
Abstract
Management of antiplatelet agents in the perioperative setting is a common clinical challenge. Although discontinuation of aspirin therapy in patients who are taking aspirin for primary or secondary prevention is common, premature cessation of antiplatelet therapy in a patient with a prior drug-eluting stent is the single most important predictor of stent thrombosis, which carries a high morbidity and mortality. Therefore, these patients should ideally continue their antiplatelet therapy throughout surgery. However, this approach to reducing the risk of stent thrombosis must be counterbalanced by the increased risk of surgical bleeding. Multiple factors require evaluation to appropriately balance the risk of stent thrombosis against the risk of surgical bleeding. These include the type and timing of surgery, type and location of coronary stents if present, extent of coronary artery disease, and patient-specific risk factors. In general, for patients with coronary stents, all elective surgeries should be delayed until dual antiplatelet therapy is no longer crucial. Most surgical procedures may be performed on aspirin with acceptable risk of bleeding.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Antiplatelet agents
- Perioperative
- Stent thrombosis
- Coronary stents
- Surgical bleeding
- Percutaneous coronary intervention
Management of antiplatelet agents in the perioperative setting is a challenging clinical dilemma. Antiplatelet agents are widely prescribed in primary and secondary prevention of various cardiovascular diseases such as coronary artery disease (CAD), peripheral arterial disease (PAD), and cerebrovascular disease. Antiplatelet therapy also plays a key role in the management of acute coronary syndromes (ACS). However, their use becomes of paramount importance in patients who have undergone percutaneous coronary intervention (PCI) with stent insertion. In these patients, maintenance of dual antiplatelet therapy (DAPT) is essential for the prevention of stent thrombosis (ST), a catastrophic complication that carries a high morbidity and mortality.
It is estimated that 5 % of patients undergoing PCI will need surgery within 12 months after stent insertion, and 40 % of cases of ST occur in the perioperative setting, often when DAPT is held [1, 2]. Although antiplatelet agents are associated with an increased risk of surgical hemorrhage, the risk of preoperative cessation of antiplatelet drugs may outweigh the risk of surgical bleeding. Therefore, the routine practice of cessation of antiplatelet agents to avoid excess bleeding in patients undergoing surgical procedures should be avoided, and each patient must be managed on a case-by-case basis by balancing the risk of ST against the risk of bleeding.
Antiplatelet Therapy in Coronary Artery Disease
Aspirin, an irreversible cyclooxygenase-1 (COX-1) inhibitor, and clopidogrel, an irreversible ADP-P2Y12 receptor inhibitor, are the most widely prescribed antiplatelet therapies for CAD (Fig. 37.1) [3]. The addition of clopidogrel to aspirin as DAPT yields a synergistic effect, which is superior to aspirin alone in reducing cardiovascular death, myocardial infarction (MI), or stroke in patients with or at risk of CAD [4, 5]. Major bleeding is increased when both agents are used, but the benefit of DAPT outweighs the bleeding risk in patients with ACS [5].

Antiplatelet agents and their target receptors [3]. Abbreviations: GP glycoprotein, PAR protease-activated receptor, ADP adenosine diphosphate, TXA 2 thromboxaneA2. Reprinted by permission from Macmillan Publishers Ltd: Nature Reviews Cardiology 2011;8(10):547–559
Prasugrel and ticagrelor are novel ADP-P2Y12 receptor inhibitors similar to clopidogrel, but with the properties of more rapid onset of action and more consistent platelet inhibition than clopidogrel (Fig. 37.1; Table 37.1). Both prasugrel and ticagrelor are superior to clopidogrel in the reduction of cardiovascular death, MI, stroke, and ST in patients with ACS undergoing PCI. However, prasugrel is associated with an increased risk of major bleeding, including fatal bleeding, compared to clopidogrel [6, 7]. Unlike prasugrel, ticagrelor is a reversible platelet inhibitor and is not associated with a significant increase in the risk of major or fatal bleeding when compared to clopidogrel. Given its reversibility, ticagrelor may prove to be a suitable agent for perioperative use. However, restoration of platelet activity takes 3–4 days after discontinuation. Thus, similar to clopidogrel, ticagrelor should be discontinued at least 5 days prior to surgery.
Antiplatelet Therapy After Percutaneous Coronary Intervention
Percutaneous coronary intervention (PCI) is known to cause endothelial destruction and medial damage which heals by neointimal formation within 2–6 weeks after placement of a bare-metal stent (BMS) [8]. This healing process may be associated with intimal hyperplasia that leads to in-stent restenosis in approximately 16–32 % of cases after BMS [9, 10]. In order to reduce the rate of restenosis, drug-eluting stents (DES) were introduced in 2002. Despite their success in reducing the rate of in-stent restenosis to less than 10 %, the recognition of late and very late ST following DES placement raised many concerns regarding their safety [11]. When a DES is used, re-endothelialization and neointimal healing are delayed resulting in prolonged exposure of thrombogenic stent struts to blood facilitating platelet adherence, aggregation, and thrombus formation within the DES [8, 12]. Complete healing of a DES may take years during which time there is an ongoing risk of late and very late ST [13]. Available data suggest about a 0.6 % incremental risk of ST with DES compared to BMS [14].
According to the 2011 American College of Cardiology Foundation/American Heart Association/Society of Cardiovascular Angiography and Interventions (ACCF/AHA/SCAI) guidelines for PCI, aspirin should be continued indefinitely, and a P2Y12 inhibitor should be given for at least 1 month and up to 12 months after PCI with a BMS and for at least 12 months after PCI with DES [15]. The 2011 updated guidelines for the management of UA/NSTEMI add that in patients with clinical features associated with an increased risk of ST, such as diabetes or renal insufficiency or procedural characteristics such as multiple stents or a treated bifurcation lesion, extension of DAPT beyond 12 months may be reasonable in patients with DES [16].
Stent Thrombosis
Stent thrombosis is a sudden and potentially catastrophic complication after PCI. It usually manifests as an acute MI, generally with ST-segment elevation, malignant arrhythmia, or death. Adding P2Y12 inhibitors to aspirin is the standard of care after PCI with stent insertion as it reduces the rate of early stent thrombosis from 3.5 % with aspirin alone to 0.5 % with DAPT [17]. Although the optimal duration of DAPT is yet to be determined in patients with DES, available data suggest that long-term use of DAPT beyond 12 months may be reasonable for the prevention of very late stent thrombosis [16, 18].
Several risk factors for stent thrombosis with DES have been described (Table 37.2) [8, 19–23]. Early stent thrombosis and subacute stent thrombosis are thought to be related to procedure-related factors. In contrast, the single most important predictor of late and very late stent thrombosis is the premature cessation of DAPT [2, 19, 24, 25].
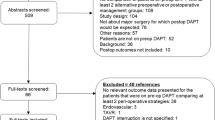
It is estimated that 5 % of patients with coronary stents will undergo a surgical procedure within the first year after PCI [1]. Furthermore, it has been reported that up to 40 % of cases of stent thrombosis with DES occur in the perioperative setting, commonly after the cessation of antiplatelet agents [2]. The increased rate of stent thrombosis in patients undergoing surgery early after PCI (<6 weeks with BMS and <12 months with DES) is likely related to the combination of a postoperative hypercoagulable state with decreased fibrinolysis, superimposed on the prothrombotic milieu of the delayed endothelialization of the stent [26]. In addition, cessation of antiplatelet agents likely triggers a rebound increase in platelet aggregation [27]. In patients with DES, discontinuation of DAPT has been associated with a 90-fold increase in ST and a mortality of 45 % [19]. A 9-fold increase in mortality has been demonstrated if thienopyridines are discontinued within the first 30 days of DES insertion [29]. ST has been shown to occur at a median of 7 days after cessation of DAPT. However, in patients maintained on aspirin with only thienopyridines discontinued, the median time to a coronary event was 122 days (Fig. 37.2) [31].

Cumulative proportion of late stent thrombosis cases among patients who discontinued antiplatelet therapy [31]. (a) Within 1 year of discontinuing antiplatelet therapy. (b) Within 30 days of discontinuing antiplatelet therapy. Abbreviations: ASA acetylsalicylic acid
Perioperative Bleeding with Antiplatelet Therapy
Surgical Bleeding in Patients on Aspirin
A meta-analysis of 50,000 patients undergoing noncardiac surgery demonstrated that continuation of aspirin led to a 50 % increase in the risk of bleeding. However, this increased risk did not translate to a higher level of the severity of bleeding complications except in intracranial surgery and, possibly, transurethral resection of the prostate (TURP) [30]. Moreover, withdrawal of aspirin was associated with a higher incidence of cardiac, cerebral, and peripheral vascular events. In a randomized controlled trial of 220 patients undergoing surgery, maintenance of aspirin was associated with a 7.2 % reduction of acute MI, cardiac arrest, severe arrhythmia, or cardiovascular death within the first 30 postoperative days without an increase in bleeding complications [32].
In general the use of aspirin in dental surgery, anterior chamber ophthalmic surgery, dermatologic surgery, biopsies, and visceral surgery is not associated with an increased risk of bleeding complications or fatal bleeding [30]. Similarly, in patients undergoing gastrointestinal endoscopic procedures including biopsies and polypectomies, the use of aspirin alone has not been associated with an increased risk of bleeding [33]. In urologic surgery, initial reports suggested an increased risk of bleeding in patients undergoing TURP if aspirin was maintained [34]. However, more recent prospective and retrospective studies indicate that even though bleeding following TURP and transrectal prostate biopsy is increased, it is not associated with a need for blood transfusions, particularly if a laser was used [35, 36]. Studies evaluating bleeding in the setting of nephrectomy or radical prostatectomy are lacking. However, the use of robot-assisted radical prostatectomy and nephrectomy on aspirin is not associated with an increased risk of bleeding [37, 38]. In orthopedic surgery, the use of antiplatelet agents has not been associated with significant surgical morbidity or mortality except in orthopedic spinal surgery [30, 39]. In peripheral vascular surgery, aspirin use is associated with increased nonfatal bleeding but a decrease in perioperative mortality [40].
Surgical Bleeding in Patients on DAPT
The effect of DAPT on surgical bleeding has been most studied in cardiac surgery. Low-dose aspirin is associated with a low risk of excessive bleeding following coronary artery bypass surgery [41]. However, the addition of a thienopyridine to aspirin results in a significant increase in bleeding, blood product transfusion, ventilation requirements, length of hospital stay, and surgical re-exploration [42]. For this reason, the American College of Cardiology/American Heart Association/European Society of Cardiology (ACC/AHA/ESC) guidelines recommend that in patients undergoing coronary artery bypass surgery, P2Y12 inhibitors should be withheld at least 5 days and up to 7 days prior to surgery unless the urgency of revascularization outweighs the risks of excess bleeding [18, 43].
Individual reports describe significant and even fatal postoperative hemorrhage with DAPT after vascular, orthopedic, and even endoscopic procedures [44–46]. However, larger studies demonstrate that, even though there is an increase in surgical bleeding and transfusion requirements, there is no change in mortality or surgical outcome [1, 28, 39, 47]. In transbronchial biopsy, the use of DAPT has been associated with significant bleeding in all cases. However, none of these bleeding events were fatal or required transfusions [45]. The use of clopidogrel is contraindicated in regional spinal or epidural anesthesia due to the risk of significant hematomas and spinal cord compression [48]. A prospective study evaluating patients with coronary stents undergoing noncardiac surgery demonstrated a major adverse cardiac event (MACE) rate of 10.9 % and a bleeding complication rate of 9.5 % [49]. Complete cessation of antiplatelet agents was an independent predictor of MACE, whereas the use of antiplatelet agents was not a predictor of bleeding complications.
Collectively the data suggest that most surgical procedures can be performed at low risk on aspirin and potentially on DAPT and that the increased risk of perioperative hemorrhage is not necessarily associated with worsened morbidity, mortality, or surgical outcome. Therefore, the risk of stopping antiplatelet agents in patients with coronary stents might outweigh the risk of continuing them, particularly in high-risk patients.
Strategies for Perioperative Management of Antiplatelet Agents in Patients with Coronary Stents
Any decisions regarding the perioperative management of antiplatelet agents is based on a limited body of evidence. Management of these patients requires an individualized, multidisciplinary approach by the patient’s cardiologist, surgeon, and anesthesiologist. The approach should take into consideration the type of surgery and its bleeding risk, the CAD burden and ischemic risk, the timing of surgery after an event or after PCI, if a DES was used or not, and the presence of concomitant risk factors of ST. Subsequently, the risk of surgical bleeding (Table 37.3) [39] should be weighed against the estimated risk of ST (Fig. 37.3).

Algorithm of perioperative management of patients with coronary stents [66]. Abbreviations: COX cyclooxygenase, BMS bare-metal stents, DES drug-eluting stent(s), NSAID nonsteroidal anti-inflammatory drug, ST stent thrombosis, DAPT dual antiplatelet therapy
Aspirin and P2Y12 Inhibitor Throughout Surgery
American and European Cardiology Society guidelines recommend delaying all elective surgical procedures until the duration of DAPT is completed (Table 37.4) [18, 50–56]. Therefore, as a general approach, all elective procedures should be delayed at least 4–6 weeks after PCI with BMS and 12 months after PCI with DES. According to the 2009 ESC guidelines for preoperative cardiac risk assessment and perioperative cardiac management in noncardiac surgery, elective surgery should be delayed for a minimum of 6 weeks and optimally 3 months after a BMS [52]. However, if surgery cannot be delayed due to urgency, then maintenance of DAPT is of paramount importance as the risk of ST is significantly increased. The 2011 ESC guidelines on the management of non-ST elevation acute coronary syndrome (NSTEACS) state that most surgical procedures can be performed under DAPT or at least aspirin alone with acceptable rates of bleeding and that surgeons should be encouraged to operate under DAPT if bleeding risk is low or moderate [18]. This applies to most surgical procedures, except those in cases in which bleeding can occur in a closed space and could be catastrophic, such as intracranial, spinal, and posterior-chamber ophthalmic surgeries (see Table 37.3).
Discontinue P2Y12 Inhibitor and Maintain Aspirin
The 2011 ESC guidelines for the management of NSTEACS state that interruption of DAPT for urgent surgical procedures 1 month after ACS while continuing aspirin in patients without a DES may be reasonable [18]. Similarly, in patients with a DES without concomitant risk factors of ST undergoing surgery more than 12 months after PCI, P2Y12 inhibitors may be safely discontinued 5–7 days prior to surgery while maintaining aspirin. If risk factors of ST are present and the risk of perioperative bleeding is significantly high, then P2Y12 inhibitors may be discontinued while aspirin is maintained, understanding that the patient is at increased risk of postoperative ST. Following surgery, P2Y12 inhibitors should be started once the risk of bleeding is felt to be sufficiently low (ideally within the first 24 h) with a loading dose of either clopidogrel 300–600 mg, prasugrel 60 mg, or ticagrelor 180 mg. Short-term discontinuation of thienopyridines has been shown to be relatively safe if aspirin is maintained; however, the risk of ST remains elevated [31].
“Bridging Therapy” with Glycoprotein IIb/IIIa Inhibitors
Glycoprotein (GP) IIb/IIIa inhibitors act by blocking fibrinogen-mediated cross-linking of platelets, thereby inhibiting platelet aggregation [57]. Abciximab causes a prolonged irreversible antagonism of GP IIb/IIIa leading to platelet aggregation inhibition that lasts for at least 48 h and up to 7 days and therefore should not be used perioperatively [58]. The synthetic peptides eptifibatide and tirofiban are competitive, reversible binders to GP IIb/IIIa receptors and dissociate rapidly. Their half-life is quite short, and platelet function is completely restored 2–4 h after stopping the infusion, making them potentially suitable for perioperative use [59].
Even though GP IIb/IIIa inhibitors have not been studied extensively in the perioperative setting, their successful use as a “bridge” when P2Y12 inhibitors are stopped before surgery has been reported [60–62]. Two small series of patients, at high risk of both ST and surgical bleeding, demonstrated that bridging with eptifibatide was associated with a favorable postoperative outcome without increased perioperative hemorrhage [61, 62]. Perioperative bridging with tirofiban was evaluated in another prospective study of 30 patients undergoing high bleeding risk surgery within 1–12 months after PCI with DES. There were no MACE, and major bleeding was observed in two patients who did not require surgical re-exploration [60].
For patients with coronary stents who are at an increased risk of perioperative bleeding and a significant risk of ST (e.g., early after PCI) but who require surgery, bridging therapy with aspirin and a GP IIb/IIIa inhibitor could be considered, although limited data exist in support of this strategy. This entails stopping P2Y12 inhibitors 5–7 days before surgery and admitting the patient to the hospital 2–4 days before surgery to begin tirofiban or eptifibatide which is discontinued 6 h before surgery. Importantly, the increased bleeding risk associated with GP IIb/IIIa inhibitor treatment also has to be considered.
Even though this strategy is not practical in most cases and is not considered evidence-based yet, it might be worthwhile in patients at extremely high risk of stent thrombosis. According to the 2010 Cardiac Society of Australia and New Zealand guidelines for the management of antiplatelet therapy in patients with coronary stents undergoing noncardiac surgery, bridging with GP IIb/IIIa inhibitors and heparin can be considered in high-risk patients [63].
Discontinue Aspirin and P2Y12 Inhibitors and Consider Alternatives
If the risk of surgical bleeding is potentially catastrophic or fatal, such as in intracranial, spinal, and posterior-chamber ophthalmic surgeries, aspirin cessation might be necessary. In these cases aspirin and P2Y12 inhibitors should be discontinued 5–7 days before surgery. Given the increased risk of ST with cessation of antiplatelet agents, intensive perioperative monitoring and early interventions are of paramount importance. Moreover, dual antiplatelet therapy should be reintroduced once the risk of hemorrhage is diminished.
Heparin has been considered as a substitute to aspirin or P2Y12 inhibitors. However, heparin is an antithrombin agent, rather than an antiplatelet agent. The use of unfractionated heparin (UFH) and low-molecular-weight heparin (LMWH) has been proposed in the perioperative management of patients with coronary stents [64]. However, data on perioperative heparin use suggest increased mortality [1]. In addition, abrupt cessation of UFH may be associated with a rebound hypercoagulable state [65]. Finally, since ST is a platelet-mediated process, it is expected that antithrombin agents such as UFH and LMWH would not be ideal agents.
Management of Postoperative Stent Thrombosis
Given that ST most often presents as an STEMI, the most appropriate management is early reperfusion therapy. Since thrombolytic therapy is contraindicated postoperatively, due to the excessive bleeding risk, primary PCI is the treatment of choice for perioperative ST.
Conclusion
Management of antiplatelet agents in the perioperative setting remains a common clinical challenge. Premature cessation of antiplatelet therapy is the single most important predictor of ST, which carries a high morbidity and mortality, particularly in the perioperative setting. Therefore, patients ideally should continue their antiplatelet medications throughout surgery to reduce the risk of ST. However, this reduction is accompanied by an increased risk of surgical bleeding. All elective surgeries should be delayed until DAPT is no longer crucial. Most surgical procedures may be performed on aspirin with an acceptable risk of bleeding. However, if the bleeding risk is unacceptable on oral antiplatelets, then bridging with a GP IIb/IIIa inhibitor could be considered.
Key Points
-
All patients with CAD should receive aspirin indefinitely, and a P2Y12 inhibitor (clopidogrel, prasugrel, or ticagrelor) should be added and maintained for at least 1 month and up to 12 months after BMS insertion and for at least 12 months after DES insertion that may be extended beyond 12 months in patients with increased risk of ST.
-
All elective surgical procedures should be delayed until the duration of DAPT is completed (at least 1 month after PCI with BMS and 12 months after PCI with DES).
-
If surgery cannot be delayed due to urgency, then maintenance of DAPT is of paramount importance for the prevention of ST.
-
Most surgical procedures can be performed under DAPT or at least aspirin alone with acceptable rates of bleeding.
-
Interruption of DAPT for necessary surgical procedures 1 month after ACS in patients without a DES may be reasonable.
-
In patients with DES without concomitant risk factors of ST undergoing surgery more than 12 months after PCI, P2Y12 inhibitors may be safely discontinued 5–7 days prior to surgery while maintaining aspirin.
References
Vicenzi MN, et al. Coronary artery stenting and non-cardiac surgery – a prospective outcome study. Br J Anaesth. 2006;96(6):686–93.
Artang R, Dieter RS. Analysis of 36 reported cases of late thrombosis in drug-eluting stents placed in coronary arteries. Am J Cardiol. 2007;99(8):1039–43.
Yousuf O, Bhatt DL. The evolution of antiplatelet therapy in cardiovascular disease. Nat Rev Cardiol. 2011;8(10):547–59.
CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet. 1996;348(9038):1329–39.
Mehta SR, Yusuf S. The clopidogrel in unstable angina to prevent recurrent events (CURE) trial programme; rationale, design and baseline characteristics including a meta-analysis of the effects of thienopyridines in vascular disease. Eur Heart J. 2000;21(24):2033–41.
Wiviott SD, et al. Prasugrel compared with high loading- and maintenance-dose clopidogrel in patients with planned percutaneous coronary intervention: the prasugrel in comparison to clopidogrel for inhibition of platelet activation and aggregation-thrombolysis in myocardial infarction 44 trial. Circulation. 2007;116(25):2923–32.
Wallentin L, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009;361(11):1045–57.
Joner M, et al. Pathology of drug-eluting stents in humans: delayed healing and late thrombotic risk. J Am Coll Cardiol. 2006;48(1):193–202.
Fischman DL, et al. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators. N Engl J Med. 1994;331(8):496–501.
Serruys PW, et al. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. Benestent Study Group. N Engl J Med. 1994;331(8):489–95.
Holmes Jr DR, et al. Stent thrombosis. J Am Coll Cardiol. 2010;56(17):1357–65.
Kotani J, et al. Incomplete neointimal coverage of sirolimus-eluting stents: angioscopic findings. J Am Coll Cardiol. 2006;47(10):2108–11.
Awata M, et al. Serial angioscopic evidence of incomplete neointimal coverage after sirolimus-eluting stent implantation: comparison with bare-metal stents. Circulation. 2007;116(8):910–6.
Mauri L, et al. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med. 2007;356(10):1020–9.
Levine GN, et al. ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58(24):e44–122.
Wright RS, et al. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;57(19):e215–367.
Leon MB, et al. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. Stent Anticoagulation Restenosis Study Investigators. N Engl J Med. 1998;339(23):1665–71.
Hamm CW, et al. ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2011;32(23):2999–3054.
Iakovou I, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005;293(17):2126–30.
Colombo A, Corbett SJ. Drug-eluting stent thrombosis: increasingly recognized but too frequently overemphasized. J Am Coll Cardiol. 2006;48(1):203–5.
Park DW, et al. Frequency of and risk factors for stent thrombosis after drug-eluting stent implantation during long-term follow-up. Am J Cardiol. 2006;98(3):352–6.
Cutlip DE, et al. Stent thrombosis in the modern era: a pooled analysis of multicenter coronary stent clinical trials. Circulation. 2001;103(15):1967–71.
Kuchulakanti PK, et al. Correlates and long-term outcomes of angiographically proven stent thrombosis with sirolimus- and paclitaxel-eluting stents. Circulation. 2006;113(8):1108–13.
Auer J, et al. Risk of noncardiac surgery in the months following placement of a drug-eluting coronary stent. J Am Coll Cardiol. 2004;43(4):713; author reply 714–5.
Kaluza GL, et al. Catastrophic outcomes of noncardiac surgery soon after coronary stenting. J Am Coll Cardiol. 2000;35(5):1288–94.
Camenzind E, Steg PG, Wijns W. Stent thrombosis late after implantation of first-generation drug-eluting stents: a cause for concern. Circulation. 2007;115(11):1440–55; discussion 1455.
Ferrari E, et al. Coronary syndromes following aspirin withdrawal: a special risk for late stent thrombosis. J Am Coll Cardiol. 2005;45(3):456–9.
Sharma AK, et al. Major noncardiac surgery following coronary stenting: when is it safe to operate? Catheter Cardiovasc Interv. 2004;63(2):141–5.
Spertus JA, et al. Prevalence, predictors, and outcomes of premature discontinuation of thienopyridine therapy after drug-eluting stent placement: results from the PREMIER registry. Circulation. 2006;113(24):2803–9.
Burger W, et al. Low-dose aspirin for secondary cardiovascular prevention – cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation – review and meta-analysis. J Intern Med. 2005;257(5):399–414.
Eisenberg MJ, et al. Safety of short-term discontinuation of antiplatelet therapy in patients with drug-eluting stents. Circulation. 2009;119(12):1634–42.
Oscarsson A, et al. To continue or discontinue aspirin in the perioperative period: a randomized, controlled clinical trial. Br J Anaesth. 2010;104(3):305–12.
Boustiere C, et al. Endoscopy and antiplatelet agents. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2011;43(5):445–61.
Watson CJ, et al. Identifiable factors in post-prostatectomy haemorrhage: the role of aspirin. Br J Urol. 1990;66(1):85–7.
Elzayat E, Habib E, Elhilali M. Holmium laser enucleation of the prostate in patients on anticoagulant therapy or with bleeding disorders. J Urol. 2006;175(4):1428–32.
Nielsen JD, et al. The effect of low-dose acetylsalicylic acid on bleeding after transurethral prostatectomy – a prospective, randomized, double-blind, placebo-controlled study. Scand J Urol Nephrol. 2000;34(3):194–8.
Patel VR, et al. Robot-assisted laparoscopic radical prostatectomy: perioperative outcomes of 1500 cases. J Endourol. 2008;22(10):2299–305.
Parikh A, et al. Preoperative aspirin is safe in patients undergoing urologic robot-assisted surgery. J Endourol. 2012;26:852–6.
Chassot PG, Delabays A, Spahn DR. Perioperative antiplatelet therapy: the case for continuing therapy in patients at risk of myocardial infarction. Br J Anaesth. 2007;99(3):316–28.
Neilipovitz DT, Bryson GL, Nichol G. The effect of perioperative aspirin therapy in peripheral vascular surgery: a decision analysis. Anesth Analg. 2001;93(3):573–80.
Sun JC, et al. Should aspirin be discontinued before coronary artery bypass surgery? Circulation. 2005;112(7):e85–90.
Purkayastha S, et al. Does clopidogrel affect outcome after coronary artery bypass grafting? A meta-analysis. Heart. 2006;92(4):531–2.
Hillis LD, et al. ACCF/AHA guideline for coronary artery bypass graft surgery. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collaboration with the American Association for Thoracic Surgery, Society of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;58(24):e123–210.
Chapman TW, et al. Haemorrhage associated with combined clopidogrel and aspirin therapy. Eur J Vasc Endovasc Surg. 2001;22(5):478–9.
Ernst A, et al. Effect of routine clopidogrel use on bleeding complications after transbronchial biopsy in humans. Chest. 2006;129(3):734–7.
Moore M, Power M. Perioperative hemorrhage and combined clopidogrel and aspirin therapy. Anesthesiology. 2004;101(3):792–4.
Wilson SH, et al. Clinical outcome of patients undergoing non-cardiac surgery in the two months following coronary stenting. J Am Coll Cardiol. 2003;42(2):234–40.
Horlocker TT, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA consensus conference on neuraxial anesthesia and anticoagulation). Reg Anesth Pain Med. 2003;28(3):172–97.
Albaladejo P, et al. Non-cardiac surgery in patients with coronary stents: the RECO study. Heart. 2011;97(19):1566–72.
Fleisher LA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 2002 guidelines on perioperative cardiovascular evaluation for noncardiac surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol. 2007;50(17):e159–241.
Grines CL, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. J Am Coll Cardiol. 2007;49(6):734–9.
Poldermans D, et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009;30(22):2769–812.
Bell AD, et al. The use of antiplatelet therapy in the outpatient setting: Canadian Cardiovascular Society guidelines. Can J Cardiol. 2011;27(Suppl A):S1–59.
Douketis JD, et al. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):299S–339.
Douketis JD, et al. Perioperative management of antithrombotic therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e326S–50.
Albaladejo P, et al. Perioperative management of antiplatelet agents in patients with coronary stents: recommendations of a French Task Force. Br J Anaesth. 2006;97(4):580–2.
Frishman WH, et al. Novel antiplatelet therapies for treatment of patients with ischemic heart disease: inhibitors of the platelet glycoprotein IIb/IIIa integrin receptor. Am Heart J. 1995;130(4):877–92.
Faulds D, Sorkin EM. Abciximab (c7E3 Fab). A review of its pharmacology and therapeutic potential in ischaemic heart disease. Drugs. 1994;48(4):583–98.
Kleiman NS. Pharmacokinetics and pharmacodynamics of glycoprotein IIb-IIIa inhibitors. Am Heart J. 1999;138(4 Pt 2):263–75.
Savonitto S, et al. Urgent surgery in patients with a recently implanted coronary drug-eluting stent: a phase II study of ‘bridging’ antiplatelet therapy with tirofiban during temporary withdrawal of clopidogrel. Br J Anaesth. 2010;104(3):285–91.
Bigalke B, et al. Perioperative antiplatelet therapy in patients at risk for coronary stent thrombosis undergoing noncardiac surgery. Clin Res Cardiol. 2009;98(5):335–9.
Chou S, et al. Bridging therapy in the perioperative management of patients with drug-eluting stents. Rev Cardiovasc Med. 2009;10(4):209–18.
Cardiac Society of Australia and New Zealand. Guidelines for the management of antiplatelet therapy in patients with coronary stents undergoing non-cardiac surgery. Heart Lung Circ. 2010;19(1):2–10.
Broad L, et al. Successful management of patients with a drug-eluting coronary stent presenting for elective, non-cardiac surgery. Br J Anaesth. 2007;98(1):19–22.
Dent H, Lekic Z, Vicenzi M. Unfractionated heparin and coronary artery stenting. Br J Anaesth. 2006;97(4):582; author reply 582.
Abualsaud AO, Eisenberg MJ. Perioperative management of patients with drug-eluting stents. JACC Cardiovasc Interv. 2010;3(2):131–42.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this chapter
Cite this chapter
Abualsaud, A.O., Eisenberg, M.J. (2014). Management of Antiplatelet Agents in the Perioperative Setting. In: Stergiopoulos, K., Brown, D. (eds) Evidence-Based Cardiology Consult. Springer, London. https://doi.org/10.1007/978-1-4471-4441-0_37
Download citation
DOI: https://doi.org/10.1007/978-1-4471-4441-0_37
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-4440-3
Online ISBN: 978-1-4471-4441-0
eBook Packages: MedicineMedicine (R0)