
Abstract
Research to date mostly supports a relationship between self-regulatory capacity (and in particular executive function) and alcohol consumption. This chapter explores the nature of this bi-directional relationship, in particular the roles of different types of executive function in different stages or modes of alcohol consumption, the findings of laboratory- and community-based research, the effectiveness of chapter and cognitive measures of self-regulatory capacity, measurement issues and interventions targeting self-regulation in alcohol studies. The diverse research in this area suggests that further interventions targeting self-regulatory capacity are warranted in the alcohol literature, and with preliminary research already existing, population level interventions would be useful.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Self-Regulation and Alcohol
The history of alcohol and executive function has tended to concentrate on deficits in executive function, however, more recently self-regulation has been implicated in a range of alcohol use areas including binge-drinking, drinking studies in the laboratory and longitudinal studies of heavy social drinking. In this chapter an explanation of these different facets of this relationship will be explored.
Self-regulation refers to the capacity to exert control over cognition and emotion in order to organise and direct thinking towards enacting an intended behaviour (Baumeister et al. 2007). According to Hagger et al. (2009) self-regulation can be defined as “the propensity of a person to invest cognitive, emotional and behavioural resources to achieve a desired goal or outcome” p. 208.
Relevance of Self-Regulatory Capacity to Alcohol Consumption
As pursuing behaviour change is a key goal for health psychology, identifying the preceding factors of self-regulation that are malleable is extremely important (Taylor 2008). It has been contended that specific facets of self-regulation may be differentially predictive for different health behaviours. With regard to alcohol consumption, self-regulatory ability has been associated with the consequences of alcohol consumption, beyond actual alcohol consumption, such that self-regulation moderates the relationship between alcohol consumption and alcohol consequences (Neal and Carey 2005).
Executive Functioning
Self-regulation is often equated with executive function, both of which are implicated in the functions of the prefrontal cortex (Koechlin et al. 2003). Different definitions of executive function exist, ranging from parsimonious to more comprehensive. For example Miyake et al. (2000) identified with factor analysis that three components of executive function (mental set shifting, information updating and monitoring and response inhibition) were related but independent. Suchy (2009) has defined executive function as the biological efficiency that underlies self-regulation, “a multifaceted neuropsychological construct that…corresponds to the abilities to (1) reason and generate goals and plans (2) maintain focus and motivation to follow through with goals and plans (3) flexibly alter goals and plans in response to changing contingencies” (p. 106). In a more comprehensive definition, Giancola (2004) considered executive function to include self-monitoring, abstract reasoning, problem solving, planning, cognitive flexibility, impulse control and systematising of relevant material.
Executive functioning is particularly important for adolescents and young adults as these abilities are afforded primarily by the frontal lobe, and research in neuropsychology has shown conclusive evidence that the frontal lobe is the last part of the brain to develop and does not reach full maturity until approximately age 25 (Huttenlocher 1990).
Alcohol and Self-Regulation
Alcohol consumption contributes to a significant proportion of death, disease and injury (Pascal et al. 2009) and the high prevalence, particularly among young adults, is a worldwide concern (Moore et al. 1994; Naimi et al. 2003). Studies examining executive function processes and drinking behaviour have found differences between drinkers and non-drinkers. Of particular note, Lejuez et al. (2010) found that impulsivity was implicated in three stages of alcohol use: initiation of use, regular use and alcohol-related disorders. Further, poorer executive function can prevent improvement in substance use behaviours (including alcohol), further implicating executive function in the maintenance of alcohol dependence (Blume and Marlatt 2009). In addition, intoxicated individuals have been found to have poor inhibition performance on executive function tasks but not on other task components such as speed (Curtin and Fairchild 2003), implicating a bi-directional relationship.
Binge-Drinking and Executive Function
Binge-drinking is characterised by the intake of an excessive amount of alcohol on a single occasion (Norman et al. 1998). In Australia, the National Health and Medical Research Council (NHMRC) defines binge-drinking as the consumption of four or more drinks in one session (NHMRC 2009). The relationship between executive function and binge-drinking has been relatively well supported (e.g., Goudriaan et al. 2007; Hartley et al. 2004). One of the first studies to consider the relationship between executive functioning and binge-drinking was conducted in 50 heavy drinking college students (Blume et al. 2000). Better Wechsler Memory Test scores along with greater negative awareness of the consequences of drinking (but not other executive function measures) were related to greater awareness of the consequences of drinking, suggesting that short-term memory may be important in motivating change in binge-drinking behaviour. This study is noteworthy as it was one of the first to show poor executive function to be associated with motivational elements of behaviour. Furthermore, it appears that executive function may not only impact alcohol consumption directly, but also through more planned and intentional factors. In another study investigating executive function and motivational predictors of social drinking in young adults (Fadardi and Cox 2008), it was found that both maladaptive motivation and greater cognitive biases were predictive of alcohol consumption, further emphasising the importance of addressing both cognitive components of behavioural processes as well as motivational elements in interventions.
Mullan et al. (2011) found that moderate drinkers had greater inhibitory control than non-drinkers, implying that avoiding a binge-drinking session requires greater inhibitory control that avoiding alcohol completely or having more than four drinks. Mullan et al. (2011) conclude that in line with self-control theory, the superior inhibitory control exhibited by moderate drinkers may be the result of constant restraint. Other research has suggested that self-regulation may affect the implementation of intentions by inhibiting habitual responses such as the decision to have another drink, assisting in overcoming the influence of environmental triggers and by enabling the development of future plans (Palfai 2004). Further evidence supporting the link between executive function and alcohol comes from a study by Weissenborn and Duka (2003) who found binge-drinkers performed poorer in spatial working memory and in pattern recognition tasks than non-binge-drinkers. In addition, Heffernan and O’Neill (2012) also found selective memory impairments in binge-drinkers, but only for time rather than event-based prospective memory.
However, some of the research surrounding some executive function components such as working memory, and their role in binge-drinking remains inconclusive. For example, early correlational research into a sample of non-clinical 18–24-year-old social drinkers, found no relationship between cognitive performance and drinking behaviours (Bates and Tracy 1990). More recently, Parada et al. (2011) investigated the relationship between executive cognitive functions and binge-drinking in a sample of university students. Using laboratory-based measures, students who engaged in binge-drinking were less able to remember and manipulate information, but displayed no differences in cognitive flexibility and planning to students who did not engage in binge-drinking.
It therefore appears that while executive functions are generally implicated in binge-drinking, evidence for the role of some components of executive function such as working memory still remains inconsistent. Still more research is needed to explore both in which aspects are most important and to determine the direction of causality (see below for more information).
Alcoholism and Executive Function
Adults diagnosed with alcohol dependence (Sullivan et al. 2000) and chronic alcoholics (Montgomery et al. 2012) have been found to have significant executive function deficits when compared to a control population. In particular, there is some evidence to suggest that when faced with a decision, at least a subgroup of substance dependent individuals tend to discount future consequences in the face of immediate benefits (Field et al. 2007; MacKillop et al. 2011; Mitchell et al. 2005). This decision-making deficit resembles decision-making patterns observed in individuals with lesions of the ventromedial prefrontal cortex (VMPC) (Bechara and Damasio 2002; Bechara et al. 2002). These VMPC lesions typically affect decision-making, with choices favouring immediate reward at the expense of goals or consideration of future consequences (Bechara et al. 1994, 1997). Substance dependent individuals may experience impaired VMPC functioning, and impairments may extend to other brain regions involved in decision-making, such as the amygdala. However, not all individuals displayed the same impairments, suggesting that individuals with substance dependence do not have uniform executive function impairments (Bechara et al. 2002). In addition, Bechara and Damasio (2002) acknowledge that it is unclear whether alcohol causes such impairments, or whether impairments can predispose individuals to alcohol abuse.
Bi-directional Relationship (Longitudinal Studies)
Research supporting the impact of alcohol consumption on executive functions indicates that the relationship is likely to be bi-directional. As Blume and Marlett (2009) state “when executive cognitive defects are identified among people abusing substances, it is generally difficult to sort out whether they represent the consequences of substance abuse or a pre-existing vulnerability for developing substance abuse” p. 118.
The bi-directional relationship between aspects of self-regulation and alcohol consumption was explored by Curtin and Fairchild (2003). When consuming alcohol individuals who had poor pre-existing central executive working memory had increased impulsivity and subsequently a reduction in behavioural inhibition. This study provides evidence that pre-existing deficits in self-regulation can serve to amplify the effects of alcohol on other aspects of self-regulatory abilities, with the potential to create a bi-directional loop between alcohol consumption and self-regulation. This was consistent with research by Finn et al. (1999). Participants were assessed on working memory, sensation seeking and impulsivity while after having consumed no alcohol or up to two doses of alcohol. They concluded that alcohol increased impulsivity only for individuals low in working memory. However, family history of alcoholism was not associated with impulsivity, suggesting that these effects are attributable to self-regulation rather than other factors in alcoholism that may be passed down genetically or environmentally.
Muraven and colleagues (Muraven 2010; Muraven et al. 1999) have demonstrated support for the direction of effect from self-regulation to alcohol consumption. The first study (Muraven et al. 2002) explored self-control and alcohol. Male social drinkers had to either exert self-control by suppressing thoughts, while the control group completed difficult math problems instead. They then took part in a pseudo taste test, where the actual measure of interest was the amount of alcohol consumed. Individuals who suppressed their thoughts consumed more beer and achieved higher blood alcohol content than control participants. The study also found that individuals higher in trait temptation to drink consumed more after suppressing their thoughts relative to those lower on this trait. The authors concluded by suggesting that alcohol consumption may be a function of both temptation to drink and self-control strength. In the second alcohol study from this research group (Muraven et al. 2005) daily changes in ability to self-regulate was the variable of interest. They found that on days where self-regulatory demands were stronger, individuals were more likely to drink more than they had planned. It therefore appears that fluctuations in regulatory capacity can impact on alcohol consumption.
Another study looking at alcohol-related consequences (D’Lima et al. 2012) found that general self-regulatory abilities predicted alcohol-related problems. However, this relationship was mediated by alcohol-specific self-regulatory abilities, such that individuals with high self-regulatory abilities had higher alcohol-specific self-regulatory abilities, and subsequently fewer alcohol-related problems. A recent review into the self-control model and health behaviours more generally included a short section on alcohol consumption (Hagger et al. 2009). The authors conclude that intentional models of health behaviour may only be relevant when people have sufficient self-regulatory capacity to act on their intentions. This conclusion is supported by the study from Australia reported above such that for individuals who intended to binge-drink, those with high planning ability or high inhibitory control were more likely to avoid doing so (Mullan et al. 2011).
There is also evidence to support an association between executive function and longitudinal consequences of alcohol consumption. Previous research has shown that acting without thinking has a stronger association with addiction symptoms than sensation seeking (Magid et al. 2007). One longitudinal study investigated the association between development of prefrontal executive function and subcortical motivational brain regions, and their impact on sensation seeking and acting without thinking over 3 years (Romer et al. 2011). They found that increases in executive function were associated with both increases in sensation seeking and decreases in thinking without acting. Another longitudinal study found that self-regulatory ability was associated with the consequences of alcohol consumption in young adults one-year later (Hustad et al. 2009).
Together this evidence suggests that executive function affects a person’s ability to restrict alcohol consumption, and that alcohol consumption can further reduce executive functioning, which has the potential to create a vicious cycle. However, carefully designed interventions that look at both alcohol consumption and executive function have the potential to be successful, which is further explored below.
Direction of Relationship (Laboratory-Based Studies)
Support for a bi-directional relationship between self-regulation and alcohol consumption is also found in laboratory-based studies. Recent research has found that in alcohol consumers, exposure to alcohol cues can activate attentional biases and subsequently disrupt behavioural control (Weafer and Fillmore 2012), suggesting that associations learnt as a result of drinking can lead to reduced executive functioning and less regulation of subsequent drinking.
Mixed results have, however, been found for the role of alcohol consumption in executive function abilities. For example, Richards et al. (1999) found that the consumption of alcohol in a laboratory setting did not influence delayed discounting responses, but argued that this may have been due to methodological problems. Weissenborn and Duka (2003) also investigated the effect of alcohol consumption on laboratory cognitive tasks, and found that compared to a placebo, a blood alcohol concentration of 1.06 g/l impaired performance on planning and spatial recognition tasks, but not pattern recognition or spatial working memory. In another study, blood alcohol concentrations of 0.4 g/kg led to impairments on executive function tasks such as planning, prioritisation, creativity and adaptability measured using a virtual reality postage-based task, however, ability to choose between two or more alternatives based on prior knowledge was not impaired.
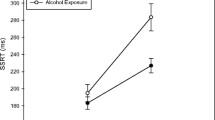
Curtin and Fairchild (2003) experimentally investigated the effects of alcohol intoxication on both evaluative (i.e. monitoring the need for control) and regulative (implementing control) control processes, as well as behaviour. Control processes were measured both with the Stroop task and electroencephalographic (EEG) recordings. Individuals who had consumed alcohol did not have generalised impairments in evaluative control, but rather a specific impairment on incongruent Stroop trials which required inhibitory control suggesting that alcohol can impact regulative control processes. Furthermore, EEG recordings of the parietal P3 revealed that both groups were able to extract the relevant information from all trials with no time delays. However, performance of two frontal lobe areas implicated in switching from automatic to controlled processes and working memory function was significantly reduced, suggesting that alcohol consumption can affect executive processes such as inhibition and regulatory control.
The lab-based literature suggests that there is likely an alcohol consumption-executive function relationship but much is not yet known. Extensive future research into both the specific aspects of executive function that are implicated in binge-drinking, and vice versa is warranted. In addition, the literature would benefit from an exploration of the moderators and mediators of this relationship.
Alcohol and Brain Damage
Rats typically sustain brain damage from the death of neurons and experience-related cognitive deficits after sustained heavy drinking (Crews and Nixon 2009). Similarly in humans, heavy alcohol consumption has been associated with frontal lobe shrinkage which is in excess of the normal ageing process (Kubota et al. 2001). A review of structural and functional changes as a result of alcohol abuse found that damage to the cerebrum and cerebellum due to alcoholism impacted frontal lobe functioning, and disrupted the fronto-cerebellar pathways, thus accounting for the cognitive effects of alcoholism, including executive dysfunction (Sullivan and Pfefferbaum 2005). Furthermore, Sullivan et al. (2000) found that no consistent pattern of deficit with respect to lateralised functions of the cerebral hemispheres emerged. In particular, executive functions, whether assessed with verbal or nonverbal material, was impaired in alcoholics when compared to non-alcoholics, however, alcohol consumption was more closely associated with motor impairments than impairments in cognitive functions such as executive function.
There is also evidence that damaged brain regions may undergo neurogenesis during periods of abstinence, suggesting that these changes are not necessarily permanent (Kubota et al. 2001; Sullivan and Pfefferbaum 2005). This change to executive function in alcoholics has implications for the treatment of alcoholism, as given the bi-directional relationship between alcohol and executive function, such neurogenesis may serve to increase self-regulatory capacity, thus enabling individuals to better restrict alcohol intake (Blume and Marlatt 2009), potentially leading to further neurogenesis and improved outcomes. The impact of executive function deficits when individuals with substance abuse first enter treatment, and the impact of different treatments on executive function deficits in this population therefore need further exploration.
Alcohol and Measurement Issues
One of the main issues to consider when exploring self-regulation is that the results may vary depending on whether paper-based or computer-based reaction time measures are used. Below is a summary of this literature, divided into these two areas, followed by a synthesis of the findings.
One longitudinal study into heavy drinking American college students with measurements points at 1, 6 and 12 months explored changes in alcohol consumption, alcohol related consequences and self-regulation. In this study the Short Self–Regulation Questionnaire (SSRQ) was used, which is designed to quantify an individual’s ability to self-regulate behaviour in seven self-regulation factors, and has demonstrated strong internal consistency (Neal and Carey 2005). Hustad et al. (2009) found that participants’ ability to self-regulate predicted base line alcohol-related consequences, as well as subsequent change in these consequences. In addition, change in self-regulation over 12 months was associated with changes in self-reported alcohol consumption. They concluded that self-regulation both acts as a protective factor from alcohol-related consequences, as well as promoting a reduction in actual alcohol use.
Given the nature of addiction, behaviour tends to occur despite intentions otherwise and outside conscious awareness (McCusker 2001). For example, Hall et al. (2006) conducted a study using the Stroop task to predict health risk and health risk behaviours, including alcohol consumption. They found that behavioural inhibition (as measured by errors on the Stroop task) predicted alcohol consumption above general cognitive function (as measured by the Peabody Picture Vocabulary Test-Revised; Dunn and Dunn 1981) and demographics variables of age, gender and education. McCusker (2001) has therefore argued that computer-based reaction measures such as the Stroop task are more appropriate than paper-based measures for this research area. These measures are beneficial as they assess the actual processes rather than perceptions of these processes, are less demanding as are not directly asking for behaviour information, and can access cognitive components that the individual is not explicitly aware of (Stacy 1997). In addition, Muraven et al. (2002) suggested that in the area of alcohol, methods which assess cognitive biases using reaction-based measures were better than those using self-report as they allow bias-free measurement.
Many reaction time measures support the executive function-alcohol consumption relationship. For example, Mullan et al. (2011) found that planning ability and inhibition control moderated the relationship between intention and behaviour such that for individuals who intended to binge-drink, those with high planning ability or high inhibitory control were more likely to avoid doing so. De Boer et al. (2011) investigated two aspects of self-control: control over initiating a response and control over inhibition or preventing a response, and found alcohol consumption was associated with poor response inhibition rather than initiation. Together these studies suggest that inhibition has a function in controlling alcohol consumption, which has implications for how interventions are designed.
However, some research using cognitive measures of self-regulation has not found consistent support for the impact of alcohol consumption on self-regulation. A systematic review and meta-analysis into the impact of heavy social drinking on executive function was recently published (Montgomery et al. 2012). In this study the authors identified seven studies which met their inclusion criteria. However, the mean effect size of executive function in social drinking was not significant. They however also conducted a study (reported in the same paper) that did show executive function differences between heavy and light drinkers.
Bates and Tracy (1990) used measures of memory, concept formation, abstract reasoning and visio-spatial skills, however, neither alcohol use in general nor excess alcohol consumption were linked to executive function. Hartley et al. (2004) explored the association between performance on computer-based executive function and memory tasks and binge-drinking. For executive function tasks, associations with binge-drinking were found for planning ability, but not for spatial working memory or mental flexibility. Binge-drinking was also associated with sustained attention and long-term memory recall but not pattern or spatial recognition memory. However, the results of this study must be interpreted with caution given their extremely small sample size.
In an attempt to identify the specific executive function components that are inhibited in alcohol users, Rossiter et al. (2012) used a modified version of the Go/No-Go task that was able to separately measure the effects of immediate punishment and delayed reward using monetary incentives on ability to respond and to inhibit responses to stimuli. In harmful drinkers who were at risk of developing alcohol dependence, impulsivity was not hampered by possible punishment, such that they were less sensitive to punishment compared to non-hazardous drinkers. However, harmful drinkers were sensitive to delayed reward, suggesting a possible avenue for future interventions.
Thus the evidence from cognitive- and paper-based tasks is mixed. A more systematic approach is needed, as many paper-based and cognitive-based measures of self-regulation are used, and research exploring the most appropriate measures is very limited.
Modification of Self-Regulation in Alcohol Studies
The mounting evidence suggests that if self-regulation can predict alcohol consumption, then interventions should aim to increase self-regulatory ability. Palfai (2004) has explored self-regulation within the context of targeting alcohol consumption, and acknowledges that automatic aspects of self-regulation play an important role in pursuing health goals, but are often downplayed in the literature compared to conscious top-down elements of decision-making. Indeed, interventions have been successful in training self-regulation in hazardous drinkers using the Alcohol Avoidance Task (Hagger et al. 2009).
However, executive function appears to have a strong genetic component. For example, Friedman et al. (2008) compared performance on three aspects of executive function (response inhibition, working memory and set shifting) in fraternal and identical twins. They found that executive function was almost entirely accounted for by general and specific genetic factors, suggesting both that executive function abilities are highly heritable and that environmental influences are limited. Such research suggests little room for interventions aimed at improving executive function.
Yet despite evidence of a strong genetic component, there is also mounting evidence that self-regulation and executive function are malleable, leading to changes in alcohol consumption. A recent model of self-regulation suggests that self-regulation use can lead to a temporary ‘depletion’ of resources, and subsequently poorer self-regulation. In particular, individuals who attempted to suppress thoughts (Christiansen et al. 2011; Muraven et al. 2002), or engaged in self-control in other aspects of their life (Muraven et al. 2005) subsequently consumed more alcohol. However, with time and training self-regulatory ability can be improved. Studies have shown that repeated exercises of behavioural self-control such as reducing sweets, squeezing a handgrip, keeping a food diary and monitoring posture can lead to improved performance on executive function tasks (Muraven 2010; Muraven et al. 1999). This lends support to the notion that executive function is a muscle that can be strengthened. Executive function therefore appears malleable, but it is yet unclear whether improving executive function performance through training can improve health behaviours, although early indicators appear promising.
The majority of research to date has been lab based and predominantly involves some cognitive retraining followed by a pseudo ‘taste test’ which is actually the behaviour measure. Using this paradigm there is preliminary evidence that executive function can be successfully manipulated to induce changes in behaviour. For example, attention training has reduced harmful drinking up to 3 months later (Fadardi and Cox 2009). Houben et al. (2011) found that training working memory decreased alcohol consumption in the following month, while Houben et al. (2010) found decreased beer consumption following evaluative conditioning of beer with negative stimuli. Inhibition training has been effective in reducing alcohol intake in interventions as short as one session (Houben et al. 2012). It therefore appears that despite a strong genetic component, executive function can be improved with meaningful implications for alcohol consumption. It is possible that inherited levels of executive function may influence the responsiveness of individuals to self-regulation interventions, and future research is needed to investigate the interaction between pre-existing levels of executive function and performance on interventions.
Conclusion
The research into self-regulation and alcohol suggests that self-regulation may be very important both in predicting alcohol use and moderating the relationship between alcohol use and other important predictors of alcohol consumption. However, the literature is currently beset by operationalisation issues such as paper-based versus cognitive measures of self-regulation, a predominance of correlational studies, inconsistencies in the type of cognitive measure used and definitions of both self-regulation and alcohol consumption. These operationalisation issues are also confounded by the use of university students in many of the lab studies as with age, as not all individuals who engage in binge-drinking in adolescence will go on to continue to drink to excess, and not all research can account for different patterns of drinking over longer time periods. In addition the ability to explore the impact of alcohol consumption on executive function is limited in this population, as the length of time and severity of alcohol use may be lower. Blume and Marlatt (2009) also highlight some important issues around interventions, as many current interventions into alcohol use appear to ignore the possibility of pre-existing executive function deficits and future research into this is needed. Moving forward, research needs to address this myriad of methodological issues. There needs to be greater cross-discipline collaboration, as research into executive function and alcohol consumption has been conducted in neuropsychology, abnormal psychology, health psychology and medicine, and these disciplines tend to approach research in different ways and a multi-disciplinary approach is needed.
References
Bates, M. E., & Tracy, J. I. (1990). Cognitive functioning in young “social drinkers”: Is there impairment to detect? Journal of Abnormal Psychology, 99(3), 242–249.
Baumeister, R. F., Schmeichel, B. J., & Vohs, K. D. (2007). Self-regulation and the executive function: The self as controlling agent. Social Psychology: Handbook of Basic Principles, 516–539.
Bechara, A., Damasio, A. R., Damasio, H., & Anderson, S. W. (1994). Insensitivity to future consequences following damage to human prefrontal cortex. Cognition, 50(1–3), 7–15.
Bechara, A., & Damasio, H. (2002). Decision-making and addiction (part I): Impaired activation of somatic states in substance dependent individuals when pondering decisions with negative future consequences. Neuropsychologia, 40(10), 1675–1689.
Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1997). Deciding advantageously before knowing the advantageous strategy. Science, 275(5304), 1293–1295.
Bechara, A., Dolan, S., & Hindes, A. (2002). Decision-making and addiction (part II): Myopia for the future or hypersensitivity to reward? Neuropsychologia, 40(10), 1690–1705.
Blume, A. W., & Marlatt, G. A. (2009). The role of executive cognitive functions in changing substance use: What we know and what we need to know. Annals of Behavioral Medicine, 37(2), 117–125.
Blume, A. W., Marlatt, G. A., & Schmaling, K. B. (2000). Executive cognitive function and heavy drinking behavior among college students. Psychology of Addictive Behaviors, 14(3), 299–302.
Christiansen, P., Cole, J. C., & Field, M. (2011). Ego depletion increases ad-lib alcohol consumption: Investigating cognitive mediators and moderators. Experimental and Clinical Psychopharmacology, 20, 118–128.
Crews, F. T., & Nixon, K. (2009). Mechanisms of neurodegeneration and regeneration in alcoholism. Alcohol and Alcoholism, 44(2), 115–127. doi:10.1093/alcalc/agn079.
Curtin, J. J., & Fairchild, B. A. (2003). Alcohol and cognitive control: implications for regulation of behavior during response conflict. Journal of Abnormal Psychology, 112(3), 424–436.
D’Lima, G. M., Pearson, M. R., & Kelley, M. L. (2012). Protective behavioral strategies as a mediator and moderator of the relationship between self-regulation and alcohol-related consequences in first-year college students. Psychology of Addictive Behaviors, 26, 330–337.
de Boer, B. J., van Hooft, E. A. J., & Bakker, A. B. (2011). Stop and start control: A distinction within self-control. European Journal of Personality, 25(5), 349–362. doi:10.1002/per.796.
Dunn, L., & Dunn, E. (1981). Peabody picture vocabulary test—revised. Circle Pines: American Guidance Service.
Fadardi, J. S., & Cox, W. M. (2008). Alcohol-attentional bias and motivational structure as independent predictors of social drinkers’ alcohol consumption. Drug and Alcohol Dependence, 97(3), 247–256.
Fadardi, J. S., & Cox, W. M. (2009). Reversing the sequence: Reducing alcohol consumption by overcoming alcohol attentional bias. Drug and Alcohol Dependence, 101(3), 137–145.
Field, M., Christiansen, P., Cole, J., & Goudie, A. (2007). Delay discounting and the alcohol Stroop in heavy drinking adolescents. Addiction, 102(4), 579–586.
Finn, P. R., Justus, A., Mazas, C., & Steinmetz, J. E. (1999). Working memory, executive processes and the effects of alcohol on Go/No-Go learning: testing a model of behavioral regulation and impulsivity. Psychopharmacology, 146(4), 465–472.
Friedman, N. P., Miyake, A., Young, S. E., DeFries, J. C., Corley, R. P., & Hewitt, J. K. (2008). Individual differences in executive functions are almost entirely genetic in origin. Journal of Experimental Psychology: General, 137(2), 201–225. doi:10.1037/0096-3445.137.2.201.
Giancola, P. R. (2004). Executive functioning and alcohol-related aggression. Journal of Abnormal Psychology, 113(4), 541–555.
Goudriaan, A. E., Grekin, E. R., & Sher, K. J. (2007). Decision making and binge drinking: A longitudinal study. Alcoholism: Clinical and Experimental Research, 31(6), 928–938.
Hagger, M. S., Wood, C., Stiff, C., & Chatzisarantis, N. L. D. (2009). The strength model of self-regulation failure and health-related behaviour. Health Psychology Review, 3(2), 208–238.
Hall, P. A., Elias, L. J., & Crossley, M. (2006). Neurocognitive influences on health behavior in a community sample. Health Psychology, 25(6), 778–782.
Hartley, D. E., Elsabagh, S., & File, S. E. (2004). Binge drinking and sex: Effects on mood and cognitive function in healthy young volunteers. Pharmacology, Biochemistry and Behavior, 78(3), 611–619.
Heffernan, T., & O’Neill, T. (2012). Time based prospective memory deficits associated with binge drinking: Evidence from the Cambridge prospective memory test (CAMPROMPT). Drug and Alcohol Dependence, 123(1–3), 207–212. doi:10.1016/j.drugalcdep.2011.11.014.
Houben, K., Havermans, R. C., Nederkoorn, C., & Jansen, A. (2012). Beer à No-Go: Learning to stop responding to alcohol cues reduces alcohol intake via reduced affective associations rather than increased response inhibition. Addiction, 107, 1280–1287.
Houben, K., Schoenmakers, T. M., & Wiers, R. W. (2010). I didn’t feel like drinking but I don’t know why: The effects of evaluative conditioning on alcohol-related attitudes, craving and behavior. Addictive Behaviors, 35(12), 1161–1163.
Houben, K., Wiers, R. W., & Jansen, A. (2011). Getting a grip on drinking behavior: Training working memory to reduce alcohol abuse. Psychological Science, 22, 968–975. doi:10.1177/0956797611412392.
Hustad, J. T. P., Carey, K. B., Carey, M. P., & Maisto, S. A. (2009). Self-Regulation, alcohol consumption, and consequences in college student heavy drinkers: A simultaneous latent growth analysis. Journal of studies on alcohol and drugs, 70(3), 373–382.
Huttenlocher, P. R. (1990). Morphometric study of human cerebral cortex development. Neuropsychologia, 28(6), 517–527.
Koechlin, E., Ody, C., & Kouneiher, F. (2003). The architecture of cognitive control in the human prefrontal cortex. Science, 302(5648), 1181–1185. doi:10.1126/science.1088545.
Kubota, M., Nakazaki, S., Hirai, S., Saeki, N., Yamaura, A., & Kusaka, T. (2001). Alcohol consumption and frontal lobe shrinkage: study of 1432 non-alcoholic subjects. Journal of Neurology, Neurosurgery and Psychiatry, 71(1), 104–106. doi:10.1136/jnnp.71.1.104.
Lejuez, C. W., Magidson, J. F., Mitchell, S. H., Sinha, R., Stevens, M. C., & De Wit, H. (2010). Behavioral and biological indicators of impulsivity in the development of alcohol use, problems, and disorders. Alcoholism: Clinical and Experimental Research, 34(8), 1334–1345. doi: 10.1111/j.1530-0277.2010.01217.x.
MacKillop, J., Amlung, M. T., Few, L. R., Ray, L. A., Sweet, L. H., & Munafò, M. R. (2011). Delayed reward discounting and addictive behavior: A meta-analysis. Psychopharmacology, 216(3), 305–321.
Magid, V., MacLean, M. G., & Colder, C. R. (2007). Differentiating between sensation seeking and impulsivity through their mediated relations with alcohol use and problems. Addictive Behaviors, 32(10), 2046–2061. doi:10.1016/j.addbeh.2007.01.015.
McCusker, C. G. (2001). Cognitive biases and addiction: an evolution in theory and method. Addiction, 96(1), 47–56.
Mitchell, J. M., Fields, H. L., D’Esposito, M., & Boettiger, C. A. (2005). Impulsive responding in alcoholics. Alcoholism: Clinical and Experimental Research, 29(12), 2158–2169.
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cognitive Psychology, 41(1), 49–100.
Montgomery, C., Fisk, J. E., Murphy, P. N., Ryland, I., & Hilton, J. (2012). The effects of heavy social drinking on executive function: A systematic review and meta-analytic study of existing literature and new empirical findings. Human Psychopharmacology: Clinical and Experimental, 27(2), 187–199.
Moore, L., Smith, C., & Catford, J. (1994). Binge drinking: Prevalence, patterns and policy. Health Education Research, 9(4), 497–505.
Mullan, B., Wong, C., Allom, V., & Pack, S. (2011). The role of executive function in bridging the intention-behaviour gap for binge-drinking in university students. Addictive Behaviors, 36, 1023–1026.
Muraven, M. (2010). Building self-control strength: Practicing self-control leads to improved self-control performance. Journal of Experimental Social Psychology, 46(2), 465–468.
Muraven, M., Baumeister, R. F., & Tice, D. M. (1999). Longitudinal improvement of self-regulation through practice: Building self-control strength through repeated exercise. Journal of Social Psychology, 139(4), 446–457.
Muraven, M., Collins, R. L., & Neinhaus, K. (2002). Self-control and alcohol restraint: An initial application of the self-control strength model. Psychology of Addictive Behaviors, 16(2), 113–120.
Muraven, M., Collins, R. L., Shiffman, S., & Paty, J. A. (2005). Daily fluctuations in self-control demands and alcohol intake. Psychology of Addictive Behaviors, 19(2), 140–147.
National Health and Medical Research Council. (2009). Australian guidelines to reduce health risks from drinking alcohol. Retrieved from http://www.nhmrc.gov.au/your_health/healthy/alcohol/index.htm.
Naimi, T., Brewer, R., Mokdad, A., Denny, C., Serdula, M., & Marks, J. (2003). Binge drinking among US adults. Journal of the American Medical Association, 289(1), 70–75.
Neal, D. J., & Carey, K. B. (2005). A follow-up psychometric analysis of the self-regulation questionnaire. Psychology of Addictive Behaviors, 19(4), 414–422.
Norman, P., Bennett, P., & Lewis, H. (1998). Understanding binge drinking among young people: An application of the theory of planned behaviour. Health Education Research, 13(2), 163–169.
Palfai, T. (2004). Automatic processes in self-regulation: Implications for alcohol interventions. Cognitive and Behavioral Practice, 11(2), 190–201.
Parada, M., Corral, M., Mota, N., Crego, A., Holguín, S. R., & Cadaveira, F. (2011). Executive functioning and alcohol binge drinking in university students. Addictive Behaviors, 37, 167–172.
Pascal, R., Chikritzhs, T., & Jones, P. (2009). Trends in estimated alcohol-attributable deaths and hospitalisations in Australia, 1996–2005. National alcohol indicators, Bulletin No.12. Perth: National Drug Research Institute, Curtin University of Technology.
Richards, J. B., Zhang, L., Mitchell, S. H., & De Wit, H. (1999). Delay or probability discounting in a model of impulsive behavior: Effect of alcohol. Journal of the Experimental Analysis of Behavior, 71(2), 121–143.
Romer, D., Betancourt, L. M., Brodsky, N. L., Giannetta, J. M., Yang, W., & Hurt, H. (2011). Does adolescent risk taking imply weak executive function? A prospective study of relations between working memory performance, impulsivity, and risk taking in early adolescence. Developmental science, 14, 1119–1133.
Rossiter, S., Thompson, J., & Hester, R. (2012). Improving control over the impulse for reward: Sensitivity of harmful alcohol drinkers to delayed reward but not immediate punishment. Drug and Alcohol Dependence, 125, 89–94.
Stacy, A. W. (1997). Memory activation and expectancy as prospective predictors of alcohol and marijuana use. Journal of Abnormal Psychology, 106(1), 61–73.
Suchy, Y. (2009). Executive functioning: Overview, assessment, and research issues for non-neuropsychologists. Annals of Behavioral Medicine, 37(2), 106–116.
Sullivan, E., Rosenbloom, M., & Pfefferbaum, A. (2000). Pattern of motor and cognitive deficits in detoxified alcoholic men. Alcoholism Clinical and Experimental Research, 24(5), 611–621.
Sullivan, E. V., & Pfefferbaum, A. (2005). Neurocircuitry in alcoholism: A substrate of disruption and repair. Psychopharmacology, 180(4), 583–594.
Taylor, S. E. (2008). Current issues and new directions in psychology and health: Bringing basic and applied research together to address underlying mechanisms. Psychology and Health, 23, 131–134.
Weafer, J., & Fillmore, M. T. (2012). Alcohol-related stimuli reduce inhibitory control of behavior in drinkers. Psychopharmacology, 222(3), 1–10.
Weissenborn, R., & Duka, T. (2003). Acute alcohol effects on cognitive function in social drinkers: Their relationship to drinking habits. Psychopharmacology, 165(3), 306–312.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Highlights
Highlights
-
The relationship between alcohol consumption and self-regulation is bi-directional.
-
Although there is a genetic component to executive function, individual level self-regulation interventions have been moderately effective in changing alcohol consumption.
-
Population-based interventions to improve self-regulation are now warranted, which may improve self-control over alcohol consumption at a more widespread level.
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Mullan, B. (2013). Alcohol Consumption and Self-Regulation. In: Hall, P. (eds) Social Neuroscience and Public Health. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-6852-3_7
Download citation
DOI: https://doi.org/10.1007/978-1-4614-6852-3_7
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-6851-6
Online ISBN: 978-1-4614-6852-3
eBook Packages: MedicineMedicine (R0)