
Abstract
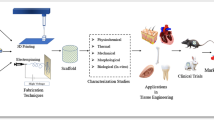
This chapter describes concepts of tissue engineering and scaffold fabrication and function as these relate to 3D cell and tissue growth and function which may lead to complex organ manufacture. Scaffold materials are described, including natural (biological) scaffold materials such as collagen, chitosan, and silk as well as metals and polymers.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Tissue cells, aside from blood cells, are anchorage dependent, residing in a solid matrix, referred to as an extracellular matrix (ECM) . Human tissue, including bone tissue, usually has different ECM types with multiple components and tissue-specific composition. Tissue engineering involves the creation of a scaffold structure having necessary biocompatibility, mechanical properties, especially bone or host tissue matching stiffness, porosity and pore or open-cellular structure, and bioresorbability; or the ability to degrade with time in vivo at a controlled rate in order to leave space for new tissue growth. Scaffolds, cells, and growth-stimulating signals are generally referred to as the tissue-engineering triad. Of course, open-cellular structures associated with permanent implant components as illustrated in Figs. 7 and 9 of chapter “Implant Materials and Structures”, and especially Figs. 13, 14, and 15 of chapter “Implant Materials and Structures”, as well as Figs. 19 and 23 of chapter “Implant Materials and Structures” can also provide a tissue-engineering scaffold. Particularly important for prospects for implanting open-cellular structures to accommodate the intramedullary, bone volume is the allowance for blood vessel formation (angiogenesis) throughout the scaffold. Current permanent implants, especially intramedullary stems or rods (Figs. 2, 5, and 7 of chapter “Implant Materials and Structures”), do not allow for any vascularization.
Scaffolds and Scaffold Materials
Scaffold properties of most importance include, as noted previously, pore size or cell size and shape, the connecting strut or ligament thickness, and surface area and structure. Figure 24 (chapter “Implant Materials and Structures”) illustrates the strut or ligament features, including surface structure, for EBM-fabricated, open-cellular structures, while Fig. 1 illustrates comparative 3D scaffold systems fabricated from Ti-6Al-4V by EBM, using two different build element (CAD software) models to be discussed in more detail in Part XI. It can be noted in Fig. 1a that the strut thickness and porosity are changing and the stiffness varies from 2.7 to 0.78 GPa (for scaffolds (1)–(3) in Fig. 1a which would in fact correspond to the cancellous (intramedullary) bone regime.

3D Ti-6Al-4 V scaffolds fabricated by EBM. (a) 3D-layer (∼3 mm thick) opaque view. 1–3 are same software element as that used to fabricate tibial stem in Fig. 85c of chapter “Chemical Forces: Nanoparticles”. 4 is a different element. (1) 82 % porosity, E = 0.92 GPa; (2) 81 % porosity, E = 1.53 GPa; (3) 72 % porosity, E = 2.70 GPa; (4) 65 % porosity, E = 6.78 GPa. (b) Transparent view of scaffolds in (a) showing pore-channel structure
Scaffolds in tissue engineering directed toward tissue replacement, restoration, or the regeneration of detective tissue as in cranio-maxillofacial replacement illustrated in Fig. 3b (chapter “Implant Materials and Structures”) are often biodegradable polymers such as those illustrated in Fig. 2 of chapter “Strategies for Bone Replacement and Tissue Augmentation”. However, natural scaffold materials (aside from autografts and allografts of cancellous and cortical bone) include collagen, chitosan (a polysaccharide derived from chitin and found in crab shells) silk, fibrin, and coral. In fact coral has proven to be an effective clinical alternative to autogenic and allogenic bone grafts for some applications (Wong and Mooney 1997). These scaffolds, along with polymer scaffolds, can be created by solid freeform fabrication (SFF) or rapid prototyping (RP) technologies which characterize other forms of 3D printing or additive layer manufacturing to be discussed in detail in Part XI following. In this regard, biodegradable Mg and Mg alloy scaffolds can be fabricated by EBM or a similar build technology using a laser beam to melt precursor (and pre-alloyed) powders in an inert atmosphere, such as argon or nitrogen. This method is described as selective laser melting (SLM) in contrast to EBM fabrication (Part XI, chapter “Laser and Electron Beam Melting Technologies”).
Major advancements in bone tissue engineering in particular have been achieved through the loading of scaffolds or scaffold material with growth factors, drugs, and gene delivery (Bose et al. 2012). Bone replacement scaffolds are similarly loaded with drugs and growth factors to treat bone defects along with introducing osteoinductivity, a property of materials that induces new bone formation through biomolecular signaling and recruitment of progenitor cells. Commonly used drugs include vancomycin, gentamicin, and methotrexate. These tissue enhancement strategies can also be incorporated into hydrogel matrices along with cells which can be injected into the porous scaffold volume, including vascular cells, since angiogenesis throughout the scaffold (including permanent implant scaffolds) is critical to the success of the scaffold because cells must be within a few hundred microns of the nearest blood supply in order to survive (Karp et al. 2003).
Figure 2 illustrates the cell attachment and tissue development for osteoblast bone cells on a PLA nanofiber mat as a scaffold. The polymer fibers were coated with a microgel loaded with an antimicrobial peptide to inhibit bacterial colonization of the scaffold while promoting adhesion, spreading, and proliferation of the osteoblasts. Figure 3 shows a cross-section view of the acetabular cup shown previously in Fig. 7 of chapter “Implant Materials and Structures”. The insert illustrates how bone cell ingrowth can occur in scaffold systems of this type.

SEM image of osteoblast bone cells on antimicrobial-coated PLA/PGA (polylactic acid/polyglycolic acid)

Section view of Ti-6Al-4V acetabular cup (Fig. 69 of chapter “Chemical Forces: Nanoparticles”) fabricated with a mesh (porous) surface by EBM. Insert shows SEM image of rabbit bone ingrowth (B) into a porous Ti implant. Arrow shows bone cells in internal pores (Adapted from Reis de Vasconcellos et al. (2010))
As we noted previously, both tissue engineering and tissue healing have a common concern: the necessity to build new blood vessels throughout the new or rebuilt tissue. This is particularly true for the rebuilding of skin, the largest body organ. Vascularization is required to keep tissue, such as skin, alive. Skin is composed of two layers: the epidermis (or outer layer) and the dermis (the inner layer). Skin functions to keep vital fluid in the body and harmful pathogens out. It also helps to regulate body temperature. The dermis contains the blood vessels, nerves, sweat glands, oil, and hair. The dermis is composed primarily of connective tissue fibers such as collagen, and it provides nourishment to the epidermis.
Tissue engineering and biotechnology have pursued the creation of suitable and optimal skin substitutes since there are roughly two million people annually who suffer various degrees of burns, frostbites, and disruption of adequate vascularization or venus macrocirculation which cause trophic skin lesions. As early as 500 BC, Hindu surgeons performed nose reconstruction involving grafting skin flaps from the patient’s nose. Xenografts (skin substitutes harvested from animals for use as temporary grafts in humans) for wound coverage have been reported to have used frog skin as early as 1500 BC, while porcine skin is the most common xerograft in modern practice. Autografts (or skin grafts constructed from a patient’s own skin) as well as allografts (skin grafts constructed from cadaver skin) were the major forms of skin repair until the late twentieth century.
The first synthetic skin was invented by John Burke and Ioannis Yannas in the 1970s who used collagen fibers and a long sugar molecule to form a porous polymer material resembling skin (Yannas and Burke 1980). They later created an artificial skin using polymers from shark cartilage and collagen from cowhide (Sheridan et al. 1994). This created a membrane covering similar to the human dermis layer, and a layer of silicone was added to act like the human epidermis. This synthetic skin functioned like a scaffold onto which new skin and blood vessels could grow, and as this process proceeded, the scaffold degraded and was absorbed by the body.
In the mid-1980s, Joseph Vacanti and Robert Langer conceived the idea of constructing a biodegradable scaffold to grow skin cells using fibroblast cells extracted from neonatal foreskin removed during circumcision (Longer and Vacanti 1995). One foreskin can yield enough cells to make roughly four acres of grafting material. The fibroblasts can be grown on biodegradable scaffolds as illustrated in Fig. 2.
A collagen matrix or mixtures of collagen and fibrin can also be used as even more biocompatible scaffolds, and cells can also be incorporated in the collagen matrix. Similarly, customized gels and hydrogels have been utilized to regrow skin with vascularization. These can be fabricated as tissue coverings or as growth matrices and can include collagen-based gels or hydrogels composed of dissolved dextran and polyethylene glycol (PEG) (Sun et al. 2011). Such hydrogels can act as scaffolds for other soft tissue growth and propagation such as nerve cells and the like.
While skin can be regenerated and grown on tissue-engineering scaffolds, it represents a shallow (or thin) 3D organ in contrast to other more complex organs which are composed of multiple cell types, extracellular matrices of proteins, and special microstructures (including tubular and sheet forms) which exhibit structure-specific biological functions. In order to fabricate these larger, more complex organs, or in fact to fabricate skin in a manufacturing process such as biofabrication or bioprinting, Makoto Nakamura, around 2002, conceived the idea of incorporating living cells in a spherical hydrogel emulating an inkjet printer ink droplet. By 2008, Nakamura and co-workers had created a working bioprinter that could print biotubing similar to a blood vessel (Nakamura et al. 2005). About the same time, Gabor Forgacs at the University of Missouri, along with his co-workers, established a commercial bioprinting company, Organovo, which printed functional blood vessels and cardiac tissue using cells from a chicken Mironov et al. 2007, 2009). In bioprinting processes, aggregates of specialized living cells create bioink spheroids which are injected by a printer head onto a substrate or biopaper made from collagen, gelatin, or other hydrogels. As more layers of bioink spheroids are selectively added layer-by-layer, the water-base substrate (biopaper) dissolves, and the bioink cell spheroids fuse together as illustrated schematically in Fig. 4.

3D bioprinting of organ or tissue structure using bioink spheroids of cells or aggregated multicell types injected into water-based biopaper. (1) bioink spheroids printed into a layer of biopaper gel. (2) additional layers printed to build the object. (3) bioink spheroids fuse together; biopaper dissolves. (4) final living tissue product which can include speciated cellular regimes forming functional components formed by self-assembly (Adapted from an Organovo, Inc. graphic (Courtesy of Organovo, Inc.))
It has been shown that specific cells contained in bioink spheroids are capable of rearranging themselves (self-assembly) after printing. As an example, experimental blood vessels have been bioprinted using such bioink spheroids comprised of aggregates of fibroblast cells, smooth muscle cells, and endothelial cells. Once printed as illustrated in Fig. 4, the endothelial cells migrate to the inside of the bioprinted blood vessel, the smooth muscle cells move to the middle of the wall, while the fibroblasts populate the outer wall (Forgacs 2012).
The implication of this technology is that human organs might be fabricated by 3D printing or additive manufacturing. Correspondingly, organs specific to an individual might be manufactured using micro-CT scans to embed the organ morphology in CAD software, while either using specific donor cells or the speciation of stem cells with donor DNA to produce a patient-specific organ similar to fabricating patient-specific implant components as described previously. We will discuss these prospects in more detail in Part XI.
References
Bose S, Roy M, Bandyopadhyay A (2012) Recent advances in bone tissue engineering scaffolds. Trends Biotechnol 30(10):546–554
Forgacs G (2012) Tissue engineering: perfusable vascular networks. Nat Mater 11:746–747
Karp JM, Dalton PD, Shoichet MS (2003) Scaffolds for tissue engineering. MRS Bull 28:301–306
Longer R, Vacanti JP (1995) Tissue engineering. Science 14:920–921
Mironov V, Prestwich G, Forgacs G (2007) Bioprinting living structures. J Mater Chem 17:2054–2060
Mironov V, Visconti RP, Kasyanov V, Forgacs G, Drake CJ, Markwald RR (2009) Organ printing: tissue spheroids as building blocks. Biomaterials 30:2164–2174
Nakamura M, Kobayashi A, Takagi F, Watanabe A, Hiruma Y, Ohuchi K, Iwasaki Y, Hovie M, Morita I, Takatoni S (2005) Biocompatible inkjet printing technique for designed seeding of individual living cells. Tissue Eng 11:1658–1666
Reis de Vasconcellos LM, Leite DO, de Oliveira FN, Carvalho YR, Alves Cairo CA (2010) Evaluation of bone ingrowth into porous titanium implant: histomorphometric analysis in rabbits. Braz Oral Res 24(4):1–9
Sheridan RL, Hegarty M, Tonpkins RG, Burke JF (1994) Artificial skin in massive burns – results to 10 years. Eur J Plast Surg 17(2):91–93
Sun G, Zhang X, Shen Y, Sebastian R, Dickinson LE, Fox-Talbot K, Reinblatt M, Steenbergen C, Harman JW, Gerecht S (2011) Dextran hydrogel scaffolds enhance angiogenic responses and promote complete skin regeneration during burn wound healing. Proc Natl Acad Sci U S A 108(52):20976–20981
Wong WH, Mooney DJ (1997) Synthesis and properties of biodegradable polymers used as synthetic matrices for tissue engineering. In: Atala A, Mooney DJ (eds) Synthetic biodegradable polymer scaffolds. Birkhausen, Boston, pp 83–95
Yannas IV, Burke JF (1980) Design of an artificial skin. I. Basic design principles. J Biomed Mater Res 14:65–81
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this entry
Cite this entry
Murr, L.E. (2015). Tissue Engineering Scaffolds and Scaffold Materials. In: Handbook of Materials Structures, Properties, Processing and Performance. Springer, Cham. https://doi.org/10.1007/978-3-319-01815-7_33
Download citation
DOI: https://doi.org/10.1007/978-3-319-01815-7_33
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-01814-0
Online ISBN: 978-3-319-01815-7
eBook Packages: Chemistry and Materials ScienceReference Module Physical and Materials ScienceReference Module Chemistry, Materials and Physics