
Abstract
A stethoscope is one of the most basic and essential tool necessary to the practicing clinician. The two types of stethoscopes available to health care workers are the conventional (portable, ergonomic, affordable) and electronic stethoscope (sound amplification/control, virtual display). Despite its importance, no guideline exists for the selection a stethoscope based on acoustic properties. Although scientific literature of stethoscope sound performance is limited, studies suggest no significant difference among acoustic stethoscopes, or between electronic and acoustic stethoscopes. In addition to the development of the electronic stethoscope, promising advancements in the field include wireless auscultation and app based clinical support tools.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Key Teaching Points
-
No gold standard or guideline exists for selecting a stethoscope based on acoustic properties.
-
Acoustic stethoscopes transmit low and high physiological frequencies and are portable and ergonomic.
-
Electronic stethoscopes have a visual display and are capable of volume controlled frequency amplification.
-
Scientific literature of stethoscope sound performance is limited and should be interpreted with caution.
-
In general, the scientific literature suggests there is no statistically significant difference between acoustic stethoscopes.
-
Albeit controversial, most studies have shown no significant difference between electronic or acoustic stethoscopes.
2 Acoustic Stethoscopes
2.1 Basic Structure of Acoustic Stethoscopes (Fig. 3.1)

Acoustic stethoscope
-
The chest piece.
-
The bell is used for low frequency sounds.
-
The diaphragm is used for high frequency sounds.
-
Some chest pieces act as both the bell and diaphragm, with pressure determining function.
-
-
The tube transmits the sound from the chest piece to the ear pieces.
-
Earpieces.
-
A variety exist for the comfort of the wearer.
-
Should always face forward.
-
2.2 Sound and Physiologic Frequencies (Fig. 3.2)

-
Sound is the oscillation of pressure through a medium, such as air. The frequency of a sound wave is perceived as pitch, and the amplitudes at intensity or loudness [1].
-
The average normal hearing range of a person is 20–20,000 Hz [1].
-
The range of clinically important heart and lung sounds is 20–1000 Hz [2]. Systolic murmurs, mitral diastolic murmurs, and S1 – S4 sounds range from 20 to 115 Hz, pericardial rubs, pulmonary regurgitation, and aortic regurgitation range from 140 to 600 Hz [2], while mechanical heart sounds are heard at ranges over 1000 Hz [3].
-
In the clinic and scientific literature, cardiac sounds are commonly characterized using ambiguous terms such as “low” and “high” frequency.
2.3 Characteristics of the Ideal Acoustic Stethoscope
-
Largest ear tips possible for a good seal in the external auditory canal.
-
Adjustable angled metal headpiece.
-
Internally smooth double vinyl tubing.
-
Shorter tubing provides less sound loss in transmission.
-
-
Separate bell and diaphragm.
-
Large diameter bell for low frequencies.
-
Smooth, stiff, and thin diaphragm for high frequencies.
-
2.4 Physical Factors Affecting Sound Transmission
From the patient’s body surface to the earpiece, factors influencing sound transmission include [2]:
-
Thickness of clothing worn by patient [4].
-
Pressure and degree of mechanical contact on the body surface by the chest piece.
-
Size and volume of bell.
-
Surface hardness of the bell cavity.
-
Diaphragm thickness, size, and tautness.
-
Inside diameter of the tube.
-
Rigidity, length, and interior surface smoothness of the tube.
-
Acoustical characteristics of the human ear.
-
Air leaks between components, such as chest piece and body surface or at the ears.
-
Ambient noise limiting auscultation [5].
2.5 Selection of an Acoustic Stethoscope
-
In 1940, a study found that medical professionals choose stethoscopes not based on the acoustic properties of the instrument, but rather on the basis of exterior finish and features, as well as on the recommendation of mentors and peers [2]. This seems true even today.
-
Currently there is no gold standard or guideline in selecting a stethoscope. This is mainly due to limited data. Furthermore, the little evidence available suggests differences may be subtle [2], with unknown clinical relevance.
2.6 Comparisons Between Acoustic Stethoscopes
-
One study by Iversen et al. compared the clinical performances of a high cost advanced stethoscope to a low cost basic stethoscope [6].
-
They used the 3MTM Littmann® Master CardiologyTM stethoscope (3 M, Cerritos, CA, USA) (higher cost and advanced) and the 3MTM Littmann® Classic IITM SE stethoscope (3 M, Cerritos, CA, USA) (lower cost and basic).
-
The two stethoscopes were randomly distributed to 72 house officers without formal training in auscultation in 10 different hospitals. After using the stethoscopes for 4 weeks, participants examined 20 patients (16 with murmurs). Diagnostic accuracy was measure.
-
33 % of patients were diagnosed correctly with the simple scope, while 35 % were diagnosed correctly with the advanced stethoscope (no statistically significant difference).
-
The authors concluded that using a more advance and expensive stethoscope does not improve the rate of murmur detection and diagnosis made by house officers.
-
-
A limited number of articles in recent scientific literature have compared the acoustic properties of different brand stethoscopes [2, 7, 8].
-
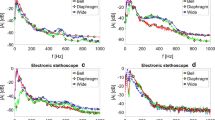
One study [2] analyzed six stethoscopes including the Littmann® Classic IITM (3MTM, St. Paul, MN, USA), the Littmann® Cardiology IITM (3MTM, St Paul, MN, USA), the Littmann® MasterTM (3MTM, St. Paul, MN, USA), the Hewlett-Packard® Rappaport-SpragueTM (Hewlett-Packard®, Palo Alto, CA, USA), the Tycos® HarveyTM Triple Head (Welch Allyn®, Skaneateles Fall, NY, USA), and the Allen® Medical Series 5ATM (Allen®, Acton, MA, USA) (Table 3.1).
Table 3.1 Comparison of six different brand stethoscopes examined by Abella et al. The three diaphragms that amplified the low frequency sounds were all Littmann® (3M, Cerritos, CA, USA) stethoscopes -
The acoustic transfer function (ratio of sound pressure at the earpiece to sound pressure at the chest piece) was used to compare the stethoscopes.
-
At low frequencies (37.5–112.5 Hz), all six bell pieces amplified the sound. Only the three Littmann diaphragms, however, amplified the low frequency sounds. Relative lower performance was statistically significant for Tycos® HarveyTM Triple Head ribbed diaphragm, the Hewlett-Packard® small diaphragm, and the Allen® Medical Series 5ATM diaphragm.
-
At high frequencies (125–1000 Hz), all six bell pieces and diaphragms attenuated but did not amplify the sound. Of the diaphragms, attenuation by the Tycos® HarveyTH Triple Head ribbed diaphragm was statistically significantly lower.
-
The authors concluded the Littmann® Cardiology IITM had the best overall performance. Generally speaking, sound attenuation between stethoscopes was not significantly different.
-
3 Characteristics of Electronic Stethoscopes (Fig. 3.3)

Example of Electronic Stethoscope: 3M™ Littmann® Electronic Stethoscope Model 3200 (Copyright © 3M Littman Stethoscopes, St. Paul, MN, USA. Used with permission)
-
The basic structure of an electronic stethoscope resembles a conventional stethoscope [3].
-
Head and chest piece.
-
Sound transducer.
-
Adjustable gain amplifier.
-
Frequency filters.
-
Mini-speaker.
-
Batteries.
-
-
Some models can be attached to an acoustic stethoscope, converting it into an electronic device [9].
-
The chest piece can be switched from a bell to a diaphragm without interruption in auscultation [10]. Certain models also have an automated mute mode to lessen impact noise [3].
-
Cardiac sounds are transmitted by a wire; therefore, there is no tubular noise or limit on length [3]. Older models may suffer from background electronic noise [3], although newer stethoscopes have the capabilities to filter electronic noise [10].
-
Users can choose whether to amplify all sounds or only certain frequencies, with the user controlling the volume [9, 10]. Ambient noise can be filtered (Littmann.com).
-
Visual display for heart rate, or phonocardiogram (Littmann.com).
-
Cardiac sounds can be recorded and transferred to a computer or Bluetooth device (Littmann.com). Once on a computer, sounds can be played back at various speeds in conjunction with waveform and spectral displays, stored, and compared. This aspect has been used to record cardiac murmurs for transmission via email to a physician for evaluation [11–13].
4 Comparisons Between Acoustic and Electronic Stethoscopes
-
A comparative clinical survey study in the early 1990s found that cardiologists, general practitioners, and nurses preferred acoustic stethoscopes to electronic [3].
-
Three acoustic stethoscopes (Littmann® Cardiology IITM (3MTM,St. Paul, MN, USA), Tycos® Harvey Elite (Welch Allyn®, Arden, NC, USA), and Hewlett-Packard Rappaport-Sprague (Hewlett-Packard®, Andover, MA, USA)) were compared to three electronic stethoscopes (Graham Field® Labtron® (Graham Field®, Hauppage, NY, USA), Bosch® EST40TM (Bosch®, Berlin, Germany), and Starkey Laboratories® ST3TM (Starkey Laboratories®, Minneapolis, MN, USA)) (Fig. 3.4).
Fig. 3.4 
Comparison of six stethoscopes among different health care professionals. The frequency of appreciation is based on the number of times a stethoscope was preferred over the others for each evaluation performed. The acoustic stethoscopes are Littmann® Cardiology IITM (3M, Cerritos, CA, USA), Tycos® HarveyTM Elite (Welch Allyn®, Skaneateles Fall, NY, USA), and Hewlett-Packard® Rappaport-SpragueTM (Hewlett-Packard®, Palo Alto, CA, USA), and the electronic are Graham Field® Labtron® (Graham Field®, Hauppage, NY, USA), Bosch® EST40TM (Bosch®, Berlin, Germany), and Starkey Laboratories® ST3TM (Starkey Laboratories®, Minneapolis, MN, USA) (Tabular portion used with permission from Grenier et al. [3])
-
For each patient examined three stethoscopes were randomly assigned. After three successive auscultations, participants evaluated the stethoscope performance on 13 different criteria ranging from sound attenuation to comfort. Overall 378 comparative evaluations and 1134 auscultations were performed.
-
Acoustic stethoscopes were rated superior 71 % of the time, while electronic were preferred only 29 % of the time.
-
Noted limitations of the acoustic stethoscope included lack of amplification and imperfect attenuation of lower frequency sounds. Subsequently, participants had to apply high pressure on the earpiece to hear.
-
Noted limitations of the electronic stethoscope included electronic noise, as well as sensitivity to impact and ambient sounds, no standard bell and diaphragm filtering, and poor design.
-
-
Another study found no significant difference in observer agreement between clinicians using acoustic stethoscopes (Littmann® Classic II SETM (3MTM, Copenhagen, Denmark) acoustic stethoscope) and those using electronic stethoscopes (Littmann® electronic stethoscope, model 4000TM (3MTM, Copenhagen, Denmark)) [14].
-
Participants included cardiologists, internal medicine practitioners, specialist registrars, senior house officers, house officers, and medical students. The two stethoscopes were randomly and evenly distributed to participants in each group. After using the assigned stethoscope for 4 weeks, 26 patients (1008 examinations) were evaluated by participants in 14 categories, including cardiac and lung sounds.
-
Agreement was statistically stronger between participants using the electronic stethoscope when diagnosing systolic murmurs at the apex of the heart, and lung rhonic sounds compared to agreement between acoustic stethoscope users. Otherwise, there was no significant difference in agreement between the two groups in the other 12 categories, or when combining all sounds.
-
-
Similarly, data shows that using an acoustic or electronic stethoscope in training does not improve performance on cardiac auscultation [15].
-
Of the 48 third year medical students enrolled in a four-month class, half used an acoustic stethoscope of their choice, and half were assigned an electronic stethoscope (Fig. 3.5).
Fig. 3.5 
Comparison of student performance after training with an acoustic stethoscope vs. an electric. No significant difference was found between the two (Tabular portion used with permission from Hoyte et al. [15].)
-
Patients in the study were examined by two cardiologists using acoustic stethoscopes, and afterwards by the medical students. Questionnaires were collected from the students and graded.
-
No significant difference in performance was observed between the group of students using the electronic stethoscope and those using the acoustic.
-
-
Two auscultation studies performed aboard airplanes, however, suggest electronic stethoscopes may improve the subjective perception of cardiac sounds.
-
In both cases the acoustic stethoscope used was a Littmann® Cardiology IIITM (3MTM, St. Paul, MN, USA) stethoscope. The electronic stethoscope was a Littmann® Electronic Stethoscope Model 3000TM (3MTM, St. Paul, MN, USA) in the study aboard a Boeing C135 [16], and a Littmann® Electronic Stethoscope Model 3100TM (3MTM, St. Paul, MN, USA) in the study aboard a Falcon 50 [17]. See Table 3.2.
Table 3.2 Comparison of electronic and acoustic stethoscopes aboard a Boeing C135 and a Falcon 50 (cardiac auscultation) -
On the C135 (88 dB ambient noise), physicians, experienced in medical air transport, made 36 comparative evaluations. Stethoscopes were randomly selected for each patient. A visual rating scale of 1–100 was used to evaluate perception of cardiac and pulmonary sounds. Improved perception of sound when using the electronic stethoscope compared to the acoustic was statistically significant for both cardiac and pulmonary sounds.
-
On the Falcon 50 (77 ± 1 dB ambient noise), 32 comparative evaluations were made by physicians experienced in medical air transport. Participants were blinded with a mask, while an independent physician placed the randomly selected stethoscope on the patient. A rating scale of 0–10 was used to describe perception of sound. On cardiac examination the small perceived improvement using the electronic stethoscope was statistically significant. There was no significant difference in pulmonary sound auscultation using the electronic stethoscope compared to the acoustic.
-


5 Beyond the Stethoscope: Precautions
Ultimately, a stethoscope is only as good as the person using it. In a study, 46 % physicians reporting “good” hearing were shown to have audiometric hearing loss. Increasing age or hearing threshold levels were not a predictor of self-reported stethoscope difficulties; 51 % of participants never took precautions when around loud noises [18]. After finding a stethoscope they are comfortable with, medical personnel should take measures to protect their ear function.
6 Stethoscope Apps
This list is meant to help introduce the reader to app based clinical tools for auscultation; it is not exhaustive and not all apps may be available.
-
3MTM Littmann® SoundBuilder (3MTM, St. Paul, MN, USA) (Free) – 14 lessons on key heart sounds.
-
Thinklabs® iMurmur 2 App (Thinklabs®, Centennial, CO, USA) ($5.99) – 16 cardiac sounds with phonocardiograms and clinical notes.
-
iStethoscope Expert 2013 (Anna Chan) ($0.99) – Assess sounds recorded with the iPhone.
-
Mobile Stethoscope ($3.99) (Keaten House, Ltd,) – Record heart sounds using iPhone; phonocardiogram display.
-
Thinklabs® Stethoscope App (Thinklabs®, Centennial, CO, USA) ($3.99) – Record a cardiac sound with an electronic stethoscope or iphone; real time waveform and spectral display; save, recall, and email.
7 Future of Stethoscopes
-
Wireless auscultation was first developed in the late 1980s to help anesthesiologists monitor patients during surgery [19]. More recently tele-stethoscope systems allow physicians to monitor patients in rural areas [20].
-
An “auscultation jacket” with embedded electronic stethoscopes and processing software was developed for semi-automated diagnosis; this may be especially helpful in underserved regions [21].
8 Conclusions
-
Ironically, the first stethoscope was invented not to improve auscultation, but for a more “aesthetic” reason; namely to avoid the embarrassment of placing one’s ear on a lady’s chest. This legacy is still in existence today as stethoscopes are not chosen based on their acoustic properties.
-
There are few completely objective or blind studies comparing stethoscope performance. Results should be interpreted with caution, especially surveys or comparative studies based on participant opinion.
-
Differences between acoustic stethoscopes are subtle. Using an acoustic or electronic stethoscope does not change clinical outcomes. Because of the limited data, stethoscope selection will probably continue to be based on personal preference.
References
Welsby PD, Earis JE. Some high pitched thoughts on chest examination. Postgrad Med J. 2001;77:617–20.
Abella M, Formolo J, Penney DG. Comparison of the acoustic properties of six popular stethoscopes. J Acoust Soc Am. 1992;91:2224–8.
Grenier MC, Gagnon K, Genest Jr J, Durand J, Durand LG. Clinical comparison of acoustic and electronic stethoscopes and design of a new electronic stethoscope. Am J Cardiol. 1998;81:653–6.
Kraman SS. Transmission of lung sounds through light clothing. Respiration. 2008;75:85–8.
Zun LS, Downey L. The effect of noise in the emergency department. Acad Emerg Med. 2005;12:663–6.
Iversen K, Sogaard Teisner A, Dalsgaard M, et al. Effect of teaching and type of stethoscope on cardiac auscultatory performance. Am Heart J. 2006;152:85.e1–7.
Hampton CS, Chaloner A. Which stethoscope? Br Med J. 1967;4:388–90.
Kindig JR, Beeson TP, Campbell RW, Andries F, Tavel ME. Acoustical performance of the stethoscope: a comparative analysis. Am Heart J. 1982;104:269–75.
Tavel ME. Cardiac auscultation: a glorious past – and it does have a future! Circulation. 2006;113:1255–9.
Wallen RD. Acoustic stethoscopes. Biomed Instrum Technol. 2006;40:367–70.
Dahl LB, Hasvold P, Arild E, Hasvold T. Heart murmurs recorded by a sensor based electronic stethoscope and e-mailed for remote assessment. Arch Dis Child. 2002;87:297–301; discussion 297–301.
Finley JP, Warren AE, Sharratt GP, Amit M. Assessing children’s heart sounds at a distance with digital recordings. Pediatrics. 2006;118:2322–5.
Kamran H, Naggar I, Oniyuke F, et al. Determination of heart rate variability with an electronic stethoscope. Clin Auton Res. 2013;23:41–7.
Iversen K, Greibe R, Timm HB, et al. A randomized trial comparing electronic and conventional stethoscopes. Am J Med. 2005;118:1289.
Hoyte H, Jensen T, Gjesdal K. Cardiac auscultation training of medical students: a comparison of electronic sensor-based and acoustic stethoscopes. BMC Med Educ. 2005;5:14.
Tourtier JP, Libert N, Clapson P, et al. Auscultation in flight: comparison of conventional and electronic stethoscopes. Air Med J. 2011;30:158–60.
Tourtier JP, Fontaine E, Coste S, et al. In flight auscultation: comparison of electronic and conventional stethoscopes. Am J Emerg Med. 2011;29:932–5.
Rabinowitz P, Taiwo O, Sircar K, Aliyu O, Slade M. Physician hearing loss. Am J Otolaryngol. 2006;27:18–23.
Hok B, Bythell V, Bengtsson M. Development of a wireless stethoscope for auscultatory monitoring during anaesthesia. Med Biol Eng Comput. 1988;26:317–20.
Foche-Perez I, Ramirez-Payba R, Hirigoyen-Emparanza G, et al. An open real-time tele-stethoscopy system. Biomed Eng Online. 2012;11:57, 925X-11-57.
Visagie C, Scheffer C, Lubbe WW, Doubell AF. Autonomous detection of heart sound abnormalities using an auscultation jacket. Australas Phys Eng Sci Med. 2009;32:240–50.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag London
About this chapter
Cite this chapter
Braileanu, M., Khan, N. (2015). Stethoscope Performance. In: Taylor, A. (eds) Learning Cardiac Auscultation. Springer, London. https://doi.org/10.1007/978-1-4471-6738-9_3
Download citation
DOI: https://doi.org/10.1007/978-1-4471-6738-9_3
Publisher Name: Springer, London
Print ISBN: 978-1-4471-6737-2
Online ISBN: 978-1-4471-6738-9
eBook Packages: MedicineMedicine (R0)