
Abstract
This review aimed to assess the evidence from observational and interventional studies in humans and animals regarding the role of selenium (Se) in male and female infertility. As oxidative stress can seriously impair male, and possibly also female, reproductive functions, it can be speculated that the antioxidant properties of Se could constitute one of the pathways by which this element is involved in fertility. Specifically, there are strong indications that Se influences the growth, maturation, and replication of oocytes, though the precise mechanisms have not as yet been fully elucidated. Given that it is not clear at present which tissue sample (blood, serum, seminal plasma, sperm, or follicular fluid) renders the most accurate picture of Se concentration in terms of its role in reproduction, the data are still insufficient to recommend routine assessment of Se status in men and women seeking fertility. Nevertheless, the existing evidence, despite being of limited quantity and somewhat low quality, suggests that Se supplementation (< 200 μg/d) is possibly beneficial in men through its improvement of sperm motility. Well-designed, randomized control studies are needed to reveal the seemingly diverse protective/positive role of Se supplementation in men and women seeking fertility treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Selenium (Se) is an essential trace element for the maintenance of human body homeostasis [1]. In the form of the amino acid selenocysteine, Se is incorporated in a large number of proteins, named selenoproteins, which exert an array of actions, such as antioxidant defense, redox state regulation, and cancer prevention, while also being involved in various metabolic pathways [2]. Because of these properties, some of the selenoproteins have emerged as potential biomarkers of both disease and Se status. As well as potentially offering some protection against the effects of heavy metals, Se also maintains the proper functioning of the reproductive system [3]. Se deficiency may, therefore, have detrimental effects on both the male and the female reproduction system.
During gestation, the recommended Se dietary allowance (RDA) ranges from 55 to 60 μg/d, higher than in the non-pregnancy state [3, 4]. A possible explanation for the augmented requirement of Se is the need for effective antioxidant defense, as gestation is characterized by increased oxidative stress, especially during early pregnancy. During normal pregnancy, placental oxidative stress (OS) is present during all three trimesters and is necessary to obtain normal cell function [4], as reactive oxygen species (ROS) and reactive nitrogen species (RNS) act as secondary messengers in various intracellular signaling cascades.
However, above a certain level, OS can negatively affect pregnancy and serious complications may arise. Higher maternal Se concentrations have been associated with a lower risk of miscarriage, preterm birth, pre-eclampsia, and autoimmune thyroid disease [5].
The current manuscript aimed to review the evidence, from observational and interventional studies in humans and animals, for a manifold role of Se in fertility and infertility, discussing the pathophysiology of this association.
Selenium and male infertility
Pathophysiology
The gonads, especially the testes, have high concentrations of Se, the latter being essential for normal testicular development, spermatogenesis, and sperm motility [5]. Two selenoproteins are required for normal spermatogenesis, the Se-dependent antioxidative enzyme phospholipid peroxide glutathione peroxidase (PHGPx) and selenoprotein P [3]. In the testes, Se occurs mainly in the PHGPx form. Thioredoxin reductase (TrxRs) is also present, notably in higher concentrations in maturing spermatids compared with mature semen. Selenoprotein V has also been detected in spermatic tubules, though its exact function has not been elucidated to date [3]. Kehr et al. used X-ray fluorescence microscopy (XFM) to visualize and quantify the tissue, cellular, and subcellular topography of Se. They demonstrated that Se is abundant in late spermatids due to increased levels of glutathione peroxidase 4 (GPX4), the levels depending on the supplies of Se by selenoprotein P (SELENOP) [6].
Se is a co-factor of antioxidative enzymes that are responsible for the neutralization, elimination, and prevention of the synthesis of ROS, which are produced during normal spermatogenesis, mitochondrial activity, and capacitation [6,7,8]. Excessive ROS production leads to oxidative damage in polyunsaturated acid (plasma membrane), nucleic acid (DNA structure), and mitochondrial dysfunction. PHGPx, together with catalase (CAT) and superoxide dismutase (SOD), exert a protective effect on the sperm. Moreover, selenoproteins in semen are involved in the maintenance of sperm structural integrity and chromatin organization [8].
Studies in humans
In a case-control study of 107 men with asthenozoospermia and 235 age-matched controls, a diet high in antioxidative agents, namely, vitamin E, vitamin D, vitamin C, zinc, folate, total fiber, polyunsaturated fatty acids, and Se, was associated with a lower risk of asthenozoospermia [9]. A major limitation was that the diet pattern was self-reported. A meta-analysis of observational studies investigating the effect of nutrients/nutritional supplements (omega-3 fatty acids and antioxidants, including Se and vitamins) on male infertility showed that some nutrients were associated with sperm quality [10]; however, no conclusion was explicitly drawn regarding Se intake.
A trial was conducted in men in the West of Scotland to determine whether a decrease in Se intake and Se status was contributing to male subfertility: 69 patients were recruited and received daily for 3 months placebo, Se alone, or Se together with vitamins A, C, and E [11]. An increase in sperm motility was observed in both of the Se-treated groups, while there was a non-significant decline in the placebo group. No effect of the additional vitamins was noted. The conclusion was that among subfertile men with low Se status, Se supplementation is capable of improving sperm motility, thus enhancing the potential for successful conception [11].
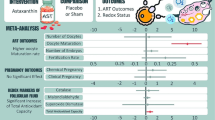
In an attempt to investigate the potential beneficial effects of Se supplementation on male fertility, Safarinejad et al. performed a randomized-controlled trial (RCT) on 468 men with idiopathic oligo-astheno-teratozoospermia, randomizing them to 200 μg Se per os daily (n = 116), 600 mg N-acetyl-cysteine per os daily (n = 118), 200 μg Se plus 600 mg N-acetyl-cysteine per os daily (n = 116), or placebo (n = 118). All three interventions had favorable outcomes in all semen parameters [12]. More recently, Lipovac et al. conducted a prospective, open-labeled, non-randomized study in which 156 infertile men received a mono-substance (500 mg l-carnitine, twice daily) and 143 a combined compound (440 mg l-carnitine, 250 mg l-arginine, 40 mg zinc, 120 mg vitamin E, 80 mg glutathione, 60 μg Se, 15 mg coenzyme Q10, 800 μg folic acid, once daily) [13]. An improvement in all semen concentration parameters (volume, concentration, morphology, and total progressive motility) was demonstrated after 3 months of treatment in both groups. Mirone et al. systematically reviewed the evidence of Se supplementation and sperm parameters, synthesizing nine interventional studies, three of which were RCTs [14]. Six of them reported a beneficial effect, two did not detect any effect, and only one reported a decrease in sperm motility. The latter was a small study of 11 healthy men (not infertile), and the supplementation dosage was 297 μg/d, the highest among all studies reviewed [15]. No meta-analysis of the studies was performed, likely due to the high degree of heterogeneity among them, regarding study type (double-blind and open-label RCTs, one-arm prospective studies, open-label prospective studies), sample size (n = 11 to 690), study population (infertile men, men with astheno-teratozoospermia or isolated asthenozoospermia, men with chronic prostatitis, and healthy men), and Se dosage (82.3–300 μg/d) [14]. Another newer meta-analysis of RCTs by Salas-Huetos et al. on the impact of various nutrients, dietary supplements, and food on sperm parameters included three RCTs involving Se supplementation that varied from 100 to 300 μg Se/d, after studies with a high risk of bias were excluded. Interestingly, beneficial effects of Se supplementation were demonstrated regarding sperm concentration [mean difference 3.91, 95% confidence intervals (CI) 3.08–4.73 spermatozoa/ml, p < 0.001], total motility (3.30, 95% CI 2.95–3.65%, p < 0.001), and morphology (1.87, 95% CI 1.50–2.24%, p < 0.001) [16].
In conclusion, evidence from both observational and interventional studies in men show a beneficial outcome of Se supplementation on sperm parameters in infertile men; thus, Se evaluation and supplementation could be considered when treating infertile men.
Selenium and female fertility
Pathophysiology
Many selenoproteins [iodothyronine deiodinase 3 (DIO3), TrxRs] are expressed in the uterus. Selenoprotein genes [GPX1, GPX2, GPX3, GPX4, selenoprotein S (SELENOS), selenoprotein H (SELENOH), and iodothyronine deiodinase 1 (DIO1) and DIO3] are detected in ovarian granulosa cells in experimental studies [4].
Oxidative stress seems to be a key player in female fertility, similarly to the male counterpart, with its role being crucial both during early pregnancy and the implantation window. At the beginning of pregnancy, trophoblasts, which form the outer layer of the blastocyst and play a major role in development and implantation, are exposed to hypoxic conditions. Se increases trophoblast migration and proliferation by reducing mitochondrial oxidative stress. Specifically, in hypoxia, Se-treated trophoblasts demonstrate increased viability, migration activity, and mitochondrial functional activity (ATP production and membrane potential) due to a decrease in ROS [17]. This finding is crucial as it shows that Se can regulate trophoblast migration, thus having a large impact on the ongoing pregnancy.
In another basic science study, Se supplementation for 8 weeks, in lymphocytes of women with PCOS who were candidates for IVF, increased gene expression of peroxisome proliferator-activated receptor gamma-γ (PPAR-γ) and glucose transporter (GLUT)-1 and decreased gene expression of low-density lipoprotein receptor (LDL-R), but did not influence lipoprotein(a) [Lp(a)] [18].
It has been suggested that Se is involved in oocyte growth, increasing the proliferation rate of theca and granulosa cells as well as that of follicles, blood vessels, and stromal tissues in ovine fetal ovaries [19]. These actions of Se were at least partly due to its repression of nitric oxide production. High Se intake through diet has been associated with decreased growth of primordial, secondary, and antral follicles, stroma, and blood vasculature in sheep fetus ovaries as compared with normal levels of Se intake [20]. In an attempt to identify Se distribution in the bovine ovary by X-ray fluorescence (XRF) imaging, Ceko et al. showed an upregulation of GPX1 and high Se concentrations in large (410 mm) healthy follicles, the latter being ten times higher than in the corpora lutea [21].
Conversely, Se deficiency has been associated with ovarian degeneration and follicle atresia in rats [22]. In another in vitro study in goat luteinized granulosa cells (LGCs), it was found that Se stimulated LGC proliferation and increased estradiol concentrations [23]. This study showed increased expression of cell proliferation pathway proteins, such as PCNA, cyclin-dependent kinase-1 (CDK1), phosphorylated adenosine monophosphate-activated protein kinase (p-AMPK; Thr172), and phosphorylated Akt (p-Akt; Ser473), as well as a decrease in the expression of p21 [23]. The estradiol production was paralleled by significantly enhanced expression of antioxidants (GPX1 and SOD2) and by steroidogenesis-related genes (3β-HSD and StAR) [23]. The increase of GPX and SOD2 are in accordance with the reported augmentation of Se and selenoproteins in large healthy follicles, where they are thought to be involved in vital antioxidant functions during later growth and the proliferation of follicles [4, 23].
Studies in humans
In humans, serum Se concentrations and GPX activity reach a trough in the early follicular phase and peak in the preovulation phase, followed by a reduction during the middle luteal phase [2]. These fluctuations in Se concentrations follow those of 17-estradiol during the menstruation cycle. However, not all studies show a clear association between Se concentrations and the phase of the cycle. In any case, the phases of the menstrual cycle should be considered when evaluating Se status in women of reproductive age.
Interestingly, low Se concentrations are reported in the serum and follicular fluid of women undergoing in vitro fertilization (IVF) or who have unexplained infertility [24]. Decreased Se-dependent GPX activity in follicular fluid was associated with no fertilization of the oocytes in women undergoing IVF [24]. The expression of GPX1 in cumulus cells [isolated from cumulus-oocyte complexes of oocytes of women undergoing IVF/intra-cytoplasmic sperm injection (ICSI) cycles] was elevated in oocytes, which led to a successful pregnancy, underlining the importance of Se as regards follicle size and quality [25].
Excessive ROS generation [as seen in endometriosis or polycystic ovary syndrome (PCOS)] may cause increased expenditure of Se. Indeed, a higher pregnancy rate was recorded in women with PCOS under Se supplementation in Iran [26]. Both Se supplementation per os and sodium selenite addition to the culture medium have been associated with favorable reproductive outcomes after ART in humans and mammals, respectively [4]. A case-control study of 98 infertile women and 43 controls positively associated concentrations of mercury and infertility, after adjusting for Se levels and age [27]. Overall, methylmercury and Se exposures seem to have an antagonistic (harmful and protective, respectively) impact on female fertility. According to a Cochrane Review on the effect of antioxidants (N-acetyl-cysteine, melatonin, l-arginine, myo-inositol, d-chiro-inositol, carnitine, Se, vitamin E, vitamin B complex, vitamin C, vitamin D and calcium, CoQ10, pentoxifylline, and omega-3-polyunsaturated fatty acids) in female subfertility, there is low-quality evidence that antioxidants are beneficial for infertile women [28]. The review included 50 RCTs involving 6510 women; insufficient evidence was gathered regarding possible adverse events [28]. Among all antioxidants, combinations and CoQ10 were associated with an increased clinical pregnancy rate, whereas this was not the case for melatonin, l-arginine, myo-inositol, or vitamin B complex.
In conclusion, evaluation of Se concentrations in women should always be followed by consideration of the phases of the menstrual cycle. Se concentrations in the follicular fluid have been suggested as a marker of infertility/unexplained infertility; however, the evidence is limited, based on small studies with probably a large degree of bias. In any case, Se supplementation (per os/addition to the culture medium) has been shown to be beneficial as concerns reproductive outcomes after ART.
Unexplained infertility
With regard to unexplained infertility, the evidence to date on its association with Se remains limited. In one study, lower Se concentrations were reported in the follicular fluid of women with unexplained infertility (0.44, 95% CI 0.41–0.51 μmol/l), compared with women who were infertile due to other causes (tubal factor 0.51, 95% 0.46–0.54 μmol/l and male factor 0.51, 95% CI 0.46–0.53 μmol/l, p = 0.002 and p = 0.01, respectively) [24]. In another study, increased concentrations of Se-binding protein-1 (SBP1) were reported in women with idiopathic infertility and premature ovarian failure (POI) [29].
Conclusion
Mitigation of oxidative stress, which is involved in both male and female infertility, would seem to constitute the primary pathway by which Se could positively affect fertility. However, the antioxidant capacity of Se does not appear to be the only way in which it influences male and female fertility. Though the mechanisms have not as yet been fully elucidated, it is likely that Se also has a positive effect on growth, maturation, and replication of oocytes.
Given that it is not thus far clear which tissue sample (blood, serum, seminal plasma, sperm, or follicular fluid) renders the most accurate picture of Se concentration in terms of its role in reproduction, there is still insufficient evidence to recommend routine assessment of Se status in men and women seeking fertility. Furthermore, there is limited evidence on the association between serum Se and in reproductive tissues Se concentrations.
Of particular interest would be investigations into whether levels of SELENOP, which functions as a transport and storage protein, may constitute a reliable bioindicator in infertility. Nevertheless, the existing evidence, despite being of limited quantity and somewhat low quality, suggests that Se supplementation (< 200 μg/d) is possibly beneficial in men through its improvement of sperm motility.
References
Duntas LH, Benvenga S (2015) Selenium: an element for life. Endocrine 48:756–775
Pieczyńska J, Grajeta J (2015) The role of selenium in human conception and pregnancy. Trace Elem Med Biol 29:31–38
Rayman MP (2004) The use of high-selenium yeast to raise selenium status: how does it measure up? Br J Nutr 92:557–573
Qazi IH, Angel C, Yang H, Pan B, Zoidis E, Zeng CJ, Han H, Zhou GB (2018) Selenium, selenoproteins, and female reproduction: a review. Molecules 23(12):E3053
Agarwal A, Durairajanayagam D, du Plessis SS (2014) Utility of antioxidants during assisted reproductive techniques: an evidence based review. Reprod Biol Endocrinol 12:112
Kehr S, Malinouski M, Finney L, Vogt S, Labunskyy VM, Kasaikina MV, Carlson BA, Zhou Y, Hatfield DL, Gladyshev VN (2009) X-ray fluorescence microscopy reveals the role of selenium in spermatogenesis. J Mol Biol 389:808–818
Aitken RJ (1995) Free radicals, lipid peroxidation and sperm function. Reprod Fertil Dev 7:659–668. https://doi.org/10.1071/RD9950659
Vessey W, Perez-Miranda A, Macfarquhar R, Agarwal A, Homa S (2014) Reactive oxygen species in human semen: validation and qualification of a chemiluminescence assay. Fertil Steril 102:1576–1583.e4
Eslamian G, Amirjannati N, Rashidkhani B, Sadeghi MR, Hekmatdoost A 2017 Nutrient patterns and asthenozoospermia: a case-control study. Andrologia 49.
Salas-huetos A, Bulló M, Salas-Salvadó J (2017) Dietary patterns, foods and nutrients in male fertility parameters and fecundability: a systematic review of observational studies. Hum Reprod Update 23:371–389
Scott R, Macpherson A, Yates RW, Hussain B, Dixon J (1998) The effect of oral selenium supplementation on human sperm motility. Br J Urol 82:76–80
Safarinejad MR, Safarinejad S (2009) Efficacy of selenium and/or N-acetyl-cysteine for improving semen parameters in infertile men: a double-blind, placebo controlled, randomized study. J Urol 181:741–751
Lipovac M, Bodner F, Imhof M, Chedraui P (2016) Comparison of the effect of a combination of eight micronutrients versus a standard mono preparation on sperm parameters. Reprod Biol Endocrinol 14:84
Mirone M, Giannetta E, Isidori AM (2013) Selenium and reproductive function A systematic review. J Endocrinol Investig 36:28–36
Hawkes WC, Turek PJ (2001) Effects of dietary selenium on sperm motility in healthy men. J Androl 22:764–772
Salas-Huetos A, Rosique-Esteban N, Becerra-Tomás N, Vizmanos B, Bulló M, Salas-Salvadó J (2018) The effect of nutrients and dietary supplements on sperm quality parameters: a systematic review and meta-analysis of randomized clinical trials. Adv Nutr 9:833–848
Na JY, Seok J, Park S, Kim JS, Kim GJ Effects of selenium on the survival and invasion of trophoblasts. Clin Exp Reprod Med. 45:10-16.
Zadeh Modarres S, Heidar Z, Foroozanfard F, Rahmati Z, Aghadavod E, Asemi Z (2018) The effects of selenium supplementation on gene expression related to insulin and lipid in infertile polycystic ovary syndrome women candidate for in vitro fertilization: a randomized, double-blind, placebo-controlled trial. Biol Trace Elem Res 183:218–225
Grazul-Bilska AT, Caton JS, Arndt W, Burchill K, Thorson C, Borowczyk E, Bilski JJ, Redmer DA, Reynolds LP, Vonnahme KA (2009) Cellular proliferation and vascularization in ovine fetal ovaries: effects of undernutrition and selenium in maternal diet. Reproduction. 137:699–707
Grazul-Bilska AT, Vonnahme KA, Bilski JJ, Borowczyk E, Soni D, Mikkelson B, Johnson ML, Reynolds LP, Redmer DA, Caton JS (2011) Expression of gap junctional connexin proteins in ovine fetal ovaries: effects of maternal diet. Domest Anim Endocrinol 41:185–194
Ceko MJ, Hummitzsch K, Hatzirodos N, Bonner WM, Aitken JB, Russell DL, Lane M, Rodgers RJ, Harris HH (2015) X-Ray fluorescence imaging and other analyses identify selenium and GPX1 as important in female reproductive function. Metallomics 7:71–82
Grabek M, Swies Z, Borzecki A (1991) The influence of selenium on the reproduction of rats. Ann Univ Mariae Curie Sklodowska Med 46:103–105
Yao X, Ei-Samahy MA, Fan L, Zheng L, Jin Y, Pang J, Zhang G, Liu Z, Wang F (2018) In vitro influence of selenium on the proliferation of and steroidogenesis in goat luteinized granulosa cells. Theriogenology. 114:70–80
Paszkowski T, Traub AI, Robinson SY, McMaster D (1995) Selenium dependent glutathione peroxidase activity in human follicular fluid. Clin Chim Acta 236:173–180
Singh AK, Chattopadhyay R, Chakravarty B, Chaudhury K (2013) Markers of oxidative stress in follicular fluid of women with endometriosis and tubal infertility undergoing IVF. Reprod Toxicol 42C:116–124
Razavi M, Jamilian M, Kashan ZF, Heidar Z, Mohseni M, Ghandi Y, Bagherian T, Asemi Z (2016) Selenium supplementation and the effects on reproductive outcomes, biomarkers of inflammation, and oxidative stress in women with polycystic ovary syndrome. Horm Metab Res 48:185–190
Maeda E, Murata K, Kumazawa Y, Sato W, Shirasawa H, Iwasawa T, Izumo K, Tatsuta N, Sakamoto M, Terada Y (2019) Associations of environmental exposures to methylmercury and selenium with female infertility: a case - control study. Environ Res 168:357–363
Showell MG, Mackenzie-Proctor R, Jordan V, Hart RJ (2017) Antioxidants for female subfertility. Cochrane Database Syst Rev 7:CD007807
Yu-Rice Y, Edassery SL, Urban N, Hellstrom I, Hellstrom KE, Deng Y, Li Y, Luborsky JL (2017) Selenium-Binding Protein 1 (SBP1) autoantibodies in ovarian disorders and ovarian cancer. Reproduction 153:277–284
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mintziori, G., Mousiolis, A., Duntas, L.H. et al. Evidence for a manifold role of selenium in infertility. Hormones 19, 55–59 (2020). https://doi.org/10.1007/s42000-019-00140-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42000-019-00140-6