US.
A short-interval follow-up of 6–12 weeks with US should be enough time for a physiologic cyst to resolve. However, it should be at a different phase of the menstrual cycle, ideally between the third and tenth day, so that development of a new cyst does not complicate interpretation.
The larger the cyst the more time it may take to resolve. If the lesion persists and continues to have indeterminate findings at US or MRI, surgery should be considered. Although size cannot be used to distinguish between benign and malignant cysts, once cyst size increases above 10 cm, the lesion has a 13 % chance of being malignant [25].
Benign Serous Tumors
Cystadenoma
Cystadenoma tumors are usually 1–10 cm in diameter (Fig. 6) but occasionally reach up to 30 cm or more (Tavassoli et al. [63]).

Laparoscopy of a serous cyst (arrows)
Ultrasonographic findings that define serous cystadenomas are described as unilocular or multilocular cysts, with liquid content and thin walls, and without solid or papillary images in their interior (Fig. 7). They show posterior acoustic enhancement and acoustic streaming. Edwards et al. [20] describe this phenomenon as a visualization of particle movement within the cyst, away from the transducer during color Doppler imaging, after the ultrasound probe had been held still for some time, and this finding was observed in 80 % of cystadenomas. Later, Van Holsbeke et al. [72] observed this phenomenon in 44 % of serous cysts by using data from 1,938 patients with an adnexal mass included in Phase 2 of the International Ovarian Tumor Analysis (IOTA) study.

(a) Transvaginal US shows a unilocular cyst, 54 mm in diameter, with fluid content and thin walls, and no solids or papillary images inside. We can observe posterior acoustic enhancement. In image (b), the prominent posterior acoustic enhancement has been brightened
The vascular features of cystadenoma according to the IOTA consensus [65] show a score of 1 (no blood flow found in the lesion) and sometimes a score of 2 (only minimal flow detected in the cyst wall or within the septa) (Fig. 8).

Transvaginal US of a unilocular cyst with vascularization score of 1. Note that the vessels are outside the cystic structure. The phenomenon of acoustic streaming can be seen inside the cyst (yellow asterisks)
The differential diagnosis of cystadenoma must include both paraovarian and functional cysts. The diagnosis of paraovarian cysts can be made when the ipsilateral ovary is clearly visible. Uncertainty as to whether the mass is ovarian or extraovarian is likely to occur when the ipsilateral ovary is not seen and is probably more likely when the cyst is large. In premenopausal patients, ultrasonographic monitoring of functional cysts will determine their diagnosis [50]. When the cyst persists, it is likely to be a serous cyst.
Guerriero et al. [34] demonstrated that a serous cyst is not difficult to diagnose and it has good interobserver agreement (k 0.72–0.80) between experts and moderately experienced sonologists.
In a prospective study of over 300 patients, Alcázar et al. [2] concluded that for selected asymptomatic premenopausal women, the most sonographically benign ovarian cysts remain unchanged during long-term follow-up. In these cases the data support conservative management.
Valentin et al. [70], in a recent paper, found that the malignancy rate in surgically removed adnexal lesions, which were judged to be unilocular cysts at transvaginal scan, is around 1 %. Postmenopausal status, personal history of breast or ovarian cancer, and hemorrhagic cyst contents at scan increase the risk of malignancy. To avoid misclassifying adnexal lesions as unilocular cysts when scanned, it is important to scrutinize unilocular cysts for the presence of solid components.
Serous cysts at CT appear as well-defined, thin-walled cystic tumors. MRI shows simple fluid signal, hypointense on T1-wieghted sequences, and hyperintense on T2 (Figs. 9 and 10).

Contrast-enhanced CT scan image shows a unilocular cyst with thin walls and water-density contents

Axial images show bilateral unilocular cysts with homogeneous hypointense signal on T1-weighted sequence (a) and hyperintense on T2 (b)
Papillary Cystadenoma
One variety of macroscopic serous cysts has projections in its external or internal wall, or both. When the papillations are present in the outer wall, as is the case with papillary surface, it is very difficult to detect with US (Fig. 11).

Gross appearance of a serous papillary cystadenoma showing yellowish papillae in cystic formation with a smooth inner surface
Thin-walled unilocular cysts with thin septa and papillary projections sonographically characterize benign papillary cystadenomas (Fig. 12).

Illustration of a unilocular cyst with a papillary projection with an irregular surface (blue arrow) and various small papillations (yellow arrows)
These projections can be small, vascularized projections that arise from the internal wall of the cyst or from the septum.
The papillary projections are an important US finding in the morphological classification of ovarian masses. They are defined as any solid projection from the internal cyst wall into the cyst cavity, with a height of ≥3 mm. The surface of the papillary projections can be smooth or irregular [65]; it is important to assess their vascularization by color/power Doppler (Fig. 13).

A unilocular cyst with papillary projection (yellow arrow) with an irregular surface. Color Doppler detected minimal flow within the papillae (score 2)
On the other hand, some echogenic structures in the inner wall of the cyst may be confused with papillary projections. This is the main cause of false-positives of blood clots; although no color flow was detected in these false-positive cases, this is not sufficient to exclude papillary projections, because color flow may be absent in benign projections (Fig. 14).

A unilocular cyst with papillation in the inner wall. Power Doppler shows absence of flow within the papillation (score 1). At follow-up it disappeared and the ovary was normalized. Papillation image corresponds to a clot
A scoring system for masses containing papillary projections was suggested in order to characterize them. It was compared with the subjective evaluation of ultrasound images by an experienced examiner [67]. The results did not improve “pattern recognition” and concluded that the scoring system was a relatively simple method that could be tested in less experienced hands. The idea was to see if its use would improve characterization of ovarian tumors by medical professionals who are not experts in gynecological ultrasonography [4].
Hassen et al. [36], using endovaginal ultrasound, evaluated the morphologic and color Doppler characteristics of papillary projections in benign epithelial stromal ovarian tumors and compared them with those that were borderline and malignant.
This study shows that using conventional ultrasound, topography, size, and morphologic findings correlate with macroscopic findings. The presence or absence of color flow can be used to characterize papillary projections. This demonstrated that benign epithelial tumors have fewer papillary projections than borderline or malignant masses. Furthermore, this study shows that a certain number of morphologic and Doppler findings can be highly suggestive of a diagnosis of benign, versus malignant, papillary projections. The same goes for borderline tumors even though an overlap exists. Large size, acute angle, irregular surface, and disseminated pattern are suggestive of malignancy, whereas absence of color flow in a papillary projection ≥10 mm is suggestive of benignity.
Valentin et al. [70], evaluating only unilocular cysts with papillary projections, found that the greater the number of and the larger the papillations, the higher the risk of malignancy. They concluded that unilocular cysts with papillary projections were more difficult to classify. One reason may be that benign papillary cysts are rare, and larger studies are needed so that more sonographic findings and clinical data can discriminate between borderline and invasive malignancy in unilocular cysts with papillations.
It is probable that in these types of difficult tumors, 3D-US can demonstrate its ability to show morphological structures such as papillary projections, their anatomical relationship with adjacent structures, and the details of their vascularization (Figs. 15 and 16).

Three-dimensional US, render mode shows detail of a papillary projection, without vascular flow signal, in the inner wall of a unilocular cyst

Three-dimensional US, displayed in Tomographic Ultrasound Image (TUI mode), of a unilocular cyst with two papillary projections (yellow arrows). Multiple slices are shown in the 9 panels. The top left image is an axial view of the cyst, which is a reference image. The lines correspond to the views shown in the panels (left to right). The relationship between the papillary projections and the wall cyst is shown
Sladkevicius et al. [60] concluded that while using 3D power Doppler ultrasound to subjectively evaluate the morphology of the vessel tree (Fig. 17), as depicted by 3D power Doppler ultrasound, the clinician can discriminate between benign and malignant ovarian tumors. It adds little to grayscale ultrasound imaging in an ordinary population of tumors.

3D-US, displayed in niche mode, shows an endocystic papillary projection (blue arrow) without vascular flow signal. Accurately observed that the blood vessels run through the cyst capsule without ramifications for papillation (yellow arrows)
Although all patients with papillary cysts will likely undergo surgical removal, preoperative assessment of a tumor as benign, borderline, or malignant is fundamental, particularly in young women, in order to preserve fertility. This also helps the surgeon decide the type of surgery.
Adenofibroma and Cystadenofibroma
Adenofibroma and cystadenofibroma of the ovary are relatively rare benign tumors. Such tumors are characterized by their malignant sonographic appearance. Guerriero et al. [32], in a study of 572 histologically benign tumors, 10 cystadenofibromas of a total of 14 were diagnosed as malignant by US and color Doppler. In those cases in which the epithelial lesion was part of a solid tumor with abundant fibrous stroma (cellular, edematous, or intense hyalinization), it was identified as serous adenofibroma. If there was a combination of solid and cystic lesions, the term cystadenofibroma was used. The images show an example of adenofibroma (Figs. 18 and 19).

(a) Transvaginal US shows a larger (about 90 mm) solid and heterogeneous mass suggestive of malignancy. (b) power Doppler shows moderate flow is present. Histology demonstrated that this corresponded to a benign adenofibroma

Axial T2-weighted image shows solid bilobulated mass (yellow arrows) with a hypointense signal corresponding to the fibrous component
The cystadenofibroma has a low frequency, with a prevalence of around 5 %. Alcázar et al. [1], in a study of 23 ovarian cystadenofibromas, observed a predominantly cystic mass in all cases, with internal septa in 30.4 % (Fig. 20), and solid nodules or papillary projections in 56.5 %, of the cases (Fig. 21); 16 masses (69.6 %) showed an anechoic pattern (Fig. 22), while 7 masses (30.4 %) had echogenic content.

Transvaginal US shows septations, but no nodularity was evident

A complex cystic mass contains evident blood flow within the solid nodule along with septations

Unilocular cyst with anechogenic cyst fluid and a few septations (yellow arrows)
Vascularization is usually peripheral with scattered vessels, however, blood flow may be found in septa and solid nodules (Fig. 23). Alcázar et al. [1] found blood flow in 47.8 % of the cases.

A unilocular cyst with low-level echogenic contents and minimal blood flow (score 2) in the thin septa
Korbin et al. [40], in a study of 14 cases of paraovarian cysts, found serous cystadenofibroma located in 8 cases. US findings were predominantly cystic, and in 9 of 14 masses (64 %), one or more small (<1 cm) solid nodules were identified.
The differential diagnosis was with papillary cystadenoma (Fig. 24), borderline ovarian tumors (Figs. 25 and 26), and papillary serous carcinoma in the initial stages. Valentin et al. [69] included the adenofibromas and cystadenofibromas in the group of unclassifiable growths (benign/malignant), given that the ultrasonographic pattern included papillary projections, multilocular cysts with >10 locules, and masses with low-level echogenicity of cyst fluid. These US features are characteristic of borderline tumors [22, 51].

A complex cyst with papillary projection. Histology corresponded to a benign papillary cystadenoma

A unilocular cyst with endocystic papillary projections, larger in the base (27 and 25 mm, respectively), with irregular surface; Histology corresponded to a serous borderline tumor

Three-dimensional US, displayed in render mode, shows three papillary projections with irregular surface. Histology demonstrated that this corresponded to a serous borderline tumor
Using MRI in 13 cystadenofibromas, Outwater et al. [48] observed 12 multicystic masses with septa of very low signal intensity ranging from 2 to 20 mm, and one was predominantly solid fibrous tissue. Pathologic correlation with the specimen images showed that the low-signal intensity material was the subepithelial fibrous component of the cystadenofibromas. Fibrous components of ovarian fibromas and cystadenofibromas are demonstrable by MR as solid components representing fibrous tissue of very low signal intensity on T2-weighted images.
Benign Mucinous Tumors
Cystadenoma
The sonographic appearance of mucinous cystadenomas usually includes large (Fig. 27) unilateral uniloculated or multiloculated cysts (Figs. 28 and 29) with homogeneous low-level echogenic contents (Fig. 30). However, sometimes the different independent cavities of the cyst contain different types of mucin: endocervical-like (Müllerian) or the intestinal type [29]. The proportion of two types of mucin-producing cells may vary among different compartments in the same tumor. The difference in mucin types may explain the variable echogenicity in the tumor compartments as detected by sonography. Variable echogenicity in cyst compartments was described by Caspi et al. [10] as a more specific sign of a mucinous tumor (Fig. 31).

Transvaginal US shows a larger cyst (140 mm), with smooth internal wall, thin septations, and homogeneous low-level echogenic contents

Transvaginal US shows a multilocular, partly echogenic cyst with multiple septae

Three-dimensional US, displayed in render mode, showing a multilocular cyst with thick and thin septae

Transvaginal US shows a large unilocular cyst, with smooth internal wall, and homogeneous low-level echogenic contents

Sonographic image of a benign mucinous cystadenoma showing variable echogenicity among different cavities
A rare presentation of mucinous cysts is described by Perlman et al. [54], which observed a multiloculated pelvic cystic mass that contained multiple compartments of various echotextures. A careful transvaginal sonographic assessment of the cyst revealed that one of the compartments contained echogenic material arranged in a pattern resembling onion skin shells.
Concentric echogenic layers are a well-known sonographic finding in other mucinous tumors. Degani et al. [16] were the first to describe this sign in a case of appendiceal mucocele, calling it the “onion skin” sign (Fig. 32).

Sagittal sonogram demonstrating contents arranged in “onion skin” thin concentric layers
The vascular features of benign mucinous cysts (Fig. 33), according to the IOTA consensus [65], tend to show a score of 2 (only minimal flow can be detected in the cyst wall or within the septae) and a score of 3 (moderate flow is present). A score of 4 (highly vascular) is rare.

Image (a) shows transvaginal US of a benign mucinous cystadenoma in a 55-year-old patient. The mass histology was 27 cm and 3,860 g. The morphologic pattern is complex with multiple septations, and a thickened and highly vascular pattern showing blood flow (score 4) within the septa. Image (b) shows a borderline mucinous tumor in a 35-year-old patient. Sonogram shows a multiloculated cystic structure containing echogenic material in some of the cavities. Moderate flow is present (score 3) within the septa and cyst walls
Mucinous benign tumors can be difficult to differentiate from mucinous borderline tumors and cystadenocarcinomas. Color flow is of limited value when characterizing these tumors (Fig. 33). This difficulty also applies to CT and MRI techniques (Figs. 34 and 35).

Contrast-enhanced CT image shows multiloculated cystic lesion (yellow arrows) with different densities inside the locus

Coronal fat-saturated T2-weighted image showing a cystic multiloculated lesion with different signal intensities and an intermediate signal corresponding to a mucinous component
The differential diagnosis of a mucinous cyst should be considered on an endometrioma with a high fluid content and with peritoneal cysts [33].
Mucinous Cystic Tumor with Mural Nodules
Mucinous cystic tumors of the ovary, whether benign or malignant, may be associated with sarcoma-like mural nodules. Prat and Scully [57] first reported mucinous tumors of the ovary with “sarcoma-like nodules.”
These nodules resemble gingival epulis or giant cell tumors of bone and are reactive rather than neoplastic.
Solid mural nodules within mucinous ovarian cysts are extremely rare. True sarcomatous nodules are usually larger than sarcoma-like mural nodules.
Benign mural nodules may appear sarcoma-like or have the features of a leiomyoma. These benign nodules are associated with favorable outcomes.
Different imaging techniques show a tumor that is usually large and multilocular, with a solid nodule in the internal wall.
Mucinous Cystic Tumor with Pseudomyxoma Peritonei
Preoperative knowledge of the mucinous nature of a tumor is of crucial importance because many of these tumors are resected laparoscopically, and spillage may occur. Overflow should be prevented not only because of the potential spread of cells in malignant tumors but also because, in these particular tumors, spillage of mucin carries a serious risk of pseudomyxoma peritonei complication, albeit rare.
Pseudomyxoma peritonei follows the perforation of a mucinous appendiceal or ovarian neoplasm which leads to an intraperitoneal dissemination of mucinous implants that range in viscosity from purely liquid to a semisolid-like texture and that form on the peritoneal surfaces of the abdominal wall and visceral organs [58]. Though epithelial cells within the mucin implants can result in mucin production, they rarely invade and hence do not metastasize into the blood stream or lymphatics.
This mucinous material remains intra-abdominal and accumulates, eventually causing severe abdominal distension and anorexia from compression of the small bowel, which are the main causes of morbidity and mortality in untreated patients.
Tumor Markers
Tumor markers are important tools for screenings and follow-ups of patients with ovarian malignancies and have also been suggested to be valuable for early diagnosis. Although CA-125 is the most useful tumor marker, it does not sufficiently distinguish malignant from benign tumors when used alone. In addition CA-125 is very nonspecific, given that it may increase in other types of non-ovarian cancers, such as those of endometrial and gastrointestinal origin, and breast cancer. It is also elevated in benign processes such as endometriosis, pelvic inflammatory disease, cirrhosis, and gestation. Wakahara et al. [76] concluded that comparatively sonography is more effective in making a diagnosis than tumor markers (CA 125, CEA CA 19–9 and 72–4) prior to surgery on an adnexal mass.
Dikensoy et al. [18], in a study of 93 menopausal patients, noted that there were 77 patients with CA-125 values of less than 35 IU/ml, and they had histological findings that were benign. On the other hand, the remaining 16 patients with borderline tumor histology had CA-125 values between 35 and 50 IU/ml and had ultrasound results showing multilocular cysts greater than 13 cm in size.
Spinelli et al. [61], in a study of 120 adolescents with adnexal masses, found 100 % positivity of the tumor markers in malignant tumors (5 cases) and 20.4 % positivity in benign ovarian cysts. Since their results were consistent with others published [59], he therefore concluded that the role of tumor markers was still controversial. This is the reason why, before considering radical treatment, we suggest caution in order to optimize future fertility.
Ultrasound-Guided Aspiration
An attractive possibility for increasing accuracy in diagnosing benign ovarian cysts, in particular serous cysts, is to aspirate the tumor in order to obtain material for cytological study.
The aspiration can be performed either by laparoscopy [11, 46] or sonographic control.
Pez et al. [55] concluded that an ovarian aspiration under sonographic control is a simple technique that avoids many laparoscopies, providing an early diagnosis so that any intervention may be done more quickly.
Montanari et al., in 1987 [46], observed a 53 % rate of recurrence in cysts that were aspirated percutaneously. Dargent and Desmettre [14] concluded that with selected patients, whether done vaginally, percutaneously, or via the urethra, the recurrence rate was equal to that obtained by laparoscopic puncture.
Granberg et al. [27] obtained results of aspirations in simple cysts under sonographic control, which were comparable to those obtained by laparoscopy by other authors [42], with a 70 % rate of no recurrence in the drained cysts.
De Crespigny et al. [15] published a new study of 109 aspirations in 88 patients with a 45 % rate of no recurrence.
In 1990 Forest and col. [24] obtained a 25.3 % rate of recurrence, and Troiano and Taylor [66] achieved good results in a study of 43 patients, which included pregnant women.
Recently, Koutlaki et al. [41], in 121 reproductive age and menopausal patients, have concluded that the aspiration of a benign cyst seems to increase success rates for any expected treatment. Previously, Duke et al. [19] had concluded that this technique was a good alternative for patients with high-surgical risk.
Nevertheless, the technique is controversial. There are authors who are against ovarian aspiration (laparoscopy or ultrasound), due to the danger presented by the spreading of cells, if the tumor is malignant [21, 30].
In our experience [49], we have not observed any cysts under sonographic control aspirated with a cytological result of malignant cells. Our results show a 53.6 % rate of nonrecurrence of benign cystic pathologies in general. If we exclude endometriotic cysts, the rate of nonrecurrence is 57.3 %; in other words, almost 2 of every 3 serous cysts are resolved with a puncture under sonographic control.
The main advantage of this technique is a reduction in surgical interventions. Consequently, the economic and social costs arising from surgical treatment of these pathologies are also reduced.
However, if the cyst recurs, the value of reaspirating the cyst is doubtful, given that of patients that are aspirated more than once, 60 % end up in surgery [27].
In our experience just 15.7 % of patients eventually required surgery. The most frequent causes of intervention were due to an inability to drain the cyst; this is the case with diagnostic aspirations (7.6 %) and the recurrence of cysts previously under sonographic control.
Complications
Torsion
Ovarian torsion is caused by rotation of the ovary or adnexa with the vascular pedicle on its axis, resulting in arterial, venous, or lymphatic obstruction (Fig. 36).

Gross appearance of an infarcted ovary. Dilated vessels can be seen on the surface
The sonographic appearance of ovarian torsion varies according to the duration and degree of the torsion, whether it is complete or incomplete, and the presence or absence of an ovarian mass [23].
Helpful sonographic findings that have been described include the appearance of a cystic, complex mass, with or without pelvic fluid; thickening of the wall; and cystic hemorrhage. All of these are indirect signs of adnexal torsion. They may represent either the cause of torsion or its effects on the ovary, but not the torsion itself. Both the clinical symptoms of torsion, as well as these classic sonographic signs are relatively unspecific.
Van Voorhis et al. [73] and Desai et al. [17] described an enlarged ovary absent of, or with markedly diminished, ovarian blood flow on transvaginal and color Doppler sonography, as a specific finding for the early diagnosis of ovarian torsion (Fig. 37).

This image shows an enlarged ovary without vascularization. It observes the vascular pedicle twisted on itself. The findings are highly suggestive of torsion. The patient immediately underwent a laparoscopy, releasing the torsion
Lee et al. [43] observed the presence of normal arterial flow, which suggested venous thrombosis without arterial occlusion, in addition to a dual blood supply to the ovary, as possible explanations for the occurrence (Fig. 38).

Transvaginal US image shows an enlarged ovary, with edematous stroma, together with signs of twisted ovary. Presence of normal arterial flow can be seen
These different results indicated that, in partial or early torsion, both arterial and venous flow could be maintained with viable ovarian tissue.
Vijayaraghavan [75] described the whirlpool sign representing vessels wrapping around the central axis. Valsky et al. [71], in a study of 80 patients with suspected ovarian torsion, 22 included a search for the whirlpool sign. They concluded that the addition of the sonographic whirlpool sign, to the preoperative sonographic evaluation of patients with suspected torsion, appeared to improve the rate of true-positive diagnoses as confirmed by laparoscopy.
In order to find the whirlpool sign, it is necessary to focus the probe on the adnexal pedicle where the torsion is suspected.
The twisted pedicle should be evaluated in both grayscale and with color/power Doppler (Fig 39). The color Doppler view confirms that the whirlpool sign contains blood vessels.

Image (a) shows a transvaginal US with free fluid surrounding the ovary (blue arrows). It is a grayscale ultrasound image of a twisted ovarian ligament that resembles a spiral or whirlpool sign. Image (b) shows a color Doppler ultrasound image showing twisted vessels around the axis
During pregnancy the relatively rapid movement of the ovaries and fallopian tubes out of the pelvis during the mid-late first trimester, and the rapid return of these structures to their normal anatomical location after delivery, places the ovaries and ovarian masses at an increased risk of torsion [13]. Most cases occur in the first half of pregnancy and, followed by the puerperium, are far less common in the second half of pregnancy.
Hemorrhage
Most hemorrhagic ovarian cysts are nonneoplastic, and the few that are neoplastic are generally benign (Fig. 40). Hemorrhagic ovarian cysts are generally due to an expanding hemorrhage within a corpus luteum or other types of functional ovarian cysts [6].

Gross appearance of a bilobulated cyst with bloody fluid
Jain [39] described the hemorrhagic cyst ultrasound pattern with precision. The average cyst diameter was 3.0–3.5 cm (range, 2.5–8.5 cm). The cyst wall was thin (2 mm), well defined, and regular. Posterior-enhanced through-transmission is seen, signifying the basic cystic nature of the mass.
Hemorrhagic cysts tend to evolve slowly into various stages of acute hemorrhage, clot formation, and clot retraction, thus giving rise to changing sonographic appearances until they completely resolve. Normally, fresh blood is anechoic. In subacute stages when the clot forms, it becomes echogenic (Fig. 41). The echogenicity of hemorrhagic cysts diminishes when hemolysis of the cells begins. In the first 24 h after hemorrhage, the blood is echogenic. However, echogenicity then decreases after 2–4 days. Understanding this pathophysiologic process, it is easier to interpret sonographic appearances and can facilitate diagnosis of hemorrhagic cysts.

A hemorrhagic cyst may occasionally appear solid, due to dense internal echoes and weak transmission. This may be seen in the subacute stage, when there is blood clot formation but the clot lysis has not yet begun
Patel et al. [53], in a study of 30 hemorrhagic cysts, found that fibrin strands (Fig. 42) and a retracting clot (Fig. 43) are vital observations that allow a degree of certainty in the diagnosis of hemorrhagic ovarian cysts. Approximately 90 % of hemorrhagic ovarian cysts will exhibit at least one of these two features.

A cystic mass is shown in the adnexal region with posterior acoustic enhancement. Within this mass, there are fine septations (fibrin strands), which have a reticular appearance. This pattern is common for a hemorrhagic cyst

Transvaginal US shows another common appearance of a hemorrhagic cyst, which is a retracting blood clot (yellow arrows). The clot may appear to be slightly homogeneous or may contain a reticular pattern due to fibrin strands. The remainder of the cystic mass appears anechoic. Occasionally, the retracting clot may simulate a papillary projection. Color and power Doppler sonography would fail to show blood flow in the clot
An acute onset of pain in the pelvis or lower abdomen, due to hemorrhagic cysts in women, closely mimics other gynecologic conditions such as ovarian torsion, ectopic pregnancy, and pelvic inflammatory disease. It can also mimic gastrointestinal disorders such as appendicitis, mesenteric adenitis, Crohn’s disease, and other gastrointestinal conditions. Clinical correlation is crucial, because hemorrhagic cysts are unlikely in the presence of fever and leukocytosis. In summary, the definitive diagnosis of hemorrhagic cysts can be made in most cases with the use of transvaginal sonography, in light of an appropriate history, as well as characteristic sonographic findings.
To ensure resolution, the Ultrasound Consensus Confer-ence Statement [44] recommends short-interval follow-up with US, for women in early postmenopause who have developed complex cysts that appear to be hemorrhagic. If the lesion does not change, then a hemorrhagic cyst is unlikely, and continued follow-up with US or MR imaging should then be considered. Since hemorrhagic cysts are not normally found in late postmenopausal women, any cyst with such an appearance should be considered neoplastic, and surgical evaluation should be considered.
Rupture
When a simple ovarian cyst ruptures, anechoic fluid is seen in the pelvis. However when a hemorrhagic cyst ruptures, echogenic fluid is seen in the pelvis. It might even result in massive hemoperitoneum. A ruptured hemorrhagic cyst with hemoperitoneum may have imaging features similar to those of hemoperitoneum resulting from other causes [37].
Echogenic blood may surround the uterus and adnexa. Moreover, sonographic findings of a ruptured hemorrhagic cyst can very closely mimic a ruptured ectopic pregnancy when a woman of childbearing age has acute pelvic pain and hemoperitoneum. This can become particularly challenging in the setting of positive pregnancy test results in a very early intrauterine pregnancy that is not visualized. The assertion that a positive β-human chorionic gonadotropin (β-hCG) finding indicates ectopic pregnancy and that a negative β-hCG finding suggests a ruptured hemorrhagic cyst becomes very limiting in such a situation [37].
Coincidental occurrence of a corpus luteal cyst rupture and an ectopic pregnancy has, in fact, been reported [35].
Complications from Aspiration
Complications during or after an ovarian aspiration have been observed, by some authors. Examples include bleeding (due to accidental puncture of an important vessel in the area), hematuria, or infections [8, 9].
However, in our experience, we have not observed such complications, either during or after the completion of the aspiration.
References
Alcázar JL, Errasti T, Minguez JA, et al. Sonographic features of ovarian cystadenofibromas. J Ultrasound Med. 2001;20:915–9.
Alcázar JL, Castillo G, Jurado M, et al. Is expectant management of sonographically benign adnexal cysts an option in selected asymptomatic premenopausal women? Hum Reprod. 2005;11:3231–4.
Alcazar JL, Guerriero S, Laparte C, et al. Diagnostic performance of transvaginal gray-scale ultrasound for specific diagnosis of benign ovarian cysts in relation to menopausal status. Maturitas. 2011;68:182–8.
Ameye L, Valentin L, Testa AC, et al. A scoring system to differentiate malignant from benign masses in specific ultrasound-based subgroups of adnexal tumors. Ultrasound Obstet Gynecol. 2009;33:92–101.
Bagué S, Rodriguez M, Prat J. Sarcoma-like mural nodules in mucinous cystic tumors of the ovary revisited: a clinicopathologic analysis of 10 additional cases. Am J Surg Pathol. 2002;26:1467–76.
Baltarowich OH, Kurtz AB, Pasto ME, et al. The spectrum of sonographic findings in hemorrhagic ovarian cysts. AJR Am J Roentgenol. 1987;148:901–5.
Baratti D, Kusamura S, Nonaka D, et al. Pseudomyxoma peritonei: biological features are the dominant prognostic determinants after complete cytoreduction and hyperthermic intraperitoneal chemotherapy. Ann Surg. 2009;249:243–9.
Bessis R, Fonty B. Punction échoguidée des kystes de l’ovaire. Contracept Fertil Sex. 1987;15:535–42.
Broussin B. Les kystes ovariens -Confrontation écho-anatomique. Contracept Fertil Sex. 1991;19:223–30.
Caspi B, Hagay Z, Appelman Z. Variable echogenicity as a sonographic sign in the preoperative diagnosis of ovarian mucinous tumors. J Ultrasound Med. 2006;25:1583–5.
Chaparro J, Vera H, Cognat et al. Traitment coelioscopique des kystes de l’ovarie. Gynecologic. 1986;37:310–8.
Chapron C, Capella-Allouc S, Dubuisson JB. Treatment of adnexal torsion using operative laparoscopy. Hum Reprod. 1996;11:998–1003.
Chiang G, Levine D. Imaging of adnexal masses in pregnancy. J Ultrasound Med. 2004;23:805–19.
Dargent D, Desmettre O. Kystes de l’ovaire: punction échoguidée, coelioscopie ou laparotomie? Rev Fr Gynecol Obstet. 1988;83:335–41.
De Crespigny LC, Robinson HP, Davoren RA, et al. The “simple” ovarian cyst; aspirate or operate? Br J Obstet Gynaecol. 1989;96:1035–9.
Degani S, Shapiro I, Leibovitz Z, et al. Sonographic appearance of appendiceal mucocele. Ultrasound Obstet Gynecol. 2002;19:99–101.
Desai SK, Allahbadia GN, Dalal AK. Ovarian torsion: diagnosis by color Doppler ultrasonography. Obstet Gynecol. 1994;84:699–701.
Dikensoy E, Balat O, Ugur MG, et al. Serum CA-125 is a good predictor of benign disease in patients with postmenopausal ovarian cysts. Eur J Gynaecol Oncol. 2007;28:45–7.
Duke D, Colville J, Keeling A, et al. Transvaginal aspiration of ovarian cysts: long-term follow-up. Cardiovasc Intervent Radiol. 2006;29:401–5.
Edwards A, Clark L, Piessens S, et al. Acoustic streaming: a new technique for assessing adnexal cysts. Ultrasound Obstet Gynecol. 2003;22:74–8.
Einhorn N, Nilsson B, Sjóvall R. Factors influencing survival in carcinoma of the ovary. Cancer. 1985;55:2019–25.
Exacoustos C, Romanini ME, Rinaldo D, et al. Preoperative sonographic features of borderline ovarian tumors. Ultrasound Obstet Gynecol. 2005;25:50–9.
Fleischer AC, Stein SM, Cullinan JA, et al. Color Doppler sonography of adnexal torsion. J Ultrasound Med. 1995;14:523–8.
Forest AM, Bremond A, Leveque J, et al. Kyste de l’ovaire. J Gynecol Obstet Biol Reprod. 1990;19:829–36.
Ghezzi F, Cromi A, Bergamini V, et al. Should adnexal mass size influence surgical approach? A series of 186 laparoscopically managed large adnexal masses. BJOG. 2008;115:1020–7.
Glanc P, Salem S, Farine D. Adnexal masses in the pregnant patient: a diagnostic and management challenge. Ultrasound Q. 2008;24:225–40.
Granberg S, Crona N, Enk L, et al. Ultrasound-guided puncture of cystic tumors in the lower pelvis of young women. J Clin Ultrasound. 1989;17:107–11.
Grapsa D, Kairi-Vassilatou E, Kleanthis C, et al. Epithelial ovarian tumors in adolescents: a retrospective pathologic study and a critical review of the literature. J Pediatr Adolesc Gynecol. 2011;6:386–8.
Grases PJ, editor. Ovario: transtornos benignos. Patología Ginecológica: Bases para el diagnóstico morfológico. Barcelona: Masson; 2003. p. 119–53.
Greer B, Rutledge F, Gallager S. Staging of restaging laparotomy in early-stage epithelial cancer of the ovary. Clin Obstet Gynecol. 1980;23:223–9.
Guerriero S, Mallarini G, Ajossa S, et al. Transvaginal ultrasound and computed tomography combined with clinical parameters and CA-125 determinations in the differential diagnosis of persistent ovarian cysts in premenopausal women. Ultrasound Obstet Gynecol. 1997;9:339–43.
Guerriero S, Alcazar JL, Coccia ME, et al. Complex pelvic mass as a target of evaluation of vessel distribution by color Doppler sonography for the diagnosis of adnexal malignancies: results of a multicenter European study. J Ultrasound Med. 2002;21:1105–11.
Guerriero S, Ajossa S, Mais V, et al. Role of transvaginal sonography in the diagnosis of peritoneal inclusion cysts. J Ultrasound Med. 2004;23:1193–200.
Guerriero S, Alcazar JL, Pascual MA, et al. Diagnosis of the most frequent benign ovarian cysts: is ultrasonography accurate and reproducible? J Womens Health. 2009;18:519–27.
Hallatt JG, Steele CH, Snyder M. Ruptured corpus luteum with hemoperitoneum: a study of 173 surgical cases. Am J Obstet Gynecol. 1984;149:5–9.
Hassen K, Ghossain MA, Rousset P, et al. Characterization of papillary projections in benign versus borderline and malignant ovarian masses on conventional and color Doppler ultrasound. AJR Am J Roentgenol. 2011;196:1444–9.
Hertzberg BS, Kliewer MA, Paulson EK, et al. Ovarian cyst rupture causing hemoperitoneum: imaging features and the potential for misdiagnosis. Abdom Imaging. 1999;24:304–8.
Houry D, Abbott JT. Ovarian torsion: a fifteen-year review. Ann Emerg Med. 2001;38:156–9.
Jain KA. Sonographic spectrum of hemorrhagic ovarian cysts. J Ultrasound Med. 2002;21:879–86.
Korbin FD, Douglas LB, William RW. Paraovarian cystoadenomas and cystoadenofibromas: sonographic characteristics in 14 cases. Radiology. 1998;208:459–62.
Koutlaki N, Niñas I, Dimitraki M, et al. Transvaginal aspiration of ovarian cysts: our experience over 121 cases. Minim Invasive Ther Allied Technol. 2011;20:155–9.
Larsen J, Pedersen O, Gregersen E. Ovarian cyst fenestration via the laparoscope. Acta Obstet Gynecol Scand. 1986;65:539–45.
Lee EJ, Kwon HC, Joo HJ, et al. Diagnosis of ovarian torsión with color Doppler sonography: depiction of twisted vascular pedicle. J Ultrasound Med. 1998;17:83–9.
Levine D, Brown DL, Andreotti RF, et al. Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology. 2010;256:943–54.
Mariani L, Atlante M, Dionis B, et al. Pseudomyxoma peritonei: a case report. J Exp Clin Cancer Res. 2000;19:537–9.
Montanari L, Saviottic C, Zara C. Aspiration of ovarian cysts: laparoscopy or echography? Acta-Europ Fertil. 1987;18:45–9.
Mavromatidis G, Sotiriadis A, Dinas K, et al. Large luteinized follicular cyst of pregnancy. Ultrasound Obstet Gynecol. 2010;36:517–20.
Outwater EK, Siegelman ES, Talerman A, et al. Ovarian fibromas and cystadenofibromas: MRI features of the fibrous component. J Magn Reson Imaging. 1997;7:465–71.
Pascual MA. Valor de la Ecotomografía en la Propedéutica de los Quistes de Ovario. Doctoral thesis, Universidad Autonoma de Barcelona; 1993.
Pascual MA, Hereter L, Tresserra F, et al. Transvaginal sonographic appearance of functional ovarian cysts. Hum Reprod. 1997;12:1246–9.
Pascual MA, Tresserra F, Grases PJ, et al. Borderline cystic tumors of the ovary: gray-scale and color Doppler sonographic findings. J Clin Ultrasound. 2002;30:76–82.
Pascual MA, Hereter L, Graupera B, et al. Prevalence of benign ovarian lesions in asymptomatic postmenopausal women. Ultrasound Obstet Gynecol. 2012;40S1:39. doi:10.1002/uog.11345.
Patel MD, Feldstein VA, Filly RA. The likelihood ratio of sonographic findings for the diagnosis of hemorrhagic ovarian cysts. J Ultrasound Med. 2005;24:607–14.
Perlman S, Hazan Y, Hagay Z, et al. “Onion skin” sign in an ovarian mucinous cyst. J Clin Ultrasound. 2012. doi:10.1002/jcu.21872.
Pez J, Henry-Suchet J, Mintz M, et al. Ponctions des kystes ovariens sous échoguidage. Contracept Fertil Sex. 1987;15:393–8.
Pickhardt PJ, Hanson ME. Incidental adnexal masses detected at low-dose unenhanced CT in asymptomatic women age 50 and older. Radiology. 2010;257:144–50.
Prat J, Scully RE. Ovarian mucinous tumors with sarcoma-like mural nodules. A report of seven cases. Cancer. 1979;44:1332–44.
Ronnett BM, Zahn CM, Kurman RJ, et al. Disseminated peritoneal adenomucinosis and peritonealmucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol. 1995;19:1390–408.
Ruttenstock EM, Saxena AK, Schwinger W, et al. Pediatric ovarian tumors - dilemmas in diagnosis and management. Eur J Pediatr Surg. 2010;20:116–20.
Sladkevicius P, Jokubkiene L, Valentin L. Contribution of morphological assessment of the vessel tree by three-dimensional ultrasound to a correct diagnosis of malignancy in ovarian masses. Ultrasound Obstet Gynecol. 2007;30:874–82.
Spinelli C, Pucci V, Buti I, et al. The role of tumor markers in the surgical approach of ovarian masses in pediatric age: a 10-year study and a literature review. Ann Surg Oncol. 2012;9:1766–73.
Sutton CL, McKinney CD, Jones JE, et al. Ovarian masses revisited: radiologic and pathologic correlation. Radiographics. 1992;12:853–77.
Tavassoli FA, Devilee P, editors. World Health Organization classification of tumours. Pathology and genetics of tumours of the breast and female genital organs. Lyon: IARC Press; 2003.
Terence C, Al-Mohaimeed K, Liauw W, et al. Pseudomyxoma peritonei: a need to establish evidence-based standard of care – is this the right trial? Ann Surg Oncol. 2009;16:2675–7.
Timmerman D, Valentin L, Bourne TH, et al. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: a consensus opinion from the International Ovarian Tumor Analysis (IOTA) group. Ultrasound Obstet Gynecol. 2000;16:500–5.
Troiano RN, Taylor KJ. Sonographically guided therapeutic aspiration of benign-appearing ovarian cysts and endometriomas. AJR Am J Roentgenol. 1998;171:1601–5.
Valentin L. Pattern recognition of pelvic masses by gray-scale ultrasound imaging: the contribution of Doppler ultrasound. Ultrasound Obstet Gynecol. 1999;14:338–47.
Valentin L. Use of morphology to characterize and manage common adnexal masses. Best Pract Res Clin Obstet Gynaecol. 2004;18:71–89.
Valentin L, Ameye L, Jurkovic D, et al. Which extrauterine pelvic masses are difficult to correctly classify as benign or malignant on the basis of ultrasound findings and is there a way of making a correct diagnosis? Ultrasound Obstet Gynecol. 2006;27:438–44.
Valentin L, Ameye L, Savelli L, et al. Unilocular adnexal cysts with papillary projections but no other solid components: is there a diagnostic method that can reliably classify them as benign or malignant before surgery? Ultrasound Obstet Gynecol. 2012. doi:10.1002/uog.12294.
Valsky DV, Esh-Broder E, Cohen SM, et al. Added value of the gray-scale whirlpool sign in the diagnosis of adnexal torsion. Ultrasound Obstet Gynecol. 2010;36:630–4.
Van Holsbeke C, Zhang J, Van Belle V, et al. Acoustic streaming cannot discriminate reliably between endometriomas and other types of adnexal lesion: a multicenter study of 633 adnexal masses. Ultrasound Obstet Gynecol. 2010;35:349–53.
Van Voorhis BJ, Schwaiger J, Syrop CH, et al. Early diagnosis of ovarian torsion by color Doppler ultrasonography. Fertil Steril. 1992;58:215–7.
Varras M, Tsikini A, Polyzos D, et al. Uterine adnexal torsión: pathologic and gray-scale ultrasonographic findings. Clin Exp Obstet Gynecol. 2004;XXXI:34–8.
Vijayaraghavan SB. Sonographic whirlpool sign in ovarian torsion. J Ultrasound Med. 2004;23:1643–9.
Wakahara F, Kikkawa F, Nawa A, et al. Diagnostic efficacy of tumor markers, sonography, and intraoperative frozen section for ovarian tumors. Gynecol Obstet Invest. 2001;52:147–52.
Acknowledgements
Under the auspices of the Càtedra d’ Investigació en Obstetrícia i Ginecologia de la Universitat Autònoma de Barcelona.
Histology images: Francisco Tresserra, MD, PhD. Department of Pathology
CT and MRI images: Belén Úbeda, MD, and Jean-Laurent Browne, MD of Gynecologic Imaging Service. Department of Obstetrics, Gynecology and Reproduction.
Instituto Universitario Dexeus. Barcelona (Spain)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Pascual, M.À. (2013). Epithelial Stromal Tumors: Serous and Mucinous (Clinical Setting and Ultrasound). In: Saba, L., Acharya, U., Guerriero, S., Suri, J. (eds) Ovarian Neoplasm Imaging. Springer, Boston, MA. https://doi.org/10.1007/978-1-4614-8633-6_6
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8633-6_6
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4614-8632-9
Online ISBN: 978-1-4614-8633-6
eBook Packages: MedicineMedicine (R0)