
Abstract
Tibial spine fractures are an avulsion of the attachment site of the anterior cruciate ligament on the tibia. They are a relatively rare type of fracture that children (ages 8–14 most commonly) may sustain. They are typically cited at less than 2% of all knee injuries in the pediatric population. The mechanism of injury is classically taught as a fall from a bike landing on a hyperflexed knee. More recent studies have supported that the mechanism of injury is similar to that of adult style anterior cruciate ligament (ACL) injury. This injury represents a failure of the chondroepiphysis. The ACL in children has a greater strength to failure than to the bone to which it is attached. It should be remembered that although the obvious injury happens at the tibial spine, a stretching injury to the anterior cruciate ligament itself can also occur. Tibial spine fractures are classified by the Myers/McKeaver classification: type 1 is minimal displacement, type 2 is anterior half of the fractured tibial spine is elevated with intact posterior hinge, and type 3 is complete avulsion of the tibial spine. A type 4 was added later which is complete displacement with rotation.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


1 Brief Clinical History
A 14-year-old young man sustained a left knee injury while playing football. He was running with the ball when a defender struck him with his helmet on the anterior knee causing a hyperextension injury. He developed immediate pain and swelling and was unable to bear weight. He went to a local emergency department where x-rays and CT scan were performed. He was then transferred to a pediatric hospital for further care.
2 Preoperative Clinical Photos and Radiographs
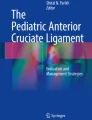
See Fig. 1.

(a–d) X-rays and CT scan showing a displaced tibial spine fracture. (a) AP radiograph knee. Tibial spine fracture is seen, (b) Lateral radiograph of the knee, displacement of tibial spine fracture fragment seen, (c,d) CT scan obtained at outside hospital demonstrating displaced tibial spine fracture
3 Preoperative Problem List
Knee hemarthrosis/effusion following an injury in the pediatric population may be secondary to:
-
1.
Patella dislocation
-
2.
ACL injury
-
a.
Ligament disruption
-
b.
Tibial spine fractur e
-
a.
-
3.
Osteochondral injury
4 Treatment Strategy
-
1.
Nonoperative treatment
-
a.
Closed reduction
-
b.
Evacuation of hemarthrosis
-
c.
Immobilization in 0–20 degrees of extension
-
d.
Indicated for type 1 and reducible type 2 fractures
-
a.
-
2.
Operative treatment
-
a.
Open reduction (ORIF) or arthroscopic reduction (ARIF)
-
b.
Indicated for type 3 fractures and nonreducible type 2 fractures
-
a.
-
3.
Surgical technique
-
a.
Arthroscopic reduction internal fixation
-
i.
Standard arthroscopic portals (medial and lateral para-patellar portals)
-
ii.
Accessory portals
-
1.
Central used for viewing while passing sutures through anterior lateral and medial portals. Can also be used when trying to reduce the fracture fragment
-
2.
High medial portal – if using cannulated screws, this portal is helpful for achieving the proper angle for screw insertion
-
3.
Use cannulas to prevent sutures from getting incarcerated in the soft tissues
-
1.
-
iii.
Debride fracture bed
-
1.
Remove clot, cancellous bone, or callus that may block reduction
-
2.
Retract entrapped meniscus/intermeniscal ligament if present
-
a.
Probe or K-wire bent as a hook can be helpful in pulling meniscus/intermeniscal ligament
-
b.
Passing a suture through the anterior horn of the meniscus by an outside-in technique can help reduce the meniscus and hold it out of the way
-
a.
-
1.
-
iv.
Reduce the fracture
-
1.
Hold reduction with probe through accessory portal or with a K-wire or 18-gauge spinal needle
-
1.
-
v.
Stabilize fracture
-
1.
Suture
-
a.
Pass one or two sutures through the base of the ACL
-
i.
Can use a 25-degree curved suture lasso or scorpion type suture passer
-
i.
-
b.
Drill two small bone tunnels in the tibial epiphysis at medial and lateral edge of the fracture bed
-
i.
ACL drill guide can be helpful
-
i.
-
c.
Pass sutures through drill holes with Hewson suture passer
-
i.
Can pass sutures exiting the medial side of ACL in medial tunnel and lateral suture in lateral tunnel or pass in a X (cross over) fashion
-
i.
-
d.
Tie sutures over bone bridge
-
i.
May use button for more security of the knot
-
i.
-
a.
-
2.
Screw fixation
-
a.
Use accessory high medial portal
-
b.
Guide wire
-
c.
Cannulated screw
-
d.
Take care not to violate the physis
-
a.
-
3.
Hybrid technique was selected for this case (Fig. 2)
-
a.
Once fracture is reduced hold reduction with bioabsorbable screw
-
b.
Once fracture is stabilized then pass sutures through ACL to re-tension the ACL and hold reduction
-
a.
Fig. 2 
Intraoperative arthroscopic images. (a) Insertion of a bioabsorbable screw into the base of the fracture fragment. (b) Passing suture through the ACL and a Hewson suture passer to be pulled through tibial tunnel. (c) Final reduction of the fragment and retensioning of the ACL.
-
1.
-
i.
-
a.

5 Basic Principles
-
1.
Obtain anatomic reduction
-
a.
If fragment is left proud it may lead to impingement and limited range of motion
-
a.
-
2.
Obtain stable fixation
-
a.
Goal is to start early range of motion to prevent arthrofibrosis
-
a.
-
3.
Arthroscopic reduction and internal fixation may be superior to ORIF in terms of
-
a.
Less morbidity
-
b.
Faster rehab
-
c.
Decreased pain
-
a.
6 Images During Treatment
See Fig. 2.
7 Technical Pearls
Blocks to reduction may include:
-
1.
Intermeniscal ligament
-
2.
Meniscus
-
a.
54% of the time there is entrapment of the anterior horn of either the medial or lateral meniscus
-
a.
-
3.
Cancellous bone
-
4.
In patients with whom there is a delay in getting into the operating room, there may be clot and callus blocking the reduction
Overcoming blocks to reduction:
-
1.
Use of accessory portals to pass instruments that can hook and pull the meniscus and hold it out of the way
-
2.
May pass a suture through the anterior horn of the meniscus using outside-in technique and hold the meniscus out of the way for the reduction
-
3.
Take time to prepare the fracture bed. Use curette to clear cancellous bone/clot/early callus from the fracture bed. If the tibial spine sits proud or remains displaced it may lead to impingement
Internal fixation with cannulated screws:
-
1.
Must avoid crossing the physis
-
2.
Ideal choice when large fragment is present
-
3.
May be difficult to get good purchase
-
a.
Epiphyseal bone is soft
-
b.
Fragment may be small
-
a.
-
4.
Tough angle
-
a.
Use accessory high medial portal off of the medial side of the patella
-
a.
Internal fixation using suture:
-
1.
Good for small fragments or comminuted fractures
-
2.
Helps restore tension in the ACL
-
3.
Near equal strength to screw fixation in lab testing
-
4.
Do not cross physis with nonabsorbable sutures
8 Outcome Clinical Photos and Radiographs
See Fig. 3.

X-rays from follow-up visit demonstrating healed fracture in normal alignment
9 Avoiding and Managing Problems
-
1.
Obtain the most rigid fixation possible to be able to start early range of motion exercises to prevent arthrofibrosis
-
2.
Passing sutures through the base of the ACL helps to restore tension in the ACL while reducing the fracture. This will help to decrease residual laxity in the ACL
10 Cross-References
References and Suggested Reading
Edmonds E, Fornari E, Dashe J, Roocroft J, King M, Pennock A (2015) Results of displaced pediatric tibial spine fractures: a comparison between open, arthroscopic, and closed management. J Pediatr Orthop 35:651–656
Gans I, Baldwin K, Ganley T (2013) Treatment and management outcomes of tibial eminence fractures in pediatric patients. Am J Sports Med 42:1743–1750
McLennan J (1995) Lessons learned after second-look arthroscopy in type III fractures of the tibial spine. J Pediatr Orthop 15:59–62
Mitchell J, Sjostrom R, Mansour A, Irion B, Hotchkiss M, Terhune B, Carry P, Stewart J, Vidal A, Rhodes J (2015) Incidence of meniscal injury and chondral pathology in anterior tibial spine fractures of children. J Pediatr Orthop 35:130–135
Shea K, Grimm N, Loar T, Wall E (2011) Bone bruises and meniscal tears on MRI in skeletally immature children with tibial eminence fractures. J Pediatr Orthop 31:150–152
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Section Editor information
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this entry

Cite this entry
Mandel, D. (2020). Arthroscopic Treatment of Tibial Spine Fractures. In: Iobst, C., Frick, S. (eds) Pediatric Orthopedic Trauma Case Atlas. Springer, Cham. https://doi.org/10.1007/978-3-319-29980-8_116
Download citation
DOI: https://doi.org/10.1007/978-3-319-29980-8_116
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-29979-2
Online ISBN: 978-3-319-29980-8
eBook Packages: MedicineReference Module Medicine