
Abstract
Scientists at the Institute for Work & Health (IWH) investigated the idea of predicting return to work (RTW) for workers with low-back pain (LBP). The objective of this study was to assess the evidence on factors from different domains that predict the duration of sick leave in workers in the beginning of a LBP-related sick leave episode. A systematic review was done in which the IWH scientists identified the studies that looked at prognostic factors associated with time until RTW for workers with LBP, covering studies published in the time frame from January 1966 to April 2011. (This work represents an update on an earlier 2005 review.) Thirty papers from 25 different studies met all of the inclusion criteria. (Eleven were articles captured in the earlier review, and 19 were published after the 2005 review.) The team assessed the methodological quality of the studies that were included. The team found five general factors with strong evidence for returning to work: recovery expectations; healthcare provider type; self-reported disability; pain intensity; and radiating pain. Additionally, workplace-specific factors predictive of RTW were physical demands; accommodation and modified duties; and job satisfaction. The study also found factors that did not predict RTW and factors with mixed evidence. The scientists discussed the review with practitioners in a knowledge transfer workshop. The findings of this systematic review can be used to develop an approach for identifying at-risk workers with LBP, or more specifically, those workers in the early stages of work disability from LBP at high risk for poor RTW outcomes. Practitioners could prioritise and allocate resources based on this new information. The factors identified in this review could be used to screen those workers at high risk of long-term or permanent disability. From these findings a screening tool could be developed, although such a tool would require validation to obtain reliable risk estimates. However, applying this new knowledge in practice should be executed in a structured way. The effectiveness of choosing interventions for workers with LBP based on prognostic information for RTW needs to be established and therefore applying this approach should be done with care.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
This chapter reports on factors that best predict disability outcomes for workers with occupational low-back pain (LBP) when evaluated early in the course of a work disability. Recommendations and implications for practice are tabled.
1 Introduction
Low-back pain (LBP) is the second most common cause of work absenteeism in industrialised countries (Andersson 1999). Most injured workers usually return to work (RTW) in a timely manner; however, some disability episodes are prolonged and disproportionately costly. The percentage of patients with acute LBP whose situation becomes chronic ranges from 2% to 33% (Hoogendoorn et al. 2000), and delays in RTW result in high compensation and treatment costs in all parts of the industrialised world (Frymoyer and Cats-Baril 1991; Maniadakis and Gray 2000; Lambeek et al. 2011; Dionne et al. 2007). Up to 90% of these costs are associated with loss of productivity (Lambeek et al. 2011). Given these facts, there is a genuine need for effective RTW programmes.
When a worker is unable to work due to a low-back injury, many parties want to know how long it will take before the injured person is able to resume employment. The worker wants to know because being off work can seem endless and lead to insecurity and anxiety. The employer wants to know if the organisation or business should make alternate work arrangements should the injured worker be off for an extended period of time. Workers’ compensation case managers want to know so that they can guide intervention decisions for early and safe RTW. Other parties that are interested in RTW include medical examiners, policymakers, clinicians, and workplace disability prevention and return-to-work practitioners.
Identifying workers who are disabled due to LBP and at risk for prolonged recovery is a good idea. This knowledge would help the workplace and other agencies to target interventions that could benefit those workers.
In this chapter, we investigated the idea of predicting RTW for workers with LBP, via a systematic review. The objective of this study was to assess the evidence on factors from different domains (World Health Organization 2001) that predict the duration of sick leave in workers in the beginning of a LBP-related sick leave episode.
As the chapter unfolds, we explain how our review was done, what studies were included in the review and the key findings. We report on factors that best predict disability outcomes for injured workers with LBP when evaluated early in the course of a work disability. The final component of this chapter tells the story of the knowledge transfer workshop where we discussed the review with practitioners. Recommendations and implications for practice are tabled and considered in the final section of the chapter.
In our systematic review, an update of our 2005 review (Steenstra et al. 2005b), we encountered numerous studies that looked at prognostic factors associated with time until RTW. Interpretation of the body of studies on prognostic factors for delayed RTW is challenging due to the sheer volume of publications and the different research design used for each study. However, with the results of our systematic review on early prognostic factors, we have a good starting point that can be used to build a prediction rule to identify the at-risk workers (Steyerberg 2009; Heymans et al. 2009).
Prediction rules go beyond the goals of the prognostic studies we have seen so far in this field. They aim to inform the field, in a direct way, by providing tools that are valid and reliable in patients seen early in the course of a work-disabling episode of LBP. From other fields where this approach seems less novel, evidence shows that prediction rules do a better job at forecasting outcomes than clinical judgement (Meehl 1954; Grove et al. 2000; Grove and Lloyd 2006). A number of prediction rules have been developed to tailor intervention in the treatment of LBP. Some of them are well validated and their impact has been examined (Apeldoorn et al. 2011; Fritz et al. 2005). It is not clear how well prediction rules do when RTW is the outcome of interest. Although prediction rules in the field of work disability prevention have seldom been validated (McGinn et al. 2000), they nevertheless hold promise.
2 How Was the Systematic Review Done?
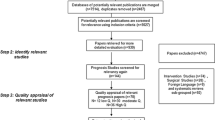
First, we identified the studies that looked at prognostic factors associated with time until RTW for workers with LBP; these were identified by three reviewers working in pairs. The search strategies included three broad categories: prognosis, LBP and RTW terms, and terms on LBP advocated by the Furlan et al. (2009). We covered studies published in the time frame from January 1966 to April 2011. Next, we made sure that the studies met the following eligibility criteria:
-
Observational, longitudinal cohort studies enrolling subjects with LBP and sick leave with a duration of more than 1 day, but less than 6 weeks.
-
Studies that examined the relationship between at least one prognostic factor and RTW.
-
Studies where the outcome was measured in absolute terms (differences in number of days between groups), relative terms (relative risks, odd ratios or hazard ratios), survival curve or duration of sick leave.
Next, we assessed the methodological quality of the studies that were considered for inclusion. The available evidence for each prognostic factor was then assessed as being at one of three levels of evidence (Hoogendoorn et al. 2000):
-
Strong evidence: consistent findings in more than one high-quality study.
-
Moderate evidence: consistent findings in one high-quality study and one or more lower-quality studies, or in more than one lower-quality study.
-
Insufficient evidence: only one study available or inconsistent findings in more than one study.
3 Studies Included in the Systematic Review
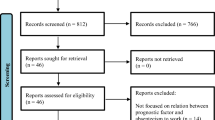
The initial search was fruitful. It yielded 4,449 citations. After a screening of all titles and abstracts, 140 papers were selected for full text review, including those where title and abstract did not provide sufficient details to assess eligibility. Thirty papers from 25 different studies met all of our inclusion criteria (Table 16.1). Eleven were articles captured in our earlier review, and 19 were published after our initial review. The updated search strategy did not identify any studies that should have been considered in our previous review. Three papers (Gatchel et al. 1995a, b; Butterfield et al. 1998) that were selected in the previous review were excluded due to stricter eligibility criteria.
4 Key Findings: Four Factors with Strong Evidence
There were a number of factors that were supported as prognostic for RTW in LBP by strong evidence. This means that there were multiple high-quality studies that agreed on the significance of a particular prognostic factor, and no conflicting results from other studies. Patient’s recovery expectations, health-care provider type, patient-reported level of disability and the presence of radiating pain were supported by strong evidence. We discuss each of the four below.
4.1 Recovery Expectations
The factor that was supported by the most evidence was ‘recovery expectations’ (Heymans et al. 2006, 2009; Du Bois and Donceel 2008; Du Bois et al. 2009; Kapoor et al. 2006; Lotters and Burdorf 2006; Schultz et al. 2004, 2005; Steenstra et al. 2005a; Turner et al. 2006, 2008). Recovery expectations mean that the worker predicts how long he or she thinks it will take before RTW is possible and/or how likely he/she thinks that he/she will be returning to work. Worker expectations of RTW or of a quicker recovery are strong indicators for RTW that could be suitable for use in screening or the assessment of workers, for instance, at the 4-week point post-injury.
Recovery expectations might be influenced by a number of factors. Turner et al. (2008) reported that patients’ expectations might be determined by injury severity, functional status, having a hectic job, receiving an offer for job accommodation, number of pain sites, previous injury and type of health-care provider.
This has practical application. Asking injured workers about their recovery expectations could identify those at high risk. Then those individuals could be further questioned as to what specific issues affect their recovery expectations, some of which may be modifiable.
4.2 Health-Care Provider Type
This factor was supported by strong evidence (Steenstra et al. 2005a; Turner et al. 2008; van der Weide et al. 1999) as well. In other words, there was an association between which type of health-care provider the worker attended following a low-back injury and time to RTW. Specifically, there was evidence that said seeking care from a chiropractor results in shorter time on disability benefits.
This finding is in agreement with evidence of the effectiveness of manipulation for acute and sub-acute LBP (Assendelft et al. 2004). However, some caution is warranted. Referral bias might play a role, by which we mean that more severe injuries may be preferentially referred to health-care providers other than chiropractors. Evidence for a causal relationship is better established through randomised controlled trials.
4.3 Disability and Pain Intensity
Workers’ ‘self-reports of disability’ (Heymans et al. 2006, 2009; Baldwin et al. 2007; Du Bois et al. 2009; Fransen et al. 2002; Lotters and Burdorf 2006; Nordin et al. 1996; Steenstra et al. 2005a; Turner et al. 2008; van der Weide et al. 1999) and ‘pain intensity’ (Heymans et al. 2006, 2009; Baldwin et al. 2007; Burdorf et al. 1998; Du Bois and Donceel 2008; Du Bois et al. 2009; Franklin et al. 2008; Fransen et al. 2002; Goertz 1990; Lotters and Burdorf 2006; Nordin et al. 1996; Prkachin et al. 2007; Schultz et al. 2004; Turner et al. 2008; van der Weide et al. 1999) are often correlated, but asking both questions seems to improve prediction of prognosis. This means that a worker should be asked both about functional limitations and about pain intensity at the start of work disability. Both can be easily measured in several ways with well-validated questionnaires. In Ontario, the Workplace Safety and Insurance Board (WSIB) uses the Roland Morris Disability Questionnaire and a 10-point Visual Analogue Scale (VAS) pain rating scale to monitor baseline values and progress at the end of treatment within their programmes of care for LBP.
4.4 Radiating Pain
Radiating pain—that is, pain that extends away from the low back, usually into the legs—is often used as a surrogate proxy for neurological involvement and reported as a measure of injury severity (Baldwin et al. 2007; Du Bois and Donceel 2008; Franklin et al. 2008; Fransen et al. 2002; Fulton-Kehoe et al. 2008; Goertz 1990; Nordin et al. 1996; Prkachin et al. 2007; Turner et al. 2008; van Doorn 1995; Abenhaim et al. 1995). This factor was supported by strong evidence to predict delays in RTW. In patient assessments, neurological findings are often considered to be a ‘red flag’ that warrants further clinical investigation. Since this fact has become more commonly known, some recent studies excluded patients with neurological complications associated with radiating pain. Therefore, this factor was often not included in the more recent high-quality studies.
5 Workplace Factors Predictive of Return to Work
Unfortunately, workplace factors are not considered in prognostic studies as often as one might expect given the amount of research concluding that RTW is a multifactorial problem. There has been a shift away from a biomedical to a biopsychosocial model in current literature (Loisel et al. 2001). However, the measurement of workplace-related factors in formal studies is clearly lagging. Often, measures are used from general work and health research (Karasek et al. 1998) that might not be valid for workers off work. However, there are a few work-related factors, supported by strong evidence, shown to be predictive for RTW. In this next section, we will discuss those workplace factors supported by the best evidence: physical demands, accommodation and modified duties, and job satisfaction.
5.1 Physical Demands
Physical demands at the workplace have been shown to be predictive of RTW (Du Bois et al. 2009; Turner et al. 2008)—in other words, those workers with more physically demanding work were slower to resume employment after a low-back injury. Physical demands of the workplace are often derived from the coding of occupations (Herbert et al. 1996). These codes may, at first, seem crude, but they have shown to be predictive more often than self-reported measures where the worker is asked about physical demands of the job. Studies that used self-reported measures only provide moderate evidence for an effect of physical demands on RTW. Some studies in our review (Fransen et al. 2002; Nordin et al. 1996) found an effect of what seemed extreme differences in physical demands that were present in the study population, for instance, when comparing rail maintenance workers to office workers in one company (Nordin et al. 1996). However, most studies did not find an effect of self-reported physical demands (Heymans et al. 2006, 2009; Alexopoulos et al. 2008; Dasinger et al. 2000; Du Bois et al. 2009; Franklin et al. 2008; Fulton-Kehoe et al. 2008; Krause et al. 2001; Lotters and Burdorf 2006; Pransky et al. 2006; Schultz et al. 2004; Turner et al. 2008). These findings suggest that physical demands classified through occupational codes and self-report of physical demands are not interchangeable. This may be because a workers’ perception of the physical demands of the job is biased by getting injured at work.
5.2 Accommodation and Modified Duties
Workplace accommodation may help address physical workplace demands as a barrier to resuming employment after a low-back injury. If so, the offer of modified duties or workplace accommodation could improve RTW outcomes. This factor was reported in a number of ways: Two high-quality studies (Fransen et al. 2002; Fulton-Kehoe et al. 2008; Turner et al. 2008) found the factor to be predictive for faster RTW, one lower-quality study reported a significant effect (Goertz 1990) and one lower-quality study found a non-significant effect of the availability of modified duties (Pransky et al. 2006).
Interestingly, goodwill goes a long way: The offer of alternate duty was more prognostic than whether or not alternate duty was actually implemented (Turner et al. 2008). In some jobs modified duties are more difficult to implement, and in that case unavailability of modified duties could also be considered as a characteristic of the job and not so much as unwillingness to provide modified duties (Fransen et al. 2002).
5.3 Job Satisfaction
There is strong evidence that a simple job satisfaction measure is predictive for RTW following a low-back injury (Baldwin et al. 2007; Fransen et al. 2002; Heymans et al. 2006; Krause et al. 2001; Nordin et al. 1996; Turner et al. 2008; van der Weide et al. 1999). Job satisfaction is probably determined by other factors at work, but it is nevertheless a strong indicator that can be used in screening or assessing at the very start of the work disability process.
6 Factors That Do Not Predict Return to Work
Some factors showed no predictive ability for RTW. There was strong evidence that there was no association between lifestyle factors (Alexopoulos et al. 2008; Burdorf et al. 1998; Du Bois et al. 2009; Franklin et al. 2008; Fransen et al. 2002; Heymans et al. 2006; Turner et al. 2008; van der Weide et al. 1999) or pain catastrophising and RTW. Pain catastrophising was profiled in two high-quality studies, and no significant effect was found among workers with acute low-back injuries. However, it might play a role at a later stage in the work disability process (see also Chap. 8).
7 Factors with Mixed Evidence
A number of factors showed moderate or mixed evidence for predicting RTW. It was difficult to summarise the evidence of workplace psychosocial factors and their relationship to RTW, due to a lack of consensus on how this construct was measured among researchers. Similarly, there was moderate evidence that having a prior claim is associated with a delay in RTW (Alexopoulos et al. 2008; Fransen et al. 2002; Pransky et al. 2006; Steenstra et al. 2005a; Turner et al. 2006), the evidence on this factor was mixed. The North American studies in our review reported a delay in RTW among employees with prior disability claims (Pransky et al. 2006; Turner et al. 2006), whereas non-North American studies did not (Alexopoulos et al. 2008; Fransen et al. 2002; Steenstra et al. 2005a).
Surprisingly, there was moderate evidence that depression does not play a major role as a prognostic factor in the first phase of work disability (Du Bois et al. 2009; Fransen et al. 2002; Fulton-Kehoe et al. 2008). Depression could, however, become important at a later stage of the work disability process, when the worker is away from work for a longer period of time.
Likewise, the results of clinical examination (Baldwin et al. 2007; Du Bois et al. 2009; Nordin et al. 1996; Prkachin et al. 2007) were not prognostic for time away from work, although some of these studies excluded red flag issues that would have been evaluated during clinical examination.
Also interestingly, age and sex were two categories for which insufficient evidence was identified. This was surprising since in our previous review, these items were identified as prognostic. Recent high-quality studies (Alexopoulos et al. 2008; Du Bois et al. 2009; Steenstra et al. 2005a; Turner et al. 2008) did not report a relationship for age and sex with RTW. Age and sex are often added as confounders to statistical models without providing actual effect estimates—oftentimes because age is deemed not modifiable. This limits our understanding of the strength of association with RTW when compared to studies where they are reported as significant.
In a working population that is ageing, reporting the effect of age might provide valuable information when devising interventions to improve RTW and stay at work outcomes in this growing segment of the population. Reporting the effect of age in RTW could be a first step in disentangling the mechanisms at play in older age groups.
‘Fear-avoidance beliefs’ were not shown to be prognostic for RTW following a low-back injury (Alexopoulos et al. 2008; Fransen et al. 2002; Gluck and Oleinick 1998; Krause et al. 2001; van Doorn 1995; van der Weide et al. 1999). This may be due to the content of the questionnaire primarily used in this field (Waddell et al. 1993). The commonly used fear-avoidance beliefs questionnaire (Waddell et al. 1993) could be less valid in a population where back pain is work related or at least work relevant (Inrig et al. 2012) because some of the items relate to fears about re-injury on the job which might be quite valid rather than fear-avoidance related.
One factor that has recently been of great interest to researchers is the association between use of pain medication in general and opioids in particular on RTW. However, this area has not yet been examined in a sufficient number of high-quality studies (Du Bois et al. 2009; Franklin et al. 2008; Pransky et al. 2006; Webster et al. 2007) to draw conclusions.
8 Knowledge Transfer Workshop: Discussing the Results with Practitioners
We wanted to get this information, the findings of our systematic review, into the hands of practitioners to make the findings applicable, to provide context for the identified factors and to improve the RTW process for injured workers with LBP. So we organised a workshop for the organisation that provided the grant for this study in Winnipeg, Manitoba, in 2011 to discuss the results of our review. The workshop was attended by 34 professionals who were active in work disability prevention. Participants were divided into seven groups to discuss the review. The workshop had four components:
-
1.
An overview of our study (design and methods).
-
2.
A discussion of prognostic factors, according to the knowledge and experience of the practitioners involved.
-
3.
Information on the strength of the evidence for all factors identified in the review.
-
4.
An exercise using cue cards to evaluate the relevance of the most important constructs found in the evidence synthesis.
The workshop involved much dialogue and discussion; the researchers heard from the practitioners. Each of these practitioner groups discussed the importance of each prognostic factor and determined relevance based on the clinical practice and experience of the groups’ members. The table below illustrates the agreement between research and practice (see Table 16.2).
9 Results of the Knowledge Transfer Workshop
The workshop revealed a number of discrepancies between the results of our systematic review and clinician’s impressions. Although we made it clear to participants that we limited our review to those workers in the early phase of work disability/sick leave, some of the discrepancies noted between the clinicians’ views and the evidence may be influenced by their clinical experience with patients at a later stage in the disability process.
Many of the factors raised by the practitioners were psychological. The shift from a biomedical model to a biopsychosocial model (Engel 1977) appears to have occurred with a strong emphasis on psychological factors. However, from our review, it seems that some of these factors should still be considered in conjunction with some of the biomedical factors. The psychosocial factors that were mentioned lacked evidence.
Another key distinction was revealed in the workshop: Participants (practitioners) considered workplace factors, such as supervisor or co-worker support and work-life interference, to be psychosocial factors. This may be important. At the workshop, we were only able to present preliminary findings. The final results on job satisfaction were not presented, and yet they could be considered as a workplace psychosocial factor.
There was no consensus among workshop participants on some of the factors supported by strong evidence: Recovery expectations was endorsed by five out of seven groups, radiating pain and disability by four of the seven groups and workplace physical factors and health-care provider by six of the seven groups.
We asked participants what they thought should be the next steps for research. The recommendation was to further translate the results into practical tools. Participants wanted research and information that could be applied in practice.
10 Discussion: Applicability and Recommendations
The findings of our systematic review can be used to develop an approach for identifying at-risk workers with LBP or, more specifically, those workers in the early stages of work disability from LBP at high risk for poor RTW outcomes. Practitioners could prioritise and allocate resources based on this new information. The factors identified in this review could be used to screen those workers at high risk of long-term or permanent disability. From these findings a screening tool could be developed, although such a tool would require validation to obtain reliable risk estimates.
How, exactly, would this be done? The steps as summarised by McGinn et al. (2000) could be followed. Such a tool should be based on prior knowledge (as summarised in this review). It should be derived in a dataset, and it should be validated. Thorough validation procedures are available (Steyerberg 2009). A first step would be internal validation within the same dataset. However, external validation in a new dataset and/or other setting is preferred. The screening tool should then be evaluated for its effectiveness on improvement of care for those off work due to LBP (McGinn et al. 2000).
Other studies and reviews may lead the way, as well. A recent systematic review on prediction rules for the physiotherapeutic management of LBP concluded that most of the identified 23 studies described the derivation of a rule and none investigated the impact phase of development (Haskins et al. 2011). Stanton et al. (2010) found 18 studies on 15 separate rules for a variety musculoskeletal complaints and found only one study that looked at the impact of the rule in practice (Flynn et al. 2002). Stanton et al. confirmed that more evidence is needed to implement prediction rules in practice on a large scale. For the work disability prevention setting evidence for the effectiveness of the application of a prediction rule is definitely lacking.
The prediction rule that was included in our review was by Heymans et al. (2009). The variables examined for the rule were chosen based on our previous review and clinicians’ input. This study used validation techniques to increase generalisability to other populations (Steyerberg et al. 2001). External validation however is still preferred when the original study is small (Bleeker et al. 2003). The prediction rule for LBP as developed by Dionne and colleagues (Dionne et al. 2005, 2006) has been validated in multiple settings. It is however not clear whether RTW had already occurred in the workers studied by Dionne, and so these papers did not meet the eligibility criteria for our review. For both prediction rules (Steyerberg 2009; Flynn et al. 2002; Steyerberg et al. 2001), it is not yet clear if their use would improve outcomes for injured workers.
Practicing physicians have considered subgroups of patients that may be more or less responsive to clinical intervention (Kent and Keating 2004, 2005), and studies have supported the impression of differential response to certain therapies based on patient characteristics (Boersma and Linton 2005, 2006; Shaw et al. 2007) or course of disease (Dunn et al. 2006). Identifying clusters or subgroups of patients is an interesting way to determine whether interventions can be more closely tailored to individual workers’ conditions (Shaw et al. 2006). A few studies of LBP have suggested that subgroup-based intervention can improve outcomes (Flynn et al. 2002; Haldorsen et al. 2002; Haldorsen 2003; Childs et al. 2004; Brennan et al. 2006). Shaw et al. have proposed an approach to match intervention strategies to potentially modifiable disability-related risk factors detected early in the course of a significant LBP episode, theoretically when risk factors may be most amenable to modification (Shaw et al. 2006). Their approach is based on a review of reviews of prognostic factors in LBP. The impact of implementing this approach in practice, however, has not been tested.
Another approach is to formally test for subgroup effects in randomised controlled intervention studies to determine effectiveness of interventions for subgroups of patients (Steenstra et al. 2009). Subgroup analysis is often done poorly (Sun et al. 2011) and should adhere to published criteria (Sun et al. 2010). Both of these approaches might be useful as complementary to the prediction rule approach to identify appropriate interventions for workers at high risk for work disability.
The effectiveness of applying a prediction rule is dependent on the quality of the rule and the availability of effective interventions suitable for those identified to be at high risk. The recently published randomised controlled study on the impact of the STarT Back tool shows that using a simple, nine-item tool and referral to appropriate interventions based on risk stratification can lead to significant improvements in care compared to usual physiotherapy care(Hill et al. 2011). The population in this study was mixed with regards to work status. Results on RTW and work productivity were not available when we were writing this chapter, but are considered in the study design (Hay et al. 2008). Although this approach shows to be an improvement to usual care in England, Koes in his commentary states that there is still room for improvement (Koes 2011), since differences might be statistically significant but still relatively small in absolute size.
11 Conclusions and Implications for Practice
In this chapter, we walked through the process of our systematic review and looked at key findings in terms of prediction factors for RTW from acute LBP. The main known prognostic factors for RTW were:
-
Patient’s recovery expectations.
-
Content of care.
-
Disability and pain rating.
-
Radiating pain.
As well, workplace factors such as physical demands, work accommodation and job satisfaction were prognostic factors for RTW.
As noted, the findings from this systematic review will be of interest to all those who play a role in RTW—in particular, policymakers, clinicians, workers’ compensation case managers and medical examiners, and workplace disability prevention and return-to-work practitioners. The findings can be used to inform decision-making in practice.
Applying this new knowledge in practice should be executed in a structured way. The effectiveness of choosing interventions for workers with LBP based on prognostic information for RTW needs to be established, and therefore applying this approach should be done with care.
References
Abenhaim, L., Rossignol, M., Gobeille, D., Bonvalot, Y., Fines, P., & Scott, S. (1995). The prognostic consequences in the making of the initial medical diagnosis of work-related back injuries. Spine, 20(7), 791–795.
Abenhaim, L., & Suissa, S. (1987). Importance and economic burden of occupational back pain: A study of 2,500 cases representative of Quebec. Journal of Occupational Medicine, 29(8), 670–674.
Alexopoulos, E. C., Konstantinou, E. C., Bakoyannis, G., Tanagra, D., & Burdorf, A. (2008). Risk factors for sickness absence due to low back pain and prognostic factors for return to work in a cohort of shipyard workers. European Spine Journal, 17(9), 1185–1192.
Andersson, G. B. J. (1999). Epidemiological features of chronic low-back pain. Lancet, 354(9178), 581–585.
Andersson, G. B., Svensson, H. O., & Oden, A. (1983). The intensity of work recovery in low back pain. Spine, 8(8), 880–884.
Apeldoorn, A. T., Ostelo, R. W., van, H. H., Fritz, J. M., Knol, D. L., van Tulder, M. W., et al. (2011). A Randomized controlled trial on the effectiveness of a classification-based system for sub-acute and chronic low back pain. Spine (Phila Pa 1976), 37(16), 1347–1356.
Assendelft, W. J., Morton, S. C., Yu, E. I., Suttorp, M. J., Shekelle, P. G. (2004). Spinal manipulative therapy for low back pain. Cochrane Database of Systematic Reviews, (1), CD000447.
Baldwin, M. L., Butler, R. J., Johnson, W. G., & Cote, P. (2007). Self-reported severity measures as predictors of return-to-work outcomes in occupational back pain. Journal of Occupational Rehabilitation, 17(4), 683–700.
Bleeker, S. E., Moll, H. A., Steyerberg, E. W., Donders, A. R. T., rksen-Lubsen, G., Grobbee, D. E., et al. (2003). External validation is necessary in, prediction research: A clinical example. Journal of Clinical Epidemiology, 56(9), 826–832.
Boersma, K., & Linton, S. J. (2005). Screening to identify patients at risk: Profiles of psychological risk factors for early intervention. The Clinical Journal of Pain, 21(1), 38–43.
Boersma, K., & Linton, S. J. (2006). Psychological processes underlying the development of a chronic pain problem: A prospective study of the relationship between profiles of psychological variables in the fear-avoidance model and disability. The Clinical Journal of Pain, 22(2), 160–166.
Brennan, G. P., Fritz, J. M., Hunter, S. J., Thackeray, A., Delitto, A., & Erhard, R. E. (2006). Identifying subgroups of patients with acute/subacute “nonspecific” low back pain—Results of a randomized clinical trial. Spine, 31(6), 623–631.
Burdorf, A., Naaktgeboren, B., & Post, W. (1998). Prognostic factors for musculoskeletal sickness absence and return to work among welders and metal workers. Occupational and Environmental Medicine, 55(7), 490–495.
Butterfield, P. G., Spencer, P. S., Redmond, N., Feldstein, A., & Perrin, N. (1998). Low back pain: Predictors of absenteeism, residual symptoms, functional impairment, and medical costs in Oregon workers’ compensation recipients. American Journal of Industrial Medicine, 34(6), 559–567.
Childs, J. D., Fritz, J. M., Flynn, T. W., Irrgang, J. J., Johnson, K. K., Majkowski, G. R., et al. (2004). A clinical prediction rule to identify patients with low back pain most likely to benefit from spinal manipulation: A validation study. Annals of Internal Medicine, 141(12), 920–928.
Dasinger, L. K., Krause, N., Deegan, L. J., Brand, R. J., & Rudolph, L. (2000). Physical workplace factors and return to work after compensated low back injury: A disability phase-specific analysis. Journal of Occupational and Environmental Medicine, 42(3), 323–333.
Dionne, C. E., Bourbonnais, R., Fremont, P., Rossignol, M., Stock, S. R., & Larocque, I. (2005). A clinical return-to-work rule for patients with back pain. Canadian Medical Association Journal, 172(12), 1559–1567.
Dionne, C. E., Bourbonnais, R., Fremont, P., Rossignol, M., Stock, S. R., Nouwen, A., et al. (2006). Determinants of “return to work in good health” among workers with back pain who consult in primary care settings: A 2-year prospective study. European Spine Journal, 16(5), 641–655.
Dionne, C. E., Bourbonnais, R., Fremont, P., Rossignol, M., Stock, S. R., Nouwen, A., et al. (2007). Determinants of “return to work in good health” among workers with back pain who consult in primary care settings: A 2-year prospective study. European Spine Journal, 16(5), 641–655.
Du Bois, M., & Donceel, P. (2008). A screening questionnaire to predict no return to work within 3 months for low back pain claimants. European Spine Journal, 17(3), 380–385.
Du Bois, M., Szpalski, M., & Donceel, P. (2009). Patients at risk for long-term sick leave because of low back pain. The Spine Journal, 9(5), 350–359.
Dunn, K. M., Jordan, K., & Croft, P. R. (2006). Characterizing the course of low back pain: A latent class analysis. American Journal of Epidemiology, 163(8), 754–761.
Engel, G. L. (1977). The need for a new medical model: A challenge for biomedicine. Science, 196(4286), 129–136.
Flynn, T., Fritz, J., Whitman, J., Wainner, R., Magel, J., Rendeiro, D., et al. (2002). A clinical prediction rule for classifying patients with low back pain who demonstrate short-term improvement with spinal manipulation. Spine, 27(24), 2835–2843.
Franklin, G. M., Stover, B. D., Turner, J. A., Fulton-Kehoe, D., & Wickizer, T. M. (2008). Early opioid prescription and subsequent disability among workers with back injuries: The Disability Risk Identification Study Cohort. Spine, 33(2), 199–204.
Fransen, M., Woodward, M., Norton, R., Coggan, C., Dawe, M., & Sheridan, N. (2002). Risk factors associated with the transition from acute to chronic occupational back pain. Spine, 27(1), 92–98.
Fritz, J. M., Childs, J. D., & Flynn, T. W. (2005). Pragmatic application of a clinical prediction rule in primary care to identify patients with low back pain with a good prognosis following a brief spinal manipulation intervention. BMC Family Practice, 6(1), 29.
Frymoyer, J. W., & Cats-Baril, W. L. (1991). An overview of the incidences and costs of low back pain. Orthopedic Clinics of North America, 22(2), 263–271.
Fulton-Kehoe, D., Stover, B. D., Turner, J. A., Sheppard, L., Gluck, J. V., Wickizer, T. M., et al. (2008). Development of a brief questionnaire to predict long-term disability. Journal of Occupational and Environmental Medicine, 50(9), 1042–1052.
Furlan AD, Pennick V, Bombardier C, van Tulder M, Cochrane Back Review Group. (2009). Updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine, 34(18), 1929–1941.
Gatchel, R. J., Polatin, P. B., & Kinney, R. K. (1995a). Predicting outcome of chronic back pain using clinical predictors of psychopathology: A prospective analysis. Health Psychology, 14(5), 415–420.
Gatchel, R. J., Polatin, P. B., & Mayer, T. G. (1995b). The dominant role of psychosocial risk factors in the development of chronic low back pain disability. Spine, 20(24), 2702–2709.
Gluck, J. V., & Oleinick, A. (1998). Claim rates of compensable back injuries by age, gender, occupation, and industry. Do they relate to return-to-work experience? Spine, 23(14), 1572–1587.
Goertz, M. N. (1990). Prognostic indicators for acute low-back pain. Spine, 15(12), 1307–1310.
Grove, W. M., & Lloyd, M. (2006). Meehl’s contribution to clinical versus statistical prediction. Journal of Abnormal Psychology, 115(2), 192–194.
Grove, W. M., Zald, D. H., Lebow, B. S., Snitz, B. E., & Nelson, C. (2000). Clinical versus mechanical prediction: A meta-analysis. Psychological Assessment, 12(1), 19–30.
Hagen, K., & Thune, O. (1998). Work incapacity from low back pain in the general population. Spine, 23(19), 2091–2095.
Haldorsen, E. M. (2003). The right treatment to the right patient at the right time. Occupational and Environmental Medicine, 60(4), 235–236.
Haldorsen, E. M., Grasdal, A. L., Skouen, J. S., Risa, A. E., Kronholm, K., & Ursin, H. (2002). Is there a right treatment for a particular patient group? Comparison of ordinary treatment, light multidisciplinary treatment, and extensive multidisciplinary treatment for long-term sick-listed employees with musculoskeletal pain. Pain, 95(1–2), 49–63.
Haskins, R., Rivett, D. A., & Osmotherly, P. G. (2011). Clinical prediction rules in the physiotherapy management of low back pain: A systematic review. Manual Therapy, 17(1), 9–21.
Hay, E. M., Dunn, K. M., Hill, J. C., Lewis, M., Mason, E. E., Konstantinou, K., et al. (2008). A randomised clinical trial of subgrouping and targeted treatment for low back pain compared with best current care. The STarT Back Trial Study Protocol. BMC Musculoskeletal Disorders, 9, 58.
Herbert, F., Duguay, P., Massicotte, P., & Levy, M. (1996). Revision des categories professionnelles utilisees dans les etudes de I’IRSST portant sur les indicateurs quinquennaux de l’ esions professionnelles (Report No.: (Rep. No. R-137)). Quebec: IRSST.
Heymans, M. W., Anema, J. R., van, B. S., Knol, D. L., van Mechelen, W., & de Vet, H. C. (2009). Return to work in a cohort of low back pain patients: Development and validation of a clinical prediction rule. Journal of Occupational Rehabilitation, 19(2), 155–165.
Heymans, M. W., De Vet, H. C. W., Knol, D. L., Bongers, P. M., Koes, B. W., & van Mechelen, W. (2006). Workers’ beliefs and expectations affect return to work over 12 months. Journal of Occupational Rehabilitation, 16(4), 685–695.
Hill, J. C., Whitehurst, D. G., Lewis, M., Bryan, S., Dunn, K. M., Foster, N. E., et al. (2011). Comparison of stratified primary care management for low back pain with current best practice (STarT Back): A randomised controlled trial. Lancet, 378(9802), 1560–1571.
Hoogendoorn, W. E., van Poppel, M. N., Bongers, P. M., Koes, B. W., & Bouter, L. M. (2000). Systematic review of psychosocial factors at work and private life as risk factors for back pain. Spine, 25(16), 2114–2125.
Inrig, T., Amey, B., Borthwick, C., & Beaton, D. (2012). Validity and reliability of the Fear-Avoidance Beliefs Questionnaire (FABQ) in workers with upper extremity injuries. Journal of Occupational Rehabilitation, 22(1), 59–70.
Kapoor, S., Shaw, W. S., Pransky, G., & Patterson, W. (2006). Initial patient and clinician expectations of return to work after acute onset of work-related low back pain. Journal of Occupational and Environmental Medicine, 48(11), 1173–1180.
Karasek, R., Brisson, C., Kawakami, N., Houtman, I., Bongers, P. M., & Amick, B. (1998). The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. Journal of Occupational Health Psychology, 3(4), 322–355.
Kent, P., & Keating, J. (2004). Do primary-care clinicians think that nonspecific low back pain is one condition? Spine, 29(9), 1022–1031.
Kent, P., & Keating, J. L. (2005). Classification in nonspecific low back pain: What methods do primary care clinicians currently use? Spine, 30(12), 1433–1440.
Koes, B. W. (2011). Management of low back pain in primary care: A new approach; comment. Lancet, 378(9802), 1530–1532.
Krause, N., Dasinger, L. K., Deegan, L. J., Rudolph, L., & Brand, R. J. (2001). Psychosocial job factors and return-to-work after compensated low back injury: A disability phase-specific analysis. American Journal of Industrial Medicine, 40(4), 374–392.
Lambeek, L. C., van Tulder, M. W., Swinkels, I. C., Koppes, L. L., Anema, J. R., & van Mechelen, W. (2011). The Trend in total cost of back pain in the Netherlands in the period 2002 to 2007. Spine (Phila Pa 1976), 36(13), 1050–1058.
Loisel, P., Durand, M. J., Berthelette, D., Vezina, N., Baril, R., Gagnon, D., et al. (2001). Disability prevention—New paradigm for the management of occupational back pain. Disease Management & Health Outcomes, 9(7), 351–360.
Lotters, F., & Burdorf, A. (2006). Prognostic factors for duration of sickness absence due to musculoskeletal disorders. The Clinical Journal of Pain, 22(2), 212–221.
Maniadakis, N., & Gray, A. (2000). The economic burden of back pain in the UK. Pain, 84(1), 95–103.
McGinn, T. G., Guyatt, G. H., Wyer, P. C., Naylor, C. D., Stiell, I. G., & Richardson, W. S. (2000). Users’ guides to the medical literature: XXII: How to use articles about clinical decision rules. Evidence-based medicine working group. Journal of the American Medical Association, 284(1), 79–84.
Meehl, P. E. (1954). Clinical versus statistical prediction. A theoretical analysis and a review of the evidence. Minneapolis: University of Minnsota.
Nordin, M., Skovron, M. L., Hiebert, R., Weiser, S., Brisson, P. M., Campello, M., et al. (1996). Early predictors of outcome. Bulletin of the Hospital for Joint Diseases, 55(4), 204–206.
Pransky, G. S., Verma, S. K., Okurowski, L., & Webster, B. (2006). Length of disability prognosis in acute occupational low back pain: Development and testing of a practical approach. Spine, 31(6), 690–697.
Prkachin, K. M., Schultz, I. Z., & Hughes, E. (2007). Pain behavior and the development of pain-related disability: The importance of guarding. The Clinical Journal of Pain, 23(3), 270–277.
Schultz, I. Z., Crook, J., Berkowitz, J., Milner, R., & Meloche, G. R. (2005). Predicting return to work after low back injury using the psychosocial risk for occupational disability instrument: A validation study. Journal of Occupational Rehabilitation, 15(3), 365–376.
Schultz, I. Z., Crook, J., Meloche, G. R., Berkowitz, J., Milner, R., Zuberbier, O. A., et al. (2004). Psychosocial factors predictive of occupational low back disability: Towards development of a return-to-work model. Pain, 107(1–2), 77–85.
Shaw, W. S., Linton, S. J., & Pransky, G. (2006). Reducing sickness absence from work due to low back pain: How well do intervention strategies match modifiable risk factors? Journal of Occupational Rehabilitation, 16(4), 591–605.
Shaw, W. S., Pransky, G., Patterson, W., Linton, S. J., & Winters, T. (2007). Patient clusters in acute, work-related back pain based on patterns of disability risk factors. Journal of Occupational and Environmental Medicine, 49(2), 185–193.
Stanton, T. R., Hancock, M. J., Maher, C. G., & Koes, B. W. (2010). Clinical prediction rules for musculoskeletal conditions response. Physical Therapy, 90(6), 858–859.
Steenstra, I. A., Knol, D. L., Bongers, P. M., Anema, J. R., van Mechelen, W., & de Vet, H. C. (2009). What works best for whom? An exploratory, subgroup analysis in a randomized, controlled trial on the effectiveness of a workplace intervention in low back pain patients on return to work. Spine (Phila Pa 1976), 34(12), 1243–1249.
Steenstra, I. A., Koopman, F. S., Knol, D. L., Kat, E., Bongers, P. M., de Vet, H. C., et al. (2005a). Prognostic factors for duration of sick leave due to low-back pain in dutch health care professionals. Journal of Occupational Rehabilitation, 15(4), 591–605.
Steenstra, I. A., Verbeek, J. H., Heymans, M. W., & Bongers, P. M. (2005b). Prognostic factors for duration of sick leave in patients sick listed with acute low back pain: A systematic review of the literature. Occupational and Environmental Medicine, 62(12), 851–860.
Steyerberg, E. W. (2009). Clinical prediction models. A practical approach to development, validation, and updating. New York: Springer.
Steyerberg, E. W., Harrell, F. E., Borsboom, G. J. J. M., Eijkemans, M. J. C., Vergouwe, Y., & Habbema, J. D. F. (2001). Internal validation of predictive models: Efficiency of some procedures for logistic regression analysis. Journal of Clinical Epidemiology, 54(8), 774–781.
Sun, X., Briel, M., Busse, J. W., You, J. J., Akl, E. A., Mejza, F., et al. (2011). The influence of study characteristics on reporting of subgroup analyses in randomised controlled trials: Systematic review. British Medical Journal, 342, d1569.
Sun, X., Briel, M., Walter, S. D., & Guyatt, G. H. (2010). Is a subgroup effect believable? Updating criteria to evaluate the credibility of subgroup analyses. British Medical Journal, 340, c117.
Turner, J. A., Franklin, G., Fulton-Kehoe, D., Sheppard, L., Stover, B., Wu, R., et al. (2008). ISSLS prize winner: Early predictors of chronic work disability: A prospective, population-based study of workers with back injuries. Spine (Phila Pa 1976), 33(25), 2809–2818.
Turner, J. A., Franklin, G., Fulton-Kehoe, D., Sheppard, L., Wickizer, T. M., Wu, R., et al. (2006). Worker recovery expectations and fear-avoidance predict work disability in a population-based workers’ compensation back pain sample. Spine, 31(6), 682–689.
van der Weide, W. E., Verbeek, J. H., Salle, H. J., & van Dijk, F. J. (1999). Prognostic factors for chronic disability from acute low-back pain in occupational health care. Scandinavian Journal of Work, Environment & Health, 25(1), 50–56.
van Doorn, J. W. (1995). Low back disability among self-employed dentists, veterinarians, physicians and physical therapists in The Netherlands. A retrospective study over a 13-year period (N = 1,119) and an early intervention program with 1-year follow-up (N = 134). Acta Orthopaedica Scandinavica, 66(Suppl 263), 1–64.
Waddell, G., Newton, M., Henderson, I., Somerville, D., & Main, C. J. (1993). A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain, 52(2), 157–168.
Webster, B. S., Verma, S. K., & Gatchel, R. J. (2007). Relationship between early opioid prescribing for acute occupational low back pain and disability duration, medical costs, subsequent surgery and late opioid use. Spine, 32(19), 2127–2132.
World Health Organization. (2001). International classification of functioning, disability and health. ICF. Geneva. World Health Organization.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Steenstra, I.A., Busse, J.W., Hogg-Johnson, S. (2013). Predicting Return to Work for Workers with Low-Back Pain. In: Loisel, P., Anema, J. (eds) Handbook of Work Disability. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-6214-9_16
Download citation
DOI: https://doi.org/10.1007/978-1-4614-6214-9_16
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-6213-2
Online ISBN: 978-1-4614-6214-9
eBook Packages: MedicineMedicine (R0)