
Abstract
The prevalence of a congenital bicuspid valve (BAV), 1–2 % of the general population, is high enough to warrant attention during auscultation of the heart. BAV occurs as a result of the congenital fusion of the coronary cusps, with the right and left coronary cusps most commonly fused. BAV is most commonly asymptomatic. However, symptoms of BAV are related to the pathologies closely associated with the anomaly, including aortic regurgitation (AR), aortic stenosis (AS), and other aortopathies. An ejection click associated with S1 is most frequently associated with BAVs. In general, clicks that are late, loud, non-varying, and/or apical are likely to be BAV. AR can result and is associated with younger age (less than 40 years of age), while AS is more likely as a patient ages, especially after 50 years of age. To definitively diagnose a BAV, the patient requires an echocardiogram. First degree relatives of an affected individual should be screened for BAV and other thoracic aorta abnormalities.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Bicuspid valve
- Ejection click
- Aortic regurgitation
- Aortic stenosis
- Aortopathies
- Systolic murmur
- Diastolic murmur
1 Key Teaching Points
-
The prevalence of a congenital bicuspid aortic valve (BAV), 1–2 %, is high enough to warrant attention for diagnosis during auscultation of the heart.
-
A BAV can produce a variety of sounds and murmurs and should therefore always be considered as a cause or as a contributor to unexplained heart sounds.
-
An ejection click associated with S1 is frequently associated with BAVs.
-
Aortic regurgitation (AR) can result and is associated with younger age (less than 40 years of age).
-
Aortic stenosis (AS) can result and is more likely as a patient ages, especially after 50 years of age.
-
-
To definitively diagnose a BAV, the patient requires an echocardiogram.
2 Case Description
2.1 History
-
A 52 year old man presents with a known BAV and moderate AR (as diagnosed by echo). He is currently asymptomatic and denies dyspnea and edema.
-
Other significant history is hyperlipidemia, for which he takes atorvastatin, and for hypothyroidism, treated with thyroid hormone replacement therapy.
-
His family history is significant for a brother that had surgery at 2 years old to correct a narrow aortic valve.
2.2 Physical Exam
-
Vital signs: BP 117/73 mmHg, Pulse 72 beats per minute.
-
His jugular venous pressure is normal, his chest is clear to auscultation, he has no abnormal cardiac impulses, and his carotids are notable for normal upstroke.
-
Cardiac auscultation.
-
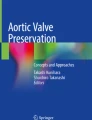
Prominent ejection click at the right sternal border (RSB) and apex that is a grade 3 out of 6 with a normal S1.
-
The patient’s AR is unnoticeable at rest; however, a handgrip accentuates a grade 1 out of 4 holodiastolic murmur at the mid-left sternal border (LSB). The S2 is normal and A2 is intact (Fig. 6.1).
Fig. 6.1 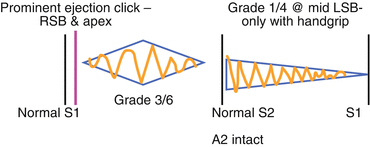
Diagram of the patient’s auscultation findings including a prominent ejection click, a diastolic crescendo decrescendo murmur and systolic decrescendo murmur
-

2.3 Test Results
-
Electrocardiogram is normal (Fig. 6.2).
Fig. 6.2 
Normal electrocardiogram in the setting of BAV
-
Echocardiogram:
-
A BAV can be seen (Fig. 6.3).
Fig. 6.3 
Echocardiogram showing BAV
-
Normal left ventricular size and function.
-
The aortic root diameter is upper normal (3.6 cm).
-
Echo Doppler shows mild AR and mild AS (2.1 m/s).
-


3 Clinical Basics
3.1 Definition
-
Most commonly, a BAV is associated with the congenital fusion of right and left coronary cusps, which is seen in 70–80 % of cases (Fig. 6.4). The other, less common fusion is of the right cusp and the posterior (noncoronary) cusp, which is seen in the other 20–30 % of cases [1].
Fig. 6.4 
There are several types of malformations characteristic of a bicuspid aortic valve
-
Median raphe is typically (60 %) in the conjoint cusp. Differential point for acquired bicuspid AV: Raphe does not reach cusp margin.

3.2 Prevalence
-
BAV is a congenital disorder that affects 1–2 % of the population [2]. Males make up 70–80 % of cases. It is the most prevalent congenital heart abnormality.
3.3 Etiology
-
BAV accounts for approximately half of all cases of AS, with a presentation typically in the 5th–6th decade. It also accounts for about one-fourth of all cases of AR, commonly presenting earlier in life.
-
A 2012 study of patients at necropsy found that 61 % of those with BAV had aortic stenosis [3, 4]. There is a significant association with aortic dilatation, with studies varying from 33 to 79 % prevalence depending on the study criteria. Increased risk for endocarditis has also been associated with BAV [4].
-
There does appear to be a significant genetic component to BAV. One epidemiological study showed a prevalence of 14.6 % of BAV in affected families, which is a much higher rate than the general population [5]. The risk of BAV among 1st degree relatives of an affected individual is 10 % [2]. A family history of BAV should raise suspicions during evaluation.
-
There is also a high association of BAV with other congenital anomalies including aortic coarctation, interrupted aortic arch, and other aortopathies [2].
3.4 Signs and Symptoms
-
Commonly asymptomatic and may be found as an incidental finding on an echo for another reason.
-
Symptoms of BAV are related to the pathologies closely associated with the anomaly, including AR, AS, and aortopathies.
4 Key Auscultation Features
-
There are several key auscultation features associated with BAV [6]. Table 6.1 describes the auscultation characteristics of the anomaly.
Table 6.1 Key auscultation characteristics associated with BAV -
It is important to differentiate between non-pathological splitting of S1 and a true ejection click. A true BAV ejection click is related to the halting of the opening of the aortic valve, and the sound occurs later than a typical split S1 (Fig. 6.5).
Fig. 6.5 
Phonogram of aortic ejection click heard in bicuspid aortic valve. Note the timing of the click relative to M1 and T1, distinguishing it from non-pathological splitting of S1. Note also the loud S2 (Used with permission from Leech et al. [6])
-
One should also note that the auscultatory hallmarks of BAV may vary depending on whether aortic stenosis or regurgitation is present.
-
Auscultation examples of bicuspid aortic valve.
-
Click here to listen to an example of bicuspid aortic valve showing an ejection click, with a mild (15 mmHg) gradient, and see an image of the phonocardiogram (Video 6.1).
-
Click here to listen to an example of an ejection sound, as described by Dr. W. Proctor Harvey (Video 6.2).
-

5 Auscultation Differential Diagnosis
-
It is important to distinguish BAV from other disorders involving an ejection click. There are several pathological processes that may present with an ejection click in addition to BAV. Key elements of the differential diagnosis of an ejection click are listed here:
-
Stiff AV associated with hypertension.
-
Pulmonary hypertension leading to delayed ejection.
-
S4 gallop timing affected by volume and respirations or apical location.
-
Tricuspid valve closure in the setting of right sided volume or pressure overload conditions.
-
Mitral valve prolapse.
-
-
In general, clicks that are late, loud, non-varying, and apical are likely to be from bicuspid AV. However, there is a relatively low positive predictive value of ejection sounds for BAV given the differential listed above. It is important to evaluate family history and determine the presence of the other key auscultatory features.
5.1 Diagnostic Implications of the Auscultation Features
-
The most specific feature for BAV may be the presence of an aortic ejection sound (an ejection “click”). BAV is found in 22 % of ejection clicks [7]. The presence of an ejection click in the absence of any other murmur, such as AS, is mostly likely a non-stenotic BAV [6].
-
Factors that increase the likelihood of BAV [6]:
-
The ejection sound is loud, and the intensity remains constant during expiration.
-
The ejection sound is heard over the entire precordium, and true “splitting” of the S1 is not heard at the apex.
-
The A2 is generally loud.
-
-
-
The aortic ejection sound can be heard from the second right interspace to the apex in a slash pattern [7].
-
In patients with mild AR, an ejection click followed by an early ejection murmur heard loudest in the second right interspace suggests BAV [8].
-
In patients with AS, the click may be difficult to hear at the second left interspace and left sternal border due to a loud AS murmur. The click would be most obvious at the apex [8].
-
-
Due to the high prevalence of AS and AR in patients with BAV, patients with these conditions should be evaluated for BAV by echo.
-
In a study of 152 autopsies of patients with BAV:
-
28 % of all deceased patients with BAV had AS. The likelihood of AS increased as the patients aged with one-third of patients aged 40–60 having evidence of the condition and over two-thirds of patients over age 70 [9].
-
40 % of all deceased patients with BAV had AR. The likelihood was higher amongst younger patients with 64 % of deceased patients 20–29 years old showing evidence of AR. The prevalence of AR in older populations (5th and 6th decades of life) was only one-fourth [9].
-
-
5.2 Prognostic Implications of the Auscultation features
-
Several studies have prospectively followed patients with BAV and reported clinical outcomes (Figs. 6.5 and 6.6).
Fig. 6.6 
Development of cardiac events in patients with BAV. This illustrates the risk of developing a cardiac event over 10 years after confirmed BAV. The risk factors include 30 years or older, moderate/severe aortic regurgitation, and/or moderate/severe aortic stenosis (Used with permission from Tzemos et al. [10])
Fig. 6.7 
Risk of aortic surgery in BAV. This illustrates the Kaplan-Meier risk of aortic surgery over 25 years after a confirmed BAV (Used with permission from Michelena et al. [11])
-
642 ambulatory patients at a Canadian Cardiac Center 1994–2001 followed for a mean period of 9 years [10]:
-
280 patients (45 %) had a dilated aortic sinus and/or ascending aorta [10].
-
161 patients (25 %) suffered from one or more cardiac events [10].
-
142 patients (22 %) required intervention on the ascending aorta or aortic valve [10].
-
11 patients (2 %) suffered from an aortic dissection or aneurysm [10].
-
Predictors of cardiac events included: older than 30 years old, moderate or severe AS, and moderate or severe AR [10].
-
-
416 consecutive patients with BAV in Olmstead County, Minnesota, from 1980 to 1999 with the last follow-up in 2008–2009:
-
2 patients suffered an aortic dissection, which translates to an age-related relative risk of 8.4 compared to the general population of the county. The incidence is still low, but it is much higher than the general population [11].
-
49 patients developed an aneurysm (out of a total of 384 who did not have an aneurysm at baseline), which translates to an age-related risk of 86.2 compared to the general population of the county [11].
-
Over 25 years, the rate of aortic surgery was 25 %, aneurysm formation was 26 %, and valve replacement was 53 % [11].
-
As in the previous study, while morbidity was high, the mortality rate over 25 years was not significantly elevated [11].
-
-
Coarctation of the aorta, as may be detected clinically as differential blood pressures between the upper and lower extremities, represents another congenital abnormality that is associated with BAV in a minority (fewer than 10 %) of individuals, and therefore should be clinically considered.


6 Management
There is no treatment to prevent the progression of this congenital abnormality. Guidelines from ACC/AHA do suggest the following:
-
First degree relatives of an affected individual should be screened for BAV and other thoracic aorta abnormalities [12].
-
Individuals with BAV should be assessed for aortic dilatation with an initial transthoracic echocardiogram [12, 13].
-
Yearly evaluation of aortic dilatation should be undertaken in patients with known BAV (with diameter >4 cm) [13].
-
Surgical repair of the dilatation may be necessary with severe dilatation (>5 cm or 4.5 cm if AR present) [13].
-
Aortic regurgitation (decreased likelihood with aging) and aortic stenosis (increased likelihood with aging) should be evaluated and managed. Additionally, it has been suggested that blood pressure management be emphasized to reduce aortopathy risk with the use of beta blockers [2].
-
Angiotensin II blockade may be a potential future intervention as it has been shown to reduce the rate of aortic root dilation in Marfan’s syndrome [14].
7 Clinical Summary of the Case
The patient, with an apparent family history of aortic valve disease, has typical findings of “mid-stage” bicuspid valve, with a prominent click, yet the early onset of aortic stenosis, and characteristically mild AR. The click is characteristically heard across the precordium. The normal blood pressure suggests against the presence of coarctation. With this established diagnosis, monitoring the patient for progression of AR or AS, and evaluating for associated conditions, such as aortic root enlargement and its consequences is required.
References
Otto C, Bonow R. Valvular heart disease. In: Bono RW, Mann DL, Zipes DP, Libby P, editors. Braunwald’s heart disease: a textbook of cardiovascular medicine. 9th ed. Philadelphia: Elsevier Sanders; 2012. p. 1468–539.
Mordi I, Tzemos N. Bicuspid aortic valve disease: a comprehensive review. Cardiol Res Pract. 2012;2012:196037.
Roberts WC, Vowels TJ, Ko JM. Natural history of adults with congenitally malformed aortic valves (unicuspid or bicuspid). Medicine (Baltimore). 2012;91:287–308.
Della Corte A, Bancone C, Quarto C, et al. Predictors of ascending aortic dilatation with bicuspid aortic valve: a wide spectrum of disease expression. Eur J Cardiothorac Surg. 2007;31:397–404; discussion 404–5.
Emanuel R, Withers R, O'Brien K, Ross P, Feizi O. Congenitally bicuspid aortic valves. Clinicogenetic study of 41 families. Br Heart J. 1978;40:1402–7.
Leech G, Mills P, Leatham A. The diagnosis of a non-stenotic bicuspid aortic valve. Br Heart J. 1978;40:941–50.
Nitta M, Ihenacho D, Hultgren HN. Prevalence and characteristics of the aortic ejection sound in adults. Am J Cardiol. 1988;61:142–5.
Constant J. Bedside cardiology. Philadelphia: Lippincott Williams & Wilkins; 1993.
Fenoglio Jr JJ, McAllister Jr HA, DeCastro CM, Davia JE, Cheitlin MD. Congenital bicuspid aortic valve after age 20. Am J Cardiol. 1977;39:164–9.
Tzemos N, Therrien J, Yip J, et al. Outcomes in adults with bicuspid aortic valves. JAMA. 2008;300:1317–25.
Michelena HI, Khanna AD, Mahoney D, et al. Incidence of aortic complications in patients with bicuspid aortic valves. JAMA. 2011;306:1104–12.
American College of Cardiology Foundation and American Heart Association. Guidelines for the diagnosis and management of patients with thoracic aortic disease: American College of Cardiology Foundation and American Heart Association. J Am Coll Cardiol 2010;55(14):e27–e129.
Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e1–142.
Brooke BS, Habashi JP, Judge DP, Patel N, Loeys B, Dietz 3rd HC. Angiotensin II blockade and aortic-root dilation in Marfan’s syndrome. N Engl J Med. 2008;358:2787–95.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
1 Electronic supplementary material
Below is the link to the electronic supplementary material.
Video 6.1
Bicuspid aortic valve showing an ejection click, with a mild (15 mmHg) gradient (Provided by Robin Winkler Doroshow, MD, Medstar Georgetown University Hospital, Washington, DC) (MP4 1141 kb)
Video 6.2
Ejection sound as described by Dr. W. Proctor Harvey (File 305 from Clinical Cardiology by W. Proctor Harvey, MD, MACC, Jules Bedynek, MD, and David Canfield and published by Laennec Publishing Inc., Fairfield, NJ. Used with permission and copyrighted by Laennec Publishing, Inc. All rights reserved) (MP4 3537 kb)
Rights and permissions
Copyright information
© 2015 Springer-Verlag London
About this chapter
Cite this chapter
Johnson, P.C., DeLuca, M. (2015). Bicuspid Aortic Valve. In: Taylor, A. (eds) Learning Cardiac Auscultation. Springer, London. https://doi.org/10.1007/978-1-4471-6738-9_6
Download citation
DOI: https://doi.org/10.1007/978-1-4471-6738-9_6
Publisher Name: Springer, London
Print ISBN: 978-1-4471-6737-2
Online ISBN: 978-1-4471-6738-9
eBook Packages: MedicineMedicine (R0)