
Abstract
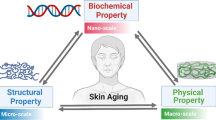
Skin aging is accompanied by a variety of epidermal, dermal, and subcutaneous alterations including changes in pigmentation, volume, skin barrier function and mechanical properties. Although most of these signs of skin aging are somehow linked, the changes in mechanical properties are of special interest as they directly contribute to the development of wrinkles. While skin laxity is often seen first and most prominent at cheeks and neck, the loss of firmness is more general and becomes evident even in sun-protected areas. Although these signs of aging become visible lately, much later than wrinkles, the changes in skin elasticity begin early in life and progress continuously. To treat them most effectively, it is mandatory to understand the underlying dermal processes and how the skin mechanical properties change with aging. In addition, it is important to understand that skin ages differently in men and women due to the gender-related differences in the morphological distinction of dermal tissue. It is further of importance to understand the mechanical properties of the skin as a multiparametric function, influenced by a myriad of factors. It is inevitable to not only recognize all parameters as a whole but also to be able to relate to the measurement technique used to assess skin elasticity.
New data shows that the mechanical properties of the skin progressively decline with aging. This aging process affects the elastic ability of the skin to recover after stretching differently than the firmness of the skin. Furthermore, the mechanical properties not only vary significantly between the sexes, they also alter differently in men and women over lifetime. This knowledge can be helpful for a better understanding of the clinical genesis of facial wrinkles and age-related skin laxity as well as for the development and evaluation of effective treatment options for skin aging.
Access provided by CONRICYT-eBooks. Download reference work entry PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Skin aging is a complex biological process associated with increasing functional deficits in the heterogeneous dermal tissue due to structural and molecular alterations [1]. The most visible and obvious morphological sign of skin aging is the development of rhytides or wrinkles [2, 3]. While the fact that wrinkle severity increases with aging is generally known and commonly accepted [4, 5], recent studies [6, 7] have shown that the clinical genesis and onset of facial wrinkles differ between the sexes. The development of facial wrinkles significantly affects men earlier and with greater severity. There is an approximately 15 year earlier onset of visible rhytides compared with women. Furthermore, wrinkle severity linearly increases over lifetime in men whereas women’s wrinkles sharply increase with perimenopause [6]. Differences between men and women have further been found regarding the morphology of dermal connective tissue. Histological analyses show a higher volume of elastic fibers in young women but at the same time a stronger decrease with aging. Collagen density and fiber volume in male dermis is, with the exception of male skin between 20 and 40 years of age, lower in comparison to age-matched women [8]. In contrast, Shuster et al. [9] found men to have more collagen, yet others were not able to detect any significant differences between men and women [10].
Although the development of wrinkles might be the most notable sign of skin aging, it is accompanied by a variety of epidermal, dermal, and subcutaneous alterations. These include changes in pigmentation, volume, skin barrier function, and mechanical properties. Although most of these signs of skin aging are somehow linked, the changes in mechanical properties are of special interest as they directly contribute to the development of wrinkles. Therefore, the treatment of skin laxity has become one of the main targets for antiaging procedures including the use of radiofrequency or focused ultrasound devices. To choose the right procedures and to use them most effectively, it is mandatory to understand the underlying dermal processes and how the skin mechanical properties change with aging. In addition, as the number of men requesting skin rejuvenating procedures increase year by year, it is important to understand that skin ages differently in men and women due to the gender-related differences in the morphological distinction of dermal tissue.
It is further of importance to understand the mechanical properties of the skin as a multiparametric function, influenced by a myriad of factors. Therefore, it is inevitable to not only recognize all parameters as a whole but also to be able to relate to the measurement technique used to assess skin elasticity.
Skin Elasticity
The protection against mechanical influences is an important function of the human skin. To serve this function, the skin must exhibit both flexibility and relative resistance to deformation, thus permitting movement and allowing temporary compression and distention of a part [11]. The tensile functional properties of the skin are due to structural and qualitative components of the epidermis, dermis, and subcutis [12, 13]. However, in terms of mechanical properties the human skin can be understood as a five-layer structure. The very top layer is formed by the compact membrane of the stratum corneum. The proximal part of the epidermis with its underlying desmosomes and the dermoepidermal junction represents the second layer. Papillary dermis, which is built of loose connective tissue, is the third layer, whereas the strong connective tissue of the reticular dermis represents the fourth layer. The subcutaneous adipose tissue is the deepest layer [14]. These layers together, consisting of fibers, colloidal substance, motile liquids, and a stiff epidermal layer, determine the mechanical properties of the skin [15]. Because of this complex composition of elastic solids and viscous liquids, the mechanical properties of the skin are neither elastic nor viscous, but rather viscoelastic [16].
Although biophysical measuring methods have been used to assess skin elasticity for more than 30 years it is not yet possible to assign elasticity parameters to one single structural element of the skin. Evidence is given that the elastic fibers permit the skin to return spontaneously to its initial shape after deformation [17, 18]. Thereby, not only the absolute amount of elastic fibers is relevant, but also their orientation. Usually, elastic fibers are vertically oriented to a net and link the dermoepidermal junction with the horizontally oriented collagen fibers. If this architectural structure is impaired due to an excessive and uncontrolled elastin proliferation, the elastic recovery of the skin is partly or totally lost [19]. Collagen fibers do not have any elastic properties but rather are essential for mechanical stability and its resistance to deformation [11]. In unstretched skin, collagen fibers are organized as disordered bundles. As the skin is stretched the bundles unfold, until the collagen fibers reach their maximum length. Therefore, a lack of collagen fibers or a degenerated collagen architecture, due to skin aging or skin disease, results in a high distensibility, slackness, and a higher sensitivity regarding mechanical tension [14, 20]. Besides elastin and collagen fibers, the hydration level of epidermis and dermis also influences skin elasticity. It is known that a moistening of the epidermis with water results in an increase of distensibility and skin fatigue but at the same time skin elasticity decreases. Also, a lack of hydration correlates in clinical evaluation with a loss of elasticity [14]. At the other end, the subcutis, the deepest layer of the skin, is of importance, too, as it serves as a cushioning layer for mechanical shear forces and plastic deformation, but also has an impact on the overlying skin layers.
Quantitative Assessment of Skin Elasticity
The noninvasive assessment of the mechanical properties of the human skin in vivo can be performed by distinct methods mainly characterized by the evaluation of the nature and orientation of skin deformation after an imposed force [11]. Thereby, the available techniques can be grouped into different classes, namely, tensile with electric dynamometers [21], torsion method [22], as well as impact testing (balistometrique technique) [23]. The elevation testing by suction chamber method is currently the most frequently used tool to assess skin mechanics [11, 14].
Tensile Testing
Tensile testing is based on recording skin extension following the imposition of a parallel force to skin’s surface [11]. Therefore, tensile testing with electric dynamometers is the oldest commercialized device for investigating mechanical properties of the skin [21]. In this procedure, based on uniaxial tension, a small disk sticks on the skin and is set into forward and backward motion by the electric dynamometers. The stretching of the skin is recorded on the x-axis as superimposed ellipses (Fig. 1). The steepness of the slope of the ellipse gives information about the mechanical properties of the skin such as stiffness and elasticity [24, 25].

Typical curve of tensile testing with electric dynamometers
Torsion Technique
The measuring probe of the torsion method consists of a central disk and a peripheral ring which are both glued firmly onto the skin with double-sided adhesive tape. Due to a constant torque of the disk, the skin is deformed depending on the mechanical properties of the skin (Fig. 2) [22, 24]. The analysis of the resulting rotation angle (in degrees) of the disk versus time (seconds) gives information about the standard deformation parameters including skin elasticity, firmness, or skin fatigue [26]. The assessment can be adapted by variation of number, duration, intensity, and rhythm of the twisting as well as by the distance between the disc and the ring. To examine the mechanical properties of the epidermis, a distance of 1 mm is used whereas greater distances are used to include underlying skin layers [24].

Schematic overview of skin deformation due to torsion method
Impact Technique
The impact testing of the human skin, also called ballistometrique technique, was designed to approach specific tensile functions of the skin involving the deeper skin layers [11]. The balistometrique technique records the successive rebounds of a small hammer being dropped on the skin’s surface with defined energy [23, 27]. The more the kinetic energy is transformed into rebound, the more elastic is the surface [24]. Because of the viscoelastic properties of the human skin, parts of the rebounding energy are getting lost with every restitution phase so that height and duration of the hammer lower with every rebound. The induced rebounds are transduced into electrical signals which can be quantified and evaluated in terms of their amplitude and frequency [11]. The main parameter of the balistometrique technique is the so called rebound-coefficient which is calculated from the ratio between the heights of the first and second rebound. The rebound-coefficient depends mainly on skin elasticity and viscosity [11, 24].
Elevation Testing
Elevation testing using suction chamber devices is commonly used to determine noninvasively the mechanical properties of the skin [28–30]. The underlying principle of the suction chamber method is to assess skin extension caused by a negative pressure [14, 31–33]. Based on the measurement of the extension in comparison to the height and the duration of the vacuum, several skin elasticity parameters can be calculated such as skin distensibility, elasticity, or firmness [14].
Besides the Dermaflex® (Cortex Technology, Denmark), the Cutometer® (Courage & Khazaka, Germany) is the most used measuring device to assess skin elasticity in vivo. It measures the vertical deformation of the skin when it is pulled by a controlled vacuum into the probe (Fig. 3). The depth of the penetration is assessed by a contact-less, optical measuring method containing an infrared light source, a receiver, and two facing prisms which project the light from sender to receiver. The intensity of the projected light depends on the penetration depth of the skin into the probe [34].

Schematic representation of the suction chamber method
The Cutometer® has a measuring probe which is connected over a hose to the vacuum pump and the measuring system. The opening of the suction probe has a standard diameter of 2 mm; alternatively, probes with a larger diameter up to 8 mm are available. While the 2 mm probe is primarily suitable to assess the elasticity of the epidermis, 4–6 mm can be used to evaluate upper skin layers up to the papillary dermis, and the 8 mm opening can be used to assess all skin layers [34]. The negative pressure can be adjusted between 20 and 500 mbar and the pressure buildup can be generated abruptly or gradually. Suction and relaxing time can vary between 0.1 and 60 s with a maximum repetition up to 99 times.
The suction chamber method represents the deformation of the skin in terms of the time and offers different measurement modes due to pressure variations. In scientific practice, a preset constant negative pressure of 200–500 mbar is commonly used. Therefore, frequent practices are measurements with 3–10 cycles and suction and relaxing time of 2–5 s [16]. Elongation and retraction of the skin is presented on an external monitor already during the measurement.
A typical measuring curve consists of four phases (Fig. 4). The first phase is characterized by a sharp increase which explains the elastic extension of the skin. The second phase, representing the viscoelastic proportion of extension, is shown by flattening of the curve. Upon pressure discontinuation, the curve sharply declines. This third phase represents the elastic proportion of recovery, which is followed by a flattening of the curve which represents the viscoelastic proportion of recovery.

Skin deformation assessed by suction chamber method
The evaluation of the stress–strain and strain–time curves obtained with the Cutometer® allows the calculation of several tensile variables representing skin’s elasticity, distensibility, or recovery after deformation [11, 35] (Table 1). Parameters that are particularly suitable to assess age-related changes of the skin include the ratio of elastic recovery to distensibility (Ur /Uf) as well as the gross elasticity (Ua/Uf) and net elasticity (Ur/Ue) for evaluation of aging effects on the mechanical properties of skin [36].
Mechanical Properties in Human Skin
While the progress of skin wrinkling is visible to the unaided eye, age-related changes in skin mechanical properties often become visible first at a higher degree of severity as skin laxity and loss of firmness. While skin laxity is often seen first and most prominent at cheeks and neck (see Fig. 5), the loss of firmness is more general and becomes evident even in sun-protected areas. Both findings are common aesthetic complains of people usually starting in their 40s and 50s. Although these signs of aging become visible lately, much later than wrinkles, the changes in skin elasticity begin early in life and progress continuously.

Neck of a 19-year-old woman (a) with no signs of skin laxity and a 66-year-old woman (b) with extensive skin laxity
As studies have shown that the clinical genesis and onset of facial wrinkles as well as the morphology of the extracellular matrix differ between the sexes [6, 8, 9], it raises the question of whether the elastic properties of skin differ between men and women, too, and how these characteristics are influenced by skin aging. These questions were answered just recently by Luebberding et al. as her studies, in accordance with previous findings [28, 30, 37], confirm the significant impact of aging on mechanical properties in human skin [38]. All assessed parameters decrease progressively with increasing age. Over lifetime, the skin’s distensibility decreases by up to 50 %, while the elasticity, the skin’s ability to recover after stretching, decreases by up to 75 %.
Although it remains elusive to assign skin mechanical parameters to single structural elements of the skin, evidence is given that the elastic fibers permit the skin to return spontaneously to its initial shape after stretching [17, 18], whereas the collagen fiber network is essential for the skin’s mechanical stability and tensile strength [11]. It is well known that both the elastic and collagen fibers degenerate and diminish with aging, resulting in increased skin laxity and rhytides [18, 39, 40]. However, study results show that the aging process likely has a stronger influence on the elastic ability of the skin to recover after stretching as opposed to its effect on the firmness of the skin. It seems likely that these results might be due to the different amounts of collagen and elastin in the dermal connective tissue. While collagen makes up 70–80 % of the dry weight of the skin, elastin accounts for only 2–4 % [1]. It seems possible that this quantitative difference in extracellular fiber components led to a relatively faster degeneration of elastic fibers resulting in decreased elasticity. This knowledge is especially relevant for the aesthetic medicine as many antiaging procedures including radiofrequency or focused ultrasound devices target the collagen fibers in the skin to decrease skin laxity. However, how these procedures affect the much more important elastin fibers is virtually unknown.
Considering the known differences in skin physiology in men and women, it seems useful to take a more detailed look at the age-related changes in mechanical properties. The comparison of men and women shows that in fact gender-related differences exist.
While the alterations in female skin occur sharply, the mechanical properties of male skin steadily decline throughout life. In women, the distensibility strongly decreases between the ages of 20–30 years, whereas the elasticity decreases between the ages of 40–50 years. It can be assumed that the abrupt decrease of skin elasticity in women’s 40s might be the result of hormonal changes resulting from perimenopause. Hillebrand et al. [41], among others [42], found that alterations in female steroid hormones due to menopausal transition years might highly impact the acceleration of skin wrinkles, compared to a relatively low hormonal status prior to menopause. As the development of wrinkles is strongly linked to skin elasticity [32], this hypothesis may be applicable to the changes in mechanical properties as well. However, further research, including the assessment of hormonal status, is needed for a better understanding of how menopause affects the mechanical properties of female skin.
In addition to the gender-specific decline of mechanical properties over lifetime, differences are also found in skin elasticity and distensibility itself [38]. Study results show that female skin is less distensible but has a higher elasticity (ability to recover after stretching) when compared to male skin. These differences are significant until the age of 40 and equilibrate with increasing age. A probable cause for these results is the gender-related difference in sex hormones. Histological analyses [8] have shown that both the collagen and elastin content in extracellular matrix does not differ significantly between boys and girls until the age of 10. Only with puberty and its hormonal changes, the connective tissue changes gender-specifically resulting in significantly higher collagen content in men and a higher content of elastic fibers in women. These differences remain until the age of 30–40 before they become equal again. Regarding the onset with puberty and the equalization with perimenopause, a connection with women’s childbearing capability seems obvious. One plausible explanation may be the need of the abdominal skin to be extensively stretchable during pregnancy and able to recover after birth. However, this may describe the higher elasticity of female skin, but does not explain the higher distensibility in men.
Conclusion
Recently published studies clearly show a progressive decline of the mechanical properties of the skin with aging. The elastic ability of the skin to recover after stretching is more strongly affected by the aging process than the firmness of the skin. Furthermore, the mechanical properties change differently in men and women over lifetime, and female’s skin is less distensible but has a higher ability to recover after stretching when compared to male skin. Perimenopause may cause an accelerated decrease in skin elasticity in women.
This knowledge can be helpful for a better understanding of the clinical genesis of facial wrinkles and age-related skin laxity as well as for the development and evaluation of effective treatment options for skin aging.
References
Tzaphlidou M. The role of collagen and elastin in aged skin: an image processing approach. Micron. 2004;35(3):173–7.
Callaghan TM, Wilhelm K-P. A review of ageing and an examination of clinical methods in the assessment of ageing skin. Part I: cellular and molecular perspectives of skin ageing. Int J Cosmet Sci. 2008;30(5):313–22.
Farage MA, Miller KW, Elsner P, Maibach HI. Intrinsic and extrinsic factors in skin ageing: a review. Int J Cosmet Sci. 2008;30(2):87–95.
Friedman O. Changes associated with the aging face. Facial Plast Surg Clin North Am. 2005;13(3):371–80.
Kligman AM, Zheng P, Lavker RM. The anatomy and pathogenesis of wrinkles. Br J Dermatol. 1985;113(1):37–42.
Luebberding S, Krueger N, Kerscher M. Life-time development of facial wrinkles of men and women: using three-dimensional fringe projection method and validated assessment scales. Dermatol Surg. 2014;40(1):22–32.
Akiba S, Shinkura R, Miyamoto K, Hillebrand G, Yamaguchi N, Ichihashi M. Influence of chronic UV exposure and lifestyle on facial skin photo-aging – results from a pilot study. J Epidemiol Jpn Epidemiol Assoc. 1999;9(6 Suppl):S136–42.
Vitellaro-Zuccarello L, Cappelletti S, Dal Pozzo Rossi V, Sari-Gorla M. Stereological analysis of collagen and elastic fibers in the normal human dermis: variability with age, sex, and body region. Anat Rec. 1994;238(2):153–62.
Shuster S, Black MM, McVitie E. The influence of age and sex on skin thickness, skin collagen and density. Br J Dermatol. 1975;93(6):639–43.
Quaglino DJ, Bergamini G, Boraldi F, Pasquali Ronchetti I. Ultrastructural and morphometrical evaluations on normal human dermal connective tissue – the influence of age, sex and body region. Br J Dermatol. 1996;134(6):1013–22.
Rodrigues L. EEMCO guidance to the in vivo assessment of tensile functional properties of the skin. Skin Pharmacol Physiol. 2001;14(1):52–67.
Wlaschek M, Tantcheva-Poór I, Naderi L, Ma W, Schneider LA, Razi-Wolf Z, et al. Solar UV irradiation and dermal photoaging. J Photochem Photobiol B. 2001;63(1–3):41–51.
Schneider LA, Wlaschek M, Scharffetter-Kochanek K. Skin aging. Clinical aspects and pathogenesis. J Dtsch Dermatol Ges. 2003;1(3):223–32; quiz 233–4.
Gniadecka M, Serup J. Suction chamber method for measuring skin mechanical properties: the Dermaflex®. In: Serup J, Jemec G, Grove G, editors. Non-invasive methods and skin. Boca Raton/New York/London: Taylor & Francis; 2006. p. 571–7.
Oomens CW, van Campen DH, Grootenboer HJ. A mixture approach to the mechanics of skin. J Biomech. 1987;20(9):877–85.
Barel A. Suction chamber method for measurement of skin mechanics. The new digital version of the Cutometer. In: Serup J, Jemec GB, Grove GL, editors. Non-invasive methods and the skin. 2nd ed. Boca Raton/London/New York: Taylor & Francis; 2006. p. 583–91.
Oxlund H. Changes in connective tissues during corticotrophin and corticosteroid treatment. Biomechanical and biochemical studies on muscle tendon, skin and aorta in experimental animals. Dan Med Bull. 1984;31(3):187–206.
Oxlund H, Manschot J, Viidik A. The role of elastin in the mechanical properties of skin. J Biomech. 1988;21(3):213–8.
Vieira ACT, Vieira WT, Michalany N, Enokihara M, Freymüller E, Cestari SCP. Elastoderma of the neck in a teenage boy. J Am Acad Dermatol. 2005;53(2 Suppl 1):S147–9.
Kolácná L, Bakesová J, Varga F, Kostáková E, Plánka L, Necas A, et al. Biochemical and biophysical aspects of collagen nanostructure in the extracellular matrix. Physiol Res Acad Sci Bohemoslov. 2007;56 Suppl 1:S51–60.
Wan Abas WA, Barbenel JC. Uniaxial tension test of human skin in vivo. J Biomed Eng. 1982;4(1):65–71.
Agache P. Twistometry measurement of skin elasticity. In: Serup J, Jemec GBE, editors. Handbook of noninvasive methods and the skin. 1st ed. Boca Raton: CRC-Press; 1995. p. 319–28.
Hargens C. Ballistometry. In: Serup J, Jemec GBE, editors. Handbook of non-invasive methods and the skin. 1st ed. Boca Raton: Informa Healthcare; 1995. p. 359–66.
Agache P, Varchon D. Mechanical behaviour assessment. In: Agache P, Humbert P, editors. Measuring the skin: non-invasive investigations, physiology, normal constants. 1st ed. Berlin: Springer; 2004. p. 446–67.
Cooper EP, Missel PJ, Hannon DP, Albright GB. Mechanical properties of dry, normal, and glycerol-treated skin as measured by the gas-bearing electrodynamometer. J Soc Cosmet Chem. 1985;36:335–48.
Bazin R, Fanchon C. Equivalence of face and volar forearm for the testing of moisturizing and firming effect of cosmetics in hydration and biomechanical studies. Int J Cosmet Sci. 2006;28(6):453–60.
Adhoute H, Berbis E, Privat Y. Ballistometric properties of aged skin. In: Leveque J-L, editor. Aging skin: properties and functional changes. Illustrated ed. Abingdon (UK): Informa Healthcare; 1993. p. 39–48.
Ahn S, Kim S, Lee H, Moon S, Chang I. Correlation between a Cutometer and quantitative evaluation using Moire topography in age-related skin elasticity. Skin Res Technol. 2007;13(3):280–4.
Cua AB, Wilhelm KP, Maibach HI. Elastic properties of human skin: relation to age, sex, and anatomical region. Arch Dermatol Res. 1990;282(5):283–8.
Ryu HS, Joo YH, Kim SO, Park KC, Youn SW. Influence of age and regional differences on skin elasticity as measured by the Cutometer. Skin Res Technol. 2008;14(3):354–8.
Grahame R. A method for measuring human skin elasticity in vivo with observations of the effects of age, sex and pregnancy. Clin Sci. 1970;39(2):223–9.
Choi JW, Kwon SH, Huh CH, Park KC, Youn SW. The influences of skin visco-elasticity, hydration level and aging on the formation of wrinkles: a comprehensive and objective approach. Skin Res Technol. 2013;19(1).
Mine S, Fortunel NO, Pageon H, Asselineau D. Aging alters functionally human dermal papillary fibroblasts but not reticular fibroblasts: a new view of skin morphogenesis and aging. PLoS One. 2008;3(12):e4066.
O’goshi K-I. Suction chamber method for measurements of mechanics: the Cutometer. In: Serup J, Jemec G, Grove G, editors. Non-invasive methods and skin. Boca Raton/New York/London: Taylor & Francis; 2006. p. 579–82.
Agache PG, Monneur C, Leveque JL, De Rigal J. Mechanical properties and Young’s modulus of human skin in vivo. Arch Dermatol Res. 1980;269(3):221–32.
Krueger N, Luebberding S, Oltmer M, Streker M, Kerscher M. Age-related changes in skin mechanical properties: a quantitative evaluation of 120 female subjects. Skin Res Technol. 2011;17(2):141–8.
Boyer G, Laquièze L, Le Bot A, Laquièze S, Zahouani H. Dynamic indentation on human skin in vivo: ageing effects. Skin Res Technol. 2009;15(1):55–67.
Luebberding S, Krueger N, Kerscher M. Mechanical properties of human skin in vivo: a comparative evaluation in 300 men and women. Skin Res Technol. 2014;20(2):127–35.
Braverman IM, Fonferko E. Studies in cutaneous aging: I. The elastic fiber network. J Invest Dermatol. 1982;78(5):434–43.
Frances C, Branchet MC, Boisnic S, Lesty CL, Robert L. Elastic fibers in normal human skin. Variations with age: a morphometric analysis. Arch Gerontol Geriatr. 1990;10(1):57–67.
Hillebrand GG, Liang Z, Yan X, Yoshii T. New wrinkles on wrinkling: an 8-year longitudinal study on the progression of expression lines into persistent wrinkles. Br J Dermatol. 2010;162(6):1233–41.
Phillips TJ, Symons J, Menon S. Does hormone therapy improve age-related skin changes in postmenopausal women? A randomized, double-blind, double-dummy, placebo-controlled multicenter study assessing the effects of norethindrone acetate and ethinyl estradiol in the improvement of mild to moderate age-related skin changes in postmenopausal women. J Am Acad Dermatol. 2008;59(3):397–404.e3.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer-Verlag Berlin Heidelberg
About this entry
Cite this entry
Krueger, N., Luebberding, S. (2017). Age-Related Changes in Skin Mechanical Properties. In: Farage, M., Miller, K., Maibach, H. (eds) Textbook of Aging Skin. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-47398-6_116
Download citation
DOI: https://doi.org/10.1007/978-3-662-47398-6_116
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-47397-9
Online ISBN: 978-3-662-47398-6
eBook Packages: MedicineReference Module Medicine