
Abstract
Asthma is a global disease of varying presentations and complex pathophysiology which contributes to chronic symptom burden, loss of function and productivity, increased healthcare costs from emergency department visits and hospitalization, and severe medical complications including death. An estimated 25 million Americans and 300 million persons worldwide are affected and epidemiologic studies indicate that the prevalence of asthma is increasing. Understanding asthma requires knowledge of: lung function, immunology and hypersensitivity, disease presentation, pulmonary function testing, treatment mechanisms, and comorbid conditions. Management of patients with asthma demands longitudinal monitoring of symptoms, medication use and compliance, and frequent reassessment of response to therapy. Due to the complexity of the disease and multitude of treatment considerations, referral to specialists and advanced centers of excellence is required to achieve acceptable disease control in some instances. However, physicians in the primary care setting, emergency department, and hospital frequently encounter, diagnose, and manage asthma. As such, understanding the core principles of definition, mechanism, diagnosis, symptom burden, associated and mimicking diseases, and treatment options is necessary for all healthcare professionals. This chapter outlines the fundamental approach to asthma definition, diagnosis, pathogenesis, presentation, comorbid conditions, and treatment modalities.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
1 Introduction
Asthma is a worldwide health problem with increasing prevalence, increasing costs due to healthcare utilization and loss of work productivity, and complex interactions with environmental and genetic risk factors. Asthma currently has the greatest estimated prevalence and societal impact since it was first described in ancient Greece (Akinbami et al. 2012). Further complicating the understanding of asthma, a wide array of treatment options exists and numerous conditions can affect or mimic asthma. Therapies include medications which reduce inflammation as well as immunotherapy meant to alter the body’s response to environmental factors. Comorbid conditions such as vocal cord dysfunction and rhinosinusitis can obscure the diagnosis or affect patients’ response to therapy. Asthma is a disease with nuance that frequently requires subspecialty, advanced knowledge but presents to general medical practitioners with regularity. Patients who have more than mild, intermittent symptoms, note that asthma has a significant impact on their quality of life and daily functioning. As such, greater efforts are being undertaken to improve education for patients and physicians alike about recognizing asthma, initializing appropriate therapy, monitoring response to treatment, considering contributing conditions, and understanding need for appropriate referral.
2 Asthma Definition and Impact
Asthma is a chronic inflammatory disease of the lungs characterized by intermittent airway obstruction and hyperreactivity (EPR3 2007). Pulmonary symptoms include but are not limited to: chest tightness, wheezing, shortness of breath with activity, and cough. People with asthma demonstrate a greater susceptibility to airway infections which results in symptom worsening during and after the infection. The infections which typically exacerbate asthma are viral infections, particularly certain strains of rhinovirus, adenovirus, influenza, parainfluenza, respiratory syncytial virus, and metapneumovirus. Asthmatics may also note pulmonary symptoms with or after exercise, when exposed to inhalant allergens or irritants, or when the air temperature and humidity change. The airflow obstruction often manifests as chest tightness and shortness of breath and is assessed by spirometry, which measures the air movement during expiration and evaluates a response to medications which dilate the airways.
One of the challenging issues surrounding asthma is the variability. Symptoms are typically episodic and patients may lack demonstrable lung dysfunction between incidences. But, there is also significant variability in the natural history and associated triggers for patients. Patients can present in infancy or early childhood with a history of wheezing with and after respiratory infections. Others have a strong allergic burden manifested by sensitivity to many potential aeroallergens. Affected individuals, both those with and without allergy, also are susceptible to worsening of symptoms following inhaled irritants. And yet, some people don’t develop asthma until they are later in adulthood and have no history of allergies, eczema, or family asthma. As a result, physicians can struggle to recognize asthma or individualize treatment appropriately when patients do not present with a stereotypical history and symptom profile.
The cost of chronic diseases is significant. Asthma, as it affects the young and the old, is particularly so. Whether considering direct economic costs from emergency department visits and prolonged hospital stays or indirect costs from lost work productivity, the impact on resource allocation and utilization is enormous. A study recently analyzed data in the USA from 2008 to 2013 and estimated a financial loss of 81.9 billion USD related to asthma over that time period (Nurmagambetov et al. 2018). In addition to economic losses, there are the incalculable costs in terms of human suffering for the people living with chronic symptoms that limit quality of life, and emotional and physical encumbrances placed upon caregivers.
3 Pathogenesis
Historically, asthma has been considered a homogenous disease involving eosinophil and mast cell inflammation, airway hyperresponsiveness, and improvement subsequent to treatment with corticosteroids (Fahy 2010). However, it is now more clearly elucidated that a multitude of inflammatory cells and signaling molecules play variable roles in disease activity with numerous pathways to airway obstruction resulting in respiratory symptoms. The unifying principle is the presence of components of the inflammatory cascade leading to lung dysfunction intermittently, often as a result of an interaction between environmental factors, the airway and resident cells in the airway.
Mast cells, basophils, eosinophils, neutrophils, Th1 lymphocytes, Th2 lymphocytes, other lymphocyte subsets, macrophages immunoglobulins, histamine, leukotrienes, chemokines, and interleukin glycoproteins (IL) are all implicated in the airway pathology of asthma. These cells and proteins modify or contribute to the inflammatory response and determine interactions between the environment and lung tissue (epithelial, vascular, and neurologic cells) that ultimately cause airway constriction in asthmatic patients (Holgate 2008). In the traditional understanding of asthma pathogenesis, there is a propensity for a Th2 predominant immune response. T-helper cells are stimulated by antigen-presenting dendritic cells, macrophages, and B cells. After activation of the T-cell receptor via the presented antigen, the T-helper cell undergoes maturation predominantly along the Th1 or Th2 pathway. The determining factors for selection of one developmental route over others are multifactorial. The microenvironment of local cytokines along with genetically-driven propensities factor heavily in the differentiation (Blumenthal and Fine 2014). Once the T-helper cell differentiates, a cascade of ensuing inflammatory mediators propagates a specific immunologic response. Subsequent to maturation into a Th2 cell, the cell releases IL-4, IL-5, IL-10, and IL-13. This results in: increased Th2 differentiation in additional T-helper cells, immunoglobulin class switching to immunoglobulin E (IgE) in antibody production, eosinophil migration, mast cell recruitment, and mucous production (Lloyd and Hessel 2010). Thus, Th2-driven immunologic response triggers greater proportions of Th2 in the cellular matrix and the process is cyclically reinforced. This immunologic phenotype is the best understood mechanism for pathophysiology of asthma.
Our understanding of asthma now encompasses a greater awareness of alternative phenotypes and how alternative mechanisms, such as IL-17-induced neutrophil recruitment, can affect patient presentations and response to therapy. A disproportionate amount of severe asthma is characterized by neutrophil dominance in the cellular profile (Pelaia et al. 2015). These patients are more likely to be poorly responsive to corticosteroids, the most fundamental treatment of eosinophilic, and classically atopic, asthma. Understanding the complex pathophysiology more completely will allow for greater decision making capabilities for treatment of refractory cases.
Whatever the means of inflammatory pathogenesis, the resultant or associated airway hyperresponsiveness and bronchial smooth muscle constriction causes reduction in airway caliber. This narrowing over time can be associated with fibrosis beneath the mucosa, hyperplasia or hypertrophy of the bronchial smooth muscle, increase in mucous producing cells, and changes in vascular supply and endothelial function (Avdalovic 2015). The process is generally referred to as airway remodeling. Based upon the critical role of inflammation and the prominent pathology of bronchospasm, treatments have traditionally and overwhelmingly focused on anti-inflammatory medications and smooth muscle dilators that act locally in the airway. Emerging understanding of the various drivers of inflammation as well as the ability to more easily measure the degree of inflammation has created new areas of study for therapeutic targets and preventative strategies.
4 Diagnosis
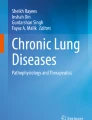
Diagnosis of asthma is based on clinical factors combined with measurement of lung function demonstrating obstruction, variability, and, typically, reversibility (GINA 2018). No single, isolated element defines the diagnosis. Spirometry is used to assess the volume of air that can be exhaled under maximal effort in an individual. The forced expiratory volume in 1 s (FEV1) as well as during the entire respiratory cycle (FVC) is assessed with spirometry. By comparing these two values, physicians can determine the presence of airflow obstruction in the lung. The FEV1/FVC ratio is predictable based on the patient’s age, gender, ethnicity, and height. A FEV1/FVC ratio less than 0.70–0.75 is generally indicative of airway obstruction; older patients may have a lower baseline without clinical obstruction and younger patients may exhibit airflow obstruction at higher ratios based on epidemiologic studies (Stanojevic et al. 2008). The airflow obstruction resultant from bronchial constriction and inflammation in the airways results in prolonging the time it takes for chest wall and alveolar recoil to propel air from the lungs thereby decreasing the FEV1 (Figs. 1 and 2).

Spirometry being performed

Volume-time plot for spirometry comparing normal and obstructive disease
In addition to demonstrating the airflow obstruction in patients with suspected asthma, the physician assesses the presence of reversibility of this obstruction (Fig. 3). Reversibility is generally considered a hallmark of asthma and a key distinguishing characteristic from chronic obstructive pulmonary disease (COPD). However, evolving understanding of how obstruction in asthma can become irreversible over time, due to remodeling of the airway, and in the nuanced understanding of patient-specific phenotypes and genotypes has led to greater appreciation that reversibility is not universally present. The accepted definition of reversibility is an increase in FEV1 of 200 mL and greater than 12% from baseline in response to inhalation of a bronchodilator (GINA 2018). FVC and FEV1/FVC ratio may also increase, but the FEV1 is generally the most reliable parameter for assessing reversibility. Reversibility may also be evaluated over a period of days to weeks following initiation of anti-inflammatory therapy, such as inhaled or oral corticosteroids (Table 1) .

Flow-volume loop from spirometry demonstrating normal, obstructive, and restrictive patterns
4.1 Biomarkers in Asthma
Supporting diagnostic features of asthma include elevated sputum eosinophil counts, elevated peripheral blood eosinophil counts, elevated serum IgE levels, increased concentration of exhaled nitric oxide (FeNO), and elevated serum periostin levels (Berry and Busse 2016). Sputum eosinophilia is the most well-described marker in asthma and has been part of the traditional understanding of allergic-asthma associated with atopy. However, as emerging understanding of various subsets of asthma has grown so too have the possible biomarkers which can be used to define the disease, treatment, or response. Furthermore, sputum eosinophils are not easily obtained and therefore have more limited clinical utility outside of clinical trials and basic science research.
Periostin has emerged as an increasingly relevant matrix protein implicated in multiple types inflammatory processes and diseases. It plays a role in fibroblast recruitment that contributes to organ fibrosis. Periostin is elevated in several types of inflammatory diseases including but not limited to: otitis media, bone marrow fibrosis, proliferative diabetic retinopathy, IgG-4 sclerosing disease, and scleroderma (Li et al. 2015). Atopic diseases, and particularly diseases associated with eosinophilia and/or increased IL-13 secretion, are strongly associated with periostin elevation. Atopic dermatitis, asthma, allergic rhinitis, and eosinophilic esophagitis are all positively correlated with increased blood periostin (Dellon et al. 2016). Asthma patients with elevated periostin are more likely to have late, adult onset asthma, concomitant nasal polyps and hyperplastic rhinitis, lower lung function, and aspirin sensitivity (Matsusaka et al. 2015).
Exhaled nitric oxide shows a relationship with airway inflammation and its elevation may predict responsiveness to inhaled corticosteroids in patients with asthma. However, titration of corticosteroid dose to lower exhaled nitric oxide is not associated with reduction of asthma exacerbation risk as consistently as the suppression of sputum eosinophilia (Jia et al. 2012).
Elevated IgE levels have long been linked with risk of asthma and risk of exacerbations (Platts-Mills 2001). This is most predominant in patients with allergic trigger-induced asthma. These patients frequently demonstrate allergen-specific IgE increases and a hypersensitivity on prick testing to specific allergens.
Blood eosinophilia is a reasonably accurate surrogate marker of sputum eosinophilia, which is more difficult to obtain and to standardize (Wagener et al. 2014).
The use of these biomarkers does not supplant the role of a thorough clinical history, understanding of the nuance of the presentation of asthma, skilled physical diagnostics, and use of spirometry for lung function assessment. However, their identification and description of biomarkers has helped in the evolution of better understanding of the heterogeneity of asthma and, in particular, the assessment of patients with difficult to control disease or asthma unresponsive to corticosteroids.
5 Presentation and Phenotypes
Numerous symptoms are related to asthma. There are contributing signs from comorbid conditions, which may or may not be present, and many patients have only intermittent or transient complaints. As such, recognizing asthma can be difficult and categorizing asthma has been challenging. A phenotype is the set of observable characteristics of a person relating to the interaction of their genetic profile with the environment. Experts have described as many as nine phenotypes with overlap in the same patient (Lockey 2009) and considerable variation exists between asthma patients in the measurements used to categorize the disease (Busse et al. 2014). Such measurements include symptoms questionnaires, peripheral blood eosinophil count, IgE levels, degree of responsiveness to inhaled corticosteroids, and exhaled nitric oxide quantity.
Patients may describe a history of cough and wheeze associated with viral infections in childhood and adolescence. There is often an atopic family or personal history including allergic rhinosinusitis, conjunctivitis, and eczema. Some patients do not present until later in life with chest tightness related to physical activity or nondescript breathlessness. The heterogeneity of asthma’s presentation to the physician mirrors the array of inflammatory pathways and mediators that have been described in its pathogenesis. Describing asthma by phenotype is a useful classification tool to help clinicians consider the diagnosis and understand the disease. It should be noted that an individual patient may demonstrate overlap in their phenotype and they are therefore not exclusionary.
5.1 Allergic Asthma
Allergic asthma is the most prototypical and also the most common phenotype of asthma. This form of asthma is characterized by allergic sensitization to an allergen and a clinical history consistent with respiratory symptoms as a result of exposure to the antigen. Allergic asthma is more common in childhood asthma and is associated with a younger age of onset than other phenotypes. However, allergic asthma is still relevant in the adult population with asthma where the prevalence is described as 60–75% of those with asthma (Lockey 2009). Sensitization is verified by either a positive reaction to skin prick testing or by detection of antigen-specific IgE in the patient’s serum. Common antigens are fungal species, such as Aspergillus and Alternaria, dog, cat, grass, pollen, dust mite, and cockroach. Patients often describe perennial symptoms when they have sensitivity to nonseasonal allergens or with classic seasonal symptoms during pollen seasons. Family history of allergies and associated rhinosinusitis are frequently present. Patients classically have elevated eosinophil counts in sputum and serum, elevated IgE, and elevated periostin.
5.2 Nonallergic/Intrinsic Asthma
Nonallergic, or intrinsic, asthma has been difficult to define clinically and has been given various nomenclature over time. Predominantly, this form of asthma has been described more in how it differs from prototypical allergic asthma than in a cogent, unified phenotype in itself. Nonallergic asthma typically presents later in life is not associated with seasonal variation driven by aeroallergens and lacks the association with other atopic diseases. Literature often refers to intrinsic asthma as being synonymous with neutrophilic asthma. Patients with intrinsic asthma are more likely to have severe asthma and asthma that is poorly responsive to inhaled corticosteroids as compared to allergic asthma. There is an absence of skin prick test positivity or antigen-specific IgE and the total IgE in the serum is not elevated. Interestingly, IgE has been demonstrated in the airways of patients who lack atopic history or antigen-specific serum IgE and therefore are not characterized as allergic. Specific IgE directed against bacterial superantigens derived from staphylococcal species have been identified. Presence of superantigens may contribute to the poor responsiveness to inhaled corticosteroids that intrinsic asthma patients can display (Barnes 2009). However, the presence of eosinophilotactic cytokines and IgE in these patients shares homology with allergic asthma. Therefore, the inflammatory cascade in intrinsic and allergic asthma may have greater similarity than previously believed (Tak et al. 2015).
5.3 Aspirin Exacerbated Respiratory Disease
Aspirin-exacerbated respiratory disease has been known by various names as well. Sampter’s Triad, Aspirin Triad, Aspirin Sensitive Asthma, and Aspirin or Nonsteroidal Anti-inflammatory Drug Exacerbated Asthma (AERD or NERD) have all been descriptive terms for the phenomenon. Epidemiologic studies suggest this form of asthma may be more common than commonly recognized. Some studies indicate the prevalence may be as high of 21% of adult asthmatics when tested by oral provocative challenge with aspirin (Lockey 2009). The age of onset is typically in early to mid-adulthood, though this may represent a diagnostic lag from lack of recognition. There is a slight female predominance in population analysis (Lockey 2009). AERD is classically associated with nasal polyposis, chronic rhinosinusitis, and peripheral eosinophilia. Frequently, the nasal symptoms of congestion, rhinorrhea, and anosmia precede the diagnosis or recognition of asthma, often by several years. Rhinosinusitis symptoms may be refractory to typical treatments and patients have a higher recurrence of polyposis after sinus surgery and more frequent need for repeat sinus surgery (Stevens and Schleimer 2016). The phenotype is defined by a documented asthmatic response after ingestion of aspirin or other nonsteroidal anti-inflammatory.
5.4 Infection-Induced Asthma
In patients with infection-induced asthma, the respiratory tract infection influences the asthma in several ways. Some patients are diagnosed with asthma after they have persistent wheezing, cough, and shortness of breath during and after a respiratory infection. In others, preceding asthma is exacerbated by the inflammatory response to infection. Respiratory infection can be the only trigger for asthma in patients or can be one of a multitude of triggers in patients with other coexisting phenotypes, such as allergic asthma or AERD. Chronic rhinosinusitis exacerbated by acute infections can contribute to the airway symptoms in these patients. Infection is recognized as an impetus for severe asthma exacerbations in patients with all types of asthma. Respiratory syncytial virus (RSV), parainfluenza virus, human metapneumovirus, rhinovirus, and influenza virus have all been identified in patients with asthma exacerbations. In particular, the role of RSV in relationship to severe asthma exacerbations, as well as risk of asthma later in life in children, has been well described (Sigurs et al. 2005). However, more recent studies also postulate a role for mycoplasma and chlamydial infections in the pathogenesis of asthma development (Johnston and Martin 2005).
5.5 Exercise-Induced Bronchospasm
Exercise-induced bronchospasm (EIB), formerly referred to as exercise-induced asthma, is a complex phenomenon that creates confusion among patients and physicians. EIB manifests with chest tightness, cough, and wheeze that occurs after exercise. Symptoms typically peak approximately 10–15 min after cessation of vigorous activity. EIB is present in a substantial percentage of world-class athletes; estimates are as high as 25% of Olympic athletes and even 55% of endurance, cold-weather athletes (Molis and Molis 2010). A significant portion of patients with EIB do not have concomitant asthma when evaluated with provocation testing. Therefore, the diagnosis or suspicion of EIB should not lead to the assumption of underlying asthma. That being said, the majority of asthmatic patients will experience EIB when they exert themselves to a sufficiently high degree. Due to the inherent episodic and variable nature of asthma, occasionally, patients with mild intermittent asthma are labeled as having EIB. EIB is believed to be due to evaporative water and/or heat loss in the airway during exercise. Rapid breathing through the mouth during endurance exercise bypasses the humidifying and warming properties of the nasal passage resulting in cold, dry air interacting with the lower airway. Inflammatory mediators are augmented by this process resulting in bronchospastic response and symptoms. Interestingly, patients may experience a refractory period, wherein subsequent exercise does not trigger symptoms, for up to 4 h after the initial onset (Lockey 2009). EIB can be treated by pretreatment with inhaled short-acting beta-agonist therapy or oral montelukast.
5.6 Asthma COPD Overlap Syndrome
Asthma COPD overlap syndrome (ACOS) has emerged as an increasingly recognized, though controversial, phenotype of obstructive lung disease. Patients with this condition have features that are typical of chronic obstructive lung disease (COPD), such as chronic respiratory symptoms and poor reversibility on spirometry. However, they also display characteristics of intermittent worsening of symptoms and qualities of asthma phenotypes listed above: history of aeroallergen sensitization, personal and family history of atopy, and wheezing after respiratory infections. Often these individuals have a history of exposure to inhaled particles (e.g., environmental and occupational air pollutants, tobacco smoke) that are recognized to cause permanent lung damage. COPD and asthma share a common final pathway of airway remodeling, mucous production and resultant lung dysfunction, although the characteristics of the remodeling differ between asthma and COPD. Epidemiologic studies have demonstrated that poorly controlled asthma in childhood confers a greater risk for the development of fixed airway obstruction earlier in life (McGeachie et al. 2016). Cohorts of patients with chronic respiratory symptoms and poor reversibility, which suggest COPD, but also report a history of asthma, have increased frequency of exacerbations, increased healthcare utilization, and a more rapid decline in lung function (Hardin et al. 2014). Patients with ACOS have a reduced FEV1/FVC ratio that typically remains less than 0.7 after bronchodilator. However, they may exhibit a pronounced response to bronchodilator therapy with increase >12% of baseline FEV1 or of >400 mL.
6 Comorbid Conditions
Numerous comorbid conditions can affect response to therapy or obscure the diagnosis of asthma. Prominent comorbid conditions that worsen asthma include: chronic rhinosinusitis, gastroesophageal reflux disease (GERD) , obesity, obstructive sleep apnea, and depression (GINA 2018). Assessment for and management of these conditions is recommended for patients who have atypical asthma features or demonstrate poor responsiveness to therapy after formal diagnosis of asthma. The prevalence of vocal cord dysfunction is unknown but may affect up to 20% of subjects with asthma (Yelken et al. 2009). Vocal cord dysfunction may be aggravated by inhaled therapy for asthma resulting in the misperception of treatment resistant asthma. Less common conditions to consider in selected asthma cases include: hypersensitivity pneumonitis, eosinophilic bronchitis, atopic cough, bronchiectasis with or without associated immunodeficiency, bronchiolitis with or without connective tissue disease, interstitial fibrosis, cardiac failure with wheeze, and pulmonary hypertension. Patients with these conditions often complain of shortness of breath, cough, or wheeze and therefore can be mislabeled as having asthma due to the common nature of asthma in the general population. However, these conditions are not associated with bronchial hyperreactivity with provocation testing, such as methacholine, or variability in lung function (Morjaria and Kastelik 2011). The most difficult situations arise when patients have the presence of asthma alongside one of these mimicking conditions; symptoms are inevitably worse and escalation of asthma therapy does not improve the control of the comorbid condition.
Asthma plus syndromes include conditions where asthma is a defining feature of the disease with additional pathology that manifests as the phenotypic disease process. These include eosinophilic granulomatosis with polyangiitis (EGPA formerly designated Churg Strauss vasculitis) and allergic bronchopulmonary aspergillosis (ABPA). EGPA is defined by the vasculitis that coexists with asthma and requires systemic immunosuppression therapy to control disease. Pauci-immune glomerulonephritis and eosinophilia are hallmarks of the disease. ABPA describes patients with asthma that is exacerbated by sensitization to Aspergillus species or other select fungal genera. There is no universally accepted standards for diagnosis but suggested criteria include: presence of asthma, skin prick test positivity or specific IgE to Aspergillus species, elevated total IgE (typically >1000 IU/mL), precipitating serum antibodies to Aspergillus fumigatus or other species, radiographic abnormalities consistent with ABPA (bronchiectasis, mucous plugging, mosaic pattern air trapping), and eosinophilia (>500 cells/μL) (Agarwal et al. 2013) (Table 2).
7 Treatment
Treatment of asthma requires an understanding of core principles but also a recognition of the availability of alternate therapies and indications for referral to specialists. The focus of this chapter is the approach to core principles of treatment. Further details regarding biologic therapy and immunotherapy for desensitization is included elsewhere in this work. It is important to recognize that close follow-up with patients to assess treatment response is a critical component of the care of the asthmatic patient. When symptoms are not improving, physicians should broaden their scope to think of comorbid or mimicking conditions as discussed above.
Education of the patient, on inhaler technique and awareness of symptoms, is fundamental to asthma treatment. This step at face value appears rudimentary but its importance cannot be overstated. Patient awareness of asthma activity and early intervention options improves outcomes (GINA 2018).
Therapy for asthma focuses on controller and rescue medications and is driven by patient symptoms and categorization of asthma by severity. There are many tables and references which outline the assessment of asthma severity and the appropriate controller medications to be considered based upon this assessment. Symptom severity is dependent on use of rescue medications, nighttime awakenings due to asthma symptoms, and limitation of activities. Asthma assessment requires measurement of lung function, usually with a peak expiratory flow rate or FEV1 measurement. A stepwise approach is recommended by experts. This includes increasing the intensity of current therapy and adding additional agents when patients are not controlled and carefully reducing the intensity of therapy when patients demonstrate a sustained response and disease control (Tables 3 and 4).
The cornerstone of asthma control is the use of inhaled corticosteroid (ICS) therapy. This the most important pharmacologic component of asthma care. It does not provide immediate relief of symptoms but suppresses the inflammatory response in the airway that drives the underlying pathophysiology. Control of the inflammatory process is critical for long-term preservation of lung function, reduction in exacerbations, control of healthcare costs, and improvement in quality of life. ICS are organized in tiers of potency based on the concentration of the corticosteroid (Tables 5 and 6) .
Inhaled corticosteroid therapy is safe and well tolerated. Dysphonia, oral candidiasis (thrush), and cough are the typical local side effects patients report. These effects are dose-dependent and a majority of patients report experiencing at least one of them (Williamson et al. 1995). The use of a spacer device and rinsing the mouth after ICS inhaler use reduces the likelihood of thrush. However, the dysphonia and cough result from laryngeal deposition and thus do not improve with these measures. Systemic effects are rare and typically only seen in patients using high dose ICS for prolonged duration. There is a measurable effect on suppression of the hypothalamic-pituitary-adrenal axis but the effect resolves when ICS therapy decreases and clinically significant adverse events are exceptionally rare (Kelly and Nelson 2003). There is also a marginal increased risk of osteoporosis with high-dose ICS taken for extended time periods (Kelly and Nelson 2003), and physicians can consider this when prescribing therapy in patients at a baseline higher risk of fracture. Reduction in growth velocity occurs in children receiving ICS therapy (CAMP 1999). This reduction in velocity of growth is typically transient after the first year of therapy but monitoring children to ensure return to normal growth patterns is a reasonable consideration. ICS use is additionally a risk factor for the development of glaucoma (Mitchell et al. 1999) and cataracts (Garbe et al. 1998). Highest risk for both of these conditions was in patients using high dose ICS for prolonged periods. Many of the reported side effects of ICS are confounded by intermittent or prior use of systemic corticosteroid therapy (Tables 7 and 8).
When ICS therapy alone is not sufficient for long-term symptom control, the addition of long-acting bronchodilators is the most typical next step in treatment. Long-acting beta-agonists (LABA) as well as long-acting anti-muscarinic agents (LAMA) are used in this capacity. There are numerous combination preparations of long-acting bronchodilators and ICS and choice of agents should be based on cost to patient with consideration of insurance coverage and potency of ICS. Long-acting bronchodilator agents are not recommended as monotherapy in asthma as there is an increased risk of mortality in asthmatic patients treated this way. The US package label of ICS combination products with LABAs previously contained a warning statement of increased asthma death with LABAs. This statement was removed from ICS/LABA combination products in 2017 after several safety studies failed to confirm a risk of severe exacerbations or death with ICS plus LABA therapy. LAMA therapy has not been associated with increased asthma risk but is not recommended as monotherapy.
Additional medications to be considered when standard therapy is not effective or clinical conditions dictate include: leukotriene modifying agents, biologic therapies, immunotherapy, and theophylline. With the exception of leukotriene modifying agents, which are well tolerated and effective in the treatment of allergic asthma, use of these therapies should generally be done under the guidance of an asthma specialist. Further discussion about the details regarding biologic therapy (anti-interleukin (IL)-5, anti-IgE) is covered elsewhere and beyond the scope of this chapter.
Select patients with limited and sporadic symptoms, those with mild intermittent asthma or EIB for example, can use short-acting rescue therapy as their only pharmacologic management.
All asthmatic patients should be given access to and education on the use of rescue medications. Short-acting bronchodilators, typically short-acting beta-agonists but also short-acting anti-muscarinic medications, are central to rescue from symptoms of wheeze, chest tightness, and shortness of breath. These medications are important in symptom control and rapid relief, but their use should be monitored by patients and physicians alike and increased use is a clear sign of poor overall control. The use of short-acting agents is accepted as a marker of increased risk for worsening lung function and active asthma inflammation (GINA 2018). There is some newer research that indicates that as needed use of combination ICS/LABA with variable dosing, that is as a rescue medication in addition to being utilized as a controller medication, is as or more effective than ICS/LABA fixed dose therapy as a controller with short-acting beta-agonist as rescue (Sobieraj et al. 2018).
Systemic corticosteroids are the mainstay treatment of significant exacerbations and rapid symptom improvement. Their side effects are well known and include hyperglycemia, hypertension, psychomotor activation, osteoporosis, diaphoresis, and others. Use of systemic corticosteroids is sometimes necessary chronically in a subset of severe asthma patients; these patients should be under the care of an asthma specialist who may consider use of advanced therapies based on biomarkers and phenotype. In some patients, often refractory to traditional therapy and disproportionately affected by exacerbations, the response to corticosteroids is blunted or lacking. Genetic alterations related to corticosteroid receptor function and responsiveness to corticosteroid administration have been identified in subpopulations (Sousa et al. 2000). Furthermore, increased numbers of neutrophils in the inflammatory substrate of some asthmatic patients and demonstration that these neutrophils do not respond as vigorously to corticosteroid-induced signaling has led to greater understanding of corticosteroid-resistant patients (Wang et al. 2016).
8 Conclusion
Asthma is a heterogeneous syndrome characterized by recognizable symptoms that are a manifestation of inflammation and maintained by a multitude of factors. Physicians need to understand the diagnosis of the disease based on measurable obstruction and variability as well as the conditions that accompany and mimic asthma. Therapy involves several medication types and potencies and guidelines are widely available to help guide clinical decision-making. Therapy should be directed at controlling inflammation and close follow-up with patients to ensure symptom control is critical to success and preservation of lung function. Whenever patients have poor response to fundamental treatments, physicians should consider referral to advanced specialists to guide care (Table 9).
References
Agarwal R, Chakrabarti A, Shah A, Gupta D, Meis JF, Guleria R, et al. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy. 2013;43(8):850.
Akinbami LJ, Moorman JE, Bailey C, Zahran HS, King M, Johnson CA, Liu X. Trends in asthma prevalence, health care use, and mortality in the United States, 2001–2010. Center for Disease Control. 2012. M.Sc. https://www.cdc.gov/nchs/products/databriefs/db94.htm. Accessed 15 May 2018.
Avdalovic M. Pulmonary vasculature and critical asthma syndromes: a comprehensive review. Clin Rev Allergy Immunol. 2015;48(1):97–103. https://doi.org/10.1007/s12016-014-8420-4.
Barnes PJ. Intrinsic asthma: not so different from allergic asthma but driven by superantigens? Clin Exp Allergy. 2009;39(8):1145–51. https://doi.org/10.1111/j.1365-2222.2009.03298.x.
Berry A, Busse WW. Biomarkers in asthmatic patients: has their time come to direct treatment? J Allergy Clin Immunol. 2016;137(5):1317–24. https://doi.org/10.1016/j.jaci.2016.03.009.
Blumenthal MN, Fine L. Definition of an allergen (Immunobiology). In: Lockey RF, Ledford DK, editors. Allergens and allergen immunotherapy: subcutaneous, sublingual and oral. Boca Raton: CRC Press; 2014. p. 25–35.
Busse WW, Holgate ST, Wenzel SE, Lin S, Lin SL, Chon Y, et al. Disease characteristics of asthma phenotypes: a pooled analysis of two phase 2 clinical trials. Am J Respir Crit Care Med. 2014;189:A1336.
Childhood Asthma Management Program (CAMP): design, rationale, and methods. Childhood Asthma Management Program Research Group. Control Clin Trials. 1999;20(1):91–120.
Dellon ES, Higgins LL, Beitia R, Rusin S, Woosley JT, Veerappan R, et al. Prospective assessment of serum periostin as a biomarker for diagnosis and monitoring of eosinophilic esophagitis. Aliment Pharmacol Ther. 2016;44(2):189–97. https://doi.org/10.1111/apt.13672.
Fahy JV. Identifying clinical phenotypes of asthma: steps in the right direction. Am J Respir Crit Care Med. 2010;181(4):296–7. https://doi.org/10.1164/rccm.200911-1702ED.
Garbe E, Suissa S, LeLorier J. Association of inhaled corticosteroid use with cataract extraction in elderly patients. JAMA. 1998;280(6):539–43.
Global Initiative for Asthma (GINA). Global Strategy for Asthma Prevention and Management. 2018. http://ginasthma.org/download/836. Accessed 12 May 2018.
Hardin M, Cho M, McDonald ML, Beaty T, Ramsdell J, Bhatt S, et al. The clinical and genetic features of COPD-asthma overlap syndrome. Eur Respir J. 2014;44(2):341–50.
Holgate ST. Pathogenesis of asthma. Clin Exp Allergy. 2008;38(6):872–97. https://doi.org/10.1111/j.1365-2222.2008.02971.x.
Jia G, Erickson RW, Choy DF, et al. Periostin is a systemic biomarker of eosinophilic airway inflammation in asthmatic patients. J Allergy Clin Immunol. 2012;130(3):647 e10–54 e10.
Johnston SL, Martin RJ. Chlamydophila pneumoniae and mycoplasma pneumoniae: a role in asthma pathogenesis? Am J Respir Crit Care Med. 2005;172(9):1078–89.
Kelly HW, Nelson HS. Potential adverse effects of the inhaled corticosteroids. J Allergy Clin Immunol. 2003;112(3):469–78; quiz 79.
Ledford R, Feldman M, Casale T. Medication for asthma and COPD. In: Bernstein JA, editor. Asthma, COPD and the overlap syndrome: a case-based overview of similarities and differences. Boca Raton: CRC Press; 2018. p. 181–200.
Li W, Gao P, Zhi Y, Xu W, Wu Y, Yin J, et al. Periostin: its role in asthma and its potential as a diagnostic or therapeutic target. Respir Res. 2015;16(1):57. https://doi.org/10.1186/s12931-015-0218-2.
Lloyd CM, Hessel EM. Functions of T cells in asthma: more than just TH2 cells. Nat Rev Immunol. 2010;10(12) https://doi.org/10.1038/nri2870.
Lockey RF. Defining phenotypes: expanding our understanding of asthma challenges in treating a heterogeneous disease world allergy organization. 2009. http://www.worldallergy.org/UserFiles/file/NHLBI%20Asthma%20Phenotypes-Lockey.pdf. Accessed 18 May 2018.
Matsusaka M, Kabata H, Fukunaga K, Suzuki Y, Masaki K, Mochimaru T, et al. Phenotype of asthma related with high serum periostin levels. Allergol Int. 2015;64(2):175–80.
McGeachie MJ, Yates KP, Zhou X, Guo F, Sternberg AL, Van Natta ML, et al. Patterns of growth and decline in lung function in persistent childhood ashtma. N Engl J Med. 2016;374(19):1842–52.
Mitchell P, Cumming RG, Mackey DA. Inhaled corticosteroids, family history, and risk of glaucoma. Ophthalmology. 1999;106(12):2301–6.
Molis MA, Molis WE. Exercise-induced bronchospasm. Sports Health. 2010;2(4):311–7. https://doi.org/10.1177/1941738110373735.
Morjaria JB, Kastelik JA. Unusual asthma syndromes and their management. Ther Adv Chronic Dis. 2011;2(4):249–64. https://doi.org/10.1177/2040622311407542.
National Institutes of Health; National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program. Expert panel report 3: guidelines for the diagnosis and management of asthma. 2007. http://www.nhlbi.nih.gov/files/docs/guidelines/asthsumm.pdf. Accessed 20 May 2018.
Nurmagambetov T, Kuwahara R, Garbe P. The economic burden of asthma in the United States, 2008–2013. Ann Am Thorac Soc. 2018;15(3):348–56. https://doi.org/10.1513/AnnalsATS.201703-259OC.
Pelaia G, Vatrella A, Busceti MT, Gallalelli L, Calabrese C, Terraciano R, et al. Cellular mechanisms underlying eosinophilic and neutrophilic airway inflammation in asthma. Mediat Inflamm. 2015. 8 pages; https://doi.org/10.1155/2015/879783.
Platts-Mills TA. The role of immunoglobulin E in allergy and asthma. Am J Respir Crit Care Med. 2001;164(8 Pt 2):S1–5.
Sigurs N, Gustafsson PM, Bjarnason R, Lundberg F, Schmidt S, Sigurbergsson F, et al. Severe respiratory syncytial virus bronchiolitis in infancy and asthma and allergy at age 13. Am J Respir Crit Care Med. 2005;171(2):137–41.
Sobieraj DM, Weeda ER, Nguyen E, Coleman CI, White CM, Lazarus SC, et al. Association of inhaled corticosteroids and long-acting β-agonists as controller and quick relief therapy with exacerbations and symptom control in persistent asthma: a systematic review and meta-analysis. JAMA. 2018;319(14):1485–96. https://doi.org/10.1001/jama.2018.2769.
Sousa AR, Lane SJ, Cidlowski JA, Staynov DZ, Lee TH. Glucocorticoid resistance in asthma is associated with elevated in vivo expression of the glucocorticoid receptor β-isoform. J Allergy Clin Immunol. 2000;105:943–50.
Stanojevic S, Wade A, Stocks J, Hankinson J, Coates AL, Pan H, et al. Reference ranges for spirometry across all ages: a new approach. Am J Respir Crit Care Med. 2008;177(3):253–60.
Stevens WW, Schleimer RP. AERD as an Endotype of chronic rhinosinusitis. Immunol Allergy Clin N Am. 2016;36(4):669–80. https://doi.org/10.1016/j.iac.2016.06.004.
Tak T, Hilvering B, Tesselaar K, Koenderman L. Similar activation state of neutrophils in sputum of asthma patients irrespective of sputum eosinophilia. Clin Exp Immunol. 2015;182(2):204–12. https://doi.org/10.1111/cei.12676.
Wagener AH, de Nijs SB, Lutter R, Sousa AR, Weersink EJM, Bel EH, et al. External validation of blood eosinophils, FENO and serum periostin as surrogates for sputum eosinophils in asthma. Thorax. 2014;70:1–6. https://doi.org/10.1136/thoraxjnl-2014-205634.
Wang M, Gao P, Wu X, Chen Y, Feng Y, Yang Q, et al. Impaired anti-inflammatory action of glucocorticoid in neutrophil from patients with steroid-resistant asthma. Respir Res. 2016;17(1):153.
Williamson IJ, Matusiewicz SP, Brown PH, Greening AP, Crompton GK. Frequency of voice problems and cough in patients using pressurized aerosol inhaled steroid preparations. Eur Respir J. 1995;8(4):590–2.
Yelken K, Yilmaz A, Guven M, Eyibilen A, Aladag I. Paradoxical vocal fold motion dysfunction in asthma patients. Respirology. 2009;14:729–33. https://doi.org/10.1111/j.1440-1843.2009.01568.x.
Author information
Authors and Affiliations
Corresponding author
Section Editor information
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this entry

Cite this entry
Ledford, R. (2019). Adult Asthma. In: Allergy and Asthma. Springer, Cham. https://doi.org/10.1007/978-3-030-05147-1_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-05147-1_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-05146-4
Online ISBN: 978-3-030-05147-1
eBook Packages: MedicineReference Module Medicine