
Abstract
Five typical locations of the appendix, in order of frequency, are retrocecal-retrocolic, free or fixed; pelvic or descending; subcecal, passing downward and to the right; ileocecal, passing upward and to the left, anterior to the ileum; and ileocecal, posterior to the ileum. Congenital absence of the appendix is too rare to be considered seriously, but an apparent absence may be the result of intussusception.
The incision for open appendectomy is usually made over McBurney’s point. To expose a deeply buried retrocecal appendix, it may be necessary to incise the posterior peritoneum lateral to the cecum. During laparoscopic appendectomy, the patient should have an orogastric tube placed to decompress the stomach. Use of a Foley catheter for bladder decompression helps to avert iatrogenic trocar injury to the bladder.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Anatomy
Relations and Positions of the Appendix
The appendix arises from the posteromedial side of the cecum about 1.7 cm from the end of the ileum. The cecum is related posteriorly to the iliopsoas muscle and the lumbar plexus of nerves. Anteriorly it is related to the abdominal wall, the greater omentum, or coils of ileum. The base of the appendix is located at the union of the teniae. For all practical purposes, the anterior tenia ends at the appendiceal origin.
Five typical locations of the appendix, in order of frequency, are:
-
Retrocecal-retrocolic, free or fixed
-
Pelvic or descending
-
Subcecal, passing downward and to the right
-
Ileocecal, passing upward and to the left, anterior to the ileum
-
Ileocecal, posterior to the ileum
Studies have found that the first two positions are the most common, but with significant variations.
Mesentery
The mesentery of the appendix is embryologically derived from the posterior side of the mesentery of the terminal ileum. The mesentery attaches to the cecum as well as to the proximal appendix. It contains the appendicular artery.
Vascular System of the Appendix
Arterial Supply
The appendicular artery arises from the ileocolic artery, an ileal branch, or from a cecal artery. Although the appendicular artery is usually singular (Fig. 11.1), duplication is often seen. In addition to the typical appendicular artery, the base of the appendix may be supplied by a small branch of the anterior or posterior cecal artery.

Blood supply to the appendix. (a, b) Usual type with a single appendicular artery. (c) Paired appendicular arteries (By permission of JE Skandalakis, SW Gray, and JR Rowe. Anatomical Complications in General Surgery. New York: McGraw-Hill, 1983).
Venous Supply
The appendicular artery and the appendicular vein are enveloped by the mesentery of the appendix. The vein joins the cecal veins to become the ileocolic vein, which is a tributary of the right colic vein.
Lymphatic Drainage
Lymphatic drainage from the ileocecal region is through a chain of nodes on the appendicular, ileocolic, and superior mesenteric arteries through which the lymph passes to reach the celiac lymph nodes and the cisterna chyli (Fig. 11.2). Some studies describe a secondary drainage (which passes anterior to the pancreas) to subpyloric nodes.

Lymphatic drainage of the appendix (By permission of JE Skandalakis, SW Gray, and JR Rowe. Anatomical Complications in General Surgery. New York: McGraw-Hill, 1983).
Technique
Appendectomy
The incision for appendectomy is usually made over McBurney’s point. It is made at right angles to a line between the anterior superior iliac spine and the umbilicus at 2/3 the distance from the umbilicus; 1/3 of the incision should be above the line, and 2/3 should be below.
The cecum should be identified first. It can be distinguished from the transverse colon by the absence of attachments of the omentum. If the cecum cannot be located, malrotation of the intestines or undescended cecum should be considered.
When the cecum has been identified, one of the teniae coli can be traced downward to the base of the appendix. In spite of the great mobility of the tip, the base of the appendix always arises from the cecum at the convergence of the teniae. In exposing a deeply buried retrocecal appendix, it may be necessary to incise the posterior peritoneum lateral to the cecum. Congenital absence of the appendix is too rare to be considered seriously, but its apparent absence may be the result of intussusception. In such a case, there should be an obvious dimple at the normal site of the appendix. Of course, the surgeon should inspect the abdomen for signs of previous operation.
-
Step 1. Choice of incision is up to the surgeon. We prefer McBurney (Fig. 11.3).
Figure 11.3. 
Locating McBurney’s point.
-
Step 2. Incise the aponeurosis of the external oblique along the lines of its fibers (Fig. 11.4).
Figure 11.4. 
Incision follows direction of fibers.
-
Step 3. Use a curved Kelly clamp to make an opening on both the internal oblique and the transversus abdominis muscles. Enlarge the opening with the Kelly clamp and insert two Richardson’s retractors.
-
Step 4. If the transversalis fascia is divided together with the flat muscles, occasionally there will be a thick stroma of preperitoneal fat which can be pushed laterally, or sometimes medially, revealing the peritoneum.
-
Step 5. Elevate the peritoneum and, if applicable, the transversalis fascia. Make a small opening in the peritoneum with a knife or scissors, then enlarge it with both index fingers and insert the retractors of your choice (Fig. 11.5).
Figure 11.5. 
Preparing the peritoneum.
-
Step 6. Take cultures of the free peritoneal fluid and, using moist gauze, pull the cecum out of the wound. In most cases, the appendix is delivered with the cecum or may be seen.
-
Step 7. Grasp and study the mesentery of the appendix and reinsert the cecum into the peritoneal cavity. Divide the mesoappendix between clamps (Fig. 11.6).
Figure 11.6. 
Examining the appendix and its mesentery.
-
Step 8. Ligate the mesoappendix with 2–0 silk (Fig. 11.7).
Figure 11.7. 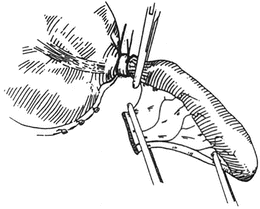
Ligation site.
-
Step 9. With hemostasis completed, lift the appendix straight up and attach two clamps to its base. Remove the clamp close to the cecum. Ligate the appendiceal base doubly with 0 chromic catgut. Stump inversion is done only when the base of the appendix is necrotic. When inverting, use a 3–0 silk purse string (Figs. 11.8 and 11.9).
Figure 11.8. 
Ligation.
Figure 11.9. 
Inversion.
-
Step 10. Divide the appendix between the clamp and the catgut ligatures using a knife with phenol and alcohol or electrocautery (Fig. 11.10). (Alternatively, the appendix can be divided with a GIA stapler.)
Figure 11.10. 
Division.
-
Step 11. Irrigate. Close in layers using catgut or absorbable synthetic suture. If peritonitis is present, close the muscle, but not the skin. The authors use iodoform gauze to pack the wound (Figs. 11.11, 11.12, and 11.13).
Figure 11.11. 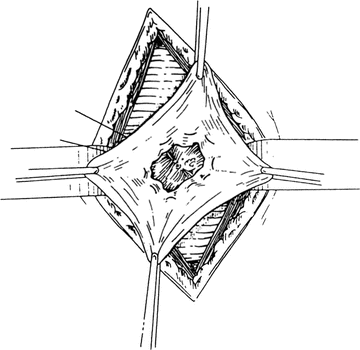
Packing the wound.
Figure 11.12. 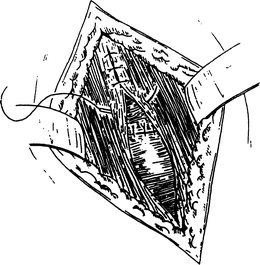
Closing in layers.
Figure 11.13. 
Skin is closed.











Laparoscopic Appendectomy
-
Step 1. Make a 5 mm umbilical incision (Fig. 11.14) and insufflate the abdominal cavity with a Veress needle.
Figure 11.14. 
Location of incision and port placement.
-
Step 2. Place a 5-mm trocar through the umbilicus. Insert the 5 mm laparoscope.
-
Step 3. Under direct vision place a 12-mm port in a suprapubic position: this size is needed for the endoscopic GIA.
-
Step 4. Place another 5-mm port left of midline, halfway between the umbilicus and the suprapubic port.
-
Step 5. Using a laparoscopic Babcock or DeBakey, grasp the appendix and apply traction such that the mesoappendix is visualized. Use the Harmonic scalpel or a LigaSure to take down the mesoappendix (Fig. 11.15).
Figure 11.15. 
Division of the appendix with the Endo GIA stapler.
-
Step 6. Through the suprapubic port, insert the GIA loaded with GI staples. Fire the endoscopic GIA, transecting the appendix. Usually one firing is sufficient; however, it may need to be repeated (Fig. 11.16).
Figure 11.16. 
Removal of the appendix.
-
Step 7. Place the appendix into an endoscopic pouch and remove it through the suprapubic incision (Fig. 11.16).
-
Step 8. Close the suprapubic fascial defect with a 0 Vicryl suture. Close the skin.
Note:
-
✓ The patient should have an orogastric tube placed to decompress the stomach, as well as a Foley catheter for bladder decompression. There are instances when the stomach can reach to the level of the umbilicus; decompression will avoid perforation with the Veress needle.
-
✓ The Foley catheter will decompress the bladder and keep it from being injured during placement of the 12 mm suprapubic trocar. However, the trocar should be carefully observed while it is being placed in the suprapubic position. The author has experienced iatrogenic trocar injury to the bladder even though the bladder was decompressed and the insertion was viewed. So, be careful.
-



Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Skandalakis, L.J., Skandalakis, J.E. (2014). Appendix. In: Skandalakis, L., Skandalakis, J. (eds) Surgical Anatomy and Technique. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-8563-6_11
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8563-6_11
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-8562-9
Online ISBN: 978-1-4614-8563-6
eBook Packages: MedicineMedicine (R0)