
Abstract
One of the most common injuries of the knee joint is a rupture of the anterior cruciate ligament (ACL). Most authors believe that early rehabilitation of patients after ACL reconstruction promotes better treatment outcomes. Less is known about the influence of the time that passes from injury to surgical reconstruction. Therefore, the goal of this study was to assess the dependence of treatment outcomes of ACL on injury-to-reconstruction and reconstruction-to-rehabilitation time lags. The study included 30 patients of the mean age 34 ± 7 years with trauma-related rupture of ACL and its surgical reconstruction. The time range from ligament rupture to its reconstruction was 120–180 days and from reconstruction to rehabilitation was 1–120 days. Postsurgical rehabilitation outcomes were assessed with the Lysholm knee scale and the IKDC 2000 subjective knee evaluation form. The scales were applied before and after rehabilitation. We found distinct improvements in all physical symptoms in the damaged knee joint, regardless of the time elapsed from trauma to ACL reconstruction and from ACL reconstruction to rehabilitation. The beneficial outcomes of rehabilitation were significantly inversely associated with the time elapsing from reconstruction to rehabilitation commencement but failed to depend on the time from ACL rupture to reconstruction. We conclude that rehabilitation should start as early as possible after ACL reconstruction to optimize the beneficial outcomes in terms of functional physical recovery, whereas the injury-to-reconstruction delay is less meaningful to this end.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
The anterior cruciate ligament (ACL) is the most frequently damaged anatomical structure in the knee joint (Anderson et al. 2016; Saka 2014). There are several possible mechanisms of ACL damage. Most often, the injury is caused by crooked or deforming torsional forces acting about the knee joint while the foot is stabilized or by sideward pressure exerted on the loaded limb, with a slight flexion of the knee joint. Young people, actively practicing sport, are most often exposed to ACL injury. Treatment of a ruptured ACL consists of its reconstruction, followed by a comprehensive patient-tailored rehabilitative process, taking into account exercise intensity and pace, extended over several months (Paschos and Howell 2016; Kruse et al. 2012). Rehabilitation programs in individuals with ACL-deficient knees should include proprioceptive and balance exercises, which helps improve outcomes and a return to a full range of knee joint motions (Cooper et al. 2005). A selection of a rehabilitation program depends, to an extent, on coexisting injuries, age, type of activity, and a physical condition of the patient. Studies suggest that post-reconstruction rehabilitation of a patient with ACL injury ought to begin as early as feasible, with the optimum delay of 2–3 days depending on the patient’s condition (Grindem et al. 2015; Beynnon et al. 2005). Differences in the effectiveness of rehabilitation have been noticed, depending on the time of its onset after surgical reconstruction (Kochański et al. 2013; Pasierbiński and Jarząbek 2002), but the exact impact of a delayed start of rehabilitative procedures on recovery performance of patients with an ACL injury and their return to full physical activity is unsettled. In this study, we addressed this issue by examining the dependency on the injury-to-ligament reconstruction and reconstruction-to-rehabilitation time delays of the expected beneficial outcomes of rehabilitation after repair of ACL injury. We found that a shortening of the former, but not the latter, associates with outcomes.
2 Methods
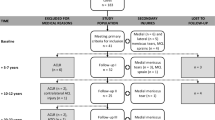
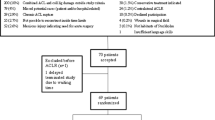
This study gained ethical approval from the Human Research Ethics Committee of the College of Rehabilitation in Warsaw, Poland. The study involved 30 patients (20 men and 10 women) of the mean age 34 ± 7 years who suffered unilateral anterior ACL ruptures, followed by arthroscopically assisted reconstruction. The reconstruction consisted of inserting hamstring autographs made with the semitendinosus and gracilis tendons, a double-bundle (STG-DB) technique (Zaffagnini et al. 2006; Fu et al. 2000). Exclusion criteria were previous knee ligament surgery, additional knee injuries, or leg bone fractures. The time range from ligament rupture to surgical reconstruction was from 120 to 180 days (mean 146 ± 96 days) and from reconstruction to rehabilitation was from 1 to 120 days (mean 66 ± 41 days). Rehabilitation was based on cryotherapy and passive and active kinesiotherapy which had all of the patients. In addition, other forms of physiotherapy treatment, such as laser therapy, magnetotherapy, electrotherapy, or patella mobilization, were variably used in some patients. The patients were assessed twice after surgery, before and after rehabilitation using the Tegner Lysholm Knee Scale-Orthopedic Scores and the 2000 International Subjective Knee Evaluation Form (IKDC 2000). The former is a 100-point scale providing information on how the patient’s symptoms affect his daily life activities. The scale consists of the following domains: pain (25 points), knee instability (25 points), locking (15 points), swelling (10 points), limping (5 points), stair climbing (10 points), squatting (5 points), and requirement for support (5 points) (Lysholm and Gillquist 1982). The main parts of the latter consisted of patient-reported current health assessment (general ailments) form and sports activities evaluation form (Irrgang et al. 2001). The score for the individual items was summed and then transformed to a scale that ranges from 0 to 100. For both scales, the greater is the score, the fewer symptoms and the better outcome.
Data were displayed as means ±SD and 95% confidence intervals. Differences in the surveyed knee symptoms before and after rehabilitation treatment were assessed with a two-tailed paired t-test. Dependence of the treatment outcome on injury-to-reconstruction time and reconstruction-to-rehabilitation time was assessed with Pearson’s correlation coefficients. A p-value <0.05 defined statistically significant differences taking place from before to after rehabilitation. The analysis was conducted using a commercial SPSS Statistics software package (IBM Corp.; Armonk, NY).
3 Results and Discussion
In the main, we noticed that the postsurgical rehabilitation had a highly beneficial effect in patients with reconstructed ACL. There were distinct across-the-board improvements in all physical symptoms depicted in both scales used for the assessment of the damaged knee joint, regardless of the time elapsed from trauma to ACL reconstruction and from ACL reconstruction to rehabilitation. Notably, the Lysholm scale shows a 6.5-fold lessening of pain perception, with the tremendous improvement in the ability to climb stairs and disappearing of knee locking symptoms (Table 1). Likewise, the 2000 IKDC scale confirms the improvement in knee joint damage-related declines in muscle strength and endurance and in general physical health, which is most probably related to increased performance of sports activities (Table 2). All these positive changes were substantial as judged from highly significant increases in the scoring of both surveys.
Our present findings confirm those of other recent studies pointing to the importance of physical rehabilitation, in terms of knee function recovery, in patients after ACL reconstruction (Villa et al. 2016; Imoto et al. 2011; Wright et al. 2008; Frańczuk et al. 2004). The main purpose of postoperative rehabilitation is to relieve pain, restore the full function of the knee and the entire limb, and return to a variety of activities as early as feasible (Kochański et al. 2013).
Uncertainty, however, exists about the influence on the effectiveness of rehabilitation of the time scale between the ligament rupture and reconstructive surgery and between the surgery and rehabilitation commencement. In the present study, we attempted to address this issue by seeking the possible association between the two time scales outlined above and the rehabilitation results assessed by the Lysholm and IKDC 2000 scores. We took advantage of the heterogeneity of patients, each having a different circumstance of the ACL injury, health condition, and health care provided thereafter. A dissimilar timeline of treatment procedures enabled the correlation of outcome benefits with the ligament injury-to-reconstruction and reconstruction-to-rehabilitation time lags. We found that all domains of both Lysholm, except knee joint swelling, and IKDC 2000 scales were significantly inversely associated with the time elapsing from reconstructive surgery to rehabilitation commencement, meaning the shorter the delay to rehabilitation, the better overall physical health outcomes and faster resuming sports activities (Table 3). However, there was no appreciable association between the time elapsing from ACL rupture to reconstructive surgery and the rehabilitation outcomes (Table 4).
In conclusion, we believe we have demonstrated that postoperative rehabilitation should start as early as possible after surgical ACL reconstruction to minimize the effects of injury that caused the ligament rupture. Thus, the present findings lend support to the notion expressed in a recent review of rehabilitation interventions after ACL reconstruction that accelerated rehabilitation may optimize the functional recovery (Grant 2013). On the other hand, we show that a time lag between the injury and undertaking surgical reconstruction is of lesser importance in terms of improved outcome of subsequent rehabilitation. Nonetheless, aggressive rehabilitation does not always bring the intended results. ACL is a sensitive ligament, and too early loading of it can lead to a re-injury (Stańczak et al. 2014). Individually targeted rehabilitation process in different patients, taking into account specific patient-oriented rehabilitation factors, may play a key role in maximizing the expected postsurgical outcomes.
References
Anderson MJ, Browning WM 3rd, Urband CE, Kluczynski MA, Bisson LJ (2016) A systematic summary of systematic reviews on the topic of the anterior cruciate ligament. Orthop J Sports Med 4(3):2325967116634074
Beynnon BD, Uh BS, Johnson RJ, Abate JA, Nichols CE, Fleming BC, Poole AR, Ross H (2005) Rehabilitation after anterior cruciate ligament reconstruction: a prospective, randomized, double-blind comparison of programs administered over 2 different time intervals. Am J Sports Med 33(3):347–359
Cooper RL, Taylor NF, Feller JA (2005) A systematic review of the effect of proprioceptive and balance exercises on people with an injured or reconstructed anterior cruciate ligament. Res Sports Med 13(2):163–178
Frańczuk B, Fibiger W, Kukiełka R, Jasiak-Tyrkalska B, Trąbka R (2004) Early rehabilitation after arthroscopic reconstruction of the anterior cruciate ligament. Ortop Traumatol Rehab 6(4):416–422
Fu FH, Bennett CH, Ma CB, Menetrey J, Menetrey J, Lattermann C (2000) Current trends in anterior cruciate ligament reconstruction: Part II. Operative procedures and clinical correlations. Am J Sports Med January 28:124–130
Grant JA (2013) Updating recommendations for rehabilitation after ACL reconstruction: a review. Clin J Sport Med 23(6):501–502
Grindem H, Granan LP, Risberg MA, Engebretsen L, Snyder-Mackler L, Eitzen I (2015) How does a combined preoperative and postoperative rehabilitation programme influence the outcome of ACL reconstruction 2 years after surgery? A comparison between patients in the Delaware-Oslo ACL Cohort and the Norwegian National Knee Ligament Registry. Br J Sports Med 49(06):385–389
Imoto AM, Peccin S, Almeida GJ, Saconato H, Atallah ÁN (2011) Effectiveness of electrical stimulation on rehabilitation after ligament and meniscal injuries: a systematic review. Sao Paulo Med J 129(6):414–423
Irrgang JJ, Anderson AF, Boland AL Harner CD, Kurosaka M, Neyret P, Richmond JC, Shelborne KD (2001) Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med 29:600–613
Kochański B, Łabejszo A, Kałużny K, Mostowska K, Wołowiec Ł, Trela E, Hagner W, Zukow W (2013) Knee injury – a diagnostic procedure. J Health Sci 3(5):439–456
Kruse LM, Gray B, Wright RW (2012) Rehabilitation after anterior cruciate ligament reconstruction: a systematic review. J Bone Joint Surq Am 94(19):1737–1748
Lysholm J, Gillquist J (1982) Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med 10:150–154
Paschos NK, Howell SM (2016) Anterior cruciate ligament reconstruction: principles of treatment. Efort Open Rev 1(11):398–408
Pasierbiński A, Jarząbek A (2002) Rehabilitation after anterior cruciate ligament reconstruction. Acta Clinica 2(1):86–100
Saka T (2014) Principles of postoperative anterior cruciate ligament rehabilitation. World J Orthop 5(4):450–459
Stańczak K, Domżalski M, Synder M, Sibiński M (2014) Return to motor activity after anterior cruciate ligament reconstruction - pilot study. Ortop Traumatol Rehabil 5(6):477–486
Wright RW, Preston E, Fleming BC, Amendola A, Andrish JT, Bergfeld JA, Dunn WR, Kaeding C, Kuhn JE, Marx RG, McCarty EC, Parker RC, Spindler KP, Wolcott M, Wolf BR, Williams GN (2008) A systematic review of anterior cruciate ligament reconstruction rehabilitation: part I: continuous passive motion, early weight bearing, postoperative bracing, and home-based rehabilitation. J Knee Surg 21(3):217–224
Villa FD, Ricci M, Perdisa F, Filardo G, Gamberini J, Caminati D, Villa SD (2016) Anterior cruciate ligament reconstruction and rehabilitation: predictors of functional outcome. Joints 3(4):179–185
Zaffagnini S, Marcacci M, Lo Presti M, Giordano G, Iacono F, Neri MP (2006) Prospective and randomized evaluation of ACL reconstruction with three techniques: a clinical and radiographic evaluation at 5 years follow-up. Knee Surg Sports Traumatol Arthrosc 14:1060–1069
Conflicts of Interest
The authors declare no conflicts of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Łyp, M., Stanisławska, I., Witek, B., Majerowska, M., Czarny-Działak, M., Włostowska, E. (2018). The Timing of Rehabilitation Commencement After Reconstruction of the Anterior Cruciate Ligament. In: Pokorski, M. (eds) Rehabilitation Science in Context . Advances in Experimental Medicine and Biology(), vol 1096. Springer, Cham. https://doi.org/10.1007/5584_2018_210
Download citation
DOI: https://doi.org/10.1007/5584_2018_210
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-95707-4
Online ISBN: 978-3-319-95708-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)