
Abstract
There is a lack of information about medical waste management in Iraq. This study aims to monitor and evaluate the current situation of medical waste management in Baghdad as it represents the capital and the biggest populated city in Iraq. About 32% of hospitals are located in Baghdad. Ten state-owned hospitals in Baghdad with the biggest bed capacity were investigated. The study used structured interviews with staff in charge of waste management in the sampled hospitals to collect data. The results showed that the generation rate of medical waste in the ten hospitals was 0.5 kg/(bed·day). The study also found that there were insufficient, ineffective, and improper isolation, collection, storing, processing, and safe disposal of medical wastes in the sampled public hospitals of Baghdad. The study recommended that the Iraqi Ministry of Health takes extensive and quick effective measures to better monitor and evaluate medical waste management and provide ongoing training to personnel responsible for waste management in the hospitals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With the increase in population, solid wastes increase in return. In the end, wastes pollution becomes a very serious environmental and public health issue. Medical waste includes all the wastes generated by health-care activities and produced by a medical institution (public or private), a medical research facility, or a laboratory [1]. But not all the waste produced by medical facilities can be considered as medical waste. About 75%–90% of the waste produced by medical facilities are general waste or municipal waste. This waste is usually managed by municipal waste services. The rest of the healthcare waste (10%–25%) is medical waste and can be very hazardous and dangerous to health [2]. Medical wastes are classified into four categories: Infectious wastes which include bandages, gloves, cultures, swabs, blood and body fluids, hazardous wastes which include sharps, instruments, and chemicals; radioactive wastes which come from cancer therapies; and finally, pharmaceutical wastes [3].
Medical waste management represents an evolving concern expanded by an absence of training, awareness, and financial resources to support solutions. The process of collecting and removing this waste is very important as it has a direct influence on the public and environmental health [4]. Unfortunately, medical waste management in developing countries faces various challenges such as illegal recycling, lack of staff training, and poor segregation of waste [5]. The World Health Organization (WHO) revealed in a study conducted in 22 countries that 18%–64% of healthcare institutions did not use waste disposal methods [6].
In Iraq, waste management has been a main environmental and health problem for the last several decades. According to the Baghdad municipality statistics, an estimate of 10,000–11,000 tons of solid wastes produced daily in Baghdad. About 7000 tons of wastes are deposited per day in landfills. The other 5000 tons were deposited in unsanitary landfills and random areas [7].
The Iraqi government developed a national solid waste management plan in 2007 [8]. However, this policy was not adopted and waste management is still considered one of the most serious and challenging environmental and health problems in Iraq [9]. A more recent bill about waste management was proposed by the Iraqi Parliament but was never approved [10]. An Iraqi government official report indicated that medical waste management in Iraq is very poor and requires extensive reform and review [3]. The current overall situation of medical waste management in Iraq is deteriorating [11]. As of 2019, there are 280 public and private hospitals in Iraq. About 32% (91 hospitals) are located in Baghdad. The purpose of this study was to monitor and evaluate the current status of health-care waste management in Baghdad, the capital and the largest city in Iraq, and to explore the current situation of the production, isolation, collection, storing, processing, and safe disposal of medical wastes in the public hospitals of Baghdad.
Materials and methods
This is an observational cross-sectional study and all data were collected during a face-to-face interview. Baghdad is the capital of Iraq and the most populated city in the country. With an estimate of more than eight million people living in Baghdad, healthcare facilities witnessed a dramatic increase within the last ten years. Hospitals in Baghdad are either government-owned or private. The sample included in this study was limited to government hospitals only. Other healthcare facilities such as private hospitals, private medical laboratories, private clinics, and pharmacies were excluded. Out of the 45 state hospitals operating in Baghdad, ten hospitals with the biggest bed capacity were selected. Table 1 shows the chosen sample with their bed capacity.
The survey included six questions about the current status of the generation, collection, on-site handling, storage, processing, recycling, transportation, safe disposal of medical waste, and personnel training. Information was collected through in-depth face-to-face interviews with supervisors and/or directors of the waste management unit at each hospital. Although direct interviews might lead to hiding some relevant information, the author’s observation and analysis of the waste management situation was included to lower any interview bias that could arise from the process. Data were collected through weekly visits to the surveyed hospitals to conduct the interviews. All data were collected during 6 months from February 2019 to July 2019.
Results
Amount of waste generated
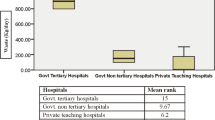
The first question of the survey was about the amount of waste that was collected monthly from hospitals. Figure 1 shows the monthly amounts of medical waste in all the ten surveyed hospitals for 6 months. In addition, Table 2 shows the average generation rate of medical waste generated by each hospital per day and month. The estimated quantity of medical waste from the hospitals was about 2.5 tons per day, representing an average generation rate of 0.5 kg/(bed·day).

Monthly weight (in kg) of medical wastes per month produced in 10 hospitals in Baghdad
Collection of waste
The second question of the survey was about how medical waste was collected and stored in each hospital. According to Table 3, the results of the current study showed that all the hospitals had temporary containers to store waste. However, nine hospitals stored general waste with hazardous waste. Also, based on the author’s actual observations, there were no specific areas at these hospitals to store the waste. Seven hospitals had the personnel manually carry waste and stock them in designated areas where they would be incinerated without being isolated or classified. Although with the presence of medical waste carts in all the surveyed hospitals, personnel collected medical waste and handled them sometimes manually and medical waste was collected and stored in black-colored plastic bags that can be easily broken without properly segregating hazardous from non-hazardous waste. Then, these bags were placed in an area near the incinerator so that they would be processed later. Two hospitals in the surveyed sample had their central incinerator broken down for 2 months during the study period and all the biomedical waste was collected and stored in heaps. During the time of the incinerator’s breakdown, wastes were collected and stored in temporary containers for several days before transferred to landfills without incineration.
Handling of waste
The third question was about how medical waste was processed and handled in each hospital. According to Table 4, the results of the current study showed that all the ten hospitals had an incinerator. However, two hospitals had their incinerators broken down and another two hospitals had working incinerators with many malfunctions.
Waste recycle
The fourth question was about how municipal waste was recycled in each hospital. According to Table 5, the results of the current study showed that all the ten hospitals that were surveyed had no waste recycle system.
Transfer of waste
The fifth question was about how medical waste was transported and disposed of in each hospital. According to Table 6, the results of the current study showed that in all the ten hospitals, there were no specialized vehicles to transport the residues of the incinerated waste to landfills. Four hospitals used their incinerators to dispose of the liquid biomedical waste. The rest of the surveyed hospitals used carts to manually move ashes from the incinerator to the main waste containers.
Training of staff
The sixth question was about staff training in waste management. According to Table 7, the results of the current study showed that personnel who were responsible for collecting and processing waste management at all the ten hospitals lack proper knowledge and training of basics and essentials of biomedical waste management. Also, workers who were responsible for transporting and processing medical waste did not wear any personal protection equipment.
Discussion
The current paper provided an overview of the current status of medical waste management in Iraq by selecting Baghdad the capital city as a case study. In this study, only ten state-owned hospitals were selected. The average generation rate of medical waste was 0.5 kg/(bed·day). The generation rate of biomedical waste in hospitals is generally influenced by the hospital’s specialization, bed capacity, number of inpatients, number of surgeries per day, and number of employees working in the hospital. Although the results of the current study showed a generation rate (0.5 kg/(bed·day)) that represents a very small number of medical facilities in Iraq, the overall generation rate of medical wastes based on the number of state-owned hospitals in Iraq could range from 3.8 to 4.2 kg/(bed·day) [3]. This amount is higher than the range of 0.6–3.7 kg/(bed·day), which was reported by several studies in other countries in the Middle East region [5, 12,13,14,15].
The Iraqi Ministry of Health and Environment has put general guidelines for hospitals to manage their medical waste. However, the results of the current study have shown that the surveyed hospitals still have serious issues in handling and collecting waste. The current results come in line with those of Al-Hashimi and Al-Mandalwi [16] and Al-Abaid [17]. In comparison with some neighboring countries, hospitals in Iran have excellent medical waste storage and collection [18]. On the other hand, medical waste management in Jordan, Syria, and Turkey still needs major improvement [19,20,21]. In general, the current situation of waste management in almost all the Middle East is characterized by insufficient jurisdiction, lack of control, and technical and financial resources [22].
In Iraq, incineration is considered the typical method used for managing wastes generated from hospitals and other healthcare facilities. The results of the current study have shown that only three hospitals had an autoclave. Al-Yarmook teaching hospital is the biggest hospital in the Al-Kharkh area in Baghdad. It has one autoclave, which was exposed to several malfunctions during the study period. Al-Imamain Al-Kadhumain medical city has also an autoclave and it had minor malfunctions during the study period. When the autoclave has malfunctioned, reusable materials were destroyed and replaced with single-use materials. The third hospital that had an autoclave was Baghdad teaching hospital-Medical City, which is the biggest hospital in Baghdad. This hospital lacked a liquid medical waste disposal system and all the liquid biomedical waste was directly dumped into the sewage system of the hospital. Since this hospital was located at the Tigris riverbank, the disposed-of biomedical waste would ultimately be in the river water. Consequently, Tigris River water would be heavily polluted and contaminated with biomedical and chemical substances. This is a very serious environmental and public health problem that was being previously raised and reported by several studies [23,24,25]. The remaining seven hospitals had incinerators but the incineration process was ineffective as the incineration temperature was not enough for complete incineration in all the surveyed hospitals. Optimum Incineration temperature must be between 540 °C and 980 °C in the primary chamber and between 980 °C and 1200 °C in the secondary chamber of the incinerator [26]. The results of this survey showed that incinerators in all the ten hospitals had their biomedical waste combusted at a temperature lower than the required temperature in the local Iraqi and international guidelines for medical waste incineration [27]. Moreover, all ten hospitals lacked proper procedures to weigh waste before being incinerated.
The current study showed that there are no waste recycling systems in the surveyed hospitals. Recycling helps in reducing the amount of waste needed to be dumped in landfills. In addition to saving more money, conserving energy, and dropping the levels of dangerous gases that might be emitted from the incineration process [28].
As for the transfer of medical waste, the results of the current study were consistent with those of Abbas and Ali [28].
Although the Iraqi Ministry of Health provided guidelines for hospitals to deal with biomedical waste, the results of the current study showed that the staff responsible for waste management in the ten surveyed hospitals did not follow these guidelines. Training has proven to be a very effective tool in improving the performance of staff responsible for medical waste management in hospitals [29, 30].
Conclusions and Recommendations
-
Private and state-owned hospitals in Baghdad are continuously growing in numbers. This will cause an increase in the size of the medical waste generated. While the Iraqi Ministry of Health has established guidelines intended to guarantee proper management of medical waste, it is very necessary to put these guidelines and rules into practice.
-
This study has shown that all the ten surveyed hospitals in Baghdad had an insufficient, ineffective, and improper collection, isolation, storing, processing, and recycling of medical wastes. Some hospitals mixed general waste with hazardous waste in addition to the absence of specialized storage for medical waste in hospitals.
-
All the incinerators in the surveyed hospitals had malfunctions and some of them were broken. Incinerators and open burning of wastes in landfills release toxic gases such as dioxin and furan. The damaged incinerators and uncontrolled burning of medical wastes that are mixed with general waste would ultimately heavily pollute the air.
-
Medical waste was dumped directly into the Tigris River leading to river pollution with dangerous chemical and biomedical contaminants.
-
Serious measures should be taken to reduce the levels of such poisonous gases in the air.
-
Personnel responsible for waste management in hospitals voluntarily or involuntarily ignored following hospital waste management best practices.
-
The amount of medical waste from the sampled hospitals in Baghdad was relatively low and that was due to the mixing of medical waste with general wastes. In the end, the weight of medical waste would be decreased.
-
Medical waste management is a complex process that must be handled by professional and well-trained personnel. For this reason, this study recommends the Iraqi Ministry of Health to conduct ongoing training to encourage and improve the performance and knowledge of waste management personnel in hospitals. In addition, enforcing better more strict laws against the improper storage or transfer of medical waste. Moreover, the Iraqi government must quickly act to provide maintenance and provide replacements to damaged incinerators in hospitals. More research should be conducted to focus on waste management in private healthcare facilities.
References
World Health Organization. 2014. Safe management of wastes from health-care activities. Switzerland: WHO.
Fraiwan, L.A., Lweesy, K.Y., Oweis, R.J., et al. 2012. Medical Waste Management. In: Yung-tse, H., ed. Handbook of Environment and Waste Management: Air and Water Pollution Control. World Scientific, pp 1015–1088.
Federal Board of Supreme Audit (FBSA). 2015. Detailed report on evaluating Ministry of Health policy of medical waste management. Republic of Iraq. Available at: https://www.fbsa.gov.iq/ar/reports/ (accessed 15 February 2019). [In Arabic].
Birpınar, M.E., Bilgili, M.S. and Erdoğan, T. 2009. Medical waste management in Turkey: A case study of Istanbul. Waste management 29 (1): 445–448.
Ali, M., Wang, W., Chaudhry, N., et al. 2017. Hospital waste management in developing countries: A mini review. Waste Management & Research 35 (6): 581–592.
Dahchour, A. and El Hajjaj, S.E. 2020. Management of solid waste in Morocco. In Negm, A.M. and Shareef, N. (eds) Waste Management in MENA Regions, Cham: Springer Water. https://doi.org/10.1007/978-3-030-18350-9_2.
Baghdad Mayoralty. 2018. Department of solid waste and environment. Monthly report. Available at: https://www.cosit.gov.iq/ar/env-ind (accessed 20 February 2019). [In Arabic].
Knowles, J.A. 2009. National solid waste management plan for Iraq. Waste Management & Research 27: 322–327. https://doi.org/10.1177/0734242X09104129.
Musheb, J.M. 2018. The Economics of Waste Recycling in Iraq: Wasted Resources and Lost Opportunities. European Journal of Economics and Business Studies 4(2): 90–98.
Iraqi Parliament. 2018. A study and a proposed bill about waste management. Available at: https://ar.parliament.iq/2018/10/13/ (accessed 12 July 2019). [In Arabic].
Federal Board of Supreme Audit (FBSA). 2019. Detailed report on The Iraqi government’s policy in solid waste management. Republic of Iraq. Available at: https://www.fbsa.gov.iq/ar/reports/ (accessed 20 August 2020). [In Arabic].
Al-Momani, H., Obaidat, M., Khazaleh, A., et al. 2019. Review of medical waste management in Jordanian health care organizations. British Journal of Healthcare Management 25 (8): 1–8.
Alzahrani, D. 2013. Environmental Legislation and the Management of Medical Waste. Global Cities Research Institute Melbourne, Australia: RMIT University.
Çetinkaya, A.Y., Kuzu, S.L. and Demir, A. 2019. Medical waste management in a mid-populated Turkish city and development of medical waste prediction model. Environment, Development and Sustainability, 22(7), 6233-6244.
Eslami, A., Nowrouz, P., and Sheikholeslami, S. 2017. Status and challenges of medical waste management in hospitals of Iran. Civil Engineering Journal 3(9): 741–748.
Al-Hashimi, M.A., and Al-Mandalwi, G.F. 2007. Management and treatment of solid waste in some hospitals in Baghdad. Journal of Technology and Engineering 25: 225–246. [In Arabic].
Al-Abaid M.M. 2002. Solid Waste Management of Hospitals in Baghdad City. MSc thesis, Al-Mustansiriya University, Baghdad.
Torkashvand, J., Pasalari, H., Jonidi-Jafari, et al. 2020. Medical waste management in Iran and comparison with neighbouring countries. International Journal of Environmental Analytical Chemistry, 1–14.
Alshraideh, H., and Qdais, H.A. 2017. Stochastic modeling and optimization of medical waste collection in Northern Jordan. Journal of Material Cycles and Waste Management 19 (2): 743–753.
İnan, O., Kumaş, K., and Akyüz, A. 2020. An overview of the medical waste disposal of Turkey. Scientific Journal of Mehmet Akif Ersoy University 3(2): 59–62.
Noufal, M.J., Maalla, Z.A., Adipah, S. 2020. Challenges and opportunities of municipal solid waste management system in Homs city, Syria. In Proceedings of the Institution of Civil Engineers-Waste and Resource Management 173(2), Thomas Telford Ltd. pp. 40–53.
Negm, A.M., and Shareef, N. (eds.). 2020. Waste Management in MENA Regions. Berlin: Springer.
Al Obaidy, A.M., Awad, E.S., and Zahraw, Z. 2016. Impact of Medical City and Al-Rasheed power plant effluents on the water quality index value of Tigris River at Baghdad city. Engineering and Technology Journal 34 (4): 715–724.
Al-Hiyaly, S.A., Warqa’a, N., and AL-Azzawi, M.N. 2016. Evaluating the Effects of Medical City Wastewater on Water Quality of Tigris River. Engineering and Technology Journal 34 (3): 405–417.
Mensoor, M., and Said, A. 2018. Determination of heavy metals in freshwater fishes of the Tigris River in Baghdad. Fishes 3(2): 23.
World Health Organization. 2001. Best practices for incineration. Available at: https://www.who.int/water_sanitation_health/medicalwaste/en/smincinerators3.pdf (Accessed 1 October 2019).
Iraqi Ministry of Health and Environment. 2009. National Guidelines for infection control in the Iraqi health institutions.
Abbas, S.M., and Ali, A.I. 2012. An analysis of the problem of solid waste transport using a transport model in Baghdad. Iraqi Journal of economic sciences 34: 149–196. [In Arabic].
Ozder, A., Teker, B., Eker, H.H., et al. 2013. Medical waste management training for healthcare managers-a necessity? Journal of environmental health science and engineering 11(1): 20.
Singh, S., Dhillon, B.S., Nityanand, A.K., et al. 2020. Effectiveness of a training program about bio-medical waste management on the knowledge and practices of health-care professionals at a tertiary care teaching institute of North India. Journal of Education and Health Promotion, 9.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mensoor, M.K. Medical waste management in Iraq: a case study of Baghdad. Waste Dispos. Sustain. Energy 2, 329–335 (2020). https://doi.org/10.1007/s42768-020-00055-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42768-020-00055-8