
Abstract
Purpose
Clinical immersion experiences provide engineering students with opportunities to identify unmet user needs and to interact with clinical professionals. These experiences have become common features of undergraduate biomedical engineering curricula, with many published examples in the literature. There are, however, few or no published studies that describe rigorous qualitative analysis of biomedical engineering student reflections from immersion programs.
Methods
Fifteen reflection prompts that align with program learning goals were developed and structured based on the DEAL model for critical reflection. Undergraduate participants in a summer immersion program responded to these prompts throughout five weeks of clinical rotations. Data from two summer cohorts of participants (n = 20) were collected, and thematic analysis was performed to characterize student responses.
Results
Students reported learning about key healthcare topics, such as medical insurance, access to healthcare (and lack thereof), stakeholder perspectives, and key medical terminology and knowledge. Most reflections also noted that students could apply newly gained medical knowledge to biomedical engineering design. Further, clinical immersion provided students with a realistic view of the biomedical engineering profession and potential areas for future professional growth, with many reflections identifying the ability to communicate with a variety of professionals as key to student training. Some students reflected on conversations with patients, noting that these interactions reinvigorated their passion for the biomedical engineering field. Finally, 63% of student reflections identified instances in which patients of low socioeconomic status were disadvantaged in health care settings.
Conclusions
Clinical immersion programs can help close the gap between academic learning and the practical experience demands of the field, as design skills and product development experience are becoming increasingly necessary for biomedical engineers. Our work initiates efforts toward more rigorous analysis of students’ reactions and experiences, particularly around socioeconomic and demographic factors, which may provide guidance for continuous improvement and development of clinical experiences for biomedical engineers.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Biomedical engineers aim to improve human health and optimize healthcare processes by designing and creating equipment, devices, systems, therapeutics, and algorithms for health care applications [1]. Engineers entering the medical device industry can lack practical design skills and product development experience, as these important skills are traditionally learned and developed through on-the-job training [2]. A key aspect of such design training is preparing engineers to be cognizant of user need considerations. To this end, engaging biomedical engineering students in clinical immersion programs may enhance their preparedness for future responsibilities [3] and their ability to identify needs in clinical settings [4]. Along with enhanced design skills, immersion in clinical environments may bring awareness of the socioeconomic diversity and disparities that exist in health care, which students may otherwise miss in a traditional classroom setting. Clinical immersion programs provide students with opportunities to develop awareness through direct exposure to the clinical environment [5]. Students can then have the opportunity to observe the current state of the health care system, identify unmet needs, and design efficient and effective engineering solutions that prioritize user needs [5].
Currently, there are 153 accredited biomedical engineering undergraduate programs within the United States [6]. These programs often aim to develop technical engineering skills by providing experiential learning opportunities, such as capstone projects and clinical immersions [7]. Witnessing firsthand how doctors interact with medical devices may develop student observational skills and enhance their ability to design more precisely and safely [8]. For example, the Food and Drug Administration’s (FDA) “Do It By Design,” guide recognizes a deficit in “human factor” consideration when design planning [9]. In it, the FDA points to the significance of distinguishing client needs and shares how doctors and stakeholders can comment on medical device designs so that students can focus on user needs and can improve their designs [9]. Moreover, several universities now offer clinical immersion programs for biomedical engineering students to help develop solutions based on user-focused design [2, 4, 5]. Among these programs, a common method is the needs-based approach [10]; however, individual program content and structure vary. Regardless of their scope and length, these programs are tailored to take advantage of organizational strengths. Some encourage interdisciplinary teams among engineering disciplines, business students, nursing students, and medical students [11, 12]. The duration of the programs can range from multiple hour-long sessions to semester and year-long experiences, but a five- to ten-week summer internship is commonly practiced among universities. In addition, programs address scalability issues by having clinicians teach classes to describe the clinical experience firsthand or using a team leader model in which a student with a primary experience conveys information to the rest of the team [8, 13]. Even though more programs are offering required or auxiliary clinical immersion experiences, to date, we have found no published studies of clinical immersion programs that include rigorous qualitative analysis of biomedical engineering student reflections. If students can critically reflect on their experiences after clinical immersion, it could help them to develop professional skills in an ongoing way [14]. Critical reflection provides students the opportunity to think of new questions and apply higher order of thinking to reach metacognition [14]. This skill is important because later students can confront bias, contrast theory, and practice, and identify systemic issues, all of which tend to lead to effective evaluations and knowledge transfer [14] and can help develop practical design skills by focusing on user needs.
Biomedical engineering educators who organize student immersion experiences can learn from clinical education programs for health professionals, particularly those that promote self-awareness through critical reflection [14]. Reflection itself is considered to be a crucial component of experiential learning, where experiences are analyzed, theories are reviewed, and further action is planned [15]. Different definitions of critical reflection share a common characteristic, which is that they seek to understand how people arrive at judgments and decisions about complex issues [16]. Social workers, physicians, occupational therapists, dentists, nurses, and physiotherapists have given this form of reflection considerable attention [14, 17], recognizing that the assumptions that underpin our beliefs and actions are primary components of critical thinking [15]. Studies report how reflection can be developed and incorporated into the curriculum, such as reflection on student performance in medical practice [18] and development of reflective skills in medical students [19]. Additional studies discuss how to measure the impact of critical reflection through reflective learning activity assessments [20, 21]. In nursing education, as an example, critical thinking has been characterized as a means of trying to link theory and practice so that nursing practice can be examined through a systematic process of exploration and reasoning [22]. This exploration and reasoning can help students to integrate theory with practical skills. In fact, one postgraduate nursing program aimed to develop deconstructive skills for critical reflection where students were facilitated in deconstructing concepts and knowledge that they applied to their own practice [22]. Reflection has also been promoted as a technique for assisting medical professionals with the inherent complexities of medical training and delivery [23]. To enhance medical knowledge and improve patient-history-taking skills, medical students are increasingly expected to demonstrate their aptitude for reflective essays, critical event reports, and portfolios [24, 25]. Unlike reflection which focuses on immediate details presented, critical reflection explores and examines the context within which a task or problem is situated [26]. Another study shared the influence of critical thinking and self-regulated learning on 193 medical students by stating that it is critical to provide medical students with ample examples and links to professional practice to escalate their perception of relevance and to improve system usability permanently [27]. Like these medical students, biomedical engineering students can also link to the professional experience by applying critical reflection after the clinical immersion experience.
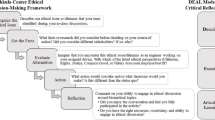
To maximize learning, biomedical engineering educators can move beyond post-experiential reflection assignments to designing learning experiences with critical reflection throughout [28,29,30]. Ash and Clayton’s DEAL (Describe, Examine, Articulate Learning) model of critical reflection has been used as a conceptual framework by numerous programs where students can examine, assess, and review their critical thinking across different curricula for enhancing critical thinking and problem-solving skills [31,32,33,34]. Our work incorporates the DEAL model [30] which structures student reflections into three sequential steps. First, students Describe their experiences; second, they Examine those experiences in the light of specific learning objectives; and finally, they Articulate the Learning in their reflections gained through observation, knowledge, and reasoning [35,36,37]. The structured nature of the DEAL model encourages students to assess and improve their own learning [37]. Although it was originally developed for use in service-learning courses [30], DEAL has since been integrated into a range of traditional and experiential pedagogies, as well as curricular and co-curricular professional training opportunities [30]. In one approach, immersing students in a fully integrated research and outreach experiential learning experience aimed to bridge the perceived research-practice barrier [31]. With both Kolb’s Experiential Learning Model (1984) and the DEAL Model for Critical Reflection (Ash & Clayton, 2009) as conceptual frameworks, the program revealed student gains as a rise in the production of scholarship, an increase in discipline-specific knowledge, and enhanced critical thinking and problem-solving skills [31]. Another program provided students the opportunity to be involved in multiple high-impact practices simultaneously and required a series of weekly journal prompts based on the DEAL model to help enhance academic performance, civic learning, and personal growth [32]. Taking part in reflections on personal growth enabled students to clarify their career goals [32]. Another study compared routine reflection with DEAL model reflection and found that students partaking in DEAL model reflection had positive educational gains when compared with students who underwent routine reflection [34].
In this paper, we report on our qualitative analysis of student reflections from a seven-week summer clinical immersion program. Our work aims to address the current lack of rigorous qualitative analyses of biomedical engineering student reflections during clinical immersion experiences. Specifically, our immersion program aims to utilize student reflection to strengthen student learning of the biomedical engineering design process and socioeconomic disparities in healthcare. The two research questions guiding our work include: (1) How do biomedical engineering undergraduates engaged in clinical immersion describe their experiences and learning? and (2) What connections do students make between clinical immersion experiences and the socioeconomics of healthcare and their own future engineering design?
Student participants in our summer program responded weekly to critical reflection prompts that were structured based on the DEAL model. Further, the students reflected on health care socioeconomics, helping them identify and explore existing problems within the clinic while challenging themselves to think critically of potential solutions. We used thematic analysis in our paper as a tool to identify source themes to analyze student reflections.
Theoretical Framework
Thematic analysis is a qualitative data analysis technique that identifies, explains, and interprets patterns of meaning (“themes”). This technique highlights which themes are important and it offers a foundation for qualitative data analysis skills. Thematic analysis can identify patterns within and across data-based lived experiences [38]. Specifically, this type of research seeks to understand what participants think, feel, and do [38] and introduces the mechanics of coding and analyzing qualitative data systematically, which can then be linked to broader theoretical and conceptual problems [39]. Using this method, we identify what is common to how a subject is discussed or written and make sense of it. It offers accessibility and flexibility by providing insights into a way of doing research that might otherwise seem vague or difficult [39]. Thematic analysis fits into our research to analyze students’ critical reflections for identifying source themes for its flexibility and systematic way of analyzing qualitative data.
Reflection is simply a process of turning back on the experience, such as a simple observation of an object, event, or state, as well as a manner of perceiving, thinking, and feeling [40]. The distinction between reflection and critical reflection is that reflection does not necessarily imply assessing the object of reflection [40]. Critical reflection involves recognizing, questioning, and evaluating our deep-held assumptions about our knowledge, perceptions, beliefs, feelings, and actions. As a key component of professional development and adult education literature (for example, Brookfield 1997; Mezirow 1981) [41, 42], critical reflection is used as an approach to encourage individuals to examine their own work critically and to position themselves relative to the ideas and practices they encounter [43]. The DEAL model for critical reflection is an example of an approach that facilitates learning outcomes through its three steps of critical reflection [30]. The DEAL model consists of Describing experiences objectively and in a detailed manner; Examining those experiences while taking into consideration of goals and objectives for learning; Articulating Learning which includes following-up goals for further practice and refinement of learning in the next experience [40]. Whatever mode of delivery is used—written or oral, individual or collaborative, light, or intensive—the DEAL model allows students to use writing or speaking as a tool for learning rather than as a means to express learning after it has already occurred [35].
The DEAL model facilitates scholarly work on teaching and learning in applied learning pedagogy, helping instructors improve the latter through improving the former [40]. In addition to facilitating in-depth critical reflection, DEAL provides prompts derived directly from hierarchical learning objectives that promote higher-order reasoning and critical thinking [40]. In our work, students have critically reflected on their responses to reflection questions by analyzing and evaluating their responses to reflection questions after participating in clinical immersion experience. During this process, they assess their immersion experiences, think critically, and challenge their thinking, and DEAL model is used in our reflection questions to guide their reflection.
Methodology
(IN)SCRIBE Program
The INdiana Summer Clinical Residency in Innovation for Biomedical Engineers or (IN)SCRIBE Program is a paid clinical immersion and team-based design internship for biomedical engineering students at a mid-sized, midwestern university in the US [44]. Our proximity to hospitals serving diverse populations offers students an opportunity for a community-engaged experience that integrates engineering skills with cultural and social competencies. The duration of the (IN)SCRIBE Program is seven weeks, and it is open to rising second, third, and fourth-year biomedical engineering undergraduate students. Once accepted, student participants identify unmet health care needs to confront the challenges of Indiana's health care system through clinical immersion and team-based design. A summary of key program activities is depicted in Fig. 1.

The (IN)SCRIBE Program includes innovation training, clinical rotations, and a culminating team-based design experience
The (IN)SCRIBE Program aims to prepare participants [(IN)SCRIBE Scholars] to (1) document experiences from full-time clinical summer rotations with a variety of medical collaborators in different clinical settings; (2) apply the biomedical engineering design process of working with medical professionals and design faculty mentors to identify and refine a current clinical need; and (3) discuss and reflect on socioeconomic strata, providing multiple perspectives on healthcare delivery.
The (IN)SCRIBE Program is organized into components that include innovation training, weeklong clinical rotations, and a culminating design experience. Before the program, students complete the necessary training and pre-work to prepare for clinical immersion. The first week of the program entails didactic instruction, team-based activities, individual activities, and group outings, all with an emphasis on clinical observation protocols, intellectual property, business model planning for medical innovation, the cost of healthcare, and city demographics. The next weeks of the program provide over 150 h of clinical immersion in varied hospitals within our city. During this time, students are challenged to identify health and medical needs, particularly those connected to social and/or economic disparities observed during their rotations. Students (in pairs) experience a total of five one-week clinical rotations. Each week, student pairings change. Finally, the last week of the program provides extended clinical immersion while student teams develop and pitch a prototype to one specific identified need providing (IN)SCRIBE Scholars opportunity to meet Program Learning Outcome (2).
Participants
Participants of the program, or (IN)SCRIBE Scholars, include biomedical engineering undergraduate students at a mid-sized, midwestern public university and are selected through an application process. This work includes data from a total of twenty participants, summarized in Table 1.
Reflection Journal
(IN)SCRIBE Scholars submitted weekly critical reflections in response to the fifteen provided reflection questions (Table 2) via a Google Doc, to which they had access throughout the program. This reflection journal aided (IN)SCRIBE Scholars in documenting their experiences from clinical summer rotations, helping them meet the first Program Learning Outcome. Scholars responded weekly to critical reflection prompts during five one-week clinical rotations. Summer 2022 (IN)SCRIBE Scholars also reflected on an additional day of clinical rotation at a community outreach clinic. During clinical rotation weeks, Scholars met virtually in groups of four with the teaching assistant on Tuesdays and with the program directors on Thursdays. These virtual meetings provided students an opportunity to openly reflect and share on the week’s rotation. They also provided the program leads an opportunity to learn of any concerns or helpful advice for students in queue for future clinical rotations. After all clinical rotations, the first day back in the classroom with all Scholars (Fig. 1, week 7) included guided group reflection and sharing of the experiences from all clinical rotations.
A total of fifteen reflection questions were developed in alignment with Program Learning Outcome (3). The questions were structured based on the DEAL model, with five questions mapped to each DEAL model phase. First, Scholars Described experiential learning-related experiences and described the big picture. Second, Scholars Examined experiences from the perspective of a biomedical engineer. Last, Scholars Articulated their Learning from the clinical immersion experience based on the first two prompts. The reflection questions given to (IN)SCRIBE Scholars are shown in Table 2. Clinical mentors were not aware of the specific questions given to Scholars to complete as they rotated through different disciplines; however, the (IN)SCRIBE program goal and objectives are shared directly with all medical professionals that help organize clinical rotations for our students.
Data Analysis
Data were downloaded from student reflection journals (via Google Docs) and then were organized and analyzed in Microsoft Excel. Each week, a pair of (IN)SCRIBE Scholars rotated through a different clinical site. In 2022, Scholars also visited a community outreach clinic as an additional one-day experience. Then, they were asked to critically reflect on all experiences. The source themes for analyzing the data were identified by inductive coding. Initial source themes for each reflection question were derived from the raw data provided by (IN)SCRIBE Scholar critical reflection responses using thematic analysis as a tool. The integration and the development of the source themes were structured according to the critical reflection responses. First, author 1 read and summarized the meaningful part of the critical reflection responses of the (IN)SCRIBE Scholars and identified source themes for each reflection question and then discussed it with author 2 and author 3, and then all came to a mutual agreement together for the source themes of each reflection question. Then, author 1 completed coding the critical reflection responses of (IN)SCRIBE Scholars using the source themes for each reflection question and after that ensured mutual agreement with author 2 and author 3. Careful analysis of the source themes reflected how students looked through general experience, socioeconomic and demographic factors, learning, and engineering design during their clinical immersion experience, and we categorized our source themes based on those four categories of the framework.
The fifteen questions that comprised student reflection each week (Table 2) were categorized into four topics for analysis (Fig. 2) based on common themes linking the questions and responses. These four topics include general experience, learning in the clinic, analysis of socioeconomic and demographic factors, and connection to biomedical engineering design.

The four topics of critical reflection questions provided to students before, during, and after their clinical immersion experiences. Specific reflection questions are noted with their abbreviations from Table 2.
Using this framework of four topics of critical reflection, we analyzed data from the summer of 2021 and the summer of 2022. In both summers, each (IN)SCRIBE Scholar experienced clinical immersion for five weeks with each rotation lasting one week. In the summer of 2022, there was an additional one-day clinical rotation at a community outreach clinic run by medical residents. Again, Scholars were asked to critically reflect on the community outreach clinic in addition to their five clinic rotations. One Scholar in 2022 did not complete answers for all the questions, and their critical reflection responses were excluded from the inductive coding. Another Scholar did not complete critical reflection on reflection questions for three rounds of clinical rotations, so no data were included for those three rounds for that Scholar. Ninety-two percent of possible student reflections (1545 completed student responses of 1680 possible) were analyzed. The results are presented as a percentage for each identified source theme. Here, the percentage is calculated for each question and for each identified source theme as the number of Scholars’ responses coded for the theme divided by the total number of responses to the reflection question (n = 103).
All program and student data collection were performed according to methods approved by the Indiana University Institutional Review Board under Protocol #2012065291.
Results
Results from the thematic analysis of student critical reflections are organized into the four topics of questions described in Fig. 2: general experience, learning in the clinic, analysis of socioeconomic and demographic factors, and connection to biomedical engineering design. The student reflections from their general experience (D1–D5 and E1–E3) questions were too varied to code, as many of these questions asked about sensory experiences that differed by person and by clinical immersion location. Thus, thematic analysis on these data did not produce consistent source themes and was deemed not successful on these student reflection questions. Student responses to the reflection questions from the remaining three categories did provide source themes during thematic analysis (Tables 3, 4, 5, 6). The sections that follow summarize the results from our thematic analysis of these questions (E4–E5 and AL1–AL5).
Learning in the Clinic
To learn how students describe their own learning in the clinic after weeklong immersions, students were specifically asked “What did you learn this week?” (AL1) and “What aspects of this week’s clinical immersion experience were the best learning opportunities?” (AL3). The source themes that emerged from these two questions and the percentages of reflections that identified these themes are shown in Table 3.
Analysis of Socioeconomic and Demographic Factors
During their (IN)SCRIBE Program experience, students had one-week clinical rotations in varied medical settings, which serve diverse patient populations. Thus, they were asked to critically reflect on the question “What connections can you now describe between socioeconomic status and health care?” (AL2). Both inferred and observed source themes emerged from this question, and the percentages of reflections that identified positive-inferred, positive-observed, negative-inferred, negative-observed, neutral-observed themes, and not inferred or observed are shown in Table 4.
In addition to reflections related to socioeconomic status, students were asked to critically reflect in response to questions “Did you notice any demographic or health-related trends among the patient populations that you observed?” (E4) and “To what extent are the economics of health care (cost, insurance, etc.) apparent in the clinical setting(s) you observed?” (E5). With regard to demographics, the source themes that emerged from the question (E4) included gender-related, race-related, age-related, health-related, and other demographic trends. In terms of economics of health care, the source themes that emerged from the question (E5) included high cost or expenses, inadequate insurance coverage, low cost or expense, adequate insurance coverage, and not observed. Our definitions of these source themes, the percentages of reflections that identified these themes, and student reflection examples are shown in Table 5.
Biomedical Engineering Design
Connections between the clinical immersion experiences and future engineering decisions were sought by asking students to critically reflect on questions “How is what you learned this week applicable to your training as a biomedical engineer?” (AL4) and “The next time you work on a design project, will this experience affect your approach?” (AL5). The three source themes identified regarding biomedical engineering training included an understanding toward design, increased knowledge of medicine and medical technologies, and communications in health care settings. Considerations identified by students when asked about their next design project included inspiration, economics, empathy, technological development, universal design, and effective communication. The source themes that emerged from these two questions and the percentages of reflections that identified these themes are shown in Table 6.
Discussion
Critical Reflection on General Experience
The first part of the DEAL model for critical reflection asked questions to Describe (D1 through D5) and to Examine (E1 through E3) student experiences; however, we found student responses to these questions were too varied to code. These questions were intentional about engaging each student in a reflection mode where they could recall and provide detailed accounts of their emotions and sensory experiences in an objective way. While source themes did not emerge for these questions, student responses were detailed and identified many aspects of the clinical immersion experiences that were new, exciting, or surprising.
Regarding their feelings upon arrival in the clinic and throughout the weeklong rotation (question D1), one of the students reported being nervous at first and how they became more comfortable with time, “I was extremely nervous. I know I am squeamish and was very anxious to see how my body reacted to the new environment. Luckily, throughout the week I gained confidence and understanding of my new limits of what I can handle.” Another student reported that “…As the week went on I was less mesmerized by the actual surgery and could focus on the tools techniques and ergonomics of the overall operation.” While this student’s excitement waned, it can be important to settle the senses in new environments to focus on the objective of the clinical immersion, which in this case was identifying user needs from a biomedical engineering perspective. The responses to this first reflection question demonstrate the value of extended (e.g., weeklong) clinical immersion rotations, as students may need time to acclimate to new environments before meeting desired learning objectives.
Students also commented on new stimuli (sight, smell, sound) they experienced (question D2), such as this student identified new smell and new sight, “The cauterizing smell was overwhelming and terrible. After watching a certain operation for a while, the bright white lights above the operating bed made my eyes hurt...” Another student talked about the new stimuli they observed based in the ophthalmology department, “The instruments used to manipulate the eyelid and eyeball were very new. They used some special blades for eye surgery as well. On top of that, there were the smallest sutures I have seen for sewing up the eye wall tissue.” Students also talked about different types of activities and procedures they observed (question D3). For example, one student quoted, “We watched stomach sleeves, hernia repair, gallbladder removal, and gastric bypass. I am not sure what each surgery accomplishes in the long run, and there are a lot of nuances that we saw in each surgery. All were very interesting to observe.” Student reflections on new stimuli varied, but it was evident that students were experiencing new things and learning new medical procedures performed with medical technologies that biomedical engineers help design. Another important aspect of a clinical immersion experience for engineering students is realizing the variety of medical professionals with whom they may interact. In response to question D4, students identified the different people they met in the clinic, often identifying the wide range of medical personnel present. For example, one student shared, “We met pediatric patients, nurses, nurse practitioners, residents, medical students, dieticians, and doctors.” Furthermore, students commented on the efficiency of communication between these health care professionals (question E2). “The primary forms of communication were e-mail, phone calls, in-person meetings, and Varian Eclipse through [a website]…In-person communications seemed to be the most efficient, especially when customers didn’t have a great grasp on what exactly they needed...Longer meetings with tangible interactions would be most effective, but difficult to schedule.”
Students also observed the use of different technologies for treating patients during clinical immersion and they reflected on those technologies. For the question of if the students have observed anything remarkable, interesting, or unexpected thing (question D5), diverse experiences were shared with most being different technologies they witnessed in clinical settings. One of the students quoted, “I observed an ultrasound-guided Botox injection, which was fascinating to see as it was for a patient with hip pain whose target nerve was behind large nerve bundles and arteries. It was a cool procedure to witness. Another patient had fascinating equipment to accommodate his ALS progression. He had gyroscopic and eye controls to perform his wheelchair motion and text-to-speech functions, which was amazing to see in practice…” For the question of different kinds of high-tech and low-tech technologies used in clinical settings observed (question E1), students reported on both types of technologies and their importance. One of the students quoted, “There were so many high-tech technologies. The single-use endoscope controllers, the small cameras, the fiber optic cables, and the anesthesia machine. Not to mention the lights, and the C- arm. All those technologies seemed high-tech. The only low-tech things I can think of are the stirrups, the pressure pump, the saline bags, and the computers and tv monitors present...” Students also observed different kinds of waste produced by these technologies like how the packaging of different technological equipment is being thrown out and how this issue is contributing to the waste production. For the question of how much waste they observed producing in the clinical settings, (question E5), one student quoted, “Waste was actually one of the problems we identified in the operating room. A lot of disposables were encased in shrink-wrap plastic and/or paper that was ultimately thrown out. The sterile covers on boxes of equipment were also thrown out rather than laundered.”
Overall, when reflecting generally on their clinic immersion, (IN)SCRIBE Scholars discussed diverse experiences such as becoming increasingly comfortable in a medical facility as the weeks passed, feeling excited and overwhelmed, and sharing of surgeries and medical procedures witnessed. Scholars reflected thoroughly on these questions and described the variety of their experiences well, achieving the goal of the “D” in the DEAL model of critical reflection. Our future work will continue including these questions as part of the critical reflection model to ensure students think deeply about what they did during each clinical immersion experience. In other words, students cannot critically reflect unless they can Describe and Examine their experiences. With more (IN)SCRIBE Scholar reflections, we can revisit these questions to determine if any meaningful patterns emerge.
From the remaining DEAL model for critical reflection questions (E4–E5 and AL1–AL5), three categories of questions emerged: questions where students reflected on their general learning from clinical immersion (AL1 and AL3, Table 3); questions where students reflected on demographic or health-related trends of patients, cost of health care, and the connection between socioeconomic status and health care (AL2, E4, and E5, Tables 4 and 5); and questions where students reflected on how their future engineering design approach (AL4 and AL5, Table 6). For Tables 3, 4, 5, and 6, some reflection responses can be classified into several source themes, causing the overall percentage to exceed 100% for some questions. On the other hand, some responses were too vague to be categorized, or some students did not answer certain questions, leading to a percentage below 100% for those particular questions.
Critical Reflection on Learning in the Clinic
The critical reflection questions on learning in the clinic asked students to self-report their own learning in a specific experiential setting (i.e., a clinic setting) and encouraged reflection on observed collaborations. Students discussed what they learned while being interactive with medical practitioners and patients which enhanced engagement and self-reportedly seemed to improve their learning retention during their clinical immersion experiences.
The majority of students (65%) identified medical knowledge as a moment of learning in the clinic (AL1, Table 3). Student reflections captured their notes on how medical equipment worked, how patients were treated, and the like. In one example, a student referred to learning medical knowledge, “I learned a lot about OR etiquette as well as the lingo within the OR. I also learned about the most common procedures done for urology including stone removal, bladder nucleation, prostate nucleation, and stent implantation and removal.” In addition to medical knowledge gains, a majority of the students (59%) identified surgical or procedural observation as impactful to learning in the clinic (AL3, Table 3). For example, one of the students quoted, “Seeing surgery up close was a fantastic learning experience, in my opinion. Being able to see first-hand laparoscopic procedures was very cool to see and real-life applications of medical devices in use—vacuum systems to bloat the abdomen during surgery, fiber optic cables to create a clean beam of light for the camera, tiny tools that allow for complete control, the Davinci XI tools, etc.” Furthermore, students also reflected on how patients were not able to receive proper treatment due to the increased cost of health care. They expanded upon different diseases, their treatment procedures, and the medical equipment they observed to use for the treatment procedures which enhanced their learning curve, and these observations led them to think about the links between engineering and innovation. Students also reflected on their experiences with medical sales representatives and other non-physician clinical team members (e.g., medical students, nurses). One student wrote, “The best learning experience was in the OR because I got to speak with an sales representative from the [a company name] company. He explained his role in the company and I got to see the different implants that are used in surgery with varying materials based on the medical professional’s needs.” Regarding other non-physician team members, one of the students quoted, “Talking to the current medical students that were actually performing the simulations was probably the best experience. They added a different perspective and bridged the gap between my (non-existent) medical knowledge and the expectations in the real world.” Overall, these learning in the clinic experiences embodied contextualized clinical environment and required the students to acquire and apply understanding on their own [15].
Critical Reflection on Analysis of Socioeconomic and Demographic Factors
The (IN)SCRIBE Program aims to challenge students to consider the implications of engineering design decisions on public health and health care equity. To better identify how students observe demographic and health-related trends of patients, economics of health care, and the connection between socioeconomic status and health care, students were asked to critically reflect on these topics after their clinical experiences. In their reflections, they grappled with the complex relationship between socioeconomic status and health care in the United States and discussed any perceived observations of health care disparity across the life cycle beginning in the pediatric department and ending among the elderly.
Categorized observations from student reflections were gender-related (9%), race-related (21%), age-related (20%), health-related (25%), and other demographic (21%) (E4, Table 5). Specific reflections noted how high cost or inadequate insurance coverage could affect patient treatment. For example, one student wrote, “This week was a little more involved with cost and insurance as most of the patients were lower income and needed things like prosthetics, boots, or other orthopedics, but weren’t able to afford them or had trouble with Medicare to be able to get the products.” They also highlighted how adequate insurance coverage (9%) helped to receive some treatment procedures and helped patients (E5, Table 5). Thirty-nine percent of students reported that some treatments have expensive costs (E5, Table 5). About adequate insurance coverage, one of the students quoted, “I got to see a list of every single tool that was used in the robot surgeries, and they are quite expensive. Although the robot costs $1.78M the tools seem to cost so much more than I would’ve thought. However, insurance does in fact cover that kind of stuff.” About cost being expensive, one of the students quoted, “The cost of the OR equipment and materials are apparent and when talking to the surgical techs the amount of money that is on the table is unbelievable.”
The majority (63%) also noted a negative impact on health care due to lower socioeconomic status, as some patients were not able to receive proper treatment (AL2, Table 4). One student quoted, “We know from data that not all demographics receive the same economic opportunities. Specifically for orthopedic trauma, these are injuries that it is extremely difficult to live with and may present death if not treated so I can see how the high cost of these procedures may cause someone with not as much economic potential as others to avoid operation…” Despite this, 16% of the student reflections inferred or observed positive aspects of health care on socioeconomic, and demographic observations. For example, one student observed, “The greatest example I saw was how cost-effective the custom bolus fitting process was for the patients and how they are fully covered by insurance. This ensures no matter the patient or area desired, everyone receiving radiation therapy has the access to a custom fit bolus to make their radiation experience better and prevent scatter burn.” Overall, in the clinical setting in the context of socioeconomic and demographic observations, they tried to identify disparity and health care economics.
Critical Reflection on Biomedical Engineering Design
Finally, students provided ample reflections on how clinical immersion experiences would affect their biomedical engineering design approach in the future. Specifically, biomedical engineering students recognized their “identity” and established a professional connection with the clinical immersion experience (AL4 and AL5, Table 6). These questions challenged the students to understand unmet user needs and they experienced the nature of engineering design for solving real-world problems [11]. Through more practice, adaptive expertise, and learning about other professionals involved in improving health care and patients, students had the opportunity to gain a better understanding of their profession and their roles within it [3]. When they were asked about which learning was most applicable to training a biomedical engineer, the majority (54%) critically reflected that knowledge of medicine and medical technology really helped (AL4, Table 6) where one of the students quoted, “This week offered a pretty deep exploration into 3D modeling and 3D printing, both of which are important skills I’ve remarked upon previously in this week’s reflection. I think these skills that I practiced this week will help tremendously in the design process of future projects through the BME curriculum and when I enter the job force.” Over one-third of students (36%) also shared that when they would work on a design project next time, they would focus more on the technological development part of the design (AL5, Table 6) where one of the students quoted, “I think for capstone, this will be something that will help me immensely from being able to talk to my sponsors better, really know how to frame my questions, think about the functionality and the user a bit more, and what kind of settings the device is intended to be used in rather than just straight functionality like my other design projects.”
Beyond the technological development of a device or process, student reflections captured that they were also able to envision situations that would use their experiences toward universal design considerations (28%) and that would consider economics during the design process (15%). Some students also identified inspiration (9%), effective communication (5%), and empathy (3%) as aspects of design that they would consider after thinking about their immersion experiences. Despite identified percentages being low, these responses show students also considered non-technical skills required to be a good designer which will help them to design devices effectively and efficiently. While these skills are not directly taught in this experience, our curriculum incorporates communication through Technical Communication (TCM) courses (i.e., Introduction to Engineering Technical Reports and Technical Data Reporting and Presentation) paired with required biomedical engineering lab courses during the second and third years in our plan of study. However, the data suggest an opportunity to explicitly ask Scholars how or where they envision communication, empathy, and inspiration belonging in the design process. Furthermore, our data suggest another opportunity to explicitly integrate inspiration and empathy into our curriculum to augment the student connections between clinical rotations and the biomedical engineering design process and stakeholders. In summary, they blended traditional engineering with issues of health care where they imagined their future self as a biomedical engineer. Due to the relatively low percentage of non-technical skills such as empathy and inspiration, instructors must prioritize the development of these skills. This is because the process of solving problems using the engineering design process in healthcare delivery requires students to think from multiple perspectives, which necessitates the use of non-technical skills.
Maximizing Learning Opportunities in Biomedical Engineering Clinical Experiences
Undergraduate biomedical engineering student reflections indicate that our clinical immersion experience exposed students to real examples related to biomedical engineering’s goal—advancing public health. Knowing that fewer than 25% of reporting biomedical engineering programs say their students have access to an immersion experience, biomedical engineering educators can use these data to advocate for integrated and/or supplemental clinical immersion experiences to augment biomedical engineering student training [45]. While formal engineering design training and technical skill development are necessary, our work suggests there exists potential for clinical immersion experiences to also provide user-centered design training, professional development, and opportunities for students to develop their oral and written communication skills. Additionally, our experience implementing the DEAL model for critical reflection in our undergraduate biomedical ethics curriculum further demonstrates the value of critical reflection for student learning [46, 47].
Our participants reflected that clinical immersion gave them the opportunity to learn about medical insurance (E5, Table 4), access to health care or lack of access to health care (AL1, Table 3 and AL2, Table 4), stakeholder perspectives (AL1 and AL3, Table 3), and medical terminology/knowledge (AL1, Table 3). These topics are connected, perhaps distinctively, to our discipline [6], so it is the collective responsibility of biomedical engineering educators to ensure we are training competent and confident individuals that can recognize “common humanity and disparate needs” [48] in their professional pursuits. User-centered design and stakeholder perspectives are particularly important when designing to ensure equity of and accessibility to medical innovations and technologies are real design outcomes. Our data show students identify a variety of populations during their clinical observations (e.g., gender, race, age, health in Table 5), highlighting an educational space where the user and stakeholders can be emphasized as a priority during the design process. Amplifying the importance of including the user and stakeholders in the design process could potentially translate to innovations that promote health equity, a core value identified in our state [49].
Our program, like many others, provided students real interactions with other medical or health professionals, increasing student understanding of biomedical engineering as a discipline (e.g., students identified physicians and sales representatives as source themes in Table 3). While we did not track in our study the implications of an immersive clinical experience on student self-identity or career biases, we are aware that other published work has helped show preliminarily that expansion of student career opportunities happens during co-curricular experiences [50]. Student recognition of these varied source themes is an important realization for biomedical engineers in training as future employers will seek those that can identify and work well on inter- or multi-disciplinary teams [45].
Furthermore, design and knowledge of medical devices were topics forefront on student minds when reflecting on their clinical immersion experiences; however, talking with patients reminded some why they chose biomedical engineering as a profession (AL3, Table 3). Still, students noted that communication with a range of audiences as a source theme when asked how their learning was applicable to their training as a biomedical engineer (AL4, Table 6). These data support the continued need for biomedical engineering educators to persist in their immersion efforts because experiential learning can provide students real opportunities to practice meaningful oral and written communication skills with medical professionals.
Training biomedical engineers requires intentional inclusion of meaningful experiences within an undergraduate curriculum. Our work confirms that some of the skills and outcomes identified by biomedical engineering educators (e.g., communication, professional development, application of medical knowledge) parallel with what our students identified when reflecting on their participation in our clinical immersion program. We also identify areas of instruction from student identified themes, such as user-centered design and empathy, to amplify to better prepare biomedical engineering students to design toward equitable and accessible medical innovations and technologies.
We recognize that not all BME undergraduate programs can accommodate clinical immersion experiences for a variety of reasons (e.g., large programs, limited access to clinical partners). Thus, we envision that future work could provide guidance on how to use critical reflection in a meaningful way for programs with larger student cohorts or that are not in close proximity geographically to clinical sites. While General Experience data suggest that students may need to acclimate to the clinic setting before taking note of some important needs, further work could identify which reflection prompts could be introduced in classroom experiences for large student cohorts. We also advocate that BME programs seek collaborative partnerships with community resources beyond traditional clinical sites [51], as a clinical immersion experience in a nearby teaching hospital may not be geographically convenient or accommodating. Most communities do have hospitals, rehabilitation centers, dialysis centers, nursing homes, or other experiential settings in which BME students could have an immersive experience. Further, program collaborations within the field of BME could help expand such immersion experiences to more students.
Limitations
Our analysis covered more than one hundred reflection journal entries written by students in our summer clinical immersion program. Nonetheless, our study remains limited by its relatively small sample size, as we have analyzed data from just twenty student participants. As we complete further instances of the clinical immersion program and collect data from additional students, we expect to have sufficient data to approach further research questions. For example, we may compare student experiences in different types of rotations (e.g., medical vs. surgical, low- vs high-resource clinics), examine how student experiences and attitudes change as they progress through the five weeklong immersion rotations in our program, or look for trends based on student class standing or student demographics.
In addition to the limitations that stem from our meager sample size, there were additional challenges related to the thematic analysis of student reflections. Most notably, student responses to several of our reflection prompts were too varied for us to identify consistent themes. This primarily affected the questions from the “Describe” section of our DEAL model-structured reflections. In our study, we were also unable to account for the potential influence of a clinical site rotation ordering effect. However, with a larger dataset, we may have the opportunity to investigate additional factors such as a comparison between (IN)SCRIBE and non-(IN)SCRIBE Scholar reflections, or the impact of the order in which (IN)SCRIBE clinical visits were conducted. In the future, we may consider reworking these questions to elicit more consistency in student responses. Alternatively, patterns may emerge once we have a larger sample size to study.
Conclusion
Despite the prevalence of clinical immersion experiences in undergraduate biomedical engineering programs, there has been little rigorous analysis of student reactions to their time in the clinic. As observed in other disciplines, critical reflection can enhance student learning and professional growth during immersion experiences. For biomedical engineers, this could entail greater skill in needs identification, communication with health care professionals, and user-centered design. Our work shows that clinical immersion experiences can help students realize how they are learning in clinical settings, identifying socioeconomic and demographic factors in the clinic, and applying these clinical immersive experiences toward future biomedical design. Our results support why biomedical engineering educators should continue to create and improve clinical immersion programs and experiences that amplify the needs of many users and stakeholders in the design process. These efforts may translate to more equitable medical innovation for all from the next generation of biomedical engineers.
Data Availability
N/A
Code Availability
N/A
References
Bioengineers and Biomedical Engineers: Occupational Outlook Handbook: U.S. Bureau of Labor Statistics. 2022. https://www.bls.gov/ooh/architecture-and-engineering/biomedical-engineers.htm. Accessed 8 Feb 2023.
Kotche M. Clinical immersion internship introduces students to needs assessment. In: 2016 ASEE annual conference & exposition. 2016.
Singh A, Ferry D, Mills S. Improving biomedical engineering education through continuity in adaptive, experiential, and interdisciplinary learning environments. J Biomech Eng. 2018. https://doi.org/10.1115/1.4040359.
Brennan-Pierce EP, Stanton SG, Dunn JA. Clinical immersion for biomedical engineers: pivoting to a virtual format. Biomed Eng Educ. 2021;1(1):175–9.
Stirling S, Kotche M. Clinical immersion program for bioengineering and medical students. In: 2017 ASEE annual conference & exposition. 2017.
APS. (n.d.). https://amspub.abet.org/aps/category-search?disciplines=9°reeLevels=B&countries=US. Accessed 4 March 2023.
Linsenmeier RA, Saterbak A. Fifty years of biomedical engineering undergraduate education. Ann Biomed Eng. 2020;48(6):1590–615.
Kotche M, Felder AE, Wilkens K, Stirling S. Perspectives on bioengineering clinical immersion: history, innovation, and impact. Ann Biomed Eng. 2020;48(9):2301–9.
Sawyer D, Aziz KJ, Backinger CL, Beers ET, Lowery A, Sykes SM. An introduction to human factors in medical devices. US Department of Health and Human Services, Public Health Service, Food and Drug Administration, Center for Devices and Radiological Health. 1996.
Schwartz JG, Kumar UN, Azagury DE, Brinton TJ, Yock PG. Needs-based innovation in cardiovascular medicine: the Stanford Biodesign process. JACC. 2016;1(6):541–7.
Kotche M, Tharp S. Interdisciplinary medical product development senior capstone design. In: 2015 ASEE annual conference & exposition. 2015. p. 26–1013.
Hotaling N, Fasse BB, Bost LF, Hermann CD, Forest CR. A quantitative analysis of the effects of a multidisciplinary engineering capstone design course. J Eng Educ. 2012;101(4):630–56.
Allen RH, Acharya S, Jancuk C, Shoukas AA. Sharing best practices in teaching biomedical engineering design. Ann Biomed Eng. 2013;41:1869–79.
Delany C, Watkin D. A study of critical reflection in health professional education: ‘learning where others are coming from.’ Adv Health Sci Educ. 2009;14(3):411–29.
Wilson H, Warmington S, Johansen ML. Experience-based learning: junior medical students’ reflections on end-of-life care. Med Educ. 2019;53(7):687–97.
King PM, Kitchener KS. Developing reflective judgment: understanding and promoting intellectual growth and critical thinking in adolescents and adults. Jossey-Bass Higher and adult education series and Jossey-Bass social and behavioral science series. San Francisco: Jossey-Bass; 1994.
Turner P. Critical thinking in nursing education and practice as defined in the literature. Nurs Educ Perspect. 2005;26(5):272–7.
Thomas DSM. The use of portfolio learning in medical education. Med Teach. 1998;20(3):192–9.
Henderson P, Johnson MH. An innovative approach to developing the reflective skills of medical students. BMC Med Educ. 2002;2(1):1–4.
Pee B, Woodman T, Fry H, Davenport ES. Appraising and assessing reflection in students’ writing on a structured worksheet. Med Educ. 2002;36(6):575–85.
Boenink AD, Oderwald AK, De Jonge P, Van Tilburg W, Smal JA. Assessing student reflection in medical practice. The development of an observer-rated instrument: reliability, validity and initial experiences. Med Educ. 2004;38(4):368–77.
Crowe MT, O’Malley J. Teaching critical reflection skills for advanced mental health nursing practice: a deconstructive–reconstructive approach. J Adv Nurs. 2006;56(1):79–87.
Schei E, Fuks A, Boudreau JD. Reflection in medical education: intellectual humility, discovery, and know-how. Med Health Care Philos. 2019;22(2):167–78.
Sandars J. The use of reflection in medical education: AMEE Guide No. 44. Med Teach. 2009;31(8):685–95.
Tawanwongsri W, Phenwan T. Reflective and feedback performances on Thai medical students’ patient history-taking skills. BMC Med Educ. 2019;19(1):1–8.
Reynolds M. Reflection and critical reflection in management learning. Manag Learn. 1998;29(2):183–200.
Gaupp R, Fabry G, Körner M. Self-regulated learning and critical reflection in an e-learning on patient safety for third-year medical students. Int J Med Educ. 2018;9:189.
Eyler J, Giles DE, Jr., Gray CJ. At a glance: what we know about the effects of service learning on students, faculty, institutions and communities, 1993–1999. Unpublished manuscript, Vanderbilt University, Nashville, TN; 1999.
Welch M. The ABCs of reflection: a template for students and instructors to implement written reflection in service-learning. NSEE Q 1999;25(2).
Ash SL, Clayton PH. Generating, deepening, and documenting learning: the power of critical reflection in applied learning. J Appl Learn High Educ. 2009;01:25–48.
Denny MDA, Hardman AM. Mississippi State University extension undergraduate apprenticeship program: a model for critical reflection through community-engaged research and outreach. Adv Agric Dev. 2020;1(1):86–96.
Shehane MR. A phenomenological study of high-impact practices: exploring learning through coupling internships and service-learning (Doctoral dissertation). (2014).
Odom SF, Shehane M, Moore LL, McKim B. An analysis of a high-impact field experience in agriculture: documenting critical thinking skills through reflection. NACTA J. 2014;58(3):214–20.
Farmer CN. Critical reflection seals the DEAL: an experiment examining the effects of different reflection methods on civic-related outcomes of service-learning (Doctoral dissertation, University of Dayton). (2015).
Ash SL, Clayton PH. The articulated learning: An approach to guided reflection and assessment. Innov High Educ. 2004;29(2):137–54.
Ash SL, Clayton PH, Moses MG. Learning through critical reflection: a tutorial for service-learning students. Raleigh: Center for Excellence in Curricular Engagement, North Carolina State; 2007.
Jameson JK, Clayton PH, Bringle RG. Investigating student learning within and across linked service-learning courses. In: Scholarship for sustaining service-learning and civic engagement; 2008. p. 3–27.
Clarke V, Braun V, Hayfield N. Thematic analysis. Qual Psychol. 2015;222(2015):248.
Braun V, Clarke V. Thematic analysis. Washington: American Psychological Association; 2012.
Mezirow J. On critical reflection. Adult Educ Q. 1998;48(3):185–98.
Brookfield SD. Assessing critical thinking. New Dir Adult Contin Educ. 1997;1997(75):17–29.
Mezirow J. A critical theory of adult learning and education. Adult Educ. 1981;32(1):3–24.
Smith E. Teaching critical reflection. Teach High Educ. 2011;16(2):211–23.
Miller S, Higbee S. Work in progress: a clinical immersion program to train biomedical engineers to identify unmet health needs in urban clinics. In: 2022 ASEE annual conference & exposition. 2022.
Billiar K, Gaver DP III, Barbee K, Singh A, DesJardins JD, Pruitt B, Margulies S. Learning environments and evidence-based practices in bioengineering and biomedical engineering. Biomed Eng Educ. 2022;2(1):1–16.
Hess JL, Miller S, Higbee S, Fore GA, Wallace J. Empathy and ethical becoming in biomedical engineering education: a mixed methods study of an animal tissue harvesting laboratory. Australas J Eng Educ. 2021;26(1):127–37.
Miller S, Higbee S, Wallace J, Schild J, Ji J. Work in progress: embedded ethical inquiry and reflection in a biomedical engineering curriculum. In: 2020 ASEE annual conference & exposition. 2020.
Monzon JE. Teaching ethical issues in biomedical engineering. Int J Eng Educ. 1999;15(4):276–81.
P. 2022-2025 IDOH strategic plan. PHPM. 2022 https://www.in.gov/health/phpm/tracking-public-health-performance/state-health-improvement-plan/. Accessed 16 March 2023.
Jamison CSE, Wang AA, Huang-Saad A, Daly SR, Lattuca LR. BME career exploration: examining students’ career perspectives. In: 2021 ASEE virtual annual conference & exposition. 2021.
Huber J, Higbee S, Espinosa C, Bazrgari B, Miller S. Immersion experiences for biomedical engineering undergraduates: comparing strategies and local partnerships at two institutions. Int J Eng Educ. 2023;39(4):961–75.
Acknowledgements
This work was supported by the National Institute of Biomedical Imaging and Bioengineering of the National Institutes of Health under Award Number R25EB031389. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors also acknowledge the support of the biomedical engineering department at Indiana University Purdue University Indianapolis and the STEM Education Innovation and Research Institute.
Funding
Research reported in this publication was supported by the National Institute of Biomedical Imaging and Bioengineering of the National Institutes of Health under Award Number R25EB031389.
Author information
Authors and Affiliations
Contributions
N/A
Corresponding author
Ethics declarations
Conflict of interest
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors also acknowledge the support of the biomedical engineering department at Indiana University Purdue University Indianapolis.
Ethical Approval
This work was approved by the Indiana University IRB: #2012065291.
Consent to Participate
Students consented to participate in this study per the Indiana University IRB: #2012065291.
Consent for Publication
N/A
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tabassum, N., Higbee, S. & Miller, S. A Qualitative Study of Biomedical Engineering Student Critical Reflection During Clinical Immersion Experiences. Biomed Eng Education 4, 15–31 (2024). https://doi.org/10.1007/s43683-023-00124-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43683-023-00124-4