
Abstract
Objectives
Atypical executive functions (EF) have long been observed in individuals with autism spectrum disorders (ASD) of any age. To compensate for EF-related difficulties and to cope with the demands of daily life, assistive technology for cognition may represent a valid solution, but at present, no information is available on the range of accessible solutions nor on their effectiveness in ASD. This paper reports on a review conducted to identify assistive technologies that may compensate for EF-related difficulties in ASD.
Methods
A systematic search was conducted following the PRISMA Extension for Scoping Reviews (PRISMA-ScR) reporting guideline recommendations.
Results
Fifteen studies met inclusion criteria, with most studies following a single-subject research design (n = 11). The assistive technologies identified were grouped into two categories (context-aware, mobile) addressing four EF-related cognitive processes classified according to the taxonomy proposed by the International Classification of Functioning (i.e., organization and planning, time management, cognitive flexibility, and insight). Insight (e.g., self-monitoring) resulted as the only intervention that may be considered evidence-based.
Conclusions
This review highlights that assistive technology may be effective in compensating for specific EF-related difficulties in ASD, but more rigorous research involving (a) a wider range of EF-related skills, (b) older participants, and (c) diverse settings (e.g., workplaces) is necessary.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Many individuals diagnosed with autism spectrum disorders (ASD) struggle with independence and coping with the demands of daily life due to atypical executive-functions skills (hereafter, EF; Abbott et al. 2018; Kenny et al. 2018; Kenworthy et al. 2008; Wallace et al. 2016). EF are higher cognitive processes that allow planning, control, and monitoring of goal-directed behavior and are involved in various aspects of everyday life such as adaptive skills, self-regulation of emotions, and social interactions (Dawson and Guare 2018; Jurado and Rosselli 2007; Mazefsky et al. 2012).
Atypical EF skills have long been observed in ASD across all ages (for a recent review and meta-analysis see Demetriou et al. 2018a; see also Velikonja et al. 2019). Although current evidence suggests that EF differences in people with ASD compared with the typical population do not reflect a diagnostic feature of ASD (Geurts et al. 2014; de Vries and Geurts 2015), EF are increasingly considered an important target for interventions to make people with ASD more resilient to the negative consequences of being on the autism spectrum and improve overall function and independence (Fletcher-Watson and Happé 2019; Leung et al. 2016; Wallace et al. 2016).
Components of EF interventions targeting ASD include teaching EF skills (i.e., treatments) and environmental modifications (Dawson and Guare 2018). Treatment interventions focusing on specific EF cognitive domains (e.g., working memory) to improve adaptive functioning, however, have produced mixed results (for a review see Wallace et al. 2016), likely due to high attrition rates and lack of generalizability of domain-specific gains to other cognitive or behavioral domains (Van Steenburgh et al. 2017; de Vries et al. 2015). Moreover, current evidence suggests that EF atypicalities in ASD may reflect an overall and non-fractionated impairment of cognitive control functions (Demetriou et al. 2018a), suggesting that more comprehensive interventions are warranted to achieve greater independence for people with ASD (Kirk et al. 2015). In this view, along with cognitive-based interventions, the use of compensatory strategies that change the environment to facilitate task performance may increase the overall effectiveness of treatments aimed at promoting the autonomy and participation of individuals with ASD (Kenworthy et al. 2014a, b).
Assistive technologies for cognition (ATC) refers to technologies that “can be used to enable, enhance, or extend cognitive function” (O’Neill and Gillespie 2014, p. 1; for similar constructs see also Cole 1999; Lopresti et al. 2004; Scherer et al. 2005; Wehmeyer and Shogren 2013) and include tools that are primarily aimed at supporting individuals with cognitive disabilities to promote independent action and social participation (Best et al. 2014; Cole 1999; O’Neill and Gillespie 2014). ATC have been applied to cope with impairments in a variety of cognitive domains such as memory (e.g., notebooks, voice recorders), language and social interaction (e.g., augmentative and alternative communication), reading and learning (e.g., text-to-speech devices, concept maps), way finding, spatial orientation, and navigation (e.g., GPS; for a review see O’Neill and Gillespie 2014).
More specifically, ATC used to compensate for EF-related difficulties have been applied to a range of cognitive impairments including poor working memory, poor time management, difficulties in planning, goal maintenance, and organization, and poor initiation (Schwartz 2014). For instance, Evans et al. (1998) reported on the use of a digital reminder that enabled a patient with EF deficits to autonomously initiate a daily task (e.g., watering houseplants) and sustain her attention to that task once initiated through continuous loud beeping and vibrations. Micro-prompting is also a common strategy to guide individuals with EF deficits through a task that has several steps (O’Neill et al. 2018). To this end, external devices that provide timely audio/video prompts have proven useful in supporting patients with cognitive impairments in a variety of daily activities such as hand-washing or cooking a meal (e.g., Mihailidis et al. 2008; for a review see Gillespie et al. 2012).
As already highlighted by Bouck (2010), technology can be broken down into low, moderate, and high technologies. Low technology includes all non-digital artifacts that may help thinking and remembering (e.g., written notes); moderate technology encompasses devices that have electronic components but are not computerized (e.g., calculators), while high technology includes computerized devices such as personal computers, smartphones or smartwatches, tablets, and robots. All these solutions can be used to compensate for the same cognitive impairment (e.g., memory), but in certain situations, high technology is considered more effective than low technology-based strategies as, for instance, one may forget to check a written note while a high-tech device can send an automatic prompt at a relevant time to remind about an event (Jamieson et al. 2017).
To date, there has been little consensus on the definition of EF, nor on the cognitive processes that should be included within this construct (Friedman and Miyake 2017). The International Classification of Functioning, Disability and Health (ICF; World Health Organization 2001) defines EF as specific mental functions especially dependent on the frontal lobes of the brain, including goal-directed behaviors such as abstract thinking, organization of ideas, time management, executing plans, mental flexibility, and deciding which behaviors are appropriate and under what circumstances (see Table 1 for a complete list of the ICF components related to EF processes as well as examples of abilities compensated for by ATC). Given the breadth and depth of the cognitive processes included in the ICF definition, for the scope of the present study, we focused only on four components of executive functioning, namely organization and planning, time management, cognitive flexibility, and insight (see Table 1 for definitions of each component). Together, these components embrace those higher-level EF-related cognitive processes that are widely considered most significantly related to adaptive capabilities (Demetriou et al. 2018b), and those in which individuals with ASD are expected to show an impairment when compared with typical populations (Wallace et al. 2016).
Existing reviews have already focused on ATC effectiveness to support training in skills which are mediated by EF-related cognitive processes, including communication (Logan et al. 2017), social skills (Wass and Porayska-Pomsta 2014), self-management (Chia et al. 2018), learning skills (Den Brok and Sterkenburg 2015), and vocational abilities (Odom et al. 2015; Smith et al. 2017; Walsh et al. 2017). However, the extent to which ATC may be primarily used to compensate for EF-related difficulties in ASD has not been systematically explored. In this view, the present review not only represents an update of the available evidence on important EF-related skills (e.g., insight (self-management); Chia et al. 2018), but it also proposes a systematic conceptualization of ATC interventions in terms of the EF-related cognitive processes being compensated (Gillespie et al. 2012).
The objectives of the present review were thus to (a) identify the range of computerized ATC that have been used to compensate for EF-related difficulties in individuals with ASD of any age, as conceptualized by the ICF taxonomy, and (b) gain an overall view of the effectiveness of such ATC for this population. Specifically, the paper (a) explores the use of ATC to compensate for EF atypicalities in individuals with ASD, and (b) identifies gaps in the existing databases so as to stimulate future research efforts aimed at developing additional effective applications of ATC in the interventions targeting EF-related skills in persons with ASD.
Method
A systematic search was conducted following the PRISMA Extension for Scoping Reviews (PRISMA-ScR) reporting guideline recommendations (Tricco et al. 2018) to identify empirical studies that used ATC solutions to compensate for EF-related difficulties in individuals with ASD. A scoping review approach was used as our primary aim was to examine how research is conducted on ATC in compensating for EF-related difficulties and identifying knowledge gaps. This study may be thus considered a precursor of a systematic review in which detailed statements to guide decision-making can be produced (Munn et al. 2018). The identified studies that met pre-determined inclusion criteria were then coded in terms of (a) participants (e.g., age, gender, sample size, and diagnosis), (b) setting (e.g., school, home, or community setting), (c) type of technology used, (d) training duration, (e) EF skill(s) addressed with the technology, (f) study design, and (g) outcomes of the intervention.
Search Strategy
We knew from previous searches that we were at risk of including few papers. We therefore extended the search to multiple databases using broad search terms. More specifically, we searched the following academic databases: MEDLINE, consulted through the free electronic access PubMed; PsycINFO; ERIC; CINAHL, consulted through EBSCOHost; and Web of Science. During this process, we used the same free-text terms for all databases: autism, ASD, autism spectrum disorder, pervasive developmental disorder, cognitive aid, assistive technology, assistive device, and cognitive prosthetics. The search terms were combined by means of Boolean logical operators (“and”, “or”) in order to reduce the number of non-pertinent results. The search was limited to English-language, peer-reviewed journals published between January 2010 and January 2019. This starting date (i.e., January 2010) was chosen as it represents the year when most of the currently used computerized ATC (e.g., touch-screen devices) were first introduced on the market (Stephenson and Limbrick 2015).
After removal of duplicates, the titles and abstracts of the remaining studies were assessed for suitability for further review by two independent researchers using the following inclusion criteria: (a) the study had to focus on ASD or previously recognized subtypes such as autism, Asperger’s syndrome (AS), or a not-otherwise-specified pervasive developmental disorder; (b) the study had to report on the implementation or use of at least one computerized ATC (mobile, desktop, wearable, virtual/augmented reality, robotics); (c) the technology was used to provide ongoing support to an individual who is completing a task by compensating for one or more EF skills (see Table 1); and (d) use of experimental design.
Exclusion criteria were the following : (a) studies employing computer-based technologies to enhance cognitive performance (i.e., cognitive training; Wass and Porayska-Pomsta 2014); (b) studies primarily aimed at teaching EF-related skills (e.g., self-monitoring) in which the technology is no longer used once the skill is acquired (e.g., Finn et al. 2015); (c) studies using technology for language or (multi-step) communication (e.g., AAC, sign language) or video modeling; (d) studies reporting the assessment of EF skills needed to operate assistive devices or ATC; and (e) reviews of literature (e.g., systematic reviews and meta-analyses), editorials, or book chapters.
Inter-Rater Agreement
Two independent raters were involved in the inter-rater agreement process. Proportional agreement on the eligibility stage (“yes” or “no”) was calculated by taking the number of agreements and dividing this by the number of agreements plus disagreements, multiplied by 100. This procedure yielded an agreement of 88%. Analysis of the records that were differently rated by the two researchers revealed that all disagreements resulted from differential interpretation of the cognitive skills addressed by the studies. After consensus building, agreement reached 100%.
Quality of Evidence
Though we did not limit our research to a specific research design (e.g., single-case studies, group-design studies), we however expected single-case research designs (SCD) to be the most represented approaches. Accordingly, we used the What Works Clearinghouse (WWC) standards (Institute of Education Sciences 2017) to assess the quality of the literature retrieved against two criteria: (1) methodological rigor and (2) replicability of the effects.
Methodological Rigor
The WWC standards categorized studies as meets standards without reservations, meets standards with reservations, or does not meet standards. To meet standards with or without reservation, studies had to meet the following criteria: (a) the researcher systematically manipulated the independent variable and decided when and how independent variable conditions changed; (b) each outcome was measured over time by more than one assessor, with inter-assessor agreement collected during each phase and at 20% of data points in each condition and that meets minimal thresholds; (c) the study had to have the minimum number of phases (i.e., multiple baseline designs require at least six phases, and withdrawal designs require at least four phases) and data points per phase as required for the different research designs. The number of data points per phase was used to differentiate studies that met standards without reservations (i.e., at least five data points per phase) from those that met standards with reservations (i.e., at least three data points per phase).
Replicability of the Effects
The WWC standards recommend that interventions under review may be considered evidence-based if at least (a) a minimum of five SCD studies examining the same intervention meet the standards either with or without reservation; (b) the studies are conducted by at least three different research teams with no overlapping authorship at three different institutions; and (c) the combined number of participants totals at least n = 20. This 5-3-20 threshold was applied to SCD studies grouped according to (1) types of technology used, and (2) ICF components addressed (as listed in Table 1).
Results
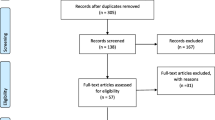
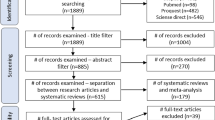
The search and selection process resulted in the inclusion of 15 studies in this review (Fig. 1). The included studies were published between the years 2010 and 2019 and were conducted primarily in the USA (n = 12; 80%). Summaries of each of the studies are presented in Table 2.

Flow diagram of the literature search
Participants, Settings, and Experimental Designs
There was a total of 117 participants diagnosed with ASD across the 15 studies, 20% females (n = 23). The majority of the studies included participants in the age range between 11 and 17 (n = 8; 53%), 33% (n = 5) included participants over 18 years old, and two studies included a sample of children aged below 10 years. Most of the studies (n = 10; 66%) involved participants without intellectual disabilities, and nearly half of the studies reported scores from formal IQ assessments (Bouck et al. 2014; Bouck et al. 2017; Cihak et al. 2010; Crutchfield et al. 2015; Cullen et al. 2017; Fage et al. 2018; Palmen et al. 2012; Xin et al. 2017). Most of the studies (n = 8) took place in school settings, two at participants’ homes, two in work-related settings, one within the community (market), one in a clinic, and one in a mixed setting (i.e., home and school). The majority of the studies followed a single-subject research design (n = 11). Details on the designs used are included in Table 2. Of the four studies employing a group design, one was a randomized control trial (Gentry et al. 2015).
Uses of Technology
Overall, the studies targeted 18 ICF components. Two studies addressed more than one component with a device (Bimbrahw et al. 2012; Gentry et al. 2015). Insight was the most addressed EF with 10 occurrences, followed by organization and planning (n = 4), time management (n = 3), and cognitive flexibility (n = 1). The devices used to compensate for EF difficulties can be grouped according to two technology types: context-aware (n = 1) and mobile (n = 14).
Context-Aware Technology
Context-aware technologies refer to devices able to determine the state of the users in their environments. Bimbrahw et al. (2012) used the COACH (Cognitive Orthosis for Assisting aCtivities in the Home) system to monitor the hand-washing activities of five children with ASD and to automatically prompt them whenever they interrupted the correct sequence of steps necessary to complete the activity. Therefore, COACH was classified as a multifunctional system supporting time management (i.e., task initiation), insight (i.e., self-monitoring of activities), and organization and planning (i.e., providing step-by-step instructions to complete the task). The acceptability of the system by children and their parents resulted as good, but the reliability of COACH was not fully satisfactory (Bimbrahw et al. 2012).
Mobile Technology
Devices in this category included personal digital assistants (PDA; Cihak et al. 2010; Gentry et al. 2010), iPods (Gentry et al. 2015; Palmen et al. 2012), iPads (Bouck et al. 2014; Bouck et al. 2017; Cullen et al. 2017; Fage et al. 2018; Hampshire & Allred, 2018; Xin et al. 2017), and android-based tablets (Clemons et al. 2016; Crutchfield et al. 2015; Huffman et al. 2019; Rosenbloom et al. 2016). Mobile devices were mostly used to support insight, namely to help students self-monitor their attention-related behaviors (i.e., being on task; Bouck et al. 2014; Bouck et al. 2017; Cihak et al. 2010; Clemons et al. 2016; Crutchfield et al. 2015; Hampshire & Allred, 2018; Huffman et al. 2019; Rosembloom et al., 2015; Xin et al. 2017). For instance, the app I-Connect (Clemons et al. 2016; Crutchfield et al. 2015; Huffman et al. 2019; Rosembloom et al., 2015) was used to cue students’ self-monitoring processes on a fixed interval schedule (e.g., every 30 s) by asking them to answer a question (“are you on task?”) appearing on the touchscreen while engaged in the academic activities. Overall, the results were positive in terms of increased rates of task completion and engagement, with encouraging results also for the use of self-monitoring devices to reduce inappropriate and stereotypic behaviors (Crutchfield et al. 2015; Huffman et al. 2019; Rosembloom et al., 2015).
Mobile technology was also used to address organization and planning (Cullen et al. 2017; Fage et al. 2018). Cullen et al. (2017) used self-directed video prompting on iPads with a young adult on the autism spectrum, showing that this technology had a positive effect on the percentage of vocational task steps completed accurately when compared with usual job coaching. Importantly, use of an iPad successfully generalized to other job-related materials (Cullen et al. 2017). Fage et al. (2018) developed and tested a package of apps (“School+”) on mobile tablets to promote school inclusion of children with ASD in secondary school settings. The package included both compensatory and cognitive training apps. The compensatory apps were specifically designed to address difficulties in planning and executing by providing guidance on daily routines such as going to the classroom, entering the classroom, getting out school supplies, taking notes, and leaving the classroom. Overall, the results showed significant improvements in terms of socio-cognitive functioning, behavior adaptation, and social response, although it is not possible to disentangle the effects of compensatory from training applications.
Time management and cognitive flexibility were addressed using a mobile device by Gentry et al. (2010) and Palmen et al. (2012) respectively. Gentry et al. (2010) trained a sample of adolescents and young adults to use a PDA as a task management tool (i.e., setting reminders and using a digital calendar). Eight weeks after training, participants self-reported improvements in their independence as well as satisfaction in performing functional activities.
Palmen et al. (2012) trained a sample of four adolescents without intellectual disability on the use of an iPod to facilitate transitioning between daily tasks and activities at a daily treatment facility. The iPod resulted effective in supporting independent transitions between activities compared with baseline. However, when no intervention was in effect, the participants still needed prompts from staff to use their device, thus showing some difficulties in independently using their ATC (Palmen et al. 2012).
While the majority of studies including mobile devices focused on a limited range of EF-related difficulties, Gentry et al. (2015) reported on a delayed randomized control trial to assess the effectiveness of an iPod-based set of applications to support a variety of adult cognitive skills (i.e., prospective memory, organization, planning) for vocational purposes. The applications included task reminders, task lists, video-based task-sequencing prompts, behavioral self-management adaptations, and way-finding tools. The results showed positive outcomes in terms of fewer hours of job-coaching support (Gentry et al. 2015), further underpinning the idea that mobile devices may indeed stand as a flexible and easy-to-use support for EF-related difficulties.
Technology Training
Seven studies provided information on the duration of the training needed to correctly operate the device. All were studies employing mobile devices. Duration ranged from a minimum of one 15-min training session (Crutchfield et al. 2015) to about 240 min over four training sessions (Gentry et al. 2015).
Quality of Evidence
Of the SCD studies assessed for methodological rigor (n = 11), eight met the standards without reservations, two with reservations, and one did not meet the standards (see Table 2). Combined research grouping studies employing mobile devices exceeded the replication threshold (5-3-20) for evidence-based practice, with a result ratio of 10-7-25. Regarding types of ICF components addressed, the replication threshold was satisfied only by insight, with a result ratio of 8-5-20.
Considerations on EF
The included studies were also inspected to assess whether the authors made explicit reference to specific EF-related skills as the target of their technology-based interventions or, more in general, recognized that their interventions might potentially address the EF-related vulnerabilities of individuals with ASD. Gentry et al. (2010) refer to the notion of “executive dysfunction” for which students with ASD may forget to refer to their schedules. Accordingly, their results are interpreted as evidence of the fact that such executive dysfunctions may be compensated for by learning to operate a mobile cognitive support such as a mobile device (Gentry et al. 2010; see also Gentry et al. 2015, for a similar discussion involving adults).
Fage et al. (2018) recognize that students with ASD might exhibit the executive functioning disorders (activity planning, time management, inhibition, flexibility) for which their compensatory apps were specifically developed. The authors thus interpret the efficacy of their intervention as the result of an effective combination between compensatory in situ assistance of executive (dys)functioning and rehabilitation interventions (Fage et al. 2018). Lastly, Huffman et al. (2019) were the only ones to report on assessment of the EF abilities of the participant involved. The researchers used the Behavior Rating Inventory of Executive Function (BRIEF), a proxy- or self-reported questionnaire that can be used to assess EF in both children and adults (Gioia et al. 2000). In this study, results from the BRIEF assessment showed that the participant needed support in areas such as inhibition, self-monitoring, and task-monitoring, thus providing robust support to the target of the intervention (Huffman et al. 2019).
Discussion
Through this review, we attempted to highlight the breadth of technology-based compensatory interventions (i.e., ATC) to support EF-related difficulties in persons with ASD. Current accounts of ASD (John et al. 2018; Valeri et al. 2019; for similar considerations regarding other neurodevelopmental disorders, see also Bertelli et al. 2018; Henry and Bettenay 2010) support the notion that assessment of EF-related skills is highly relevant for the understanding of the person’s ability to manage environmental demands, in certain cases even more so than assessment of a more global intellectual functioning alone (e.g., IQ; Bertelli et al. 2018). Accordingly, our assumption was that clinicians may benefit from evidence-based knowledge that helps them in linking results from their assessments of specific cognitive functions with reliable interventions aimed at fostering adaptive behaviors in ASD individuals of any age. Overall, the results from the current search of the literature show a paucity of literature in this respect, thus suggesting that the potential of ATC in compensating for EF-related difficulties in ASD is rather under-investigated. Despite limited evidence, however, a number of considerations stemming from the present findings may be put forward.
Firstly, from the results of the present review, it emerges that there is reliable evidence on the effectiveness of ATC in supporting higher-level functions related to the insight component of the ICF (i.e., meta-cognitive processes), and in particular self-monitoring, for improving task completion and performance. This result is not surprising given the amount of research on technology-based self-management interventions targeting autism (for a relevant review, see Chia et al. 2018), and is consistent with wider evidence on the benefits of interventions that provide typically and atypically developing children with strategies of self-regulation (e.g., goal setting, self-instruction, self-evaluation; for relevant reviews, see Bruhn et al. 2015; Takacs and Kassai 2019). Technology-based self-monitoring, in particular, refers to the use of electronic devices to analyze one’s own behavior (Bruhn et al. 2016). The available literature emphasizes the added value of employing technology-based self-monitoring interventions compared with traditional ones (e.g., paper and pencil methods) as the former may allow for (a) timely prompting, (b) more precise recording of target behaviors, and (c) better efficiency in collecting and analyzing data (Bruhn and Wills 2018). As emerged in the current paper, technology-based self-monitoring resulted effective not only to promote on-task behaviors but also to reduce inappropriate and stereotypic behaviors (Rosenbloom et al. 2016). As such, this intervention represents a relatively affordable strategy to deliver concurrent interventions. A matter of further inquiry, however, is related to the effectiveness of such concurrent interventions in other settings other than primary education, such as workplaces.
Secondly, the majority of participants in the studies included in this review were between 11 and 17 years old, suggesting that young adults and adults are under-represented in the available literature on ATC for EF supports. It is recognized that, due to developmental maturity and/or increased use of compensatory strategies, adults with ASD perform better in EF than younger age groups do (Demetriou et al. 2018a). As such, it is reasonable that research is mainly focused on compensating for EF-related difficulties in school-aged populations. However, there is general agreement that EF is an under-investigated construct in adulthood (Brady et al. 2017; Kiep and Spek 2017), an age in which individuals with ASD and without cognitive and language impairments may actively contribute in community life (e.g., Frank et al. 2018). Planning skills and cognitive flexibility, in particular, are widely considered the EF sub-components in which adults with ASD who have IQs in the average range are expected to show reduced performance compared with typical populations (Wallace et al. 2016). Such EF-related difficulties may represent one of the main factors, together with social difficulties, negatively affecting access to and maintenance of employment (Frank et al. 2018). The study by Gentry et al. (2015) on the use of a mobile support in vocational settings suggests that providing ATC in compensating for EF-related skills may be an effective strategy to allow individuals with ASD to successfully transition into employment. More research is however needed on this topic to understand what (personal and environmental) factors may facilitate or hinder the adoption and use of ATC in workplaces.
Thirdly, the female-to-male ratio found in our review (i.e., 1:5) mirrors available estimates reported in the ASD literature (e.g., Rivet and Matson 2011), with an even lower female-to-male ratio (1:10) for those with a diagnosis of autism without intellectual disabilities (Dworzynski et al. 2012). Irrespective of whether such gender-related differences in prevalence of ASD diagnoses are due to, for instance, autism as an extreme of the male brain characteristics (Baron-Cohen 2002), biological factors (e.g., Ferri et al. 2018), or girls’ and women’s better abilities in camouflaging their difficulties (Dean et al. 2017), robust evidence exists on weaker EF-related abilities and adaptive skills in girls and women when compared with men (White et al. 2017). It can be thus argued that girls and women are the subjects who would benefit more from ATC support, even if at present, there is no evidence of possible gender-related differences in technology needs and applications. An additional aspect that deserves further consideration is whether differences between males and females in technology acceptance and use often observed in the general population (e.g., Cai et al. 2017) also occur in ASD.
Fourthly, only one of the studies included in this review assessed the participants’ EF (Huffman et al. 2019). BRIEF may be of immediate practical utility for both clinicians and educators as it allows identification of problems related to a wide variety of EF skills that have implications for adaptive functioning in everyday activities. The results obtained could thus be used to guide professionals in matching a user with the available ATC. For instance, Huffman et al. (2019) used BRIEF to document that the participant included in the study showed difficulties related to self-monitoring, for which the I-Connect app could stand as a valid support.
Fifthly, and differently from the available reviews, the present paper was primarily focused on the use of ATC as a compensatory strategy. Indeed, the use of computerized technologies to increase the effectiveness of interventions targeting children and adults with ASD is a well-established field of research, and a number of influential systematic reviews have been published that report on a broader number of studies and devices compared with those included here (Aresti-Bartolome and Garcia-Zapirain 2014; Chia et al. 2018; Den Brok and Sterkenburg 2015; Grynszpan et al. 2014; Kagohara et al. 2013; Logan et al. 2017; Odom et al. 2015; Smith et al. 2017; Walsh et al. 2017; Wass and Porayska-Pomsta 2014). The majority of the available evidence, however, is mainly concerned with using technology to improve the effectiveness of training or teaching interventions (e.g., shopping; Burckley et al. 2015) in which the device is no longer used once the skill is acquired and generalized to other similar contexts. In such studies, a variety of technological solutions were employed, including, for instance, virtual reality (Bradley and Newbutt 2018), social robotics (Pennisi et al. 2016), or wearable technologies (Koumpouros and Kafazis 2019). In contrast, our paper was specifically focused on compensatory interventions in which it is expected that the device is used any time the subject performs the target activity. In this view, our results suggest that research on the use of ATC to compensate for EF-related difficulties in individuals with ASD lags well behind the available research on the use of technology to train their cognitive and social skills. It is thus important that future research addresses this evident gap by focusing on the link between specific EF processes and ASD individuals’ adaptive behaviors, with a view to identifying which ATC is most effective in promoting independent participation in a variety of contexts (e.g., education, employment).
Limitations and Future Research
Two main limitations must be taken into account when interpreting the present findings. First, only a few studies among those included in the present review made explicit reference to EF-related difficulties as the target of their interventions employing ATC (i.e., Fage et al. 2018; Gentry et al. 2010, 2015; Huffman et al. 2019). It may thus be argued that the majority of included papers did not directly address EF in their proposed interventions. While we recognize this as a potential limit of our paper, it should also be highlighted that the use of ICF constructs and related definitions (see Table 1) was instrumental in linking assumed cognitive processes to observable behaviors directly or partly related to EF skills, as already done by similar investigations (see e.g., Gillespie et al. 2012). In this view, the current results may be illustrative of the potential use of ATC to support EF-related difficulties. Future research may learn from the available recent studies in which ASD participants’ EF skills were assessed prior to the intervention taking place (Huffman et al. 2019) in order to advance the understanding of the effects of ATC solutions on cognitive processes and related adaptive behaviors.
A second limitation concerns the modularity of the cognitive processes assumed by the ICF framework. While, on one hand, it must be recognized that the same ATC may support a variety of cognitive processes other than those addressed in the present paper (e.g., working memory, emotion regulation), on the other hand, the use of ICF classification may be useful for clinicians and assistive technology professionals in linking neuropsychological functions with observable outcomes (e.g., being independent in performing activities). Further reviews are however needed to understand the effectiveness of ATC in compensating areas of functioning not addressed in this paper, such as working memory.
In conclusion, the present review further supports the available evidence on the positive effects of ATC for self-monitoring interventions in ASD (Chia et al. 2018). It however adds to the current evidence base on the need to broaden the spectrum of EF-related difficulties that may benefit from the use of ATC. Little research has indeed been conducted that systematically investigates the effectiveness of ATC in supporting EF-related difficulties in ASD individuals of any age, from early childhood to late adulthood. As technology continues to evolve and the estimates of those diagnosed with ASD grow, understanding the potential of ATC to address the core vulnerabilities of ASD may become increasingly important to improving the quality of life and social inclusion of this population. Future studies in this regard, for instance, may further explore the usefulness and effectiveness of combinations of emerging forms of technologies such as wearable devices (e.g., smartwatches, smartglasses) and Internet of Things (IoT) in providing online cognitive support to ASD individuals in different settings.
References
References marked with an * were included in the review
Abbott, P., Happé, F. G., & Charlton, R. A. (2018). Exploratory study of executive function abilities across the adult lifespan in individuals receiving an ASD diagnosis in adulthood. Journal of Autism and Developmental Disorders, 48(2), 4193-4206. https://doi.org/10.1007/s10803-018-3675-x.
Aresti-Bartolome, N., & Garcia-Zapirain, B. (2014). Technologies as support tools for persons with autistic spectrum disorder: a systematic review. International Journal of Environmental Research and Public Health, 11(8), 7767–7802. https://doi.org/10.3390/ijerph110807767.
Baron-Cohen, S. (2002). The extreme male brain theory of autism. Trends in Cognitive Sciences, 6(6), 248–254. https://doi.org/10.1016/S1364-6613(02)01904-6.
Bertelli, M. O., Cooper, S. A., & Salvador-Carulla, L. (2018). Intelligence and specific cognitive functions in intellectual disability: implications for assessment and classification. Current Opinion in Psychiatry, 31(2), 88–95. https://doi.org/10.1097/YCO.0000000000000387.
Best, C., O’Neill, B., & Gillespie, A. (2014). Assistive technology for cognition: An updated review. In G. Naik and Y. Guo (Eds.), Emerging theory and practice in neuroprosthetics (pp. 215-236). Pennyslvania: IGI Global.
*Bimbrahw, J., Boger, J., & Mihailidis, A. (2012). Investigating the efficacy of a computerized prompting device to assist children with autism spectrum disorder with activities of daily living. Assistive Technology, 24(4), 286–298. https://doi.org/10.1080/10400435.2012.680661
Bouck, E. C. (2010). Technology and students with disabilities: does it solve all the problems. In E. C. Bouck (ed.), Current issues and trends in special education: Research, technology, and teacher preparation (pp. 91-104). Emerald Group Publishing Limited.
*Bouck, E. C., Savage, M., Meyer, N. K., Taber-Doughty, T., & Hunley, M. (2014). High-tech or low-tech? Comparing self-monitoring systems to increase task independence for students with autism. Focus on Autism and Other Developmental Disabilities, 29(3), 156–167. https://doi.org/10.1177/1088357614528797.
*Bouck, E. C., Satsangi, R., & Bartlett, W. (2017). Supporting grocery shopping for students with intellectual disability: a preliminary study. Disability and Rehabilitation: Assistive Technology, 12(6), 605–613. https://doi.org/10.1080/17483107.2016.1201152.
Bradley, R., & Newbutt, N. (2018). Autism and virtual reality head-mounted displays: a state of the art systematic review. Journal of Enabling Technologies. https://doi.org/10.1108/JET-01-2018-0004.
Brady, D. I., Saklofske, D. H., Schwean, V. L., Montgomery, J. M., Thorne, K. J., & McCrimmon, A. W. (2017). Executive functions in young adults with autism spectrum disorder. Focus on Autism and Other Developmental Disabilities, 32(1), 31–43. https://doi.org/10.1177/1088357615609306.
Bruhn, A., & Wills, H. (2018). Emerging research and development in technology-based self-monitoring. Advances in Learning and Behavioral Disabilities, 30, 51–68. Emerald Publishing Limited. https://doi.org/10.1108/S0735-004X20180000030005.
Bruhn, A. L., McDaniel, S., & Kreigh, C. (2015). Self-monitoring interventions for students with behavior problems: a systematic review of current research. Behavioral Disorders, 40(2), 102–144. https://doi.org/10.17988/BD-13-45.1.
Bruhn, A. L., Waller, L., & Hasselbring, T. S. (2016). Tweets, texts, and tablets: the emergence of technology-based self-monitoring. Intervention in School and Clinic, 51(3), 157–162.
Burckley, E., Tincani, M., & Guld Fisher, A. (2015). An iPad™-based picture and video activity schedule increases community shopping skills of a young adult with autism spectrum disorder and intellectual disability. Developmental Neurorehabilitation, 18(2), 131–136. https://doi.org/10.3109/17518423.2014.945045.
Cai, Z., Fan, X., & Du, J. (2017). Gender and attitudes toward technology use: a meta-analysis. Computers & Education, 105, 1–13. https://doi.org/10.1016/j.compedu.2016.11.003.
Chia, G. L. C., Anderson, A., & McLean, L. A. (2018). Use of technology to support self-management in individuals with autism: systematic review. Review Journal of Autism and Developmental Disorders, 5(2), 142–155. https://doi.org/10.1007/s40489-018-0129-5.
*Cihak, D. F., Wright, R., & Ayres, K. M. (2010). Use of self-modeling static-picture prompts via a handheld computer to facilitate self-monitoring in the general education classroom. Education and Training in Autism and Developmental Disabilities, 45(1), 136–149.
*Clemons, L. L., Mason, B. A., Garrison-Kane, L., & Wills, H. P. (2016). Self-monitoring for high school students with disabilities: a cross-categorical investigation of I-Connect. Journal of Positive Behavior Interventions, 18(3), 145–155. https://doi.org/10.1177/1098300715596134.
Cole, E. (1999). Cognitive prosthetics: an overview to a method of treatment. Neurorehabilitation, 12, 39–51.
*Crutchfield, S. A., Mason, R. A., Chambers, A., Wills, H. P., & Mason, B. A. (2015). Use of a self-monitoring application to reduce stereotypic behavior in adolescents with autism: a preliminary investigation of I-Connect. Journal of Autism and Developmental Disorders, 45(5), 1146–1155. https://doi.org/10.1007/s10803-014-2272-x.
*Cullen, J. M., Alber-Morgan, S. R., Simmons-Reed, E. A., & Izzo, M. V. (2017). Effects of self-directed video prompting using iPads on the vocational task completion of young adults with intellectual and developmental disabilities. Journal of Vocational Rehabilitation, 46(3), 361–375. https://doi.org/10.3233/JVR-170873.
Dawson, P., & Guare, R. (2018). Executive skills in children and adolescents: a practical guide to assessment and intervention. Guilford Publications.
de Vries, M., & Geurts, H. (2015). Influence of autism traits and executive functioning on quality of life in children with an autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(9), 2734–2743. https://doi.org/10.1007/s10803-015-2438-1.
de Vries, M., Prins, P. J., Schmand, B. A., & Geurts, H. M. (2015). Working memory and cognitive flexibility-training for children with an autism spectrum disorder: a randomized controlled trial. Journal of Child Psychology and Psychiatry, 56(5), 566–576. https://doi.org/10.1111/jcpp.12324.
Dean, M., Harwood, R., & Kasari, C. (2017). The art of camouflage: gender differences in the social behaviors of girls and boys with autism spectrum disorder. Autism, 21(6), 678–689. https://doi.org/10.1177/1362361316671845.
Demetriou, E. A., Lampit, A., Quintana, D. S., Naismith, S. L., Song, Y. J. C., Pye, J. E., et al. (2018a). Autism spectrum disorders: a meta-analysis of executive function. Molecular Psychiatry, 23(5), 1198. https://doi.org/10.1038/mp.2017.75.
Demetriou, E. A., Song, C. Y., Park, S. H., Pepper, K. L., Naismith, S. L., Hermens, D. F., et al. (2018b). Autism, early psychosis, and social anxiety disorder: a transdiagnostic examination of executive function cognitive circuitry and contribution to disability. Translational Psychiatry, 8. https://doi.org/10.1038/s41398-018-0193-8.
Den Brok, W. L. J. E., & Sterkenburg, P. S. (2015). Self-controlled technologies to support skill attainment in persons with an autism spectrum disorder and/or an intellectual disability: a systematic literature review. Disability and Rehabilitation: Assistive Technology, 10(1), 1–10. https://doi.org/10.3109/17483107.2014.921248.
Dworzynski, K., Ronald, A., Bolton, P., & Happé, F. (2012). How different are girls and boys above and below the diagnostic threshold for autism spectrum disorders? Journal of the American Academy of Child & Adolescent Psychiatry, 51(8), 788–797. https://doi.org/10.1016/j.jaac.2012.05.018.
Evans, J. J., Emslie, H., & Wilson, B. A. (1998). External cueing systems in the rehabilitation of executive impairments of action. Journal of the International Neuropsychological Society, 4(4), 399–408.
*Fage, C., Consel, C. Y., Balland, E., Etchegoyhen, K., Amestoy, A., Bouvard, M., & Sauzéon, H. (2018). Tablet apps to support first school inclusion of children with autism spectrum disorders (ASD) in mainstream classrooms: a pilot study. Frontiers in Psychology, 9, 2020. https://doi.org/10.3389/fpsyg.2018.02020.
Ferri, S. L., Abel, T., & Brodkin, E. S. (2018). Sex differences in autism spectrum disorder: a review. Current Psychiatry Reports, 20(2), 9. https://doi.org/10.1007/s11920-018-0874-2.
Finn, L., Ramasamy, R., Dukes, C., & Scott, J. (2015). Using WatchMinder to increase the on-task behavior of students with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(5), 1408–1418. https://doi.org/10.1007/s10803-014-2300-x.
Fletcher-Watson, S., & Happé, F. (2019). Autism: A new introduction to psychological theory and current debate. Routledge.
Frank, F., Jablotschkin, M., Arthen, T., Riedel, A., Fangmeier, T., Hölzel, L. P., & van Elst, L. T. (2018). Education and employment status of adults with autism spectrum disorders in Germany–a cross-sectional-survey. BMC Psychiatry, 18(1), 75. https://doi.org/10.1186/s12888-018-1645-7.
Friedman, N. P., & Miyake, A. (2017). Unity and diversity of executive functions: individual differences as a window on cognitive structure. Cortex, 86, 186–204. https://doi.org/10.1016/j.cortex.2016.04.023.
*Gentry, T., Wallace, J., Kvarfordt, C., & Lynch, K. B. (2010). Personal digital assistants as cognitive aids for high school students with autism: results of a community-based trial. Journal of Vocational Rehabilitation, 32(2), 101–107. https://doi.org/10.3233/JVR-2010-0499.
*Gentry, T., Kriner, R., Sima, A., McDonough, J., & Wehman, P. (2015). Reducing the need for personal supports among workers with autism using an iPod touch as an assistive technology: delayed randomized control trial. Journal of Autism and Developmental Disorders, 45(3), 669–684. https://doi.org/10.1007/s10803-014-2221-8.
Geurts, H., Sinzig, J., Booth, R., & Happé, F. (2014). Neuropsychological heterogeneity in executive functioning in autism spectrum disorders. International Journal of Developmental Disabilities, 60(3), 155–162. https://doi.org/10.1179/2047387714Y.0000000047.
Gillespie, A., Best, C., & O’Neill, B. (2012). Cognitive function and assistive technology for cognition: a systematic review. Journal of the International Neuropsychological Society, 18(1), 1–19. https://doi.org/10.1017/S1355617711001548.
Gioia, G. A., Isquith, P. K., Guy, S. C., & Kenworthy, L. (2000). Test review behavior rating inventory of executive function. Child Neuropsychology, 6(3), 235–238.
Grynszpan, O., Weiss, P. L., Perez-Diaz, F., & Gal, E. (2014). Innovative technology-based interventions for autism spectrum disorders: a meta-analysis. Autism, 18(4), 346–361. https://doi.org/10.1177/1362361313476767.
Hampshire, P. K., & Allred, K. W. (2018). A parent-implemented, technology-mediated approach to increasing self-management homework skills in middle school students with autism. Exceptionality, 26(2), 119–136. https://doi.org/10.1080/09362835.2016.1216848
Henry, L. A., & Bettenay, C. (2010). The assessment of executive functioning in children. Child and Adolescent Mental Health, 15(2), 110–119. https://doi.org/10.1111/j.1475-3588.2010.00557.x.
*Huffman, J. M., Bross, L. A., Watson, E. K., Wills, H. P., & Mason, R. A. (2019). Preliminary investigation of a self-monitoring application for a postsecondary student with autism. Advances in Neurodevelopmental Disorders, 3(4), 226-235. https://doi.org/10.1007/s41252-019-00124-y.
Institute of Education Sciences (2017). What Works Clearinghouse: Standards Handbook Version 4.0. Retrieved online at: https://ies.ed.gov/ncee/wwc/Docs/referenceresources/wwc_standards_handbook_v4.pdf. Accessed 24 Oct 2019.
Jamieson, M., Cullen, B., McGee-Lennon, M., Brewster, S., & Evans, J. (2017). Technological memory aid use by people with acquired brain injury. Neuropsychological Rehabilitation, 27(6), 919–936. https://doi.org/10.1080/09602011.2015.1103760.
John, T. S., Dawson, G., & Estes, A. (2018). Brief report: executive function as a predictor of academic achievement in school-aged children with ASD. Journal of Autism and Developmental Disorders, 48(1), 276–283. https://doi.org/10.1007/s10803-019-04102-0.
Jurado, M. B., & Rosselli, M. (2007). The elusive nature of executive functions: a review of our current understanding. Neuropsychology Review, 17(3), 213–233. https://doi.org/10.1007/s11065-007-9040-z.
Kagohara, D. M., van der Meer, L., Ramdoss, S., O’Reilly, M. F., Lancioni, G. E., Davis, T. N., et al. (2013). Using iPods® and iPads® in teaching programs for individuals with developmental disabilities: a systematic review. Research in Developmental Disabilities, 34(1), 147–156. https://doi.org/10.1016/j.ridd.2012.07.027.
Kenny, L., Cribb, S. J., & Pellicano, E. (2018). Childhood executive function predicts later autistic features and adaptive behavior in young autistic people: a 12-year prospective study. Journal of Abnormal Child Psychology, 47(6), 1089–1099. https://doi.org/10.1007/s10802-018-0493-8.
Kenworthy, L., Yerys, B. E., Anthony, L. G., & Wallace, G. L. (2008). Understanding executive control in autism spectrum disorders in the lab and in the real world. Neuropsychology Review, 18(4), 320–338. https://doi.org/10.1007/s11065-008-9077-7.
Kenworthy, L., Anthony, L., & Alexander, K. (2014a). Solving executive function challenges: simple ways to get kids with autism unstuck and on target. Brookes Publishing.
Kenworthy, L., Anthony, L. G., Naiman, D. Q., Cannon, L., Wills, M. C., Luong-Tran, C., et al. (2014b). Randomized controlled effectiveness trial of executive function intervention for children on the autism spectrum. Journal of Child Psychology and Psychiatry, 55(4), 374–383. https://doi.org/10.1111/jcpp.12161.
Kiep, M., & Spek, A. A. (2017). Executive functioning in men and women with an autism spectrum disorder. Autism Research, 10(5), 940–948. https://doi.org/10.1002/aur.1721.
Kirk, H. E., Gray, K., Riby, D. M., & Cornish, K. M. (2015). Cognitive training as a resolution for early executive function difficulties in children with intellectual disabilities. Research in Developmental Disabilities, 38, 145–160. https://doi.org/10.1016/j.ridd.2014.12.026.
Koumpouros, Y., & Kafazis, T. (2019). Wearables and mobile technologies in autism spectrum disorder interventions: a systematic literature review. Research in Autism Spectrum Disorders, 66, 101405.
Leung, R. C., Vogan, V. M., Powell, T. L., Anagnostou, E., & Taylor, M. J. (2016). The role of executive functions in social impairment in autism spectrum disorder. Child Neuropsychology, 22(3), 336–344. https://doi.org/10.1080/09297049.2015.1005066.
Logan, K., Iacono, T., & Trembath, D. (2017). A systematic review of research into aided AAC to increase social-communication functions in children with autism spectrum disorder. Augmentative and Alternative Communication, 33(1), 51–64. https://doi.org/10.1080/07434618.2016.1267795.
Lopresti, E. F., Mihailidis, A., & Kirsch, N. (2004). Assistive technology for cognitive rehabilitation: state of the art. Neuropsychological Rehabilitation, 14(1–2), 5–39. https://doi.org/10.1080/09602010343000101.
Mazefsky, C. A., Pelphrey, K. A., & Dahl, R. E. (2012). The need for a broader approach to emotion regulation research in autism. Child Development Perspectives, 6(1), 92–97.
Mihailidis, A., Boger, J. N., Craig, T., & Hoey, J. (2008). The COACH prompting system to assist older adults with dementia through handwashing: an efficacy study. BMC Geriatrics, 8(1), 28. https://doi.org/10.1186/1471-2318-8-28.
Munn, Z., Peters, M. D., Stern, C., Tufanaru, C., McArthur, A., & Aromataris, E. (2018). Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology, 18(1), 143. https://doi.org/10.1186/s12874-018-0611-x.
O’Neill, B., & Gillespie, A. (2014). Assistive technology for cognition. Psychology Press.
O’Neill, B., Best, C., O’Neill, L., Ramos, S. D., & Gillespie, A. (2018). Efficacy of a micro-prompting technology in reducing support needed by people with severe acquired brain injury in activities of daily living: a randomized control trial. Journal of Head Trauma Rehabilitation, 33(5), e33–e41. https://doi.org/10.1097/HTR.0000000000000358.
Odom, S. L., Thompson, J. L., Hedges, S., Boyd, B. A., Dykstra, J. R., Duda, M. A., et al. (2015). Technology-aided interventions and instruction for adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(12), 3805–3819. https://doi.org/10.1007/s10803-014-2320-6.
*Palmen, A., Didden, R., & Verhoeven, L. (2012). A personal digital assistant for improving independent transitioning in adolescents with high-functioning autism spectrum disorder. Developmental Neurorehabilitation, 15(6), 401–413. https://doi.org/10.3109/17518423.2012.701240.
Pennisi, P., Tonacci, A., Tartarisco, G., Billeci, L., Ruta, L., Gangemi, S., & Pioggia, G. (2016). Autism and social robotics: a systematic review. Autism Research, 9(2), 165–183. https://doi.org/10.1002/aur.1527.
Rivet, T. T., & Matson, J. L. (2011). Review of gender differences in core symptomatology in autism spectrum disorders. Research in Autism Spectrum Disorders, 5, 957–976. https://doi.org/10.1016/j.rasd.2010.12.003.
*Rosenbloom, R., Mason, R. A., Wills, H. P., & Mason, B. A. (2016). Technology delivered self-monitoring application to promote successful inclusion of an elementary student with autism. Assistive Technology, 28(1), 9–16. https://doi.org/10.1080/10400435.2015.1059384
Scherer, M. J., Hart, T., Kirsch, N., & Schulthesis, M. (2005). Assistive technologies for cognitive disabilities. Critical Reviews in Physical and Rehabilitation Medicine, 17(3), 195–215. https://doi.org/10.1615/CritRevPhysRehabilMed.v17.i3.30.
Schwartz, D. M. (2014). Breaking through barriers: using technology to address executive function weaknesses and improve student achievement. Applied Neuropsychology: Child, 3(3), 173–181. https://doi.org/10.1080/21622965.2013.875296.
Smith, D. L., Atmatzidis, K., Capogreco, M., Lloyd-Randolfi, D., & Seman, V. (2017). Evidence-based interventions for increasing work participation for persons with various disabilities: a systematic review. OTJR: Occupation, Participation and Health, 37(2_suppl), 3S–13S. https://doi.org/10.1177/1539449216681276.
Stephenson, J., & Limbrick, L. (2015). A review of the use of touch-screen mobile devices by people with developmental disabilities. Journal of Autism and Developmental Disorders, 45(12), 3777–3791. https://doi.org/10.1007/s10803-013-1878-8.
Takacs, Z. K., & Kassai, R. (2019). The efficacy of different interventions to foster children’s executive function skills: a series of meta-analyses. Psychological Bulletin, 145(7), 653–697. https://doi.org/10.1037/bul0000195.
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850.
Valeri, G., Casula, L., Napoli, E., Stievano, P., Trimarco, B., Vicari, S., & Scalisi, T. G. (2019). Executive functions and symptom severity in an Italian sample of intellectually able preschoolers with autism spectrum disorder. Journal of Autism and Developmental Disorders, 1–9. https://doi.org/10.1007/s10803-019-04102-0.
Van Steenburgh, J. J., Varvaris, M., Schretlen, D. J., Vannorsdall, T. D., & Gordon, B. (2017). Balanced bifrontal transcranial direct current stimulation enhances working memory in adults with high-functioning autism: a sham-controlled crossover study. Molecular autism, 8(1), 40. https://doi.org/10.1186/s13229-017-0152-x.
Velikonja, T., Fett, A. K., & Velthorst, E. (2019). Patterns of nonsocial and social cognitive functioning in adults with autism spectrum disorder: a systematic review and meta-analysis. JAMA Psychiatry, 76(2), 135–151. https://doi.org/10.1001/jamapsychiatry.2018.3645.
Wallace, G. L., Yerys, B. E., Peng, C., Dlugi, E., Anthony, L. G., & Kenworthy, L. (2016). Assessment and treatment of executive function impairments in autism spectrum disorder: an update. International Review of Research in Developmental Disabilities, 51, 85–122.
Walsh, E., Holloway, J., McCoy, A., & Lydon, H. (2017). Technology-aided interventions for employment skills in adults with autism spectrum disorder: a systematic review. Review Journal of Autism and Developmental Disorders, 4(1), 12–25. https://doi.org/10.1007/s40489-016-0093-x.
Wass, S. V., & Porayska-Pomsta, K. (2014). The uses of cognitive training technologies in the treatment of autism spectrum disorders. Autism, 18(8), 851–871. https://doi.org/10.1177/1362361313499827.
Wehmeyer, M. L., & Shogren, K. A. (2013). Establishing the field of applied cognitive technology. Inclusion, 1(2), 91–94. https://doi.org/10.1352/2326-6988-01.02.91.
White, E. I., Wallace, G. L., Bascom, J., Armour, A. C., Register-Brown, K., Popal, H. S., et al. (2017). Sex differences in parent-reported executive functioning and adaptive behavior in children and young adults with autism spectrum disorder. Autism Research, 10(10), 1653–1662. https://doi.org/10.1002/aur.1811.
World Health Organization. (2001). International classification of functioning, disability and health: ICF. World Health Organization https://apps.who.int/iris/handle/10665/42407. Accessed May 2020.
*Xin, J. F., Sheppard, M. E., & Brown, M. (2017). Using iPads for self-monitoring of students with autism. Journal of Autism and Developmental Disorders, 47(5), 1559–1567. https://doi.org/10.1007/s10803-017-3055-y.
Author information
Authors and Affiliations
Contributions
LD and ADS were responsible for setting up the review, acquiring/analyzing the data, and writing/editing the manuscript. All the authors contributed in editing the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
Not pertinent.
Informed Consent
Not pertinent.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Desideri, L., Di Santantonio, A., Varrucciu, N. et al. Assistive Technology for Cognition to Support Executive Functions in Autism: a Scoping Review. Adv Neurodev Disord 4, 330–343 (2020). https://doi.org/10.1007/s41252-020-00163-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41252-020-00163-w