
Abstract
Background
Management of cardiovascular risk factors includes commitment from patients to adhere to prescribed medications and adopt healthy lifestyles. Unfortunately many fail to take up and maintain the four key healthy behaviours (not smoking, having a balanced diet, limiting alcohol consumption and being more active). Five factors (beliefs, knowledge, transport and other costs, emotions, and friends and family support) are known to predict uptake of lifestyle behaviour change. The key factors influencing maintenance of healthy lifestyles are not known but would be helpful to support the development of relapse prevention programmes for this population. Our review aimed to clarify the main patient perceived factors thought to influence maintenance of changed healthy lifestyles.
Methods
We performed a systematic review of qualitative observational studies and applied the principles of content synthesis and thematic analysis to extract reported factors (barriers and facilitators) considered by individuals to be influential in maintaining changed healthy lifestyle behaviours. Factors were then organised into an existing framework of higher order categories which was followed by an analysis of the interrelationships between factors to identify key themes.
Results
Twenty two studies met our inclusion criteria. Participants reported barriers and facilitators within 13 categories, the majority of which were facilitators. The most commonly reported influences were those relating to social support (whether provided formally or informally), beliefs (about the self or the causes and management of poor health, and the value of maintaining lifestyle behaviours), and other psychological factors (including attitude, thinking and coping styles, and problem solving skills). Physical activity was the most commonly investigated behaviour in four categories, but overall, the main barriers and facilitators were related to a range of behaviours. Through analysis of the interrelationships between factors within categories, ‘social support’, ‘education and knowledge’, and ‘beliefs and emotions’ were all considered key themes.
Conclusions
Our review suggests that for the most part, factors that influence lifestyle change are also important for maintaining healthy behaviours. This indicates that addressing these barriers and facilitators within lifestyle support programmes would also be of value in the longer-term.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Evidence supporting the role of healthy lifestyles in the prevention and management of a range of long-term conditions including cardiovascular disease is compelling [1, 2]. Despite this, many individuals struggle to take up and maintain healthy lifestyle behaviours. Uptake for cardiac rehabilitation, for example, is poor (44%) [3] and there are high attrition rates for commercial weight management programmes [4]. For those who are successful in making changes, relapse rates are high. For example, over 75% of quitters return to smoking within one year [5, 6], and 50% of dieters regain lost weight after one year [7]. Poor uptake rates can be attributed to a myriad of social, psychological and practical barriers that are challenging to address within healthcare consultations. However, by focusing on a few factors that are known to predict uptake (beliefs, knowledge, transport and other costs, emotions, and support from family and friends) [8, 9], practitioners can start to consider the most appropriate type and level of support for each individual. As with uptake, there are likely to be a range of factors that influence an individual’s ability to maintain their healthy behaviours. Knowledge of the main barriers and facilitators that influence maintenance of healthy lifestyles could be used by formal programmes to develop more effective behavioural relapse prevention interventions.
Much of the theory and evidence informing relapse prevention strategies comes from the addictions literature in relation to alcoholism, smoking and obesity [10–12], with comparatively little relating to physical activity and poor diet. Whilst all these behaviours are important in the context of reducing cardiovascular risk, we hypothesise that the types of barriers and facilitators and thereafter the relapse prevention strategies observed in the addictions literature may not be fully appropriate or comprehensive for individuals at high risk of cardiovascular events (including diabetes, hypertension, and hypercholesterolemia). Many patients in this category will need to change and maintain multiple lifestyle behaviours that involve diet modification, alcohol reduction and increased physical activity levels, with clinical aims and benefits that may be less tangible to the lay person. This is particularly the case for those who have been given a prospective cardiovascular risk score through screening, a common practice in primary care in many developed countries [13–16]. Further, this particular population may perceive more severe consequences and greater levels of fear associated with failure of lifestyle change compared to individuals with, for example, obesity in the absence of other cardiovascular risk factors. Finally, lifestyle management of individuals at high risk of cardiovascular events may not necessarily involve provision of statutory services such as smoking cessation or obesity weight management, and rates of relapse might be different than in those who change their behaviours without formal support [12]. Given these uncertainties, we considered it important to conduct a thorough review of the literature to elicit the main factors that influence maintenance of lifestyle behaviour change in individuals at high risk of cardiovascular events. Our ultimate aim is to inform the development of relapse prevention interventions that are relevant to these particular populations.
Methods
Selection criteria
We included empirical qualitative observational studies reporting factors related to the maintenance of specified lifestyle behaviours (diet for weight loss or healthy eating purposes, alcohol consumption, smoking and physical activity). Participants were adults (≥18 years) who: were previously or currently obese (BMI ≥30); experienced angina, myocardial infarction or transient ischemic attack or; were living with coronary artery disease, chronic obstructive pulmonary disease(COPD), hypertension, hyperlipidemia, metabolic syndrome or type II diabetes. Studies were excluded if they focused on a selected population such as tribal groups or people with mental health difficulties.
Given the range of definitions of maintenance for the numerous healthy lifestyle behaviours [17–22], and the lack of clear consensus on which is most appropriate, we adopted a flexible approach to guide study selection and data extraction. Studies were required to demonstrate that at least some of the participants had, at some point in the past, successfully made changes to their lifestyle and that any current attempts to maintain the changed behaviours were without any on-going formal support programme, such as, for example, weight management or smoking relapse prevention support. However, studies involving those attending a local leisure centre by their own volition and those receiving ongoing support as part of their condition (i.e. attending a diabetes clinic) would be included. Studies including data on both changing and maintaining lifestyles needed to report separate findings for each.
Searching
An electronic search strategy was developed (available on request from authors) and run (November 2011) in Embase, Medline, PsycInfo, Applied Social Sciences Index and Abstracts (ASSIA), Allied and Complimentary Medicine (AMED) databases. Key search terms were also applied in Cumulative Index to Nursing and Allied Health (CINAHL), and all databases were searched from 1970 onwards or from database inception if more recent. Search results (managed in Endnote, Version X5) underwent title, abstract and full paper screening by at least two independent reviewers (JM, GF, SH, ACB) against pre-defined selection criteria. Disagreements about inclusion were referred to a third reviewer, and all were resolved. Personal contact was made with authors of several papers to clarify details necessary for determining inclusion. Non-response led to exclusion.
Data extraction: identification of factors
Data extraction of factors reported in included studies was performed independently by at least two reviewers (SH, GF, JM, ACB) followed by consensus checking. We extracted those factors demonstrating consensus between participants and deemed them relevant if they were reported as helping (facilitators) or hindering (barriers) maintenance of healthy lifestyle behaviours. Each factor was entered as an individual record into a Microsoft Excel 2007 spreadsheet along with contextual data relating to the health condition and behaviour(s) under investigation, and facilitator or barrier status.
Data analysis: aggregation of factors into categories
Through an iterative process involving interpretation and consensus (GF & JM), we then systematically applied principles of content synthesis and thematic analysis [23, 24]. This involved a detailed analysis of extracted factors and their interrelationships, and, wherever possible, organising extracted factors to an existing framework of higher order categories [25]. As the previous framework was derived from literature that primarily focused on changing behaviours, extracted factors that did not fit were grouped and assigned to new categories.
Identification of key themes
Two reviewers (GF & JM) simultaneously reviewed individual factors within each category to identify links with other categories. Links were then used to create a relationship map (Figure 1). JM and GF then examined the map to identify categories that might represent key themes. This involved identification of the categories that appeared to occupy a central role in the map, having multiple links to and from other categories. Thereafter, judgements were made about which of these categories might usefully inform the core components of a relapse prevention intervention.

Relationships between categories of identified facilitators and barriers to the maintenance of changed lifestyle behaviours. Green boxes represent categories in which 60% or more factors were facilitative. Red represents categories which 60% or more factors were barriers. Orange represents categories with a relatively balanced mix of barriers and facilitators. Unidirectional arrows indicate that factors in one category related to another (e.g. thinking about the future was related to beliefs about the benefits of healthy lifestyles). Bidirectional arrows indicate that factors in both categories made links with each other.
Quality assessment
The quality of the studies was assessed using a 36-item tool [26, 27]. The tool primarily comprised items from the widely used COREQ [26] with additional questions that were considered important from Long & Godfrey [27]. Each item scored 2, 1, or 0 representing the extent to which each criterion was met, with a maximum possible score of 72. We applied arbitrary cut-offs to categorize studies as good (>65%), fair (35%-65%) and poor (<35%), and used this as a descriptive tool rather than exclusion criterion.
Results
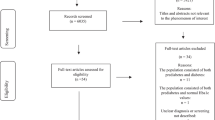
The electronic search strategy identified 15,731 publications and following title and abstract screening, 332 full papers were obtained. Of these, 309 were rejected because they: reported quantitative data only (n=248); were not empirical (n=19) or a peer reviewed paper (n=1), or did not meet other inclusion criteria, including a lack of focus on the target population or not reporting maintenance related themes (n=41). Included in the review were 22 studies, reported in 23 papers [28–50].
Summary of the studies
The studies recruited 723 participants (Table 1). The majority of studies were conducted in the UK (n=10; 45%), with 41% (n=9) in the USA, two in Taiwan and one in Australia. Most participants belonged to the majority ethnic group of their country, and most studies collected data through individual interviews (n=15). The conditions under investigation were Type 2 diabetes (n=7), heart disease (n=6), obesity or COPD (n=3 each) hyperlipidemia (n=2) and hypertension (n=1). More than half of the studies (n=15) focussed on two or more lifestyle behaviours, with physical activity being the most often investigated behaviour (20 studies) and alcohol intake the least (one study) [34]. The shortest period of maintenance was within one month following completion of an intervention [40] with 46 years’ post-diagnosis being the longest [28]. The majority of studies focused on a possible maintenance period of up to two years following a particular event (either diagnosis or onset, treatment or programme participation).
Factors, categories and key themes
A total of 97 factors (1–11 per study) were extracted and organised into 13 categories (Table 2). Six of the categories were those from our previous framework [25], five were modified (to better reflect the range of factors in the current review), and the remaining two emerged from the extracted data (‘future focus’ and ‘monitoring and planning’). Unlike the previous review that reported the majority of factors as barriers to lifestyle behaviour change [8], most of the factors in the current review were deemed to be facilitators (n=64; 66%). The category containing the greatest proportion of barriers was ‘physical wellbeing’. The largest category (containing the most factors) was ‘social support’ followed by ‘psychological (other)’ and ‘beliefs’ (Table 3). Two studies with a particular focus in these areas contributed substantially to these categories [28, 30]. However even without their contribution, these types of factors would remain the most common. No other categories were excessively influenced by any one study.
In relation to the distribution of behaviours across the categories, physical activity dominated ‘social support’ and ‘balancing and integrating healthy behaviours with everyday life’, and was the exclusive behaviour in ’physical wellbeing’ and ‘environment’. All other categories covered a broader range of behaviours.
We identified four potential key themes (Figure 1). Factors in ‘social support’ related to five other categories. In turn two other categories also made links back to ‘social support’. Its position within the relationship map demonstrates that social support may be the main gatekeeper to ‘balancing and integrating healthy behaviours with everyday life’ which in turn links to ‘monitoring and planning’ and ‘environment’. This category was therefore considered a key theme. Examination of the ‘education and knowledge’ category revealed that the five factors within this made reference to two other categories (‘formal support’ and ‘personal choice and cultural preferences’). In turn, factors within ‘formal support’ and four other categories (‘psychological (other)’, ‘emotions’, ‘physical wellbeing’, and ‘cost’ made reference back to ‘education and knowledge’. Thus ‘education and knowledge’ seems to be at the core of many factors and this category was considered a key theme. Finally, ‘beliefs’ also represented a large category and although it might be influenced by good social support, its influence on a number of other categories and the specific nature of some of the factors (relating to poor self-belief) suggest that it may be a key theme. Closely linked with this category is ‘emotions’, which if presented as depression or anxiety may be a significant barrier to maintenance and hence require specific attention. Emotions could therefore be combined with beliefs to act as a key theme.
Quality assessment
Two papers were ‘poor’ in quality [39, 44], 20 were ‘fair’ and one was ‘good’ [38]. The median score was 44 (51%, range 26–60). Studies were most likely to score well on reporting the background to the study and aspects of the study design, including their use of an analytic framework, methods of data collection and description of theme generation (Table 4). They scored least well in providing details about characteristics of the research team, relationships between the researchers and participants, information about the presence of others during data collection and whether themes were validated with participants.
Discussion
To our knowledge, this is the first systematic review of the qualitative literature reporting the main patient perceived factors that influence maintenance of changed healthy behaviours in individuals at high risk of cardiovascular events. Information such as this is important because maintenance rates of changed healthy behaviours in this particular population diminish with time [30, 50] and lifestyle support programmes that do not deal with addictions are unlikely to offer evidence-based relapse prevention interventions [51]. Highlighting the key factors that patients consider important in maintaining their healthy behaviours will be needed to support the development of such interventions.
Comparison with existing literature
Although some individuals change and maintain their healthy behaviours with relative ease and little support, many undergo a series of steps (often termed stages of change [17]), that can be non-linear, involving contemplation, action and maintenance. Maintenance therefore represents the tail end of a continuum of change and so should not be viewed in isolation. Previous reviews examining factors associated with changing lifestyles in this population found that low mood, misplaced beliefs about the causes and value of healthy lifestyles, poor knowledge, limited social support (from friends and family) and difficulties with transport and related costs predicted non-uptake of lifestyle behaviour change and non-completion of related programmes [9]. The current review seems to suggest that for the most part, the areas that influence change of lifestyle behaviours also influence maintenance. Furthermore, as with change, the influencing factors are interlinked. The literature, however, only offers us the factors and as such we cannot explain the nature of the links or how they may differ between individuals or perhaps types of individuals. Insight into this might offer a clearer explanation as to why some maintain and others do not. Based on our current knowledge, we at least have some guidance as to a core framework that would inform the development of approaches for improving uptake and participation of lifestyle behaviour change, as well as maintenance. This would be aided by a more detailed comparison of the factors relating to change and maintenance to ensure that programmes provided relevant support for each stage.
Summary of main findings
We considered at the outset that maintenance of changed lifestyle behaviours, as reported in the cardiovascular literature, would potentially highlight some differences from the addictions literature. As predicted, we have observed that individuals are attempting to maintain multiple changed lifestyles, though the literature failed to describe particular challenges associated with their simultaneousness. Further, physical activity was the most commonly investigated behaviour in this review, while sedentary lifestyles are not addressed in the addictions literature.
Social support was identified as a key theme in the current review. Also a key theme in the active stage of changing lifestyle behaviours [8], its continued importance in the longer-term is unsurprising. This is a challenging area to address where social support is lacking. In order to facilitate maintenance of changed behaviours, good social support will be needed much earlier on to ensure that beliefs about the benefits of healthy lifestyles are more stable and effective planning and problem solving are in place to support continued integration with everyday life. Evidence suggests that whilst changing behaviours with a friend is more likely to be successful [52–54], this is not sustained where obesity and overweight are the norm in the broader social network [55, 56]. A more creative approach to tackling obesity through a predominantly social model may therefore be required.
The ‘beliefs’ core theme comprised mostly barriers and to some extent this was unexpected. Given that the included studies comprised individuals who had attempted to make changes to their lifestyle (presumably because of their conditions), it was assumed that beliefs about the value of a healthy approach to life would be relatively stable. However there was evidence that individuals were still questioning the benefits of healthy lifestyles and we can only speculate about the reasons why. Changes to lifestyle may have been triggered by an event or diagnosis. However, if clinical outcomes (e.g. blood pressure, cholesterol, HbAC1 levels) do not respond as anticipated, or perceptions of risk alter through time (due to, for example, absence of subsequent events), beliefs may be challenged. Clearer information about the impact of changing behaviours on cardiovascular risk would be beneficial, particularly given that patients tend to underestimate their personal risk [57]. Currently Framingham and QRISK, algorithms for calculating cardiovascular risk [58, 59] are used routinely in primary care, and their associated software enables visual adjustment of risk scores according to behaviour for one variable, smoking. This is not currently available for diet, physical activity and alcohol, although should be possible with good epidemiological data such as that reported for multiple lifestyle factors in the prevention of cerebrovascular events [60]. Development of a decision aid for lifestyle behaviours, such as that used for statin prescribing in the UK [61] would be of value. However, training in their use would be required, as health care professionals tend to avoid discussions of risk that incorporate visual and numerical framing [57, 62].
Some of the factors were reported as strategies (facilitative thoughts and actions) that individuals applied whilst trying to maintain healthy diets and physical activity. These included planning meals, getting into a routine and self-monitoring, all of which are typical of the cognitive behavioural and problem solving approaches that form the basis for relapse prevention programmes [10, 11]. Evidence suggests that use of such strategies are common amongst successful abstainers of weight loss and smoking [17, 63]. In our review, only one facilitative factor (formation of a new identity) [44] was specifically related to maintenance of smoking cessation, but in the absence of further detail it cannot be considered a strategy. Five studies [32, 40, 43, 49, 50, 64] explicitly stated that participants had previously been in a formal lifestyle programme. There is no suggestion from these that individuals were given any relapse prevention training and indeed from these studies there were numerous examples of barriers. The facilitative strategies observed across the studies may therefore have been acquired by chance rather than through any formal support mechanism.
Strengths and limitations
The studies included in the current review were individually small, as is typical for qualitative research however collectively they form a substantial evidence base.
None of the included studies defined what they meant by maintenance and therefore we had to make subjective judgements about factors that appeared to be relevant. To some extent we reduced the risk of reporting factors about ‘changing’ behaviours by excluding studies in which the participants were actively involved in or had just recently completed a formal lifestyle programme. Nonetheless, extra diligence was required during data extraction to ensure that inadequately described retrospective data on the change process in included studies was omitted. Factors that were particularly challenging included those that appeared to be about preparation for maintenance (having the right knowledge to continue by oneself with the healthy lifestyle behaviour, and making the ‘right personal choice’ of venue for exercising). These have been reported in this review.
As with factors, decisions on key themes were somewhat subjective. The process did however involve two reviewers and take into account the number of links to and from categories. The only category that lacked clarity as to whether or not it represented a key theme was ‘psychological (other)’. Our interpretation is only a guide and we suggest that the development of any associated intervention for relapse prevention also considers individual attitudes, motivations and confidence.
All but two studies appeared to report inductively generated results that were independent of their stated aims [28, 30]. These studies contributed substantially to three categories: ‘social support’, ‘psychological (other)’ and ‘beliefs’, although in their absence these categories would have remained large. From this perspective any bias appears to have been limited. We cannot however, rule out the possibility that the authors themselves may have held particular philosophical viewpoints that may have biased the collection or analysis of the original data.
Apart from maintained weight loss, the studies did not indicate that any objective measures had been used to demonstrate continued abstinence of unhealthy behaviours. We were therefore reliant on the truthfulness of the participants within the studies. Many of the studies examined factors relating to maintenance of a healthy diet (for their condition rather than for weight loss) and physical activity. As none of the studies indicated whether these activities met with existing recommendations, we might assume that some individuals, although possibly unaware, were not fully compliant. This being the case, perceptions about the ease with which healthy behaviours are maintained may bias the findings towards facilitators. This might explain why we observed more facilitators than barriers in the studies.
Conclusions
Social support, education and knowledge, and beliefs and emotions are key areas that lifestyle support services need to focus on within the context of facilitating lifestyle behaviour change and maintenance. While further confirmation about their role in predicting maintenance of changed behaviours is required, it remains likely that these key areas are those that collectively appear to provide the framework that binds changed behaviours to everyday living. In delivering this type of support there needs to be better integration between health and social care. In the UK there is a large strategic shift towards better preventive services through the creation of Public Health England, the core of which comprises health and social care professionals working within Integrated Health and Wellbeing Boards [65] to commission local services according to needs. The bringing together of these very different philosophical stances will bring challenges but also opportunities to more effectively tackle the unhealthy consequences of societal problems.
Authors’ information
Jenni Murray, BSc, MSc, Phd, Senior Research Fellow
Grania Fenton, BA, PGCert, DClinPsychol, Research Fellow
Stephanie Honey, BSc, MSc, Phd, Research Fellow
Ana Claudia Bara, BSc, BA, PhD, Research Fellow
Kate Hill, BSc, MSc, Phd, Senior Research Fellow
Allan House BSc. MBBS, MRCP, MRCPsych DM, Professor of Liaison Psychiatry.
References
Blair S: Physical inactivity: the biggest public health problem of the 21st century. Br J Sports Med. 2009, 43: 1-2.
Gillies C, Abrams K, Lambert P, Cooper N, Suton A, Hsu R, et al: Pharmacological and lifestyle interventions to prevent or delay type 2 diabetes in people with impaired glucose tolerance: systematic review and meta-analysis. Br Med J. 2007, 334 (7588): 299-10.1136/bmj.39063.689375.55.
British Heart Foundation: The National Audit of Cardiac Rehabilitation. Annual Report. 2012, London: British Heart Foundation
Tsai A, Wadden T: Systematic review: An evaluation of major commercial weight loss programs in the United States. Ann Intern Med. 2005, 142: 56-66. 10.7326/0003-4819-142-1-200501040-00012.
Hughes J, Keely J, Naud S: Shape of the relapse curve and long-term abstinence among untreated smokers. Addiction. 2004, 99: 29-38. 10.1111/j.1360-0443.2004.00540.x.
Ferguson J, Bauld L, Chesterman J, Judge K: The English smoking treatment services: one year outcomes. Addiction. 2005, 100 (Suppl 2): 59-69.
Curioni CC, Lourenco PM: Long-term weight loss after diet and exercise: a systematic review. Int J Obes. 2005, 29: 1168-1174. 10.1038/sj.ijo.0803015.
Murray J, Hill K, Honey S, Craigs C, House A: Qualitative synthesis: factors affecting lifestyle change to reduce cardiovascular risk. Br J Gen Pract. 2012, 61: 296-297. 10.3399/bjgp12X649089. (abridged text, in print at
Murray J, Craigs C, Hill K, Honey S, House A: A systematic review of patient reported factors associated with uptake and completion of cardiovascular lifestyle behaviour change. BMC Cardiovasc Disord. 2012, 12: 120-10.1186/1471-2261-12-12.
Marlett GA, Gordon JR: Relapse prevention: Maintenance strategies in the treatment of addictive behaviours. 1985, New York: Guildford Press
Perri M, Nezu A, Viegener B: Improving the long-term management of obesity: Theory, research and clinical guidelines. 1992, New York: Wiley
Coleman T, Agboola S, Leonardi-Bee J, Taylor M, McEwen A, McNeill A: Relapse prevention in UK Stop Smoking Services: current practice, systematic reviews of effectiveness and cost-effectiveness analysis. Health Technol Assess. 2010, 14: 49-
Department of Health: Putting prevention first. Vascular checks: risk assessment and management. 2008, London: Department of Health
Lim LS, Haq N, Mahmood S, Hoeksema L: Atherosclerotic cardiovascular disease screening in adults: American College of Preventive Medicine position statement on preventive practice. American Journal Preventative Medicine. 2011, 40 (381): e1-e10.
NVDPA: Australian Guidelines for the management of absolute cardiovascular disease (CVD) risk. 2012, Canberra: National Vascular Disease Prevention Alliance
Brotons C, Bulc M, Sammut MR, Sheehan M, Manuel da Silva Martins C, Björkelund C, et al: Attitudes toward preventive services and lifestyle: the views of primary care patients in Europe. The EURO PREVIEW patient study. Fam Pract. 2012, 29 (suppl 1): i168-i176. 10.1093/fampra/cmr102.
Prochaska J, Di Clemente C: Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983, 51 (3): 390-395.
Hall RF, Joseph DH, Schwartz-Barcott D: Behavioral maintenance: a closer look. Nurs Forum. 2002, 37 (1): 5-11. 10.1111/j.1744-6198.2002.tb01185.x.
Attebring MF, Hartford M, Hjalmarson A, Caidahl K, Karlsson T, Herlitz J: Smoking habits and predictors of continued smoking in patients with acute coronary syndromes. J Adv Nurs. 2004, 46 (6): 614-623. 10.1111/j.1365-2648.2004.03052.x.
Barte JCM, ter-Bogt NCW, Bogers RP, Teixeira PJ, Blissmer B, Mori TA, et al: Maintenance of weight loss after lifestyle interventions for overweight and obesity, a systematic review. Obes Rev. 2010, 11 (12): 899-906. 10.1111/j.1467-789X.2010.00740.x.
Reid RD, Tulloch H, Kocourek J, Morrin LI, Beaton LJ, Papadakis S, et al: Who will be active? Predicting exercise stage transitions after hospitalization for coronary artery disease. Can J Physiol Pharmacol. 2007, 85 (1): 17-23. 10.1139/Y07-002.
Nelson KM, McFarland L, Reiber G: Factors influencing disease self-management among veterans with diabetes and poor glycemic control. J Gen Intern Med. 2007, 22 (4): 442-447. 10.1007/s11606-006-0053-8.
CRD: Systematic Reviews: CRD’s guidance for undertaking reviews in health care. 2008, York: Centre for Reviews and Dissemination, University of York
Thomas J, Harden A: Methods for thematic analysis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008, 8: 45-10.1186/1471-2288-8-45.
Murray J, Hill K, Honey S, Craigs C, House A: Qualitative synthesis: factors affecting lifestyle change to reduce cardiovascular risk (abridged text). Br J Gen Pract. 2012, 61: 296-297.
Tong A, Sainsbury P, Craig J: Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007, 19 (6): 349-357. 10.1093/intqhc/mzm042.
Long AF, Godfrey M: An evaluation tool to assess the quality of qualitative research studies. Int J Social Research Methodology. 2004, 7 (2): 181-196. 10.1080/1364557032000045302.
Beverly EA, Wray LA: The role of collective efficacy in exercise adherence: a qualitative study of spousal support and type 2 diabetes management. Health Educ Res. 2010, 25 (2): 211-223. 10.1093/her/cyn032.
Bidgood J, Buckroyd J: An exploration of obese adults’ experience of attempting to lose weight and to maintain a reduced weight. Couns Psychother Res. 2005, 5 (3): 221-229. 10.1080/17441690500310395.
Byrne S, Cooper Z, Fairburn C: Weight maintenance and relapse in obesity: a qualitative study. Int J Obes Relat Metab Disord. 2003, 27 (8): 955-962. 10.1038/sj.ijo.0802305.
Chen K, Chen M, Lee S, Cho H, Weng L: Self-management behaviours for patients with chronic obstructive pulmonary disease: a qualitative study. J Adv Nurs. 2008, 64 (6): 595-604. 10.1111/j.1365-2648.2008.04821.x.
Coghill N, Cooper AR: Motivators and de-motivators for adherence to a program of sustained walking. Prev Med. 2009, 49 (1): 24-27. 10.1016/j.ypmed.2009.04.017.
Dailey R, Schwartz KL, Binienda J, Moorman J, Neale AV: Challenges in making therapeutic lifestyle changes among hypercholesterolemic African-American patients and their physicians. J Natl Med Assoc. 2006, 98 (12): 1895-1903.
Darr A, Astin F, Atkin K: Causal attributions, lifestyle change, and coronary heart disease: illness beliefs of patients of South Asian and European origin living in the United Kingdom. Heart Lung. 2008, 37 (2): 91-104. 10.1016/j.hrtlng.2007.03.004.
Davis EM, Clark JM, Carrese JA, Gary TL, Cooper LA: Racial and socioeconomic differences in the weight-loss experiences of obese women. Am J Public Health. 2005, 95 (9): 1539-1543. 10.2105/AJPH.2004.047050.
Gazmararian JA, Ziemer DC, Barnes C: Perception of barriers to self-care management among diabetic patients. Diabetes Educ. 2009, 35 (5): 778-788. 10.1177/0145721709338527.
Gregory S, Bostock Y, Backett-Milburn K: Recovering from a heart attack: a qualitative study into lay experiences and the struggle to make lifestyle changes. Fam Pract. 2005, 23 (2): 220-225. 10.1093/fampra/cmi089.
Gulanick M, Bliley A, Perino B, Keough V: Recovery patterns and lifestyle changes after coronary angioplasty: the patient’s perspective. Heart Lung. 1998, 27 (4): 253-262. 10.1016/S0147-9563(98)90037-1.
Lee L-L, Avis M, Arthur A: The role of self-efficacy in older people’s decisions to initiate and maintain regular walking as exercise - findings from a qualitative study. Prev Med. 2007, 45 (1): 62-65. 10.1016/j.ypmed.2007.04.011.
Lewis R, Cramp F: Facilitators and barriers to exercise maintenance in chronic obstructive pulmonary disease: patient views. Physiotherapy Ireland. 2010, 31 (2): 19-24.
Malpass A, Andrews R, Turner KM: Patient Perception, Preference and Participation: patients with Type 2 Diabetes experiences of making multiple lifestyle changes: a qualitative study. Patient Education and Counselling. 2009, 74 (2): 258-263. 10.1016/j.pec.2008.08.018.
Nagelkerk J, Reick K, Meengs L: Perceived barriers and effective strategies to diabetes self-management. J Adv Nurs. 2006, 54 (2): 151-158. 10.1111/j.1365-2648.2006.03799.x.
O’Shea SD, Taylor NF, Paratz JD: But watch out for the weather: factors affecting adherence to progressive resistance exercise for persons with COPD. J Mol Signal. 2007, 27 (3): 166-174.
Parry O, Fowkes F, Thomson C: Accounts of quitting among older ex-smokers with smoking-related disease. J Health Psychol. 2001, 6 (5): 481-493. 10.1177/135910530100600502.
Peel E, Douglas M, Parry O, Lawton J: Type 2 diabetes and dog walking: patients’ longitudinal perspectives about implementing and sustaining physical activity. Br J Gen Pract. 2010, 60 (577): 570-577. 10.3399/bjgp10X515061.
Peterson JC, Allegrante JP, Pirraglia PA, Robbins L, Lane KP, Boschert KA, et al: Living with heart disease after angioplasty: a qualitative study of patients who have been successful or unsuccessful in multiple behavior change. Heart Lung. 2010, 39 (2): 105-115. 10.1016/j.hrtlng.2009.06.017.
Rahim-Williams B: Beliefs, behaviors, and modifications of type 2 diabetes self-management among African American women. J Natl Med Assoc. 2011, 103 (3): 203-215.
Sullivan ED, Joseph DH: Struggling with behavior changes: a special case for clients with diabetes. Diabetes Educ. 1998, 24 (1): 72-77. 10.1177/014572179802400110.
White S, Bissell P, Anderson C: Patients’ perspectives on cardiac rehabilitation, lifestyle change and taking medicines: implications for service development. J Health Serv Res Policy. 2010, 15 (Suppl 2): 47-53. 10.1258/jhsrp.2009.009103.
White S, Bissell P, Anderson C: A qualitative study of cardiac rehabilitation patients’ perspectives on making dietary changes. J Hum Nutr Diet. 2011, 24 (2): 122-127. 10.1111/j.1365-277X.2010.01136.x.
Jolly K, Lewis A, Beach J, Denley J, Adab P, Deeks J, et al: Comparison of range of commercial or primary care led weight reduction programmes with minimal intervention control for weight loss in obesity: lighten-up randomised controlled trial. BMJ. 2011, 343: d6500-10.1136/bmj.d6500.
Malchodi CS, Oncken C, Dornelas EA, Caramanica L, Gregonis E, Curry SL: The effects of peer counselling on smoking cessation and reduction. Obstet Gynecol. 2003, 101: 504-510. 10.1016/S0029-7844(02)03070-3.
Hughes J, Todorovic V, Kemp H: ‘The Sugar Buddies’: An intervention programme for ‘obese’ patients with poorly controlled diabetes. J Hum Nutr Diet. 1999, 12 (SUPPL. 1): 71-78.
Wing RR, Jeffery R: Benefits of recruiting participants with friends and increasing social support for weight loss and maintenance. J Consult Clin Psychol. 1999, 1999 (67): 132-138.
Christakis NA, Fowler JF: The spread of obesity epidemic in a large social network over 32 years. N Engl J Med. 2007, 357: 370-379. 10.1056/NEJMsa066082.
Bahr DB, Browning RC, Wyatt HR, Hill JO: Exploiting social networks to mitigate the obesity epidemic. Obesity. 2009, 17 (4): 723-728. 10.1038/oby.2008.615.
Niknian M, McKinlay SM, Rakowski W, Carleton R: A comparison of perceived and objective CVD risk in a general population. Am J Public Health. 1989, 79 (12): 1653-1654. 10.2105/AJPH.79.12.1653.
Hippisley-Cox J, Coupland C, Vinogradova Y, Robson J, Minhas R, Sheikh A, et al: Predicting cardiovascular risk in England and Wales: prospective derivation and validation of QRISK2. Br Med J. 2008, 336: a332-10.1136/bmj.39609.449676.25.
D’Agostino RB, Vasan RS, Pencina M, Wolf P, Cobain M, Massaro J, et al: General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation. 2008, 117: 743-753. 10.1161/CIRCULATIONAHA.107.699579.
Zhang Y, Tuomilehto J, Jousilahti P, Wang Y, Hu G, Antikainen R: Lifestyle factors on the risks of ischemic and hemorrhagic stroke. Archives of Internal Medicine. 2011, 171 (20): 1811-1818. 10.1001/archinternmed.2011.443.
National Prescribing Centre: Statins patient decision aid. 2009, NHS, National Prescribing Centre, http://www.npc.nhs.uk/patient_decision_aids/pda.php,
Webster R, Heeley E: Perceptions of risk, understanding cardiovascular disease. Risk Management and Healthcare Policy. 2010, 3: 49-60.
Head S, Brookhart A: Lifestyle modification and relapse-prevention training during treatment for weight loss. Behav Ther. 1997, 28 (2): 307-321. 10.1016/S0005-7894(97)80049-4.
Lee L-L, Avis M, Arthur A: The role of self-efficacy in older people’s decisions to initiate and maintain regular walking as exercise – Findings from a qualitative study. Prev Med. 2007, 45 (1): 62-65. 10.1016/j.ypmed.2007.04.011.
Department of Health: Public Health England’s Operating Model. 2011, London: Department of Health
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2261/13/48/prepub
Acknowledgements
This work was supported by the National Institute of Health Research (KRD/012/001/006).
The National Institute for Health Research Collaborations for Leadership in Applied Health Research and Care (NIHR CLAHRC) for LYB (Leeds, York and Bradford) – a collaboration between two Universities, the NHS and Social Services. We acknowledge funding from the National Institute for Health Research Collaborations for Leadership in Applied Health Research and Care. The views and opinions expressed in this paper are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
The Leeds York Bradford Collaboration for Applied Health Research and Care (CLAHRC) vascular theme collaborators: Professors Bob Lewin, Simon Gilbody, Ian Watt at the University of York, and Lucy Jackson at NHS Leeds.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
JM wrote the study protocol and led the review process and writing of the manuscript. GF was involved in all stages of conducting the review, including screening, data extraction and the writing of the manuscript. SH was involved in screening and data extraction and reviewed the manuscript. ACB was involved in screening and reviewed the manuscript. KH reviewed the study protocol and the manuscript. AH conceived the idea for the review and reviewed the study protocol and the manuscript. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Murray, J., Fenton, G., Honey, S. et al. A qualitative synthesis of factors influencing maintenance of lifestyle behaviour change in individuals with high cardiovascular risk. BMC Cardiovasc Disord 13, 48 (2013). https://doi.org/10.1186/1471-2261-13-48
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2261-13-48