
Abstract
We have previously presented evidence that the polymorphism of the FCGR3A gene, encoding the receptor for Fc fragment of immunoglobulin G IIIa (FcγRIIIa) plays a role in the enhancement of circulating immune complexes (CIs) with the occurrence of Mycobacterium tuberculosis heat shock proteins in patients with sarcoidosis (SA). The immunocomplexemia might be caused by decreased affinity of CIs to Fcγ receptors, with the subsequently decreased receptor clearance by immune cells. In the present study we examined whether the polymorphisms of other related genes (FCGR2A, FCGR2C, FCGR3B) encoding other activatory Fcγ receptors, could have a similar effect. To this end, we genotyped 124 patients with sarcoidosis and 148 healthy volunteers using polymerase chain reaction with sequence-specific primers. We revealed a significant decrease in the percentage of the FCGR2A and FCGR2C variants that ensure effective CIs clearance, with a concomitant increase of less functional variants of these genes in Stages I/II, compared with Stages III/IV of SA. There was no aberration in FCGR3B allele/genotype frequencies. We conclude that the FCGR2A and FCGR2C polymorphisms may also contribute to immunocomplexemia present in SA. The assessment of FCGR genes could become a tool in presaging a clinical course of sarcoidosis and in its personalized therapy.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Sarcoidosis (SA) is a multisystem, granulomatous disorder of unknown etiology. Infectious, genetic factors, and autoimmunity have been explored as potential causes of SA (American Autoimmune Related Diseases Association 2015; Spagnolo and Grunewald 2013; Baughman et al. 2011; American Thoracic Society et al. 1999). Due to similarities between SA and tuberculosis, Mycobacterium tuberculosis (Mtb) and its antigens, e.g., KatG, A85, SOD2, and heat shock proteins (Mtb-hsps), have been studied as causative factors for sarcoidosis (Dubaniewicz 2013; Dubaniewicz et al. 2012a; Dubaniewicz 2010; Kivity et al. 2009).
Mtb-hsps, involved in the formation of immune complexes (CIs), may be crucial in connecting infection and autoimmunity, both considered in sarcoidosis. Recently, we have shown the presence of immunocomplexemia with the involvement of Mtb-hsps in SA patients, especially of Mtb-hsp16 - the main marker of a dormant stage of mycobacteria. A high level of CIs suggests the occurrence of antigenemia, which may result from the persistent presence of phagocyted mycobacteria releasing Mtb-hsps. Mtb-hsps, in turn, presented through the human leukocyte antigen (HLA) system to T and B lymphocytes would trigger the cellular and humoral immune response (Dubaniewicz 2010; 2013; Dubaniewicz et al. 2012a; Baughman et al. 2011; Kivity et al. 2009). The immunocomplexemia may also be caused by altered elimination of antigen(s) by monocytes/macrophages and neutrophils. Both phagocytosis and clearance of CIs may be disrupted due to dysfunction of receptors, especially for Fc fragments of immunoglobulin G (FcγR): FcγRI, FcγRII, and FcγRIII. We have recently revealed an increased number of blood FcγRI+-, FcγRII+-, and FcγRIII+-monocytes with a higher phagocytic activity in SA patients (Dubaniewicz 2013; Dubaniewicz et al. 2012b). Increased phagocytosis and immunocomplexemia in SA patients may result from dysfunction of FcγRI-III receptors due to their functional polymorphism. To this end we have revealed the FCGR3A-V158F polymorphism, responsible for decreased affinity of FcγRIIIa to CIs and decreased FcγRIIIa clearance in SA (Typiak et al. 2014). Similar findings have been presented by Maertzdorf et al. (2012) who report increased expression of genes connected with FcγR-mediated phagocytosis in SA patients, although the authors did not specify the receptors involved in the process.
The immunocomplexemia also may result from aberrant interaction of neutrophils with FcγRIIa, FcγRIIc and FcγRIIIb receptors, encoded by the polymorphic FCGR2A, FCGR2C, and FCGR3B genes (Behnen et al. 2014; Li et al. 2009; Tutor-Ureta et al. 2006; Schmekel et al. 1985). These receptors are important for the recognition and phagocytosis of IgG-opsonized pathogens, CIs, degranulation, antibody-dependent cell-mediated cytoxicity, release of proinflammatory cytokines, oxidative burst, and apoptosis. It has also been reported that neutrophils are among the first cells to arrive at the site of mycobacterial infection; often an underlying pathogenetic mechanism of sarcoidosis. Therefore, dysfunction of FcγRs on neutrophils may play a role in the CIs-mediated inflammatory process and thus in the induction of autoimmunity in sarcoidosis.
The FCGR2A-H131R, FCGR2C-X57Q, and FCGR3B-NA1/NA2/SH polymorphisms have been detected in different autoimmunological disorders, such as systemic lupus erythematosus, rheumatoid arthritis, and idiopatic thrombocytopenic purpura (Li et al. 2009), but not yet in SA. Therefore, the aim of the current study was to evaluate the polymorphism of these genes in patients with sarcoidosis.
2 Methods
Ethical approval for the study was granted by the Bioethics Committee for Scientific Research of the Medical University of Gdansk, Poland (NKEBN/337/2009). Written informed consent was obtained from the study participants. Recruitment of patients, collection of blood samples, and genotyping all were conducted in the period January 2007 to June 2014.
2.1 Patients
Patients with sarcoidosis were followed by for at least three years to ensure the acquisition of data about disease recurrence and its chronic character (the average follow-up duration amounted to four years). There were 124 untreated patients (69 smokers, 55 non-smokers) with newly diagnosed pulmonary sarcoidosis enrolled into the study (Table 1). The diagnosis of SA was based on histological (scalenobiopsy of lymph nodes), clinical, and radiological evidence. Disease staging was performed using high resolution computed tomography according to the classification of Scadding (1961): Stage I – bilateral hilar lymphadenopathy (38 patients); Stage II – bilateral hilar lymphadenopathy and diffuse pulmonary infiltrations (60 patients); Stage III – diffuse pulmonary infiltrations (20 patients); Stage IV – fibrosis and cavities (6 patients). Twenty five patients had Löfgren’s syndrome. Microbiological and cytological examination of lymph nodes and sputum samples revealed no acid-fast bacilli (PCR, culture of the M. tuberculosis strain), fungi, or atypical cells.
The control group consisted of 148 unrelated healthy volunteers (80 smokers, 68 non-smokers) recruited in the same time period as that for sarcoidosis patients (Table 1). All these individuals had normal chest radiographs, blood and serum analysis, as well as no acid-fast bacilli in sputum smears or sputum cultures of the M. tuberculosis strain. None of the controls or SA patients had a familial history of tuberculosis, sarcoidosis, or autoimmune disease. All participants of the study were free of HIV infection.
2.2 Sample Collection and DNA Isolation
Peripheral blood samples (10 ml) were collected into tubes with EDTA (Becton Dickinson Company, Franklin Lakes, NJ), and were stored at 4 °C for a maximum of 4 h and then at −20 °C for a maximum of one month. In case of patients, blood collection took place before treatment. Subsequently, samples were thawed in room temperature and DNA was isolated using a non-enzymatic method, according to the method of Lahiri and Nurnberger (1991). Analyzes were performed always by the same persons at the Department of Forensic Medicine of the Medical University of Gdansk in Poland.
2.2.1 Polymerase Chain Reaction for FCGR2 Genes Polymorphism
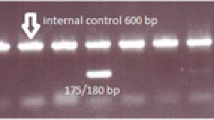
Polymerase chain reaction with the sequence specific primers (PCR-SSP) was used for the gene polymorphism analysis in both groups (Table 2). The FCGR2A-H131R polymorphism, involving A > G at 519 nucleotide position, causing a change in H131R aminoacid in the second extracellular domain of FcɣRIIa, resulting in the presence of two variants of the protein: 131H and 131R (rs1801274) was analyzed. To determine the genotype of a person, two separate PCR-SSP reactions were conducted for the two FCGR2A gene alleles according to the method of Edberg et al. (2002) with modifications, due to the same length of amplified products for 131H and 131R variants (371 bp). We used a reverse primer (5’-TCAAAGTGAAACAACAGCCTGACT-3’) that ensured gene specificity for the FCGR2A and either a forward 131H allele-specific (5’- GGAAAATCCCAGAAATTCACACA-3’) or 131R allele-specific primer (5’-GGAAAATCCCAGAAATTCACACG-3’). To eliminate false negatives, each reaction was supplemented with an internal control of amplification. For this purpose, primers specific for human growth hormone (hGH) gene fragments were used after checking for and excluding unwanted primer interactions. Sequences of the primers for the amplification of the internal control (439 bp) were as follows: a forward primer 5’-CAGTGCCTTCCCAACCATTCCCTTA-3’ and a reverse primer 5’- ATCCACTCACGGATTTCTGTTGTGTTTC-3’.
The PCR-SSP reaction for 131H (519A) allele was performed with 20 ng of genomic DNA in 1x Pol Buffer B, 1.75 mM MgCl2, 0.3 mM of each dNTP, 0.2 μM of the FCGR2A gene-specific and 131H-specific primers, 0.16 μM of both hGH-specific primers and 1.0 U of Taq polymerase (EURx; Gdańsk, Poland) in a total volume of 10 μl. The PCR-SSP reaction for 131R (519G) allele was performed similarly, but with 30 ng of genomic DNA with 0.25 μM of both FCGR2A gene-specific and 131R-specific primers, and 0.32 μM of both hGH-specific primers. A temperature profile for the 131H allele comprised 2 min at 95 °C, 35 amplification cycles (1 min at 94 °C, 1 min of annealing at 56 °C, and 2 min at 72 °C), followed by a final elongation at 72 °C for 10 min. A temperature profile for the amplification of the 131R(519G) allele was identical except for a higher annealing temperature of 57 °C.
The FCGR2C-X57Q polymorphism involving T > C at 202 nucleotide position causing a change from STOP codone to a triplet coding for glutamine in the first extracellular domain of FcɣRIIc, resulting in the presence of two variants of the protein: 57X (a shortened protein in the absence of the other variant) and 57Q (a full-length, functional receptor protein) was analysed (rs1801274). To determine the genotype of a person, two separate PCR-SSP reactions were performed for the two FCGR2C gene alleles according to the method of Su et al. (2002) with modifications, due to the same length of amplified products for 57X (202 T) and 57Q (202C) variants (124 bp). We used a reverse primer (5’- GAGATTCCCATTGTGGACCTACG-3’) that ensured gene specificity for FCGR2C and either a forward 57X allele-specific (5’- GGCTGTGCTGAAACTGGAGACCT-3’) or 57Q allele-specific primer (5’- GGCTGTGCTGAAACTGGAGCCAC–3’). To eliminate false negatives, we supplemented reactions with an internal control of amplification (439 bp). For this purpose, primers specific for the hGH gene fragments were used after checking for and excluding unwanted primer interactions (sequences of the hGH-specific primers were outlined above in the section describing the PCR-SSP for FCGR2A).
The PCR-SSP reaction for 57Q (202C) allele consisted of 10 ng of genomic DNA in 1x Pol Buffer B, 3 mM MgCl2, 0.2 mM of each dNTP, 1 μM of FCGR2C gene-specific and 57Q-specific primers and 1.25 U of Taq polymerase (EURx; Gdansk, Poland), in a total volume of 10 μl. The PCR-SSP for 57X (202 T) allele was performed similarly, but with 0.15 μM of both FCGR2C gene-specific and 57X-specific primers and 1.0 U of Taq polymerase. Both primers for the internal control of amplification (hGH) were added in the proper amount to reach the concentration of 0.1 μM. A temperature profile for the 57Q (202C) allele comprised 5 min at 95 °C, 37 amplification cycles (30 s at 94 °C, 30 s of annealing at 55 °C and 10 s at 72 °C), followed by a final elongation at 72 °C for 7 min. A temperature profile for the amplification of the 57X (202 T) allele was identical except for a higher annealing temperature of 57 °C and a lower number of amplification cycles of 35.
The FCGR3B-NA1/NA2/SH (HNA-1a/HNA-1b/HNA-1c) polymorphism was also analyzed. The NA1 and NA2 alleles differ in five nucleotide positions (C147T/L38L, rs447536 and four mutations leading to the following aminoacid changes: G141C/R36S, rs403016; A227G/N65S, rs448740; G277A/D82N, rs428888; G349A/V106I, rs2290834) in the sequence coding for the first extracellular domain of FcɣRIIIb. The SH allele is similar to NA2, except for one nucleotide (C266A, rs5030738), which, however, changes the sequence of the receptor protein (A78D) in the above mentioned domain.
To determine the genotype of a person, one PCR-SSP reaction was performed for the three FCGR3B gene alleles according to the method of Siriboonrit et al. (2003) with modifications, due to different lengths of amplified products for the NA1 (140 bp), NA2 (219 bp), and SH variants (102 bp). Therefore, the internal control of amplification was unneeded. In every reaction we used a common reverse primer (5’- ATGGACTTCTAGCTGCAC-3’) that ensured gene specificity for FCGR3B, and three forward primers: NA1-specific (5’-CAGTGGTTTCACAATGAGAA-3’), NA2/SH-specific (5’- CAATGGTACAGCGTGCTT-3’), and SH allele-specific primer (5’-TCGAGCTACTTCAT TGACGA-3’).
The PCR-SSP reaction for all three alleles was performed with 10 ng of genomic DNA in 1x Pol Buffer B, 3 mM MgCl2, 0.32 mM of each dNTP, 0,5 μM FCGR3B gene-specific primer, 0.3 μM of NA1-specific, 0.08 μM of NA2/SH-specific and 0.16 μM of SH-specific primers, and 0.5 U of Taq polymerase (EURx; Gdańsk, Poland) in a total volume of 10 μl. A temperature profile for the tested alleles comprised 2 min at 96 °C, 32 amplification cycles (30 s at 96 °C, 1 min of annealing at 63 °C, and 30 s at 72 °C), followed by a final elongation at 72 °C for 5 min.
Due to a close connection of the SH allele to NA2, which differ in only one of six nucleotides that define the allele, the PCR-SSP method used for the FCGR3B gene has a specific limitation. The NA2/SH-specific and FCGR3B gene-specific primers are substrates for the PCR product, which is specific for both NA2 and SH allele (NA2/SH product). It is worth emphasizing that supplementation of the PCR reaction with SH-specific primer allows obtaining a product that is specific only for the SH, and not NA2, variant. In the conjoint presence of both NA2/SH- and SH-specific products, the method cannot differentiate the NA2/SH and SH/SH genotypes. Therefore, two values were given for the frequencies of NA2 and SH alleles, as well as of NA2/SH and SH/SH genotypes.
Electrophoresis of the amplified DNA samples was performed in 14 % polyacrylamide gels (acrylamide-bisacrylamide, 3 % of cross-linking). GeneRuler 100 bp DNA Ladder (Thermo Fisher Scientific, Waltham, MA) was used as a molecular weight marker (range 100–1000 bp). Gels were stained in 0.1 % silver nitrate solution.
2.2.2 Optimization of Methods
Our own contribution to the presented molecular methodology was a creation of a primer for the 57Q (202C) allele of FCGR2C and a changed sequence of the primer for the NA1 allele of FCGR3B, to enhance the specificity of connection of primers with DNA matrix. Further, to eliminate false negatives, we selected an internal control of amplification for the alleles of the FCGR2A and FCGR2C genes. The primers for an internal control were chosen on the basis of similarity of their length and annealing temperature to the primers amplifying the FCGR genes fragments and after excluding unwanted primer interactions (primer-dimer, hairpin structure). The use of internal control of amplification was unneeded in the method created for the FCGR3B gene analysis due to performing the amplification of all three gene alleles in one reaction (a lack of PCR product only in case of amplification error or gene deletion, which did not take place). In the PCR-SSP methods used we optimized the composition of reaction mixture (reaction buffer with ammonium sulfate, suitable concentrations of MgCl2, dNTP, Taq polymerase, DNA, and primers for FCGR genes fragments and internal control of amplification) and temperature profile (annealing temperature, time of amplification steps, and number of amplification cycles). Finally, we also optimized the poliacrylamide gels concentration to achieve a clear distinction of the obtained PCR-products in the range of 100–1000 bp.
2.2.3 Statistical Analysis
The χ 2 test was used to compare the genotype and allele frequencies in the groups studied. Yates’s correction was implemented when a number lower or equal to ten was included in the comparison. Odds ratios with 95 % confidence intervals were calculated for the FCGRs alleles and genotypes tested. Concordance with Hardy-Weinberg equilibrium was confirmed for each FCGR genotype using online software (Rodriguez et al. 2009). A p-value ≤0.05 was considered to indicate significant differences. Statistical elaboration was performed using STATISTICA for Windows ver.10.0 (StatSoft, Tulsa, OK).
3 Results
3.1 FCGR2A Gene
There was no significant difference in the FCGR2A allele or genotype frequency between the SA and control groups. Nor was there any difference in the FCGR2A allele frequency between the particular stages of SA and controls. However, in Stage III of SA, there was a significant increase in the occurrence of 131HH homozygotes and a decrease in 131HR heterozygotes compared with healthy individuals. In Stage II, in contrast, there was a significant decrease in 131HH homozygotes and an increase in the frequency of 131HR heterozygotes. In Stage I, we also found a lower presence of 131HH homozygotes and a higher percentage of 131HR heterozygotes than those in Stage III. Concerning the occurrence of particular genotypes of FCGR2A in patients with Stages I-IV of SA, we found a significant decrease in the percentage of 131HH homozygotes and an increase in 131HR heterozygotes in Stages I/II compared with Stages III/IV (Table 3).
3.2 FCGR2C Gene
There was no significant difference in the FCGR2C allele or genotype frequency between the SA and control groups. In Stage III of SA, there were a significant increase in the occurrence of the 57Q allele and a decrease in the 57X allele compared with healthy individuals. Likewise, in Stages III/IV an increase in the 57Q allele and a decrease in the frequency of the 57X allele were found compared with healthy individuals. In Stages III and III/IV, we found a significant decrease in the percentage of 57XX homozygotes and an increase of 57XQ heterozygotes, which was in contrast to the findings in healthy individuals. In Stages I/II and II, there was a significant decrease in the percentage of 57XQ heterozygotes compared with Stage III. A significant decrease in the frequency of 57XQ heterozygotes was also detected in Stages I/II versus Stages III/IV (Table 4).
3.3 FCGR3B Gene
There were no significant differences in the FCGR3B allele or genotype frequency between the SA and control groups, particular stages of SA and controls, or between SA stages themselves (Table 5).
4 Discussion
In the current study, we found significant differences in the occurrence of alleles and genotypes of the FCGR2A gene in SA patients in Stages III and IV compared with Stages I and II, and with healthy individuals. In Stages III and IV there was a decrease in the frequency of FCGR2A-131HR heterozygotes and an increase in FCGR2A-131HH homozygotes compared with Stages II and II. We also found a lower frequency of FCGR2A-131H allele in Stage II than that in Stage III or IV. Further, a comparative analysis of the FCGR2A-H131R polymorphism in particular stages of SA versus healthy controls revealed an increased frequency of FCGR2A-131H allele and 131HH homozygotes in Stages III and IV. Concerning the FCGR2C-X57Q polymorphism, we found a decrease in the frequency of the 57XQ genotype with 57Q allele in Stages I and II compared with Stages III and IV. Moreover, in contrast to controls, a significant decrease in the frequency of the 57X allele and 57XX genotype, and an increase in the 57Q allele and 57XQ genotype were found in Stages III and IV. However, there were no appreciable differences in the frequency of FCGR3B-NA1/NA2/SH alleles or genotypes of the gene between SA patients and controls.
To the best of our knowledge, it is the first study of the polymorphism of the FCGR2A, FCGR2C, and FCGR3B genes in sarcoidosis and its particular stages; the stages that are, by some authors, considered as composing separate disease entities. However, studies of these genetic variations were performed in other autoimmune disorders, such as systemic lupus erythematosus (SLE), idiopathic trombocytic purpura (IPP), systemic sclerosis, rheumatoid arthritis (RA), idiopathic pulmonary fibrosis (IPF), granulomatosis with polyangiitis, giant cell arthritis (GCA), anti-glomerular basement membrane antibody disease, Kawasaki disease, microscopic polyangiitis, antiphospholipid syndrome, Sjögren’s syndrome, Behçet's disease, Guillain-Barré syndrome (GBS), colitis ulcerosa, Crohn's disease, and myasthenia gravis (Li et al. 2014; Vigato-Ferreira et al. 2014; Wang et al. 2014; Haldorsen et al. 2013; Ji et al. 2013; Sanchez et al. 2011; Bournazos et al. 2010; Weersma et al. 2010; Asano et al. 2009; Bournazos et al. 2009; Li et al. 2009; Aksu et al. 2008; Morgan et al. 2006a; Morgan et al. 2006b; Hughes et al. 2004; Radstake et al. 2003; Manger et al. 2002).
In line with the present results concerning Stages I and II of SA, a decrease in the frequency of the FCGR2A-131HH genotype, with a simultaneous increase in 131RR homozygotes, was reported in SLE and GCA. The FCGR2A-131RR genotype has also been linked to earlier development of SLE and lupus nephritis. Further, the FCGR2A-131RR genotype, along with the presence of HLA-DRB1*04 allele, has been associated with a six-fold increase in the risk of developing GCA in Spanish patients, compared with individuals with the FCGR2A-131HH and 131HR genotype and a lack of DRB1*04 allele (Morgan et al. 2006a). Increased risk of disease development has also been reported in individuals having the FCGR2A-131R in GCA, SLE, antiphospholipid syndrome, ITP, granulomatosis with polyangiitis, and in RA (Vigato-Ferreira et al. 2014; Sanchez et al. 2011; Bournazos et al. 2009; Li et al. 2009; Morgan et al. 2006b; Manger et al. 2002), akin to what we found in Stage II of SA patients of the present study. In contrast to our results, however, the presence of FCGR2A-131R allele has been linked to a more severe course of disease in RA, myasthenia gravis, and in some patients with SLE. Increases in the frequency of 131H variant, like in our patients with Stage III of SA, and in 131HH homozygotes, like in our patients with Stages III and IV of SA have been reported in colitis ulcerosa, Crohn's disease, GBS, childhood-onset ITP, and in Chinese patients with Kawasaki disease (Wang et al. 2014; Ji et al. 2013; Weersma et al. 2010; Asano et al. 2009; Bournazos et al. 2009). In patients with Guillain-Barré syndrome having the FCGR2A-131HH genotype, increased risk of disease development has been reported, compared with individuals having the FCGR2A-131RR or 131HR genotype, which corresponds to our patients in advanced Stages III and IV of SA. However, some investigations of a genetic predisposition to develop RA in Caucasian and Asian populations, in European patients with systemic sclerosis, Japanese patients with microscopic polyangiitis, Greek patients with Kawasaki disease, and in Scandinavian patients with Sjögren’s syndrome failed to connect the FCGR2A-H131R polymorphism to risk of disease development (Haldorsen et al. 2013; Bournazos et al. 2009; Radstake et al. 2003).
In a study on the FCGR2C-X57Q polymorphism in ITP patients versus healthy controls, increased percentage of the 57Q allele and 57XQ genotype has been reported (Bournazos et al. 2009), which corresponds to our patients with advanced Stages III and IV of SA. Likewise, the present results are in line with those concerning the FCGR3B-NA1/NA2/SH polymorphism reported in Chinese patients with anti-GBM disease, the majority of patients with RA and SLE from Europe and Asia, in Indian patients with GBS, and in Scandinavian patients with Sjögren’s syndrome, where no association was revealed between this genetic variation and risk of disease development (Haldorsen et al. 2013; Li et al. 2009; Radstake et al. 2003; Manger et al. 2002). On the other hand, in Dutch and Norwegian patients with GBS, Spanish patients with RA, in Turkish patients with Behçet's disease, or in Asian populations suffering from SLE, higher risk of disease development has been reported in those having the NA2 allele or NA2/NA2 genotype (Bournazos et al. 2009; Aksu et al. 2008; Morgan et al. 2006a). Some authors, however, have reported a decrease in the frequency of this genotype in Korean patients with SLE (Li et al. 2009). The FCGR3B-NA2 allele is linked to increased susceptibility to concomitant respiratory infections in some RA patients (Hughes et al. 2004). In contrast, increased frequency of the NA1 allele and NA1/NA1 genotype reported in patients with IPF plays a mitigating role in disease progression. A similar advantageous predisposition is reported in ITP patients having the FCGR3B-NA1 variant, whereas in patients with myasthenia gravis this variant seems associated with more severe disease course (Bournazos et al. 2010).
In the autoimmune disorders above outlined, the FCGR2A-H131R polymorphism affects FcɣRIIa affinity to IgG2, phagocytosis, and CIs clearance. The FcɣRIIa, with histidine (131H) in the second extracellular domain of the receptor protein, binds IgG2-CIs more effectively than the FcɣRIIa with arginine in this site (131R). Therefore, decreased presence of the 131H allele and 131HH genotype in Stages I and II of SA may lead to lower binding of IgG2 with bacteria or antigen in immune complexes, lower phagocytosis and clearance of CIs by monocytes/macrophages and neutrophils, and in consequence antigenemia and immunocomplexemia. As a result, an excessive (auto)immune, granulomatous reactions may arise in affected organs. Likewise, these reactions can be triggered by lower frequency of the 57Q allele of FCGR2C noted in our patients in Stages I and II of SA, since this allele shapes the expression of a full-length, functional FcɣRIIc receptor and effective CIs binding. In contrast, 57X allele produces a truncated, nonfunctional receptor protein. On the other hand, increased frequency of the FCGR2C-131H and FCGR2C-131HH variants in advanced Stages III and IV of SA may enhance FcγRIIa affinity to IgG2, its binding to bacteria or antigen, which accelerates CIs clearance. All these phenomena have been previously reported in SA patients (Dubaniewicz 2010; 2013; Dubaniewicz et al. 2012a; b; Bournazos et al. 2009; Kivity et al. 2009; Li et al. 2009).
After absorption of bacteria or antigen through FcγRIIa, their presence in phagocytes of SA patients is extended due to lower bactericidal activity of phagocytes, compared with tuberculosis patients. A dormant presence of M. tuberculosis in a phagocyte would subsequently cause heat shock protein secretion from both bacterial and host cells, which may cause extended antigenemia and immunocomplexemia with the subsequent (auto)antigen presentation to T and B lymphocytes in the context of HLA, their increased activation, proliferation, and formation of a sarcoid granuloma (Dubaniewicz et al. 2012a; Dubaniewicz 2010). Further, IgG2, through C1q binding, would initiate a classical pathway of complement activation, which greatly accelerates inflammatory reactions, present especially in patients with Stages III and IV of SA (Li et al. 2009). Increased occurrence of the 57Q allele and 57XQ genotype of FCGR2C, with the 57Q functional allele, in our patients with advanced Stages III and IV of SA, may also enhance phagocytosis of CIs by monocytes/macrophages and neutrophils and lead to excessive Hsp production, antigen presentation, and lymphocyte over-proliferation, causing granulomatous formation (Dubaniewicz et al. 2012b). Increased frequency of the NA1 allele of FCGR3B, with higher affinity to IgG1 and IgG3 bound in CIs, compared with the NA2 and SH alleles, could also enhance inflammatory processes accompanied by abundant neutrophil involvement (Bournazos et al. 2009; Li et al. 2009). Since the distribution of the NA1/NA2/SH variants of FCGR3B remained basically unchanged in the patients of the present study, the FCGR2A and FCGR2C polymorphisms found, and that of FCGR3A previously reported, may drive the excessive (auto)immune response in sarcoidosis (Typiak et al. 2014). This plausibility is supported by the finding that FcγRIIa, but not FcγRIIIb, induces L-selectin shedding of neutrophils to enable their arrival at the site of infection (Kocher et al. 1997). Additionally, solely FγRIIa-mediated neutrophil interactions with CIs result in the formation of neutrophil extracellular traps in tissues, a proinflammatory process that is linked to autoimmunity (Chen et al. 2012).
Differences in the allele and genotype distribution concerning the FCGR2A and FCGR2C genes may suggest the presence of different pathomechanisms underlying less severe Stages I/II and more advanced, parenchymal Stages III/IV of sarcoidosis. Furthermore, variations in the distribution of polymorphic FCGR2A, FCGR2C, along with the previously reported FCGR3A, may explain the immunocomplexemia combined with the presence of Fcɣ receptors on the surface of phagocytes, observed in patients with sarcoidosis. The genotyping analysis may help anticipate the clinical run of sarcoidosis, i.e., the transition from initial mild to later advanced phases, and thus may help personalize therapy.
References
Aksu K, Kitapcioglu G, Keser G, Berdeli A, Karabulut G, Kobak S, Ozmen M, Inal V, Kabasakal Y, Oksel F, Kocanaogullari H, Doganavsargil E (2008) FcgammaRIIa, IIIa and IIIb gene polymorphisms in Behçet’s disease: do they have any clinical implications? Clin Exp Rheumatol 26:S77–83
American Autoimmune Related Diseases Association (2015) List of autoimmune and autoimmune-related diseases. Available from: www.aarda.org/autoimmune-information/list-of-diseases. Accessed on 11 June 2015
American Thoracic Society, European Respiratory Society, World Association of Sarcoidosis and Other Granulomatous Disorders (1999) Statement on sarcoidosis. Am J Respir Crit Care Med 160:736–755
Asano K, Matsushita T, Umeno J, Hosono N, Takahashi A, Kawaguchi T, Matsumoto T et al (2009) Genome-wide association study identifies three new susceptibility loci for ulcerative colitis in the Japanese population. Nat Genet 41:1325–9
Baughman R, Culver D, Judson M (2011) A concise review of pulmonary sarcoidosis. Am J Respir Crit Care Med 183:573–581
Behnen M, Leschczyk C, Moller S, Batel T, Klinger M, Solbach W, Laskay T (2014) Immobilized immune complexes induce neutrophil extracellular trap release by human neutrophil granulocytes via FcγRIIIB and Mac-1. J Immunol 193:1954–65
Bournazos S, Bournazou I, Murchison JT, Wallace WA, McFarlane P, Hirani N, Simpson AJ, Dransfield I, Hart SP (2010) Fcγ receptor IIIb (CD16b) polymorphisms are associated with susceptibility to idiopathic pulmonary fibrosis. Lung 188:475–81
Bournazos S, Woof J, Hart S, Dransfield I (2009) Functional and clinical consequences of Fc receptor polymorphic and copy number variants. Clin Exp Immunol 157:244–54
Chen K, Nishi H, Travers R, Tsuboi N, Martinod K, Wagner DD, Stan R, Croce K, Mayadas TN (2012) Endocytosis of soluble immune complexes leads to their clearance by FcγRIIIB but induces neutrophil extracellular traps via FcγRIIA in vivo. Blood 120:4421–31
Dubaniewicz A (2010) Mycobacterium tuberculosis heat shock proteins and autoimmunityin sarcoidosis. Autoimmun Rev 9:419–24
Dubaniewicz A (2013) Microbial and human heat shock proteins as ‘danger signals’ in sarcoidosis. Hum Immunol 74:1550–8
Dubaniewicz A, Holownia A, Kalinowski L, Wybieralska M, Dobrucki IT, Singh M (2012a) Is mycobacterial heat shock protein 16 kDa, a marker of the dormant stage of Mycobacterium tuberculosis, a sarcoid antigen? Hum Immunol 74:45–51
Dubaniewicz A, Typiak M, Wybieralska M, Szadurska M, Nowakowski S, Staniewicz-Panasik A, Rogoza K, Sternau A, Deeg P, Trzonkowski P (2012b) Changed phagocytic activity and pattern of Fcɣ and complement receptors on blood monocytes in sarcoidosis. Hum Immunol 73:788–4
Edberg JC, Langefeld CD, Wu J, Moser KL, Kaufman KM, Kelly J, Bansal V, Brown WM, Salmon JE, Rich SS, Harley JB, Kimberly RP (2002) Genetic linkage and association of Fcγ receptor IIIA (CD16A) on chromosome 1q23 with human systemic lupus erythematosus. Arthritis Rheum 46:2132–40
Haldorsen K, Appel S, Le Hellard S, Bruland O, Brun JG, Omdal R, Kristjansdottir G et al (2013) No association of primary Sjögren’s syndrome with Fcγ receptor gene variants. Genes and Immunity 14:234–7
Hughes LB, Criswell LA, Beasley TM, Edberg JC, Kimberly RP, Moreland LW, Seldin MF, Bridges SL (2004) Genetic risk factors for infection in patients with early rheumatoid arthritis. Genes and Immunity 5:641–7
Ji Y, Zhang H, Lin S (2013) Single nucleotide polymorphism of FCGR2A gene in Han Chinese children with Kawasaki disease. Chinese Journal of Contemporary Pediatrics 15:196–200
Kivity S, Agmon-Levin N, Blank M, Shoenfeld Y (2009) Infections and autoimmunity – friends or foes? Trends Immunol 30:409–14
Kocher M, Siegel M, Edberg J, Kimberly R (1997) Cross-linking of Fc gamma receptor IIa and Fc gamma receptor IIIb induces different proadhesive phenotypes on human neutrophils. J Immunol 159:3940–8
Lahiri D, Nurnberger J Jr (1991) A rapid non-enzymatic method for the preparation of HMW DNA from blood for RFLP studies. Nucleic Acids Res 19:5444
Li R, Peng H, Chen GM, Feng CC, Zhang YJ, Wen PF, Qiu LJ, Leng RX, Pan HF, Ye DQ (2014) Association of FCGR2A-R/H131 polymorphism with susceptibility to systemic lupus erythematosus among Asian population: a meta-analysis of 20 studies. Arch Dermatol Res 306:781–91
Li X, Ptacek T, Brown E, Edberg JC (2009) Fcɣ receptors: structure, function and role as genetic risk factors in SLE. Genes and Immunity 10:380–9
Maertzdorf J, Weiner J 3rd, Mollenkopf HJ, TBornot TB, Network, Bauer T, Prasse A, Muller-Quernheim J, Kaufmann SH (2012) Common patterns and disease-related signatures in tuberculosis and sarcoidosis. Proc Natl Acad Sci USA 109:7853–7858
Manger K, Repp R, Jansen M, Geisselbrecht M, Wassmuth R, Westerdaal NA, Pfahlberg A, Manger B, Kalden JR, van de Winkel JG (2002) Fcgamma receptor IIa, IIIa, and IIIb polymorphisms in German patients with systemic lupus erythematosus: association with clinical symptoms. Ann Rheum Dis 61:786–92
Morgan AW, Barrett JH, Griffiths B, Subramanian D, Robinson JI, Keyte VH, Ali M et al (2006a) Analysis of Fcγ receptor haplotypes in rheumatoid arthritis: FCGR3A remains a major susceptibility gene at this locus, with an additional contribution from FCGR3B. Arthritis Research & Therapy 8:R5
Morgan AW, Robinson JI, Barrett JH, Martin J, Walker A, Babbage SJ, Ollier WE, Gonzalez-Gay MA, Isaacs JD (2006b) Association of FCGR2A and FCGR2A-FCGR3A haplotypes with susceptibility to giant cell arteritis. Arthritis Research & Therapy 8:R109
Radstake T, Petit E, Pierlot C, van de Putte LB, Cornelis F, Barrera P (2003) Role of Fcgamma receptors IIA, IIIA, and IIIB in susceptibility to rheumatoid arthritis. J Rheumatol 30:926–33
Rodriguez S, Gaunt T, Day I (2009) Hardy–Weinberg equilibrium testing of biological ascertainment for Mendelian randomization studies. Am J Epidemiol 169:505–14
Sanchez E, Comeau ME, Freedman BI, Kelly JA, Kaufman KM, Langefeld CD, Brown EE et al (2011) Identification of novel genetic susceptibility loci in African American lupus patients in a candidate gene association study. Arthritis Rheum 63:3493–3501
Scadding JG (1961) Prognosis of intrathoracic sarcoidosis in England. Br Med J 2:1165–72
Schmekel B, Hakansson L, Hallgren R, Nou E, Stalenheim G, Venge P (1985) Neutrophil phagocytosis in sarcoidosis. Reduced C3b receptor-mediated phagocytosis in active and silent sarcoidosis. Clin Exp Immunol 60:191–5
Siriboonrit U, Tsuchiya N, Sirikong M, Kyogoku C, Bejrachandra S, Suthipinittharm P, Luangtrakool K et al (2003) Association of Fcγ receptor IIb and IIIb polymorphisms with susceptibility to systemic lupus erythematosus in Thais. Tissue Antigens 61:374–83
Spagnolo P, Grunewald J (2013) Recent advances in the genetics of sarcoidosis. J Med Genet 50:290–7
Su K, Wu J, Edberg JC, McKenzie SE, Kimberly RP (2002) Genomic organization of classical human low-affinity Fcγ receptor genes. Genes Immunity 3:S51–6
Tutor-Ureta P, Citores MJ, Castejon R, Mellor-Pita S, Yebra-Bango M, Romero Y, Vargas JA (2006) Prognostic value of neutrophils and NK cells in bronchoalveolar lavage of sarcoidosis. Cytometry Part B Clin Cytometry 70:416–22
Typiak M, Rabala K, Dudziak M, Dubaniewicz A (2014) Polymorphism of FCGR3A gene in sarcoidosis. Hum Immunol 75:283–8
Vigato-Ferreira IC, Toller-Kawahisa JE, Pancoto JA, Mendes-Junior CT, Martinez EZ, Donadi EA, Louzada-Júnior P, Del Lama JE, Marzocchi-Machado CM (2014) FcγRIIa and FcγRIIIb polymorphisms and associations with clinical manifestations in systemic lupus erythematosus patients. Autoimmunity 47:451–8
Wang D, Hu S, Cheng X, Yang JY (2014) FCGR2A rs1801274 polymorphism is associated with risk of childhood-onset idiopathic (immune) thrombocytopenic purpura: evidence from a meta-analysis. Thromb Res 134:1323–7
Weersma RK, Crusius JB, Roberts RL, Koeleman BP, Palomino-Morales R, Wolfkamp S, Hollis-Moffatt JE et al (2010) Association of FcgR2a, but not FcgR3a, with inflammatory bowel diseases across three Caucasian populations. Inflamm Bowel Dis 16:2080–9
Acknowledgements
The study was funded by the Ministry of Science and Higher Education and the National Science Centre in Poland (grant number 5160/B/P01/2010/39). The funding source had no role in the study design, collection, analysis, and interpretation of data.
Conflicts of Interest
The authors declare no conflicts of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Typiak, M., Rębała, K., Dudziak, M., Słomiński, J.M., Dubaniewicz, A. (2015). Polymorphism of FCGR2A, FCGR2C, and FCGR3B Genes in the Pathogenesis of Sarcoidosis. In: Pokorski, M. (eds) Respiratory Contagion. Advances in Experimental Medicine and Biology(), vol 905. Springer, Cham. https://doi.org/10.1007/5584_2015_193
Download citation
DOI: https://doi.org/10.1007/5584_2015_193
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-30603-2
Online ISBN: 978-3-319-30604-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)