
Abstract
This study examined predictors of households’ calorie demand using consumer expenditure survey data during the time frame of millennium development goals. It draws suggestions for achieving sustainable development goals to eliminate calorie-poverty. We used the log of per-capita calorie intake as the calorie demand. Endogeneity corrected quantile regression was applied to examine the distributional effect of predictors. Findings revealed calorie-monthly per-capita consumption expenditure (MPCE) elasticities were positively statistically significant across quantiles in rural-and urban-areas, but, contrary to traditional wisdom, elasticities are lower for calorie-poor than calorie-rich households. Dietary diversification of food items, relative food price, and share of medical-and education-expenditure were the main adverse drivers of calorie demand. Our results are robust to the under-reporting and measurement error. The policy implications are: (a) only focusing on pro-poor income enhancing strategies will not able to reduce calorie deprivation, it should be backed by imparting awareness about food choice and nutritional value of low price food items, (b) to implement necessary policy to maintain stable food inflation and effectively targeted food subsidy for calorie poor, (c) to adopt forward-looking medical-and education-policy such as free health and education facilities to all by enhancing public spending to revive the quality of public hospitals and educational institutions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
One of the essential objectives of millennium development goals (MDGs) was to eradicate extreme poverty by 2015. This is upgraded to eliminate “any poverty” by 2030 under the sustainable development goals (SDGs). India, being an active member of the UN, should attempt to achieve the goal of SDGs. The government of India has initiated a variety of policies to tackle direct and indirect povertyFootnote 1 from 2002 to 2017. Programs such as Mahatma Gandhi National Rural Employment Guarantee Act is designed to reduce the indirect poverty, whereas, the subsidised food items under the public distribution system (PDS) for direct poverty. However, direct poverty remained high even if food assistance programs such as subsidies food items, integrated child development services, mid-day meals to school students are policy interventions to reduce direct poverty. For instance, the decline rate of malnutrition caused by calorie deprivation is very low in India (Panagariya 2013). Besides, some of the previous studies stated that the per-capita calorie intake has been declining and incidence of calorie-poverty (i.e., direct poverty) has been increasing (Bhuyan et al. 2020; Chandrasekhar and Ghosh 2003; Deaton and Drèze 2009; Kumar et al. 2007; Meenakshi and Vishwanathan 2003; Patnaik 2004; Patnaik 2007; Suryanarayana and Silva 2007). Therefore, there is a need to examine significant predictors of calorie intake under the framework of consumer demand theory. It will provide inputs to better implement its’ programs and policy to address direct poverty.
Previous studies have provided following conjectures of calorie intake decline; leakages in PDS (Dreze and Khera 2015; Khera 2011), food budget squeeze (Basole and Basu 2015), rise in relative food price (Gaiha et al. 2010), increase in eating out meals and snacks (Gaiha et al. 2013), dietary diversification towards expensive sources of calorie (Landy 2009; Mittal 2007), increase in education-and medical-expenditure (Mehta and Venkatraman 2000), choice of luxuries goods over food items (Banerjee and Duflo 2011), demographic characteristics (Mahadevan and Suardi 2013), low requirement due to mechanisation of agriculture and better transport facility (Deaton and Drèze 2009; Rao 2000), under-reporting of food consumed away from home (Smith 2015), and improvement in disease environment (Zakaria et al. 2017). However, the above studies were unable to provide sufficient evidence due to the exclusion of major variables and methodological drawbacks. Therefore, this study has contributed by addressing four issues.
First, India achieved remarkable success on indirect poverty reduction (Panagariya and Mukim 2014). However, direct poverty remained high, and the largest number of undernourished people are living in India (World Bank 2017). In the previous decades, out-of-pocket expenditure on medical (Berman et al. 2010) and educational (Tilak 1996, 2004) have been increasing due to the disinvestment policy of the government. This rising expenditure on education and health of poor households expected to have an adverse effect on calorie demand because of income constraints. Nevertheless, there is a lack of empirical evidence on it. This study aims to fulfill this gap in direct poverty.
Two, a few studies have carried out to examine why calorie intake declines in India. Behrman and Deolalikar (1989) used calorie-income and food expenditure-income elasticity to examine dietary diversification. Their findings revealed income elasticity of calorie demand is lower than income elasticity of food expenditure, and hence, ascertain the possibility of an increase in food varieties as income increases. However, they have not examined the hypothesises of the impact of food diversification by constructing a diversification index. Similarly, Mittal (2007) has not empirically evaluated dietary diversification; however, it is their concluding argument in support of diversification by empirically examining substitution and income effects. Landy (2009) has theoretically argued in favour of dietary diversification. To overcome this research gap, our study has constructed a dietary diversification index and assume this might be a major predictor of calorie decline. Along with the above predictors, we have examined the impact of relative cereal price and income of the household. While Basole and Basu (2015) have examined the relationship between relative price and calorie demand assuming linearity, we have extended it using a non-linear framework.
Three, another drawback of the previous studies was the presumption of linearity (Behrman and Deolalikar 1989; Mittal 2007; Basole and Basu 2015). They have used linear calorie demand regression that has restricted assumption of linearity and conditional on full distribution, which may not be practical. Particularly in calorie intake literature, this leads to the specification bias when the data characteristics are non-linear. The predictors, which are affecting calorie-poor families, may not behave effectively for calorie-rich families similarly. Therefore, sign and magnitude of coefficients may vary across the distribution. By addressing these issues, there is a need for study, which can examine varied impacts across the distribution of calorie demand. Our study fulfills this gap by using bootstrapping quantile regression, which is a more suitable method in the calorie demand literature.
Fourth, we have extended analysis by using the latest available data set which the previous study has not used. For example, Basole and Basu (2015) have used historical data from 1987 to 2009 and ignored recent survey data. Our research has used full-fledged data surveyed, which covered 61st round (2004–05), 66th round (2009–10), and 68th round (2011–12) survey data.
The rest of this paper organised as follows. Section 2 reviewed previous literature and hypotheses development. Section 3 outlines the theoretical model. Section 4 includes the method. Section 5 explains the estimation technique. Results and discussions are presented in Sects. 6 and 7 respectively. Section 8 presents the conclusion, limitation, and policy implication.
Literature Review and Hypotheses Development
Calorie-Income
There is a general perception of the positive calorie-income relationship. A higher total calorie-income elasticity found in 1999 than 1996 for Indonesia (Skoufias 2003). Other studies such as Bouis and Haddad (1992) for Philippine; Grimard (1996) for Pakistan; Subramanian and Deaton (1996) for India; Gibson and Rozelle (2002) for Urban Papua New Guinea; Aromolaran (2004), Abdulai and Aubert (2004a) and Abdulai and Aubert (2004b) for Nigeria have found positive relationship between income and calorie demand. Also, empirical literature has revealed that calorie-income elasticity is not significantly different from zero. For instance, Behrman and Wolfe (1984) examined calorie-income elasticity for Nicaragua and found insignificant and inverse relationships. Behrman and Deolalikar (1987) examined for India and observed that calorie-income elastic is close to zero, similar to the study of Bouis (1994) for poor countries Kenya and Philippines; Skoufias et al. (2011) for Indonesia.
It appears empirical literatures are divided on the relationship between calorie-income relationships. This leads to a debate on the effectiveness of income on calorie intake. We propose:
Hypothesis 1
The increase in household income will positively influence calorie demand.
Calorie and Relative Food Price
There has been an unprecedented rise in global food prices (Faridi and Wadood 2010) and domestic food prices since 2007 (Chand and Jumrani 2013). The increase in food prices resulted in an adverse impact on calorie demand. Rise in food price has caused 115 million people to add to hunger (FAO 2009). In India, between January 2008 to July 2010, supply constraints and wrong policy framework fuelled food inflation (Chand 2010). For instance, rice output had touched more than 90 million tons from 2004–05 to 2009–10, which was more than buffer norms. Unfortunately, rice inflation went along with rice production due to the massive export of rice, which is a reflection of the mismanagement of rice policy. As a result, on an average, per-capita availability of rice for consumption declined and led to volatile price (Kozicka et al. 2017). The ratio of procurement quantity to the total output of rice increased, therefore, leading to the rising price level. The decline in oilseed output leads to a low level of oil cake production. The oil cake is often used for animal feed. As a result, milk and its’ product has declined, which leads to food inflation (Nair and Eapen 2012). The rise in food prices will hurt the consumption of food items and consequently a negative effect on calorie demand. Therefore, we purpose,
Hypothesis 2
Relative high cereal to non-cereal price will negatively influence calorie demand.
Calorie Intake and Food Diversification
In the past few decades, rapid economic growth, urbanization, and globalisation have shifted the choice of staple food items towards non-staple food items such as livestock, fruits and vegetables, and fat and oil. Besides, food preference is converging to western diets (Gaiha et al. 2012). The increasing trend of dietary diversification has been documented in poor-and-developing countries in Asia, Africa, and Latin America (Behrman and Deolalikar 1989; Mendez and Popkin 2004). In Asia, particular for India, majority of household prefers rice consumption. The rice consumption in Asia has declined as the income has grown despite the preference of households (Ito et al. 1989; Huang and David 1993). Previous studies such as Behrman and Deolalikar (1989), Mittal (2007), Landy (2009) argued in the favor of food habit transition in India. Hence,
Hypothesis 3
The increase in diet diversification towards expensive sources of calorie will negatively influence calorie demand.
Calorie and Medical and Educational Expenditure
The households’ medical and educational expenditure has been increasing due to the disinvestment policy of the government of India (Dev and Mooij 2002; Tilak 2004). As India is a developing nation, every household may not have purchasing power for adequate spending on medical and education. Due to the disinvestment policy in medical, physical access and facilities have been declining in government hospitals, which encourage households to choose private hospitals. Hence, households' health care system heavily depends on out-of-pocket expenditure in India (Ghosh 2011). Households are spending on educations because of their expectations of long-term high returns (Psacharopoulos and Patrinos 2004). The quality of education in government schools has been declining (Härmä 2011; Singh and Sarkar 2012). As a result, parents are preferring private schools or private tuition for the education of their children, which is more expensive. The high expensive creates heavy financial burden on the poor households. Therefore, they may compensate it from their purchasing of food items, which ultimately decline calorie demand. Hence,
Hypothesis 4
The increasing share of medical and educational expenditure will negatively influence calorie demand.
Theoretical Framework
The analysis of calorie demand modelled within the framework of consumer demand theory, where a household assumed to maximise utility. Household’s utility function specified as:
where U is a utility function that is assumed to be well behaved (twice differentiable and strictly quasi-concave); \(Q_{c}\) and \(Q_{nc}\) are quantity of cereal and non-cereal food items; \(S_{h}\) and \(E_{h}\) are other social and economic predictors. The utility that the household derives from various combinations and levels depends on the price of particular food items and availability of income. Households’ limited income curtailed power to purchase unlimited amounts of cereals and non-cereals food items, which presented as:
where \(Y^{0}\) is limited income, \(p_{c}\) and \(p_{nc}\) are the price of cereal and non-cereal food items respectively. \(Y\) is total income, \(E\) is expenditure on education, \(M\) is expenditure on medical, and \(D\) is expenditure on durable goods. Household’s desire is to maximise Eq. (1) subject to constraints given in Eq. (2). From the Lagrange function
where \(\lambda\) is undetermined multiplier. The first-order condition is obtained by setting the partial derivatives of Eq. (4) with respect to \(Q_{c}\), \(Q_{nc}\), and \(\lambda\) equals to zero:
Transposing the second terms in the first two equations of Eq. (5) to the right and dividing the first by the second yields
The left side of Eq. (6) is the optimal demand of cereal and non-cereal food items. The per-capita calorie conversion of optimal demand used as dependent variable. Right-hand side is relative price acted as independent variable. Therefore, by using the above condition of consumer choice, demand curve derived as:
where \(C_{i}\) is per-capita calorie intake, depends on relative price, income, and other socio-economic predictors.
Method
Data and Sampling
This study employed three rounds i.e., 2004–05 (61st), 2009–10 (66th) and 2011–12 (68th) of household-level NSS consumer expenditure data. A stratified multistage design adopted and remained consistent across rounds of the sample survey. The first stage units were the 2001 census villages (Panchayat wards in case of Kerala) in the rural sector and urban frame survey blocks in the urban areas. The ultimate stage units were households. If the first stage unit is large, one intermediate stage of sampling selected of two hamlet-groups/sub-blocks from each rural/ urban first stage unit. For detail discussion on sampling, refer to NSS reports number 513, 540, and 560. The analysis carried out on the household level. We have removed the invalid households. The remaining families for rural and urban areas were 151,589 and 94,375 and used for econometric analysis, respectively.
Variables
Dependent Variable
This study used per-capita calorie intake as the dependent variable. Total unit of each food items multiplied by their calorie availability. Calorie values per unit were drawn from NSS reports 513, 540, and 560 based on “Nutritive Values of Indian Foods” (by Gopalan et al. 1993. Revised and updated by Rao 1993). Total calorie intake measured by summing calorie intakeFootnote 2 of each item. Then, per-capita calorie consumption of a household computed as:
where \(C_{i}\) is per-capita calorie intake (PCI); \(N_{i}\) household size, \(R_{j}\) per-unit calorie of jth food item, \(X_{ji}\) quantity of jth commodity for ith household.
There may be measurement error due to some food items not listed in the NSS survey. The conversion factor depends upon the method of preparation of food. There are composite food items such as cooked meals and vegetables, for which an exact conversion factor is difficult to acquire. These measurement errors may be stable over a period, and hence, can be utilised for comparison.
Construction of Predictors
The study divided all covariates into two groups, variable of interest and other controlled variables. Variable of interest were monthly per-capita consumption expenditure (MPCE),Footnote 3 relative cereal price, dietary diversification index, and share of medical and education expenditure. Control variables were caste, religion, and household with a regular salary, the household with ration-card, household size and its’ square, the age of household head and its’ square, child dependency ratio, households’ livelihood, education level and gender of household head, land per-capita, and major occupation of the household. In Appendix 1 control variables necessity and their construction were discussed.
MPCE
Total expenditures were computed by adding the expenditure of households on different items listed in the survey schedule. Mixed recall periodFootnote 4 was used for measuring total expenditure. Total expenditure converted to a monthly basis. By dividing with household size, monthly per-capita expenditure obtained, then, adjusted with the consumer price inflationFootnote 5 to obtain real MPCE. The natural logarithm of real MPCE was used in the analysis to represent the economic level of the household.
There is an increasing divergence between National Account Statistics and National sample survey per capita expenditure data: it puts a question on the validity of NSS data (Deaton 2001; Bhalla 2003). However, expenditure by a mixed reference period (MRP) reduces the divergence (GOI 2015; Datt et al. 2016). Therefore, we have used MPCE mrp as the proxy of the income.
Relative Price
The ratio of cereal and non-cereal prices used to measure the effect of relative price on calorie demand. All cereals and non-cereals food items pertaining to 2004–05, 2009–10, and 2011–12 considered for construction of relative price ratio. The unit value of each item calculated by dividing total expenditure incurred by the household with the total quantity consumed of respective items. Then, the total unit value of cereals divided with the total unit value of non-cereals items to generate the price ratio.Footnote 6 A higher relative price will decline calorie intake and vice-versa because cereals-and-substitutes are the low-cost source of calories.
Diet Diversification
Diversification index (DI) used to measure the change in food preference from cereals-and-substitutes to non-cereal food items. Higher diversification declines per-capita calorie intake due to the income constraints. We proposed the Herfindahl–Hirschman index for measuring dietary diversification of food items. The Herfindahl–Hirschman index is given by:
Here, \(X_{ij}\) indicates expenditure of ith household on jth sub-group food expenditure. There are \(k\) food sub-groups. Sub-groups are cereals and its’ substitute, pulses-products, milk and its’ products, edible oils, egg-fish-meat, vegetables, fruits, sugar-salt-spices, beverages, pan-tobacco-intoxicants. Higher DI value indicates lower diversification and vice versa.
Share of Medical and Education Expenditure
Total household expenditure on medical measured obtained by adding institutional and non-institutional medical spending. Then, share of medical expenditures measured by dividing total medical expenditure incurred during last 30 days with total household monthly expenditure.Footnote 7 A similar procedure followed for measurement of the share of education expenditure.
Other control variables are caste, religion, national industrial classification, state, household size, age and education of household head, the gender of head, and the year. The details of the control variables are presented in the Appendix 1.
Estimation Technique
Ordinary least square regression (OLS) and quantile regression (QR) proposed by Koenker et al. (1978) applied for analysis. QR used to examine conditional distributional effects of covariates on the log of Per-capita calorie intake (LPCI).
OLS and Quantile Regression
OLS
The OLS regression describes the cause and effect relationship between the outcome variable of interest and a set of regressors, which assume conditional mean function and whole observation as a unit of one sample. Consider,
where \(\ln \;C_{i}\) is natural log of PCI (LPCI), \(RP\) is relative price, DI is diversification index, ME is medical expenditure, EE is education expenditure, \(x^{\prime}_{ij}\) is vector of control variables, and \(u_{i}\) is the error term, assumed to \(iid \approx N(0,1)\).
By combining all variables of interest and control variables, we can rewrite Eq. (8) into
where ‘k + 5’ is the number of independent variables included in the regression.
Quantile Regression
OLS assumes normal distribution, which is not practical in cross-section data. In this case, quantile regression (QR) introduced by Koenker et al. (1978) provides a better picture by splitting the distribution into different quantile. Unlike OLS and other classical regression models, which assumes conditional on mean, QR assumes conditional on median. Estimator of QR is a weighted sum of absolute deviation, hence robust to the outliers in contrast to OLS and Logit estimates (Koenker 2005). QR is a semi-parametric method and avoids usual OLS assumptions \(iid \approx \left( {0,1} \right)\) of error terms; therefore, more suitable for heteroscedasticity data. Also, QR provides richer characteristics of data by allowing examining the impact of covariates at different quantile, whereas OLS allows only on full distribution. For calorie demand literature, covariates impact may not be equal for richer and poor household. Therefore, QR is more relevant to this study.
From Eq. (9), \(i\) is household, where \(i = 1 \ldots n\). QR assumes \(\Phi {\text{th}}\) quintile \(\left( {0 < \Phi < 1} \right)\) of the conditional distribution of ln Ci is linear in \(k \times 1\) vector of covariates \(x_{iz}\)
\(Q_{0} \left( {\frac{{\ln C_{i} }}{{\sum\nolimits_{z = 1}^{k + 5} {x^{\prime}_{iz} } }}} \right) = x^{\prime}_{iz} \beta\) is the conditional quintile function and \(\beta\) is the unknown \(k \times 1\) vector of parameters of covariates. This unknown vector solved by the minimum sum of the weighted of absolute deviation using \(\Phi\) as weights. Therefore, the function is written as:
The above minimisation problem has a linear programming solution with a finite number of simplex iterations (Buchinsky 1998). For greater robust results, this study employed a bootstrap estimation procedure (Buchinsky 1995). In the bootstrapping procedure, QR estimated by randomly drawing a sub-sample with replacement from the original sample. Fifty bootstrap replication is often enough to provide a reasonable estimate and seldom are more than 200 (Efron and Tibshirani 1993). Therefore, this study restricted bootstrap arbitrarily 100 to minimise computation time.
Endogeneity and Control Function
Endogeneity
The theory of wage-efficiency advocates that wage/income and calorie intake affects each other. As income increases, there is a possibility of an increase in calorie intake. In reverse, an increase in calorie intake leads to more physical strength to work longer duration. When labour is increasing his/her working duration, his/her wages/income increases. Therefore, the simultaneity exists between income and calorie intake, creating simultaneity bias, in turn, estimates become inconsistency. Therefore, MPCE is an endogenous variable.
In the presence of endogeneity, estimated coefficients will be inconsistent and lead to endogeneity bias. The error ‘\(u_{i}\)’ in Eq. (8) embodied with other determinants other than, \(MPCE_{i}\) and \(x_{ij}\), which are not included in model. Therefore, \(u_{i}\) expected to be highly correlated with MPCE, and thus, \(E(u_{i} /MPCE_{i} ) \ne 0\).
Control Function
To obtain consistence coefficient, endogeneity is addressed using control function (CF) approach. CF provides better results compare to the two stage least square and Generalised method of moment estimation (Wooldridge 2007) when the endogenous explanatory variables are non-linear and remain identical as the 2SLS for the linear endogenous variables. Following (Wooldridge 2010) CF defined from Eq. (9).
where \(l\) is number of instruments. In Eq. (12) the expectation of independent variable with the error is zero. Endogeneity of \(MPCE_{i}\) arises if and only if \(u_{i}\) is correlated with \(v_{i}\). Therefore, linear projection of \(u_{1}\) and \(v_{2}\) in error form:
\(\rho_{1} = E(v_{i} u_{i} )/E(v_{i}^{2} )\) and \(E(v_{i} e_{i} ) = 0,\;E(x_{ij} e_{1} ) = 0,\) because \(u_{i}\) and \(v_{i}\) are both uncorrelated with \(x_{ij}\). Now, putting Eq. (13) in Eq. (8) we get:
Equation (14) is free from endogeneity issue and used for analysis to estimate parameter of interest at different quantile and whole distribution. If \(\rho_{1}\) is significant, then our instruments are valid and MPCE is endogenous. The OLS or quantile estimates from Eq. (14) are control function estimates.
Identifying Valid Instrument
It may be noted that the identification of valid instruments and empirical prove of those are challenging. An instrument is valid when it is correlated with the endogenous independent variable and uncorrelated with the error term. It does not have a direct effect on the dependent variable but has an indirect effect on it. However, empirical validation of the instrument is not possible because the actual error term is unknown. Therefore, the instrument should be based on previous literature, theory, or logical argument. This study used durables expenditure as an instrumental variable following the previous literature (Subramanian and Deaton 1996; Babatunde et al. 2010). The durable spending does not directly affect the household calorie intake but indirectly affect it through the income of the household. Therefore, if the durable expenditure increases, it will directly affect the MPCE and indirectly to the calorie intake.
Result
This section only reported results. Discussions are presented in the next section.
Descriptive Statistics
Table 1 shows the mean and standard deviation of main variables of interest, which are used as the predictors for rural and urban areas. Relative price, diversification, medical expenditure, low activity and medium activityFootnote 8 are more in urban areas than the rural areas. However, MPCE, education expenditure, and heavy activity are more in rural areas.
Table 2 presented the summary statistics of dependent variables, i.e., LPCI. The average value of LPCI was lower in urban compared to the rural area. However, the standard error was high for urban, indicating higher inequality. The skewness statistics were positive, indicating positively skewed. The Kurtosis value was more than three, conforming lepto-kurtosis. The Doornik–Hansen chi-square statistics were significant at 1% level, rejecting the hypothesis of normality. Breusch and Pagan (1979) and Cook and Weisberg (1983) test used for identifying heteroscedasticity, which revealed the presence of heteroscedasticity against the null hypothesis in rural and urban. The descriptive statistics were showing enough evidence to use quantile regression than linear ordinary least square (OLS). However, to illustrate how OLS coefficients are different from quantile regression coefficients, we have estimated and plotted coefficients of OLS and quantiles in the next sections.
Furthermore, we have estimated the per-capita calorie intake and diversification index across the income deciles and over the years to examine their movement. The results are presented in Figs. 1 and 2. The low diversification index indicates the higher diversifications, vice versa. We found that the degree of decline in calorie intake for higher-income deciles are higher from 2004–05 to 2011–12 relative to the lower deciles (Fig. 1) in rural and urban areas, whereas their diversification is found to be more (Fig. 2).

Source Author’s calculations
Distribution of per-capita calorie intake over the income deciles. Note The figures are using weight.

Source Author’s calculation
Distribution of diversification index over the income deciles. Note: The low index suggests the higher diversification and vice-versa. The figures are using weight.
Control Function Results
In the first stage, regression Eq. (12) is estimated, where endogenous MPCE is regressed on all exogenous variables, including instrument variables log per-capita durable expenditure. Figure 3 presents coefficients of instrument variables estimated in the first stage regression for rural-and-urban India. Per-capita durable expenditure is positively significant for OLS and each quantile, suggesting a one-unit increase in durable goods expenditure has a positive impact on the MPCE of different distributions. Then, we undertake further analysis in the second-stage estimation. The study estimates the QR using Eq. (14) for rural-and-urban, where LPCI regressed on the variable of interest controlling other predictors. Besides, predicted error from Eq. (12) or derived from the first stage regression included as regressors-known as control function estimates. The coefficients were plotted over the quantiles with their marked the significance level (Fig. 4). In the rural-and-urban areas, the coefficients of error term were statistically significant, indicating MPCE is endogenous and our instrument is good enough to control endogeneity.

Source Authors’ own calculation
Coefficients of instrument variables used in first stage regression. Note Red and yellow dots indicate the coefficient is significant at 5% and 10% level of significance, respectively.

Control function
Figure 5 presented the coefficient movements over the quantiles of the variable of interest. Calorie-MPCE elasticities were positively statistically different from zero across quantiles in rural-and-urban areas and supported Hypothesis 1. However, the elasticities were low and in the range of 0.20 to 0.43 in rural areas: In the urban area, those were between 0.20 and 0.33.


Source Author’s calculation
Quantile regression results. Note The red and yellow dots indicate the coefficient is significant at 5 and 10% level of significance level, respectively.
In rural-and-urban areas, coefficients of relative price were negative and statistically significant in lower and upper quantiles in rural and urban areas, indicating relative cereal prices adversely influencing calorie demand. Therefore, Hypothesis 2 was accepted in the case of lower and upper quantiles.
Diversification index, which measures the intensity of food habit transition, was significant across quantile in rural-and-urban areas. The positive coefficient observed for rural and urban areas except for a few lower quantiles in urban areas, which suggests that an increase in the diversification will decline the calorie intake. Therefore, the findings accepted the Hypothesis 3 for most of the quantiles. Nevertheless, it does not hold for the few households that are falling under lower quantiles in urban areas.
The sign of coefficients of medical and education expenditures were consistently negative and significant. There was a minor exception for lower and higher quantiles in rural and urban areas, where the coefficients are negative but not statistically significant. As expected, the decline in calorie intake is associated with an increase in the share of spending on health and education, which supports Hypothesis 4.
We also examined the notion that the calorie demand itself has reduced due to the increase in sedentary lifestyle by adding the occupation dummy. We have categorised the activity level into three types, low activity, middle activity, and heavy activity (Basu and Basole 2013). Most of the quantile coefficients of medium activity in rural areas are negative and insignificant, whereas, in urban areas, most of the coefficients are positive but insignificant. In the case of the heavy activity, negative and significant coefficient found in rural areas, whereas, in urban areas, few quantiles are significant with negative signs. Deaton and Drèze (2009) and Rao (2000) argued that calorie need declines due to the low requirement as a result of the mechanization of the agriculture and better transport facility, however, taken together, our results suggest that even though the argument hold but not so strong for most of the quantiles. Our results are similar to the findings of Basu and Basole (2013).
Calorie-Income Elasticity Results over the Years
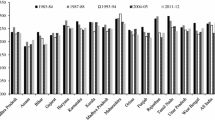
Furthermore, we have also examined the calorie-income elasticity over the years for rural and urban areas. Therefore, we have estimated our specifications separately for each year and sector. The results are presented in the Fig. 6. The results suggested that the pattern of the calorie-income elasticity is similar in the rural areas over the quantiles from 2005 to 2012. However, in urban areas, the pattern is similar for the years 2010 and 2012. Besides, the figure revealed that the elasticity has been declining since 2005 in rural and urban areas.

Calorie expenditure elasticity across quantiles over the years in rural and urban areas
Sensitivity Analysis
In this section, we undertake two types of sensitivity analysis. First, we have re-estimated the structural equation using the 2SLS procedure and verified the coefficients along with the relevance of the instruments. Second, we have used the adjusted calorie intake as the dependent variable to examine the consistency of the coefficients.
We have gone through the details literature on whether there is any econometric test that can be used to verify the validity of the instruments in the quantile regression framework; unfortunately, we did not find any test. Therefore, we applied 2SLS in our data set using the per-capita durable expenditure of the household as the instruments. The obtained results are presented in Table 3. The Anderson canon. Corr. LM statistic applied for the checking of the under-identification of the structural equation. The test of whether the equation is identified, i.e., that the excluded instruments are "relevant", meaning that it is correlated with the endogenous variable. The significance of the test statistics suggested the rejection of the null of the equation is under-identified. So, the instrument is relevant. We used Cragg–Donald Wald F-statistic and Stock–Yogo weak ID test critical values to examine the weak identification of the instruments (Cragg and Donald 1993; Stock and Yogo 2005). The weak identification test is significant and suggested to rejects the null of weak identification. In our case, the over-identification test using the Sargan statistic and the LM test for redundancy test are not required, because our model is exactly identified. The coefficients derived from the 2SLS are similar to the control function results.
The durable expenditure is a part of the MPCE. If a households’ MPCE will increase there is a possibility of an increase in the durable expenditure of that family. If that is the case, then the instrument may not provide consistent results. To examine the above argument, we used the average level of the durable expenditure at the village level as the instruments. Our view is that, if the average level of the durable expenditure will increase at the village level, it will influence the income level of households because of the ratchet effect and demonstration effect. For instance, when most of the family will buy durable goods, the remaining households will also start buying. However, it is less likely that a household’s income can affect the village level durable expenditure at the same degree. The results are presented in Table 3, columns 2 and 4. The results by using the village level of the durable expenditure (See Table 3, columns 2 and 4) show that our coefficients are consistent with the household level of durable expenditure (See Table 3, columns 1 and 3) as an instrument. Therefore, we concluded that our results are not inconsistent due to the choice of instruments.
The calorie intake we have considered as the dependent variable may not reflect the actual level of calorie consumption for two reasons. First, NSSO data is under-reporting (Palmer-Jones and Sen 2001; Smith 2015; Gibson 2016) true consumption; because one person recalling the individual details of food consumption, may not able to capture the exact level of consumption of each member. Second, there might be guest meals served to other household members. These meals are not recorded as the consumptions of receiving households and considered as part of meals serving households. Hence, the nutrition received out of guest meals omitted from the recipients’ households and gets included in serving household expenditure. This will make the calorie-expenditure elasticity up-ward bias (Bouis and Haddad 1992). The former is likely to depress the reported per capita level of the calorie intake of the receiving household, and the latter will tend to inflate it of serving households. It is adjusted following Minhas (1991) to bring the calorie intake closer to the actual consumption.
NSSO data collected the individual-level information on detail meal consumption at home and outside the home. The decompositions of meal consumptions are, meal consumption at home, at schools, balwdies, ceremonies, from the employer as perquisites or part of wages, and on the payment basis at restaurants and hotels. The adjusted calorie intake of the households defined as
where \(Adj{\text{ C}}_{{\text{i}}}\) is the total adjusted calorie intake, \(M_{h}\) represents number of meals consumed by the household members in the household or received through purchase or as assistance or payment (excluding meals received from other households, \(M_{f}\) is number of meals received free from other households by households members, \(M_{g}\) is number of meals consumed by non-members as guest, employees, etc. This adjusted calorie is converted into log of per-capita calorie intake and then a similar procedure followed to as we had estimated Eq. (14). The adjusted results were presented in Fig. 7. The estimated coefficient using log of adjusted per capita per day calorie intake and adjusted per capita per day calorie intake were similar for variable of interest such as log of MPCE, relative price, diversification, share of medical and educational expenditure, and activity level for rural-and-urban area.


Source Author’s calculation
Quantile regression results (Dependent variable: log adjusted per-capita calorie intake). Note The red and yellow dots indicates the coefficient is significant at 5 and 10% level of significance level, respectively.
Discussion
Household Income/Expenditure and Calorie Demand
The results show that household income is enhancing the calorie demand and support the previous study (Shahraki et al. 2016). However, contrary to traditional wisdom, the magnitude of elasticities is smaller at lower quantile and higher at higher quantile in rural-and-urban areas. It indicated that increases in income of households associated with higher intensity of succeeding quantiles compare to preceding quantiles. This might be due to the calorie-poor household may willing to purchase a better quality of similar food as income increases. For instance, a family can buy rice at rupees 20/kg as well as at 40/kg. If a household was earlier purchasing rice at 20/kg, but after income rise purchases better quality of rice with 40/kg, then the elasticity will be low. Since our data set does not capture the quality of food items may lead to low estimated elasticity.
Calorie poor households may have a larger family size. Due to the calorie overhead or fixed cost, which leads to low-calorie intake, may be a reason why low elasticity is associated with calorie poor (Deaton and Paxson 1998). Furthermore, high-calorie intake households are richer as is evident from their higher per-capita real MPCE, and richer households have higher intake capacity than poorer households (Eli and Li 2015), this may have resulted in higher calorie-expenditure elasticities. Moreover, calorie poor probably spends more from the increased income on ‘temptation goods’ such as tobacco, alcohol (Banerjee and Mullainathan 2010), and on the festival, cultural and religious rituals (Banerjee and Duflo 2007, 2011) and that results in lower calorie-income elasticities. There has been increasing expenditure on non-food items, particularly on mobile recharge and fuel for two-wheeler at the expense of food in recent years among the calorie poor households. This may be a possible reason for the low-calorie elasticity of the calorie poor households. Low-calorie households may have settled for a self-fulfillment low-equilibrium because of aspiration failure (Dalton et al. 2016). These households may have little access to sanitation and safe drinking water and frequently fall ill, so even after the required food intake their health status does not improve (Duh and Spears 2017). Therefore, over time, they might have settled for a self-fulfillment low-equilibrium calorie consumption behavior.
The study findings are similar to Ravallion (1990), Subramanian and Deaton (1996), Jha et al. (2009), but different from the finding of Behrman and Deolalikar (1987) and Bouis and Haddad (1992).Footnote 9 Economic status affects the calorie demand level of households through the effect of food accessibility (Shahraki et al. 2016). Therefore, policy maker should focus on two aspects to improve calorie intake; first, pro-poor income enhancing strategies, and second, awareness programs that will educate the calorie poor on the benefit of spending on food and to decline diverting income towards non-food items. As a result, a household can improve economic level, and hence, can increase accessibility power. At the same time, it is necessary to conduct an awareness program, which will educate the calorie poor on the benefit of spending on food than non-food items.
Relative Price and Calorie Demand
The results of relative price are negatively influencing calorie demand. The calorie availability is more in cereal compare to the non-cereal items. Therefore, the rise in cereal prices decline calorie demand. But, the negative coefficients were closer to zero.
Although the coverage of food subsidies program is large in India, and become a major source of primary food for poor households, it is limited to rice and wheat. The exclusion and inclusion errorsFootnote 10 and food leakages are prime reasons to hinder the calorie demand of calorie poor households (Mahamallik and Sahu 2011; Dreze and Khera 2015). Besides, there are also other cereal items that are necessary for a healthy life and not provided at the subsidies rate. Therefore, probably, the rise in other cereal prices has a dominant power to affect the calorie demand of households adversely. As a result, households are facing the negative impact of an increase in relative cereal prices. Therefore, policy maker should focus to maintain food inflation stable. Along with policy maker should emphasise on effective implementation of the food subsidy programs, which can improve the calorie status of calorie poor.
Food Diversification and Calorie Demand
A major challenge for calorie demand comes from the dietary diversity of food consumption. Our results are in line with previous literature, except for a few lower quantiles in urban areas. With reference to calorie intake, dietary diversification implies a movement towards the expensive source of calories. The previous study argued that diversification is responsible for declining calorie intake (Behrman and Deolalikar 1989; Landy 2009; Mittal 2007). Along with the previous study, our results suggested that it is persistent for all quantiles in rural areas and urban areas except calorie poor households such as the bottom 4% in urban areas. Further, our results support the argument of Gaiha et al. (2012), which says that dietary diversification towards non-staple food items results in calorie intake decline.
Medical Expenditure and Calorie Demand
In rural-and-urban, the coefficients of the share of medical expenditure across quantiles are negatively significant, indicating an increase in household expenditure on health care will decline calorie demand. Therefore, medical expenditure is a major concern for rising out-of-pocket expenditure burden in private medicals. The rising burden of health expenditure has forced households to divert their resources from food consumption to medical expenditure. Thus, it is resulting in adverse effects on calorie intake. There are several reasons of increasing out-of-pocket expenditure in India which are as follows.
India is the home of one of the largest private health care provider in the world (Sharma 2015). Continuously declining medical expenditure of government, increasing investment of private entity, and increasing burden of diseases are significant predictors of household medical expenditure (Bhat 1996; Dev and Mooij 2002).
The national household survey shows that the private sector became the leading provider of inpatient care (Selvaraj and Karan 2009); it plays a dominant role in the existing health care systems. In the absence of the pre-financing mechanisms, such as insurance, leads to the higher expenditure burden of poor households (Ladusingh and Pandey 2013; Quintussi et al. 2015).
The public expenditure on health services has been declining at the national level. Per-capita health care expenditure is low compared to the middle-income countries Brazil, Russia, China and South Africa (Engelgau et al. 2012). As a result of the low level of public expenditure on health services, it came far below the expectation and failed to meet the health needs of people. Therefore, they are forced to take health services from private players (Berman et al. 2010).
During the 1990s, public expenditure on medical was squeezed at state levels (Dev and Mooij 2002); as a result, private players took the opportunity to enter into the market (Bhat 1996). Medical reform in the eighth five-year plan was introduced. Most of the state governments adopt the World Bank-sponsored medical system during the late 1990s to early 2000s and administrated medical policy, which led to the imposition of user fees at several times. Although fees were not applicable for below poverty line households, the choice and definition of the poor are arbitrary, which leads to the limited benefit of the poorest people (Thakur et al. 2009). On the other side, the evidence of out-of-pocket expenditure on medical has been increasing since 1994 (Ghosh 2011), and hence, adversely affecting calorie demand.
Treatments in the hospital are becoming expensive. About more than one-third of expense is paid out of borrowing money (Mahal et al. 2010). For inpatient care, drug expenditure accounts a larger portion of health expenditure (Garg and Karan 2009). For instance, drugs, diagnostic test, and medical appliance accounts more than half of the out-of-pocket expenditure on health (Mahal et al. 2010), which are mostly not covered by the public provision of health facilities.
Physical access is a barrier of rural populous for curative health services in the rural areas. The number of beds available for inpatient services is lower in public health services compare to private services, also, more in urban areas than in rural areas. The rapid development of private health services in urban than rural leads to the movement of rural poor to expensive private health centers located in urban areas. As a consequence, households are facing a higher financial burden (Selvaraj and Karan 2009).
Dissatisfaction in the quality of care in public health service is another reason for opting for private health services (Wagstaff 2002). The proportion of households spending on health has increased mostly in the poorest families (Yip and Mahal 2008). The policy recommendation of our findings suggested enhancing public spending to revive the public hospitals, so that, money burden of households can decline.
Education Expenditure and Calorie Demand
The results suggested an adverse effect of education spending on calorie demand. Although the Government of India has implemented Sarva Shiksha Abhiyan since 2001 and other initiatives, its' achievement is low. The private tutoring is rapidly expanding in India. Many students are receiving private tutoring in academic subjects outside the school hours and weekends. The students from urban, better economic background, and private schools are more likely to take private tutoring (Azam 2016). Demand for private tutoring is inelasticity at each level of schooling; therefore, private tutoring became a necessary good in the household consumption baskets (Azam 2016). As a result, the education burden has increased and led to an adverse impact on calorie demand. For instance, during 2007–08, the average annual expenditure for private tutoring of age between 5 and 29 pursuing primary education is Rs. 934, for middle Rs. 1394, and for secondary and higher secondary level Rs. 2898 (GOI 2010). Parents are motivated to spend in education due to the expectation of a higher return on education despite the higher cost of education. This leads to the higher burden and adversely affecting calorie intake.
During the early 1990s, the development policy on higher education, which introduced the new economic policy, had opened the door to the private player to invest in higher education (Tilak 1996). As a result, public disinvestment in higher education has increased rapidly, leading to a movement towards laissez-faireism in higher education (Tilak 2004). The faulty assumption of higher education is not a part of the development policy and withdrawing responsibility of states has been creating an adverse impact on households’ purchasing power. As returns on education are more for higher education than primary and secondary (Psacharopoulos and Patrinos 2004), the household is preferring to compensate for their spending on food items for higher education. Therefore, probably, households prefer to spend on education, often more on private education since 2004, which leads to a shortage of purchasing power to spend on food items. Ultimately, more education expenditure is reducing household calorie demand.
Quality of education is one of the primary determinants of choosing private schools. Despite the intervention of the government of India, the poor quality of teaching is associated with government schools due to the low teacher's attendance and behavior (Härmä 2011; Singh and Sarkar 2012). As a result, parents are choosing private schools to educate their children. The cost of private schooling is higher than public schooling; therefore, creating a huge burden for the household. From the above discussion and our results, it is concluded that government policy needs to be pro-active compare to the private player.
The movement of the coefficient indicated that as the quantile increase the magnitude of adverse impact increases in urban areas. It might be due to the threshold effect. For instance, calorie poor households are preferring government schools up to a certain threshold. After the threshold, they prefer private education, which causes an adverse impact on a larger extends relative to the calorie poor households.
Conclusions, Limitations and Future Research
This study examined predictors of household calorie demand using recent household-level data on consumer expenditure by using log of per-capita calorie intake as a proxy for calorie demand. Instead of applying usual regression analysis and assuming linearity, which considers whole sample conditional mean function E(yi/xi), we use quantile regression to identify intra-distributional impact. This study considered primary determinants such as the economic level of the household, relative price, diet diversification, the share of medical and education expenditure by controlling other possible household-level predictors.
The economic level of a household is positively affecting calorie demand in a rural-and-urban area with varied magnitude. The low intensity observed in lower quantile compares to the higher quantile. The policy maker should focus on both the pro-poor income growth strategy by creating space for income-generating sources and awareness programs on the importance of calorie-rich cereal items. As a result, a household can improve the economic level and will spend on cereal items, which will increase calorie intake.
There have been more concerns about an increase in food prices during the last decade. Therefore, higher price expects to dominate the purchasing power of poor households in rural-and-urban India. Our findings suggested that price have a significant adverse effect on calorie intake in rural-and-urban area. Policy maker should focus to maintain stable food inflation and should emphasis on effective implementation of the food subsidy programs. Food diversification is adversely affecting the calorie demand of households in rural and urban areas. The share of medical and education expenditure are major determinants of decline in calorie demand, probably due to a rapid deterioration of public investment, in turn, leading to insufficient net availability income to spend on food items. The policy recommendation of our findings suggested to adopt forward-looking medical and education policies such as free health facilities and free education to all by enhancing public spending to revive the public hospitals and to improve the quality of public education.
Limitations and Future Research
This study has the following limitations. There are varieties of socio-economic factors such as culture, taste, environment that affect household calorie demand. This study explicitly excluded these variables due to the unavailability of data in NSS. Though the inclusion of state, year, caste, and religion dummies capture some of these variations, these dummies may not be fully representative. Therefore, this study highlights a few essential predictors of the calorie demand in India based on policy relevance. In the discussion, we provided arguments to support our results using findings of previous studies and our personal conjectures. These personal conjectures can be used for empirical validation to explore more on why calorie intake has been declining.
Further, this study could not able to use quality-adjusted price due to lack of information in our data set (Silver and Heravi 2003); Besides the village and district level amenities, information on the better health of people, and market microstructure information’s are not available in the data set, which can be explored in future.
Notes
We have followed the conceptual difference and similarity between direct and indirect poverty from the existing literature by Sen (1981) and Ringen (1988). Moreover, these terminologies are used in the Indian context by Patnaik (2007, 2010, 2011) and Suryanarayana and Silva (2007), and other context by Lipton (1983, 1988). Direct poverty indicates the shortfall in per-capita calorie intake from benchmarking calorie level, whereas indirect poverty refers to the deficit in monthly per-capita expenditure from the expenditure-based poverty line. So, the calorie deprivation or calorie poor are otherwise named as direct poverty. We have used indirect, money metric, income, and expenditure-based poverty interchangeable.
Calorie availability and calorie intake are different. Some amount of calorie burns during the cooking process and there may be plate waste. Unfortunately, the amount of burned and wasted calorie is not measurable. Therefore, both have been used interchangeably.
NSS follows expenditure approach to measure household income, which used as proxy of income. Therefore, MPCE and income are used interchangeable.
The NSS is a large cross-sectional survey, which collects data on socio-demographic and household expenditure on different food and non-food items of Indian households. The survey has divided into Type I and II. We used type I survey. In this survey two types of recall period used for collection of data: Uniform reference period (URP) and mixed reference period (MRP). This involved asking people of their consumption of food and non-food items. Food items were cereals, pulses and pulses products, milk and milk products, sugar, edible oil, egg-fish-meat, vegetables, fruits, beverages, pan, tobacco, and intoxicants. Non-food items were consumption of energy for thirty-days. Under MRP method, data on less frequency such as health, education, clothing, durables, etc. were collected on a one-year basis and sticking to the thirty-days for rest of the items.
The consumer price index for agriculture and consumer price index for industrial worker used for rural and urban. The index data were obtained from Reserve Bank of India annual time series publication. The index was converted to 1960 base year priory to measure real MPCE.
CPIag and CPIiw industry are not available for each sub-group. Therefore, this study has deflated each subgroup with the CPIag for rural and CPIiw for urban household.
Similar procedure followed to deflate Medical and Educational expenditure as the diversification index. This onwards, we omitted share, and have written medical and education expenditure to minimise word count.
We categorised the activity level into three types; heavy activity, medium activity, and low activity. Low activity households includes Legislator, senior official, managers, professionals, administrative, executive, and managerial workers; Medium activity includes Technicians, Associates Professionals; High activity are Clerk, Services worker and shop and market sales workers, Skilled agriculture and fishery workers, Craft and related trade workers, Plant and machine operators and assemblers. We have dropped those households are not classified in NCO.
These studies have not examined movement of coefficients over the quantiles. They assumed linearity. However, in this study, we examined and shows the elasticities are not constant, rather, varying over the quantiles. Our study has similarities and dissimilarities by considering elasticities ranges. For instance, calorie-Income/expenditure elasticities estimated by Behrman and Deolalikar (1987) in between 0.17 to 0.37 statically insignificant at 5% level, suggesting close to zero. Bouis and Haddad (1992)elasticity estimate in the range 0.08 to 0.14. But statistically significant elasticities were found by Ravallion (1990), estimates elasticity of 0.15 at mean; Subramaniam and Deaton (1996), estimated it in the rage of 0.3 to 0.5; Jha, Gaiha and Sharma (2009) estimated elasticity was 0.06.
If a household is above the poverty line and receives benefits from food programs, known as inclusion error. If a household is below the poverty line and excluded from the benefit of the food programs, known as exclusion error. While the former is known as the Type-I error, the latter is Type-II error.
References
Abdulai, Awudu, and Dominique Aubert. 2004a. A cross section analysis of household demand for food and nutrients in Tanzania. Agricultural Economics 31: 67–79.
Abdulai, Awudu, and Dominique Aubert. 2004b. Nonparametric and parametric analysis of calorie consumption in Tanzania. Food Policy 29: 113–129.
Aromolaran, Adebayo B. 2004. Household income, women’s income share and food calorie intake in South Western Nigeria. Food Policy 29: 507–530. https://doi.org/10.1016/j.foodpol.2004.07.002.
Azam, Mehtabul. 2016. Private tutoring: Evidence from India. Review of Development Economics 20: 739–761. https://doi.org/10.1111/rode.12196.
Babatunde, Raphael Olanrewaju, Adedeji Olusayo Adejobi, and Segun Bamidele Fakayode. 2010. Income and calorie intake among farming households in rural Nigeria: Results of parametric and nonparametric analysis. Journal of Agricultural Science 2: 135–146. https://doi.org/10.5539/jas.v2n2p135.
Banerjee, Abhijit V., and Esther Duflo. 2007. The economic lives of the poor. Journal of Economic Perspectives 21: 141–167. https://doi.org/10.1257/jep.21.1.141.
Banerjee, Abhijit, and Esther Duflo. 2011. More than 1 billion people are hungry in the world. Foreign Policy 186: 66–72.
Banerjee, Abhijit, and Sendhil Mullainathan. 2010. The shape of temptation: Implications for the economic lives of the poor. Doi: 10.3386/w15973.
Basole, Amit, and Deepankar Basu. 2015. Fuelling calorie intake decline: Household-level evidence from rural India. World Development 68: 82–95. https://doi.org/10.1016/j.worlddev.2014.11.020.
Basu, Deepankar, and Amit Basole. 2013. An empirical investigation of the calorie consumption puzzle in India. Working Paper 2013–03.
Behrman, Jere R., and Anil B. Deolalikar. 1987. Will developing country nutrition improve with income ? A case study for rural south. Journal of Political Economy 95: 492–507.
Behrman, Jere R., and Anil Deolalikar. 1989. Is variety the spice of life ? Implications for calorie intake. The Review of Economics and Statistics 71: 666–672.
Behrman, Jere R., and Barbara L. Wolfe. 1984. More evidence on nutrition demand: Income seems overrated and women’s schooling underemphasized. Journal of Development Economics 14: 105–128. https://doi.org/10.1016/0304-3878(84)90045-2.
Berman, Peter, Rajeev Ahuja, and Laveesh Bhandari. 2010. The impoverishing effect of healthcare payments in India: New methodology and findings. Economic and Political Weekly 45: 65–71.
Bhalla, Surjit S. 2003. Recounting the poor: Poverty in India, 1983–99. Economic and Political Weekly 38: 338–349.
Bhat, R. 1996. Regulation of the private health sector in India. International Journal of Health Planning and Management 11: 253–274.
Bhuyan, B., B.K. Sahoo, and D. Suar. 2020. Nutritional status, poverty, and relative deprivation among socio-economic and gender groups in India: Is the growth inclusive? World Development Perspectives. https://doi.org/10.1016/j.wdp.2020.100180
Bouis, Howarth E. 1994. The effect of income on demand for food in poor countries: Are our food consumption databases giving us reliable estimates? Journal of Development Economics 44: 199–226. https://doi.org/10.1016/0304-3878(94)00012-3.
Bouis, Howarth E., and Lawrence J. Haddad. 1992. Are estimates of calorie-income elasticities too high? A recalibration of the plausible range. Journal of Development Economics 39: 333–364.
Breusch, T.S., and A.R. Pagan. 1979. A simple test for heteroscedasticity and random coefficient variation. Econometrica 47: 1287–1294.
Buchinsky, Moshe. 1995. Estimating the asymptotic covariance matrix for quantile regression models A Monte Carlo study. Journal of Econometrics 68: 303–338.
Buchinsky, Moshe. 1998. The dynamics of changes in the female wage distribution in the USA: A quantile regression approach. Journal of Applied Econometrics 13: 1–30.
Chand, Ramesh. 2010. Understanding the nature and causes of food inflation. Economic and Political Weekly 45: 10–13.
Chand, Ramesh, and Jaya Jumrani. 2013. Food security and undernourishment in India: Assessment of alternative norms and the income effect. Indian Journal of Agricultural Economics 68: 39–53.
Chandrasekhar, C. P., and Jayati Ghosh. 2003. The calorie consumption puzzle. The Hindu Business Line.
Cook, R.Dennis, and Sanford Weisberg. 1983. Diagnostics for heteroscedasticity in regression. Biometrika 70: 1–10.
Dalton, Patricio S., Sayantan Ghosal, and Anandi Mani. 2016. Poverty and aspirations failure. The Economic Journal 126: 165–188. https://doi.org/10.1111/ecoj.12210.
Datt, Gaurav, Martin Ravallion, and Rinku Murgai. 2016. Growth. Urbanization and Poverty Reducation in India. https://doi.org/10.3386/w21983.
Deaton, Angus. 2001. Counting the World’s poor: Problems and possible solutions. The World Bank Research Observer 16: 125–147. https://doi.org/10.1093/wbro/16.2.125.
Deaton, Angus, and Jean Drèze. 2009. Food and nutrition in India: Facts and interpretations. Economic and Political Weekly 44: 42–65.
Deaton, Angus, and Christina Paxson. 1998. Economies of scale, household size, and the demand for food. Journal of Political Econom 106: 897–930.
Dev, S. Mahendra, and Jos Mooij. 2002. Social sector expenditures in the 1990s: Analysis of central and state budgets. Economic and Political Weekly 37: 853–866.
Cragg, John G., and Donald, Stephen G . 1993. Testing identifiability and specification in instrumental variable models. Econometric Theory 9: 222–240.
Dreze, Jean, and Reetika Khera. 2015. Understanding leakages in the public distribution system. Economic and Political Weekly. 50: 39–42.
Duflo, E. 2003. Grandmothers and granddaughters: Old-age pensions and intrahousehold allocation in South Africa. The World Bank Economic Review 17: 1–25. https://doi.org/10.1093/wber/lhg013.
Duh, Josephine, and Dean Spears. 2017. Health and hunger: Disease, energy needs, and the indian calorie consumption puzzle. The Economic Journal 127: 2378–2409. https://doi.org/10.1111/ecoj.12417.
Efron, Bradley, and Robert J. Tibshirani. 1993. Introduction to the bootstrap world. Boca Raton: Chapman & Hall/CRC.
Eli, Shari, and Nicholas Li. 2015. Calorie Requirements and Food Consumption Patterns of the Poor. 21697. NBER Working Paper Series.
Engelgau, Michael M., Anup Karan, and Ajay Mahal. 2012. The economic impact of non-communicable diseases on households in India. Globalization and Health 8: 9–12. https://doi.org/10.1186/1744-8603-8-9.
FAO. 2009. Trade reforms and food security: Conceptualizing the linkages.
Faridi, R, and S.N. Wadood. 2010. An Econometric assessment of household food security in Bangladesh. Bangladesh Development Studies XXXIII: 1–15.
Gaiha, Raghav, Raghbendra Jha, and Vani S. Kulkarni. 2013. How pervasive is eating out in India? Journal of Asian and African Studies 48: 370–386. https://doi.org/10.1177/0021909612472040.
Gaiha, Raghav, N. Kaicker, K. Imai, V.S. Kulkarni, and G. Thapa. 2012. Has dietary transition slowed down in India: An analysis based on 50th, 61st and 66th Rounds of NSS. 2012/17. ASARC Working Paper.
Garg, Charu C., and Anup K. Karan. 2009. Reducing out-of-pocket expenditures to reduce poverty: A disaggregated analysis at rural–urban and state level in India. Health Policy and Planning 24: 116–128. https://doi.org/10.1093/heapol/czn046.
Ghosh, Soumitra. 2011. Catastrophic payments and impoverishment due to out-of-pocket health spending. Economic & Political Weekly 46: 63–70.
Gibson, John. 2016. Poverty measurement: We know less than policy makers realize. Asia and the Pacific Policy Studies 3: 430–442. https://doi.org/10.1002/app5.141.
Gibson, John, and Scott Rozelle. 2002. How elastic is calorie demand? Parametric, nonparametric and semiparametric results for urban Papua New Guinea. Journal of Development Studies 38: 23–46. https://doi.org/10.1080/00220380412331322571.
GOI. 2010. Education in India: 2007–08 Participation and Expenditure.
GOI. 2015. Report of the Committee on Private Final Consumption Expenditure.
Gopalan C, Ramasastri BV, Balasubramanian SG. Revised and updated by Rao BSN, Deosthale YB and Pant KC. 1993. Nutritive value of Indian foods. National Institute of Nutrition, Hyderabad, India. Hyderabad: National Institute of Nutrition.
Grimard, Franque. 1996. Does the poor’s consumption of calories respond to changes in income? Evidence from Pakistan. The Pakistan Development Review 35: 257–283.
Härmä, Joanna. 2011. Low cost private schooling in India: Is it pro poor and equitable? International Journal of Educational Development 31: 350–356. https://doi.org/10.1016/j.ijedudev.2011.01.003.
Huang, Jikun, and Cristina C. David. 1993. Demand for cereal grains in Asia: The effect of urbanization. Agricultural Economics 8: 107–124.
Ito, Shoichi, E. Wesley, F. Peterson, and Warren R. Grant. 1989. Rice in Asia: Is it becoming an Inferior good? American Journal of Agricultural Economics 71: 32–42. https://doi.org/10.2307/1241772.
Jha, Raghbendra, Raghav Gaiha, and Anurag Sharma. 2009. Modelling variety in consumption expenditure on food in India. International Review of Applied Economics 23: 503–519. https://doi.org/10.1080/02692170902954809.
Khera, Reetika. 2011. Trends in diversion of grain from the public distribution system. Economic and Political Weekly 46: 106–114.
Koenker, Roger. 2005. Quantile regression. Cambridge: Cambridge University Press.
Koenker, Roger, Gilbert Bassett, and Jr. 1978. Regression quantiles. Econometrica 46: 33–50.
Kozicka, Marta, Matthias Kalkuhl, and Jan Brockhaus. 2017. Food grain policies in India and their implications for stocks and fiscal costs: A dynamic partial equilibrium analysis. Journal of Agricultural Economics 68: 98–122. https://doi.org/10.1111/1477-9552.12176.
Kumar, P., Mruthyunjaya, and M.M. Dey. 2007. Long-term changes in Indian food basket and nutrition. Economic and Political Weekly 42: 3567–3572.
Ladusingh, Laishram, and Anamika Pandey. 2013. Health expenditure and impoverishment in India. Journal of Health Management 15: 57–74. https://doi.org/10.1177/0972063413486031.
Landy, Frédéric. 2009. India, “cultural density” and the model of food transition. Economic and Political Weekly 44: 59–61.
Lipton, M 1983. Poverty, undernutrition and hunger. The World Bank Staff Working Papers nos. 597. Washington, DC: World Bank.
Lipton, M. 1988. The poor and the poorest: Some interim findings. World Bank Discussion Paper 25. Washington: The World Bank.
Lundberg, Shelly J., Robert A. Pollak, and Terence J. Wales. 1997. Do husbands and wives pool their resources ? Evidence from the United Kingdom child benefit. The Journal of Human Resources 32: 463–480.
Mahadevan, Renuka, and Sandy Suardi. 2013. Is there a role for caste and religion in food security policy? A look at rural India. Economic Modelling 31: 58–69. https://doi.org/10.1016/j.econmod.2012.11.060.
Mahal, Ajay, Anup Karan, and Michael Engelgau. 2010. The economic implications of non-communicable disease for India. HNP Discussion paper.
Mahamallik, Motilal, and Gagan Bihari Sahu. 2011. Identification of the poor: Errors of exclusion and inclusion. Economic and Political Weekly 46: 71–77.
Meenakshi, J.V., and Brinda Vishwanathan. 2003. Calorie deprivation in rural India, 1983–1999/2000. Economic and Political Weekly 38: 369–375.
Mehta, Jaya, and Shanta Venkatraman. 2000. Poverty statistics: Bermicide’s feast. Economic and Political Weekly 35: 2377–2379+2381–2382.
Mendez, Michelle A., and Barry M. Popkin. 2004. Globalization, urbanization and nutritional change in the developing world. Electronic Journal of Agricultural and Development Economics 1: 220–241.
Minhas, B.S. 1991. On estimating the inadequacy of energy intakes: Revealed food consumption behaviour versus nutritional norms (nutritional statusof indian people in 1983). The Journal of Development Studies 28: 1–38. https://doi.org/10.1080/00220389108422220.
Mittal, Surabhi. 2007. What affects changes in cereal consumption? Economic and Political Weekly 42: 444–447.
Nair, Stanu R., and Leena Mary Eapen. 2012. Food price infation in India (2008 to 2010) A commodity-wise analysis of the causal factors. Economic and Political Weekly 47: 46–54.
Palmer-Jones, Richard, and Kunal Sen. 2001. On India’s Poverty Puzzles and Statistics of Poverty. Economic And Political Weekly 36: 211–217.
Panagariya, Arvind. 2013. Does India really suffer from worse child malnutrition than Sub-Saharan Africa? Economic and Political Weekly 48: 98–111.
Panagariya, Arvind, and Megha Mukim. 2014. A comprehensive analysis of poverty in India. Asian Development Review 31: 1–52.
Patnaik, Utsa. 2004. The republic of hunger. Social Scientist 32: 9–35.
Patnaik, Utsa. 2007. Neoliberalism and rural poverty in India. Economic and Political Weekly 42: 3132–3150.
Patnaik, U. 2010. A critical look at some propositions on consumption and poverty. Economic and Political Weekly 45 (6): 74–80.
Patnaik, U. 2011. On deepening poverty of the masses including deprived social groups in rural and urban India under economic reforms, in P.K Trivedi, ed., The Globalization Turbulence: Emerging Tensions in Indian Society. Delhi: Rawat Publications.
Psacharopoulos, George, and Harry Anthony Patrinos. 2004. Returns to investment in education: A further update. Education Economics 12: 111–134. https://doi.org/10.1080/0964529042000239140.
Quintussi, Marta, Ellen Van de Poel, Pradeep Panda, and Frans Rutten. 2015. Economic consequences of ill-health for households in northern rural India. BMC Health Services Research 15: 1–11. https://doi.org/10.1186/s12913-015-0833-0.
Rao, C.H.Hanumanth. 2000. Declining demand for food grains in rural India: Causes and implications. Economic and Political Weekly 35: 201–206.
Rao, Nitya. 2006. Land rights, gender equality and household food security: Exploring the conceptual links in the case of India. Food Policy 31: 180–193. https://doi.org/10.1016/j.foodpol.2005.10.006.
Ravallion, Martin. 1990. Income effects on undernutrition. Economic Development and Cultural Change 38: 489–515.
Ringen, S. 1988. Direct and indirect measures of poverty. Journal of Social Policy 17 (3): 351–365
Selvaraj, Sakthivel, and Karan, Anup K. 2009. Deepening Health Insecurity in India: Evidence from National Sample Surveys since 1980s. Economic and Political Weekly 44: 55–60.
Sen A. 1981. Poverty and famines: An essay on entitlement and deprivation. Oxford, UK: Clarendon Press.
Shahraki, Soudabeh Hamedi, Farshad Amirkhizi, Behzad Amirkhizi, and Sousan Hamedi. 2016. Household food insecurity is associated with nutritional status among iranian children. Ecology of Food and Nutrition 55: 473–490. https://doi.org/10.1080/03670244.2016.1212710.
Sharma, Smriti. 2015. Caste-based crimes and economic status: Evidence from India. Journal of Comparative Economics 43: 204–226. https://doi.org/10.1016/j.jce.2014.10.005.
Siddiqui, Md Zakaria, Ronald Donato, and Jaya Jumrani. 2017. Looking past the Indian calorie debate: What is happening to nutrition transition in India. Journal of Development Studies. https://doi.org/10.1080/00220388.2017.1408798.
Silver, Mick, and Saeed Heravi. 2003. In The measurement of quality-adjusted price changes. eds. Robert C. Feenstra and Matthew D. Shapiro. Vol. I. Chicago: University of Chicago Press.
Singh, Renu, and Sudipa Sarkar. 2012. Teaching quality counts: How student outcomes relate to quality of teaching in private and public schools in India. Young Lives.
Skoufias, Emmanuel. 2003. Is the calorie–income elasticity sensitive to price changes? Evidence from Indonesia. World Development 31: 1291–1307. https://doi.org/10.1016/S0305-750X(03)00070-6.
Skoufias, Emmanuel, Sailesh Tiwari, and Hassan Zaman. 2011. Crises, food prices, and the income elasticity of micronutrients: Estimates from Indonesia. World Bank Economic Review 26: 415–442. https://doi.org/10.1093/wber/lhr054.
Smith, Lisa C. 2015. The great Indian calorie debate: Explaining rising undernourishment during India’s rapid economic growth. Food Policy 50: 53–67. https://doi.org/10.1016/j.foodpol.2014.10.011.
Stock, James H., and Motohiro Yogo. 2005. Testing for weak instruments in Linear Iv regression. In Identification and inference for econometric models: Essays in honor of Thomas Rothenberg, eds. D. W. K. Andrews and J. H. Stock, 80–108. Cambridge: Cambridge University Press. doi:10.1017/CBO9780511614491.006.
Subramanian, Shankar, and Angus Deaton. 1996. The demand for food and calories. Journal of Political Economy 104: 133–162. https://doi.org/10.1086/262020.
Suryanarayana, M.H., and Dimitri Silva. 2007. Is targeting the poor a penalty on the food insecure? Poverty and food insecurity in India. Journal of Human Development 8: 89–107. https://doi.org/10.1080/14649880601101457.
Thakur, Harshad P., Soumitra Ghosh, M. Mariappan, and M Bhatia. 2009. User fees in India’s health sector: Can the poor hope for any respite? Artha Vijnana 51: 139–158.
Thomas, Duncan. 1990. Intra-household resource allocation: An inferential approach. The Journal of Human Resources 25: 635–664.
Tilak, Jandhyala B.G. 1996. How free is ’free primary education in India? Economic and Political Weekly 31: 275–282.
Tilak, Jandhyala B.G. 2004. Absence of policy and perspective in higher education. Economic and Political Weekly 39: 2159–2164.
Wagstaff, Adam. 2002. Poverty and health sector inequalities. Bulletin of the world health organization 80: 97–105.
Wooldridge, Jeff. 2007. What’s new in econometrics? Lecture 6 control functions and related methods. NBER Summer Institute.
Wooldridge, Jeff. 2010. Econometric analysis of cross section and panel data. Cambridge: MIT Press.
World Bank. 2017. World Development Indicators data base.
Yip, Winnie, and Ajay Mahal. 2008. The health care systems of China and India: Performance and future challenges. Health Affairs 27: 921–932. https://doi.org/10.1377/hlthaff.27.4.921.
Acknowledgements
We would like to thank the participants of the 18th World Congress of International Economic Association (IEA), Santa Fe, Mexico City for their helpful discussions of the earlier versions of the draft. We also thank the Minister of Human Resource Development, Government of India for providing financial support to carry out this research at the Indian Institute of Technology Kharagpur, Kharagpur, West Bengal, India. This study is a part of the Ph.D work of first author. The views expressed are of the authors only. The usual disclaimer applies.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix 1: Control Variables
Appendix 1: Control Variables
Castes
Similarly, among castes, majorities of STs and SCs, usually leaves in forest areas of India, where non-agricultural and agricultural job opportunities are limited, leading to their food insecurity. Household categorised by castes such as scheduled tribes, scheduled castes, other backward castes, and forward castes. Dummy variable were generated for each category. Forward caste treated as the reference category.
Religions
Among the religion, Muslims are more food insecure than the Hindus because of their sub-optimal food choices (Mahadevan and Suardi 2013). They have concentrated in backward states like Bihar, Uttar Pradesh, where job and educational opportunities are low. Religions were divided into Hindus, Muslims, and other minorities. All categories converted into separate dummy variable. References categories assigned to Hindus.
National Industrial Classifications
To account physical activity, we included four categorical dummies on the basis of the national industrial classifications. We have considered two digits to categories into agriculture, manufacturing, non-manufacturing, and service sector. Service sector assigned as the reference category.
State
Administrative set up and regional policies differed between Indian states, which is likely to influence calorie demand level of the households. Also, inter-state difference in food preference may influence on calorie demand. To control these influence, state dummy was used as control variables. Union territories are under control of the Government of India, leading to the similar administrative set up. Therefore, all union territories clubbed into single dummy variable. Dummy variable associated to the state of Odisha were used as the reference category.
Household Size
Household size directly influences choice and amount of varieties food items. Therefore, the effect of family size on calorie demand may increases at increasing rate or increases at decreasing rate. These effects controlled using the square of household size.
Age
Age and physical efficiency have a nonlinear relationship. Physical efficiency determines calorie intake through income. Therefore, the age of household head has a nonlinear effect on calorie intake, which controlled by the square of it. The child dependency was measured as the ratio between number of children aged below 14 and total number of family members.
Gender of the Household
In Indian society, women serve food to family members; look after children, and their concerns for calorie demand remains high compared to men. On an average, the income of women is 55% of men and contribution towards family welfare is about 70% (Mencher 1988 as cited in Rao 2006). Women do not prefer to spend on non-food items such as tobacco and intoxicants; however, their male counterpart does, particularly in the rural area. As a result, the proportion of spending on food items out of income is more for a female-headed household. Empirical research shows that households under the control of women spends more on education, nutrition, and health and less on personal material gain (Duflo 2003; Lundberg et al. 1997; Thomas 1990).Therefore, their control over household income may have a positive impact on calorie demand.
Gender of the household head used to control the effect of intra-household resources allocation, because in India, it is believed that resources controlled by female-headed households are properly utilised compare to their counterpart. Therefore, gender of the household head divided into the male-headed household and female-headed household. Male-headed household were used as reference category.
Household Head’s Years of Schooling
In this study, the education of household head categorised into the lower, middle, and higher education. Lower education includes below primary, whereas middle education covers from primary to secondary level. Above the secondary level was considered as higher education. The lower education used as a benchmark category in the regression analysis.
Household Type
Household livelihoods are classified for the rural area are self-employed in agriculture, self-employed in non-agriculture, regular wage/salary earnings, casual labour in agriculture, non-agriculture, others; and for urban area, self-employed, regular wage/salary earnings, casual labour, and others. For comparison of the 68th round (2011–12) with other two rounds, we have merged regular wage/salary earner and casual labour in non- agriculture in rural area, and named as “Other labours.” Dummy for other labours and regular wage/salary earner used as the reference category for rural-and-urban respectively.
Year
We have added years dummy to capture the transition of the economy over the years. Dummy assigned to 2004 is used as reference category.
Ration Card
We have used the ration card dummy variable.
Land Per-capita
Land per-capita is measured by dividing total land with the family size of household.
Rights and permissions
About this article

Cite this article
Bhuyan, B., Sahoo, B.K. & Suar, D. Quantile Regression Analysis of Predictors of Calorie Demand in India: An Implication for Sustainable Development Goals. J. Quant. Econ. 18, 825–859 (2020). https://doi.org/10.1007/s40953-020-00200-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40953-020-00200-4